Back to Journals » International Medical Case Reports Journal » Volume 18
Diagnosis and Management Challenges of Spontaneous Quadruplet Pregnancy in a Resource-Limited Setting: A Case Report
Authors Tjandraprawira KD, Santoso DPJ, Bayuaji H ![]() , Nugrahani AD
, Nugrahani AD ![]() , Susandi D
, Susandi D ![]()
Received 12 August 2024
Accepted for publication 25 February 2025
Published 11 March 2025 Volume 2025:18 Pages 325—332
DOI https://doi.org/10.2147/IMCRJ.S491180
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Thomas E Hutson
Kevin Dominique Tjandraprawira,1 Dhanny Primantara Johari Santoso,2 Hartanto Bayuaji,1 Annisa Dewi Nugrahani,2 Dadan Susandi2
1Department of Obstetrics and Gynecology, Faculty of Medicine, Universitas Padjadjaran – Dr. Hasan Sadikin General Hospital, Bandung, Indonesia; 2Department of Obstetrics and Gynecology, Dr. Slamet General Hospital, Garut, Indonesia
Correspondence: Kevin Dominique Tjandraprawira, Department of Obstetrics and Gynecology, Faculty of Medicine, Universitas Padjadjaran – Dr. Hasan Sadikin General Hospital, Bandung, Indonesia, Email [email protected]
Introduction: Higher-order pregnancy is considered as a high-risk pregnancy, followed by various maternal and foetal complications. The diagnosis and management of higher order pregnancy have abundant and complex challenges, especially in rural areas where antenatal care (ANC) is often inadequate. Late booking and low awareness of complications necessitates priority management and referral to a tertiary center for fetal medicine expertise. This is our experience managing a spontaneously conceived quadruplet pregnancy delivered prematurely in a low-resource setting.
Case Presentations: A 27-years-old primigravida of 7.5 months of gestation presented with preterm labor. Her membrane was intact, and she noted active fetal movements. Her history was notable due to her pregnancy being spontaneously conceived and that her antenatal consultations had mistakenly identified her pregnancy as a triplet pregnancy. At presentation, her fundal height was 49 cm, and her cervix was 5– 6 cm dilated. As she was in active labor, she underwent an emergency caesarean section. Four neonates were delivered but only two were transferred to the neonatal intensive care unit due to infrastructure limitations. She made an uneventful recovery and was discharged 2 days later. However, only two of four neonates eventually survived. This quadruplet pregnancy signified the pertinent complications of multifetal pregnancy: misidentification of chorionicity; preterm delivery; and early neonatal deaths due to prematurity.
Conclusion: Higher order pregnancies present their own challenges for diagnosis and treatment. Preterm delivery and its associated neonatal complications are well-known complications, and a multidisciplinary management is crucial.
Keywords: case report, multiple pregnancy, pregnancy, quadruplet
Introduction
Higher-order pregnancy is defined when more than two (multiple) fetuses are present simultaneously in the uterus.1,2 Such high-risk pregnancies can be the result of a single zygote duplication (monozygotic) or multiple zygotes duplication (multizygotic). Once implanted, the zygotes may further divide, producing multiple fetuses that may or may not share the same placental mass/chorions and/or the same amniotic sac. Increased rates of ovulation induction, assisted reproductive technologies (ARTs), and advanced maternal age at conception have all been linked to an increase in the occurrence of higher-order pregnancy worldwide.3 The incidence of pregnancies with higher-order pregnancy ranges from 0.01% to 0.07%.1,2 Reports of triplet pregnancies abound, but quadruplet pregnancies, especially when conceived naturally, are exceedingly rare, with estimates around 1/512,000 to 1/677,000 births.4,5
Both maternal and foetal complications including miscarriage, preterm birth, low neonatal birthweight, caesarean delivery, neonatal deaths, hypertension in pregnancy, anaemia, hyperemesis gravidarum, gestational diabetes mellitus and psychological disorder are linked to higher-order pregnancies.6,7 The National Institute of Clinical Excellence (NICE) states that up to 75% of all triplet pregnancies are born prematurely before 35 weeks of gestation.8 No similar data exist for quadruplets, but case reports in the literature consistently report preterm deliveries before 34 weeks.4 Antunes et al reported that from their experience and literature review, quadruplets tended to deliver around 32 weeks with birthweights not exceeding 1500 grams.4
Previous studies reported that neonates born from higher-order pregnancy (triplets and quadruplets) tended to have lower 1 minute APGAR scores (7.27 vs 7.83, p = 0.001) and 5 minutes APGAR scores (8.61 vs 9.12, p = 0.0001) than twin pregnancies.9 Triplet or higher-order births had an increased likelihood of receiving 1 dose of surfactant when compared to singletons (88.3% vs 80.9%).10 According to Umeora et al, higher-order pregnancies have increased perinatal mortality rates when compared to singletons (276/1000 vs 71/1000 live births).1
