Back to Journals » ClinicoEconomics and Outcomes Research » Volume 18
Model-Based Cost-Effectiveness Analysis of Routine Omega-3 Testing and Targeted Supplementation to Reduce Early Preterm Birth in Australia Compared with Current Practice
Authors Haji Ali Afzali H, Linedale E ![]() , Martin C, Ahmed M, Quinlivan J, McPhee AJ, Coates P, Semmler L, Cox D
, Martin C, Ahmed M, Quinlivan J, McPhee AJ, Coates P, Semmler L, Cox D ![]() , Gibson RA, Makrides M, Best KP
, Gibson RA, Makrides M, Best KP
Received 4 December 2025
Accepted for publication 12 May 2026
Published 26 May 2026 Volume 2026:18 585692
DOI https://doi.org/10.2147/CEOR.S585692
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Samer Hamidi
Hossein Haji Ali Afzali,1 Ecushla Linedale,1– 3 Craig Martin,4 Muktar Ahmed,1 Julie Quinlivan,5 Andrew J McPhee,2 Penelope Coates,6 Lucas Semmler,7 David Cox,8 Robert Alan Gibson,2,9 Maria Makrides,2,10,* Karen P Best2,10,*
1School of Public Health, Adelaide University, Adelaide, Australia; 2SAHMRI Women and Kids, South Australian Health and Medical Research Institute, Adelaide, SA, Australia; 3College of Nursing and Health Sciences, Flinders University, Adelaide, Australia; 4Commission on Excellence and Innovation in Health, Adelaide, SA, Australia; 5Institute for Health Research, University of Notre Dame Australia, Fremantle, Western Australia; 6Chemical Pathology, SA Pathology, Adelaide, Australia; 7Public Pathology Australia Incorporated, St Ives, NSW, Australia; 8Genetics and Molecular Pathology, SA Pathology, Adelaide, Australia; 9School of Agriculture, Food and Wine, University of Adelaide, Waite Campus, Glen Osmond, SA, Australia; 10Adelaide Medical School, Faculty of Health and Medical Sciences, University of Adelaide, Adelaide, Australia
*These authors contributed equally to this work
Correspondence: Karen P Best, SAHMRI Women & Kids, South Australian Health and Medical Research Institute, 72 King William Road, North Adelaide, SA, 5006, Australia, Tel +61 8 81284044, Email [email protected]
Background: Preterm birth remains a leading cause of newborn death, disability, and long-term health challenges globally, with a substantial impact on families, the health system, and society. Omega-3 supplementation in women with low omega-3 status in early pregnancy has been shown to reduce the risk of preterm birth, particularly early preterm birth (< 34 weeks of gestation). The cost implications of incorporating omega-3 testing and targeted supplementation into routine antenatal care to reduce early preterm birth in Australia are unclear.
Methods: A decision analytic model was developed using Australian epidemiological, clinical, and cost data to compare routine omega-3 testing and targeted supplementation with current practice. The model predicted the number of early preterm births prevented and associated cost savings over an 18-year time horizon. Deterministic sensitivity analyses were conducted to examine uncertainty in key model inputs.
Results: Among 289,195 singleton pregnancies in 2022, an estimated 17.5% of women would have low omega-3 status and be eligible for supplementation. Making conservative assumptions, the model predicted that, relative to current practice, omega-3 testing and supplementation would be a dominant strategy, preventing 640 early preterm births, with projected savings of $26.1 million in direct healthcare costs. Sensitivity analyses indicated that the results were robust across most scenarios and identified the treatment effect estimate as the strongest driver of model predictions.
Conclusion: Omega-3 testing in early pregnancy with targeted supplementation may offer a scalable and cost-effective strategy to reduce early preterm birth with potential benefits for mothers, infants, and the health system. The modelling suggests meaningful health and economic benefits. Cost savings were robust across most plausible scenarios, supporting the potential value of this approach on a national scale.
Plain Language Summary: Every year, thousands of babies in Australia are born too early, putting them at risk of serious health problems and placing a heavy burden on families and the health system. Babies born before 34 weeks of pregnancy face the greatest risks of death, intensive care, long hospital stays, and lifelong challenges.
Evidence shows that omega-3 supplementation lowers the risk of preterm birth for women with low omega-3 levels, and this recommendation was included in Australia’s National Pregnancy Care Guidelines. We assessed whether introducing a simple omega-3 blood test and offering high-dose supplements to women with low levels, as part of routine pregnancy care, would be cost-effective.
Using Australian data, we built a model to compare this approach with current care. Under conservative assumptions, the model predicted that testing and targeted supplementation could prevent about 640 births before 34 weeks of gestation each year and save $26 million in direct healthcare costs and $44.7 million overall. For every dollar invested, the health system could save $1.67 in direct costs and $3.00 in total costs.
Adding omega-3 testing with targeted supplementation to routine pregnancy care has the potential to improve outcomes for mothers and babies while reducing healthcare costs substantially. This is an affordable, evidence-based change that could deliver significant benefits nationwide.
Keywords: cost-effectiveness, health economics, antenatal screening, preterm birth prevention, omega-3 supplementation, maternal nutrition, pregnancy care
Introduction
Preterm birth, defined as birth before 37 weeks of pregnancy, is a major cause of death in children under five and a major contributor to long-term disability and healthcare costs worldwide.1,2 In 2020, an estimated 13.4 million babies were born preterm globally, underscoring its continuing public health significance.1 Globally, it ranks fourth among all causes of lifetime health and productivity loss, exceeding the burden of chronic diseases such as chronic obstructive pulmonary disease, diabetes, and stroke.3
In Australia, preterm birth has been recognised as a key priority for national action and investment and imposes a substantial economic and service burden on the health and education systems.4,5 In 2022, the Australian Institute of Health and Welfare (AIHW) reported around 25,000 babies born preterm.6 The total cost to government for a single year of preterm births in Australia has been estimated at AUD 1.41 billion, much of which (67%) is direct healthcare costs (largely driven by neonatal care) followed by costs associated with special education services (24%).4 Babies born before 34 weeks of gestation are classified as “early preterm” and face substantially greater risks of both immediate and lifelong adverse outcomes.7–9 These include impaired growth and neurodevelopment, intellectual disabilities, mental health conditions, and earlier onset of chronic diseases,3 imposing a heavy economic burden on health, education and social support systems.4 The toll on families in terms of emotional distress, financial strain, disrupted employment, long-term caregiving responsibilities and parental mental health issues is also considerable.3 Studies have shown an inverse relationship between gestation age at delivery, costs and health outcomes.7–9 This highlights the importance of strategies that prevent early preterm birth and reduce its associated long-term costs and harms.
