Back to Journals » Blood and Lymphatic Cancer: Targets and Therapy » Volume 16
Natural Killer/T-Cell Lymphoma-Associated Hemophagocytic lymphohistiocytosis—a Rare and Dangerous Disease
Authors Meng G ![]() , Wang M
, Wang M ![]() , Sun C, Feng G, Ren J, Feng S, Wang Y
, Sun C, Feng G, Ren J, Feng S, Wang Y
Received 15 October 2025
Accepted for publication 19 January 2026
Published 27 January 2026 Volume 2026:16 574445
DOI https://doi.org/10.2147/BLCTT.S574445
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Wilson Gonsalves
Guangqiang Meng,1 Manzhi Wang,1 Congcong Sun,1 Gege Feng,2 Jing Ren,1 Saran Feng,1 Yan Wang1
1Department of Hematology, The First Affiliated Hospital of Shandong First Medical University & Shandong Provincial Qianfoshan Hospital, Jinan, Shandong, People’s Republic of China; 2Department of Hematology, Qilu Hospital of Shandong University, Jinan, Shandong, People’s Republic of China
Correspondence: Guangqiang Meng, Email [email protected]
Abstract: Hemophagocytic lymphohistiocytosis (HLH) is a clinical syndrome characterised by the reactive activation of cytotoxic T-lymphocytes and macrophages along with a substantial amount of cytokine secretion caused by various inductions. Natural killer/T-cell lymphoma (NKTL)-associated HLH (NK/T-LAHLH) is rare in clinical practice with an incidence rate of 7.1– 11.9% in NKTL patients. Currently, there is no standard first-line treatment with good efficacy for NK/T-LAHLH. The treatment of NK/T-LAHLH is still mainly based on chemotherapy regimens containing etoposide and dexamethasone. Recently, many new therapeutic drugs and schemes have been trialled for the treatment of NK/T-LAHLH, such as ruxolitinib, immune checkpoint inhibitors, pegaspargase, and the DEP regimen. However, NK/T-LAHLH is associated with overall poor prognosis. Improving overall understanding of NK/T-LAHLH is of great significance to ameliorating patient prognosis. This review systematically discussed the epidemiology, pathogenesis, clinical features, current treatment regimens, and prognosis of NK/T-LAHLH to comprehensively elucidate this disease.
Keywords: NK/T-cell lymphoma, hemophagocytic lymphohistiocytosis, pathogenesis, treatment regimens, prognosis
Background
Hemophagocytic lymphohistiocytosis (HLH) is a rare immune-mediated syndrome wherein cytotoxic T lymphocytes and the mononuclear macrophage system over-activate and oversecrete inflammatory cytokines, leading to multiple organ injuries.1,2 The pathophysiological feature of HLH is hyper-inflammatory cytokinemia, and its main clinical and laboratory features include fever, hemocytopenia, hepatosplenomegaly, hyperferritin, organ injury, and coagulation dysfunction.1,2 Depending on its aetiology, HLH can be divided into primary and secondary types. Primary HLH is a recessive genetic disease,1,3 whereas secondary HLH’s aetiology includes infections, malignant tumours and autoimmune diseases. Lymphoma is the common cause of secondary HLH.4,5 In secondary lymphoma-based HLH, T-cell and NK/T-cell lymphoma (NKTL) are more common, and NKTL accounts for approximately 35% of cases.6 NKTL-associated HLH (NK/T-LAHLH) typically exhibits rapid progression, impaired treatment response, and poor prognosis. This study aimed to synthesise recent studies on NK/T-LAHLH and provide an overview of its epidemiology, pathogenesis, diagnosis, current therapies, and prognostic factors.
Epidemiology of NK/T-LAHLH
NK/T-LAHLH incidence varies among studies. Regarding the increased prevalence of NKTL in Asia and Latin America, its main epidemiological data are derived from Asian studies. Moreover, NKTL is the predominant cause of lymphoma-triggered HLH in Asia7,8 and is divided into nodal and extranodal NKTL (ENKTL). In Asia, North America, and Europe, ENKTL accounts for 22.4%, 5.1%, and 4.3% of peripheral T-cell and NKTL, respectively.9 Thus, ENKTL-related HLH is the most common type of NK/T-LAHLH. According to studies on the Chinese population, NK/T-LAHLH incidence ranges from 7.1% to 57.1%.10–15 In a study involving 202 patients with ENKTL, 11.4% had HLH, and Jia et al reported that in a 202 cohort of patients with ENKTL, HLH incidence was 11.4% (23/202).11 In a retrospective study by Li et al, HLH occurred in 21 of 295 patients with ENKTL, with an incidence of 7.1%.12 Wei et al revealed that of 363 patients with ENKTL, 43 developed HLH with an incidence rate of 11.9%.13 Moreover, He et al discovered that HLH occurred in 108 of 1134 ENKTL cases, and that the incidence of NK/T-LAHLH was 9.5%.14 In contrast, another study conducted by a large HLH centre in Beijing found that 57.1% of patients had HLH.15 While, HLH incidence should increase in specialised centres, the substantial risk of underdiagnosis in studies that reported a relatively lower incidence could not be overlooked. Through previous large-sample studies reported, it was found that the incidence of NK/T-LAHLH was approximately 7.1–11.9%.11–14 NK/T-LAHLH incidence has not been reported in large-scale case studies in Europe and North America.
