Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
COTE and Pulmonary Comorbidities Predict Moderate-to-Severe Acute Exacerbation and Hospitalization in COPD
Authors Chen Q, Wang X, Yao X, Zhang L ![]() , Liu X
, Liu X
Received 18 January 2025
Accepted for publication 31 May 2025
Published 11 June 2025 Volume 2025:20 Pages 1893—1913
DOI https://doi.org/10.2147/COPD.S518218
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Fanny Wai San Ko
Qinglin Chen,1,* Xinmao Wang,1,* Xiujuan Yao,1 Luo Zhang,2– 4 Xiaofang Liu1
1Department of Respiratory and Critical Care Medicine, Beijing Tongren Hospital, Capital Medical University, Beijing, People’s Republic of China; 2Beijing Laboratory of Allergic Diseases, Beijing Municipal Education Commission, Beijing, People’s Republic of China; 3Department of Otolaryngology Head and Neck Surgery, Beijing Tongren Hospital, Capital Medical University, Beijing, People’s Republic of China; 4Key Laboratory of Otolaryngology Head and Neck Surgery of Ministry of Education of China, Beijing Institute of Otolaryngology, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaofang Liu, Department of Respiratory and Critical Care Medicine, Beijing Tongren Hospital, Capital Medical University, No.2, Xinanhuan Road, Yizhuang District, Beijing, 100176, China, Email [email protected] Luo Zhang, Department of Otolaryngology Head and Neck Surgery, Beijing Tongren Hospital, Capital Medical University; Key Laboratory of Otolaryngology Head and Neck Surgery of Ministry of Education of China, Beijing Institute of Otolaryngology, No. 17, Hougou Hutong, Chongnei, Dongcheng District, Beijing, 100730, China, Email [email protected]
Purpose: The aim of this study was to explore the predictive value of the chronic obstructive pulmonary disease (COPD) specific comorbidity test index (COTE) and pulmonary comorbidities for moderate-to-severe acute exacerbation and hospitalization in COPD patients.
Patients and Methods: This was a retrospective cohort study. We included 470 patients with stable COPD. Patients were divided into high or low-risk comorbidity group according to whether COTE score ≥ 4, and pulmonary comorbidities and extrapulmonary comorbidities group according to comorbidity origin. Moderate-to-severe acute exacerbation events and other clinical parameters were compared between groups. Multifactorial analysis and Lasso regression were used to screen risk factors and establish predictive models for moderate-to-severe acute exacerbation and hospitalization. The receiver operating characteristic (ROC) curve was used to assess the value COTE score and pulmonary comorbidities in predicting moderate-to-severe acute exacerbation and hospitalization.
Results: When compared with the low-risk comorbidity and extrapulmonary comorbidities group, the rate of patients with ≥ 2 moderate-to-severe acute exacerbations and requiring hospitalization due to acute exacerbations is higher in high-risk comorbidity and pulmonary comorbidities group (χ²=18.45, χ²=40.15, χ²=8.82, χ²=23.68). Multifactorial analysis showed that comorbid with asthma, lung cancer were risk factors for moderate-to-severe acute exacerbations, while asthma, bronchiectasis, lung cancer, and high COTE score were risk factors for patients requiring hospitalization due to acute exacerbations. The AUC for COTE > 5.5 and a combination of at least one pulmonary comorbidity as potential indication of moderate-to-severe acute exacerbations of COPD and hospitalization due to acute exacerbations was 0.667 (95% CI: 0.615, 0.719) and 0.740 (95% CI: 0.688, 0.792), respectively. The prediction models including COTE and pulmonary comorbidities can predict moderate-to-severe acute exacerbations (internal validation of AUC: 0.984, 95CI%: 0.964– 1) and hospitalization (internal validation of AUC: 0.978, 95CI%: 0.959– 0.998) of COPD.
Conclusion: COTE score and a combination of at least one pulmonary disease can predict the risk of moderate-to-severe acute exacerbations and hospitalization due to acute exacerbations in patients with COPD.
Keywords: acute exacerbation, chronic obstructive, comorbidity, hospitalization, pulmonary disease
Introduction
Chronic obstructive pulmonary disease (COPD) is a pervasive and severe pulmonary disease, ranking as the third most common cause of death in China.1,2 Comorbidity is typically characterized by the simultaneous occurrence of two or more chronic diseases that may have comparable etiologies or therapies.3 The mortality increases when COPD patients have comorbidities.4–6 Previous studies indicate that higher Charlson Comorbidity Index (CCI) is associated with severe clinical symptoms, increased mortality, high hospitalization expenses, and more hospitalizations in the previous year in COPD.7–9 The COPD specific comorbidity test index (COTE), developed in 2012, was the first specific clinical tool for predicting the risk of death with comorbid COPD.4 It has also been used for predicting acute exacerbations of COPD.10 However, the clinical features of COPD patients with high-risk comorbidity based on COTE index are still not well evaluated. Furthermore, COTE index only includes lung cancer and pulmonary fibrosis and does not consider other common pulmonary comorbidities, such as asthma and bronchiectasis. However, asthma, bronchiectasis and other chronic respiratory diseases (which can be called pulmorbidome6) are also common comorbidities of COPD11,12 and have been shown to be related to acute exacerbations of COPD.13 In this retrospective cohort study, we aim to explore the clinical features of COPD patients with higher COTE index (≥4) and with pulmonary comorbidities. We also assess the value of COTE index and pulmonary comorbidities in predicting the risk of moderate-to-severe acute exacerbations and hospitalization due to acute exacerbations.
Materials and Methods
Ethics Statement
This study was a retrospective cohort study and followed with the Helsinki Declaration and was approved by the Ethics Review Committee (TREC2024-KY004). Due to the retrospective nature of the study, informed consent was waived. All methods were performed in accordance with institutional and national guidelines and regulations. All patient data were anonymized before analysis, and strict confidentiality was maintained throughout, in compliance with institutional and national data protection regulations.
Study Design and Protocol
Study Population
All patients were stable COPD from the Respiratory and Critical Care Medicine outpatient clinics, Beijing Tongren Hospital and Mentougou Hospital, Capital Medical University, the study period was from April 2020 to March 2023. Eligible patients were fulfilling those inclusion criteria, including: (1) Global Initiative for Chronic Obstructive Lung Disease (GOLD), a post-bronchodilator forced expiratory volume in 1 s (FEV1)/forced vital capacity (FVC) index <0.70;1 (2) age >40 years and ≤ 85 years; (3) diagnosed COPD for more than 1 year, stable COPD: the patient had stable or mild symptoms of cough, sputum, and shortness of breath, had the usage of inhaled glucocorticoids (ICS) and/or long-acting beta agonists (LABA) were not increased in the prior 4 weeks, and was not taking antibiotics or systemic glucocorticoids; (4) case data documented moderate-to-severe acute exacerbation events, defined as moderate: use of short-acting bronchodilators and antimicrobials, with or without oral glucocorticoids (OCS), severe: hospitalization or treatment in an emergency room or intensive care unit (ICU);14 (5) case data documented diagnosis of comorbidities, which meets the applicable guideline diagnostic criteria.
Patients with interstitial lung disease (ILD), active tuberculosis, pleural effusion, pulmonary embolism, cognitive dysfunction and impairment of physical activity, depression and insufficient clinical data were excluded (Figure 1).
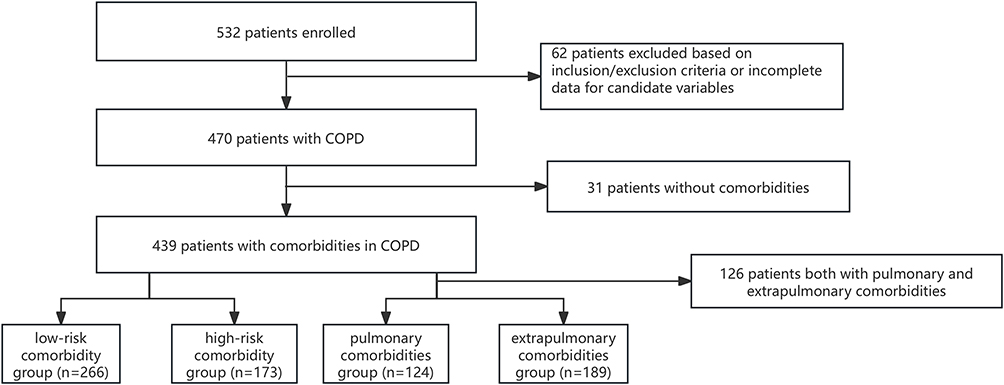 |
Figure 1 Flow of participants through the study. Abbreviations: COPD, chronic obstructive pulmonary disease. |
Definition of Low-Risk and High-Risk Comorbidity Group
Chronic Obstructive Pulmonary Specificity Index (COTE) was employed, which included 12 comorbidities with major points of 6, 2 and 1. The 6 points including lung/esophageal/pancreatic and breast cancer and anxiety. The 2 points including all other cancers, liver cirrhosis, atrial fibrillation/flutter, diabetes with neuropathy, pulmonary fibrosis. The 1 point including congestive heart failure, gastric/duodenal ulcers and coronary heart disease.4,10 We defined high-risk comorbidity group as COTE score ≥4, low-risk comorbidity group as COTE <4.10
Definition of Pulmonary Comorbidities and Extrapulmonary Comorbidities Group
We defined pulmonary comorbidities group as at least one of asthma, bronchiectasis, lung cancer, OSA and pulmonary hypertension, and extrapulmonary comorbidities group at least one chronic disease except respiratory disease. Pulmonary comorbidities include: lung cancer, bronchiectasis, asthma, and obstructive sleep apnea (OSA),12 according to Chinese COPD comorbidities study.14 Extrapulmonary comorbidities include: cardiovascular diseases including hypertension, coronary atherosclerotic heart disease (CHD), arrhythmia, and peripheral arterial atherosclerosis; cerebrovascular diseases including ischemic cerebrovascular disease, endocrine metabolic diseases including diabetes and osteoporosis, and digestive diseases including reflux esophagitis and gastric/duodenal ulcer. Anxiety and depression were identified by a total score ≥8 on the Hospital Anxiety and Depression Rating Scale15 during the visit.
