Back to Journals » Journal of Hepatocellular Carcinoma » Volume 13
Multimodal Conversion Therapy Enabling Curative Resection in Giant Hepatocellular Carcinoma with Arteriovenous Fistula: A Case Report
Authors Zhong H, Tan L, Le W, Luo N ![]() , Shen Y, Long G, Xiong C, Tao H
, Shen Y, Long G, Xiong C, Tao H
Received 28 January 2026
Accepted for publication 18 May 2026
Published 26 May 2026 Volume 2026:13 599120
DOI https://doi.org/10.2147/JHC.S599120
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ali Hosni
Hengcheng Zhong,1,* Lanju Tan,2,* Wenjun Le,1 Ning Luo,3 Yongqi Shen,1 Guangyu Long,4 Chun Xiong,1 Haiyun Tao1
1Department of Tumor Hematology, The First Affiliated Hospital of Guangxi University of Science and Technology, Liuzhou, Guangxi, People’s Republic of China; 2First Clinical Medical College, Guangxi University of Science and Technology, Liuzhou, Guangxi, People’s Republic of China; 3Department of General Surgery, Xiangzhou County Hospital of Traditional Chinese Medicine, Laibin, Guangxi, People’s Republic of China; 4Department of Diagnostic Radiology, The First Affiliated Hospital of Guangxi University of Science and Technology, Liuzhou, Guangxi, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Haiyun Tao, Department of Tumor Hematology, The First Affiliated Hospital of Guangxi University of Science and Technology, Liuzhou, Guangxi, People’s Republic of China, Email [email protected]
Background: Giant hepatocellular carcinoma (GHCC) with arteriovenous fistula (AVF) is often considered a surgical no-go zone, lacking a standardized conversion therapy. This paper reports a case in which the implementation of sequential, integrated multimodal therapy, simultaneously targeting the tumor’s biological behavior and the fistula’s abnormal hemodynamics, successfully achieved substantial downstaging of the tumor, ultimately accomplishing curative resection.
Case Presentation: A 38-year-old male patient presented with recurrent abdominal distension and was diagnosed GHCC complicated by AVF, as confirmed by computed tomography (CT). The patient underwent tumor downstaging through a multimodal therapeutic approach, which integrated targeted therapy, immunotherapy, hepatic artery infusion chemotherapy (HAIC), transcatheter arterial chemoembolization (TACE), and radiotherapy. This comprehensive treatment strategy subsequently facilitated curative surgical resection. To date, the patient has attained an overall survival duration of 32 months.
Conclusion: This case suggests that a sequential multimodal strategy may enable downstaging and potential curative resection in selected patients; however, validation in larger cohorts is required.
Keywords: Giant Hepatocellular Carcinoma, Arteriovenous fistula, Immunotherapy, Targeted Therapy, Radiotherapy Interventions
Introduction
Primary hepatocellular carcinoma (HCC) frequently invades the hepatic venous system, leading to the development of hepatic arteriovenous fistulas (AVF). AVF occurs in approximately 14%–63.2% of HCC cases, with arterioportal shunts being the most common subtype.1 GHCC complicated by AVF represents an ultra-high-risk clinical subtype with a uniquely aggravated pathophysiology and dismal prognosis (mOS of 3–4 months without intervention).2 Due to risks of life-threatening hemorrhage and tumor dissemination, radical hepatectomy has conventionally been regarded as a relative contraindication.3 Additionally, AVF formation may cause ectopic embolization and reduce intratumoral drug deposition, further complicating treatment.4 This challenge is reflected in the BCLC 2025 strategy, which emphasizes the need for tailored approaches in advanced HCC with complex vascular invasions.5,6
In recent years, the integrated paradigm combining systemic therapies centered on targeted and immunotherapeutic agents with localized interventions has profoundly transformed the treatment landscape for advanced HCC.5,7–9 Conversion therapy—defined as downstaging initially unresectable tumors to enable curative resection—has emerged as a promising strategy, with reported resection rates of 15%–42% and improved survival outcomes in selected patients.10,11 However, the application of this paradigm to HCC with AVF remains a critical yet underexplored domain in clinical practice. Current literature focuses primarily on AVF diagnosis and complication management,12 with limited reports on multimodal protocols targeting AVF to enable radical surgery.