A secondary analysis of the ORIP (Omega-3 to Reduce the Incidence of Prematurity) randomised controlled trial showed that omega-3 long-chain polyunsaturated fatty acid (LCPUFA) supplementation reduced the risk of early preterm birth (<34 weeks’ gestation) by 77%, with significantly greater benefit observed in women with low or depleted omega-3 levels in early pregnancy.10–12 This is consistent with the broader evidence base, including the 2018 Cochrane review, which found reductions in preterm and early preterm birth with omega-3 supplementation during pregnancy overall,10 and subsequent international trials that suggested greater benefit among women with lower baseline omega-3 intake or status.13,14 The National Australian Pregnancy Care Guidelines15 reflected this evidence and recommended omega-3 LCPUFA supplementation with 800 mg docosahexaenoic acid (DHA) and 100 mg eicosapentaenoic acid (EPA) daily in women with low omega-3 status to reduce the risk of preterm birth.
The Omega-3 Test and Treat Program was developed and embedded into routine antenatal care in South Australia (SA) as a practical, low-cost mechanism to translate this guideline into practice.16 The program leverages existing workflows within SA Pathology, South Australia’s public pathology provider, via the SA Maternal Serum Antenatal Screening (SAMSAS) program to embed omega-3 testing and tailored supplementation advice into standard maternity care pathways. Blood testing is considered the gold standard for identifying at-risk women as omega-3 levels cannot be reliably estimated from dietary intake alone.17,18
Outside South Australia, routine omega-3 testing and targeted supplementation advice are not currently implemented. Some women may choose to use prenatal supplements containing relatively low doses of omega-3, but this differs from the targeted therapeutic supplementation strategy evaluated in this study.
While early implementation of the Omega-3 Test and Treat Program in South Australia has demonstrated feasibility, reach, and strong fidelity,16 evidence on the economic value of this approach is currently lacking. This study aims to generate new evidence on the economic impact of omega-3 testing and supplementation on early preterm birth in Australia when compared with current practice.
Materials and Methods
Overview
A decision analytic model was developed to predict incremental costs of omega-3 testing and supplementation if implemented nationally and the potential cost savings due to its impact on early preterm birth rates, when compared with current practice. The cohort entering the model includes live early preterm births (defined as <34 weeks of gestation) stratified by the gestational age at delivery ie, extremely preterm (20–27 weeks), moderately preterm (28–31 weeks) and late preterm (32–33 weeks). We used the best available evidence from Australian national figures and published literature to populate the model. Expert opinion was sought where the required data was unavailable from the review or national databases. The model schematic diagram is presented in Figure 1, which represents a decision tree structure comparing the impact of alternative interventions on cost estimates associated with birth outcomes (term and early preterm) until 18 years of age. The model was developed using Microsoft Excel.
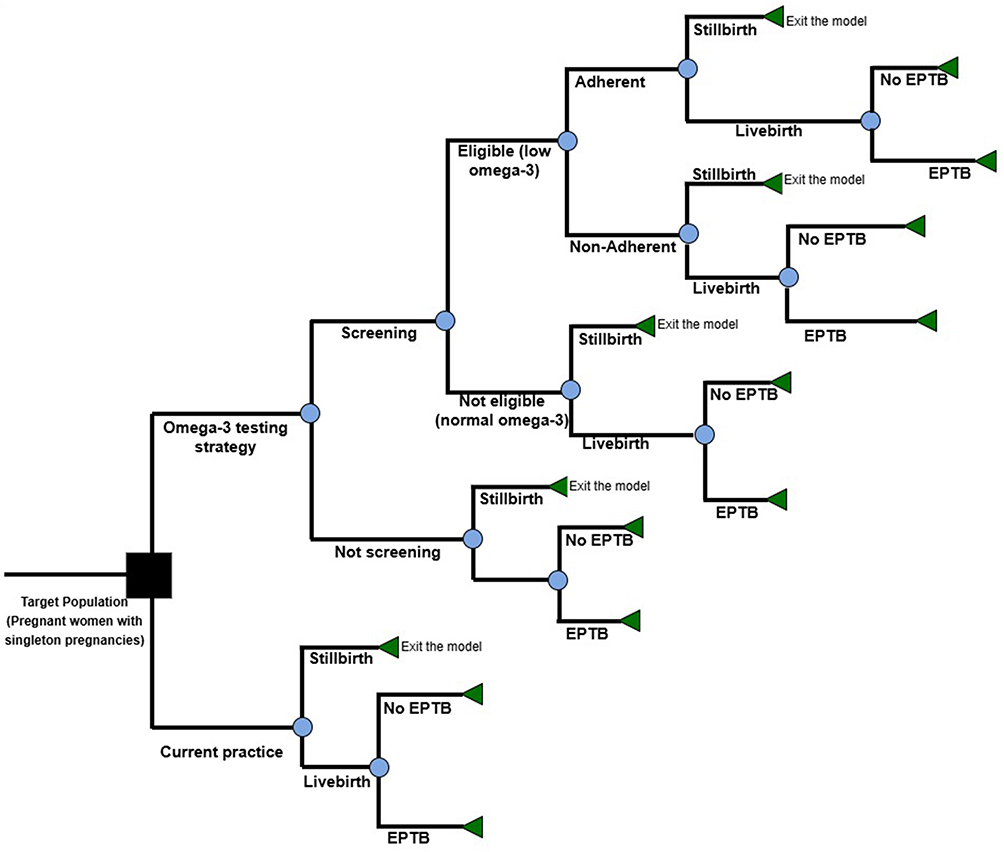 |
Figure 1 Schematic diagram of the model structure. Abbreviations: EPTB, early preterm birth; RR, relative risk. Notes: The model compares current practice with a strategy of omega-3 testing followed by targeted supplementation in eligible women. The model cohort includes 289,195 singleton pregnancies in Australia. Pathways include screening uptake (80%), eligibility based on low omega-3 status (17.5%), supplementation adherence (65%), and treatment effect (relative risk [RR] = 0.23). Blue circles represent decision nodes, while green triangles represent terminal nodes. Final outcomes are early preterm birth (EPTB; <34 weeks) or no EPTB. Costs are assigned based on gestational age at delivery and accumulated over a time horizon from birth to 18 years. |
Model Inputs
Key model inputs with their base case values, their ranges, and sources are presented in Supplementary Table 1.
