Back to Journals » International Journal of Women's Health » Volume 18
Neglected Syphilis in Pregnancy Presenting as Condyloma Lata with Subsequent Congenital Syphilis: A Case Report
Authors Fitriyanto IA ![]() , Tjahyadi D
, Tjahyadi D
Received 18 March 2026
Accepted for publication 11 July 2026
Published 15 July 2026 Volume 2026:18 609265
DOI https://doi.org/10.2147/IJWH.S609265
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Iqbal Anugrah Fitriyanto,1 Dian Tjahyadi2
1Department of Obstetrics and Gynecology, Faculty of Medicine, Universitas Padjadjaran, Dr. Hasan Sadikin General Hospital, Bandung, Indonesia; 2Subdivision of Fertility and Reproductive Endocrinology, Department of Obstetrics and Gynecology, Faculty of Medicine, Universitas Padjadjaran, Dr. Hasan Sadikin General Hospital, Bandung, Indonesia
Correspondence: Iqbal Anugrah Fitriyanto, Department of Obstetrics and Gynecology, Faculty of Medicine, Universitas Padjadjaran, Dr. Hasan Sadikin General Hospital, Bandung, Indonesia, Tel +6281399962004, Email [email protected]
Purpose: The likelihood of developing concurrent infections, such as bacterial vaginosis (BV) and sexually transmitted syphilis, tends to increase. Delayed diagnosis of maternal syphilis may allow progression to secondary syphilis and substantially increase the risk of vertical transmission. We report a neglected case of syphilis during pregnancy presenting as condyloma lata with concurrent bacterial vaginosis that subsequently resulted in congenital syphilis.
Case Illustration: A 17-year-old married woman, gravida 1 para 0 abortus 0 (G1P0A0), at 34– 35 weeks of gestation, presented with progressively enlarging vulvar warty lesions for three weeks and malodorous vaginal discharge for one month. Physical examination demonstrated multiple confluent yellowish-white plaques involving both labia majora and the vaginal introitus, consistent with condyloma lata. Serological screening showed reactive TPHA and VDRL with non-reactive HIV and HBsAg. She was diagnosed with secondary syphilis presenting as condyloma lata, bacterial vaginosis, urinary tract infection, and premature uterine contractions. Treatment consisted of intramuscular benzathine penicillin G (2.4 million units) and oral metronidazole (2 g). Because labor progressed with extensive vulvovaginal lesions, an emergency cesarean section was performed. The newborn had reactive TPHA and VDRL and was diagnosed with congenital syphilis despite the absence of overt clinical manifestations.
Conclusion: This case highlights that delayed antenatal syphilis screening and late maternal treatment may allow progression to secondary syphilis with condyloma lata and increase the risk of congenital syphilis. Early screening and timely treatment are essential to prevent vertical transmission.