This case report describes a patient with HCC complicated by AVF who achieved successful tumor downstaging through sequential multimodal therapy, ultimately enabling curative resection. The principal significance lies in challenging the conventional view of AVF as an absolute surgical contraindication and providing a practical framework for this ultra-high-risk population.
Case Presentation
In May 2023, a 38-year-old male patient with chronic hepatitis B virus infection was found to have two hepatic lesions: one in the right lobe (17.8 cm × 13.6 cm × 17.2 cm) and one in the left lobe (6.6 cm× 4.7 cm × 6.9 cm). Abdominal MRI revealed primary HCC of the right and left lobes, characterized as a giant mass type. The right lobe lesion exhibited hemorrhage, an AVF with cancerous thrombosis in the right hepatic vein, and possible invasion of the right peritoneum and omentum. Potential retroperitoneal lymph node metastasis was also noted (Figure 1). At diagnosis, liver function was Child-Pugh A and serum AFP level was 12424.36ng/mL (Figure 2). The patient was diagnosed with primary hepatocellular carcinoma (CNLC stage IIIb, TNM stage IVa).
 |
Figure 1 Contrast-enhanced MRI (2023.05.08) of the lesions before treatment. Maximum tumor diameters measured 17.8 cm in the right hepatic lobe and 6.9 cm in the left hepatic lobe.The imaging demonstrates a giant, bilobar hepatocellular carcinoma with heterogeneous arterial enhancement and washout in the delayed phase. |
 |
Figure 2 Changes in serum AFP levels (ng/mL) during anticancer therapy. The y-axis represents AFP concentration (ng/mL), and the x-axis represents the date of measurement. The AFP level decreased from 12,424.36 ng/mL at diagnosis (2023.05.05) to 1.96 ng/mL at the latest follow-up (2026.01.19). |
The multidisciplinary team (MDT) recommended against immediate surgical resection due to the GHCC with AVF, a MELD score of 17, and a FLR of only 28.06%. Instead, a combined regimen of targeted therapy, immunotherapy and interventional therapy (HAIC and/or TACE) was proposed.
Treatment summary: The patient received a sequential multimodal conversion therapy following the roadmap: donafenib plus tislelizumab (D+T) combined with HAIC → D+T plus HAIC and TACE → D+T plus external beam radiotherapy (EBRT) → curative liver resection → postoperative D+T. The complete timeline is presented in Figure 3.
 |
Figure 3 Timeline scheme of the major clinical events since HCC diagnosis. Upper row: Disease status at each timepoint. Lower row: Corresponding treatment regimen. The patient achieved PR after HAIC and maintained PR through subsequent treatments, ultimately achieving CR following surgery. Abbreviations: PR, partial response; CR, complete response; D, donafenib; T, tislelizumab; HAIC, hepatic artery infusion chemotherapy; TACE, transcatheter arterial chemoembolization; EBRT, external beam radiotherapy. |
Detailed treatment course: in May 2023, treatment with tislelizumab (200mg, q21d) in combination with donafenib (200mg, twice daily) was initiated, along with two concurrent cycles of HAIC, in August 2023, combined HAIC (FOLFOX4)-TACE was performed. Subsequently, in October 2023, EBRT (36Gy/12 fractions) was delivered to the left hepatic lesion. Following these treatments, the AFP level decreased to 6.29 ng/mL, and the patient achieved a partial response (PR) per RECIST 1.1 criteria (Figure 4).
