Back to Journals » International Medical Case Reports Journal » Volume 15
Unilateral Twin Ectopic Pregnancy: A Case Report from the Eastern Part of Ethiopia, Harar
Authors Gure Eticha T ![]()
Received 17 July 2022
Accepted for publication 15 September 2022
Published 19 September 2022 Volume 2022:15 Pages 521—527
DOI https://doi.org/10.2147/IMCRJ.S382708
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ronald Prineas
Tadesse Gure Eticha
Department of Obstetrics and Gynecology, Haramaya University, Harar, Ethiopia
Correspondence: Tadesse Gure Eticha, Tel +251913868714, Email [email protected]
Introduction: Twin ectopic pregnancy is the implantation of both embryos outside of the endometrial lining occurring in 1 in 20,000 up to 1 in 125,000 pregnancies. Commonly, twin ectopic pregnancies occur inside the fallopian tube either unilateral or bilateral. Unless early diagnosis and interventions are made, it may rupture causing intraperitoneal bleeding with a high risk of maternal death.
Case Report: I am reporting a rare type of ectopic pregnancy: unilateral twin ectopic pregnancy with positive cardiac activity on the left side of the fallopian tube in a 30 years old gravida III para II mother. Left side salpingectomy was done for her and discharged from the hospital after two postoperative days.
Conclusion: Twin ectopic pregnancy with a live embryo is a very rare type of pregnancy that needs a high index of suspicion to diagnose and treat early to prevent complications and maternal death.
Keywords: twin ectopic, pregnancy, unilateral, case report, Ethiopia
Introduction
Two embryos or blastocysts implanting outside of the uterine cavity is known as a twin ectopic pregnancy. Though it may implant in other locations, the twin ectopic often implants in the fallopian tube. Ectopic pregnancies are typically discovered after tubal rupture in low-income countries; which is associated with the high rate of maternal mortality and morbidity unless they are identified and treated timely. Twin ectopic pregnancies are harder to identify than singleton ectopic pregnancies, and they are also more dangerous for the mother and have higher rates of morbidity and mortality. Because of this, preventing morbidity and death requires early identification and treatment.
Case Description
A 30 years old gravida III para II (both by cesarean section and alive), whose gestational age from her last menstrual period was 6 weeks plus five days presented with the chief complaint of lower abdominal and back pain of one-week duration. Other than the pain, she had no vaginal bleeding, blurring of vision, tinnitus, vertigo, headache, nausea, or vomiting. She never had a history of sexually transmitted diseases or infertility treatment. Except for the two cesarean sections, she never had other types of abdominopelvic surgeries.
On physical examination, her vital sign was stable with Blood Pressure =125/82mmhg, Pulse Rate = 84bpm, Respiratory Rate = 18, and Temperature = 36.9°C.
On Abdominal examination; the abdomen was flat, moving with respiration, soft and non-tender. There was no sign of fluid collection (no fluid thrill or shifting dullness). Bimanual pelvic examination indicates that the uterine size was 8 weeks sized with left side adnexal mass. She also had left adnexal and cervical motion tenderness. For this, both abdominal and transvaginal ultrasound were performed showing an empty uterus, with normal endometrial echo and thickness (Figure 1). On the left side of the adnexa, there were two gestational sacs with their yolk sac and fetal embryo separated by a thick intertwin membrane (Figure 2). In both of the embryos, cardiac activity was seen on color Doppler flow (Figure 3). In addition, the following laboratory requests were performed with results of; Complete Blood Count; Hemoglobin = 13.5g/dl, White Blood Cell = 8.69 × 103 /ul, the platelet count was 236 × 103, and serum HCG value was 86,456.00. Urine analysis and sexually transmitted tests were unremarkable.
