Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Multifactorial Determinants of Refractory Breathlessness in COPD: Development of the Refractory Breathlessness Score for Risk Stratification
Authors Lee HW ![]() , Lee HJ, Park H, Heo EY, Lee CH
, Lee HJ, Park H, Heo EY, Lee CH ![]() , Kim DK
, Kim DK ![]() , Lee JK
, Lee JK ![]()
Received 3 February 2026
Accepted for publication 27 June 2026
Published 8 July 2026 Volume 2026:21 601086
DOI https://doi.org/10.2147/COPD.S601086
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Zijing Zhou
Hyun-Woo Lee1, Hyo Jin Lee1, Heemoon Park1, Eun Young Heo1, Chang-Hoon Lee2, Deog Kyeom Kim1, Jung-Kyu Lee1
1Division of Respiratory and Critical Care, Department of Internal Medicine, Seoul Metropolitan Government-Seoul National University Boramae Medical Center, Seoul National University College of Medicine, Seoul, South Korea; 2Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, South Korea
Correspondence: Jung-Kyu Lee, Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Seoul National University College of Medicine, Seoul Metropolitan Government-Seoul National University Boramae Medical Center 20, Boramae-ro 5-gil, Dongjak-gu, Seoul, 07061, Republic of Korea, Tel +82-2-870-2235, Email [email protected]
Purpose: Despite optimized dual-bronchodilator therapy, many chronic obstructive pulmonary disease (COPD) patients continue to experience refractory breathlessness. This study aimed to identify the factors contributing to refractory breathlessness in patients with COPD, and to construct a clinically useful risk stratification tool, the Refractory Breathlessness Score (RB-Score).
Patients and methods: In this retrospective cohort study conducted at a single teaching hospital between January 2014 and December 2023, patients with COPD who maintained the same type of dual-bronchodilator therapy, with or without inhaled corticosteroids, for one year were included. Refractory breathlessness was defined as the absence of at least a 1-point improvement in the mMRC dyspnea score at 12 months following treatment initiation. Independent predictors for refractory breathlessness were identified, and weighted points were assigned based on adjusted odds ratios (aORs) to develop the RB-Score.
Results: Among 405 eligible patients, 244 (60.2%) had refractory breathlessness. Significant contributors included exacerbation events during treatment, comorbidities (severe anemia, cardiovascular disease, depression/anxiety, pulmonary hypertension), structural abnormalities (giant bulla, endobronchial stenosis), and inhaler-related factors (poor adherence, improper technique, multiple device use). In adjusted restricted cubic spline curve, RB-Score <1.92 was associated with a decreased risk of refractory breathlessness (aOR=0.77, 95% CI=0.59–1.00), while RB-Score >3.51 indicated increased risk (aOR=1.53, 95% CI=1.00–2.35). The RB-Score achieved good predictive performance (AUROC=0.854 [95% CI=0.818–0.891], AUPRC=0.899 [95% CI=0.865–0.928]).
Conclusion: Refractory breathlessness in COPD results from multiple factors, including pulmonary, comorbid, and inhaler-related issues. The RB-Score may facilitate risk stratification and guide individualized interventions though external validation is required.
Plain Language Summary Refractory breathlessness in COPD remains prevalent even with guideline-redual-bronchodilatorchodilator therapy, yet no established clinical marker reliably predicts its persistence. Prior research has examined individual factors but lacked an integrative approach to risk stratify refractory breathlessness in real-world populations.
This study identifies a comprehensive set of clinical, structural, and inhaler-related factors independently associated with refractory breathlessness in COPD. A novel composite index, the Refractory Breathlessness Score (RB-Score), was developed and validated, demonstrating excellent discriminative performance. The RB-Score enables stratification of patients into risk categories and outperforms individual predictors in identifying those at risk of refractory symptoms.
The RB-Score may inform individualized COPD management and support future strategies for targeted interventions to reduce symptom burden in patients with refractory breathlessness.
Keywords: pulmonary disease, chronic obstructive, dyspnea, inhalation administration, risk assessment, comorbidity
Introduction
Chronic obstructive pulmonary disease (COPD) is a major global health burden and the third leading cause of death worldwide. In 2022, COPD accounted for approximately 3.2 million deaths globally, and by 2050, COPD-related mortality is projected to increase by 102%, reaching an estimated 6.5 million deaths annually.1 The disease is characterized by irreversible airflow limitation and chronic respiratory symptoms, with breathlessness being one of the most challenging symptoms. Higher dyspnea severity, as assessed by the modified Medical Research Council (mMRC) dyspnea scale, is linked to an increased risk of hospitalization risk,2 greater mortality,3 and reduced physical activity.4 Higher mMRC scores are significantly correlated with greater breathlessness severity, increased healthcare utilization, and diminished overall quality of life.5 Moreover, refractory breathlessness is closely associated with psychological distress, with depressive symptoms present in up to 20% of patients with COPD.6
Given the notable impact of dyspnea on clinical outcomes, symptom management remains an important therapeutic goal in COPD. However, despite guideline-directed therapy, more than 50% of patients with COPD continued to experience refractory breathlessness, which is closely linked to adverse clinical outcomes.7–9 Unlike prior studies predicting breathlessness in smokers or the general population, the present study focuses on patients with COPD already receiving optimized dual-bronchodilator therapy, in whom breathlessness persists despite treatment.10,11 Exacerbation history serves as a key determinant for treatment escalation, and blood eosinophil levels guide the use of inhaled corticosteroids (ICSs) to reduce exacerbation risk. However, no comparable marker exists to identify patients at risk of refractory breathlessness despite optimized therapy, making it difficult to recognize those who may benefit from alternative interventions. A comprehensive approach that considers both disease-related and non-disease-related contributors may help enhance risk stratification, refine symptom management approaches, support individualized treatment strategies, and potentially improve patient outcomes.
We hypothesized that refractory breathlessness in COPD arises from multiple contributory factors across pulmonary, comorbid, and inhaler-related domains. This study aimed to identify these factors in patients with COPD receiving dual-bronchodilator therapy with or without ICSs, develop the Refractory Breathlessness Score as a risk stratification tool, and examine its association with all-cause mortality as a measure of overall disease burden.
Methods
Our study adhered to the guidelines outlined in the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement.12
Study Design and Participants
This retrospective cohort study was conducted at a teaching hospital, including patients with COPD who visited between January 2014 and December 2023. COPD was diagnosed by pulmonologists based on chronic respiratory symptoms, risk factors, and spirometric evidence of non-fully reversible airflow limitation, defined as a post-bronchodilator forced expiratory volume in 1 second (FEV1)/forced vital capacity (FVC) ratio <0.7.13
Patients prescribed long-acting β2-agonist/long-acting muscarinic antagonist (LABA/LAMA) or inhaled corticosteroid/LABA/LAMA (ICS/LABA/LAMA) for one year were screened if their mMRC dyspnea scores were assessed at both baseline and one year. Inclusion criteria required patients to have undergone spirometry and chest computed tomography (CT) scans at the time of LABA/LAMA or ICS/LABA/LAMA initiation, attended outpatient clinic visits at least three times over 12 months, and consistently used the same inhaler drug class and device during the observation period. Patients with a diagnosis of asthma or missing data on demographics, clinical information, or dyspnea severity assessments were excluded.