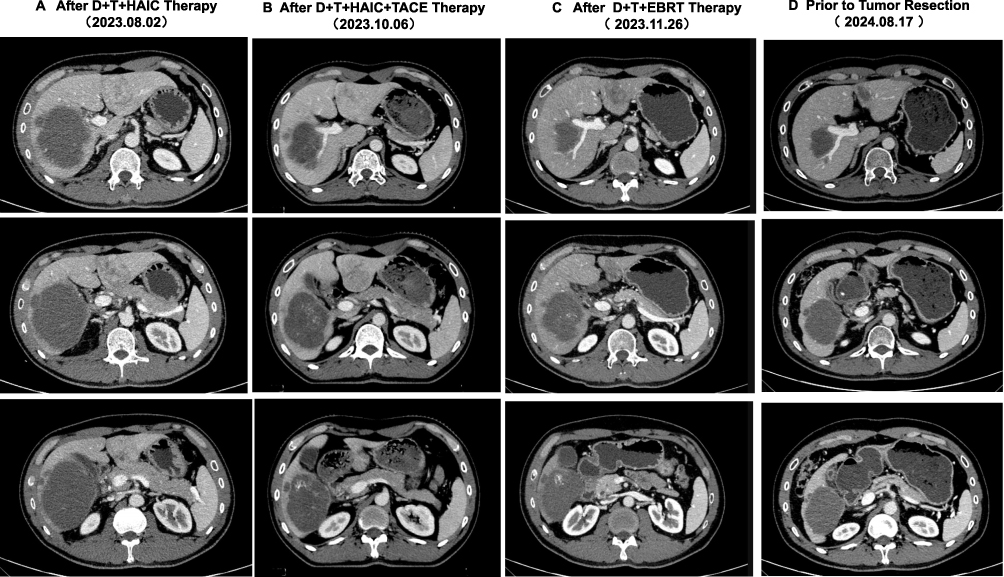 |
Figure 4 Contrast-enhanced CT imaging demonstrating tumor response at different treatment stages. (A) Contrast-enhanced CT imaging (2023.08.02) after the second cycle of D+T+HAIC therapy, Maximum tumor diameters measure 9.0 cm in the right hepatic lobe and 4.5 cm in the left hepatic lobe, representing significant tumor shrinkage. (B) Contrast-enhanced CT imaging (2023.10.06) after D+T+HAIC+TACE therapy, Maximum tumor diameters measure 8.0 cm in the right hepatic lobe and 4.5 cm in the left hepatic lobe, showing continued response. (C) Contrast-enhanced CT imaging (2023.11.26) of the left lesion after D+T+EBRT therapy, Maximum tumor diameters measure 7.3 cm in the right hepatic lobe and 3.5 cm in the left hepatic lobe. (D) Contrast-enhanced CT imaging (2024.08.27) prior to tumor resection, Maximum tumor diameters measure 7.3 cm in the right hepatic lobe and 3.0cm in the left hepatic lobe, achieving further downstaging and meeting surgical criteria. |
In August 2024, imaging showed significant reduction: right lobe lesion measured: 7.3 cm× 5.6 cm × 5.6cm; left lobe lesion measured: 3.0 cm× 2.8 cm×2.1cm (Figure 4). Repeat MDT review confirmed successful downstaging (MELD score: 18; ICGR15: 3.6%; FLR: 86.91%; Child-Pugh A). In September 2024, the patient underwent hepatectomy combined with cholecystectomy. Postoperative pathological revealed no viable carcinoma in the right liver lobe tumor or gallbladder, with negative surgical margins. The residual tumor in the left lobe: the maximum dimension of the residual tumor measuring “0.5 cm × 0.4 cm”(Figure 4). Postoperative liver function normalized, and maintenance therapy with donafenib and tislelizumab was continued.
Follow-up: MRI scans were routinely every 3 months along with blood routine, liver function, kidney function, electrolyte, thyroid function, and pituitary function. As of January 2026, the serum AFP level had decreased to 1.96ng/mL (Figure 2), with no tumor evidence of recurrence or metastasis (Figure 5). Treatment-related adverse events were mild: elevated ALT (grade 1), decreased hemoglobin (grade 1), and hypokalemia (grade 1). The timeline scheme of the major clinical events of the patient since HCC diagnosis is illustrated in Figure 3.
 |
Figure 5 Contrast-enhanced MRI (2026.01.19) 16 months post-operative, no significant abnormality was observed in the residual liver, with no evidence of tumor recurrence or metastasis, confirming sustained complete response after radical hepatectomy. |
Discussion
This case suggests that tumor downstaging and curative resection in GHCC complicated by high-risk AVF may be achievable through an integrated treatment strategy. While no generalizable conclusions can be drawn from a single case, the following insights are hypothesis-generating and warrant further investigation.