 |
Figure 1 Transvaginal ultrasound showing an empty uterus. |
 |
Figure 2 Transvaginal ultrasound. (A) Two gestational sacs. (B) Embryo in each of both gestational sac. |
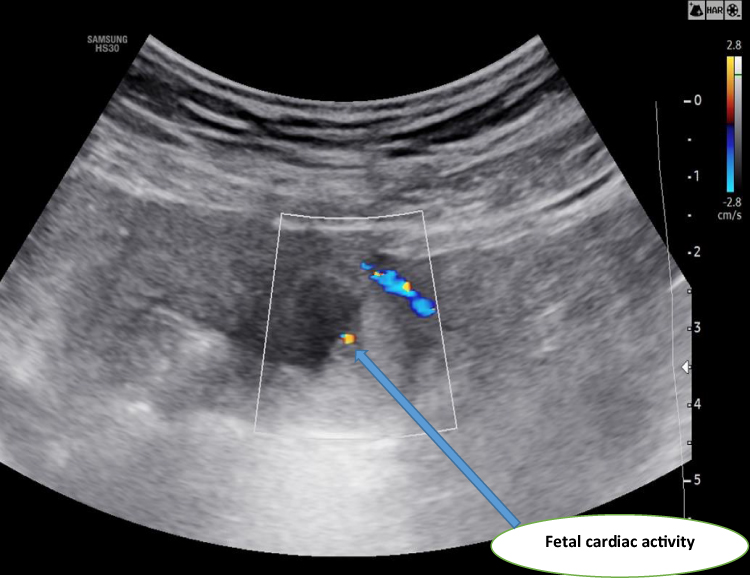 |
Figure 3 Demonstrating one of the embryos with positive cardiac activity on color Doppler. |
Using the above evidence, a diagnosis of unilateral live twin ectopic pregnancy was made and laparotomy was decided. After taking informed consent and preparing for laparotomy, she was taken to the operation theater. Under general anesthesia, the abdomen was entered through a Pfannenstiel incision (through the previous 2 cesarean section scars). Upon entry into the abdomen, there was dense adhesion between the abdominal wall and uterus, 3cm by 4cm intact left intact ampulla (tubal) ectopic pregnancy (Figure 4). After adhesion was released, left side salpingectomy was performed and the abdomen was closed in layers. Dissecting the resected tube shows two separate gestational sacs (Figure 5). The woman was discharged home after two smooth post-operative days in the hospital.
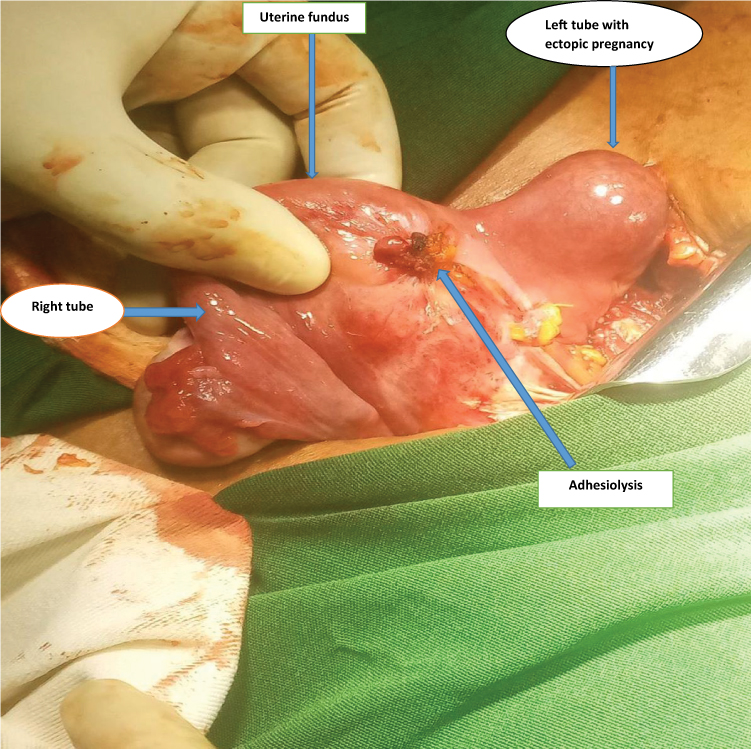 |
Figure 4 Left tubal ectopic pregnancy after adhesiolysis. |
 |
Figure 5 Resected tube with two gestational sacs. |
Discussion
Ectopic pregnancy is the implantation of the embryo outside of the endometrial cavity with an incidence of 1–2% among all types of pregnancies.1 The most common site of implantation outside the endometrial lining is tubal accounting for more than 90% of the cases. The other sites of implantation include: ovarian, cervical, abdominal, cesarean scar, or interstitial.