Eligible patients were classified into the refractory breathlessness group if their mMRC scores at one year was not improved compared to baseline and the improved breathlessness group if their scores decreased.14
The study protocol was approved by the Institutional Review Board of the Seoul Metropolitan Government-Seoul National University Boramae Medical Center (IRB No. 20–2024-24). Written informed consent was waived because this was a retrospective analysis of anonymized data. All procedures in this study were conducted in accordance with relevant guidelines and regulations, and with the principles of the Declaration of Helsinki.
Variables and Measurements
We collected demographic variables such as age, sex, and body mass index (BMI), as well as smoking status and pack-years. Clinical features comprised the Charlson Comorbidity Index (CCI), history of moderate-to-severe exacerbations within the prior year, and symptom burden assessed using the mMRC dyspnea score. Laboratory parameters included white blood cell (WBC) count, neutrophil percentage and count, lymphocyte percentage and count, neutrophil-to-lymphocyte ratio (NLR), eosinophil percentage and count, and the proportion of patients with eosinophil counts ≥300/µL. Pulmonary function test results included spirometric indices such as FEV1 (L, %, z-score), FVC (L, %, z-score), FEV1/FVC ratio (%, z-score), forced expiratory flow at 25% to 75% of FVC (FEF25-75) (L/s, %), and diffusing capacity for carbon monoxide (DLCO) (mL/min/mmHg, %). The z-scores were calculated using the Global Lung Function Initiative 2022 reference equations.15 All demographic, clinical, laboratory, pulmonary function, and radiological variables were collected at baseline, defined as the time of initiation of LABA/LAMA or ICS/LABA/LAMA therapy.
Quantitative CT Analysis
All patients underwent chest CT scans at full inspiration. Images were acquired using either a Philips Ingenuity or a GE Revolution CT scanner and reconstructed using a soft or standard kernel with slice thicknesses of 0.67–1.25 mm, in accordance with the institutional CT acquisition protocol. Quantitative CT analysis was performed using Aview software (Coreline Soft, Seoul, Korea). The proportion of low-attenuation areas below −950 HU on inspiratory CT (%LAA-950) was used as a measure of emphysema extent. Airway wall thickness was quantified as the square root of the wall area of a hypothetical airway with an internal perimeter of 10 mm (Pi10), derived using the bronchial anatomical detection method.
Potential Causes of Refractory Breathlessness
We conducted a structured literature review to identify potential causes of refractory breathlessness in patients with COPD. We searched electronic databases, including PubMed, Embase, and Cochrane Library, covering studies published from inception to December 31, 2023. The search strategy incorporated Medical Subject Headings (MeSH) terms and free-text keywords related to COPD, refractory breathlessness, and potential contributing factors across four domains: COPD-related factors, non-respiratory comorbidities, respiratory comorbidities, and device-related factors. Key search terms included “COPD” OR “chronic obstructive pulmonary disease”, AND “refractory dyspnea” OR “persistent dyspnea” OR “refractory breathlessness” OR “persistent breathlessness”. The search was restricted to human studies published in English, focusing on adult populations, with the exclusion of case reports and editorials. Studies that did not report on potential causes or contributors to breathlessness in patients with COPD were subsequently excluded upon title and abstract review. From the identified factors, we selected those verifiable through electronic medical records, categorizing them into COPD-related factors (current smoking, exacerbation events during treatment, occupational exposure, severe airflow limitation, severe emphysema, and severe hyperinflation), non-respiratory comorbidities (advanced deconditioning, arrhythmia, cardiovascular disease, cognitive impairment, depression or anxiety, obesity, pulmonary hypertension, and severe anemia), respiratory comorbidities (bronchiectasis, endobronchial stenosis, fungal infection, giant bulla, interstitial lung disease, lung cancer, non-tuberculous mycobacteria (NTM) pulmonary disease, pulmonary thromboembolism, TB-destroyed lung, thoracic wall abnormality, and upper airway disease), and device-related factors (low inhalability, multiple device use, poor adherence, and poor inhaler technique).
For potential causes of refractory breathlessness without established definitions, three pulmonologists reached a consensus to develop operational definitions. Occupational exposure was defined as a documented history of exposure to vapors, gases, dust, and fumes in medical records. Severe airflow limitation was defined according to the GOLD report as FEV1 <50% predicted.13 Severe emphysema was defined as a %LAA-950 exceeding 20% on inspiratory chest CT.16–18 Severe hyperinflation was determined if at least one of the following criteria was met: 1) residual volume to total lung capacity ratio (RV/TLC) >60%19 or 2) parametric response mapping of small airway disease (PRMfSAD) ≥40%.20,21 Advanced deconditioning was defined as a Clinical Frailty Scale score of 5 or higher.22 According to the World Health Organization (WHO) Asia-Pacific criteria, obesity was defined as a BMI >25 kg/m2. Severe anemia was defined as hemoglobin (Hb) <8.0 g/dL. Non-respiratory comorbidities were assessed only in patients with suggestive symptoms who underwent evaluations by cardiologists, neurologists, or psychiatrists. Respiratory comorbidities were assessed based on pulmonologists’ medical records, with further evaluations by thoracic surgeons or otolaryngologists when clinically indicated, and radiologic assessments by chest radiologists. For device-related factors, low inhalability was defined as a maximum forced inspiratory flow (FIFmax) <120 L/min, based on previous studies evaluating dry powder inhaler (DPI) use in relation to peak inspiratory flow rate (PIFR).23,24 This cutoff was chosen because previous studies indicate that only a small proportion of COPD patients using DPIs had FIFmax values below 100–120 L/min.23–25 Poor adherence was defined as a prescribed medication possession rate (MPR) <80%, while poor inhaler technique was determined based on medical record documentation.
Outcomes
The primary outcome was refractory breathlessness, defined as a mMRC dyspnea score that remained unchanged or increased by at least one point at the 12-month outpatient clinic visit following the initiation of LABA/LAMA or ICS/LABA/LAMA therapy. Although the minimal clinically important difference of the mMRC dyspnea scale has been reported as approximately 0.5 points,26,27 the mMRC is an ordinal scale measured in whole-number increments at the individual patient level, and a 1-point change therefore represents the smallest practically detectable difference in routine clinical practice. Improved breathlessness was defined as a reduction of at least one point in the mMRC score at the 12-month follow-up.
We assessed the prevalence of potential causes contributing to refractory breathlessness and identified independent associations with this outcome. Based on these identified significant factors, the Refractory Breathlessness Score (RB-Score) was developed by assigning points to each contributing variable by rounding the natural logarithm of the adjusted odds ratio to the nearest integer, producing a clinically intuitive whole-number scoring system, and summing the total points.
To evaluate the long-term prognostic value of the RB-Score, all-cause mortality data were obtained from the national death registry of Statistics Korea. Mortality status and date of death were ascertained through linkage with official death records using unique personal identification numbers. Follow-up time was calculated from the index date (initiation of LABA/LAMA or ICS/LABA/LAMA therapy) to the date of death or the end of the observation period, whichever came first.
Statistical Analysis
Comparisons between the refractory breathlessness group and the improved breathlessness group were performed using the chi-squared test or Fisher’s exact test for categorical variables and the Student’s t-test or Wilcoxon rank-sum test for continuous variables. To assess the association between potential risk factors and refractory breathlessness, univariable and multivariable logistic regression models were applied. Univariable odds ratios (ORs) with 95% confidence intervals (CIs) were estimated to identify candidate variables. A Directed Acyclic Graph (DAG) (Supplementary Figure S1) was constructed to delineate the causal relationships between refractory breathlessness and its associated factors, facilitating the identification of confounders.