In this case, the pivotal insight is that conversion therapy for HCC with AVF should systematically address the AVF itself, not merely tumor volume. Current literature on advanced HCC with AVF focuses predominantly on optimizing TACE technique to avoid non-target embolism, and reporting survival outcomes of TACE combined with systemic therapies.5,13,14 By contrast, our strategy reconceptualized the AVF—from a static “contraindication” limiting therapeutic options—into a dynamic “therapeutic target” actively modulated throughout treatment.
A key innovation of our regimen is the establishment of a “HAIC-prioritized-over-TACE- and-radiotherapy” hierarchical intervention system. Facing a massive tumor burden and significant arteriovenous shunt, in this patient, we employed HAIC (FOLFOX regimen) as the first-line local intervention for two case-specific reasons: firstly, it delivered high-intensity cytotoxic assault to the main tumor mass4 (AFP decline from >12000 ng/mL to 170.14 ng/mL). Secondly, it circumvented the inherent risks of early TACE, namely ectopic embolization through the AVF, which could cause acute hepatic deterioration or pulmonary/cerebral embolism.7 Following tumor shrinkage and stabilization, TACE was sequentially administered with enhanced safety and efficiency. Radiotherapy was then added to target residual lesions and the fistula region, and to address residual tumor foci and disrupt AVF-mediated chemotherapy triage,15 addressing components difficult to eradicate with pharmacological or embolic interventions. This sequential approach was tailored to the patient’s clinical status.
In this case, HAIC and TACE induced tumor antigen release and reduced intratumoral regulatory T cells.6,8 Thus, it can turn the immunosuppressive “cold tumor” into an immunogenic “hot tumor” by restoring the immune microenvironment to further improve immune response.15–17 Radiotherapy may have further enhanced immunogenicity by promoting antigen release,18,19 upregulating MHC class,20,21 and facilitating the infiltration of tumor-infiltrating lymphocytes (TILs).19,22,23 This shifts the tumor immune phenotype from “cold” to “hot”.21,23
The combination of donafenib and tislelizumab was selected based on complementary mechanisms: donafenib may normalize aberrant tumor vasculature and reduce AVF-mediated shunting, while tislelizumab reactivates depleted CD8+ T cells.9,14,16,24 This synergistic interaction aligns with the findings from the IMbrave150 trial,13 but remains preliminary in the context of AVF.
To our knowledge, unlike recent studies on TACE-HAIC with targeted-immunotherapy in advanced HCC, none specifically enrolled the “giant tumor with AVF” subtype, emphasized the chronological sequence of interventions, or incorporated radiotherapy.5 In contrast, while multiple prior studies7,25–28 have established the efficacy of TACE combined with targeted-immunotherapy. Thus, this case provides a hypothesis-generating framework for a complete clinical decision-making pathway from multimodal conversion therapy to curative resection in this ultra-high-risk population.
In this patient, surgery was performed when three criteria were met: ①significant tumor downstaging;29,30 ② deep biological response (marked AFP decline); and ③ significant future liver remnant volume. Radical hepatectomy was performed when these multidimensional parameters were simultaneously met. Postoperative pathology confirmed R0 resection with no vascular invasion. Adjuvant targeted-immunotherapy was continued postoperatively, and as of the latest follow-up in January 2026, the patient remains in a recurrence-free survival state.This outcome illustrates the potential value of dynamic, parameter-driven decision-making in multimodal conversion therapy, though this remains to be validated in larger studies.