Pathogenesis of NK/T-LAHLH
The specific pathogenesis of NK/T-LAHLH remains unclear at present. Several possible mechanisms have been suggested for its involvement in NK/T-LAHLH (Figure 1). Wen et al demonstrated an association between a mutation (c.419T>C) in the evolutionarily conserved signalling intermediate in the Toll pathway (ECSIT) gene and NK/T-LAHLH.16 The variant triggers NF-κB pathway through increasing its binding with S100A8/S100A9 heterodimer, elevating the affinity of arachidonic acid to S100A9, promoting the assembly of NADPH oxidase as well as overproduction of interferon gamma (IFN-γ) and tumour necrosis factor α (TNF-α), inducing macrophages and cytokine storm. However, in another multiple-cohort study, the researchers prompted a contrary view.17 The ECSIT-T419 mutation was verified to be a germline mutation, as reported in previous studies, with no association to NK/T-LAHLH.17 Therefore, additional studies are required to assess the role of the ECSIT-T419 variant in NK/T-LAHLH.
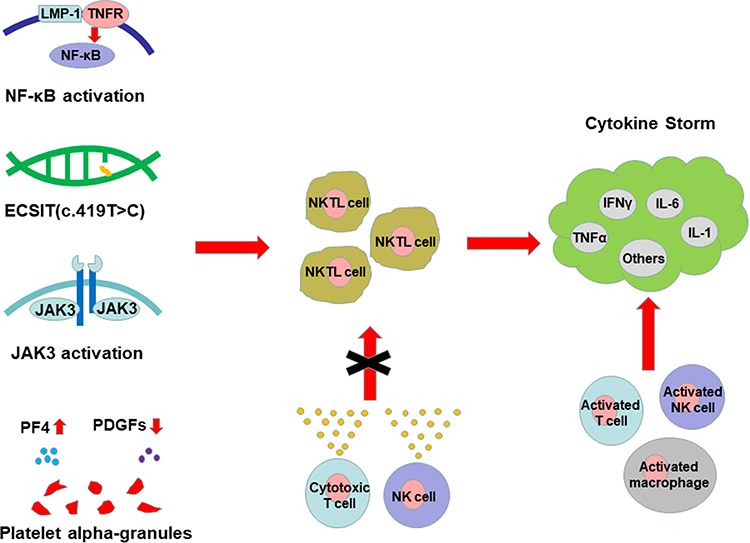 |
Figure 1 Pathogenesis diagram of NK/T-LAHLH. |
Studies have demonstrated the essential role of JAK3 and its related signalling in NKTL pathogenesis.18–20 Picod et al reveal that constitutively activated JAK3 leads to the hypersecretion of IFN-γ through the increase of NK cells sensitivity to interleukin-2.21 When transplanting JAK3A573V-transduced bone marrow cells into a wild-type model, researchers observed an expansion of NK cells and the development of HLH in recipients.
Platelets are essential to this process, as the specific platelets produced in patients with NK/T-LAHLH releasing alpha-granules containing upregulated platelet factor 4 (PF4) and reducing platelet-derived growth factor (PDGFs), ultimately contributing to inflammation overactivation.22
Epstein–Barr virus (EBV), a DNA virus belonging to the genus Lymphocytophilus in the Herpesviridae family, which drives the development of primary HLH and participates in lymphoma-related HLH.23–28 Moreover, EBV is present in >90% of NKTL cases. Several studies have attempted to elucidate the mechanism whereby EBV triggers T-cell lymphoma-associated HLH. When infecting T cells, EBV expresses latent membrane protein 1 (LMP-1) and induces TNFR-associated factor/NF-κB/ERK signalling to promote cytokine secretion.29,30 Additionally, the activated NF-κB signalling protects the infected T cells from TNF-α-induced apoptosis. In another study, the localisation of EBV infection had highly significant effects on patient prognosis. In PTCL, patients with T-cell infection have a worse prognosis than those with B-EBV, as EBV exclusively localises to B cells and is correlated with a low incidence of HLH.31
Clinical Characteristic and Risk Factors of NK/T-LAHLH
NK/T-LAHLH diagnosis relies on the criteria for both NKTL and HLH, of which the most widely accepted criteria for HLH are the HLH-2004 revised by the International Histopathological Society.32 Owing to the similarities between the clinical symptoms of NKTL and HLH, diagnosing lymphoma-related early-stage HLH is difficult. The reported common clinical features of NK/T-LAHLH include: Fever,12,33 splenomegaly,12,15,33 lymphadenopathy,12 younger age,11,15 type B symptoms,15 Ann Arbor stage III/IV,15 international prognostic index (IPI) score ≥3,15,34 bone marrow involvement.11,15 Furthermore, the most common laboratory test features were hyperferriminemia,12,33 cytopenia,12,15,33 hypertriglyceridemia,12,33 hypofibrinogenemia,12,33 liver dysfunction,12 elevated lactate dehydrogenase (LDH),12,15 decreased serum albumin levels,15 and the higher positive rate of EBV.34 Multivariate analysis showed that the risk factors of NK/T-LAHLH were higher Eastern Cooperative Tumor Group (ECOG) score,33 upper respiratory extrinsic NK/T-cell lymphoma (EUNKTL),33 skin involvement,33 bone marrow involvement,12 hepatosplenomegaly,12 and elevated LDH,12,15 Ann Arbor stage III/IV,15 younger age15 and decreased serum albumin level.15
Treatment of NK/T-LAHLH
Currently, no unified or effective first-line treatment for NK/T-LAHLH exits.13,15,35 The treatment regimens for NK/T-LAHLH mainly include the HLH-1994/HLH-2004 regimen, a chemotherapy regimen containing L-asparaginase or pegaspargase, and the DEP (liposomal doxorubicin, etoposide and methylprednisolone) regimen. The above regimens mainly focus on the treatment of HLH itself. There are also many studies reporting that patients directly receive chemotherapy regimens for lymphoma. In conclusion, in the current reports on NK/T-LAHLH, various treatment regimens have been applied, and the therapeutic responses have varied (Table 1). However, current studies on the treatment of NK/T-LAHLH are limited in number and generally small in sample size, making it difficult to draw definitive conclusions about the efficacy of specific therapeutic agents. Moreover, in the treatment of NK/T-LAHLH, the treatment of lymphoma itself is very important. After HLH is controlled, a transition to the treatment of lymphoma should be made as soon as possible in order to achieve long-term survival.