To mitigate confounding bias, the multivariable model included covariates deemed clinically relevant and statistically significant in the univariable analysis. This approach ensured the retention of key confounding variables while minimizing overadjustment. The final multivariable model incorporated age, sex, BMI, smoking history, CCI, baseline mMRC dyspnea score, prior moderate-to-severe exacerbations within one year, blood neutrophil and lymphocyte counts, spirometric indices (FEV1 z-score, FEV1/FVC z-score, and DLCO % predicted), and radiologic parameters (%LAA-950 and Pi10) using an automatic segmentation software (Aview; Coreline Soft, Seoul, South Korea). To evaluate the robustness of the findings to potential unmeasured confounding, E-values were calculated for statistically significant ORs.
Restricted cubic spline models were used to explore the non-linear relationship between the RB-Score and refractory breathlessness risk. Predictive performance of the RB-Score was assessed using the area under the receiver operating characteristic curve (AUROC) and area under the precision-recall curve (AUPRC). Optimal cutoff values were determined using the Youden index. Model calibration was assessed using the Hosmer–Lemeshow goodness-of-fit test and bootstrap-based calibration plot.
The association between RB-Score and all-cause mortality was assessed using Cox proportional hazards models, adjusting for relevant baseline covariates. In addition, Kaplan–Meier survival curves were generated by stratifying patients into four risk groups based on RB-Score thresholds (≤1.5, 2.0–3.0, 3.5–5.5, ≥6.0), and survival differences were evaluated using the Log rank test. Risk stratification thresholds were derived post hoc using two complementary data-driven approaches. The boundaries between the low-, intermediate-, and high-risk groups were defined by the statistically significant inflection points identified in the restricted cubic spline analysis, rounded to the nearest integer to align with the integer-based scoring system. The threshold for the very high-risk group was set at the optimal cutoff value identified by the Youden index from the AUROC analysis. For each risk stratum, the number of patients, observed event rates, and 95% confidence intervals for the proportion of refractory breathlessness were calculated using the Wilson score method.
Statistical significance was set at P <0.05, and all analyses were conducted using R statistical software (version 4.4.2).
Results
A total of 725 patients with COPD who were prescribed LABA/LAMA or ICS/LABA/LAMA for one year were screened (Figure 1). Of these, 162 patients with concurrent asthma and 10 patients who did not undergo spirometry or chest CT scans at the initiation of LABA/LAMA or ICS/LABA/LAMA therapy were excluded, resulting in 553 patients. Among them, 72 patients who did not attend three or more regular outpatient clinic visits within one year were excluded, leaving 481 patients eligible for further analysis. Additionally, 76 patients who switched inhaler devices during the observation period were excluded, yielding a final cohort of 405 patients who consistently used the same inhaler device and drug component for one year. These patients were subsequently categorized into the refractory breathlessness group (n=244, 60.2%) and the improved breathlessness group (n=161, 39.8%).
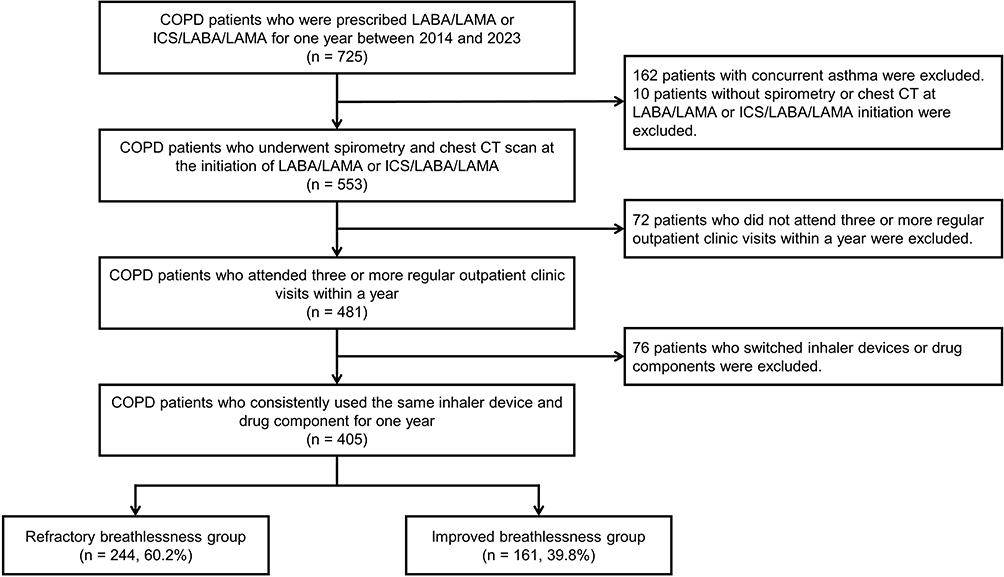 |
Figure 1 Flow diagram of inclusion. |
Baseline Characteristics
The refractory breathlessness group showed a lower BMI, greater smoking burden, higher comorbidity burden, more severe dyspnea, and a higher frequency of exacerbations (Table 1). Blood tests revealed elevated WBC counts and reduced neutrophil and lymphocyte percentages compared to the improved breathlessness group. Spirometry measurements indicated significantly lower FEV1, FEV1/FVC, and DLCO values in the refractory breathlessness group. Radiological analysis indicated a greater extent of emphysema, reflected by an increased %LAA-950 on inspiratory CT scans. In multivariable analyses, current smoking, a higher CCI, a higher mMRC, prior exacerbation history, DLCO (% of predicted value), and Pi10 were independently associated with refractory breathlessness (Supplementary Table S1).