In pregnancies involving triplets and above, they should always receive tertiary centre referral and foetal medicine care. Novel complications, such as twin-to-twin transfusion syndrome, may arise between the fetuses.11 In addition, delivery must be carried out by caesarean section.8 However, such access may not always be possible in low-resource settings, including Indonesia. Despite there being a tertiary hospital with foetal medicine expertise, not all quadruplet pregnancies are managed there, as this case describes. No reimbursement of travel costs, lack of affordable accommodation arrangements, lengthy referral waiting times and the lack of widespread availability of foetal medicine teams may deter patients from regular follow-ups at tertiary centres.12
Based on these issues, the diagnosis and management of higher order pregnancy have their own challenges, especially in rural areas where antenatal care (ANC) is usually inadequate, accompanied by more limited diagnostic and treatment options. In addition, a spontaneous quadruplet pregnancy is even rarer, and the lack of patient understanding may further complicate the management. We present a case that highlights the lack of patient awareness of the high-risk nature of her pregnancy whilst demonstrating the subsequent management and dire outcome of such a high-risk case.
Case Description
This case report is reported according to the CARE guidelines and is exempt from ethical review procedures as defined by the policy from our local hospital (Dr Hasan Sadikin General Hospital) ethical committee.13 The patient has given us permission to present her case details and the accompanying images and written informed consent was obtained.
A 27-years-old primigravida of 7.5 months of gestation presented to our regional hospital in Garut, Indonesia, with regular contractions for the past 12 hours. Her membrane was intact and she reported active fetal movements. She was referred to our facility from a private clinic due to preterm labour.
Her history was noted that she had previously been married for 6 years but had suffered from primary infertility. Her menstrual cycles were irregular, but she denied any formal diagnosis of polycystic ovarian syndrome or other causes of oligomenorrhea. Prior to this pregnancy, she recounted a consultation with a general gynaecologist for regulating her menstrual cycles. She was prescribed only combined hormonal contraceptive pills. She denied the prescription of ovarian induction drugs, and she had not presented to a fertility centre. There was no history of twins in the patient’s family nor in her husband’s family.
Attempts to trace her antenatal care (ANC) documents were unsuccessful. Several lines of contact were pursued with the obstetrician caring for her in early pregnancy, but there were no replies. Based on her account, she had her first antenatal visit at around 4–5 weeks of gestation. Her history was notable for severe nausea and vomiting during pregnancy, which appeared around 6–7 weeks of gestation. She learned that her pregnancy was a quadruplet pregnancy during her initial visit. However, during her subsequent visits, her obstetrician could only identify triplets. She underwent her antenatal visits in Cirebon, Indonesia, but at around 7 months of gestation, she relocated to her hometown of Garut, Indonesia, with plans to deliver there. Even after relocating, she underwent all her antenatal care with a local obstetrician. She denied any recommendations or requests for transfer/referral to a tertiary centre with foetal medicine expertise. A timeline of her antenatal care and her subsequent presentation to our hospital is presented in Figure 3.
At presentation, her vital signs were within normal limits. Her obstetrical examinations revealed a fundal height of 49 cm, abdominal circumference of 120 cm. Her contractions were regular and increasingly powerful. The first and the second fetuses were cephalic, the third one was breech. All fetuses had normal fetal heart rates (152, 148, and 136 beat per minutes, respectively). A bimanual examination revealed a completely effaced cervix with an opening of 5–6 cm and intact membranes.
She was immediately transferred to the theatre to undergo an emergency caesarean section. Members of the neonatal team were present in the operating room at the start of the caesarean section. A low transverse incision was made on the lower uterine segment. To our surprise, her pregnancy was indeed a quadruplet pregnancy with the neonatal details listed in Table 1. The fetuses in cephalic presentation were delivered routinely. The fetuses in breech were delivered by footling extraction (neonate 3) and breech extraction (neonate 4). There was little difficulty in delivering the fetuses due to their relatively small sizes, despite the different fetal presentations. The placenta was removed by a controlled traction of the placenta (Figure 1). An intrauterine device was inserted during the C-section. Intraoperative bleeding was 400 cc. After the surgery, a close examination of the placenta demonstrated that it was quadrichorionic quadriamniotic.
