Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Non-Pharmacological Interventions for Emotional Symptoms in COPD Centered on Anxiety and Depression: An Evidence Synthesis Study
Authors Yu J, Fu J, Zhao S, Zhang S, Huang R, Li T, Li Y ![]()
Received 16 October 2025
Accepted for publication 28 December 2025
Published 11 February 2026 Volume 2026:21 574777
DOI https://doi.org/10.2147/COPD.S574777
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Jie Yu,* Jianmei Fu,* Shujuan Zhao, Shuting Zhang, Rui Huang, Tong Li, Yulan Li
Department of Respiratory and Critical Care Medicine, Hebei CNPC Central Hospital, Langfang, Hebei, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yulan Li, Department of Respiratory and Critical Care Medicine, Hebei CNPC Central Hospital, No. 51, Xinkai Road, Guangyang District, Langfang, Hebei, 065000, People’s Republic of China, Email [email protected]
Abstract: Emotional symptoms, particularly anxiety and depression, are common in COPD patients but are often under-managed. This study aimed to synthesize evidence on non-pharmacological interventions for these symptoms in COPD. An umbrella review of guidelines, systematic reviews, and expert consensus was conducted. Literature searches were performed in databases including PubMed, Embase, Cochrane Library, CINAHL, Web of Science, CNKI, Wan Fang Data, and VIP, as well as guideline repositories (eg, GIN, NICE, GOLD) from January 1, 2000, to August 3, 2025. Inclusion criteria focused on moderate-to-severe COPD patients with anxiety/depression, non-pharmacological interventions, and evidence-based literature types (guidelines, systematic reviews, expert consensus). Literature quality was assessed using AGREE II for guidelines, AMSTAR 2 for systematic reviews, and JBI tools for expert consensus. Evidence was summarized and graded using the JBI evidence pre-grading system (2014). From 1812 identified records, 13 articles (4 guidelines, 2 expert consensuses, 7 systematic reviews) were included. Physical exercise training was the most strongly recommended intervention (Level 1a evidence, strong recommendation). Pulmonary rehabilitation, cognitive-behavioral therapy (including group, individual, and telephone-based formats), and psycho-educational interventions also showed consistent benefits (Level 1a-5b, strong recommendations). Evidence for mindfulness and relaxation techniques was less consistent. A total of 26 evidence statements were synthesized across six domains: psychological assessment, psychological interventions, exercise/nutrition, management models, special interventions, and other methods. A range of non-pharmacological interventions, particularly exercise and structured psychological therapies, can be effective for anxiety and depression in COPD and should be considered for integration into comprehensive care. Future research should address long-term effectiveness and cost-effectiveness.
Keywords: COPD, emotional symptom clusters, non-pharmacological interventions, cognitive behavioral therapy, pulmonary rehabilitation
Introduction
Chronic obstructive pulmonary disease (COPD) is a significant global health issue. Its progressive nature and characteristic symptoms, such as dyspnea, significantly impair patients’ quality of life and often lead to emotional symptoms, particularly anxiety and depression.1,2 Affective symptom clusters include lack of motivation, fatigue, feelings of loneliness, depressive mood, and anhedonia, referencing source.3 These emotional symptoms are prevalent in COPD patients, with studies indicating that approximately 13.93% to 23.37% of stable patients experience clinically significant anxiety or depressive symptoms.4 Compared to COPD patients without such symptoms, those with affective symptom clusters experience worse clinical outcomes, including increased risk of exacerbations, longer hospital stays, reduced treatment adherence, and greater healthcare burden.5–7 Current management of COPD primarily involves pharmacological and non-pharmacological interventions; however, the efficacy of pharmacological treatments varies significantly among individuals and may be associated with adverse reactions.8,9
Currently, clinical guidance specifically addressing the non-pharmacological management of emotional symptoms, especially anxiety and depression, in COPD remains insufficient. While major guidelines like GOLD acknowledge the issue, they offer limited specific recommendations.10 More importantly, a significant gap exists in the literature: a comprehensive synthesis that systematically identifies, critically appraises, and consolidates high-quality evidence on various non-pharmacological interventions (eg, psychological therapies, exercise training, integrated management models) is lacking. This gap hinders the translation of fragmented research findings into clear, actionable guidance for clinical practice. To address this, the present study, based on evidence-based principles, aims to systematically retrieve, evaluate, and summarize the best available evidence. The objective is to generate a structured summary of non-pharmacological interventions, complete with quality assessments and recommendation grades, to provide direct, evidence-based support for clinical decision-making in managing emotional symptoms in patients with COPD.
Materials and Methods
Problem Identification
According to the PIPOST model of the Evidence-Based Nursing Center at Fudan University, an evidence-based nursing question is formulated as follows:11 Population (P): Patients with moderate to severe COPD who experience complex emotions such as anxiety, depression, anger, or fear, and have difficulties in individual perception, emotional expression, and regulation. Intervention (I): Non-pharmacological intervention methods. Professional (P): Clinical practitioners such as doctors, psychologists, nurses, and rehabilitation therapists. Outcome O: Scales that can assess the emotional and psychological states of COPD patients, such as the Center for Epidemiologic Studies Depression Scale (CES-D), the Kessler Psychological Distress Scale (10-item or 6-item version), the Beck Depression Inventory-II (BDI-II), and the Emotion Regulation Questionnaire (ERQ); Setting: The location or scenario where the intervention is implemented, such as hospitals, communities, homes, etc. Type of evidence (Type of evidence T): Used to support the level of evidence, including guidelines, evidence summaries, clinical decision-making, best practices, systematic reviews, expert consensus.
Search Strategy
Literature Search: According to the “6S” evidence pyramid model,12 a computer-based search of domestic and international literature databases related to non-pharmacological interventions for emotional symptom clusters in COPD was conducted from the top to the bottom of the pyramid. Clinical decision support system websites included: UpToDate, BMJ Best Practice, etc.; guideline sources mainly included the Guidelines International Network (GIN), the Agency for Healthcare Research and Quality (AHRQ), the National Institute for Health and Clinical Excellence (NICE), the Scottish Intercollegiate Guidelines Network (SIGN), and Medlive Clinical Guidelines, etc. Global Initiative for Chronic Obstructive Lung Disease (GOLD), Chinese Medical Association (CMA), etc. PubMed, JBI Evidence-Based Healthcare Center (Joanna Briggs Institute, JBI), Embase, CINAHL, Web of Science, Cochrane Library, OVID, CNKI, VIP, Wan Fang Data, SinoMed. The search terms for literature mainly consist of four parts: the first part is COPD management/chronic obstructive pulmonary disease management, the second part is emotional symptoms/psychology/anxiety/mood disorders, the third part is non-pharmacological interventions/cognitive behavioral therapy/exercise therapy and other non-pharmacological interventions, and the fourth part is the type of literature retrieved such as systematic reviews/guidelines/expert consensus/meta-analysis. For example, the search formula: (COPD management or chronic obstructive pulmonary disease) and (psychology/anxiety/depression) and (non-pharmacological interventions), with the search time limit from January 1, 2000 to August 3, 2025. The specific search process is shown in Figure 1.