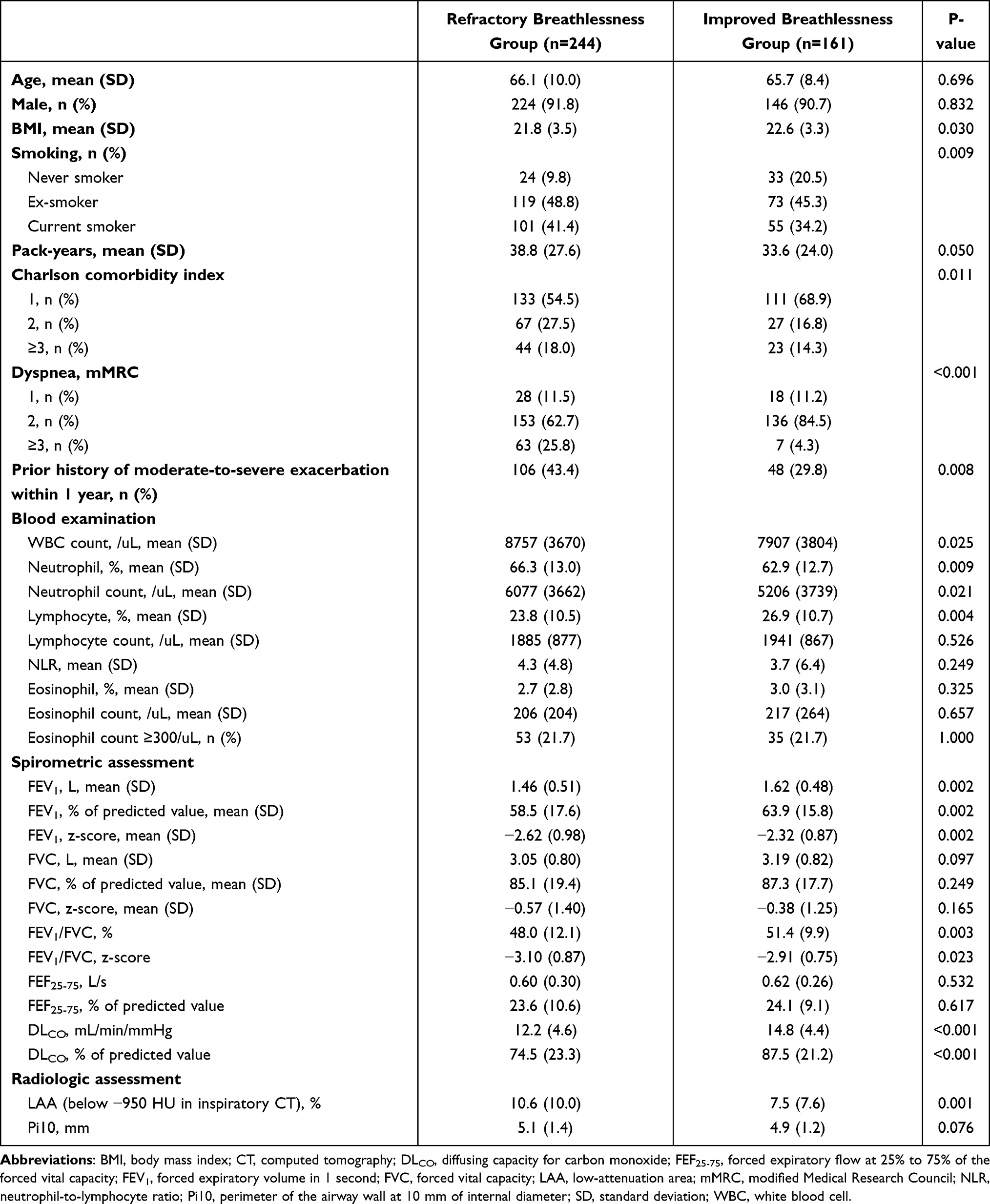 |
Table 1 Baseline Characteristics |
Potential Causes for Refractory Breathlessness
Within the refractory breathlessness group, we investigated potential causes and identified factors such as the use of multiple devices (50.0%), severe airflow limitation (48.4%), severe emphysema (48.4%), poor adherence (43.9%), and advanced deconditioning (37.7%) (Supplementary Figure S2). However, not all potential causes were significantly more prevalent in the refractory group compared to the improved group (Supplementary Table S2).
In the unadjusted analysis, exacerbation events during treatment, severe airflow limitation, severe emphysema, and current smoking demonstrated significant associations with refractory breathlessness (Supplementary Figure S3). Pulmonary hypertension, advanced deconditioning, depression or anxiety, cardiovascular disease, and arrhythmia were prominent among non-respiratory comorbidities, while giant bulla was a significant respiratory comorbidity. Device-related factors, such as poor adherence, poor technique, multiple device use, and low inhalability, showed significant associations.
After adjustment, only exacerbation events during treatment retained an independent association with refractory breathlessness (aOR=5.673 [95% CI=2.722–11.822], P-value <0.001) among COPD-related factors (Figure 2). Among non-respiratory comorbidities, severe anemia (aOR=4.760 [95% CI=1.001–22.664], P-value=0.049), cardiovascular disease (aOR=2.920 [95% CI=1.561–5.461], P-value<0.001), depression or anxiety (aOR=2.845 [95% CI=1.142–7.089], P-value=0.025), advanced deconditioning (aOR=2.694 [95% CI=1.554–4.669], P-value <0.001), and pulmonary hypertension (aOR=2.622 [95% CI=1.007–6.830], P-value=0.048) remained significant. Respiratory comorbidities, including giant bulla (aOR=11.775 [95% CI=1.502–92.278], P-value=0.019) and endobronchial stenosis (aOR=7.982 [95% CI=1.454–43.801], P-value=0.017), also showed significant associations. Device-related factors such as poor adherence (aOR=4.945 [95% CI: 2.830–8.641], P-value <0.001), poor technique (aOR=3.042 [95% CI: 1.774–5.217], P-value <0.001), multiple device use (aOR=2.217 [95% CI: 1.378–3.567], P-value=0.001), and low inhalability (aOR=1.852 [95% CI: 1.043–3.290], P-value=0.035) remained significantly associated with refractory breathlessness.
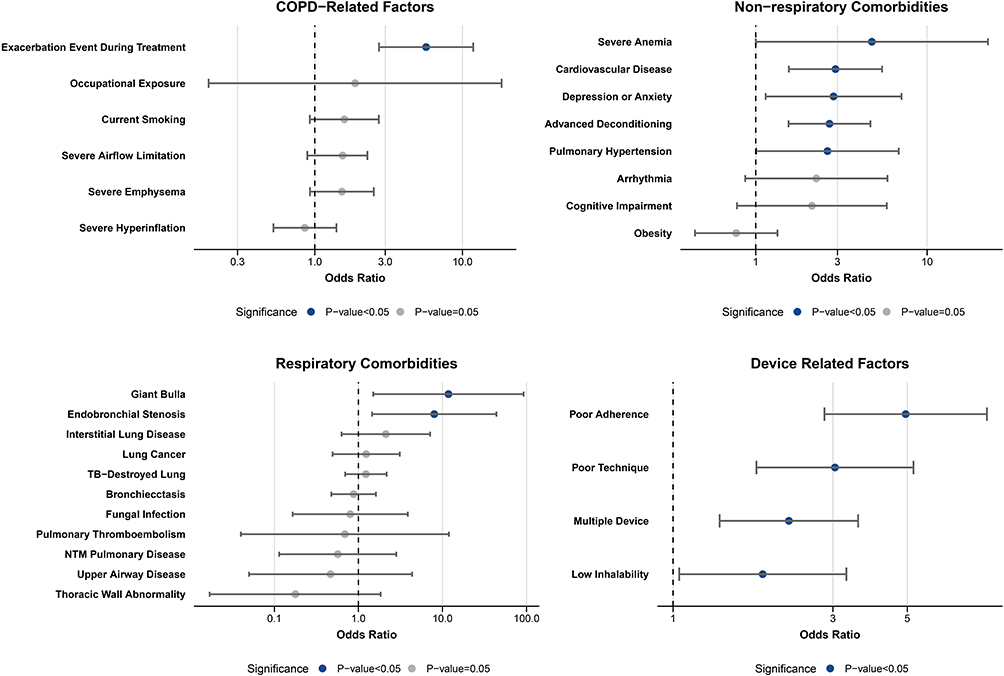 |
Figure 2 Adjusted odds ratios of potential contributors to refractory breathlessness. The multivariable logistic regression model includes covariables such as age, sex, BMI, smoking history, CCI, mMRC dyspnea score, prior history of moderate-to-severe exacerbations within one year, blood neutrophil count, blood lymphocyte count, FEV1 (z-score), FEV1/FVC (z-score), DLCO (% predicted), LAA (%), and Pi10 (mm). |
Refractory Breathlessness Score
A scoring system for refractory breathlessness was developed based on potential causes identified through multivariable logistic regression analyses (Table 2). Points were assigned to each potential cause according to the natural logarithm of their aORs. The robustness of these associations with refractory breathlessness was further supported by sensitivity analyses addressing the potential impact of unmeasured confounding, as demonstrated by the E-values (Supplementary Table S3). The total of these points, which is RB-Score, ranges from 0 to 16, with higher scores reflecting a greater overall association with refractory breathlessness.