Naturally, as a single-center case report, this study carries inherent selection bias. Conclusions require validation in prospective cohorts. Longer follow-up is needed given to the high recurrence risk of AVF-related HCC. Additional limitations include: (1) potential influence of patient-specific factors—such as underlying liver function reserve, immune status, and tumor biology—in determining the favorable outcome; and (2) the optimal sequencing and dosing of each therapeutic modality remain undefined and require prospective investigation.
Data Sharing Statement
Due to ethical concerns and to protect patient confidentiality, the data are not publicly available. Access can be granted upon reasonable request and approval by the corresponding author.
Ethics Statement
The publication of this case report has been approved under an ethics waiver granted by the Ethics Committee of The First Affiliated Hospital of Guangxi University of Science and Technology. This waiver applies as the study is a retrospective analysis of anonymized clinical data. The patient has signed a written informed consent form regarding treatment and publication, and has agreed in the form to the release of case details and any related images.
Acknowledgments
Hengcheng Zhong and Lanju Tan are co-first authors for this study. We acknowledged the patient that agreed us to publish the case. We also extend our sincere gratitude to Dr. Xinkang Chen for his significant contribution to the measurement of the patient’s future liver remnant and radiological interpretation.
Author Contributions
Hengcheng Zhong (first author) was responsible for patient care, treatment coordination, and manuscript drafting. Lanju Tan (co-first author) acquired clinical data and co-drafted the initial manuscript. Wenjun Le performed the HAIC and TACE procedures. Ning Luo conducted longitudinal data follow-up. Yongqi Shen critically revised the manuscript for intellectual content. Guangyu Long acquired and interpreted all imaging studies. Chun Xiong performed radiotherapy (EBRT). Haiyun Tao (corresponding author) had overall responsibility for conception, design, supervision, and final approval. All authors meet ICMJE authorship criteria and have approved the final manuscript. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors disclose the receipt of the following financial support for the research, authorship, and/or publication of this article: The author(s) declare that financial support was received for the search and publication of this article. This work was supported by Clinical Study on the Efficacy and Psychological Impact of Autologous Platelet-Rich Plasma Gel Treatment for Grade III-IV Acute Radiation Dermatitis in Malignant Tumor Patients (Contract No.: S2024123); An Exploratory Study on Low-Dose Fractionated Radiotherapy Enhancing the Efficacy of Radiotherapy Immunotherapy Combination Therapy for Advanced Malignant Tumors (Contract No.: Z20230962); Integrating Social Work to Innovate Ideological and Political Education for Medical Students—Taking Hematological Diseases Teaching as an Example (Contract No.: 2024KCS Z10).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Li YY, Duan YY, Yan GZ, et al. Application of ultrasonography in the diagnosis and treatment tracing of hepatocellular carcinoma-associated arteriovenous fistulas. Liver Int. 2007;27(6):869–7. doi:10.1111/j.1478-3231.2007.01520.x
2. Forner A, Llovet JM, Bruix J. Hepatocellular carcinoma. Lancet. 2012;379(9822):1245–1255. doi:10.1016/s0140-6736(11)61347-0
3. Zhou J, Sun H, Wang Z, et al. Guidelines for the diagnosis and treatment of hepatocellular carcinoma (2019 Edition). Liver Cancer. 2020;9(6):682–720. doi:10.1159/000509424
4. Huang M, Lin Q, Wang H, et al. Survival benefit of chemoembolization plus Iodine125 seed implantation in unresectable hepatitis B-related hepatocellular carcinoma with PVTT: a retrospective matched cohort study. Eur Radiol. 2016;26(10):3428–3436. doi:10.1007/s00330-015-4198-x
5. Liu X, Yin L, Liu B, Hou X, Li Y, Liu R. TACE-HAIC plus targeted therapy and immunotherapy for HCC with tumor thrombus and arteriovenous fistula. J Hepatocell Carcinoma. 2025;12:2951–2969. doi:10.2147/jhc.S567414
6. Reig M, Sanduzzi-Zamparelli M, Forner A, et al. BCLC strategy for prognosis prediction and treatment recommendations: the 2025 update. J Hepatol. 2025. doi:10.1016/j.jhep.2025.10.020
7. Lin Z, Chen D, Hu X, et al. Clinical efficacy of HAIC (FOLFOX) combined with lenvatinib plus PD-1 inhibitors vs. TACE combined with lenvatinib plus PD-1 inhibitors in the treatment of advanced hepatocellular carcinoma with portal vein tumor thrombus and arterioportal fistulas. Am J Cancer Res. 2023;13(11):5455–5465.