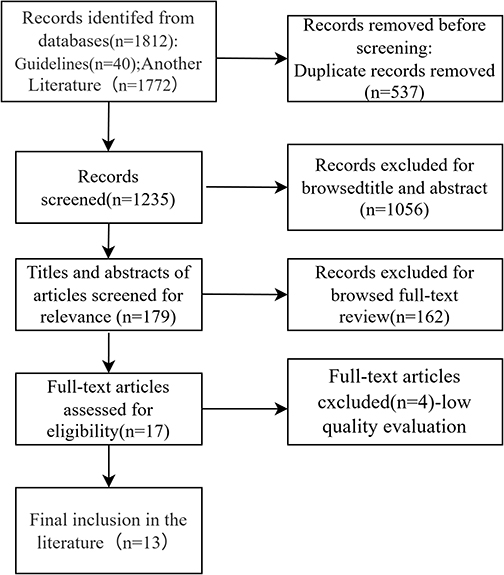 |
Figure 1 Flowchart of literature screening. |
Inclusion and Exclusion Criteria for Literature
Inclusion criteria: ① The study subjects are patients with moderate to severe COPD who have complex emotions such as anxiety/depression/anger/fear, and difficulties in individual perception, emotional expression, and regulation; ② The study involves various non-pharmacological interventions for COPD patients; ③ The types of literature include guidelines, evidence summaries, clinical decision-making, best practices, systematic reviews, and expert consensus; ④ The languages of the literature are English and Chinese.
Exclusion criteria: ① Literature with missing content; ② Literature published multiple times; ③ Literature with low quality evaluation.
Literature Quality Evaluation Criteria
The evaluation criteria for guidelines: The updated 2017 AGREE II system from the United Kingdom was employed,13 which is an internationally widely used clinical guideline evaluation tool. It includes six dimensions: scope and purpose, stakeholder involvement, rigor of development, clarity of presentation, applicability, and editorial independence, comprising a total of 23 items. Each item is scored from 1 to 7, where 1 indicates that the guideline completely fails to meet the criteria of the item, and 7 indicates that the guideline fully complies with the criteria of the item. The evaluators score each item, and the score for each dimension is the sum of the scores of all items within that dimension. The total score is then standardized using the following formula: ((Actual total score for each dimension - Minimum possible score) / (Maximum possible score for each dimension - Minimum possible score)) × 100%. A higher standardized score percentage indicates a higher level of evidence.
Systematic review criteria: The AMSTAR 2 assessment tool was employed.14 This evaluation criteria scale primarily includes 11 items, with each item indicated by “Yes,” “No,” “Unclear,” or “Not applicable.” The more items marked as “Yes” in the comprehensive assessment results, the higher the quality of the systematic review.
Evaluation criteria for expert consensus literature: The evaluation criteria developed by JBI for this type of literature were adopted.15 This evaluation tool includes 6 items, with each item represented by “Yes,” “No,” “Unclear,” or “Uncertain.” In the comprehensive assessment results, the higher the number of items marked as “Yes,” the higher the quality of the expert consensus.
Evidence Quality Assessment Process
Four researchers with expertise in evidence-based nursing evaluated the quality of the selected literature according to the literature quality assessment criteria. In cases where there was inconsistency in the evaluation results, an expert in the field of evidence-based nursing was invited to participate in the assessment, forming a quality evaluation panel to collectively discuss whether to include the literature.
Evidence Summary and Grading
Four researchers summarized and graded the evidence from the literature, with specific extraction and summarization requirements detailed in Table 1. After the evidence was extracted and summarized, the JBI Evidence Pre-grading and Evidence Recommendation Level System (2014 Edition) was used,16 which classifies evidence levels from 1 to 5, with each level further divided into sub-levels a-e, to stratify the evidence accordingly. Based on the JBI FAME structure, the applicability, adaptability, clinical significance, and effectiveness of the evidence were evaluated, and the recommendation strength of the evidence was categorized, with Grade A indicating strong recommendation and Grade B indicating weak recommendation. The detailed principles of evidence summarization are presented in Table 1.
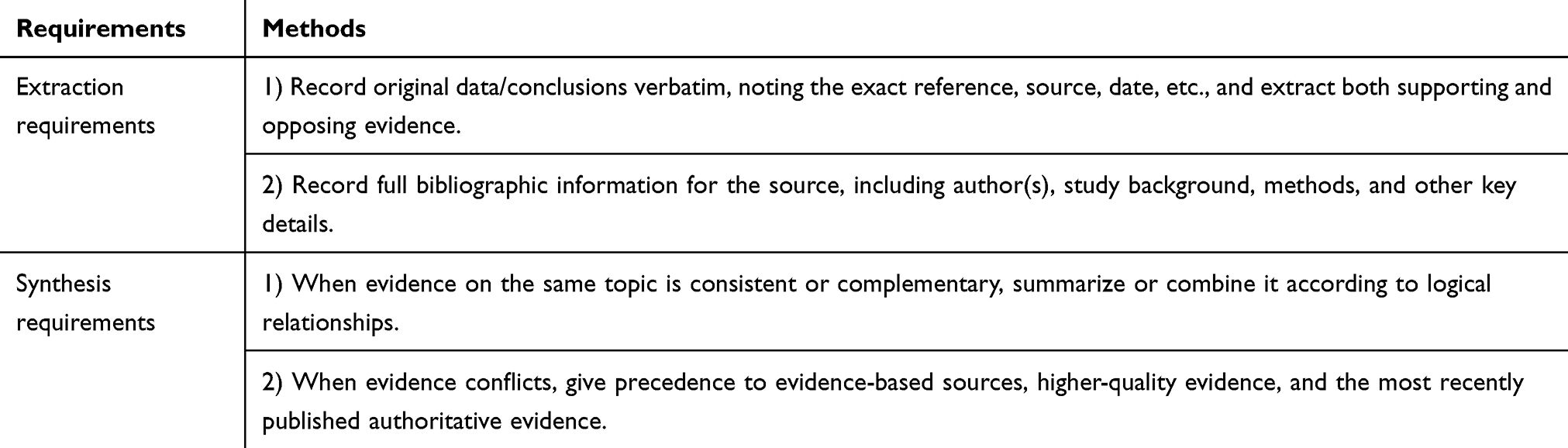 |
Table 1 Principles for Evidence Extraction and Synthesis |
Results
General Characteristics of Included Literature
A total of 1812 articles were included through searches of domestic and international medical official websites and databases. Duplicates were removed using the Zetero reference manager, and 1794 articles were excluded after reviewing their titles, tables of contents, abstracts, and keywords. An additional 5 articles were excluded after full-text review, resulting in a final inclusion of 13 articles, comprising 4 guidelines, 2 expert consensus documents, and 7 systematic reviews. The literature screening process is illustrated in Figure 1, and the basic characteristics of the included articles are presented in Table 2.