Data Collection
All medical records in the electronic database were independently reviewed by two trained and experienced researchers. We enrolled stable COPD patients with gender, age, body mass index (BMI), duration of COPD, duration of smoking, smoking index, whether or not quit smoking, number of moderate-to-severe acute exacerbations and hospitalizations in the past one year, GOLD grade, ABE group1 and medicine use of COPD.
Objective Tests
Blood Test
We enrolled routine blood counts including peripheral blood leukocyte count, neutrophil percentage (NE), NE count, eosinophil percentage (EOS), EOS count, hemoglobin, brain natriuretic peptide (BNP), albumin, triglycerides, total cholesterol, low-density lipoprotein (LDL), high-density lipoprotein (HDL) and glycosylated hemoglobin (HbA1c).
Pulmonary Function Tests
We enrolled lung function index when patients come to the outpatient clinics, including total lung capacity (TLC), residual volume (RV), RV/TLC, forced expiratory volume in one second (FEV1), FEV1%pred, FEV1/forced vital capacity (FVC), maximal expiratory flow at 25% of FVC (MEF25%), maximal expiratory flow at 25%–75% (MEF75/25%), maximal expiratory flow at 50% of FVC (MEF50%), diffusion capacity for carbon monoxide of the lung (DLCO), fractional exhaled nitric oxide (FeNO) (NIOX Aerocrine AB, Sweden).
Questionnaires
All patients completed the following questionnaires during the visiting to outpatient clinics:
1. Frail scale: Frailty was evaluated through the Fatigue, Resistance, Ambulation, Illnesses, and Loss of weight scale, a questionnaire with five self-report items for which the possible answers are “yes” or “no”, with an attribution of 1 or 0 points, respectively.16
2. modified British medical research coucil (mMRC): mMRC scale was the first questionnaire developed to measure breathnessless, which was consisting of 0–4 grade of dyspnea.1
3. COPD assessment test (CAT): The CAT was an 8-item questionnaire including cough, phlegm, chest tightness, shortness of breath, activity limitations at home, confidence in leaving home, sleep, and energy. Each item is given a score from 0 to 5.1
Statistical Analysis
Data were analysed by using SPSS version 26, R version 4.4.2 and prism version 9. Descriptive results for continuous variables were reported as means ± standard deviation (SD), while categorical variables were presented as frequencies (%) and non-normally distributed continuous measures as median (quartiles). Normally distributed data were analysed by using Independent Samples T-test or one-way ANOVA depending on the number of groups. For non-normally distributed continuous, group comparisons were calculated using either the Mann–Whitney U-test or the Kruskal–Wallis test. For categorical variables, we employed the χ2 test or Fisher’s exact probability tests. The univariate analysis included descriptive variables and categorical variables, multivariate logistic regression analysis included variables with statistically significant differences in the univariate analysis. The results were represented by forest plots. The multicollinearity test was used to determine whether the multifactorial logistic regression has multicollinearity. Variables with a variance inflation factor (VIF) value of <10 were regarded to without multicollinearity. Selected risk factors were fitted to construct a moderate-to-severe acute exacerbation and a hospitalization warning model, and the receiver operating characteristic (ROC) curve was used to evaluate the related efficacy of the two models. To further examine the relationship between COTE and moderate-to-severe acute exacerbation and hospitalizations, we employed tetrachoric correlations and performed a correlation heatmap. Lasso regression was used to screen the influencing factors and build a predictive model for moderate-to-severe acute exacerbation and hospitalization in COPD. We use internal validation (Bootstrap), calibration curve and DCA decision curve to determine the models predicted efficacy. We also analyzed the impact of COTE score and pulmonary comorbidities on acute exacerbation and hospitalization in different age subgroups. A two-tailed p-value <0.05 was considered significant.
Results
Prevalence of Comorbidities in Patients with COPD
A total of 470 patients were enrolled in this cohort. Among them, 31 patients had no comorbidities (Figure 1), while 439 patients (93.40%) had comorbidities. Respiratory diseases (269/439, 61.28%) were the most common comorbidities, of which 102 (23.23%) were asthma, 87 (19.82%) were bronchiectasis, 47 (10.71%) were lung cancer and 33 (7.50%) were OSA. Others comorbidities include hypertension (252/439, 57.40%), CHD (123/439, 28.02%), diabetes (116/439, 26.42%), anxiety (98/439,22.32%), depression (85/439, 19.40%), peripheral arterial atherosclerosis (78/439, 17.77%), cerebrovascular disease (72/439, 16.40%), arrhythmia (68/439, 15.49%), osteoporosis (14/439, 3.19%), gastric/duodenal ulcer (92/439, 20.96%), and reflux esophagitis (53/439, 12.07%). We also found that 124 (28.25%) patients only complicated with pulmonary diseases, 189 (43.05%) only with extrapulmonary diseases, and 126 (28.70%) both with pulmonary and extrapulmonary diseases (Figure 1).
Comparison of Clinical Features Between High- and Low-Risk Comorbidity Group According to COTE Index
A total of 266 patients (60.59%) were classified into the low-risk comorbidity group, while 173 patients (39.41%) were into the high-risk comorbidity group (Figure 1). Compared with the low-risk comorbidity group, the high-risk comorbidity group had a higher proportion of older age, longer duration of COPD and a higher proportion of comorbidities, including asthma, bronchiectasis, lung cancer, OSA, hypertension, coronary atherosclerotic heart disease, arrhythmia, diabetes, peripheral arterial atherosclerosis, gastric/duodenal ulcer, reflux esophagitis, anxiety and depression (all P< 0.05). There were no statistically significant differences between the two groups regarding gender, BMI, smoking status, duration of smoking, smoking index, smoking cessation, comorbid with cerebrovascular disease or osteoporosis (all P> 0.05) (Table 1). The high-risk group showed significantly lower levels of peripheral blood hemoglobin, FEV1, FEV1%pred, FEV1/FVC, MEF25%, and MEF75/25%, and higher levels of BNP and HbA1c (all P< 0.05) (Table 2). Patients with high-risk comorbidity showed higher frailty, mMRC, and CAT scores. The proportion of patients with ≥2 moderate-to-severe acute exacerbations in the past year and those requiring hospitalization due to acute exacerbations was also higher in high-risk comorbidity group. Additionally, the proportion of severe and very severe GOLD stage, E of ABE group, the use of SABA or SAMA and ICS were also higher in high-risk comorbidity group (all P< 0.05) (Table 3).