Keywords: syphilis in pregnancy, condyloma lata, congenital syphilis, vertical transmission, bacterial vaginosis
Introduction
Syphilis remains a major global public health concern and continues to affect millions of people worldwide. According to the World Health Organization (WHO), an estimated 8 million adults aged 15–49 years acquired syphilis in 2022, reflecting the persistent global burden of the disease despite the availability of effective screening and treatment strategies.1 Untreated maternal syphilis is associated with serious maternal, fetal, and neonatal complications, with adverse pregnancy outcomes occurring in approximately 50–80% of affected pregnancies.2,3 These complications include miscarriage, stillbirth, preterm birth, low birth weight, neonatal death, and congenital syphilis resulting from vertical transmission of Treponema pallidum.2,4 In 2022, WHO estimated approximately 700,000 congenital syphilis cases and 390,000 adverse birth outcomes worldwide, emphasizing the urgent need for early diagnosis and effective antenatal screening to eliminate mother-to-child transmission.1
Syphilis infection is conventionally categorized into four distinct clinical stages: primary, secondary, latent, and tertiary. Secondary syphilis is characterized by systemic manifestations, one of which is condyloma lata (CL), a highly infectious lesion presenting as broad, flat-topped, moist papules or plaques. CL has been reported in approximately 6–23% of patients with secondary syphilis.5,6 Early diagnosis through routine antenatal screening is essential to prevent maternal disease progression and vertical transmission.7,8
Bacterial vaginosis (BV) is the most common cause of vaginal dysbiosis among women of reproductive age and has been associated with adverse obstetric outcomes, including preterm labor, premature rupture of membranes, and postpartum infections.9–11 Pregnancy is accompanied by physiological, hormonal, and immunological adaptations, as well as alterations in the vaginal microbiota, which may influence susceptibility to specific genital tract infections rather than uniformly increasing the risk of all infections.12,13 These complex interactions may contribute to the coexistence of BV and sexually transmitted infections, including syphilis, particularly in the presence of behavioral and socioeconomic risk factors.12,14 Furthermore, BV has been associated with increased susceptibility to sexually transmitted infections, including syphilis, HIV infection, chlamydia, and gonorrhea, potentially complicating clinical management during pregnancy.10 Although condyloma lata in pregnancy has been reported, published cases describing neglected secondary syphilis presenting as condyloma lata concomitant with bacterial vaginosis and resulting in congenital syphilis remain limited.
This case report describes a pregnant woman with neglected secondary syphilis presenting as condyloma lata accompanied by bacterial vaginosis, resulting in congenital syphilis, who was managed at Dr. Hasan Sadikin General Hospital, Bandung, Indonesia, in January 2024. This case highlights the importance of routine antenatal screening, early diagnosis, and timely treatment in preventing severe maternal and neonatal complications.
Case Illustration
Clinical information was obtained through direct patient interview, physical examination, laboratory investigations, imaging studies, and review of the patient’s medical records.
A 17-year-old married woman, gravida 1 para 0 abortus 0 (G1P0A0), at approximately 34–35 weeks of gestation (8 months of pregnancy), initially presented to the Dermatology Outpatient Clinic at Dr. Hasan Sadikin General Hospital, Bandung, Indonesia, with multiple warty lesions around the vulva that had appeared 3 weeks before admission and progressively increased in number and size. She was subsequently referred to the Obstetrics Outpatient Clinic for further evaluation and management. The lesions were accompanied by intermittent pain in the pubic region without itching. She also complained of thick, malodorous vaginal discharge for one month but had not previously sought medical attention. Fetal movements were perceived normally. She denied watery vaginal discharge and lower urinary tract symptoms.
The patient had attended antenatal care only once at a midwife clinic. Her initial body mass index (BMI) during antenatal care was 20.28 kg/m2 (normal weight). She had no history of hypertension, diabetes mellitus, heart disease, asthma, or previous diagnosis or treatment for syphilis. She had never received COVID-19 vaccination.
Regarding her sexual history, the patient reported her first sexual intercourse at 13 years of age and had engaged in premarital sexual intercourse with more than five partners without barrier contraception. She married at the age of 17 years to her fifth sexual partner. Her husband was a 20-year-old laborer with an elementary school education. Information regarding her husband’s history of sexually transmitted infections and serological status was unavailable.
On physical examination, her general condition was good, and no cutaneous lesions suggestive of secondary syphilis were identified elsewhere on the body. No residual primary syphilitic chancre was observed. Examination of the external genitalia revealed multiple verrucous lesions of varying sizes involving both labia majora and extending into the vaginal introitus, consistent with condyloma lata (Figure 1). Venereological examination demonstrated no inguinal lymphadenopathy, and the pubic region appeared normal. The lesions on both labia majora were predominantly confluent, measuring approximately 0.5×0.5 cm to 3×5 cm, appearing as dry yellowish-white plaques arising from the skin surface. The labia minora and perianal region were unremarkable, with no ulceration or features suggestive of malignancy.
 |
Figure 1 Clinical appearance of condyloma lata involving the vulva. Multiple confluent yellowish-white, broad-based plaques involving both labia majora and extending into the vaginal introitus, consistent with condyloma lata as a manifestation of secondary syphilis. |
Gram staining of vaginal secretions demonstrated polymorphonuclear leukocytes (PMN) >30/high-power field, a positive whiff test, vaginal pH of 5, and no clue cells (Figure 2). Potassium hydroxide (KOH) examination of the vulvar lesions revealed no fungal elements (Figure 3).