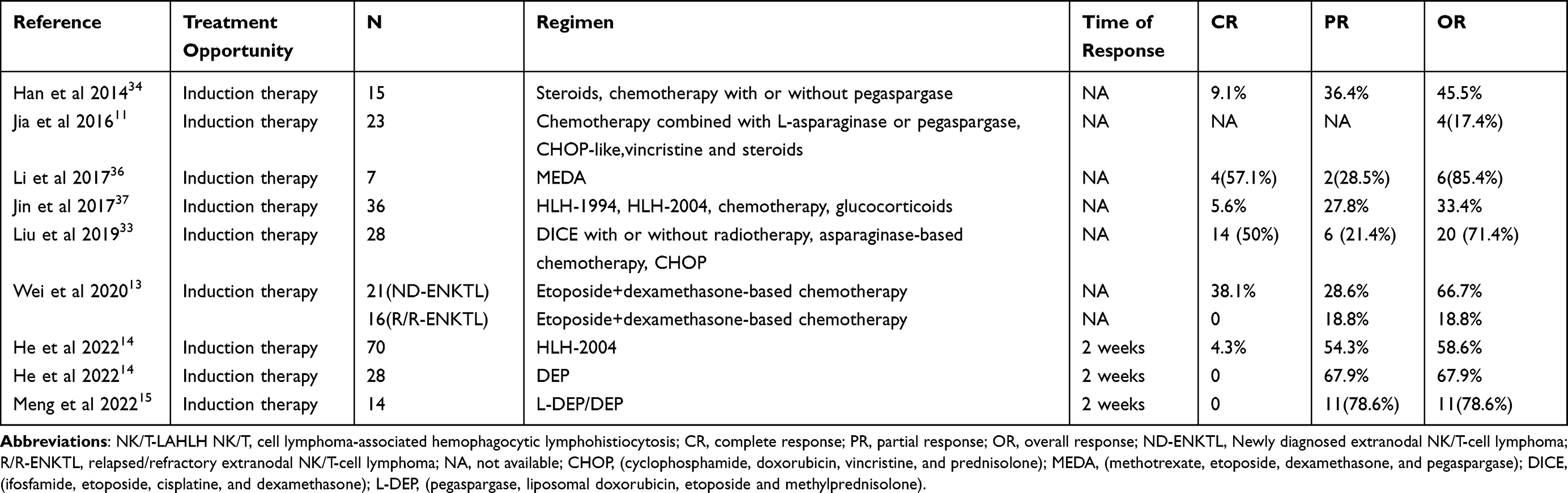 |
Table 1 Treatment Regimens and Responses for NK/T-LAHLH |
In the treatment of HLH, etoposide and dexamethasone-based HLH-1994 regimen and HLH-2004 regimen are still recommended as first-line therapy.35,38 Therefore, for the treatment of NK/T-LAHLH, this type of regimen is relatively common and has achieved good therapeutic effects. He et al reported that 70 patients with NK/T-LAHLH were treated using the HLH-2004 regimen.14 Although the complete response (CR) rate was only 4.3%, the total efficacy rate was 58.6%. Wei et al reported that patients with NK/T-LAHLH received etoposide in combination with dexamethasone-based combination chemotherapy.13 In 21 patients newly diagnosed with lymphoma-based HLH, the overall response (OR) rate was 66.7%. In addition, Jin et al reported 36 cases of NK/T-LAHLH, where in addition to the HLH-1994 and HLH-2004 regimens, some patients still received lymphoma chemotherapy and glucocorticoid therapy regimens alone, with a total effective treatment rate of only 33.4%.37
In addition, some studies have reported that patients directly receive chemotherapy regimens for lymphoma. For instance, Liu et al reported 28 cases of NK/T-LAHLH.33 After DICE (ifosfamide, etoposide, cisplatine, and dexamethasone) regimen with or without radiotherapy, asparaginase-based chemotherapy, and CHOP (cyclophosphamide, doxorubicin, vincristine, and prednisolone) regimen, the CR rate was 50%, OR rate was 71.4%, and a good response rate was obtained. However, Jia et al reported that 23 patients received chemotherapy, including CHOP-like regimens, and the total response rate post-treatment was only 17.4%.11 The response rate varied among patients who primarily received a chemotherapy regimen for lymphoma.