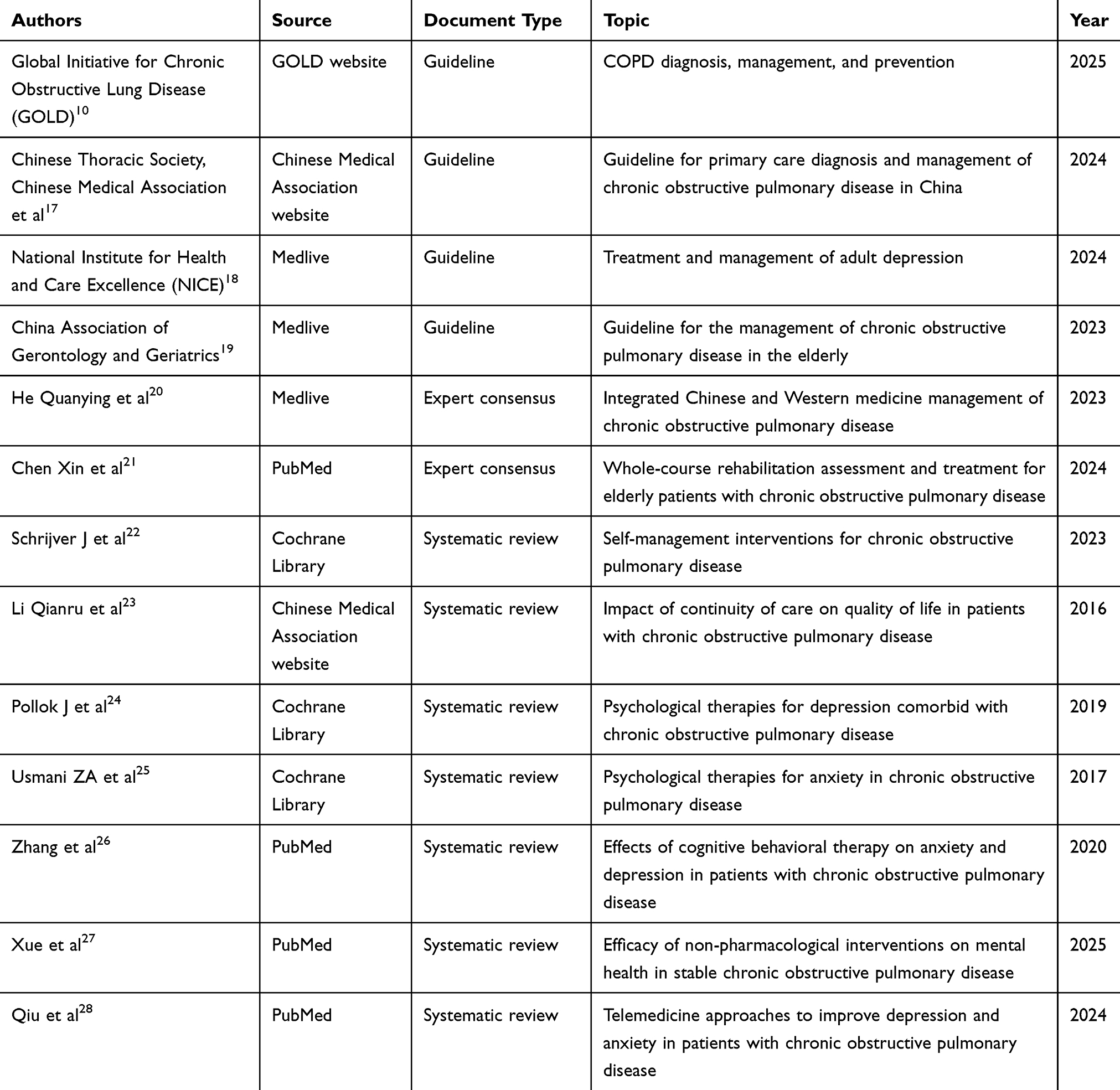 |
Table 2 Basic Characteristics of Included Literature |
Quality Assessment Results of Included Literature
Results of Guideline Quality Assessment
This study included a total of 4 guideline documents, which were evaluated using the AGREE II system. The specific quality assessment results are presented in Table 3. All four guideline documents had at least 4 domains with standardized percentages ≥60%. Consequently, 3 guidelines were classified as Grade A recommendations, and 1 guideline was classified as Grade B recommendation. All documents were considered high-quality guidelines and were eligible for inclusion.
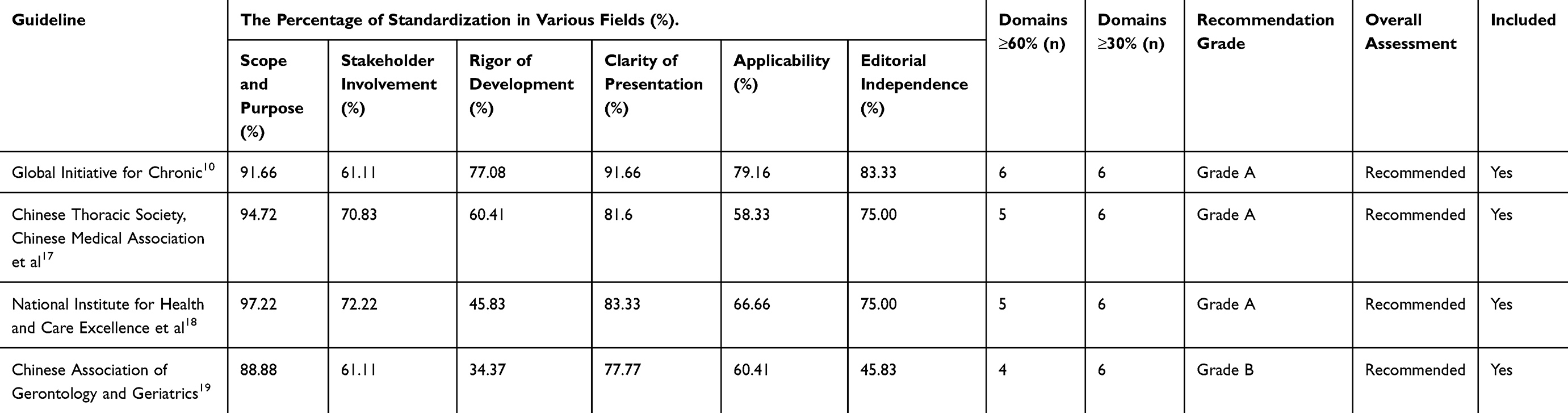 |
Table 3 Quality Assessment Results for the Included Guidelines |
Quality Assessment Results of Systematic Reviews
A total of 7 systematic review articles were included. The quality assessment was conducted according to the JBI systematic review criteria, with specific results presented in Table 4. Among these, 6 systematic review articles received “Yes” ratings for all 11 items. In the study by Xue et al,27 the assessment result for the item was the search strategy appropriate? was “No”. The quality of the results from all 7 systematic reviews was considered high, and they were approved for inclusion.