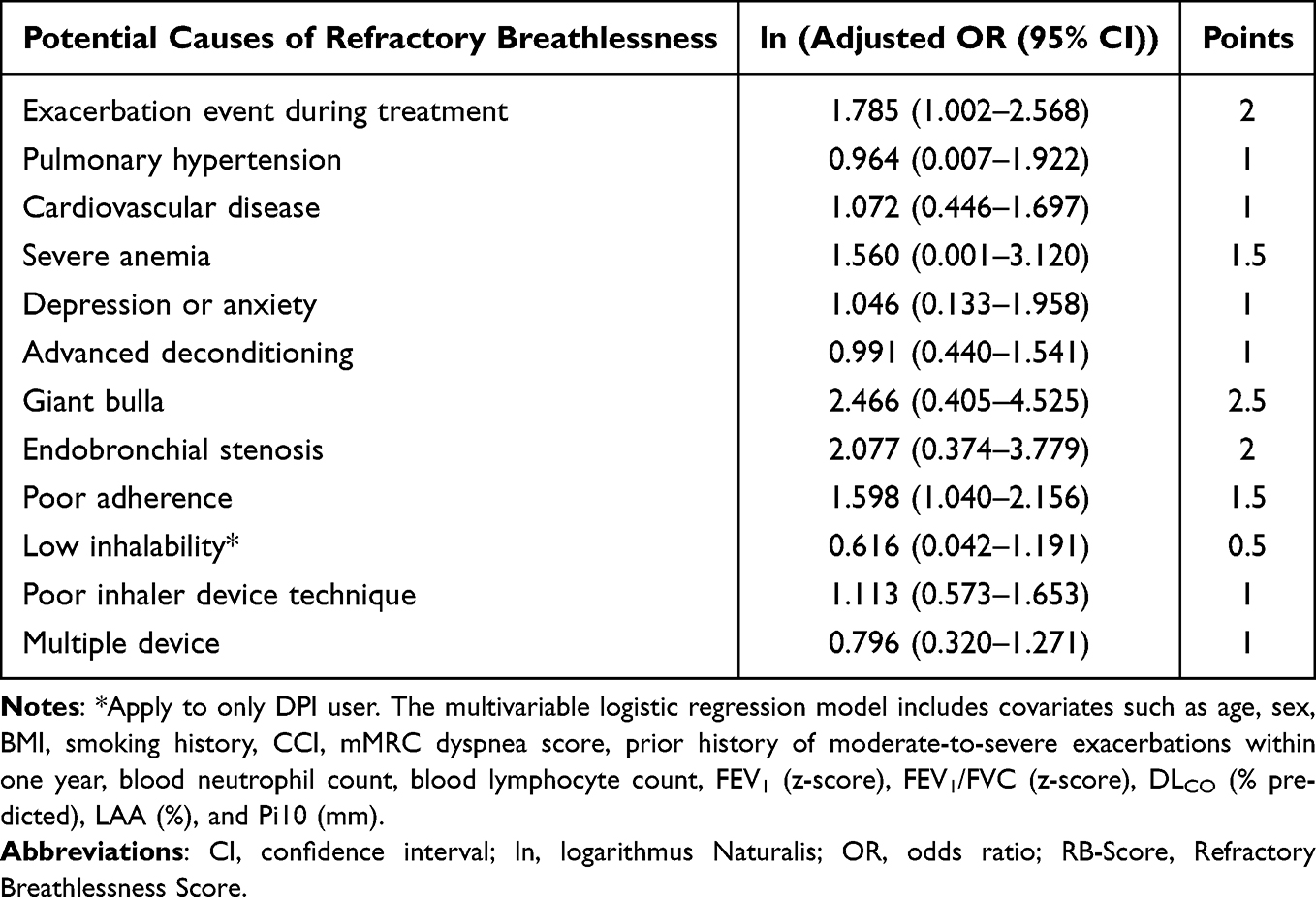 |
Table 2 Estimation of Refractory Breathlessness Score |
The RB-Score in the improved breathlessness group had a median of 1.0 (IQR=0–2.0), whereas the refractory breathlessness group had a median of 3.5 (IQR=2.5–5.0) (Supplementary Figure S4). Patients with higher RB-Scores exhibited a progressively greater proportion of refractory breathlessness (Supplementary Figure S5). In the adjusted restricted cubic spline curve, the aOR for refractory breathlessness became statistically significant at an RB-Score of 1.92 (aOR=0.77 [95% CI=0.59–1.00]) and at an RB-Score of 3.51 (aOR=1.53 [95% CI=1.00–2.35]) (Figure 3).
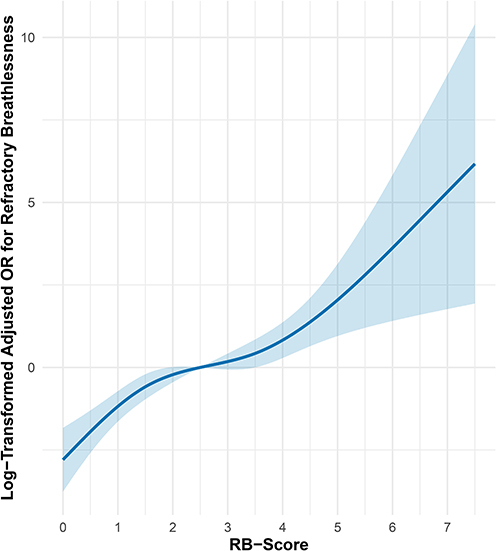 |
Figure 3 Adjusted restricted cubic spline curve of the RB-score for refractory breathlessness. |
Risk stratification based on the RB-Score identified distinct risk groups for refractory breathlessness, with a 26% likelihood in the low-risk group (RB-Score ≤1.5), 66% in the intermediate-risk group (RB-Score 2.0–3.0), 85% in the high-risk group (RB-Score 3.5–5.5), and 100% in the very high-risk group (RB-Score ≥6.0) (Supplementary Table S4).
The RB-Score achieved an AUROC of 0.854 (95% CI=0.818–0.891, P-value <0.001) with an optimal cutoff value of 6.0 for identifying refractory breathlessness (Figure 4). The AUPRC was 0.899 (95% CI=0.865–0.928), indicating consistent performance in predicting refractory breathlessness across different prevalence thresholds. The RB-Score showed the highest predictive performance for refractory breathlessness, compared to individual potential causes (Supplementary Table S5). Model calibration was assessed using the Hosmer–Lemeshow goodness-of-fit test, which showed no significant lack of fit (P-value=0.283) and was further supported by a bootstrap-based calibration plot demonstrating close agreement between predicted and observed probabilities (Supplementary Figure S6).