8. Cui R, Yu X, Jiang Y, Li X. Efficacy and safety of the immune checkpoint inhibitor-radiotherapy combination in advanced/unresectable hepatocellular carcinoma: a systematic review and meta-analysis. Oncol Lett. 2025;30(4):460. doi:10.3892/ol.2025.15206
9. He M, Li Q, Zou R, et al. Sorafenib plus hepatic arterial infusion of oxaliplatin, fluorouracil, and leucovorin vs sorafenib alone for hepatocellular carcinoma with portal vein invasion: a randomized clinical trial. JAMA Oncol. 2019;5(7):953–960. doi:10.1001/jamaoncol.2019.0250
10. European Association for the Study of the Liver. EASL Clinical Practice Guidelines on the management of hepatocellular carcinoma. J Hepatol. 2025;82(2):315–374. doi:10.1016/j.jhep.2024.08.028
11. Sun HC, Zhou J, Wang Z, et al. Chinese expert consensus on conversion therapy for hepatocellular carcinoma (2021 edition). Hepatobiliary Surg Nutr. 2022;11(2):227–252. doi:10.21037/hbsn-21-328
12. Cai Z, Ran M, Song J, Zhen W, Li M. Imaging diagnosis and interventional treatment for hepatocellular carcinoma combined with arteriovenous fistula. J Healthc Eng. 2021;2021:6651236. doi:10.1155/2021/6651236
13. Finn RS, Qin S, Ikeda M, et al. Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. New Engl J Med. 2020;382(20):1894–1905. doi:10.1056/NEJMoa1915745
14. Finn RS, Ryoo BY, Merle P, et al. Pembrolizumab as second-line therapy in patients with advanced hepatocellular carcinoma in KEYNOTE-240: a randomized, double-blind, Phase III trial. J Clin Oncol. 2020;38(3):193–202. doi:10.1200/jco.19.01307
15. Miyayama S, Matsui O, Zen Y, et al. Portal blood supply to locally progressed hepatocellular carcinoma after transcatheter arterial chemoembolization: observation on CT during arterial portography. Hepatol Res. 2011;41(9):853–866. doi:10.1111/j.1872-034X.2011.00836.x
16. Li C, Wang MD, Lu L, et al. Preoperative transcatheter arterial chemoembolization for surgical resection of huge hepatocellular carcinoma (≥ 10 cm): a multicenter propensity matching analysis. Hepatol Internat. 2019;13(6):736–747. doi:10.1007/s12072-019-09981-0
17. Kudo M. Recent advances in systemic therapy for hepatocellular carcinoma in an Aging Society: 2020 update. Liver Cancer. 2020;9(6):640–662. doi:10.1159/000511001
18. Arnold KM, Flynn NJ, Raben A, et al. The impact of radiation on the tumor microenvironment: effect of dose and fractionation schedules. Cancer Growth Metastasis. 2018;11:1179064418761639. doi:10.1177/1179064418761639
19. Chami P, Diab Y, Khalil DN, et al. Radiation and immune checkpoint inhibitors: combination therapy for treatment of hepatocellular carcinoma. Int J Mol Sci. 2023;24(23):16773. doi:10.3390/ijms242316773
20. Trommer M, Rühle A, Lamrani A, et al. Radiotherapy-induced abscopal effects in immune checkpoint inhibitor-refractory metastatic disease: results from a large multicenter real-world cohort study. Oncoimmunology. 2026;15(1):2610529. doi:10.1080/2162402x.2025.2610529
21. Liu Y, Dong Y, Kong L, Shi F, Zhu H, Yu J. Abscopal effect of radiotherapy combined with immune checkpoint inhibitors. J Hematol Oncol. 2018;11(1):104. doi:10.1186/s13045-018-0647-8