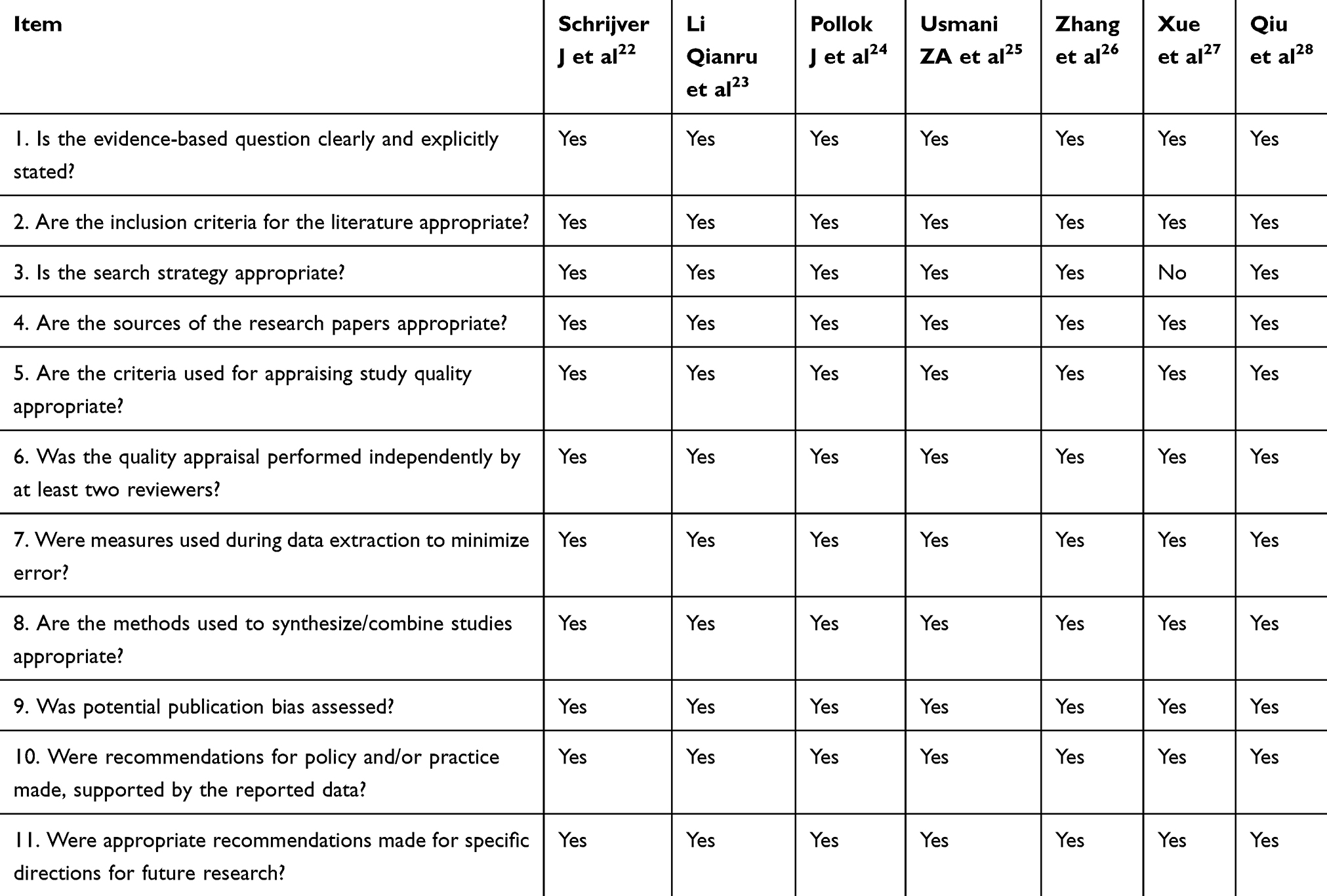 |
Table 4 Quality Assessment Results for the Included Systematic Reviews |
Quality Assessment Results of Expert Consensus
This study included a total of 2 expert consensus documents. The quality assessment was conducted using the corresponding JBI criteria, which comprised 6 items. After evaluation, both expert consensus documents received a “Yes” for each item, indicating high-quality literature that can be included.
Summary of Evidence
Based on the principles of evidence extraction and synthesis, the best recommended evidence was obtained from the 13 included articles. A total of 26 pieces of evidence were summarized and consolidated, primarily reflecting six aspects: emotional and psychological assessment and diagnosis, psychological intervention, exercise and nutritional intervention, management intervention models, special interventions, and other intervention methods. In terms of empirical support, physical exercise (particularly structured exercise training) and cognitive-behavioral therapy (CBT) received the most consistent high-level evidence support (Level 1a) and should be regarded as first-line core interventions. Pulmonary rehabilitation and psycho-educational interventions also demonstrated clear benefits (Levels 1a-5b). For clinical integration, these effective interventions can be combined according to an “assessment-psychological-exercise-management” framework to form individualized comprehensive management plans. Methods such as traditional exercises (eg, Tai Chi, Baduanjin) and relaxation training, whose evidence often originates from specific studies or cultural contexts, are recommended as supplements to the first two categories or as individualized choices based on patient preferences.
Therefore, it is advised to prioritize the recommendation and implementation of interventions with the highest strength of evidence, while also considering the feasibility of the interventions and patient preferences. This approach ensures that clinical practice is guided by the most robust evidence available, tailored to individual patient needs and circumstances, thereby optimizing the management of emotional symptoms in COPD patients.
The findings indicate that a hierarchical approach to intervention, starting with the most strongly evidence-supported strategies, provides a clear pathway for clinicians. Future research should continue to explore the long-term effectiveness and optimal combinations of these interventions within diverse patient populations and healthcare settings. Detailed evidence is presented in Table 5.