 |
Table 1 Clinical Features Between Low- and High-Risk Comorbidity Group |
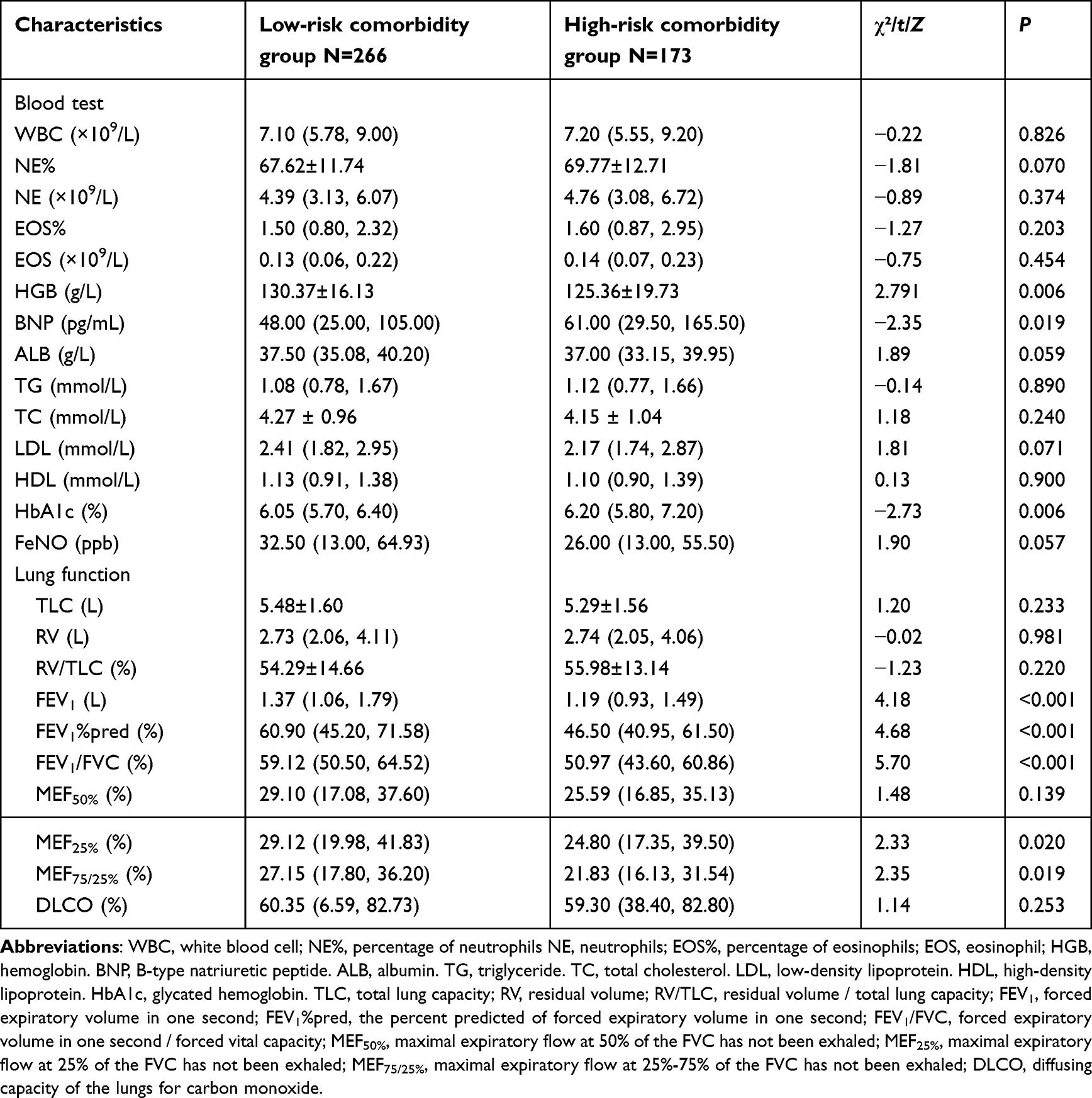 |
Table 2 Blood Test and Lung Function Between Low- and High-Risk Comorbidity Group |
 |
Table 3 System Features and Drug Use Between Low- and High-Risk Comorbidity Group |
Tetrachoric Correlations Between COTE Index and Other Clinical Features
The COTE index score was positively correlated with the number of hospitalizations and moderate-to-severe acute exacerbation, mMRC, CAT, BNP, HbA1c, age and BMI (r > 0). Conversely, it was negatively correlated with FEV1, FEV1%, FEV1/FVC, MEF75/25%, and hemoglobin (r < 0) (Figure 2, Table S1).
 |
Figure 2 Correlation heatmap of COTE. Abbreviations: BMI, body mass index; HbA1c, glycated hemoglobin; BNP, B-type natriuretic peptide; HGB, hemoglobin; MEF75/25%, maximal expiratory flow at 25%–75% of the FVC has not been exhaled; FEV1/FVC, forced expiratory volume in one second/forced vital capacity; FEV1%, the percent predicted of forced expiratory volume in one second; FEV1, forced expiratory volume in one second; CAT, chronic obstructive pulmonary disease assessment test; mMRC, modified British medical research council; AE Events, acute exacerbation events; COTE, chronic obstructive pulmonary disease-specific comorbidity test index. |
Logistic Regression for Moderate-to-Severe Acute Exacerbation of COPD
Univariate analysis showed that male, duration of COPD >10 years, high COTE score, high frailty score, combined with asthma, bronchiectasis, lung cancer, diabetes, anxiety, gastric/duodenal ulcer, high mMRC, high CAT score, use of ICS, high NE% and high EOS were risk factors for moderate-to-severe acute exacerbation. In contrast, high FEV1/pred%, high FEV1/FVC, high DLCO, and high albumin levels were protective factors (all P< 0.05) (Figure 3a).
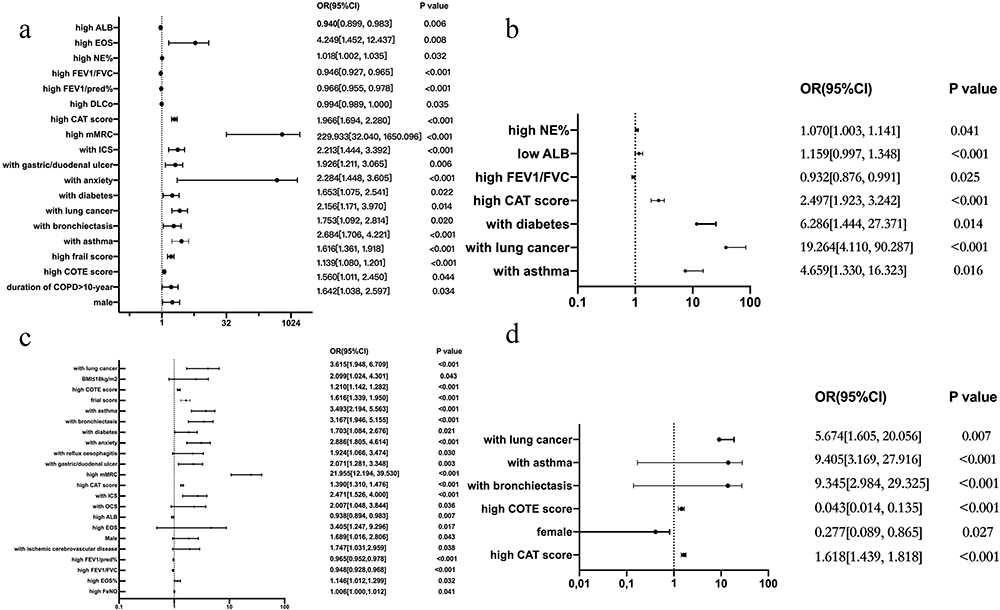 |
Figure 3 Logistic analysis of moderate-to-severe acute exacerbation and hospitalization of COPD. Abbreviations: ALB, albumin; EOS, eosinophil; NE%, percentage of neutrophils; FEV1/FVC, forced expiratory volume in one second/forced vital capacity; FEV1%pred, the percent predicted of forced expiratory volume in one second; DLCO, diffusing capacity of the lungs for carbon monoxide; CAT, chronic obstructive pulmonary disease assessment test; mMRC, modified British medical research council; ICS, inhaled glucocorticoids; COTE, chronic obstructive pulmonary disease-specific comorbidity test index; COPD, chronic obstructive pulmonary disease; BMI, body mass index; OCS, oral corticosteroids; FeNO, fractional exhaled nitric oxide; EOS%, percentage of eosinophils. Notes: (a) Univariate analysis of moderate-to-severe acute exacerbation of COPD; (b) Multivariate analysis of moderate-to-severe acute exacerbation of COPD; (c) Univariate analysis of hospitalization of COPD; (d) Multivariate analysis of hospitalization of COPD. |
Multivariate analysis showed that combined with asthma, lung cancer, diabetes, high mMRC, high CAT score, high NE%, and low albumin were risk factors for moderate-to-severe acute exacerbation, while high FEV1/FVC was a protective factor (all P< 0.05). The VIF values for all variables were <10 (Figure 3b).
Logistic Regression for Hospitalization of COPD
Univariate analysis indicated that BMI ≤ 18 kg/m², male, high COTE score, combined with asthma, bronchiectasis, lung cancer, anxiety, diabetes, ischemic cerebrovascular disease, reflux esophagitis, gastric/duodenal ulcer, high frailty score, high mMRC, high CAT score, use of ICS, use of OCS, high EOS, high EOS%, high FeNO, and low HDL were risk factors for hospitalization. In contrast, high FEV1/pred%, high FEV1/FVC, and high albumin levels were protective factors (all P< 0.05) (Figure 3c).
Multivariate analysis indicated that combined with asthma, bronchiectasis, lung cancer, high CAT score, and high COTE score were risk factors for hospitalization, while female was a protective factor (all P< 0.05). The VIF values for all variables were <10 (Figure 3d).
Comparison of Clinical Features Between Pulmonary and Extrapulmonary Group
Compared with the extrapulmonary comorbidities group, patients in pulmonary comorbidities group were younger, had lower frailty and COTE score, higher mMRC and CAT score. A higher proportion of patients with ≥2 moderate-to-severe acute exacerbations in the past year, a higher proportion of patients requiring hospitalization due to acute exacerbation, and a higher proportion of E group in ABE group were also seen in pulmonary comorbidities group. (all P< 0.05) (Table 4). Patients in pulmonary comorbidities group also had higher level of EOS and EOS% (all P< 0.05) (Table S2).