The DEP regimen was initially reported as a salvage treatment for relapsed/refractory HLH in adults, and the total efficacy rate post-treatment was 76.2%.39 Since then, the DEP regimen has been reported to treat various types of HLH, all of which have shown good therapeutic response.40–43 Compared to the traditional HLH regimen, the DEP regimen included a new drug, liposomal doxorubicin, with a mechanism of action involving the primary targeting of activated monocytes and macrophages.44,45 In a clinical study of lymphoma-associated HLH, the OR rates after 4 weeks of first-line treatment with the DEP and HLH-1994 regimens were 89.4% and 68.0%, respectively, suggesting that the DEP regimen was superior to the HLH-1994 regimen.41 He et al reported that 28 patients with NK/T-LAHLH received the DEP regimen for 2 weeks and had a total effective rate of 67.9%, achieving a good therapeutic response.14 In another clinical study on NK/T-LAHLH, some patients received DEP regimen-based pegaspargase, with a total effective rate of 78.6% following 2 weeks.15 These studies suggest that the DEP regimen may be suitable for treating NK/T-LAHLH.
At present, studies have shown that pegaspargase targets tumour cells, causing them to fail to synthesise L-asparagine and die. It may also target EBV-infected T and NK cells, inhibiting the proliferation of EBV-infected cells, resulting in a decline of EBV-DNA.46,47 Therefore, pegaspargase may be more suitable for patients with NK/T-LAHLH, as >90% of these patients are EBV-positive. Han et al added pegaspargase to a chemotherapy regimen for NK/T-LAHLH, achieving a total response rate of 45.5%.34 In a clinical study by Li et al, seven patients with NK/T-LAHLH were treated with a MEDA (methotrexate, etoposide, dexamethasone, and pegaspargase) regimen containing pegaspargase, with an OR rate as high as 85.4%.36 In addition, the total response rate of NK/T-LAHLH was 78.6% with the pegaspargase-containing an L-DEP/DEP regimen.41 Thus, pegaspargase is an important therapeutic agent for patients with NK/T-LAHLH.
The JAK1/JAK2 inhibitor, ruxolitinib, treats HLH by blocking the JAK-STAT pathway and reducing the production of inflammatory factors.48–53 Currently, ruxolitinib is used to treat NK/T-LAHLH. For instance, Zhou et al reported that ruxolitinib combined with DED (doxorubicin, etoposide, and dexamethasone) regimen was used to treat lymphoma-associated HLH.54 Among them, 36 patients (23 with NK/T-LAHLH) treated with the R-DED regimen had total response rate of 83.3%, significantly higher than that of the HPH-1994 regimen (54.8%). However, patients with NK/T-LAHLH were excluded from this analysis. Zhao et al reported that a patient with NK/T-LAHLH achieved partial remission post-treatment with ruxolitinib and dexamethasone.55 Therefore, ruxolitinib combination therapy may be a safe and effective treatment option for patients with NK/T-LAHLH.
Immune checkpoint inhibitors have been widely used to treat relapsed/refractory NKTL,56–58 as programmed cell death protein 1 (PD-1) inhibitors have been reported to improve the overall survival of patients with NK/T-LAHLH. He et al reported on 98 NK/T-LAHLH cases,14 after receiving the HLH-2004 and DEP regimens to treat HLH, the patients were coupled with anti-ENKTL chemotherapy with or without a PD-1 inhibitor. They found that patients treated with a PD-1 inhibitor achieved better survival. He et al also discovered that the EBV DNA of patients in the group receiving anti-ENKTL chemotherapy combined with a PD-1 inhibitor was significantly lower than before.14 Moreover, Liu et al documented seven cases of relapsed/refractory EBV-associated HLH were treated with PD-1 inhibitors, of which six cases showed a treatment response and five cases achieved and maintained clinical complete remission,59 with EBV-DNA being negative in four patients. Therefore, the use of PD-1 inhibitors in HLH induction therapy was attempted for EBV-positive NK/T-LAHLH. Xu et al reported that two patients with ENKTL-related HLH were treated with a PD-1 inhibitor combined with chidamide, and that HLH and ENKTL were alleviated post-treatment.60 Two patients achieved durable survival without immune-related adverse events. Thus, PD-1 inhibitors can safely and effectively treat NK/T-LAHLH.
Hematopoietic stem cell transplantation (HSCT) is recommended for patients with primary and relapsed/refractory HLH. Currently, few studies exits on patients with NK/T-LAHLH receiving HSCT, of which, most are case reports and small-sample clinical studies. Inoue et al reported that a patient with NK/T-LAHLH did not respond to treatment with etoposide and glucocorticoid, and PR was obtained following treatment with SMILE (dexamethasone, methotrexate, ifosfamide, L-asparaginase, and etoposide) regimen combined with local radiotherapy. Additionally, CR was obtained after autologous HSCT (auto-HSCT), and a second auto-HSCT was performed post-chemotherapy,61 and the CR continued following 2 years of follow-up. Liu et al reported a patient with NK/T-LAHLH who received allogeneic HSCT (allo-HSCT) post-HLH treatment and remained alive at the last follow-up.33 In addition, Han et al reported that four cases of lymphoma-associated HLH underwent auto-HSCT, of which one case was ENKTL, and achieved PR post-transplantation.62 In another study involving 48 cases of NK/T-LAHLH, six patients survived to the last follow-up, of which two received auto-HSCT and two received allo-HSCT.41 Recent studies have shown that HSCT improved the prognosis of patients with NK/T-LAHLH and prolonged their survival. Therefore, HSCT is recommended in patients with NK/T-LAHLH.