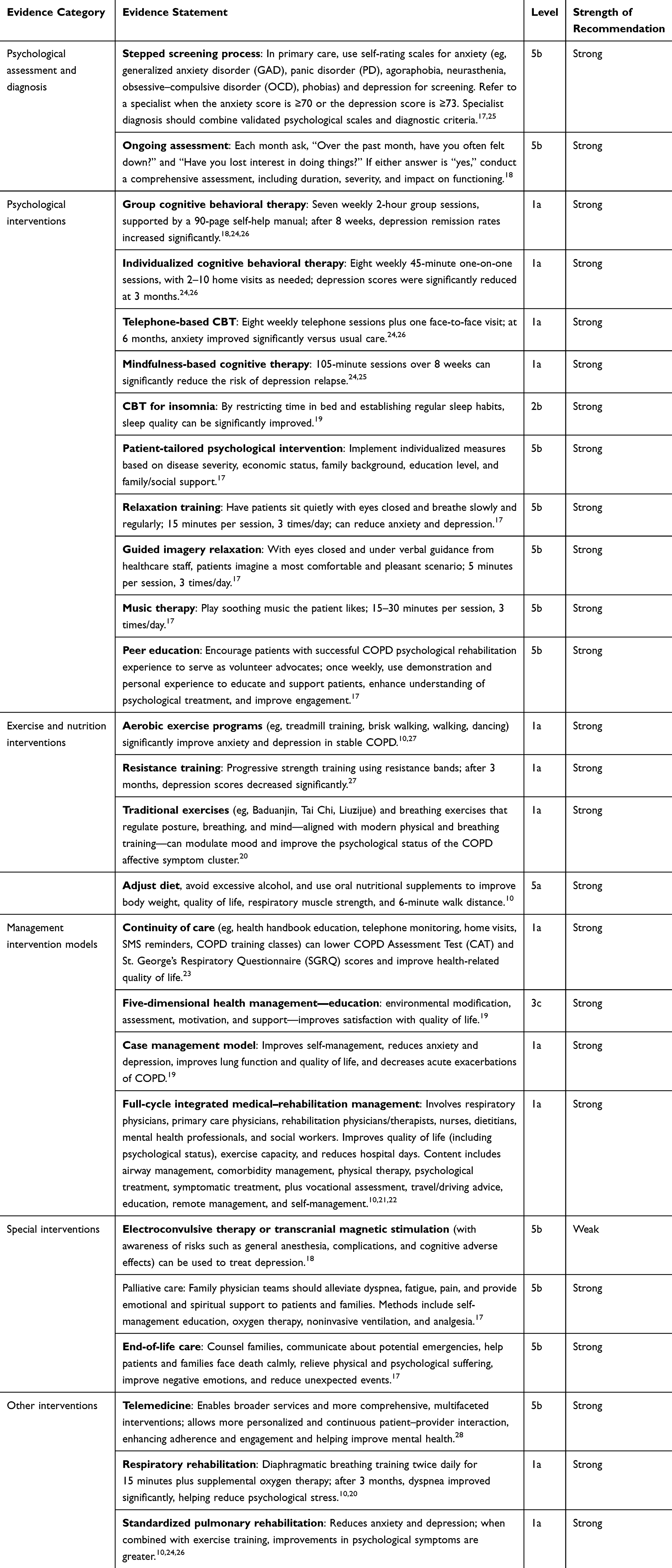 |
Table 5 Best Evidence Summary of Non-Pharmacological Interventions for the Affective Symptom Cluster in COPD |
Discussion
The Importance of Diagnostic Assessment of Emotional Symptoms in COPD Patients
The emotional symptoms in COPD patients are prone to be overlooked, and there is relatively less authoritative literature on the management of related emotional symptoms compared to the health management of COPD disease. However, the occurrence of emotional symptoms in COPD is gradually becoming a common phenomenon.29 Therefore, it is essential to pay attention to the emotional and psychological assessment and diagnosis of COPD patients and incorporate it into the diagnostic assessment of COPD. Currently, various assessment tools for psychological evaluation criteria, such as the Center for Epidemiologic Studies Depression Scale (CES-D) and the Self-Rating Anxiety Scale (SAS), are widely used. However, there is no psychological assessment diagnostic tool specifically developed for COPD, and the commonly used emotional and psychological assessment tools present certain issues in clinical practice. For instance, there is an overlap in symptoms, where clinical symptoms of COPD (eg, dyspnea, sleep disturbances) can be easily confused with emotional symptoms (eg, lack of energy, pessimistic insomnia). Furthermore, the screening of psychological symptoms is difficult to implement in primary healthcare settings as part of COPD diagnostic evaluation.30 It is recommended to integrate emotional and psychological assessment into the routine follow-up diagnosis of COPD. For example, the Canadian Thoracic Society’s “Recommendations for the Management of Chronic Obstructive Pulmonary Disease” (2022) suggests including psychological status screening in the comprehensive assessment of COPD.31
Psychotherapy is a Fundamental Measure to Improve the Emotional Symptoms of COPD Patients
A meta-analysis targeting COPD patients with comorbid anxiety and depression showed that the results support the potential of psychological interventions to improve the physical and mental health of COPD patients.32 Reaves, C et al applied a relaxation meditation technique (RRMT) that can elicit a relaxation response to the treatment of COPD patients and found that RRMT significantly improved the patients’ anxiety levels, recommending its incorporation into the rehabilitation care of COPD patients.33 Cognitive Behavioral Therapy (CBT) aims to break the vicious cycle of “negative cognition-negative emotions-problematic behaviors” by identifying and modifying automatic negative thoughts (eg, “I am definitely going to fail”) and maladaptive behavioral patterns (eg, avoiding social activities) that individuals generate in specific situations. It helps patients establish a more adaptive cognitive framework and coping strategies, ultimately alleviating emotional distress (such as anxiety and depression), improving social functioning, and enhancing quality of life. Therefore, CBT has significant advantages in ameliorating emotional symptoms in COPD.26 Combining group and individual cognitive intervention methods is a cost-effective non-pharmacological intervention for depression. Group cognitive interventions can stimulate the initiation of the treatment process in individuals with depression, while additional individual cognitive therapy can effectively sustain the treatment process. The two approaches complement each other to collectively improve patients’ depressive symptoms.34 The respiratory dysfunction present in COPD patients leads to certain sleep disturbances, which are often overlooked by the patients themselves. Therefore, cognitive behavioral interventions targeting sleep are of significant importance. A study involving 14 COPD patients with insomnia who underwent sleep cognitive behavioral therapy showed that this therapy significantly improved patients’ positive attitudes and beliefs towards sleep.35
Exercise and Nutritional Interventions Have Significant Auxiliary Value
Aerobic exercise and resistance training can improve patients’ mood by releasing endorphins and regulating inflammation.36 Traditional Chinese exercises (such as Tai Chi and Baduanjin) emphasize breath regulation and mental focus, achieving deep physical and psychological relaxation through intense concentration, mindful meditation, and breath control, which effectively alleviates stress and stabilizes emotions, offering distinct advantages in improving psychological well-being.37 However, the dyspnea symptoms of COPD often become the primary reason for patients’ reluctance to engage in exercise, necessitating the encouragement of self-motivated behavior.