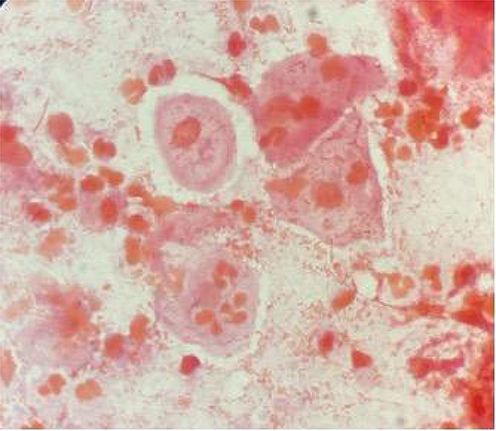 |
Figure 2 Gram examination of vaginal secretion shown negative clue cells. |
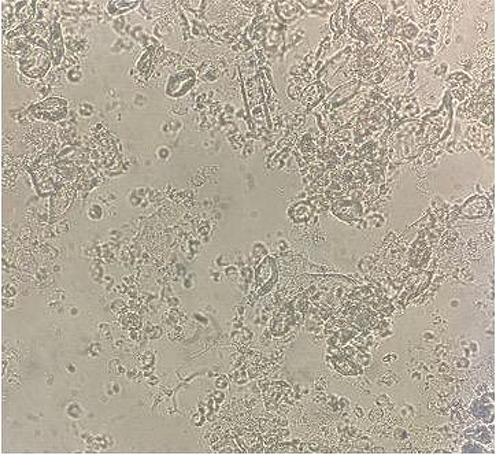 |
Figure 3 KOH result of the lesion. No fungal elements were identified on KOH examination. |
Serological screening showed non-reactive Human Immunodeficiency Virus (HIV) and hepatitis B surface antigen (HBsAg), whereas the Treponema pallidum hemagglutination assay (TPHA) and Venereal Disease Research Laboratory (VDRL) tests were qualitatively reactive. Quantitative serological testing was not performed.
Obstetric examination demonstrated a fundal height of 26 cm, fetal heart rate of 150–154 beats/minute, longitudinal cephalic presentation, intact membranes, and cervical dilatation of 1 cm. Obstetric ultrasonography demonstrated a singleton live intrauterine fetus corresponding to approximately 35 weeks and 2 days of gestation. Basic fetal biometry is shown in Figure 4, while fetal echocardiography demonstrated cardiomegaly with chamber dilatation and tricuspid valve regurgitation (Figure 5). Routine hematological investigations were unremarkable. Urinalysis demonstrated leukocyturia (695.4/µL) with significant bacteriuria (34,520.9/µL), consistent with urinary tract infection. The laboratory findings are summarized in Table 1.