Ectopic pregnancies are commonly singleton with rare findings of twin ectopic pregnancy occurring in 1:20,000 up to 1:125,000 pregnancies. One ectopic pregnancy can happen with one intrauterine (heterotopic) or the other with molar pregnancy.1–3
Twin ectopic pregnancy is the implantation of both embryos outside of the endometrial lining; it can implant commonly on tubes but there are reports of twin ectopic implanted on the ovary,4 abdominal,5 cesarean scar,6 cornual7 and cervical.8 Different case reports indicate that there are twins with or without cardiac activity. In cases of tubal twin pregnancies, reports showed the majority are unilateral tubal pregnancies while few are bilateral tubal pregnancies.3,9–12 In this woman, the implantation was on the left side of the uterine tube with both positive cardiac activities.
Even though half of the ectopic pregnancies has no predisposing or risk factors, most risk factors associated with singleton or twin ectopic pregnancy are previous history of ectopic pregnancy, sexually transmitted infection/Pelvic inflammatory disease, previous tubal surgery, invitro fertilization, ovulation inducing drugs like clomiphene citrate, smoking, advanced maternal age, failed contraception use or previous cesarean section.1,8,13–15 In this case, except for the two cesarean sections that may increase the risk of cesarean scar ectopic not tubal, she has no well-known risk factors.
The clinical features of twin ectopic pregnancy are similar to singleton ectopic pregnancy which is, triad of amenorrhea, vaginal bleeding and abdominal pain.1 After the ectopic has ruptured, individuals may exhibit abnormal vital signs, acute abdominal symptoms, and anemia-related signs and symptoms. Amenorrhea and abdominal pain are present in this patient, but there is no vaginal bleeding. The likelihood of an unruptured ectopic pregnancy is increased by the absence of any peritoneal or diaphragmatic irritation. The risk of rupture in tubal ectopic pregnancy is higher in twin unilateral tubal pregnancy than singleton tubal pregnancy occurring in 30–50% of cases.10,16
Diagnosis of twin ectopic pregnancy depends on the clinical feature, laboratory tests and imaging. The definitive diagnosis will be made by demonstration of two alive cardiac activity fetuses outside of the uterus using sonography or confirmation of removed tissue by laparoscopy or laparotomy using pathologic evaluation. The serum HCG of the twin ectopic pregnancy is higher than the same gestational age of singleton ectopic or intrauterine pregnancy.4–6 Using transvaginal ultrasound is more sensitive and specific than transabdominal ultrasound. With ultrasound, we can visualize two gestational sac with or without separating membrane, or fetal cardiac activity.6,17–21 In difficult cases, we can use MRI to diagnose twin ectopic pregnancy.22
Management of the twin ectopic pregnancy is similar to the singleton ectopic pregnancy and depends on the site of implantation. These can be medical or surgical treatments. The medical treatments include intra-gestational feticidal, use of the methotrexate either systemic or intra-gestation. In some case reports there was a shift from medical to surgical after it failed. Surgical management used for the treatment of twin ectopic are hysteroscopic resection (used for cesarean sac twin ectopic), laparoscopic or laparotomy resection. Laparoscopically and by laparotomy salpingectomy, linear salpingostomy can be performed. Currently, arterial embolization is also used for twin ectopic pregnancy and found to be effective.3,16,17,19,23–25 In this case, laparotomy was done since there is no laparoscopy in the area and medical was not preferred since there was cardiac activity and poor adherence to it.