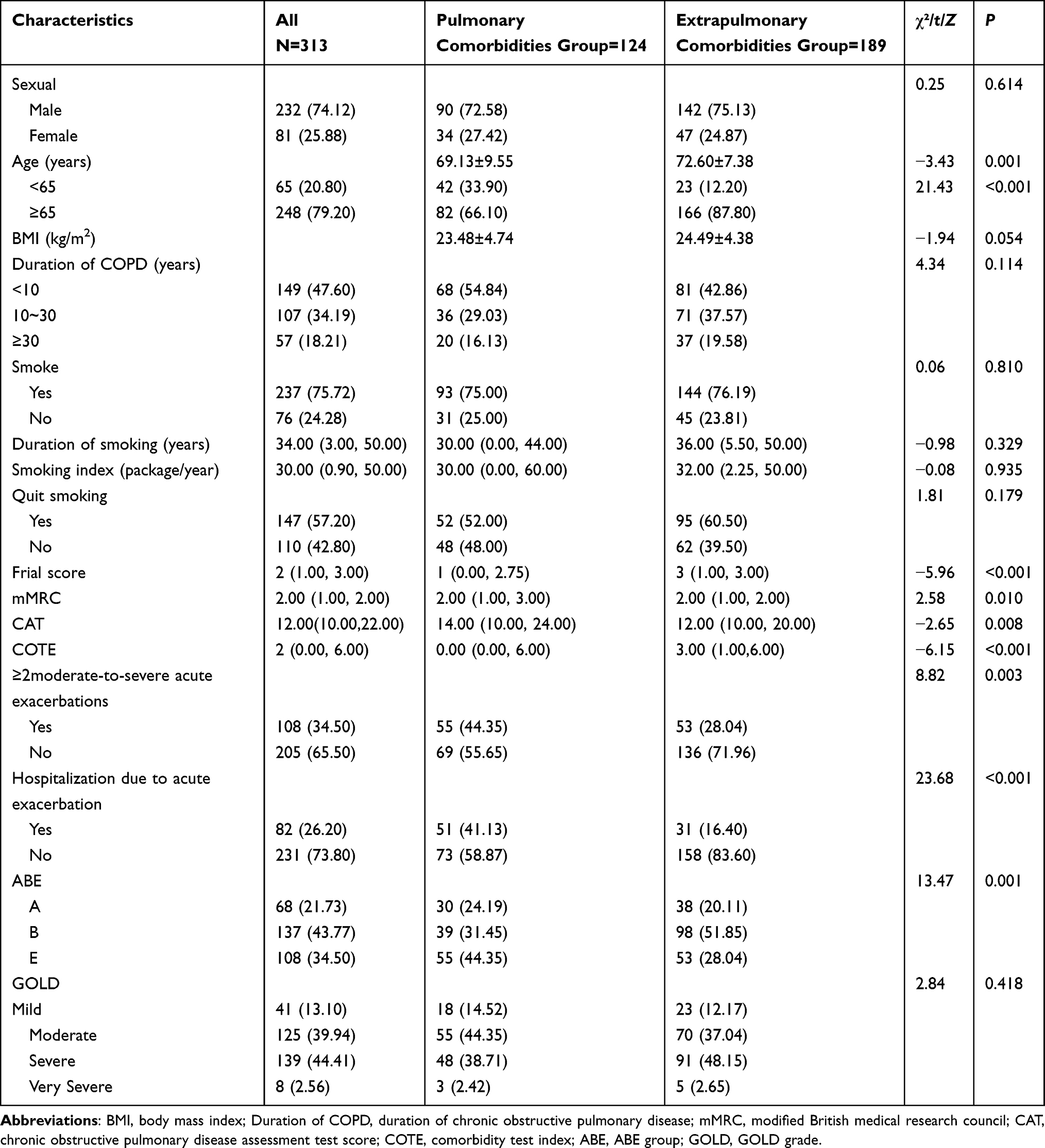 |
Table 4 Clinical Features Between Pulmonary and Extrapulmonary Comorbidities Group |
Relationship of COTE Index Alone or Combined with the Number of Pulmorbidome in Moderate-to-Severe Acute Exacerbation of COPD
The cut-off value of COTE index for moderate-to-severe acute exacerbation of COPD was 5.5 (AUC: 0.624; 95% CI 0.569–0.679, Youden index 0.255, sensitivity 50.30%, specificity 75.20%). The cut-off value of EOS% was 1.65% (AUC: 0.547; 95% CI 0.492–0.602), while the cut-off value for EOS was 0.115x109/L (AUC: 0.571; 95% CI 0.515–0.626). The cut-off value of pulmonary comorbidities (pulmorbidome) was 0.5 (AUC: 0.607; 95% CI 0.553–0.661). COTE index combined with one pulmorbidome as potential indication of moderate-to-severe acute exacerbation with AUC of 0.667 (95% CI 0.615–0.719, Youden index 0.271, sensitivity 43.80%, specificity 83.30%) (Figure 4a).
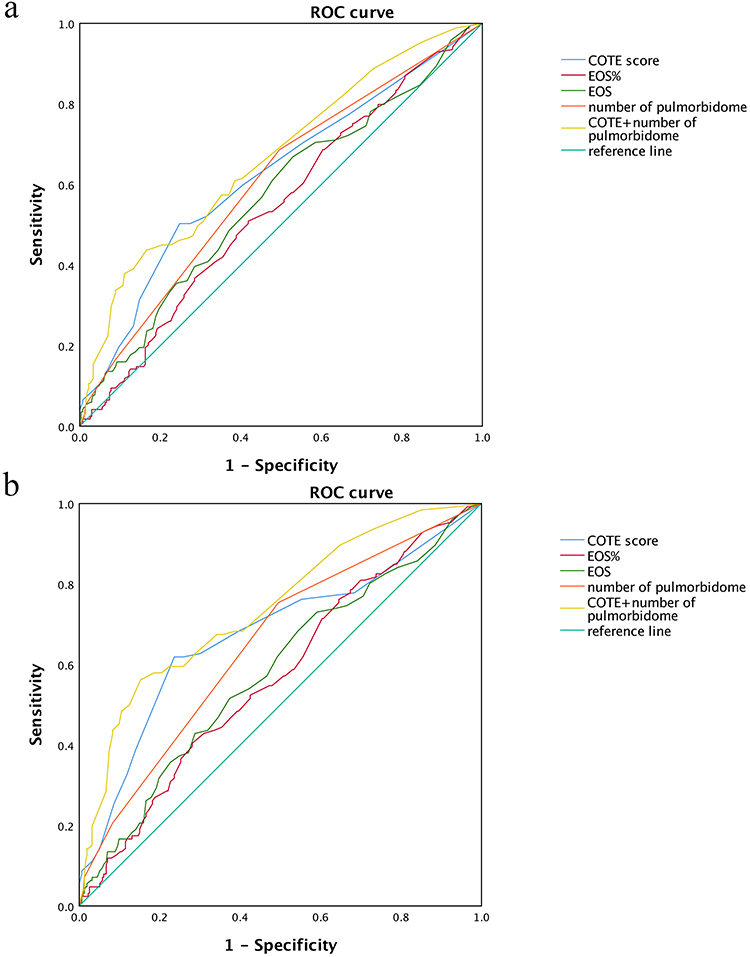 |
Figure 4 ROC curve of moderate-to-severe acute exacerbation and hospitalization of COPD. Abbreviations: COTE, chronic obstructive pulmonary disease-specific comorbidity test index; EOS, eosinophil; EOS%, percentage of eosinophils; pulmorbidome, pulmonary comorbidities. Notes: (a) ROC curve of moderate-to-severe acute exacerbation of COPD; (b) ROC curve of hospitalization of COPD. |
Relationship of COTE Index Alone or Combined with the Number of Pulmorbidome in Hospitalization of COPD
The cut-off value of COTE index for hospitalization due to acute exacerbation was 5.5 (AUC: 0.675; 95% CI 0.616–0.735), Youden index 0.383, sensitivity 61.90%, was 76.40%. The cut-off value of EOS% was 2.24% (AUC: 0.570; 95% CI 0.512–0.629), and EOS was 0.155x109/L (AUC: 0.582; 95% CI 0.522–0.641). The cut-off value of Pulmorbidome was 0.5 (AUC: 0.651; 95% CI 0.594–0.707, Youden index 0.259, sensitivity 75.40%, specificity 50.50%). The AUC for COTE index combined with pulmorbidome as potential indication of hospitalization due to acute exacerbation was 0.740 (95% CI 0.688–0.792, Youden index 0.410, sensitivity 55.30%, specificity 84.70%) (Figure 4b).