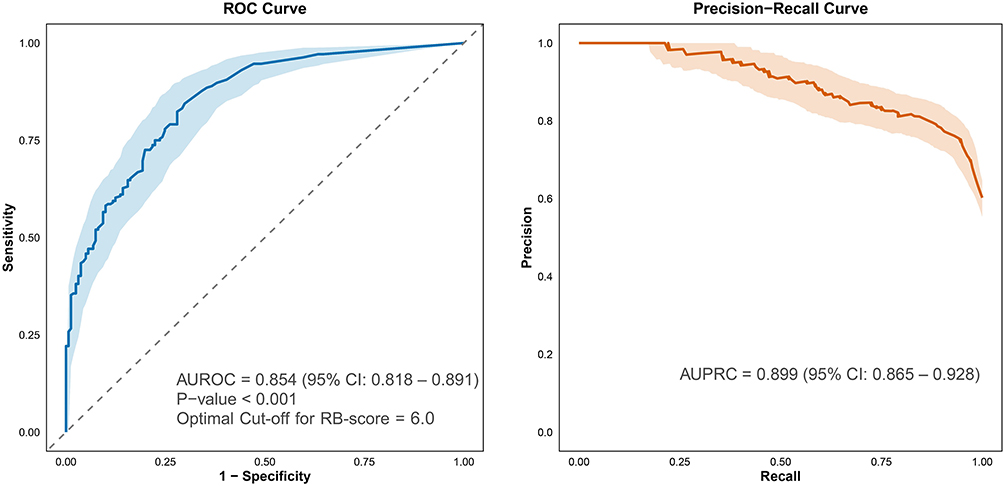 |
Figure 4 Predictive performance of the RB-Score for identifying refractory breathlessness. Abbreviations: AUPRC, Area Under the Precision–Recall Curve, AUROC, Area Under the Receiver Operating Characteristic Curve. |
The RB-Score was significantly associated with time to all-cause mortality in the unadjusted analysis (Hazard ratio [HR]=1.171 [95% CI=1.080–1.270], P-value <0.001), and Kaplan–Meier curves showed significantly lower mortality in the group with RB-Score <1.5 (P-value <0.001, Supplementary Figure S7). Even after adjustment for covariates including age, sex, BMI, smoking status, comorbidities, prior exacerbation history, and FEV1/FVC z-score, this association was significant (adjusted HR=1.111 [95% CI=1.014–1.218], P-value=0.024).
Discussion
This study evaluated the prevalence and contributors to refractory breathlessness in patients with COPD receiving dual-bronchodilator therapy with or without ICSs, emphasizing the multifactorial nature of refractory breathlessness despite standard treatment. A substantial proportion of patients continued to experience breathlessness, suggesting that factors beyond airflow limitation contribute to symptom persistence. Exacerbation events during treatment were a major contributor, reinforcing the notion that recurrent exacerbations can perpetuate symptom burden beyond their immediate impacts. Additionally, non-respiratory comorbidities, structural lung abnormalities, and inhaler-related issues were associated with refractory breathlessness, suggesting the need for a broader clinical assessment that extends beyond conventional parameters. Incorporating evaluations of cardiovascular and musculoskeletal comorbidities, inhaler technique and adherence, and imaging-based structural abnormalities may improve risk stratification and inform more tailored symptom management strategies. The RB-Score may also support broader clinical decision-making, given its observed association with long-term all-cause mortality.
While airflow limitation remains a defining characteristic of COPD, the persistence of dyspnea despite optimized bronchodilator therapy suggests the involvement of additional pathophysiological mechanisms. In the present cohort, 60.2% of patients experienced refractory breathlessness at 12 months, consistent with prior estimates of 50–70% reported in outpatient COPD populations receiving guideline-directed therapy.7,8 Exacerbation events during treatment may sustain airway inflammation,28 impair ventilatory efficiency29 and heighten the respiratory neural drive, amplifying dyspnea perception through altered respiratory mechanics.30,31 Also, patients with frequent exacerbations exhibit distinctly altered dyspnea perception compared to infrequent exacerbators, supporting the independent contribution of exacerbation burden during treatment observed in the present study.30 The proposed role of neuroinflammatory processes in modulating central dyspnea perception should be considered hypothesis-generating rather than an evidence-based conclusion within the scope of the present study.32
Beyond pulmonary factors, non-respiratory comorbidities such as cardiovascular disease and advanced deconditioning may further contribute through impaired oxygen delivery, autonomic dysfunction, and skeletal muscle weakness, leading to exertional intolerance.33,34 The independent contribution of depression and anxiety aligns with evidence that depressive symptoms exert an impact on COPD outcomes comparable to that of FEV1 impairment,6 underscoring the importance of routine psychological assessment in patients with refractory breathlessness. Structural abnormalities, including airway remodeling, emphysematous destruction,35 and central airway narrowing, may exacerbate dyspnea by increasing dynamic hyperinflation,36,37 altering ventilatory mechanics, and elevating the work of breathing.38 To our knowledge, the independent contributions of giant bulla and endobronchial stenosis as discrete structural predictors of refractory breathlessness have not been previously quantified in a multivariable framework. Furthermore, suboptimal inhaler use or insufficient inspiratory flow may lead to inadequate drug deposition, limiting bronchodilator effectiveness and reducing the potential for exacerbation prevention.25,39 The independent contributions of multiple device use and low inhalability as distinct predictors of symptom persistence have similarly not been previously reported in an integrated multivariable analysis. These findings suggest that refractory breathlessness can be influenced by multiple factors, indicating the potential value of a broader assessment approach to better characterize its contributors. Although the RB-Score was originally developed to assess refractory breathlessness, its association with long-term all-cause mortality suggests potential surrogate marker of overall disease burden in COPD.
Given this complexity, a systematic approach to risk stratification is necessary to guide individualized management. The RB-Score developed in this study provides a structured framework for identifying patients at risk of refractory breathlessness despite optimized therapy by incorporating multiple contributing factors beyond airflow limitation. By integrating exacerbation history, comorbid conditions, structural lung abnormalities, and inhaler-related factors, the RB-Score offers a comprehensive method for evaluating the mechanisms underlying dyspnea persistence. In practice, the score can be calculated using information routinely available at outpatient visits without requiring additional specialized investigations. Patients in the low-risk group (RB-Score ≤1.5) may be managed with standard therapy optimization, whereas those in the intermediate- or high-risk groups (RB-Score ≥2.0) may benefit from a structured review of contributing factors, including comorbidity management, inhaler technique reassessment, and consideration of pulmonary rehabilitation. This approach may allow for the early identification of patients who are unlikely to respond to standard therapy and who may benefit from targeted interventions, such as pulmonary rehabilitation for deconditioning, cardiovascular management for coexisting disease, or inhaler technique optimization to enhance drug delivery.
Beyond its role in individualizing treatment, the RB-Score may complement existing COPD risk stratification models, which primarily focus on exacerbation risk, by addressing the distinct challenge of refractory breathlessness. While exacerbation prevention remains a key therapeutic goal, a more refined approach to systematically assessing and identifying patients at risk for refractory breathlessness may help guide targeted interventions aimed at optimizing symptom management. Future studies are required to validate its predictive performance across diverse clinical settings and to assess its potential utility in refining treatment algorithms for patients with COPD who continue to experience refractory breathlessness despite optimized therapy.
This study has several strengths. The RB-Score was developed through a comprehensive and structured assessment of contributing factors spanning four clinical domains, informed by a structured literature search. The use of a real-world cohort with detailed clinical, radiological, and inhaler-related data allowed for a multifactorial evaluation that reflects routine clinical practice. Furthermore, the integer-based scoring system was designed to maximize clinical applicability without requiring specialized investigations beyond those available at standard outpatient visits.