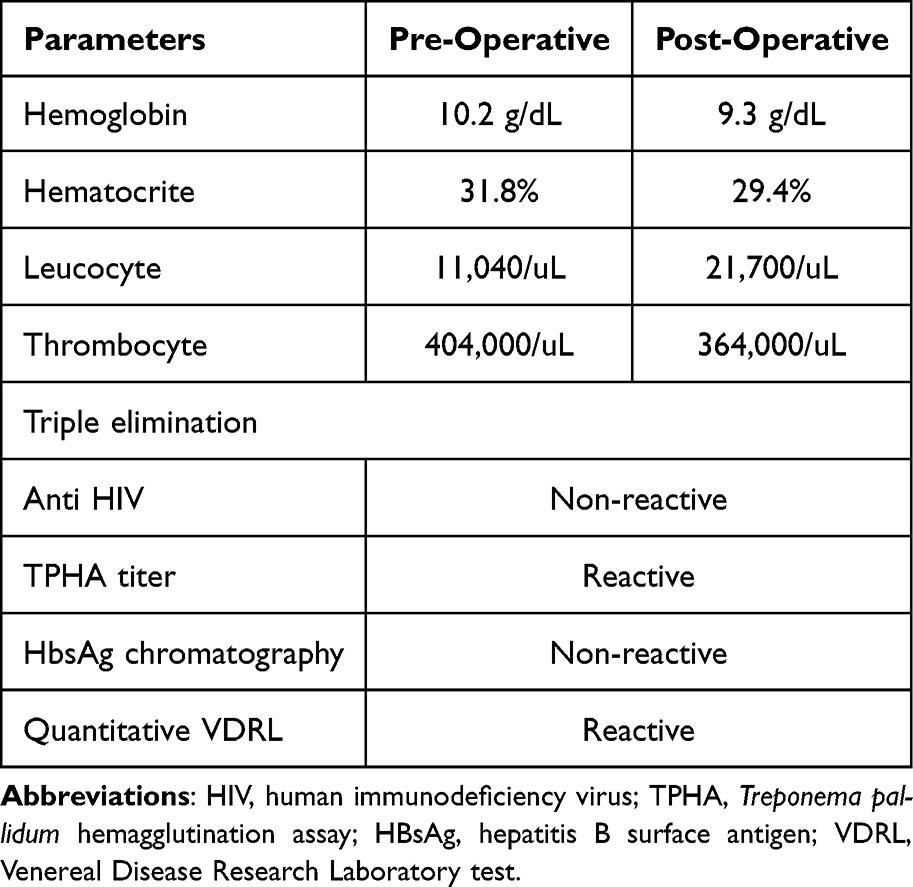 |
Table 1 Laboratory Result of the Patient |
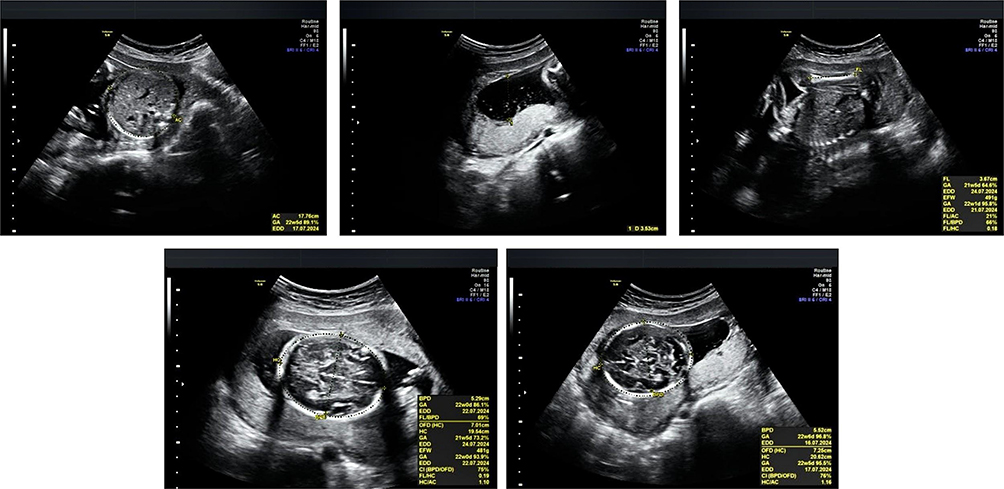 |
Figure 4 Obstetric ultrasonography showing fetal biometric assessment. |
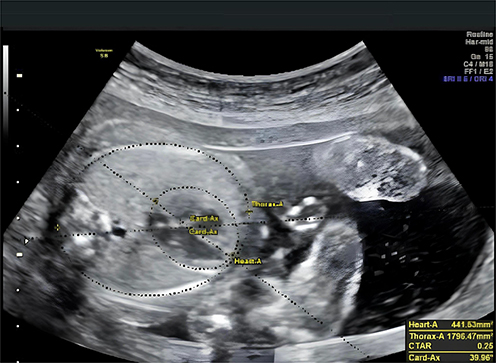 |
Figure 5 Fetal echocardiographic four-chamber view. Ultrasonography demonstrating cardiomegaly with chamber dilatation and tricuspid valve regurgitation. |
Based on the clinical findings and laboratory investigations, the patient was diagnosed with secondary syphilis presenting as condyloma lata, bacterial vaginosis, urinary tract infection, and premature uterine contractions at 34–35 weeks of gestation (G1P0A0). Conservative management was initiated with nifedipine as a tocolytic agent and four doses of dexamethasone for fetal lung maturation. Syphilis was treated with a single intramuscular dose of benzathine penicillin G (2.4 million units), while bacterial vaginosis was treated with a single oral dose of metronidazole (2 g).