In conclusion, for the induction therapy of newly diagnosed NK/T-LAHLH patients, it is recommended to accept regimens containing chemotherapy drugs, such as the HHL-1994 regimen, HHL-2004 regimen, DEP regimen and MEDA regimen. Moreover, the combination of the above chemotherapy regimens with pegaspargase or ruxolitinib can achieve a better response. For relapsed/refractory NK/T-LAHLH, the combination of PD-1 inhibitors on the basis of the above chemotherapy regimens may achieve a good therapeutic response. And HSCT can improve the prognosis of NK/T-LAHLH and prolong the survival.
Prognostic Factors of NK/T-LAHLH
NK/T-LAHLH has a poor prognosis and short survival time. Most studies have found that the median survival time of such patients is <1 month, and occasional reports have indicated that the median survival time is >2 months.11,33,34,41 Therefore, exploring the factors that can predict patient survival has always been an important focus of clinical research. Several studies identified various prognostic factors. For instance, Liu et al found that elevated serum LDH, hypofibrinogenaemia, and splenomegaly suggests poor survival in patients with NK/T-LAHLH.33 Meanwhile, Jia et al found that patients with NK/T-LAHLH, an LDH level >1000 U/L, and disseminated intravascular coagulation had a shorter survival time.11 In addition, Han et al found that poor survival in NK/T-LAHLH was associated with the following predictors: HLH onset at lymphoma diagnosis, high Ki-67 index, and poor treatment response.34 Using multivariate Cox regression model analysis, Wei et al found that relapsed/refractory NKTL and non-nasal disease were independent risk factors for poor survival and prognosis in patients with NK/T-LAHLH.11 He et al conducted multivariate analysis to determined that ECOG PS ≥2 was an independent prognostic risk factor for NK/T-LAHLH.14 Therefore, PD-1 inhibitor and pegaspargase treatment were independent factors for prolonged survival. The above mentioned predictors are of great significance for predicting NK/T-LAHLH prognosis and guiding clinical treatment in advance.
Conclusions
NK/T-LAHLH is a rare clinical syndrome associated with poor treatment outcomes, high mortality rates, and an unclear pathogenesis. NKTL and HLH have many overlapping clinical features, such as fever, hemocytopenia, hepatosplenomegaly, liver function impairment, and elevated lactate dehydrogenase. Therefore, for NKTL patients with rapid disease progression and organ failure in the short term, HLH should be vigilant, and serum ferritin, soluble CD25 and NK cell activity should be paid attention to HLH related indicators to determine whether there is HLH. In addition, studies have found that chemotherapy regimens based on etoposide and dexamethasone, such as the HLH-1994 and HLH-2004 regimens, DEP regimen, and MEDA regimen, can enable NK/T-LAHLH patients to achieve good therapeutic responses. And HSCT can improve the long-term prognosis of patients. However, no recognised unified first-line treatment regimen exists for NK/T-LAHLH. Thus, an appropriate and effective treatment regimen needs to be further explored.
Data Sharing Statement
No datasets were generated or analysed during this study.
Funding
This work was supported by Natural Science Foundation of Shandong Province (ZR2025MS1378, ZR2024QH282) and Scientific Research Nurturing Fund of the First Affiliated Hospital of Shandong First Medical University & Shandong Provincial Qianfoshan Hospital (QYPY2025NSFC0801).
Disclosure
There are no conflicts of interest.
References
1. Griffin G, Shenoi S, Hughes GC. Hemophagocytic lymphohistiocytosis: an update on pathogenesis, diagnosis, and therapy. Best Pract Res Clin Rheumatol. 2020;34(4):101515. doi:10.1016/j.berh.2020.101515
2. Al-Samkari H, Berliner N. Hemophagocytic Lymphohistiocytosis. Annu Rev Pathol. 2018;13:27–9. doi:10.1146/annurev-pathol-020117-043625
3. Ramachandran S, Zaidi F, Aggarwal A, et al. Recent advances in diagnostic and therapeutic guidelines for primary and secondary hemophagocytic lymphohistiocytosis. Blood Cells Mol Dis. 2017;64:53–57. doi:10.1016/j.bcmd.2016.10.023
4. Setiadi A, Zoref-Lorenz A, Lee CY, Jordan MB, Chen LYC. Malignancy-associated haemophagocytic lymphohistiocytosis. Lancet Haematol. 2022;9(3):e217–e227. doi:10.1016/S2352-3026(21)00366-5
5. Rivière S, Galicier L, Coppo P, et al. Reactive hemophagocytic syndrome in adults: a retrospective analysis of 162 patients. Am J Med. 2014;127(11):1118–1125. doi:10.1016/j.amjmed.2014.04.034
6. Lehmberg K, Nichols KE, Henter JI, Study Group on Hemophagocytic Lymphohistiocytosis Subtypes of the Histiocyte Society, et al. Consensus recommendations for the diagnosis and management of hemophagocytic lymphohistiocytosis associated with malignancies. Haematologica. 2015;100(8):997–1004. doi:10.3324/haematol.2015.123562
7. Wang H, Fu BB, Gale RP, Liang Y. NK-/T-cell lymphomas. Leukemia. 2021;35(9):2460–2468. doi:10.1038/s41375-021-01313-2
8. He X, Gao Y, Li Z, Huang H. Review on natural killer/T-cell lymphoma. Hematol Oncol. 2023;41(2):221–229. doi:10.1002/hon.2944
9. Vose J, Armitage J, Weisenburger D. International T-cell lymphoma project. International peripheral T-cell and natural killer/T-cell lymphoma study: pathology findings and clinical outcomes. J Clin Oncol. 2008;26(25):4124–4130.