Epidemiological and Clinical Data
The 2022 cohort of 289,195 pregnant women with a singleton pregnancy in Australia was used as our reference population for all estimates (the most recent year with complete national data at the inception of the study).6 Consistent with our data source for clinical effectiveness,12 the model was restricted to singleton pregnancies resulting in live births; therefore, multiple births, foetal loss, and stillbirth were not included in the analysis. According to data from AIHW,6 there were 5752 live early preterm births defined as delivery before 34 weeks of gestation, representing approximately 25% of all preterm births (<37 weeks of gestation).4
Data from SAMSAS indicates that approximately 80% of pregnant women participate in their early pregnancy screening program in South Australia. Verified by experts, we used an 80% screening uptake rate among pregnant women in our base case analysis, assuming that SAMSAS can be used for omega-3 status testing to identify eligible women.
Data to estimate the number of eligible pregnant women (with low blood omega-3 levels before 20 weeks’ gestation) and omega-3 supplementation adherence were derived from a national Australian randomised controlled trial (ORIP),11,12 showing that 17.5% of pregnant women are eligible for supplementation and 65% of treated women adhere to the supplement regimen.
Estimates of effectiveness were sourced from a secondary analysis of the ORIP trial showing that, among women with low omega-3 status (<4.1% of total fatty acids in whole blood) and a singleton pregnancy, supplementation reduced the risk of early preterm birth by 77% compared with control (Relative risk = 0.23, 95% CI: 0.07–0.79).12 The analysis also showed that 3.16% of pregnancies in the control group resulted in early preterm birth.
Cost Data
Considering data availability, we included cost items (mainly from birth to 18 years of age), capturing important costs to the government (both health system and wider government costs such as education), and costs to the family.
Cost estimates were primarily derived from Newnham et al4 who estimated the discounted health and education costs associated with preterm birth up to age 18 in Australia, stratified by gestational age at delivery: extremely preterm (20–27 weeks), moderately preterm (28–31 weeks) and late preterm (32–36 weeks), noting that early preterm birth in our analysis is defined as <34 weeks of gestation. All cost estimates were adjusted to 2022 Australian dollars using the health care related Consumer Price Index (CPI).19
We included the following cost items in our analysis to capture incremental costs:
- Intervention costs: These include omega-3 status testing for pregnant women (before 20 weeks of gestation) to identify eligible women followed by omega-3 supplementation administered from 20 weeks gestation until delivery for women identified as omega-3 deficient, with adherence incorporated into the model when estimating intervention effectiveness and costs. Sourced from SA Pathology (South Australia’s state-wide, public pathology service), we included an estimated cost of $50 per pregnant woman for testing, reflecting the approximate laboratory processing cost for the blood test within the existing antenatal screening infrastructure.20 The cost of supplementation was estimated at $100 per pregnant woman based on current market prices for omega-3 supplements.
- Birth and neonatal admissions costs.
- Hospitalisation costs (ages 1–5, 6–12, and 13–18).
- Out of hospital costs, eg, doctor visits, imaging services, pathology tests, and government subsidised pharmaceuticals (ages 0–4 and 5–9).
- Education costs including primary and high school special support needs for preterm infants.
- Out of pocket costs associated with accessing health services having a preterm birth.21
- Valuation of mothers’ income losses (representing indirect costs associated with time away from work following preterm birth).21
Data Analysis
In line with recommendations made by national funding bodies in Australia,22 our main analysis was undertaken from the perspective of government-funded health system which included direct healthcare costs. Taking a broader perspective, a further analysis included total costs (direct costs, educational costs, costs to the family, and indirect cost captured by maternal wage loss).
To estimate potential cost savings associated with reduction in early preterm birth, first we estimated mean excess costs attributable to prematurity (early preterm, stratified by the gestational age at delivery). Given estimates of effectiveness of omega-3 testing and supplementation, we estimated the number of early preterm births which can be prevented as the product of screening coverage, adherence rate, and effect size in the cohort of eligible women.
In the absence of gestational age-specific treatment effect data, our analysis assumed similar treatment effects in eligible women, regardless of gestational age at delivery. Including the intervention costs as induced costs, we calculated net direct and total cost savings. If no dominant scenario, the cost-effectiveness was assessed via the incremental cost-effectiveness ratio (ICER).
Deterministic sensitivity analyses around key model inputs were conducted to quantify the impact of variables on predictions of both main analysis (ie, direct healthcare costs) and additional analyses representing a broader perspective (ie, total costs). This included varying the following inputs over their plausible upper and lower estimates: (i) Relative risk; (ii) Screening coverage; (iii) Adherence rate; (iv) Testing cost; (v) Supplement cost; and (vi) Neonatal admission costs stratified by the gestational age at delivery (the largest share of direct costs). An additional two-way sensitivity analysis was conducted to explore the impact of a higher adherence rate (90%) (assuming that national implementation can increase public awareness, which can influence treatment adherence) and a higher relative risk (0.90) representing a more conservative assumption (given limitations associated with the secondary analysis of the ORIP trial). Results from sensitivity analyses were presented as a tornado diagram. Threshold analyses were also performed to determine the critical values of influential inputs where the model remains cost neutral. As the main cost items (age range aggregated data) derived from published literature4 were discounted in the primary analysis, no discounting was applied.