Implication
An extremely uncommon type of pregnancy called twin ectopic pregnancy has a substantial risk of maternal morbidity and mortality after the ectopic site ruptures. Ectopic pregnancy, especially twin ectopic, requires prompt identification and therapy in order to reduce morbidity and mortality.
Patient Consent
Written consent has been obtained from the patient after she has seen the detailed description of the case and the pictures to be published. No institutional approval was required for the publishing of this case report.
Acknowledgments
I want to thank the patient for giving me consent to publish.
Funding
No grant support or funding was given.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Pek JH, Simpson WLJ, Owen J, Nelson B. Live twin ectopic pregnancy. J Emerg Med. 2020;59(2):e77–e79. doi:10.1016/j.jemermed.2020.04.033
2. Li J, Sun W, Jin X, Fei X. A live tubal twin pregnancy. Arch Gynecol Obstet. 2021;303:1371–1372. doi:10.1007/s00404-021-06001-1
3. Lategan HE, Gillispie VC. Spontaneous unilateral tubal twin ectopic pregnancy. Ochsner J. 2019;19:178–180. doi:10.31486/toj.17.0110
4. Uludag SZ, Serdar Kutuk M, Dolanbay M, Ulker F, Tuncay Ozgun M. Primary ovarian monochorionic twin ectopic pregnancy. Case Rep. 2016;61(9–10):516–518.
5. Chughtai F. Twin abdominal pregnancy - a rare scenario. J Pak Med Assoc. 2017;67(5):793–795.
6. Bringley J, Denefrio C, Rijhsinghani A. Twin cesarean scar ectopic pregnancy treated with systemic and local methotrexate. Am J Obstet Gynecol. 2017;216(1):77.e1–77.e2. doi:10.1016/j.ajog.2016.09.080
7. Asch E, Levine D, Robens J. Cornual ectopic pregnancy of dichorionic diamniotic twins, with one live fetus and co-twin demise. Ultrasound Q. 2012;28(3):189–191. doi:10.1097/RUQ.0b013e318262cb73
8. Anev I, Wang J, Palep-Singh M, Seif MW. Monochorionic diamniotic twin cervical ectopic pregnancy following assisted conception: a case report. J Reprod Med. 2013;58(9–10):445–447.
9. Seak C-J, Goh ZNL, Wong AC, Seak JC-Y, Seak C-K. Unilateral live twin tubal ectopic pregnancy presenting at 12 weeks of gestation: a case report. Medicine. 2019;98(38):e17229. doi:10.1097/MD.0000000000017229
10. Ghanbarzadeh N, Nadjafi-Semnani M, Nadjafi-Semnani A, Nadjfai-Semnani F, Shahabinejad S. Unilateral twin tubal ectopic pregnancy in a patient following tubal surgery. J Res Med Sci. 2015;20:196–198.
11. Vohra S, Mahsood S, Shelton H, Zaedi K, Economides DL. Spontaneous live unilateral twin ectopic pregnancy - a case presentation. Ultrasound. 2014;22:243–246. doi:10.1177/1742271X14555565
12. Amine BHH, Haythem S. Extra-uterine twin pregnancy: case report of spontaneous bilateral tubal ectopic pregnancy. Pan Afr Med J. 2015;20:435. doi:10.11604/pamj.2015.20.435.6338
13. Yamane D, Stella M, Goralnick E. Twin ectopic pregnancy. J Emerg Med. 2015;48(6):e139–e140. doi:10.1016/j.jemermed.2014.12.061
14. Mollo A, Alviggi C, Conforti A, Insabato L, De Placido G. Intact removal of spontaneous twin ectopic Caesarean scar pregnancy by office hysteroscopy: case report and literature review. Reprod Biomed Online. 2014;29(5):530–533. doi:10.1016/j.rbmo.2014.06.017
15. Longoria TC, Stephenson ML, Speir VJ. Live unilateral twin ectopic pregnancy in a fallopian tube remnant after previous ipsilateral salpingectomy. J Clin Ultrasound. 2014;42(3):169–171. doi:10.1002/jcu.22074