10. Tong H, Ren Y, Liu H, et al. Clinical characteristics of T-cell lymphoma associated with hemophagocytic syndrome: comparison of T-cell lymphoma with and without hemophagocytic syndrome. Leuk Lymphoma. 2008;49(1):81–87. doi:10.1080/10428190701713630
11. Jia J, Song Y, Lin N, et al. Clinical features and survival of extranodal natural killer/T cell lymphoma with and without hemophagocytic syndrome. Ann Hematol. 2016;95(12):2023–2031. doi:10.1007/s00277-016-2805-9
12. Li N, Zhang L, Liu J, et al. A clinical study of 21 patients with hemophagocytic syndrome in 295 cases diagnosed with nasal type, extranodal nature killer/T cell lymphoma. Cancer Biol Ther. 2017;18(4):252–256. doi:10.1080/15384047.2017.1295176
13. Wei L, Yang L, Cong J, et al. Using etoposide + dexamethasone-based regimens to treat nasal type extranodal natural killer/T-cell lymphoma-associated hemophagocytic lymphohistiocytosis. J Cancer Res Clin Oncol. 2021;147(3):863–869. doi:10.1007/s00432-020-03376-7
14. He Y, Gao Y, Ping L, et al. The emerging role of anti-PD-1 antibody-based regimens in the treatment of extranodal NK/T-cell lymphoma-associated hemophagocytic lymphohistiocytosis. J Cancer Res Clin Oncol. 2023;149(5):2017–2027. doi:10.1007/s00432-022-04147-2
15. Meng G, Wang J, Cui T, Wang Z. Clinical characteristics and treatment of NK/T-cell lymphoma-associated HLH. Ann Hematol. 2022;101(10):2289–2296. doi:10.1007/s00277-022-04953-1
16. Wen H, Ma H, Cai Q, et al. Recurrent ECSIT mutation encoding V140A triggers hyperinflammation and promotes hemophagocytic syndrome in extranodal NK/T cell lymphoma. Nat Med. 2018;24(2):154–164. doi:10.1038/nm.4456
17. Ong SY, Lim JQ, Grigoropoulos N, et al. No association between ECSIT germline mutations and hemophagocytic lymphohistiocytosis in natural killer/T-cell lymphoma. Haematologica. 2021;106(6):1737–1739. doi:10.3324/haematol.2020.269209
18. Bouchekioua A, Scourzic L, de Wever O, et al. JAK3 deregulation by activating mutations confers invasive growth advantage in extranodal nasal-type natural killer cell lymphoma. Leukemia. 2014;28(2):338–348. doi:10.1038/leu.2013.157
19. Sim SH, Kim S, Kim TM. Novel JAK3-activating mutations in extranodal NK/T-cell lymphoma, nasal type. Am J Pathol. 2017;187(5):980–986. doi:10.1016/j.ajpath.2017.01.004
20. Lee S, Park HY, Kang SY, et al. Genetic alterations of JAK/STAT cascade and histone modification in extranodal NK/T-cell lymphoma nasal type. Oncotarget. 2015;6(19):17764–17776. doi:10.18632/oncotarget.3776
21. Picod A, Martino S, Cervera P, et al. Deregulated JAK3 mediates growth advantage and hemophagocytosis in extranodal nasal-type natural killer/T-cell lymphoma. Haematologica. 2022;107(9):2218–2225. doi:10.3324/haematol.2021.280349
22. Ren Q, Chan KW, Huang H, et al. Platelet-derived alpha-granules are associated with inflammation in patients with NK/T-cell lymphoma-associated hemophagocytic syndrome. Cytokine. 2020;126:154878. doi:10.1016/j.cyto.2019.154878
23. Nowalk A, Green M. Epstein-Barr Virus. Microbiol Spectr. 2016;4(3). doi:10.1128/microbiolspec.DMIH2-0011-2015
24. El-Mallawany NK, Curry CV, Allen CE. Haemophagocytic lymphohistiocytosis and Epstein-Barr virus: a complex relationship with diverse origins, expression and outcomes. Br J Haematol. 2022;196(1):31–44. doi:10.1111/bjh.17638
25. Imashuku S, Morimoto A, Ishii E. Virus-triggered secondary hemophagocytic lymphohistiocytosis. Acta Paediatr. 2021;110(10):2729–2736. doi:10.1111/apa.15973
26. Williams M, Afify Z. Epstein-Barr virus-associated hemophagocytic lymphohistiocytosis in X-linked lymphoproliferative disease. Blood. 2022;139(18):2847. doi:10.1182/blood.2022015531
27. Xu L, Guo X, Guan H. Serious consequences of Epstein-Barr virus infection: hemophagocytic lymphohistocytosis. Int J Lab Hematol. 2022;44(1):74–81. doi:10.1111/ijlh.13736
28. Hoffman J, Lossos IS. Lymphoma associated hemophagocytic syndrome: it’s going viral. Leuk Lymphoma. 2014;55(9):1964–1965. doi:10.3109/10428194.2014.914200