Face validity of all model inputs (base case estimates and their ranges for sensitivity analysis), assumptions, and model predictions were assessed through presentation to an expert panel.
Results
The model estimated the potential impact of omega-3 testing and supplementation, if implemented nationally, on early preterm births and associated costs compared with current practice in Australia.
Base Case Analysis
Table 1 presents the results of the base case analysis. Among the cohort of 289,195 women with a singleton pregnancy, 50,609 women (17.5%) would be omega-3 depleted and hence eligible for omega-3 supplementation.
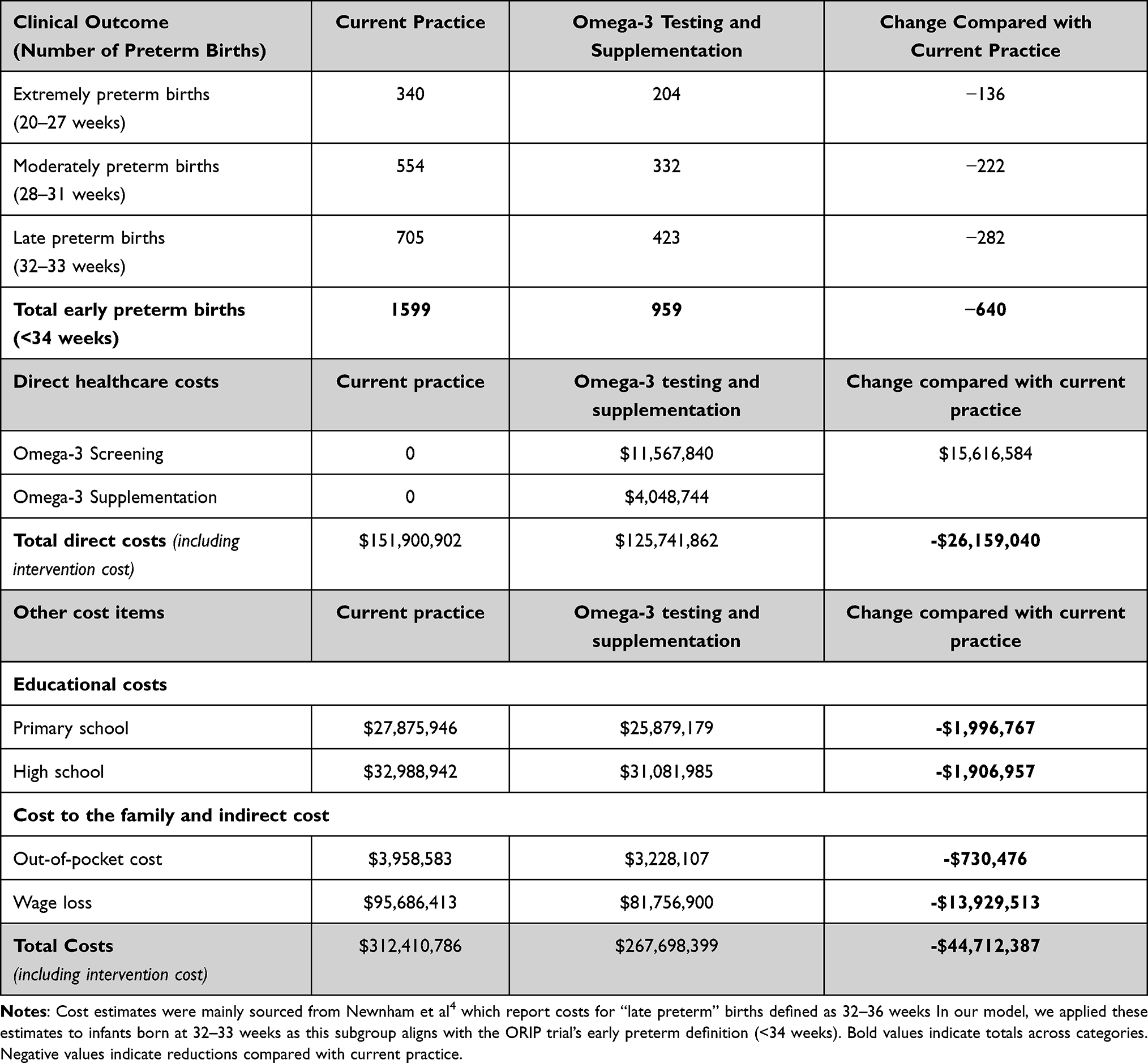 |
Table 1 Base-Case Results Comparing Current Practice with Omega-3 Testing and Supplementation |
In the current practice scenario, the model predicts that 1599 early preterm births are likely to occur with a total direct cost of $151.9 million and a total cost of $312.4 million (with direct costs representing 49% of the total). In terms of the distribution of direct costs, the total cost for extremely preterm infants (20–27 weeks) was over 2 times the cost of late preterm infants (32–33 weeks).
In the omega-3 testing and supplementation scenario, the model predicts that 959 early preterm births are likely to occur, resulting in an estimated prevention of 640 early preterm births (Table 1). Compared with previous approaches that have primarily focused on direct healthcare costs, our model incorporates both screening and supplementation pathways, includes adherence and coverage assumption, and extends the analysis to a broader societal perspective.
The total cost of the intervention (including testing and supplementation) is estimated at $15.6 million. Our base case analysis shows omega-3 testing and supplementation is a dominant strategy under the model assumptions (more effective and less costly) compared with current practice, saving more than $26.1 million and $44.7 million in direct costs and total costs, respectively. For every dollar invested in omega-3 testing and supplementation about $1.67 in direct costs and $3 in total costs related to prematurity can be saved. A structured comparison with prior approaches is presented in Supplementary Table 2.
Sensitivity Analyses
Table 2 presents the results of the sensitivity analyses in which one or more model inputs were varied. Omega-3 testing and supplementation remained a dominant strategy compared with current practice in most analyses, except when the assumed effect size was varied.