Prediction Model to Predict Risk of Moderate-to-Severe Acute Exacerbation and Hospitalization of COPD
Lasso regression was used to analyze the relationship between moderate-to-severe acute exacerbation and the following variables: mMRC, duration of COPD, COTE, FEV1/FVC, CAT, combined with lung cancer, asthma. Lasso regression was also used to analyze the relationship between hospitalization due to AECOPD and the following variables: combined with lung cancer, asthma, bronchiectasis, COTE, mMRC, CAT (Figure S1 and S2). Each of these variables was included in the predictive model, and the regression results were internally validated by the Bootstrap method. The results showed that the AUC was 0.992 (95CI%: 0.986–0.998, sensitivity 91.5%, specificity 98.8%) for the train set, while theAUC was: 0.984 (95CI%: 0.964–1, sensitivity 91.5%, specificity 98.8%) for the validation set of moderate-to-severe acute exacerbation of COPD in the prediction model (Figure 5a and b). We also showed that the AUC was 0.98 (95CI%: 0.967–0.992, sensitivity 97.1%, specificity 90.7%) for the train set, while the AUC was 0.978 (95CI%: 0.959–0.998, sensitivity 97.1%, specificity 90.7%) for the validation set of hospitalization of COPD in the prediction model (Figure 6a and b).
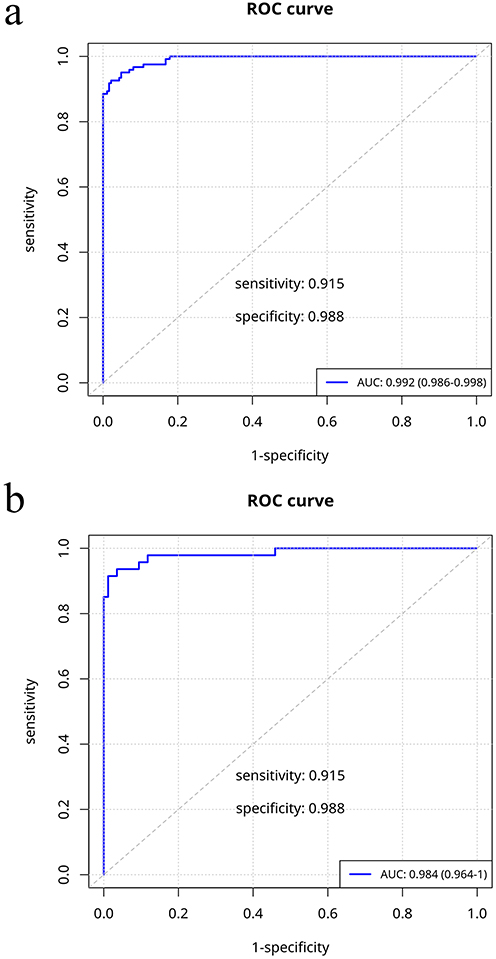 |
Figure 5 Prediction model of ROC curve of moderate-to-severe acute exacerbation in COPD. Notes: (a) the train set of ROC curve of prediction model of moderate-to-severe acute exacerbation in COPD; (b) the validation set of ROC curve of prediction model of moderate-to-severe acute exacerbation in COPD. |
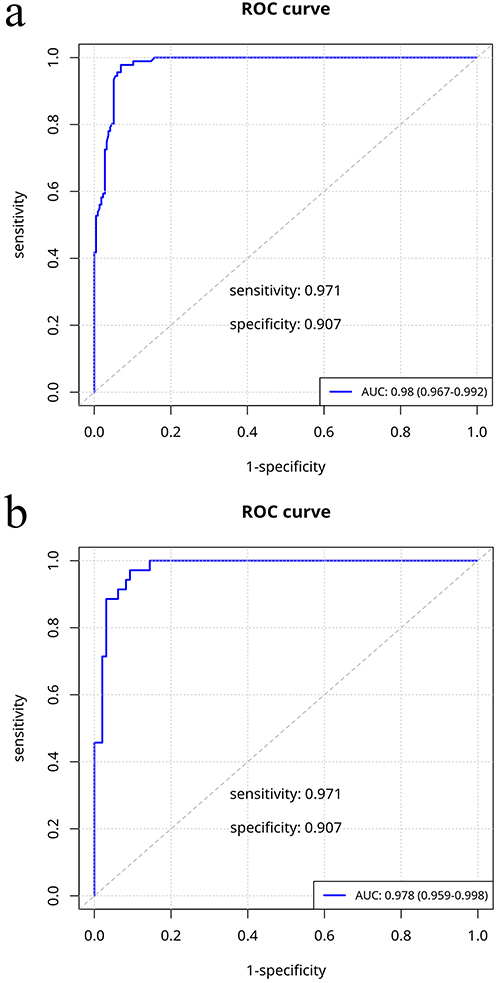 |
Figure 6 Prediction model of ROC curve of hospitalization in COPD. Notes: (a) the train set of ROC curve of prediction model of hospitalization in COPD; (b) the validation set of ROC curve of prediction model of hospitalization in COPD. |
The calibration curve for the train and validation sets is well fitted and the DCA showed that the model works well (Figure S3–S12). The above indicators were incorporated into a Nomogram (Figures 7, 8), which included points, each of the indicators, the total points and the linear predictor, and the risk of the outcome. Each patient could be assigned a score for each indicator in the nomogram, and the sum of the individual scores was labeled as the predicted probability of risk in the horizontal line of the total score.
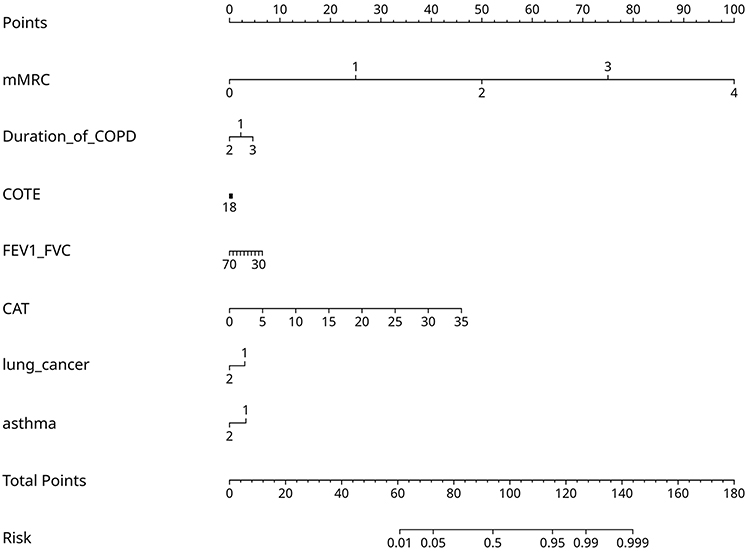 |
Figure 7 Nomogram to predict the risk of moderate-to-severe acute exacerbation in COPD. Lung_cancer/asthma (1: with; 2: without). Abbreviations: mMRC, modified British medical research council; Duration_of_COPD, Duration of chronic obstructive pulmonary disease (1: <10 years; 2: 10–30 years; 3: ≥30 years); COTE, chronic obstructive pulmonary disease-specific comorbidity test index; FEV1_FVC, forced expiratory volume in one second/forced vital capacity; CAT, chronic obstructive pulmonary disease assessment test score. |
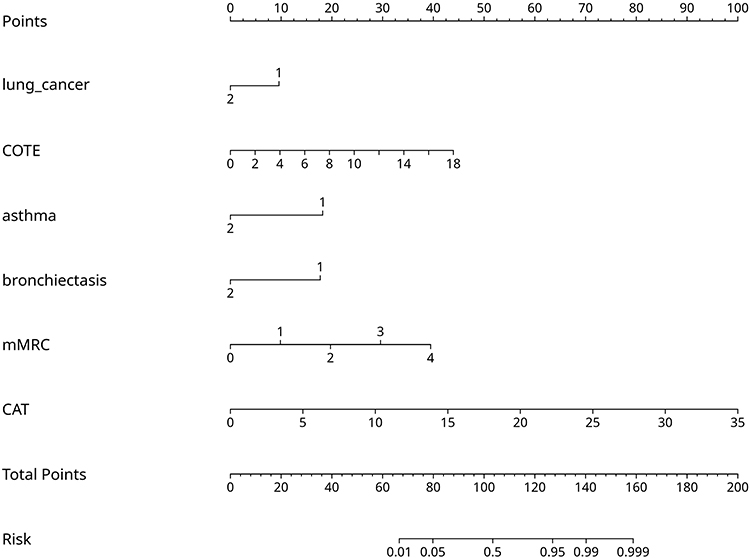 |
Figure 8 Nomogram to predict the risk of hospitalization in COPD. Lung_cancer/asthma/bronchiectasis (1: with; 2: without). Abbreviations: COTE, chronic obstructive pulmonary disease-specific comorbidity test index; mMRC, modified British medical research council; CAT, chronic obstructive pulmonary disease assessment test score. |
Impact of Age Subgroup to COTE and the Number of Pulmorbidome in Moderate-to-Severe Acute Exacerbation and Hospitalization of COPD
We divided the cohort into two groups according to age, ie, ≥65 years group (n=336) and <65 years group (n=103). After adjusted sexual, somke and FEV1%, we analyzed the impact of age on the ability of COTE and the number of pulmorbidome to predict moderate-to-severe acute exacerbation and hospitalization of COPD by Logistic regression. The results showed both in ≥65 years and in <65 years group, COTE is an independent predictor for moderate-to-severe acute exacerbation (OR: 1.103 [95% CI: 1.037, 1.174] and OR: 1.244 [95% CI: 1.099, 1.409], respectively, P<0.05) and hospitalization (OR: 1.189 [95% CI: 1.110, 1.274] and OR: 1.286 [95% CI: 1.129, 1.464], respectively, P<0.05). Also, the number of pulmorbidome was related to moderate-to-severe acute exacerbation (OR: 1.651 [95% CI: 1.228, 2.221] and OR: 1.773 [95% CI: 1.039, 3.024], respectively, P<0.05) and hospitalization (OR: 2.045 [95% CI: 1.480, 2.826] and OR: 2.199 [95% CI: 1.245, 3.885], respectively, P<0.05) in both ≥65 years and <65 years group (Figure 9).