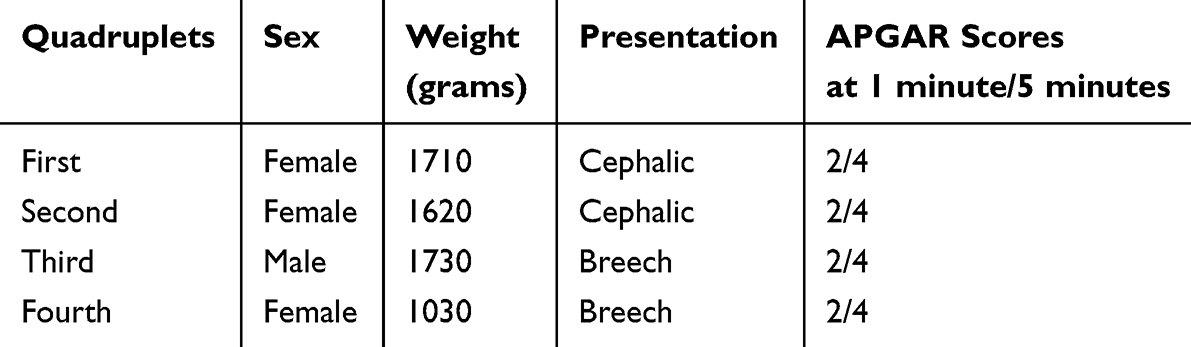 |
Table 1 Neonatal Details of Patient’s Quadruplet |
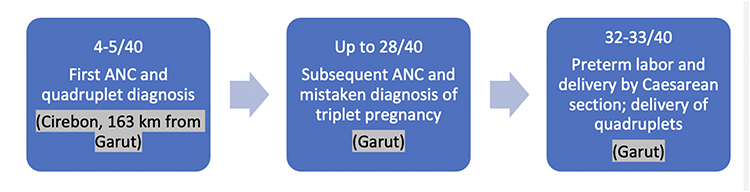 |
Figure 1 Antenatal Care and Delivery Timeline. |
Due to the low APGAR scores, her neonates were resuscitated in the operating theatre and immediately transferred to the perinatology ward but only two could be transferred to neonatal intensive care unit (NICU) due to the lack of available cots (Figure 2) with only ventilators, syringe pump, and infusion pumps were the equipment available here. Efforts were made to refer the remaining neonates to a nearby hospital with available NICU cots. However, the parents refused such care despite our repeated offers. Their refusal was due to their lack of funds to cover the travel costs between the hospitals as we would have transferred the neonates to a tertiary facility in another city. Eventually, two neonates passed away (neonates number 3 and number 4) due to respiratory distress syndrome whilst the other two neonates survived. They were discharged after spending 3 weeks in care.
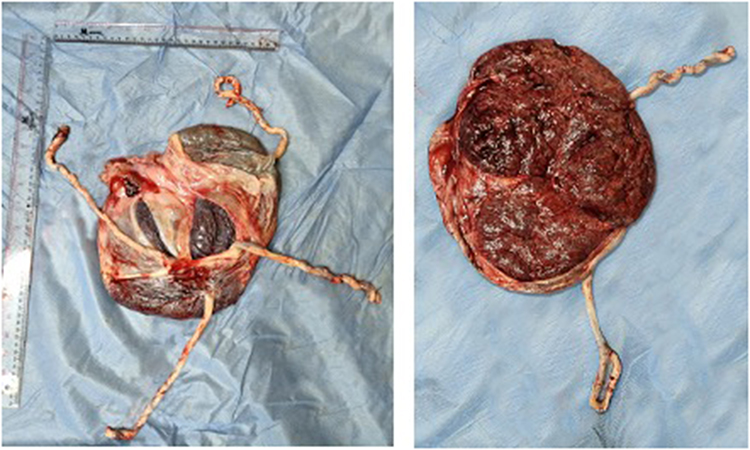 |
Figure 2 Placenta under examination, (left) fetal side, (right) maternal side. |
 |
Figure 3 The four neonates. |
The mother was transferred to the obstetric ward post-surgery. She received continuous infusion of oxytocin in the ward for the first 24 hours postpartum as per local hospital protocol. She was monitored for potential complications, particularly postpartum hemorrhage and uterine atony. She made an uneventful recovery and was discharged 2 days post-surgery. Both the mother and the infants were encouraged to attend further follow-ups at the hospital.