22. Chen L, Zhang R, Lin Z, Tan Q, Huang Z, Liang B. Radiation therapy in the era of immune treatment for hepatocellular carcinoma. Front Immunol. 2023;14:1100079. doi:10.3389/fimmu.2023.1100079
23. Ning C, Zhang X, Wang Y, et al. Radiation therapy with combination therapy of immune checkpoint inhibitors and antiangiogenic therapy for hepatocellular carcinoma. Int J Radiat Oncol Biol Phys. 2024;118(5):1461–1471. doi:10.1016/j.ijrobp.2023.07.001
24. Qin S, Bi F, Gu S, et al. Donafenib versus sorafenib in first-line treatment of unresectable or metastatic hepatocellular carcinoma: a randomized, open-label, parallel-controlled phase II-III trial. J Clin Oncol. 2021;39(27):3002–3011. doi:10.1200/jco.21.00163
25. Li H, Wang J, Zhang G, et al. Transarterial chemoembolization combined donafenib with/without PD-1 for unresectable HCC in a multicenter retrospective study. Front Immunol. 2023;14:1277329. doi:10.3389/fimmu.2023.1277329
26. Zhang X, Cai H, Peng W, et al. Lenvatinib plus transarterial chemoembolization and PD-1 inhibitors as conversion therapies for unresectable intermediate-advanced hepatocellular carcinoma: a Phase 2 trial and exploratory biomolecular study. Signal Transduct Target Ther. 2026;11(1):37. doi:10.1038/s41392-025-02498-z
27. Liu X, Wang Z, Lv X, et al. Immune effect of Traditional Chinese Medicine combined with transcatheter arterial chemoembolization in treatment of liver cancer: a meta-analysis. BMC Cancer. 2026. doi:10.1186/s12885-026-15562-w
28. Huang Z, Zhu T, Chen X, et al. Postoperative adjuvant TACE combined with lenvatinib and immune checkpoint inhibitors for hepatocellular carcinoma with high recurrence risks: a multicenter retrospective study. BMC Cancer. 2026. doi:10.1186/s12885-026-15586-2
29. Tabrizian P, Jibara G, Shrager B, Schwartz M, Roayaie S. Recurrence of hepatocellular cancer after resection: patterns, treatments, and prognosis. Ann Surg. 2015;261(5):947–955. doi:10.1097/sla.0000000000000710
30. Iancu I, Bartoş A, Cioltean C, et al. Up to Date and perspectives for hepatocellular carcinoma’s intraoperative ultrasound. Chirurgia. 2021;116(4):399–408. doi:10.21614/chirurgia.116.4.399
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Therapeutic Approaches to Penile Cancer: Standards of Care and Recent Developments
White J, Mason R, Lawen T, Spooner J, Faria KVM, Rahman F, Ramasamy R
Research and Reports in Urology 2023, 15:165-174
Published Date: 2 June 2023
Extensive-Stage Small-Cell Lung Cancer: Current Landscape and Future Prospects
Saida Y, Watanabe S, Kikuchi T
OncoTargets and Therapy 2023, 16:657-671
Published Date: 2 August 2023
Breast Cancer: An Overview of Current Therapeutic Strategies, Challenge, and Perspectives
Wang J, Wu SG
Breast Cancer: Targets and Therapy 2023, 15:721-730
Published Date: 20 October 2023
Sintilimab Plus Lenvatinib with or Without Radiotherapy for Advanced Hepatocellular Carcinoma with Pulmonary Metastasis
Liu C, Jiang W, Sun J, Cui J, He D, Cheng S, Shi J
Journal of Hepatocellular Carcinoma 2024, 11:2283-2292
Published Date: 19 November 2024
Diagnosis, Prognosis, and Treatment of Triple-Negative Breast Cancer: A Review
Jie H, Ma W, Huang C
Breast Cancer: Targets and Therapy 2025, 17:265-274
Published Date: 17 March 2025