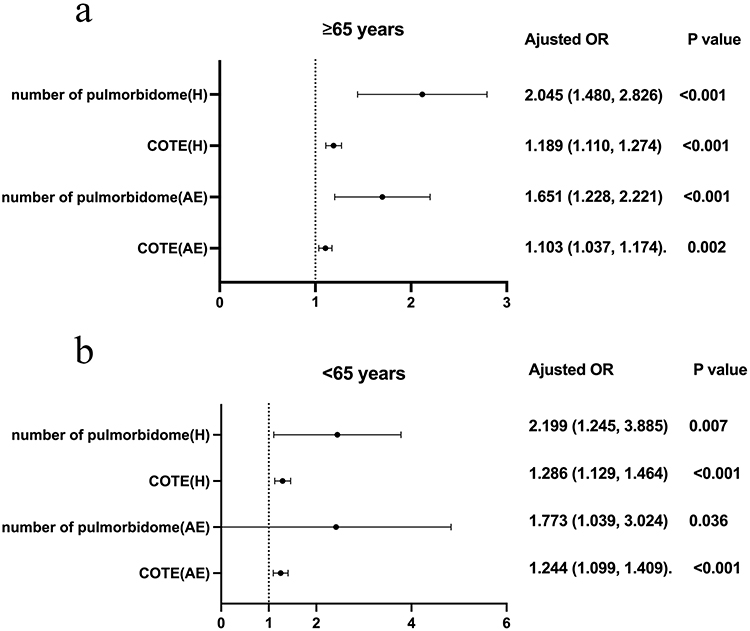 |
Figure 9 Impact of age subgroup to COTE and the number of pulmorbidome in moderate-to-severe acute exacerbation and hospitalization of COPD. Abbreviations: COTE, chronic obstructive pulmonary disease-specific comorbidity test index; pulmorbidome, pulmonary comorbidities; AE, moderate-to-severe acute exacerbation; H, hospitalization. Note: (a) forest plot of moderate-to-severe acute exacerbation of COPD; (b) forest plot of hospitalization of COPD. |
Discussion
Acute exacerbation is a common feature of COPD and seriously affects the prognosis. How to accurately predict or identify patients who will develop acute exacerbations in COPD is not fully understood. In this current retrospective cohort study, we found that the rate of patients with ≥2 moderate-to-severe acute exacerbations and requiring hospitalization due to acute exacerbations is significantly higher in COPD patients with high-risk comorbidities and with pulmonary comorbidities. We also found that COTE score >5.5 and a combination of one pulmonary disease can predict the risk of moderate-to-severe acute exacerbations and hospitalization due to acute exacerbations in patients with COPD. Predictive models including COET score and pulmonary comorbidities can predict acute exacerbation and hospitalization with good sensitivity and specificity. COPD is regarded as the outcome of intricate, cumulative gene–environment interactions that affect not only the lungs but also other organ systems, resulting in the simultaneous appearance of many comorbidities as individuals age.17,18 Putcha N and Huang K revealed that 86–98% of COPD patients had at least one comorbidity, with the predominant five being hypertension, diabetes, asthma, bronchiectasis, and coronary artery disease.8,14 Similarly, our study revealed that 93% of COPD patients had at least one comorbidity, most of which are respiratory illnesses (such as asthma, bronchiectasis, lung cancer, and obstructive sleep apnea), cardiovascular diseases, and anxiety, similar to previous studies.11 Taken together, previous and our studies show that pulmonary comorbidities are quite prevalent in COPD, requiring further concern.
In this study, we compared the clinical features between patients with high- and low-risk comorbidities based on COTE index. The results showed that patients with high-risk comorbidity had worse obstructive ventilatory dysfunction, older age, and longer duration of COPD. They also had higher mMRC and CAT scores, a higher proportion of patients use SABA or SAMA or ICS, and a higher incidence of moderate-to-severe acute exacerbation and hospitalizations in the past year. Additionally, there was a higher proportion of group E patients based on ABE group. Huang YL and Uzunlar EA19,20 found higher frequency of hospital admission due to acute exacerbation, higher mMRC score and more courses of systemic corticosteroids in high-risk comorbidity group, similar to those studies, in our study, patients with high-risk comorbidity had a longer duration of chronic obstructive pulmonary disease and a higher risk of moderate-to-severe acute exacerbation. All of these showed that patients with high-risk comorbidity had more severe dyspnea symptoms, frequently use SABA or SAMA or ICS, and higher incidence of moderate-to-severe acute exacerbation and hospitalizations, which may also the reason for a higher proportion of patients use ICS. COTE index, which predicts the mortality risk associated with comorbidities in COPD, includes 12 diseases.4 Similar to Doğan’s research,10 our study showed that the risk classification of the COTE index score reflects the severity of the acute exacerbation and the load of symptoms. Asthma, bronchiectasis, lung cancer, OSA, cardiovascular disease, diabetes, gastric/duodenal ulcer, reflux esophagitis, anxiety and depression were more prevalent in high-risk comorbidity group. Additionally, they had higher frailty scores, higher level of BNP and HbA1c, and lower level of hemoglobin. Li L et al21 found that frailty may be a predictor of hospitalization due to acute exacerbations in COPD, and Li J et al22 showed that having more than two acute exacerbations in the past year is a risk factor for readmission in COPD patients with frailty. This suggested that the coexistence of multiple comorbidities adversely affects various aspects of patient function and health status, potentially contributing to the severity of symptoms and the increased risk of acute exacerbation in COPD.
We showed that COTE index score was positively correlated with the level of BNP and HbA1c, and negatively correlated with the level of hemoglobin, indicating that higher COTE index scores are associated with the increased risks of heart failure, poor blood glucose control in diabetes and anemia. COTE index score was positively correlated with age, the number of hospitalizations due to acute exacerbation and moderate-to-severe acute exacerbation events, mMRC, CAT and BMI, while it was negatively correlated with FEV1, FEV1%/pred, FEV1/FVC, MEF75/25%. A study about COPD23 found that patients who had greater change in hemoglobin concentration were more likely to be hospitalized for COPD comorbidities and experienced higher rates of morbidity and mortality due to COPD-related complications. It suggested that assessment of hemoglobin was important for early detection and prevention of complication related to COPD for leading a healthy life. Our study found that in the high-risk comorbidity group, hemoglobin levels were lower, but there were no correlation between hemoglobin levels and hospitalization due to acute exacerbation. The high level of BNP also indicates more severe heart failure. Brassington K et al24 revealed that more than half of COPD patients were hospitalized and died from combined with cardiovascular diseases, they also indicated that acute exacerbation to hospitalization was more common in COPD with heart failure. The high level of HbA1c in high-risk comorbidity group may be due to more severe diabetes complications and poor blood glucose control, potentially related to the coexistence of COPD with diabetes, coronary heart disease, OSA and obesity.25–27 Other studies have shown that COPD with diabetes have a higher risk of acute exacerbation and mortality.28 All of those studies and our study suggested that early intervention for abnormal laboratory tests could help reduce the risk of acute exacerbation of comorbidities in COPD.
Our study also discovered that the number of moderate-to-severe acute exacerbation events and hospitalizations due to acute exacerbation were significantly positively correlated with the COTE index score, mMRC and CAT score, while negatively correlated with FEV1% and FEV1/FVC. This indicates that the COTE index score, mMRC, CAT, FEV1% and FEV1/FVC may be used as predictors for moderate-to-severe acute exacerbation and hospitalizations in COPD with comorbidities. Our additional analysis of risk factors for moderate-to-severe acute exacerbation in COPD with comorbidities revealed that females were the protective factors, high FEV1/FVC can reflect the severity of COPD, whereas having history of asthma, lung cancer, diabetes, high mMRC and CAT scores, high NE% and low albumin levels were risk factors. The incidence of lung cancer, asthma, bronchiectasis, high CAT score and high COTE index score were found to be risk factors for hospitalizations resulting from acute exacerbation in COPD with comorbidities. The presence of pulmonary comorbidities in COPD significantly increases the risk of moderate-to-severe acute exacerbation and hospitalizations. In accordance with our study, previous studies29–32 have demonstrated that comorbidities such as asthma, lung cancer, gastroesophageal reflux disease, depression, heart failure and cerebrovascular diseases increase the risk of acute exacerbations in COPD.