Comprehensive Application of Other Specialized Non-Pharmacological Interventions
Other interventions play a synergistic role in the management of emotional symptoms. Pulmonary rehabilitation not only improves lung function in COPD patients but also has a positive impact on psychological symptoms. Through enhancing exercise endurance and reducing dyspnea symptoms in COPD patients, pulmonary rehabilitation leads to improved physical fitness, thereby increasing self-efficacy and enhancing psychological well-being.38 A randomized controlled trial conducted by Sohanpal, R. et al found that their tailored cognitive behavioral therapy for COPD patients with comorbid anxiety and depression may optimize the synergistic effects between psychological interventions and pulmonary rehabilitation interventions.39 However, many patients lack relevant knowledge, resulting in low overall participation compliance, frequent dropouts, and thus, pulmonary rehabilitation is not fully utilized, with accessibility and personalization urgently needing improvement.40 It is recommended to integrate pulmonary rehabilitation interventions into the comprehensive medical rehabilitation management throughout the entire cycle, enhancing the accessibility and continuity of rehabilitation. The applicability of electroconvulsive therapy and transcranial magnetic stimulation interventions should be noted. These therapies are generally applied to patients with severe depression, with risks including general anesthesia and complications such as cognitive impairment. Therefore, a risk assessment must be conducted, and treatment criteria must be met before proceeding with these therapies.18 The team led by Charlotte Scheerens successfully developed a palliative home care intervention approach and simulated clinical practice interventions, concluding that the early integration of palliative care (PC) into routine care could potentially improve the daily activity capacity, emotional state, and social functioning of patients with end-stage COPD.41
The Non-Pharmacological Intervention Management Model Improves Patients’ Emotional and Psychological States Through a Multidimensional, Interdisciplinary Collaborative Approach
Comprehensive full-cycle management and case management address the complex “physiological-psychological-social” needs of COPD patients by integrating multidisciplinary resources, including respiratory specialists, rehabilitation teams, and psychologists. For instance, the involvement of psychiatric departments directly targets the emotional symptoms of COPD patients,42 while the social support provided by social workers alleviates patients’ sense of isolation.43 Through health education and remote monitoring, patients transition from passive treatment recipients to active participants in their management, thereby enhancing compliance. Studies indicate that such interventions significantly reduce SGRQ scores (improving quality of life), supporting the research conclusion that continuous follow-up has a positive effect on emotional regulation.44 The “Education” and “Motivation” modules in the Five-Dimensional Health Management, along with personalized guidance in case management, all aim to enhance patients’ disease awareness and self-management skills, thereby reducing anxiety and depression caused by a sense of “loss of control.”.
In synthesizing the available evidence, a degree of variability in the effect estimates of certain interventions across different systematic reviews was observed. Regarding psychological interventions, while most studies support the beneficial effect of cognitive-behavioral therapy (CBT) on anxiety and depression, significant heterogeneity was noted in intervention parameters such as duration, frequency, and mode of delivery (group vs individual, face-to-face vs remote). This variability may influence the consistency of the reported effects. For exercise interventions, the evidence for aerobic and resistance training is relatively consistent. However, evidence for traditional exercises, such as Tai Chi and Baduanjin, predominantly originates from studies within specific cultural contexts, and their generalizability requires further validation. Furthermore, the recommended strength for mindfulness and relaxation techniques varied across studies, with some showing no significant difference compared to usual care. These inconsistencies may stem from methodological differences, variations in population characteristics, or the choice of outcome measures.
Future research needs to further clarify the optimal implementation protocols for each intervention and explore key moderating factors through subgroup analyses to provide more targeted recommendations. It is also important to note that the methodological quality of some included systematic reviews was only moderate.18,23,25 And primary studies often had limitations such as small sample sizes, difficulties in blinding implementation, and heterogeneity in control group settings. Additionally, although psychological interventions show positive effects, evidence regarding their long-term efficacy and effectiveness across different patient subgroups remains insufficient. Therefore, clinical application of these recommendations requires careful consideration of the specific context, and more high-quality studies with long-term follow-up are warranted to strengthen the evidence base.
The synthesis underscores that while promising interventions exist, their real-world application must be nuanced. Clinicians are advised to prioritize interventions with the strongest evidence, such as CBT and structured exercise, while remaining aware of the limitations and contextual factors affecting other modalities like mindfulness. Future work should aim not only to confirm efficacy but also to identify the specific circumstances under which each intervention is most beneficial, ultimately leading to more personalized and effective management strategies for emotional symptoms in COPD patients. This approach will bridge the gap between research evidence and clinical practice, improving patient outcomes.