Upon further follow-up, the mother and the infants have not presented again to our clinic. However, the authors managed to contact her by phone. On her account, the two surviving infants have grown well whilst hitting the appropriate milestones. She has not provided further details on any complications or other developmental concerns. As for the mother, she did not have any postnatal follow-ups, despite our encouragement. She did not describe any problems regarding her health.
Discussions
Higher Order Pregnancy
A multiple gestation can result from the division of a single fertilized ovum (monozygotic), the fertilization of numerous eggs simultaneously (multi-zygotic), or even from the combination of the processes. The time of the fertilized ovum splitting determines the pregnancy chorionicity in monozygotic pregnancies.14 It was a coincidence that this pregnancy was quadrichorionic quadriamniotic, with similar reports elsewhere.15–17 In theory, there could be different mechanisms leading to quadruplet pregnancy, including monochorionic, dichorionic, and trichorionic quadriamniotic pregnancy. Such combinations would be subject to additional risks of complications unique to such arrangements, including twin-to-twin transfusion syndrome and selective intrauterine growth resistance.15,16
Higher-order pregnancies are also either monozygotic or multizygotic.16 Monozygotic quadruplets would all produce neonates of the same sex, whilst multizygotic quadruplets may be all female, all male or a combination of both.16 Our case was a multizygotic quadruplet pregnancy due to there being 3 female neonates and 1 male neonate.
Numerous variables have been linked to an increased likelihood of multiple pregnancies. The risk factors for multiple pregnancies are different for monozygotic and multizygotic pregnancies. Due to the small case series and data limitations, it is challenging to identify any risk factors for quadruplet and higher order births. In our case, the patient received contraceptive pills due to her irregular menstrual cycles. There has been evidence of multiple pregnancies being linked to contraceptive pills and the following time interval after their discontinuation. This theory is based on the hypothesis that gonadotropin secretion may increase soon after pill withdrawal, perhaps leading to numerous pregnancies.15
Higher order pregnancies are typically linked to substantial maternal and fetal morbidity and mortality. Preterm labor, placenta abruption, cervical incompetence, cardiopulmonary disorder, preeclampsia, and gestational diabetes mellitus are among the well-documented maternal problems.16 Preterm labor is due to the inability of the uterus to accommodate the high number of fetuses and the accompanying amniotic fluid.8,18 There may be additional complications such as intraventricular hemorrhage, twin to twin transfusion syndrome, congenital abnormalities, respiratory distress syndrome, and ultimately perinatal death.19
Challenges of Antenatal Care in Higher Order Pregnancy
Close prenatal monitoring and regular antenatal visits are a prerequisite since preterm delivery and development abnormalities are the main causes of neonatal mortality and disability in multiple pregnancies. In our case, the patient’s antenatal visits were sporadic and inadequate for a high-risk quadruplet pregnancy. Another issue with higher-order pregnancy is determining the chorionicity of the pregnancy and a systematic assessment of all the fetuses. There is a risk of mislabeling and misidentifying the fetuses with a non-standardised approach. This occurred in our patient as she was falsely informed that her pregnancy had spontaneously reduced to a triplet pregnancy during her antenatal visits. Such misidentification would have resulted in a non-standardised numbering and mapping of the fetuses, resulting in one fetus missing from the evaluation.
Another issue is the higher risk of genetic syndrome and congenital abnormalities that may be present in the fetuses. Near the end of the first trimester, singleton pregnancies would be eligible for noninvasive prenatal screening. However, such screening methods are often inaccurate for higher-order pregnancies. In resource-limited settings, such options are often limited or unavailable. Thus, ultrasound is often the only screening method available. This is, in part, due to an initiative by the Indonesian government to provide an ultrasound machine to every community primary healthcare center (Pusat Kesehatan Masyarakat).20 However, the widespread availability of examiners adept at performing ultrasound for high-risk pregnancies is not yet achieved.
If a higher-order pregnancy is discovered, such as in our case, a referral to a fetal medicine center is imperative to allow a systematic and detailed ultrasound assessment of the fetuses, along with a detailed delivery plan. In an ideal setting, periodic ultrasound assessment would also be carried out to measure cervical lengths and hence, identify the indications for a prophylactic cerclage. Additional diagnostic tests, such as advanced imaging or genetic testing, could have confirmed the zygosity and chorionicity, providing better clarity on the pregnancy’s nature and associated risks. However, there is little evidence that noninvasive prenatal testing (NIPT) can be used for higher-order pregnancies. Whilst there has been a report on the use of NIPT for triplets, no official recommendations are endorsing NIPT beyond twin pregnancies.21,22 Nevertheless, prophylactic cerclage is not recommended for use in twins and/or higher-order pregnancies for solely preventing preterm delivery.23,24 Unfortunately, our patient did not receive such care, and her high-risk pregnancy was managed antenatally as if it was a low-risk pregnancy. The refusal of intercity referral by the parents warrants further investigation into potential cultural, financial, or logistical barriers that influenced their decision. Whilst patient’s autonomy with regard to her desired place of care should be respected, the lack of initiative to recommend an immediate referral to a tertiary hospital with neonatal intensive care facilities was alarming.