After two days of hospitalization, uterine contractions increased in frequency and intensity despite conservative management. On the third hospital day, the patient entered active labor with cervical dilatation of 4 cm. An emergency cesarean section was performed because extensive condyloma lata involved both the vulva and vagina.
The infant was delivered without intraoperative complications and cried immediately after birth, with APGAR scores of 7 and 9 at one and five minutes, respectively. Physical examination revealed no respiratory distress, congenital anomalies, cardiac murmur, hepatosplenomegaly, jaundice, skin lesions, skeletal abnormalities, or other clinical manifestations suggestive of congenital syphilis. However, neonatal TPHA and VDRL tests were qualitatively reactive. Following evaluation by the Infection and Tropical Medicine Department, the infant was diagnosed with congenital syphilis based on maternal syphilis together with reactive neonatal serological findings despite the absence of overt clinical manifestations. A single intramuscular dose of benzathine penicillin G (100,000 U) was planned. Supportive neonatal management included fluid therapy, formula milk/breastfeeding, oxytetracycline ophthalmic ointment, intramuscular vitamin K (1 mg), and hepatitis B vaccination.
The postoperative course was uneventful, with no bleeding or signs of sepsis. Physical examination remained unremarkable. The patient received intravenous oxytocin infusion (20 IU in 500 mL Ringer’s lactate), oral amoxicillin (500 mg three times daily), and ketoprofen (100 mg twice daily) for postoperative management. She was discharged in stable condition on postoperative day 3. Laboratory findings are summarized in Table 1.
Discussion
Clinical Significance and Diagnostic Challenges of Condyloma Lata in Pregnancy
Condyloma lata is a characteristic mucocutaneous manifestation of secondary syphilis resulting from hematogenous dissemination of Treponema pallidum. Clinically, it presents as broad-based, flat-topped, moist or hypertrophic papules and plaques involving intertriginous areas, particularly the vulva and perianal region. Because these lesions may closely resemble condyloma acuminata caused by human papillomavirus (HPV), careful clinical assessment supported by serological testing is essential to establish the correct diagnosis and initiate appropriate treatment.5,6,15
In the present case, the patient presented with multiple confluent yellowish-white plaques involving both labia majora and extending into the vaginal introitus, accompanied by reactive TPHA and VDRL serological results. These findings were consistent with condyloma lata rather than condyloma acuminata. Although secondary syphilis is frequently accompanied by generalized rash, mucous patches, or systemic symptoms, condyloma lata may occasionally represent the predominant or only clinical manifestation, making diagnosis challenging and increasing the likelihood of delayed recognition.6,16
An important feature of this case was the delayed diagnosis during late pregnancy. The patient attended antenatal care only once and did not undergo routine antenatal screening for syphilis, allowing the infection to progress to secondary syphilis before appropriate treatment was initiated. This delay is clinically significant because secondary syphilis reflects active systemic dissemination with the highest burden of maternal spirochetemia, thereby substantially increasing the risk of vertical transmission.2,3,8
Early antenatal screening remains the cornerstone of preventing maternal complications and congenital syphilis, particularly among women with recognized behavioral and socioeconomic risk factors. In the present case, limited antenatal care and the absence of early syphilis screening likely contributed to delayed diagnosis and disease progression.2,4,17
Maternal Treatment Timing and Prevention of Congenital Syphilis
Vertical transmission of Treponema pallidum may occur at any stage of pregnancy, with the highest transmission risk occurring during primary and secondary syphilis because maternal spirochetemia is greatest during these stages. Untreated maternal syphilis is associated with miscarriage, stillbirth, preterm birth, neonatal death, and congenital syphilis, highlighting the importance of early antenatal screening and timely treatment.3,8