Conclusions
In summary, this study screened the literature and extracted and summarized 26 pieces of best evidence to provide theoretical reference for healthcare professionals in the non-pharmacological intervention of emotional symptom clusters in COPD, covering six aspects: emotional and psychological assessment and diagnosis, psychological intervention, exercise and nutrition intervention, special intervention, management intervention models, and other interventions. The non-pharmacological interventions for emotional symptom clusters in COPD are diverse in form and rich in content. It is recommended that medical personnel provide personalized treatment and care plans based on the actual needs of patients and clinical scenarios to improve patients’ emotional and psychological conditions. This study also has certain limitations: the follow-up periods of most systematic reviews are relatively short (≤6 months), and there is a lack of cost-effectiveness analysis of non-pharmacological interventions, making it difficult to guide health resource allocation. The included guideline literature was predominantly from China. While this reflects the research activity in this field locally, it may introduce a certain degree of geographic bias. In the future, we will select literature such as systematic reviews with longer research cycles, and conduct economic evaluations of non-pharmacological interventions for emotional symptom clusters in COPD based on health economic evaluation criteria, in order to improve the cost-effectiveness of non-pharmacological interventions. And further expand the scope of international guideline retrieval to enhance the global representativeness of the evidence.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. GBD 2021 Causes of Death Collaborators. Global burden of 288 causes of death and life expectancy decomposition in 204 countries and territories and 811 subnational locations, 1990-2021: a systematic analysis for the Global Burden of Disease Study 2021, Lancet. 2024;403(10440):2100–14. Erratum in: Lancet. 2024 May 18;403(10440):1988. doi: 10.1016/S0140-6736(24)00824-9. PMID: 38582094; PMCID: PMC11126520. doi:10.1016/S0140-6736(24)00367-2
2. Zhang M, Zhao T. Research progress of knowledge assessment tools for chronic obstructive pulmonary disease. Evid Based Nurs. 2025;11(15):3098–3102. doi:10.12102/j.issn.2095-8668.2025.15.013
3. Jiayuan X, Nana L, Elli P, et al. Effects of urban living environments on mental health in adults. Nature Med. 2023;29(6):1456–1467. doi:10.1038/S41591-023-02365-W
4. Wu D, Zhao X, Huang D, et al. Outcomes associated with comorbid anxiety and depression among patients with stable COPD: a patient registry study in China. J Affect Disord. 2022;313:77–83. PMID: 35760193. doi:10.1016/j.jad.2022.06.059
5. Eisner MD, Blanc PD, Yelin EH, et al. Influence of anxiety on health outcomes in COPD. Thorax. 2010;65(3):229–234. PMID: 20335292; PMCID: PMC3111227. doi:10.1136/thx.2009.126201
6. Laurin C, Moullec G, Bacon SL, Lavoie KL. Impact of anxiety and depression on chronic obstructive pulmonary disease exacerbation risk. Am J Respir Crit Care Med. 2012;185(9):918–923. PMID: 22246177. doi:10.1164/rccm.201105-0939PP
7. Guarascio AJ, Ray SM, Finch CK, Self TH. The clinical and economic burden of chronic obstructive pulmonary disease in the USA. Clinicoecon Outcomes Res. 2013;5:235–245. PMID: 23818799; PMCID: PMC3694800. doi:10.2147/CEOR.S34321
8. Xu Y, Pang Y. Clinical efficacy of long-acting β2 agonists and long-acting muscarinic antagonist for moderate to severe chronic obstructive pulmonary disease. Pharm Chem J. 2023;57:365–372. doi:10.1007/s11094-023-02891-4
9. Lu C, Mao X. Risk of adverse reactions associated with inhaled corticosteroids for chronic obstructive pulmonary disease: a meta-analysis. Medicine. 2024;103(3):e36609. PMID: 38241558; PMCID: PMC10798756. doi:10.1097/MD.0000000000036609
10. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease (2025 Report). Available from: https://goldCOPD.org/2023-gold-report-2/.
11. Hu Y, Hao YF. Evidence-Based Nursing.
12. Alper BS, Haynes RB. EBHC pyramid 5.0 for accessing preappraised evidence and guidance. Evid Based Med. 2016;21(4):123–125. PMID: 27325531. doi:10.1136/ebmed-2016-110447
13. Brouwers MC, Kerkvliet K, Spithoff K. AGREE next steps consortium. The AGREE reporting checklist: a tool to improve reporting of clinical practice guidelines. BMJ. 2016;352:i1152. Erratum in: BMJ. 2016 Sep 06;354:i4852. doi: 10.1136/bmj.i4852. PMID: 26957104; PMCID: PMC5118873. doi:10.1136/bmj.i1152
14. Zhang F, Shen A, Zeng X, Qiang W, Jin Y. An introduction to AMSTAR 2: a critical appraisal tool for systematic reviews. Chin J Evid Based Cardiovasc Med. 2018;10(1):14–18.
15. The Joanna Briggs Institute. Critical appraisal tools [Internet]. 2017. Available from: http://joannabriggs.org/research/critical-appraisal-tools.
16. Wang CQ, Hu Y. JBI evidence pre-grading and evidence recommendation level system (2014 edition). J Adv Nurs Stud. 2015;11:964–967.
17. Chinese Medical Association, Chinese Medical Association Press, General Practice Branch of the Chinese Medical Association, et al. Chinese guideline for management of chronic obstructive pulmonary disease in primary care (2024). Chin J Gen Pract. 2024;23(6):578–602. doi:10.3760/cma.j.cn114798-20240326-00174
18. National Collaborating Centre for Mental Health (UK). Depression in Adults with a Chronic Physical Health Problem: Treatment and Management. PMID: 22259826. Leicester (UK): British Psychological Society (UK);2010.
19. The Gerontological Society of China and the Geriatric Medicine Society of China. Guidelines for the management of chronic obstructive pulmonary disease in the elderly. Res Integr Tradit Chin West Med. 2023;15(3):154–164. doi:10.3969/j.issn.1674-4616.2023.03.003
20. Expert Consensus Writing Group on Integrated Traditional Chinese and Western Medicine Management of Chronic Obstructive Pulmonary Disease. Expert consensus on integrated traditional Chinese and western medicine management for chronic obstructive pulmonary disease (2023 edition). Chin Gen Pract. 2023;26(35):4359–4371. doi:10.12114/j.issn.1007-9572.2023.0348
21. Chen X, Jia J, Ding YP, et al. Respiratory and rehabilitation expert consensus on full-cycle rehabilitation assessment and treatment for elderly patients with chronic obstructive pulmonary disease. J Rehabil. 2024;34(6):544–555. doi:10.3724/SP.J.1329.2024.06003
22. Schrijver J, Lenferink A, Brusse-Keizer M, et al. Self-management interventions for people with chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2022;1(1):CD002990. PMID: 35001366; PMCID: PMC8743569. doi:10.1002/14651858.CD002990.pub4
23. Li QR, Zhou YQ, Zou JH, et al. Effect of transitional care intervention on quality of life for patients with chronic obstructive pulmonary disease: a Meta-analysis. Chin J Pract Nurs. 2016;32(19):1508–1512. doi:10.3760/cma.j.issn.1672-7088.2016.19.019
24. Pollok J, van Agteren JE, Esterman AJ, Carson-Chahhoud KV. Psychological therapies for the treatment of depression in chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2019;3(3):CD012347. PMID: 30838649; PMCID: PMC6400788. doi:10.1002/14651858.CD012347.pub2
25. Usmani ZA, Carson KV, Heslop K, Esterman AJ, De Soyza A, Smith BJ. Psychological therapies for the treatment of anxiety disorders in chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2017;3(3):CD010673. PMID: 28322440; PMCID: PMC6464539. doi:10.1002/14651858.CD010673.pub2
26. Zhang X, Yin C, Tian W, Lu D, Yang X. Effects of cognitive behavioral therapy on anxiety and depression in patients with chronic obstructive pulmonary disease: a meta-analysis and systematic review. Clin Respir J. 2020;14(10):891–900. PMID: 32510764. doi:10.1111/crj.13226
27. Xue Y, Tang K, Liu H, Jin X. Efficacy of non-pharmacological interventions on psychological well-being in stable COPD: a systematic review and network meta-analysis. J Psychosom Res. 2025;196:112324. PMID: 40682982. doi:10.1016/j.jpsychores.2025.112324
28. Qiu YF, Hu JS, Wu M, et al. The effects of tele-based interventions for depression and anxiety symptoms in patients with Chronic Obstructive Pulmonary Disease (COPD): a systematic review and meta-analysis. Gen Hosp Psychiatry. 2024;91:143–150. PMID: 39481315. doi:10.1016/j.genhosppsych.2024.10.014
29. Zareifopoulos N, Bellou A, Spiropoulou A, Prevalence SK. Contribution to disease burden and management of comorbid depression and anxiety in chronic obstructive pulmonary disease: a narrative review. COPD. 2019;16(5–6):406–417. PMID: 31638445. doi:10.1080/15412555.2019.1679102
30. Yu A, Yu D. Study on the impact of the construction of public management system in rural areas on alleviating the mental pressure of rural residents. Psychiatry Danub. 2022;34:780.