Delivery Management
Higher-order pregnancies, such as a quadruplet pregnancy, constitutes a very high-risk category. A multidisciplinary approach is necessary for a safer transition into motherhood. Successful outcomes depend not only on the consultant obstetrician but also on the early involvement of neonatologists and anesthesiologists for assessment and management planning. Multiple pregnancies are linked to higher perinatal mortality than singleton pregnancies, primarily due to preterm delivery and its subsequent consequences.
Caesarean sections are the preferred common delivery method in higher-order pregnancies.15,19,25 Transverse incisions in the lower uterine region are indicated in most cases. An adequate myometrial incision line advances upward in circumstances where uterine effacement is adequate and uterine internal ostium is opened.26 Despite having similar techniques, adequate planning is imperative due to several important caveats. First, the placenta is larger, bulkier and frequently found near the anterior corpus of the multiple pregnancy, which could lead to placenta previa with large blood vessels being present. Second, there is evidence to recommend a U-shaped incision followed by a sharp dissection the lower uterine segment. This is to prevent the uterine incision extending to the lateral plexus of arteries and veins. Third, caution is necessary prior to rupturing each amniotic sac in view of the possibility of fetal malpresentation.26 In our case, a transverse incision of the lower uterine segment was performed, rupture of each amniotic sac was carried out and the surgery went smoothly.
Neonatal Management
There is a higher risk of poor perinatal outcomes when the pregnancy is term or near term when multiple pregnancies are delivered vaginally compared to caesarean section.27 Interestingly, there was no conclusive evidence of any differences in maternal death or serious morbidity between planned vaginal delivery and caesarean section (risk ratio [RR] = 0.86, 95% confidence interval [CI]: 0.67–1.11) nor was there a significant difference between planned vaginal delivery and caesarean section in terms of perinatal or neonatal death or serious neonatal morbidity (RR = 1.15, 95% CI: 0.80–1.67). Moreover, a lower 5-minute APGAR score was less common for planned caesarean sections if the first twin is in vertex presentation and the fetuses weighing at least 1500 g or reach at least 32 weeks’ gestation.27,28 In our case, the local hospital protocol required us to deliver any higher-order pregnancy, starting from a triplet pregnancy, with caesarean section. This was due to fears of malpresentations obstructing labor progress, including the entanglement of umbilical cords when the membranes are ruptured.
Another challenge was in reducing perinatal mortality in such a high-risk pregnancy. There is still large disparity in perinatal mortality across various regions in Indonesia. Perinatal mortality affects up to 1.5% of total births in Indonesia. The lowest perinatal mortality rate is in the island of Java at 1.3% of total births, whilst the highest is in the West Papua area at 2.5%.29 However, within Java itself there are still a lot of variations and differences depending on the availability of hospitals and the supply of NICU cots. The shortcomings of this case reflect the challenges in providing adequate neonatal intensive care facilities evenly across regions. As noted from a previous study on patient’s awareness of obstetric danger signs and this patient’s own account, she was unaware that there was a significant risk of preterm delivery from the start of her pregnancy. As such, she did not recognize the signs and symptoms of her impending preterm delivery and hence, she did not make the necessary preparations beforehand. The patient’s unawareness of preterm labor signs reflects systemic issues, including insufficient patient education and gaps in community health worker training. This also reflected a failure of the health professionals involved in her care, who did not pressure her on making a referral to a tertiary care facility with adequate NICU availability.30
Infrastructure-wise, the hospital was also unprepared for such delivery at such a short notice. Being a district general hospital, the NICU beds were very few and since this patient had not booked into our hospital, there were no contingency plans for her delivery and the neonatologists had not been aware of such high-risk pregnancy in the community. Thus, immediately post-delivery, not enough NICU cots were available, leading to only two neonates surviving.