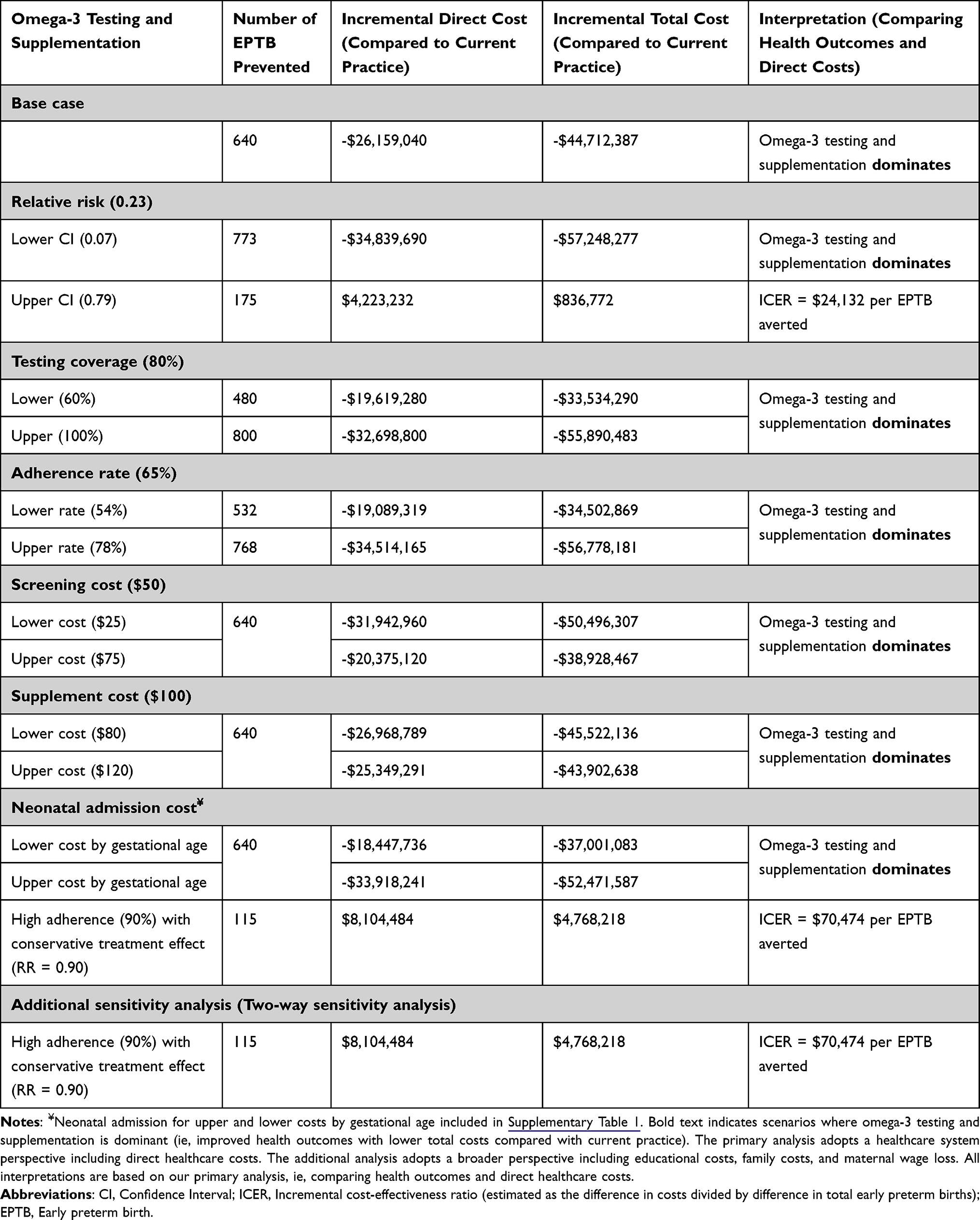 |
Table 2 Results of Deterministic Sensitivity Analyses |
When the upper confidence limit of the relative risk (0.79; ie, 21% relative reduction) was applied, the cost savings observed in the base case were reversed, resulting in an incremental cost of $4,223,232 million in total direct healthcare costs. In this scenario, the intervention was more effective, preventing an estimated 175 early preterm births, but also more costly than current practice. This translates to an incremental cost-effectiveness ratio (ICER) of $24,132 per early preterm birth prevented ($4,223,232/175), meaning an additional $24,132 would need to be spent to prevent one additional early preterm birth. In contrast, applying the lower confidence limit for the relative risk (0.07), corresponding to a 93% relative reduction in early preterm births, would result in 773 early preterm births prevented generating total direct cost savings of $34.8 million, the largest savings. An additional two-way sensitivity analysis using a higher adherence rate (90%) and a higher relative risk (0.90) found that the proposed intervention is more expensive than current practice, preventing 115 early preterm births (ICER = $70,474 per early preterm birth prevented).
Figure 2 (tornado diagram) presents the results of the main deterministic sensitivity analyses, ordered by the size of their impact on total direct cost estimates. The analysis identified the relative risk as the primary driver of the base case results. As the relative risk of early preterm birth increases (indicating a smaller estimated effect of omega-3 testing and supplementation), the associated cost savings diminish.