Both GOLD 2024 and Global Strategy for Asthma Management and Prevention (GINA) 2024 emphasize that COPD and asthma are distinct diseases, and asthma should be included in the management of COPD comorbidities, as they may share some common treatable traits and clinical features.1,33 Jeong SH et al34 found that asthma is a risk factor for more frequent acute exacerbations within one year in COPD with comorbidities. Similar to asthma, previous studies on pulmonary comorbidities in COPD have often focused on one of comorbidities such as bronchiectasis35,36 or lung cancer37 or OSA,6 while there is quite little knowledge available on the characteristics of COPD comorbidities that include the coexistence of COPD with these pulmonary comorbidities. Our research also showed that a high prevalence of pulmonary comorbidities was present in COPD, asthma for 23.23%, bronchiectasis for 19.82%, lung cancer for 10.71%, and OSA for 7.50%. According to an analysis of clinical characteristics between pulmonary and extrapulmonary comorbidities in COPD, the pulmonary comorbidities group had higher mMRC and CAT score, a higher percentage of patients with more than two times moderate-to-severe acute exacerbations in the past year, and a higher proportion in E group based on ABE group. Previous studies38 have showed that COPD with asthma may have more symptoms, worse quality of life, more exacerbations of disease and higher healthcare utilization rates, moderate-to-severe COPD with bronchiectasis was linked to an increased risk of all-cause death and patients with bronchiectasis also experience acute exacerbations more frequently, female were also more likely to die from asthma and OSA,6 all suggesting that COPD with pulmonary comorbidities have worse quality of life, higher mortality risks, more frequent acute exacerbation events, more severe clinical symptoms and higher healthcare expenses. Our laboratory data analysis of the pulmonary comorbidities group revealed the level of peripheral blood EOS% and EOS were higher, high EOS levels were a risk factor for moderate-to-severe acute exacerbation in COPD. Similar to other studies,39 our research found eosinophilic airway inflammation existed in COPD with pulmonary comorbidities. However, we did not conduct further analysis to determine whether this phenomenon is solely related to the presence of asthma, but the effectiveness of targeted biological therapies may stem from this characteristic.40
Increased mortality and medical expenses linked to COPD are largely caused by acute exacerbations, especially moderate-to-severe exacerbations.41,42 How to exactly identify patients with high risk of acute exacerbations is still an outstanding question. Our study found that COTE index score over 5.5 is related to moderate-to-severe acute exacerbation and hospitalizations due to acute exacerbation in COPD, with AUC of 0.624 and 0.675, respectively. As previously shown, lower COTE index score, younger and lower frailty scores were found in COPD patients with pulmonary comorbidities. This suggests that COTE index to assess COPD with pulmonary comorbidities may be insufficient, because it only includes lung cancer and pulmonary fibrosis. The AUCs for the number of pulmonary comorbidities in predicting moderate-to-severe acute exacerbation and hospitalizations due to acute exacerbations were 0.607 and 0.651, respectively, which indicates that the number of pulmonary comorbidities do not have good predictive value. However, we showed that the AUCs for COTE index score in combination with the number of pulmonary comorbidities in predicting moderate-to-severe acute exacerbation and hospitalizations due to acute exacerbations were 0.667 and 0.740, respectively. This indicates that COTE index score combined with the number of pulmonary comorbidities in COPD has a better predictive ability. Taken together, we concluded that COTE, the number of pulmonary comorbidities or both is not the perfect prediction indicator, only as potential indication of moderate-to-severe acute exacerbations of COPD and hospitalization due to acute exacerbations.
We further constructed clinical prediction models and produced Nomogram were the best models for predicting moderate-to-severe acute exacerbation and hospitalization. By using internal validation, it was found that the AUC of the training and validation sets for the two models were over 0.9. The prediction curves of the two models were well fitted to the ideal curves and both showed good accuracy. The evaluation of its clinical application effect by DCA showed that this model has a good clinical application effect for predicting moderate-severe acute exacerbation events and can be used as a clinical assessment tool. In particular, the Nomogram of the prediction model can predict the moderate-to-severe acute exacerbation events in COPD patients, the Nomogram score is used to calculate the risk probability, and interventions that manage comorbidities and symptoms may reduce the risk of acute exacerbation.
We further conducted age-based subgroup analysis. In moderate-to-severe acute exacerbation and hospitalization in COPD, we found a higher incidence of pulmonary comorbidities but a reduced risk of COTE-risk in the subgroup aged <65 years. Classification by age may reduce the risk of acute exacerbation and hospitalization. Pulmonary comorbidities in COPD are not limited to lung cancer, comorbidities such as asthma, bronchiectasis and OSA also increase the risk of acute exacerbation and hospitalizations, necessitating integrated management alongside COPD.
This study has some limitations. First, being a retrospective study, it may have incomplete patient medical records, which could affect the results. Second, the sample size is not sufficient, and future studies should aim to increase the sample size and extend follow-up periods to better explore the impact of COTE index score and pulmonary comorbidities on COPD. Finally, our prediction model lacks external validation. This will be needed in the future to determine whether the Nomogram have clinical utility. Despite with these limitations, our study still has the power to illustrate COTE and pulmonary comorbidities can predict the risk of moderate-to-severe acute exacerbation in COPD.
Conclusion
In summary, pulmonary comorbidities in COPD are high and contribute to a higher risk of acute exacerbation and hospitalization. COTE index score combined with pulmonary comorbidities and other indicators can predict the risk of moderate-to-severe acute exacerbation and hospitalization due to acute exacerbations in COPD.
Data Sharing Statement
All available data are presented in the manuscript, and no additional data will be provided. Data are not available to be shared.
Ethics Approval and Consent to Participate
This study was followed with the Helsinki Declaration and was approved by the Ethics Review Committee of Beijing Tongren Hospital, Capital Medical University. Due to the retrospective nature of the study, informed consent was waived. All methods were performed in accordance with institutional and national guidelines and regulations.
Acknowledgments
Qinglin Chen and Xinmao Wang are co-first authors for this study. This research was supported by the Department of Respiratory and Critical Care Medicine, Beijing Tongren Hospital, Capital Medical University, Beijing, China.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by a grant from Beijing Natural Science Foundation (No.7212018).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease 2024 report [EB/OL]. (2023-11-13)[2024-12-18]. Available from: https://goldcopd.org/2024-gold-report/.
2. Momtazmanesh S, Moghaddam SS, Ghamari S-H, GBD 2019 Chronic Respiratory Diseases Collaborators. Global burden of chronic respiratory diseases and risk factors, 1990-2019: an update from the global burden of disease study 2019. EClinicalMedicine. 2023;59:101936. doi:10.1016/j.eclinm.2023.101936
3. WHO. Multimorbidity. Geneva: world health organization. 2016. Available from: http://apps.who.int/iris/handle/10665/252275.