This study has several limitations. First, although the RB-Score showed good predictive performance in the current cohort, its generalizability remains uncertain. The score was derived and evaluated in the same single-center retrospective dataset, and formal internal validation procedures such as bootstrapping or cross-validation were not performed. Accordingly, the reported predictive performance metrics may overestimate the true discriminative ability of the score, and the risk stratification thresholds were determined post hoc rather than prespecified, raising additional concerns regarding overfitting. Second, while this study identified multiple contributors to refractory breathlessness, it remains unclear whether modifying these factors leads to meaningful improvements in clinical outcomes. The retrospective nature of the study precludes direct assessment of causality, and interventional studies are needed to determine whether targeted management strategies such as optimizing inhaler technique, addressing cardiovascular comorbidities, or implementing pulmonary rehabilitation can reduce refractory breathlessness. Third, this study did not incorporate real-time symptom tracking tools such as digital health monitoring, which may offer additional insights into the day-to-day variability of breathlessness and treatment adherence. Integrating wearable sensors, mobile applications for symptom reporting, and adherence-monitoring devices could refine risk stratification and support individualized treatment adjustments. Fourth, this study lacked long-term follow-up beyond the 12-month observation period. Therefore, it is limited to determine whether refractory breathlessness is truly refractory or if some patients experience delayed improvement beyond one year. Fifth, the exclusion of patients who frequently switched inhaler devices during the observation period may have introduced selection bias. While this criterion ensured a standardized assessment of inhaler-related factors, it potentially excluded a subset of patients with unstable disease, poor treatment adherence, or difficulties in inhaler use. Sixth, the very high-risk group comprised a relatively small number of patients, and the observed 100% event rate should therefore be interpreted with caution, as this finding likely reflects sparse data rather than a true ceiling effect.
Conclusions
In patients with COPD receiving optimized dual-bronchodilator therapy, refractory breathlessness arises from multiple independent contributors spanning exacerbation burden, non-respiratory comorbidities, structural lung abnormalities, and inhaler-related factors. The RB-Score, incorporating these contributors, showed good discriminative performance and enabled meaningful risk stratification, with an independent association with all-cause mortality suggesting broader prognostic relevance. External validation and interventional studies are needed to confirm its generalizability and clinical utility.
Artificial Intelligence Involvement
ChatGPT 5.1 was used to assist with English grammar refinement and clarity during manuscript preparation.
Abbreviations
AUPRC, area under the precision–recall curve; AUROC, area under the receiver-operating characteristic curve; BMI, body mass index; CCI, Charlson comorbidity index; CI, confidence interval; COPD, chronic obstructive pulmonary disease; CT, computed tomography; DAG, directed acyclic graph; DLCO, diffusing capacity for carbon monoxide; DPI, dry powder inhaler; FEF50, forced expiratory flow at 50% of forced vital capacity; FEF25₋75, forced expiratory flow at 25–75% of forced vital capacity; FEV1, forced expiratory volume in 1 second; FEV1/FVC, forced expiratory volume in 1 second to forced vital capacity ratio; FIFmₐₓ, maximum forced inspiratory flow; FVC, forced vital capacity; GOLD, Global Initiative for Chronic Obstructive Lung Disease; Hb, hemoglobin; ICS, inhaled corticosteroid; LABA, long-acting β2-agonist; LABA/LAMA, long-acting β2-agonist/long-acting muscarinic antagonist; LAA₋950, low-attenuation area below −950 Hounsfield units; LAMA, long-acting muscarinic antagonist; MPR, medication possession ratio; mMRC, modified Medical Research Council; NLR, neutrophil-to-lymphocyte ratio; NTM, non-tuberculous mycobacteria; OR, odds ratio; PIFR, peak inspiratory flow rate; Pi10, square root of the wall area of a theoretical airway with an internal perimeter of 10 mm; PRMfˢAD, parametric response mapping of small airway disease; RB-Score, refractory breathlessness score; RV/TLC, residual volume to total lung capacity ratio; STROBE, Strengthening the Reporting of Observational Studies in Epidemiology; TB, tuberculosis; WBC, white blood cell; WHO, World Health Organization.
Data Sharing Statement
The datasets analyzed during the present study contain protected health information. Public sharing is not permitted due to institutional and regulatory requirements for patient privacy. Deidentified data may be made available upon reasonable request to the corresponding author after approval by the Institutional Review Board and execution of a data use agreement.
Ethics Approval and Consent to Participate
The study protocol was approved by the Institutional Review Board of the Seoul Metropolitan Government-Seoul National University Boramae Medical Center (IRB No. 20-2024-24). Written informed consent was waived because this was a retrospective analysis of anonymized data. All procedures in this study were conducted in accordance with relevant guidelines and regulations, and with the principles of the Declaration of Helsinki.
Acknowledgments
The interim findings of this paper were presented in part at the 29th Congress of the Asian Pacific Society of Respirology on November 2025.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare no support from any organization for the submitted work; no financial relationship with any organization that might have an interest in the submitted work, and no other relationships or activities that may have influenced the submitted work.
References
1. GBD. Forecasting collaborators. Burden of disease scenarios for 204 countries and territories, 2022-2050: a forecasting analysis for the Global Burden of Disease Study 2021. Lancet. 2024;403(10440):2204–14. doi:10.1016/S0140-6736(24)00685-8
2. Hurst JR, Vestbo J, Anzueto A, et al. Susceptibility to exacerbation in chronic obstructive pulmonary disease. N Engl J Med. 2010;363(12):1128–1138. doi:10.1056/NEJMoa0909883
3. Casanova C, Marin JM, Martinez-Gonzalez C, et al. Differential effect of modified medical research council dyspnea, COPD assessment test, and clinical COPD questionnaire for symptoms evaluation within the new GOLD staging and mortality in COPD. Chest. 2015;148(1):159–168. doi:10.1378/chest.14-2449
4. Hayata A, Minakata Y, Matsunaga K, Nakanishi M, Yamamoto N. Differences in physical activity according to mMRC grade in patients with COPD. Int J Chron Obstruct Pulmon Dis. 2016;11:2203–2208. doi:10.2147/COPD.S109694
5. Ding B, Small M, Bergström G, Holmgren U. COPD symptom burden: impact on health care resource utilization, and work and activity impairment. Int J Chron Obstruct Pulmon Dis. 2017;12:677–689. doi:10.2147/COPD.S123896
6. O’Toole J, Woo H, Putcha N, et al. Comparative impact of depressive symptoms and FEV(1)% on chronic obstructive pulmonary disease. Ann Am Thorac Soc. 2022;19(2):171–178. doi:10.1513/AnnalsATS.202009-1187OC
7. Sundh J, Ekström M. Persistent disabling breathlessness in chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2016;11:2805–2812. doi:10.2147/COPD.S119992
8. Carette H, Zysman M, Morelot-Panzini C, et al. Prevalence and management of chronic breathlessness in COPD in a tertiary care center. BMC Pulm Med. 2019;19(1):95. doi:10.1186/s12890-019-0851-5
9. Hanania NA, O’Donnell DE. Activity-related dyspnea in chronic obstructive pulmonary disease: physical and psychological consequences, unmet needs, and future directions. Int J Chron Obstruct Pulmon Dis. 2019;14:1127–1138. doi:10.2147/COPD.S188141
10. Olsson M, Björkelund AJ, Sandberg J, et al. Factors most strongly associated with breathlessness in a population aged 50-64 years. ERJ Open Res. 2024;10(2):00582–2023. doi:10.1183/23120541.00582-2023
11. Shin J, Cooley ME, Hammer MJ, et al. Clinical History, Spirometry, and CT Features Can Predict Dyspnea in Smokers with and without Spirometry-Defined COPD. Lung. 2026;204(1):10. doi:10.1007/s00408-026-00871-5
12. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. PLoS Med. 2007;4(10):e296. doi:10.1371/journal.pmed.0040296
13. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. Available from: http://www.goldcopd.org/.