In this case, the patient first presented at 34–35 weeks of gestation with condyloma lata, indicating secondary syphilis. The diagnosis was established only in late pregnancy after the period during which fetal infection may already have occurred. Although benzathine penicillin G was administered immediately after diagnosis, treatment was initiated only a few days before delivery. Current guidelines recommend that maternal treatment should both follow the appropriate stage-specific penicillin regimen and be completed at least 30 days before delivery to effectively reduce the risk of congenital syphilis.2,4,18
The newborn had reactive TPHA and VDRL without clinical manifestations such as hepatosplenomegaly, jaundice, skin lesions, or skeletal abnormalities. Previous studies have demonstrated that many infants with congenital syphilis are asymptomatic at birth; therefore, diagnosis should integrate maternal history, neonatal serological findings, and assessment of treatment adequacy rather than relying solely on physical examination.19
Delayed diagnosis in this patient most likely reflected missed opportunities for antenatal screening rather than treatment failure. The WHO continues to identify inadequate antenatal syphilis screening as one of the major contributors to persistent congenital syphilis worldwide, particularly in resource-limited settings.1,17 This case therefore emphasizes that routine syphilis screening during early pregnancy, followed by prompt maternal treatment and partner management, remains essential to interrupt vertical transmission.10,18
Postpartum Management and Public Health Implications
Comprehensive postpartum management should include maternal serological follow-up, neonatal evaluation, partner notification, and counseling to prevent reinfection and subsequent adverse pregnancy outcomes. Maternal serological monitoring after treatment is essential to assess treatment response and identify possible reinfection, particularly when partner treatment has not been confirmed. Likewise, sexual partners should undergo clinical evaluation, serological testing, and appropriate treatment to interrupt ongoing transmission within the community.10,20
Although the newborn in this case had no overt clinical manifestations of congenital syphilis, reactive neonatal serology warranted further evaluation and pediatric follow-up. Congenital syphilis may be clinically silent at birth, and management should be guided by maternal treatment history, neonatal serological findings, and assessment of treatment adequacy rather than physical examination alone. Serial non-treponemal serological follow-up is recommended until serological resolution, because delayed manifestations involving the auditory, skeletal, or neurological systems may develop during infancy.19,21
This case also illustrates a missed opportunity for prevention through routine antenatal screening. The patient attended antenatal care only once and underwent syphilis testing only in late pregnancy, limiting the opportunity to prevent congenital infection. Strengthening universal antenatal screening programs, ensuring timely maternal treatment, and integrating partner management into routine obstetric care remain fundamental public health strategies to reduce the burden of congenital syphilis.1,3,17
Overall, this case highlights the importance of early antenatal syphilis screening, timely maternal treatment, multidisciplinary management, and comprehensive neonatal follow-up to prevent congenital syphilis and improve maternal and neonatal outcomes. In this case, long-term maternal and neonatal follow-up data were unavailable, and information regarding evaluation and treatment of the patient’s sexual partner could not be obtained. These limitations further emphasize the importance of comprehensive postpartum surveillance, partner management, and continued infant follow-up in preventing reinfection and improving outcomes in future pregnancies.