29. Chuang HC, Lay JD, Chuang SE, Hsieh WC, Chang Y, Su IJ. Epstein-Barr virus (EBV) latent membrane protein-1 down-regulates tumor necrosis factor-alpha (TNF-alpha) receptor-1 and confers resistance to TNF-alpha-induced apoptosis in T cells: implication for the progression to T-cell lymphoma in EBV-associated hemophagocytic syndrome. Am J Pathol. 2007;170(5):1607–1617. doi:10.2353/ajpath.2007.061026
30. Chuang HC, Lay JD, Hsieh WC, Su IJ. Pathogenesis and mechanism of disease progression from hemophagocytic lymphohistiocytosis to Epstein-Barr virus-associated T-cell lymphoma: nuclear factor-kappa B pathway as a potential therapeutic target. Cancer Sci. 2007;98(9):1281–1287. doi:10.1111/j.1349-7006.2007.00549.x
31. Chen YP, Jones D, Chen TY, Chang KC. Epstein-Barr virus present in T cells or B cells shows differential effects on hemophagocytic symptoms associated with outcome in T-cell lymphomas. Leuk Lymphoma. 2014;55(9):2038–2047. doi:10.3109/10428194.2013.861068
32. Henter JI, Horne A, Aricó M, et al. HLH-2004: diagnostic and therapeutic guidelines for hemophagocytic lymphohistiocytosis. Pediatr Blood Cancer. 2007;48(2):124–131. doi:10.1002/pbc.21039
33. Liu YZ, Bi LQ, Chang GL, Guo Y, Sun S. Clinical characteristics of extranodal NK/T-cell lymphoma-associated hemophagocytic lymphohistiocytosis. Cancer Manag Res. 2019;11:997–1002. doi:10.2147/CMAR.S183784
34. Han L, Li L, Wu J, et al. Clinical features and treatment of natural killer/T cell lymphoma associated with hemophagocytic syndrome: comparison with other T cell lymphoma associated with hemophagocytic syndrome. Leuk Lymphoma. 2014;55(9):2048–2055. doi:10.3109/10428194.2013.876629
35. Rosée P L, Horne A, Hines M, et al. Recommendations for the management of hemophagocytic lymphohistiocytosis in adults. Blood. 2019;133(23):2465–2477. doi:10.1182/blood.2018894618
36. Li DH, Zhang XY, Du C, et al. Successful treatment of extranodal natural killer/T-cell lymphoma-associated hemophagocytic lymphohistiocytosis with MEDA chemotherapy. Leuk Lymphoma. 2017;58(5):1238–1241. doi:10.1080/10428194.2016.1228931
37. Jin Z, Wang Y, Wang J, et al. Multivariate analysis of prognosis for patients with natural killer/T cell lymphoma-associated hemophagocytic lymphohistiocytosis. Hematology. 2018;23(4):228–234. doi:10.1080/10245332.2017.1385191
38. Summerlin J, Wells DA, Anderson MK, Halford Z. A review of current and emerging therapeutic options for hemophagocytic lymphohistiocytosis. Ann Pharmacother. 2023;57(7):867–879. doi:10.1177/10600280221134719
39. Wang Y, Huang W, Hu L, et al. Multicenter study of combination DEP regimen as a salvage therapy for adult refractory hemophagocytic lymphohistiocytosis. Blood. 2015;126(19):2186–2192. doi:10.1182/blood-2015-05-644914
40. Wang J, Wang Y, Wu L, Zhang J, Lai W, Wang Z. PEG-aspargase and DEP regimen combination therapy for refractory Epstein-Barr virus-associated hemophagocytic lymphohistiocytosis. J Hematol Oncol. 2016;9(1):84. doi:10.1186/s13045-016-0317-7
41. Meng G, Wang Y, Wang J, Wang Z. The DEP regimen is superior to the HLH-1994 regimen as first-line therapy for lymphoma-associated haemophagocytic lymphohistiocytosis. Leuk Lymphoma. 2021;62(4):854–860. doi:10.1080/10428194.2020.1849671
42. Pi Y, Wang J, Zhou H, et al. Modified DEP regimen as induction therapy for lymphoma-associated hemophagocytic lymphohistiocytosis: a prospective, multicenter study. J Cancer Res Clin Oncol. 2023;149(7):3033–3041. doi:10.1007/s00432-022-04157-0
43. Chen L, Wang J, Wang Z. L-DEP regimen is effective as an initial therapy for adult EBV-HLH. Ann Hematol. 2022;101(11):2461–2470. doi:10.1007/s00277-022-04946-0
44. Schiffelers RM, Storm G, Bakker-Woudenberg IA. Host factors influencing the preferential localization of sterically stabilized liposomes in Klebsiella pneumoniae-infected rat lung tissue. Pharm Res. 2001;18(6):780–787. doi:10.1023/A:1011080211226
45. Huwyler J, Drewe J, Krähenbuhl S. Tumor targeting using liposomal antineoplastic drugs. Int J Nanomed. 2008;3(1):21–29. doi:10.2147/IJN.S1253
46. Ando M, Sugimoto K, Kitoh T, et al. Selective apoptosis of natural killer-cell tumours by l-asparaginase. Br J Haematol. 2005;130(6):860–868. doi:10.1111/j.1365-2141.2005.05694.x
47. Jinta M, Imadome K, Komatsu H, et al. L-Asparaginase monotherapy for EBV-positive T/NK lymphoproliferative diseases: a pilot study. J Med Dent Sci. 2015;62(1):1–9. doi:10.11480/620101