16. Martin A, Balachandar K, Bland P. Management of a spontaneously conceived live unilateral twin ectopic pregnancy in Australia: a case report. Case Rep Women’s Health. 2021;30:e00300. doi:10.1016/j.crwh.2021.e00300
17. Papiccio M, Boschi AC, Ferrara F, et al. Spontaneous angular dichorionic diamniotic twin pregnancy: a case report. Fertil Steril. 2022;117(1):155–159. doi:10.1016/j.fertnstert.2021.09.003
18. Kusumo F, Adegoke OA, Guelfguat M. Reprint of: twin live gestation in a cesarean section scar ectopic pregnancy. Dis Mon. 2022;101380. doi:10.1016/j.disamonth.2022.101380
19. Madaan S, Jaiswal A, Banode P, Dhok A, Dewani D. Spontaneous twin ectopic pregnancy managed successfully with methotrexate-mediated ultrasound-guided fetal reduction: a fertility-preserving approach. Cureus. 2021;13:e17077. doi:10.7759/cureus.17077
20. Rottenstreich M, Sela HY. Twin pregnancy in non-communicating rudimentary horn. Eur J Obstet Gynecol Reprod Biol. 2018;228:337–338. doi:10.1016/j.ejogrb.2018.07.010
21. Errázuriz J, Racca A, Schutyser V, Frederix B, Blockeel C. Cornual twin pregnancy following IVF/ICSI treatment. Ultrasound Obstet Gynecol. 2018;52(2):287–288. doi:10.1002/uog.19109
22. Nepal P, Ojili V, Lu SC, Nagar A. Utility of MRI in management of a rare case of unilateral dichorionic-diamniotic twin tubal ectopic pregnancy. Curr Probl Diagn Radiol. 2021;50:551–553. doi:10.1067/j.cpradiol.2019.06.001
23. Chong Y, Wang W, Zhang A, Zhao Y. Ultrasound for monitoring twin cesarean scar pregnancy following feticide. J Int Med Res. 2022;50(4):3000605221095683. doi:10.1177/03000605221095683
24. Tsakiridis I, Chatzikalogiannis I, Dagklis T, Athanasiadis A, Mamopoulos A. Spontaneous unilateral twin tubal pregnancy: a rare case report with conservative management. J Obstet Gynaecol. 2019;39(7):1030–1031. doi:10.1080/01443615.2019.1586859
25. Betti M, Vergani P, Damiani GR, et al. Unilateral twin tubal pregnancy: a case report and review of the literature. Acta Biomed. 2018;89(3):423–427. doi:10.23750/abm.v89i3.6915
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Osteitis Fibrosa Cystica; A Forgotten Manifestation of Secondary Hyperparathyroidism Due to End-Stage Renal Disease: A Case Report
Usmael SA, Ansa SM, Tufa DW
International Medical Case Reports Journal 2022, 15:529-535
Published Date: 21 September 2022
Isolated Asymptomatic Fetal Intracardiac Mass: A Case of Rhabdomyoma

Eticha TG, Ararso R, Sultan S, Terefe K, Berhe SW, Tsega T, Abebe Y, Baye C
International Medical Case Reports Journal 2023, 16:97-102
Published Date: 28 February 2023
Pregnancy Associated Invasive Apocrine Carcinoma of the Breast: Case Report from Ethiopia
Alemu HK, Hammad N, Tola MA, Vanderpuye V
Breast Cancer: Targets and Therapy 2023, 15:429-433
Published Date: 23 June 2023
Rare Unilateral Twin Ectopic Pregnancy After Frozen Embryo Transfer: A Case Report and Literature Review
Zhang Y, Lu X, Wang X, Wu X, Jing X, Cui X
International Medical Case Reports Journal 2023, 16:731-737
Published Date: 13 November 2023
A Case Report of Pregnancy Complicated with Primary Hemophagocytic Lymphohistiocytosis
Chen Y, Huang X, Chen H, Tong J, Huang L, Su J, Deng L
International Journal of Women's Health 2024, 16:843-851
Published Date: 17 May 2024