Conclusion
This case highlights the diagnostic challenges of secondary syphilis presenting as condyloma lata during pregnancy and underscores the importance of differentiating it from other anogenital lesions. Delayed antenatal screening and late diagnosis resulted in maternal treatment being initiated only shortly before delivery. This case also demonstrates that congenital syphilis may occur even in the absence of overt neonatal clinical manifestations, emphasizing the importance of maternal history, neonatal serological evaluation, and appropriate follow-up. Early universal antenatal syphilis screening, timely administration of benzathine penicillin G, partner evaluation and treatment, and multidisciplinary maternal–neonatal management remain essential strategies to reduce vertical transmission and improve maternal and neonatal outcomes.
Registration of Research Studies
Research registration was not required for this case.
Abbreviations
CL, condyloma lata; BV, bacterial vaginosis; STIs, sexually transmitted infections; BPG, benzathine penicillin G; HIV, human immunodeficiency virus; TPHA, Treponema pallidum hemagglutination assay; HBsAg, hepatitis B surface antigen; VDRL, Venereal Disease Research Laboratory test.
Ethical Approval
Institutional and departmental review boards determined that ethical approval was not required for this study.
Informed Consent Patient Statement
Written informed consent for publication of the case details and accompanying images was obtained from the patient’s parent after a full explanation of the case. The parent provided consent for the publication of this report and any accompanying images.
Acknowledgment
This publication charge was funded by Unpad through the Indonesian Endowment Fund for Education (LPDP) on behalf of the Indonesian Ministry of Higher Education, Science, and Technology and managed under the EQUITY Program (Contract No. 4030/B3/DT.03.08/2025 and 3927/UN6. RKT/HK.07.00/2025). The authors thank Anita Rachmawati for her guidance. The authors also thank the Obstetrics and Gynecology residents of Universitas Padjadjaran for technical support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study did not receive external funding.
Disclosure
The authors declare no conflicts of interest associated with this study.
References
1. World Health Organization. Syphilis. World Health Organization; 2025. Available from: https://www.who.int/news-room/fact-sheets/detail/syphilis.
2. Stafford IA, Workowski KA, Bachmann LH. Syphilis complicating pregnancy and congenital syphilis. N Engl J Med. 2024;390(3):242–9. doi:10.1056/NEJMra2202762
3. Gomez GB, Kamb ML, Newman LM, Mark J, Broutet N, Hawkes SJ. Untreated maternal syphilis and adverse outcomes of pregnancy: a systematic review and meta-analysis. Bull World Health Organ. 2013;91(3):217–226. doi:10.2471/BLT.12.107623
4. World Health Organization. WHO Guideline on Syphilis Screening and Treatment for Pregnant Women. World Health Organization; 2017.
5. Kang S, Amagai M, Bruckner AL, et al. Fitzpatrick’s Dermatology.
6. Pourang A, Fung MA, Tartar D, Brassard A. Condyloma lata in secondary syphilis. JAAD Case Rep. 2021;10:18–21. doi:10.1016/j.jdcr.2021.01.025
7. Rahman MM, Abdul Wahab A, Ali UK, Mohammad M, Md. Monoto EM. Syphilis in pregnancy. Pak J Med Sci. 2014;31(1). doi:10.12669/pjms.311.5932
8. De Santis M, De Luca C, Mappa I, et al. Syphilis infection during pregnancy: fetal risks and clinical management. Infect Dis Obstet Gynecol. 2012;2012:1–5. doi:10.1155/2012/430585
9. Chen X, Lu Y, Chen T, Li R. The female vaginal microbiome in health and bacterial vaginosis. Front Cell Infect Microbiol. 2021;11. doi:10.3389/fcimb.2021.631972
10. Dalby J, Stoner BP. Sexually transmitted infections: updates from the 2021 CDC guidelines. Am Fam Physician. 2022;105(5):514–520.