Following delivery, postpartum depression was a feared complication due to the deaths of her two neonates. Research has shown that perinatal death could trigger a depressive episode.31 Postpartum depression is notable, particularly for those with a prior history of depression.32 Postpartum depression may also lead to untimely deaths in the mother if not treated appropriately.32 Providing structured support programs could have mitigated the psychological impact on the patient.33 Unfortunately, our patient declined further counselling by our psychiatric team post-discharge. Efforts on contacting the patient have not been fruitful in encouraging her to attend counselling sessions.
Studies reported in advanced settings show that the majority of cases managed have yielded favorable outcomes.34,35 Comparing the outcomes of this case with similar cases in better-resourced settings could illustrate the impact of systemic factors and provide insights into potential improvements. Whilst preterm deliveries were reported in many case reports, the provision of quality neonatal intensive care would ensure no long-term sequelae in the neonates. The latest study by Rasmussen et al compared adverse outcomes on quadruplet pregnancies with and without fetal reduction.36 They demonstrated that quadruplet pregnancies reduced to twins and singleton pregnancies had fewer adverse outcomes with significant reductions in preterm delivery.36 However, they reported that despite fetal reduction being performed, the outcomes were still poorer than dichorionic diamniotic twins. Unfortunately, such aggressive approach is not possible in Indonesia due to the national law barring selective fetal reduction in higher-order pregnancies in the absence of congenital anomalies.37 To address challenges in our setting, with limited maneuvers sanctioned by the law, preventive measures would be key. Early identification of high-risk pregnancies by community healthcare workers should be prioritized. Providing them with extra training and developing robust integrative referral protocols should be considered as viable public health programs.
Conclusion
Managing a quadruplet pregnancy in a low-resource setting with limited neonatal intensive care unit availability is challenging and may be associated with a poorer prognosis. An immediate referral to a fetal medicine centre in a tertiary referral hospital to allow a multidisciplinary approach should have been arranged early in pregnancy.
Abbreviations
ANC, Antenatal care; ARTs, Assisted reproductive technologies; NEC, necrotizing enterocolitis; NICU, Neonatal intensive care unit.
Patient’s Perspective
The patient would be happy to see if all physician all over the world will learn from her baby’s case. She did not mind if her baby condition is discussed in this report.
Consent for Publication
According to Dr Hasan Sadikin General Hospital policy, this case report is exempt from ethical review procedures since it does not contain any personally identifying information about patients. Informed consent was obtained for the publication of the case. This article adheres to the applicable CAse REport (CARE) guidelines.
Author Contributions
Each author contributed significantly to the work reported, whether it was through conception, study design, execution, data acquisition, analysis, and interpretation, or in all of these areas; they all helped draft, revise, or critically review the article; they approved the final version that was published; they all agreed on the journal to which the article was submitted; and they are accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Umeora OU, AneziOkoro EA, Egwuatu VE. Higher-order multiple births in Abakaliki, Southeast Nigeria. Singapore Med J. 2011;52(3):163–167.
2. Lama LD, Das T, Neupane A, Lama R, Pandey R, Karki U. Management of quadruplet pregnancy: a case report. JNMA J Nepal Med Assoc. 2020;58(222):122–124. doi:10.31729/jnma.4861
3. Fajolu IB, Ezeaka VC, Adeniyi OF, Iroha EO, Egri-Okwaji MT. Prevalence and outcome of higher order multiple pregnancies in Lagos, Nigeria. J Matern Fetal Neonatal Med. 2013;26(13):1342–1345. doi:10.3109/14767058.2013.784260
4. Antunes D, Marques F, Santos Silva I, Branco M. Spontaneous monochorionic quadramniotic pregnancy: a rare and challenging diagnosis. Acta Med Port. 2023;36(4):300–302. doi:10.20344/amp.19283
5. Dhavliker M, Mehta M, Sau A. Spontaneous quadruplet pregnancy: a case report and review of literature. J Obstet Gynaecol. 2022;42(2):349–350. doi:10.1080/01443615.2021.1907743
6. Committee on Practice Bulletins—Obstetrics; Society for Maternal–Fetal Medicine. Practice bulletin no. 169: multifetal gestations: twin, triplet, and higher-order multifetal pregnancies. Obstet Gynecol. 2016;128(4):e131–46. doi:10.1097/AOG.0000000000001709
7. Practice Committee of the Society for Reproductive Endocrinology and Infertility, Quality Assurance Committee of the Society for Assisted Reproductive Technology, and the Practice Committee of the American Society for Reproductive Medicine. Multiple gestation associated with infertility therapy: a committee opinion. Fertil Steril. 2022;117(3):498–511. doi:10.1016/j.fertnstert.2021.12.016
8. Gibson JL, Castleman JS, Meher S, Kilby MD. Updated guidance for the management of twin and triplet pregnancies from the National Institute for Health and Care Excellence guidance, UK: what’s new that may improve perinatal outcomes? Acta Obstet Gynecol Scand. 2020;99(2):147–152. doi:10.1111/aogs.13785
9. Nasseri F, Azhir A. The neonatal outcome in twin versus triplet and quadruplet pregnancies. J Res Med Sci. 2009;14(1):7–12.