14. Massart A, Hunt DP. Management of Refractory Breathlessness: a Review for General Internists. J Gen Intern Med. 2021;36(4):1035–1040. doi:10.1007/s11606-020-06439-0
15. Bowerman C, Bhakta NR, Brazzale D, et al. A race-neutral approach to the interpretation of lung function measurements. Am J Respir Crit Care Med. 2023;207(6):768–774. doi:10.1164/rccm.202205-0963OC
16. Lee KY, Wu SM, Kou HY, et al. Association of air pollution exposure with exercise-induced oxygen desaturation in COPD. Respir Res. 2022;23(1):77. doi:10.1186/s12931-022-02000-1
17. Chen KY, Kuo HY, Lee KY, et al. Associations of the distance-saturation product and low-attenuation area percentage in pulmonary computed tomography with acute exacerbation in patients with chronic obstructive pulmonary disease. Front Med Lausanne. 2022;9:1047420. doi:10.3389/fmed.2022.1047420
18. Zemans RL, Jacobson S, Keene J, et al. Multiple biomarkers predict disease severity, progression and mortality in COPD. Respir Res. 2017;18(1):117. doi:10.1186/s12931-017-0597-7
19. Das N, Topalovic M, Aerts JM, Janssens W. Area under the forced expiratory flow-volume loop in spirometry indicates severe hyperinflation in COPD patients. Int J Chron Obstruct Pulmon Dis. 2019;14:409–418. doi:10.2147/COPD.S185931
20. Bhatt SP, Soler X, Wang X, et al. Association between functional small airway disease and FEV1 decline in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2016;194(2):178–184. doi:10.1164/rccm.201511-2219OC
21. Davis CW, Lopez CL, Bell AJ, et al. The severity of functional small airway disease in military personnel with constrictive bronchiolitis as measured by quantitative computed tomography. Am J Respir Crit Care Med. 2022;206(6):786–789. doi:10.1164/rccm.202201-0153LE
22. Rockwood K, Theou O. Using the clinical frailty scale in allocating scarce health care resources. Can Geriatr J. 2020;23(3):210–215. doi:10.5770/cgj.23.463
23. Duarte AG, Tung L, Zhang W, Hsu ES, Kuo YF, Sharma G. Spirometry measurement of peak inspiratory flow identifies suboptimal use of dry powder inhalers in ambulatory patients with COPD. Chronic Obstr Pulm Dis. 2019;6(3):246–255. doi:10.15326/jcopdf.6.3.2018.0163
24. Anderson M, Collison K, Drummond MB, et al. Peak inspiratory flow rate in COPD: an analysis of clinical trial and real-world data. Int J Chron Obstruct Pulmon Dis. 2021;16:933–943. doi:10.2147/COPD.S291554
25. Kim DH, Jeon ET, Lee HJ, et al. Longitudinal changes in maximal forced inspiratory flow and clinical outcomes in patients with COPD. Chest. 2025;167(1):76–86. doi:10.1016/j.chest.2024.07.162
26. Oliveira A, Machado A, Marques A. Minimal Important and detectable differences of respiratory measures in outpatients with AECOPD(†). Copd. 2018;15(5):479–488. doi:10.1080/15412555.2018.1537366
27. Ammous O, Feki W, Lotfi T, et al. Inspiratory muscle training, with or without concomitant pulmonary rehabilitation, for chronic obstructive pulmonary disease (COPD). Cochrane Database Syst Rev. 2023;1(1):Cd013778.
28. Bathoorn E, Kerstjens H, Postma D, Timens W, MacNee W. Airways inflammation and treatment during acute exacerbations of COPD. Int J Chron Obstruct Pulmon Dis. 2008;3(2):217–229. doi:10.2147/COPD.S1210
29. O’Donnell DE, Parker CM. COPD exacerbations. 3: pathophysiology. Thorax. 2006;61(4):354–361. doi:10.1136/thx.2005.041830
30. Scioscia G, Blanco I, Arismendi E, et al. Different dyspnoea perception in COPD patients with frequent and infrequent exacerbations. Thorax. 2017;72(2):117–121. doi:10.1136/thoraxjnl-2016-208332
31. O’Donnell DE, Banzett RB, Carrieri-Kohlman V, et al. Pathophysiology of dyspnea in chronic obstructive pulmonary disease: a roundtable. Proc Am Thorac Soc. 2007;4(2):145–168. doi:10.1513/pats.200611-159CC
32. O’Donnell DE, Milne KM, James MD, de Torres JP, Neder JA. Dyspnea in COPD: new mechanistic insights and management implications. Adv Ther. 2020;37(1):41–60. doi:10.1007/s12325-019-01128-9
33. Decramer M, Rennard S, Troosters T, et al. COPD as a lung disease with systemic consequences--clinical impact, mechanisms, and potential for early intervention. Copd. 2008;5(4):235–256. doi:10.1080/15412550802237531
34. Patel AR, Hurst JR. Extrapulmonary comorbidities in chronic obstructive pulmonary disease: state of the art. Expert Rev Respir Med. 2011;5(5):647–662. doi:10.1586/ers.11.62
35. O’Donnell DE, Laveneziana P. Dyspnea and activity limitation in COPD: mechanical factors. Copd. 2007;4(3):225–236. doi:10.1080/15412550701480455
36. Soffler MI, Hayes MM, Schwartzstein RM. Respiratory sensations in dynamic hyperinflation: physiological and clinical applications. Respir Care. 2017;62(9):1212–1223. doi:10.4187/respcare.05198
37. O’Donnell DE, Laveneziana P. The clinical importance of dynamic lung hyperinflation in COPD. Copd. 2006;3(4):219–232. doi:10.1080/15412550600977478
38. O’Donnell DE, Laveneziana P. Physiology and consequences of lung hyperinflation in COPD. Eur Respir Rev. 2007;15(100):61–67. doi:10.1183/09059180.00010002
39. Rogliani P, Calzetta L, Coppola A, et al. Optimizing drug delivery in COPD: the role of inhaler devices. Respir Med. 2017;124:6–14. doi:10.1016/j.rmed.2017.01.006
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
U-Shaped Relationship Between Serum Lactate Dehydrogenase with All-Cause Mortality in Patients with Chronic Obstructive Pulmonary Disease
Huang L, Lu Z, Zhou X, He L, You X, Chen C, Zou C
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:305-316
Published Date: 15 March 2023
Characteristics of Inhaler Technique in COPD Patients in a Specialized Center in Armenia, Colombia: A Cross-Sectional Study
Montes Cardona JA, Hincapié Erira DA, Nati-Castillo HA, Sánchez-Vallejo J, Izquierdo-Condoy JS
Patient Preference and Adherence 2023, 17:2025-2038
Published Date: 16 August 2023
Adherence to Inhalation Devices in Patients with Chronic Obstructive Pulmonary Disease
Valladales-Restrepo LF, Oyuela-Gutiérrez MC, Delgado-Araujo AC, Calvo-Salazar J, Osorio-Bustamante D, Lerma-Barco CE, Machado-Alba JE
Patient Preference and Adherence 2023, 17:3233-3244
Published Date: 8 December 2023
The Dosing Strategy to Improve Adherence to Roflumilast in Treatment for Chronic Obstructive Lung Disease: A Systemic Review and Meta-Analysis
Lee J, Song JU
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:655-663
Published Date: 5 March 2024
COTE and Pulmonary Comorbidities Predict Moderate-to-Severe Acute Exacerbation and Hospitalization in COPD
Chen Q, Wang X, Yao X, Zhang L, Liu X
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:1893-1913
Published Date: 11 June 2025