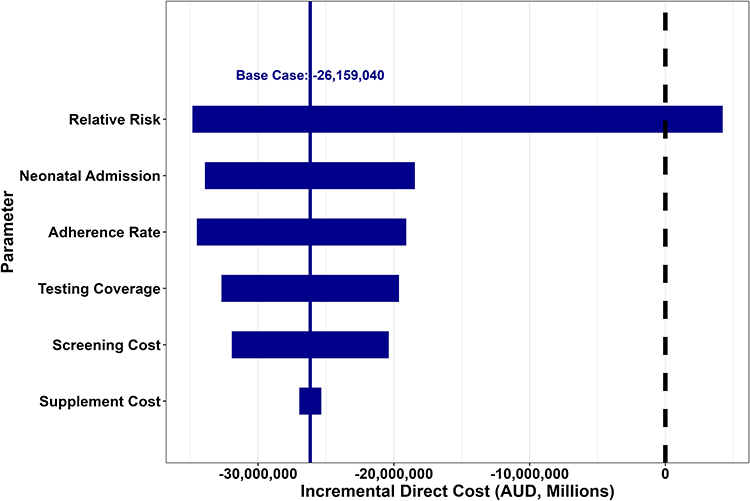 |
Figure 2 Tornado diagram showing results of the sensitivity analyses (Direct Costs). Notes: The tornado diagram ranks model inputs demonstrating the extent to which the base case result (direct costs) is sensitive to change in inputs. Solid line represents the base case results. (–$26,159,040). Bars extending to the left or right indicate the change in cost associated with the lower and upper values of each parameter. A dashed vertical line at zero indicates the value at which the intervention becomes cost neutral. |
The results of sensitivity analyses strongly indicate that the estimated treatment effect is the key driver of our model-based analysis. Given the importance of the relative risk, a threshold analysis was conducted to determine the value at which omega-3 testing and supplementation becomes cost-neutral (ie, incremental direct cost = $0) under varying the relative risk (Figure 3). The analysis shows that omega-3 testing and supplementation would remain cost-saving when the relative risk is below 0.7122 (ie, 28.78% reduction in early preterm birth). In Figure 2, the vertical dashed line marks this threshold of value, at which the incremental direct cost of the proposed intervention becomes zero (cost neutral).
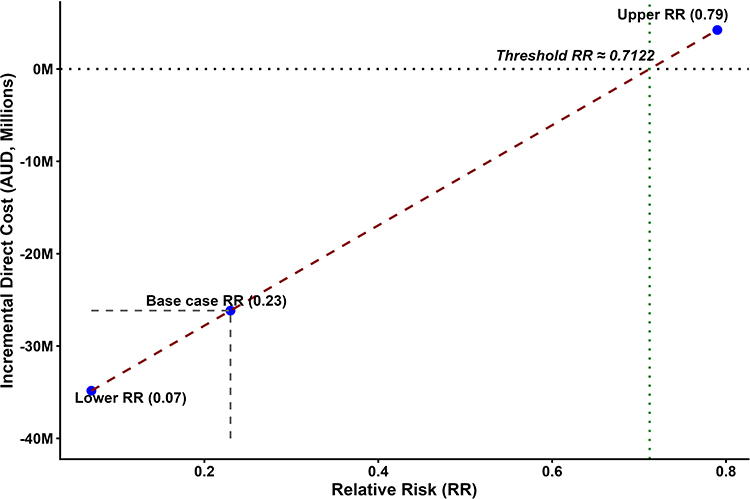 |
Figure 3 Threshold analysis: Relationship between relative risk and incremental direct costs. Abbreviation: RR, relative risk. Notes: The dashed red line shows the fitted linear relationship between relative risk (RR) and incremental direct costs. The lower (RR = 0.07), base case (RR = 0.23), and upper (RR = 0.79) estimates are plotted with labelled reference points. The partial grey dashed lines illustrate the base-case cost at RR = 0.23. The horizontal dotted line at zero marks the cost-neutral point. The vertical dotted green line indicates the threshold relative risk (RR ≈ 0.712), above which the intervention is no longer cost saving. |
Discussion
To our knowledge, this is the first cost-effectiveness analysis comparing omega-3 testing and supplementation with current practice in reducing preterm births globally. Making conservative assumptions, the analysis of the cohort of 289,195 pregnant women in 2022 in Australia showed that incorporating omega-3 testing and supplementation into routine antenatal care to reduce preterm birth represents an efficient use of resources within the health system. Our results indicated that omega-3 testing and supplementation is likely to be a dominant strategy, under the base-case assumption, improving health outcomes at a lower cost than current practice. The base case analysis predicted 640 early preterm births can be prevented, saving more than $26.1 million in direct healthcare costs and $44.7 million in total costs. A range of sensitivity analyses suggested that the results are robust to plausible variations in key input values, except for upper value of CI for relative risk which results in the prevention of 175 early preterm births with an additional direct cost of $4,223,232 million (ICER = $24,132 per early preterm birth prevented) ((ie, $4,223,232/175). This highlights that the economic results are strongly sensitive to the treatment effect estimate. A threshold analysis found that supplementation would be a cost saving option compared with current practice as long as it prevented 28% or more PTBs.
For illustrative purposes, it is possible to estimate crude figures for quality adjusted life year (QALY) gained from preventing preterm birth. Recent systematic reviews and meta-analyses of health utility values found preterm birth is associated with a mean utility decrement of 0.066 in comparison to birth at term. Using this conservative utility decrement and an 18-year time horizon (birth to 18 years of age, in line with the cost analysis), this implies a discounted QALY gain of 0.937 expected for the prevention of a preterm birth.22 Applying the QALY gain estimate to the total number of preterm births prevented in the base case analysis (640 × 0.937), omega-3 testing and supplementation can generate 600 additional QALYs. This finding indicates that, compared with current practice, omega-3 testing and supplementation would remain strongly cost-effective when using conservative estimates of QALY gains (ie, less costly and more effective in terms of QALY gained). Applying the above QALY gain estimate to the only sensitivity analysis scenario in the main analysis with no savings using upper bound of the relative risk confidence interval (Table 2) can generate 164 additional QALYs (0.937 × 175 EPTB prevented) resulting in an incremental (direct) cost per QALY gained (ICER) of $25,751 (ie, $4,223,232/164), which represents a cost-effective use of resources as it is lower than the willingness-to-pay threshold of $50,000 per QALY (the implicit threshold commonly used by national funding bodies in Australia).23 The ICER of AUD 25,751 also represents value for money when compared with the empirical estimate of the reference ICER in the Australian health system ($28,000 per QALY).24
Strengths, Limitations and Implications for Future Research
A key strength of this model is its conservative assumptions, which were intended to avoid overestimating the economic value of omega-3 testing and supplementation. Real-world implementation is likely to deliver even greater benefits, as both testing uptake and supplementation adherence are expected to be higher when embedded in routine antenatal care. In the ORIP trial, adherence may have been lower because participants were blinded to treatment allocation and to their omega-3 status, leaving them unaware of any potential personal benefit and reducing motivation to adhere to the supplementation regimen. Evidence from other antenatal interventions supports this expectation. For example, when cervical length screening to identify risk of preterm birth was integrated into routine mid-trimester ultrasound, uptake of screening increased substantially25 with the US opt-out program achieving 87.8% participation (95% CI, 86.3–88.9%).26 Given that blood tests are already a standard component of antenatal care in Australia, adding omega-3 testing to existing panels is similarly likely to achieve strong compliance.