10. Wadhawan R, Oh W, Vohr BR, et al. Neurodevelopmental outcomes of triplets or higher-order extremely low birth weight infants. Pediatrics. 2011;127(3):e654–60. doi:10.1542/peds.2010-2646
11. Faber S, Riße S, Steinke H, Thome U, Stepan H. Monochorionic quadruplet pregnancy without severe complications: sonographic work-up and placental findings. Ultrasound Obstet Gynecol. 2013;41(6):707–708. doi:10.1002/uog.12333
12. Khanna RC, Kim S, Giridhar P, Mettla AL, Marmamula S, Rao GN. Barriers to uptake of referral services from secondary care to tertiary care and its associated factors in L V Prasad Eye Institute network in Southern India: a cross-sectional study. BMJ Open. 2018;8(7):e020687. doi:10.1136/bmjopen-2017-020687
13. Riley DS, Barber MS, Kienle GS, et al. CARE guidelines for case reports: explanation and elaboration document. J Clin Epidemiol. 2017;89:218–235. doi:10.1016/j.jclinepi.2017.04.026
14. Elito J. Multiple Pregnancy - New Challenges. Rijeka: IntechOpen; 2019. doi: 10.5772/intechopen.73973.
15. Nnadi D, Nwobodo E, Ibrahim A. Spontaneous monochorionic tetra-amniotic quadruplet pregnancy at term. J Basic Clin Reprod Sci. 2013;2(1):57. doi:10.4103/2278-960X.112597
16. Rathod S, Samal SK, Singh S, Swain S. Quadruplet pregnancy following spontaneous conception: a rare case report. J Clin Diagn Res. 2015;9(4):Qd01–2.
17. Hafizi L, Rezaii Asgarieh E, Taheri N, Ghomian N. Successful management of spontaneous quadruplet pregnancy: a case report. J Family Reprod Health. 2018;12(3):173–176.
18. Keith LG, Goldman RD, Breborowicz G, Blickstein I. Triplet pregnancies in women aged 40 or older: a matched control study. J Reprod Med. 2004;49(8):683–688.
19. Shrestha D, Thapa B, Aryal S, Shrestha BK, Panthee K, Kalakheti B. Successful management of quadruplet pregnancy following spontaneous conception: a rare case report. J Lumbini Med Coll. 2017;4(1):46–49. doi:10.22502/jlmc.v4i1.88
20. Ministry of Health RoI. Kemenkes Penuhi Kebutuhan USG dan Antropometri di Semua Puskesmas dan Posyandu Jakarta: ministry of Health [Indonesian], Republic of Indonesia; 2022 Available from: https://sehatnegeriku.kemkes.go.id/baca/umum/20221223/3942104/kemenkes-penuhi-kebutuhan-usg-dan-antropometri-di-semua-puskesmas-dan-posyandu/#:~:text=Kemenkes%20menargetkan%20semua%20Puskesmas%20memiliki,di%206.886%20puskesmas%20(66.7%25).
21. Scotland N. Non-invasive prenatal testing Scotland: NHS Scotland; 2024. Available from: https://www.nhsinform.scot/healthy-living/screening/pregnancy/non-invasive-prenatal-testing-nipt/#:~:text=NIPT%20is%20completely%20safe%20and,with%203%20or%20more%20babies.
22. Zakaria H, Kleinfinger P, Lohmann L, et al. Performance of cell-free DNA testing for common fetal trisomies in triplet pregnancies. Prenat Diagn. 2024;44(5):555–561. doi:10.1002/pd.6548
23. Practice Committee of the American Society for Reproductive Medicine. Multiple gestation associated with infertility therapy: an American Society for Reproductive Medicine Practice Committee opinion. Fertil Steril. 2012;97(4):825–834. doi:10.1016/j.fertnstert.2011.11.048