4. Divo M, Cote C, de Torres JP, et al. Comorbidities and risk of mortality in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2012;186:155–161. doi:10.1164/rccm.201201-0034OC
5. Calverley PMA, Walker PP. Contemporary concise review 2022: chronic obstructive pulmonary disease. Respirology. 2023;28:428–436. doi:10.1111/resp.14489
6. Trudzinski FC, Jörres RA, Alter P, et al. Sex-specific associations of comorbidome and pulmorbidome with mortality in chronic obstructive pulmonary disease: results from COSYCONET. Sci Rep. 2022;12:8790–8800. doi:10.1038/s41598-022-12828-8
7. Chan MC, Lin CH, Kou YR. Hyperlipidemia in COPD is associated with decreased incidence of pneumonia and mortality: a nationwide health insurance data-based retrospective cohort study. Int J Chron Obstruct Pulmon Dis. 2016;11:1053–1059. doi:10.2147/COPD.S102708
8. Putcha N, Drummond MB, Wise RA, et al. Comorbidities and chronic obstructive pulmonary disease: prevalence, influence on outcomes, and management. Semin Respir Crit Care Med. 2015;36:575–591. doi:10.1055/s-0035-1556063
9. Chang HC, Liu SF. Impact of smoking cessation and Charlson comorbidity index on influenza vaccination efficacy in COPD patients. Microorganisms. 2024;12:1437–1446. doi:10.3390/microorganisms12071437
10. Doğan Mülazimoğlu D, Bilgin B, Ayöz S, et al. Reliability of comorbidity indices as predictive indicators for frequent severe chronic obstructive pulmonary disease exacerbations. Tuberk Toraks. 2024;72(1):16–24. doi:10.5578/tt.202401833
11. Fabbri LM, Celli BR, Agustí A, et al. COPD and multimorbidity: recognising and addressing a syndemic occurrence. Lancet Respir Med. 2023;11:1020–1034. doi:10.1016/S2213-2600(23)00261-8
12. He Z, Wang Y, Shan L, et al. Reflections on COPD comorbidities. Chin Med J. 2024;137:1504–1506. doi:10.1097/CM9.0000000000003131
13. Huang K, Zheng Z, Li W, et al. Sociodemographic correlates with prevalence of comorbidities in patients with chronic obstructive pulmonary disease: a study from a Chinese national survey. Lancet Reg Health West Pac. 2023;42:100937. doi:10.1016/j.lanwpc.2023.100937
14. Chronic Obstructive Pulmonary Disease Group of Chinese Thoracic Society. Chronic obstructive pulmonary disease committee of Chinese association of chest physician. Zhonghua Jie He He Hu Xi Za Zhi. 2021;44:170–205. doi:10.3760/cma.j.cn112147-20210109-00031
15. Cheung G, Patrick C, Sullivan G, et al. Sensitivity and specificity of the geriatric anxiety inventory and the hospital anxiety and depression scale in the detection of anxiety disorders in older people with chronic obstructive pulmonary disease. Int Psychogeriatr. 2012;24:128–136. doi:10.1017/S1041610211001426
16. Dias LS, Ferreira ACG, da Silva Junior JLR, et al. Prevalence of frailty and evaluation of associated variables among COPD patients. Int J Chron Obstruct Pulmon Dis. 2020;15:1349–1356. doi:10.2147/COPD.S250299
17. Stolz D, Mkorombindo T, Schumann DM, et al. Towards the elimination of chronic obstructive pulmonary disease: a lancet commission. Lancet. 2022;400:921–972. doi:10.1016/S0140-6736(22)01273-9
18. Agustí A, Noell G, Brugada J, et al. Lung function in early adulthood and health in later life: a transgenerational cohort analysis. Lancet Respir Med. 2017;5:935–945. doi:10.1016/S2213-2600(17)30434-4
19. Huang YL, Mao B, Mim J, et al. The associations between comorbidity and exacerbation risk in patients with chronic obstructive pulmonary disease. Zhonghua Jie He He Hu Xi Za Zhi. 2018;41:349–354. doi:10.3760/cma.j.issn.1001-0939.2018.05.009
20. Uzunlar EA, Yildiran H, Kokturk N, et al. Obesity, Charlson comorbidity index, and neutrophil-to-lymphocyte ratio in chronic obstructive pulmonary disease: relationship to disease severity. Bratisl Lek Listy. 2023;124:520–526. doi:10.4149/BLL_2023_080
21. Li L, Zhang L, Wang L, et al. Frailty and in-hospital mortality in older patients with acute exacerbation of COPD: a real-world prospective cohort study. Respir Med. 2024;228:107663. doi:10.1016/j.rmed.2024.107663
22. Li J, Ma X, Zeng X, et al. Risk factors of readmission within 90 days for chronic obstructive pulmonary disease patients with frailty and construction of an early warning model. Int J Chron Obstruct Pulmon Dis. 2023;18:975–984. doi:10.2147/COPD.S400638
23. Sharmin A, Nessa A, Yeasmin F, et al. Evaluation of hemoglobin concentration in male patients with chronic obstructive pulmonary disease. Mymensingh Med J. 2024;33:383–386.
24. Brassington K, Selemidis S, Bozinovski S, et al. New frontiers in the treatment of comorbid cardiovascular disease in chronic obstructive pulmonary disease. Clin Sci. 2019;133:885–904. doi:10.1042/CS20180316
25. Voulgaris A, Archontogeorgis K, Pataka A, et al. Burden of comorbidities in patients with OSAS and COPD-OSAS overlap syndrome. Medicina. 2021;57:1201–1211. doi:10.3390/medicina57111201
26. Mitra AK, Bhuiyan AR, Jones EA. Association and risk factors for obstructive sleep apnea and cardiovascular diseases: a systematic review. Diseases. 2021;9:88–103. doi:10.3390/diseases9040088
27. Larsson SC, Burgess S. Causal role of high body mass index in multiple chronic diseases: a systematic review and meta-analysis of Mendelian randomization studies. BMC Med. 2021;19:320–330. doi:10.1186/s12916-021-02188-x
28. Castañ-Abad MT, Montserrat-Capdevila J, Godoy P, et al. Diabetes as a risk factor for severe exacerbation and death in patients with COPD: a prospective cohort study. Eur J Public Health. 2020;30:822–827. doi:10.1093/eurpub/ckz219
29. Westerik JA, Metting EI, van Boven JF, et al. Associations between chronic comorbidity and exacerbation risk in primary care patients with COPD. Respir Res. 2017;18:31–48. doi:10.1186/s12931-017-0512-2
30. Çolak Y. Cardiac disease from accelerated FEV1 decline and acute exacerbations: time to rethink comorbidities in COPD. Eur Respir J. 2021;57:2004008. doi:10.1183/13993003.04008-2020
31. Donaldson GC, Hurst JR, Smith CJ, et al. Increased risk of myocardial infarction and stroke following exacerbation of COPD. Chest. 2010;137:1091–1097. doi:10.1378/chest.09-2029
32. Hurst JR, Vestbo J, Anzueto A, et al. Susceptibility to exacerbation in chronic obstructive pulmonary disease. N Engl J Med. 2010;363:1128–1138. doi:10.1056/NEJMoa0909883
33. Global strategy for asthma management and prevention 2024 report [EB/OL]. (2024-10-1)[2024-3-22]. Available from: https://ginasthma.org/2024-report/.
34. Jeong SH, Lee H, Carriere KC, et al. Comorbidity as a contributor to frequent severe acute exacerbation in COPD patients. Int J Chron Obstruct Pulmon Dis. 2016;11:1857–1865. doi:10.2147/COPD.S103063
35. Martinez-Garcia MA, Miravitlles M. Bronchiectasis in COPD patients: more than a comorbidity? Int J Chron Obstruct Pulmon Dis. 2017;12:1401–1411. doi:10.2147/COPD.S132961
36. Kawamatawong T, Onnipa J, Suwatanapongched T. Relationship between the presence of bronchiectasis and acute exacerbation in Thai COPD patients. Int J Chron Obstruct Pulmon Dis. 2018;13:761–769. doi:10.2147/COPD.S139776
37. Hernandez D, Cheng CY, Hernandez-Villafuerte K, et al. Survival and comorbidities in lung cancer patients: evidence from administrative claims data in Germany. Oncol Res. 2023;30:173–185. doi:10.32604/or.2022.027262
38. Negewo NA, Gibson PG, McDonald VM. COPD and its comorbidities: impact, measurement and mechanisms. Respirology. 2015;20:1160–1171. doi:10.1111/resp.12642
39. Mathioudakis AG, Janssens W, Sivapalan P, et al. Acute exacerbations of chronic obstructive pulmonary disease: in search of diagnostic biomarkers and treatable traits. Thorax. 2020;75:520–527. doi:10.1136/thoraxjnl-2019-214484
40. Bhatt SP, Rabe KF, Hanania NA, et al. Dupilumab for COPD with blood eosinophil evidence of type 2 inflammation. N Engl J Med. 2024;390:2274–2283. doi:10.1056/NEJMoa2401304
41. Vogelmeier CF, Román-Rodríguez M, Singh D, et al. Goals of COPD treatment: focus on symptoms and exacerbations. Respir Med. 2020;166:105938. doi:10.1016/j.rmed.2020.105938
42. Hurst JR. Precision medicine in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2016;193:593–594. doi:10.1164/rccm.201601-0104ED
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comorbid Heart Disease in Patients with COPD is Associated with Increased Hospitalization and Mortality – A 15-Year Follow-Up
Giezeman M, Sundh J, Athlin Å, Lisspers K, Ställberg B, Janson C, Montgomery S, Kisiel MA, Nager A, Sandelowsky H, Hasselgren M
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:11-21
Published Date: 9 January 2023
U-Shaped Relationship Between Serum Lactate Dehydrogenase with All-Cause Mortality in Patients with Chronic Obstructive Pulmonary Disease
Huang L, Lu Z, Zhou X, He L, You X, Chen C, Zou C
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:305-316
Published Date: 15 March 2023
Characteristics of Inhaler Technique in COPD Patients in a Specialized Center in Armenia, Colombia: A Cross-Sectional Study
Montes Cardona JA, Hincapié Erira DA, Nati-Castillo HA, Sánchez-Vallejo J, Izquierdo-Condoy JS
Patient Preference and Adherence 2023, 17:2025-2038
Published Date: 16 August 2023
Adherence to Inhalation Devices in Patients with Chronic Obstructive Pulmonary Disease
Valladales-Restrepo LF, Oyuela-Gutiérrez MC, Delgado-Araujo AC, Calvo-Salazar J, Osorio-Bustamante D, Lerma-Barco CE, Machado-Alba JE
Patient Preference and Adherence 2023, 17:3233-3244
Published Date: 8 December 2023
Multifactorial Determinants of Refractory Breathlessness in COPD: Development of the Refractory Breathlessness Score for Risk Stratification
Lee HW, Lee HJ, Park H, Heo EY, Lee CH, Kim DK, Lee JK
International Journal of Chronic Obstructive Pulmonary Disease 2026, 21:601086
Published Date: 8 July 2026