Additionally, the model defines early preterm birth as occurring before 34 weeks of gestation, whereas cost estimates were drawn from Newnham et al4 who reported costs for births between 32 and 36 weeks. Although not fully matched, the stratification in our analysis represents a conservative approach, as the risk of complications (and hence healthcare utilisation) tends to increase with decreasing gestational age.
By incorporating mortality rates at each gestational age into the model, our analysis estimated ongoing costs for infants who survive, excluding intangible costs such as family psychological distress.
The model followed a time horizon from birth to 18 years of age; a longer time horizon could capture additional long-term complications and associated costs. Therefore, the true cost savings are likely greater than our projections.
In the sensitivity analyses, we found that variation in the relative risk was the most influential driver of cost effectiveness. The confidence interval around this estimate was wide, likely because only a relatively small proportion of women in the ORIP trial (17.5%) were classified as having low omega-3 status. As this treatment effect estimate was derived from a subgroup analysis, it introduces some uncertainty into the modelled outcomes. However, the effect of supplementation in singleton pregnancies was large and significant (77% reduction in early preterm birth) and larger11 than the effect size reported in the Cochrane systematic review (42% reduction),10 where omega-3 status was not verified and which included some studies conducted in settings with higher background omega-3 intake than Australia. The anticipated reduction in early preterm birth from the Cochrane review remains greater than the treatment effect size required for cost neutrality.
Additionally, our population estimates of omega-3 depletion in Australian pregnant women have confirmed that this proportion is approximately 17%.16 Although additional real-world data on the treatment effect would help narrow the confidence intervals and refine cost-effectiveness estimates, the finding that omega-3 testing and supplementation is a dominant strategy suggests that it is likely to be both cost-saving and more effective than current practice, providing a strong basis for policy adoption. Beyond adoption, embedding evaluation within implementation will add further value. Monitoring health outcomes in practice will support optimisation of delivery strategies, ensuring the intervention achieves its full potential at a population level. While the Australian example is used for illustrative purposes, the open-source model can be used by any health service or jurisdiction to explore data from their own patient population and setting.
Implications for Health Systems and Policy
Adopting omega-3 testing and supplementation into routine antenatal care would require only modest upfront investment yet is projected to generate substantial net savings by reducing the high costs associated with early preterm birth. Although these projections strongly depend on assumptions regarding treatment effect, the modelling indicates substantial potential value for health systems. The testing process can be implemented within existing diagnostic infrastructure in public laboratories across Australia. Once established, it can be incorporated into standard antenatal blood panels without major changes to the existing workflow. This makes the approach compatible with current models of care and easily scalable across primary, secondary, and tertiary health settings, including rural and remote areas.
The economic rationale for adoption extends beyond the immediate cost savings. Current estimates are based on a single birth cohort expressed in 2021 Australian dollars; however, each subsequent year brings another cohort of preterm infants who will generate similar long-term health, education, and social service costs. These overlapping cohorts create a compounding societal burden that far exceeds single-year projections, and rising healthcare and education costs will further amplify this effect. Preventive strategies such as omega-3 testing and supplementation therefore deliver increasing value over time as they reduce both immediate and cumulative system pressures.
Equity implications are also significant. Aboriginal and Torres Strait Islander women experience disproportionately high rates of early preterm birth and infant mortality, which contribute to intergenerational disadvantage. Integrating omega-3 testing and supplementation into standard antenatal care has the potential to benefit Aboriginal and Torres Strait Islander women. Broader implementation, including through Aboriginal Community Controlled Health Services, could help narrow these disparities and support national Closing the Gap priorities.6
Conclusion
Omega-3 testing and targeted supplementation during pregnancy has the potential to reduce early preterm birth and generate substantial cost-saving. In the base-case analysis, national implementation was estimated to prevent approximately 640 early preterm births annually, save more than AUD 26 million in direct healthcare costs, and reduce total costs by 44.7 million compared with current practice.
The magnitude of the economic benefit is sensitive to the treatment effect estimate derived from the ORIP trial subgroup analysis. However, the modelling results suggest that omega-3 testing and supplementation could represent a cost-effective or cost-saving strategy. Further evaluation during real-world implementation will be important to confirm effectiveness, uptake, and economic outcomes.
With demonstrated feasibility and acceptability in South Australia, this approach has the potential to provide a practical and scalable strategy for early preterm birth prevention, with potential benefits for mothers, infants, and the health system.
Abbreviations
AIHW, Australian Institute of Health and Welfare; AUD, Australian dollar; CI, Confidence Interval; CPI, Consumer Price Index; DHA, docosahexaenoic acid; EPA, eicosapentaenoic acid; EPTB, early preterm birth; ICER, incremental cost-effectiveness ratio; LCPUFA, long-chain polyunsaturated fatty acid; ORIP, Omega-3 to Reduce the Incidence of Prematurity; PTBs, preterm births; QALY, quality adjusted life year; SA, South Australia; SAMSAS, SA Maternal Serum Antenatal Screening; U.S., United States.
Data Sharing Statement
The authors confirm that the data supporting the findings of this study are available within the article and its supplementary materials. The Australian Institute of Health and Welfare (AIHW) data are available via: https://www.aihw.gov.au/reports-data/population-groups/mothers-babies/reports.
Acknowledgments
ChatGPT (OpenAI GPT-5.1) was used to assist with language editing, improve clarity, and draft the plain language summary. The authors reviewed, verified and take responsibility for all content.