31. O’Donnell DE, Aaron S, Bourbeau J, et al. Canadian thoracic society. Canadian thoracic society recommendations for management of chronic obstructive pulmonary disease--2003. Can Respir J. 2003;10:11A–65A. doi:10.1155/2003/567598
32. Farver-Vestergaard I, Danielsen JTT, Løkke A, Zachariae R. Psychosocial intervention in chronic obstructive pulmonary disease: meta-analysis of randomized controlled trials. Psychosom Med. 2022;84(3):347–358. PMID: 35067652. doi:10.1097/PSY.0000000000001043
33. Reaves C, Angosta AD. The relaxation response: influence on psychological and physiological responses in patients with COPD. Appl Nurs Res. 2021;57:151351. PMID: 32893088. doi:10.1016/j.apnr.2020.151351
34. Frick A, Thinnes I, Stangier U. Metta-based group meditation and individual cognitive behavioral therapy (MeCBT) for chronic depression: study protocol for a randomized controlled trial. Trials. 2020;21(1):20. PMID: 31907002; PMCID: PMC6945547. doi:10.1186/s13063-019-3815-4
35. Kapella MC, Herdegen JJ, Perlis ML, et al. Cognitive behavioral therapy for insomnia comorbid with COPD is feasible with preliminary evidence of positive sleep and fatigue effects. Int J Chron Obstruct Pulmon Dis. 2011;6:625–635. PMID: 22162648; PMCID: PMC3232169. doi:10.2147/COPD.S24858
36. Privitera GJ, Antonelli DE, Szal AL. An enjoyable distraction during exercise augments the positive effects of exercise on mood. J Sports Sci Med. 2014;13(2):266–270. PMID: 24790478; PMCID: PMC3990878.
37. Wu WW, Lan XY, Kuang HR, Jiang XY. The effects of traditional exercises on sleep quality in older adults: a Meta-analysis. Chin J Nurs. 2016;51(2):216–224. doi:10.3761/j.issn.0254-1769.2016.02.016
38. Yohannes AM, Casaburi R, Dryden S, Hanania NA. The effectiveness of pulmonary rehabilitation on chronic obstructive pulmonary disease patients with concurrent presence of comorbid depression and anxiety. Respir Med. 2022;197:106850. PMID: 35427843. doi:10.1016/j.rmed.2022.106850
39. Chan CL, Smuk M, Sohanpal R, Pinnock H, Taylor SJC. TANDEM Investigators. Tailored, psychological intervention for anxiety and/or depression in people with chronic obstructive pulmonary disease (COPD), TANDEM (Tailored intervention for ANxiety and DEpression Management in COPD): statistical analysis plan for a randomised controlled trial. Trials. 2020;21(1):858. PMID: 33059755; PMCID: PMC7559776. doi:10.1186/s13063-020-04786-1
40. Zhang XX, Zhu XX, Zhang Y, Wu NH, Gu F. Current status and reflections on pulmonary rehabilitation nursing management for patients with chronic obstructive pulmonary disease. J Tuberc Lung Dis. 2025;6(3):249–255. doi:10.19983/j.issn.2096-8493.20250044
41. Scheerens C, Chambaere K, Pardon K, et al. Development of a complex intervention for early integration of palliative home care into standard care for end-stage COPD patients: a Phase 0-I study. PLoS One. 2018;13(9):e0203326. PMID: 30231042; PMCID: PMC6145576. doi:10.1371/journal.pone.0203326
42. Yohannes AM, Kaplan A, Hanania NA. Anxiety and depression in chronic obstructive pulmonary disease: recognition and management. Cleve Clin J Med. 2018;85(2 Suppl 1):S11–S18. PMID: 29494328. doi:10.3949/ccjm.85.s1.03
43. Hirakawa Y, Aita K, Nishikawa M, Arai H, Miura H. Contemporary issues and practicalities in completing advance care planning for patients with severe COPD living alone: a qualitative study. J Soc Work End Life Palliat Care. 2022;18(1):80–95. PMID: 34605374. doi:10.1080/15524256.2021.1976353
44. Janjua S, Carter D, Threapleton CJ, Prigmore S, Disler RT. Telehealth interventions: remote monitoring and consultations for people with chronic obstructive pulmonary disease (COPD). Cochrane Database Syst Rev. 2021;7(7):CD013196. PMID: 34693988; PMCID: PMC8543678. doi:10.1002/14651858.CD013196.pub2
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Listen to Me! – A Mixed-Methods Study of Thoughts and Attitudes Towards Participation in Pulmonary Telerehabilitation Among People with Severe and Very Severe COPD Who Declined Participation in Pulmonary Rehabilitation
Skibdal KM, Emme C, Hansen H
Patient Preference and Adherence 2022, 16:2781-2798
Published Date: 18 October 2022
Effect of Singing on Symptoms in Stable COPD: A Systematic Review and Meta-Analysis
Fang X, Qiao Z, Yu X, Tian R, Liu K, Han W
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2893-2904
Published Date: 14 November 2022
Exploring the Presence of Implicit Bias Amongst Healthcare Professionals Who Refer Individuals Living with COPD to Pulmonary Rehabilitation with a Specific Focus Upon Smoking and Exercise
Barradell AC, Robertson N, Houchen-Wolloff L, Singh SJ
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:1287-1299
Published Date: 21 June 2023
Can Blood Biomarkers Be Used to Assess Oxidative Stress in COPD Patients After Pulmonary Rehabilitation
Beykumül A, Ersoy Y, Gülbaş G, Neselioglu S
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2179-2186
Published Date: 5 October 2023
Advocating for Action: Exploring the Potential of Virtual Reality in Breathing Exercise – A Review of The Clinical Applications
Alhammad SA
Patient Preference and Adherence 2024, 18:695-707
Published Date: 19 March 2024