48. Morris R, Kershaw NJ, Babon JJ. The molecular details of cytokine signaling via the JAK/STAT pathway. Protein Sci. 2018;27(12):1984–2009. doi:10.1002/pro.3519
49. Villarino AV, Kanno Y, O’Shea JJ. Mechanisms and consequences of Jak-STAT signaling in the immune system. Nat Immunol. 2017;18(4):374–384. doi:10.1038/ni.3691
50. Xin P, Xu X, Deng C, et al. The role of JAK/STAT signaling pathway and its inhibitors in diseases. Int Immunopharmacol. 2020;80:106210. doi:10.1016/j.intimp.2020.106210
51. Keenan C, Nichols KE, Albeituni S. Use of the JAK inhibitor Ruxolitinib in the treatment of hemophagocytic lymphohistiocytosis. Front Immunol. 2021;12:614704. doi:10.3389/fimmu.2021.614704
52. Zhang Q, Zhao YZ, Ma HH, et al. A study of ruxolitinib response-based stratified treatment for pediatric hemophagocytic lymphohistiocytosis. Blood. 2022;139(24):3493–3504. doi:10.1182/blood.2021014860
53. Zhou D, Huang X, Xie M, et al. Ruxolitinib combined with dexamethasone in adult patients with newly diagnosed Hemophagocytic lymphohistiocytosis: a single-center pilot trial. Am J Hematol. 2023;98(5):E106–E109. doi:10.1002/ajh.26877
54. Zhou L, Liu Y, Wen Z, et al. Ruxolitinib combined with doxorubicin, etoposide, and dexamethasone for the treatment of the lymphoma-associated hemophagocytic syndrome. J Cancer Res Clin Oncol. 2020;146(11):3063–3074. doi:10.1007/s00432-020-03301-y
55. Zhao L, Yang H, Qu WY, Lu YJ, Feng Z. Case report: ruxolitinib plus dexamethasone as first-line therapy in haemophagocytic lymphohistiocytosis. Front Oncol. 2023;13:1054175. doi:10.3389/fonc.2023.1054175
56. Kwong YL, Chan TSY, Tan D, et al. PD1 blockade with pembrolizumab is highly effective in relapsed or refractory NK/T-cell lymphoma failing l-asparaginase. Blood. 2017;129(17):2437–2442. doi:10.1182/blood-2016-12-756841
57. Li B, VanRoey M, Wang C, Chen TH, Korman A, Jooss K. Anti-programmed death-1 synergizes with granulocyte macrophage colony-stimulating factor--secreting tumor cell immunotherapy providing therapeutic benefit to mice with established tumors. Clin Cancer Res. 2009;15(5):1623–1634. doi:10.1158/1078-0432.CCR-08-1825
58. Bi XW, Wang H, Zhang WW, et al. PD-L1 is upregulated by EBV-driven LMP1 through NF-κB pathway and correlates with poor prognosis in natural killer/T-cell lymphoma. J Hematol Oncol. 2016;9(1):109. doi:10.1186/s13045-016-0341-7
59. Liu P, Pan X, Chen C, et al. Nivolumab treatment of relapsed/refractory Epstein-Barr virus-associated hemophagocytic lymphohistiocytosis in adults. Blood. 2020;135(11):826–833. doi:10.1182/blood.2019003886
60. Xu QY, Yang HY, Li MW, He ZD, Hong HY, Peng ZG. Sintilimab combined with chidamide in the treatment of extranodal nature killer/T-cell lymphoma with secondary hemophagocytic lymphohistiocytosis: two case reports and literature review. Medicine. 2022;101(38):e30731. doi:10.1097/MD.0000000000030731
61. Inoue D, Nagai Y, Takiuchi Y, et al. Successful treatment of extranodal natural killer/T-cell lymphoma, nasal type, complicated by severe hemophagocytic syndrome, with dexamethasone, methotrexate, ifosfamide, L-asparaginase, and etoposide chemotherapy followed by autologous stem cell transplant. Leuk Lymphoma. 2010;51(4):720–723. doi:10.3109/10428191003682742
62. Han AR, Lee HR, Park BB, et al. Lymphoma-associated hemophagocytic syndrome: clinical features and treatment outcome. Ann Hematol. 2007;86(7):493–498. doi:10.1007/s00277-007-0278-6
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Patients with Hemophagocytic Lymphohistiocytosis Who Need Intensive Care Can Be Successfully Rescued by Timely Using Etoposide-Based HLH Regimens
Lv K, Cheng X, Zhou Y, Yu M, Wang S, Shen H, Li F
International Journal of General Medicine 2024, 17:431-446
Published Date: 3 February 2024
Influence of Type 2 Diabetes Mellitus on the Clinical Outcomes in Hospitalized Patients with Active Pulmonary Tuberculosis: A Retrospective, Single-Center, Real-World Study in China
Shi C, Shen X, Liu J, Huang L, Ni H, Tang P, Feng Y, Wu M, Zhang J
Infection and Drug Resistance 2025, 18:2415-2425
Published Date: 8 May 2025