24. Shennan AH, Story L. Cervical Cerclage. Green-Top Guideline No 75 BJOG. 2022;129(7):1178–1210.
25. Minakami H, Kosuge S, Fujiwara H, Mori Y, Sato I. Risk of premature birth in multifetal pregnancy. Twin Res. 2000;3(1):2–6. doi:10.1375/twin.3.1.2
26. Tanigaki S, Takemori S, Osaka M, et al. Caesarean section of multifetal pregnancy. Surg J. 2020;6(Suppl 2):S92–s7. doi:10.1055/s-0040-1712924
27. Barrett JF, Hannah ME, Hutton EK, et al. A randomized trial of planned cesarean or vaginal delivery for twin pregnancy. N Engl J Med. 2013;369(14):1295–1305. doi:10.1056/NEJMoa1214939
28. Ogumu EI, Anikwe CC, Okorochukwu BC, et al. Fetal and maternal outcome of higher-order multiple pregnancies in a tertiary hospital: a 5-year single-center observational study from Nigeria. SAGE Open Med. 2022;10:20503121221127160. doi:10.1177/20503121221127160
29. Misnaniarti, Sariunita N, Idris H, Idris H. Regional perinatal mortality differences in Indonesia: evidence from Indonesian Demographic Health Survey. Public Health Pract. 2024;7:100501. doi:10.1016/j.puhip.2024.100501
30. Tjandraprawira KD, Ghozali I. Knowledge of pregnancy and its danger signs not improved by maternal and child health handbook. J Obstet Gynaecol India. 2019;69(3):218–224. doi:10.1007/s13224-018-1162-0
31. Arach AAO, Nakasujja N, Nankabirwa V, et al. Perinatal death triples the prevalence of postpartum depression among women in Northern Uganda: a community-based cross-sectional study. PLoS One. 2020;15(10):e0240409. doi:10.1371/journal.pone.0240409
32. Hagatulah N, Bränn E, Oberg AS, Valdimarsdóttir UA, Shen Q, Lu D. Perinatal depression and risk of mortality: nationwide, register based study in Sweden. BMJ. 2024;384:e075462.
33. Thomson G, McNally L, Nowland R. Experiences and impacts of psychological support following adverse neonatal experiences or perinatal loss: a qualitative analysis. BMC Pregnancy Childbirth. 2024;24(1):569. doi:10.1186/s12884-024-06713-7
34. Lai SY, Hsieh CT, Liao IL, et al. Monochorionic-triamniotic triplet pregnancy following artificial reproductive technology: report of a rare case in Taiwan. Taiwan J Obstet Gynecol. 2024;63(3):409–413. doi:10.1016/j.tjog.2023.12.002
35. Yıldırım E. Spontaneous triplet pregnancy and trap sequence, case report. BMC Pregnancy Childbirth. 2019;19(1):328. doi:10.1186/s12884-019-2484-3
36. Rasmussen MK, Kristensen SE, Ekelund CK, et al. Quadruplet pregnancy outcome with and without fetal reduction: Danish national cohort study (2008–2018) and comparison with dichorionic twins. Ultrasound Obstet Gynecol. 2024;63(4):514–521. doi:10.1002/uog.27497
37. Mirani P. Selective termination for fetal anomaly in twin pregnancy. Indonesian J Obstet Gynecol. 2013;37(1):57–60.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Unilateral Twin Ectopic Pregnancy: A Case Report from the Eastern Part of Ethiopia, Harar
Gure Eticha T
International Medical Case Reports Journal 2022, 15:521-527
Published Date: 19 September 2022
Pregnancy Associated Invasive Apocrine Carcinoma of the Breast: Case Report from Ethiopia
Alemu HK, Hammad N, Tola MA, Vanderpuye V
Breast Cancer: Targets and Therapy 2023, 15:429-433
Published Date: 23 June 2023
A Case Report of Pregnancy Complicated with Primary Hemophagocytic Lymphohistiocytosis
Chen Y, Huang X, Chen H, Tong J, Huang L, Su J, Deng L
International Journal of Women's Health 2024, 16:843-851
Published Date: 17 May 2024
Pregnancy-Triggered Hereditary Thrombotic Thrombocytopenic Purpura: A Case Report
Xing X, Yu N, Zhang Z
International Journal of Women's Health 2025, 17:3897-3906
Published Date: 25 October 2025
Severe Mitral Stenosis in Term Pregnancy Presenting During Labor in a Resource-Limited Setting: A Case Report from Borama, Awdal Region of Somalia

Jama AM, Osman AA, Deria HM, Mousa MM, Jama AM, Ali AO
International Medical Case Reports Journal 2026, 19:564292
Published Date: 26 February 2026