11. Ng BK, Chuah JN, Cheah FC, et al. Maternal and fetal outcomes of pregnant women with bacterial vaginosis. Front Surg. 2023:10. doi:10.3389/fsurg.2023.1084867
12. Mor G, Aldo P, Alvero AB. The unique immunological and microbial aspects of pregnancy. Nat Rev Immunol. 2017;17(8):469–482. doi:10.1038/nri.2017.64
13. Koren O, Goodrich JK, Cullender TC, et al. Host remodeling of the gut microbiome and metabolic changes during pregnancy. Cell. 2012;150(3):470–480. doi:10.1016/j.cell.2012.07.008
14. Van Gerwen OT, Muzny CA, Marrazzo JM. Sexually transmitted infections and female reproductive health. Nat Microbiol. 2022;7(8):1116–1126. doi:10.1038/s41564-022-01177-x
15. Deshpande DJ, Nayak CS, Mishra SN, Dhurat RS. Verrucous condyloma lata mimicking condyloma acuminata: an unusual presentation. Indian J Sex Transm Dis AIDS. 2009;30(2):100–102. doi:10.4103/0253-7184.62766
16. Escamilla Galindo EP, Barahona San Millan E, Del Rosario Lorenzo SN, et al. Condyloma Lata: a Vulvar Manifestation of Secondary Syphilis. J Clin Gynecol Obstet. 2024;13(2):41–47. doi:10.14740/jcgo960
17. Elendu C, Amaechi DC, Elendu ID, et al. Global perspectives on the burden of sexually transmitted diseases: a narrative review. Medicine. 2024;103(20):e38199. doi:10.1097/MD.0000000000038199
18. Kementerian Kesehatan RI. Pedoman Program Pencegahan Penularan HIV, Sifilis, Dan Hepatitis B Dari Ibu Ke Anak. 2019.
19. Sankaran D, Partridge E, Lakshminrusimha S. Congenital Syphilis—An Illustrative Review. Children. 2023;10(8):1310. doi:10.3390/children10081310
20. Kingston M, Wilson J, Dermont S, et al. British Association of Sexual Health and HIV (BASHH) UK guidelines for the management of syphilis in pregnancy and children 2024. Int J STD AIDS. 2024;35(14):1161–1173. doi:10.1177/09564624241280387
21. Salomè S, Cambriglia MD, Montesano G, Capasso L, Raimondi F. Congenital syphilis: a re-emerging but preventable infection. Pathogens. 2024;13(6):481. doi:10.3390/pathogens13060481
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Unilateral Twin Ectopic Pregnancy: A Case Report from the Eastern Part of Ethiopia, Harar
Gure Eticha T
International Medical Case Reports Journal 2022, 15:521-527
Published Date: 19 September 2022
Pregnancy Associated Invasive Apocrine Carcinoma of the Breast: Case Report from Ethiopia
Alemu HK, Hammad N, Tola MA, Vanderpuye V
Breast Cancer: Targets and Therapy 2023, 15:429-433
Published Date: 23 June 2023
A Case Report of Pregnancy Complicated with Primary Hemophagocytic Lymphohistiocytosis
Chen Y, Huang X, Chen H, Tong J, Huang L, Su J, Deng L
International Journal of Women's Health 2024, 16:843-851
Published Date: 17 May 2024
Diagnosis and Management Challenges of Spontaneous Quadruplet Pregnancy in a Resource-Limited Setting: A Case Report
Tjandraprawira KD, Santoso DPJ, Bayuaji H, Nugrahani AD, Susandi D
International Medical Case Reports Journal 2025, 18:325-332
Published Date: 11 March 2025
Acute Myocardial Infarction Due to Spontaneous Coronary Dissection in Pregnancy: A Case Report and Management Considerations
Hrebenyk M, Komorovsky R, Zhehestovska D, Oryshchyn L, Kotsyuba O, Zelenenka L
International Journal of Women's Health 2025, 17:1923-1932
Published Date: 5 July 2025