Funding
This work was supported by the Australian Government Medical Research Future Fund (MRFF) [grant number APP2022061]. The funder had no role in the study design, data collection, data analysis, interpretation of findings, preparation of the manuscript, or decision to submit the manuscript for publication.
Disclosure
KPB and MM, and RAG received institutional grant funding from the Medical Research Futures Fund (APP2022061) and The Hospital Research Foundation. MM, and RAG received institutional grants from the National Health and Medical Research Council (APP1135155, APP1050468). MM served as an unpaid board and executive member of the International Society for the Study of Fatty Acids and Lipids. RG received project funding from Nestlé Institute of Health Sciences SA. KPB serves as Co-chair of the MyTIME Data Safety Monitoring Committee for a melatonin in pregnancy trial at Curtin University (unpaid role) and LS holds a paid leadership role as Director of Policy and Practice at Public Pathology Australia. All other authors declare no conflicts of interest in this work.
References
1. Ohuma EO, Moller A-B, Bradley E, et al. National, regional, and global estimates of preterm birth in 2020, with trends from 2010: a systematic analysis. Lancet. 2023;402(10409):1261–13. doi:10.1016/S0140-6736(23)00878-4
2. Perin J, Mulick A, Yeung D, et al. Global, regional, and national causes of under-5 mortality in 2000-19: an updated systematic analysis with implications for the sustainable development goals. Lancet Child Adolesc Health. 2022;6(2):106–115. doi:10.1016/S2352-4642(21)00311-4
3. WHO. Born too soon: decade of action on preterm birth. Born Too Soon. 2023.
4. Newnham JP, Schilling C, Petrou S, et al. The health and educational costs of preterm birth to 18 years of age in Australia. Aust N Z J Obstet Gynaecol. 2022;62(1):55–61. doi:10.1111/ajo.13405
5. Alliance APBP. Every Week Counts National Collaborative. 2025. Available from: https://pretermalliance.com.au/mothers-to-be/every-week-counts-national-collaborative/.
6. AIHW. Australia’s mothers and babies. Available from: https://www.aihw.gov.au/reports/mothers-babies/australias-mothers-babies/contents/summary.
7. Boyle EM, Poulsen G, Field DJ, et al. Effects of gestational age at birth on health outcomes at 3 and 5 years of age: population based cohort study. BMJ. 2012;344:e896. doi:10.1136/bmj.e896
8. Ancel PY, Goffinet F, Group E-W, et al. Survival and morbidity of preterm children born at 22 through 34 weeks’ gestation in France in 2011: results of the EPIPAGE-2 cohort study. JAMA Pediatr. 2015;169(3):230–238. doi:10.1001/jamapediatrics.2014.3351
9. Bird TM, Bronstein JM, Hall RW, Lowery CL, Nugent R, Mays GP. Late preterm infants: birth outcomes and health care utilization in the first year. Pediatrics. 2010;126(2):e311–9. doi:10.1542/peds.2009-2869
10. Middleton P, Gomersall JC, Gould JF, Shepherd E, Olsen SF, Makrides M. Omega-3 fatty acid addition during pregnancy. Cochrane Database Syst Rev. 2018;11(11):CD003402. doi:10.1002/14651858.CD003402.pub3
11. Makrides M, Best K, Yelland L, et al. A randomized trial of prenatal n−3 fatty acid supplementation and preterm delivery. N Engl J Med. 2019;381(11):1035–1045. doi:10.1056/NEJMoa1816832
12. Simmonds LA, Sullivan TR, Skubisz M, et al. Omega-3 fatty acid supplementation in pregnancy-baseline omega-3 status and early preterm birth: exploratory analysis of a randomised controlled trial. BJOG. 2020;127(8):975–981. doi:10.1111/1471-0528.16168
13. Carlson SE, Gajewski BJ, Valentine CJ, et al. Higher dose docosahexaenoic acid supplementation during pregnancy and early preterm birth: a randomised, double-blind, adaptive-design superiority trial. EClinicalMedicine. 2021;36:100905. doi:10.1016/j.eclinm.2021.100905
14. Olsen SF, Halldorsson TI, Li M, et al. Examining the effect of fish oil supplementation in chinese pregnant women on gestation duration and risk of preterm delivery. J Nutr. 2019;149(11):1942–1951. doi:10.1093/jn/nxz153
15. Collaboration ALE. Australian Pregnancy Care Guidelines. Vol. 6.1. Australian Government Department of Health DaA: 2025; 64–71. https://livingevidence.org.au/living-guidelines/leapp/.
16. Best KP, Northcott C, Simmonds LA, et al. The early implementation phase of the Omega-3 Test-and-Treat Program for reducing the risk of preterm birth, South Australia, 2021-22: an implementation evaluation study. Med J Aust. 2025;223(11):626–633. doi:10.5694/mja2.70101
17. de Groot RHM, Meyer BJ. ISSFAL Official Statement Number 6: the importance of measuring blood omega-3 long chain polyunsaturated fatty acid levels in research. Prostaglandins Leukot Essent Fatty Acids. 2020;157:102029. doi:10.1016/j.plefa.2019.102029
18. von Schacky C. Omega-3 fatty acids in pregnancy-the case for a target omega-3 index. Nutrients. 2020;12(4). doi:10.3390/nu12040898
19. Statistics ABo. Consumer Price Index, Australia. Available from: https://www.abs.gov.au/statistics/economy/price-indexes-and-inflation/consumer-price-index-australia/oct-2025.
20. Pathology S. The Omega-3 Test-and-Treat Program: Reducing Preterm Births in SA. 2024. Available from: https://www.sapathology.sa.gov.au/insights/the-omega-3-test-and-treat-program-reducing-preterm-births-in-sa.
21. Fox H, Callander E. Cost of preterm birth to Australian mothers: assessing the financial impact of a birth outcome with an increasing prevalence. J Paediatr Child Health. 2021;57(5):618–625. doi:10.1111/jpc.15278
22. Guidelines for preparing assessments for MSAC (MSAC) (2021).
23. Edney LC, Haji Ali Afzali H, Cheng TC, Karnon J. Estimating the reference incremental cost-effectiveness ratio for the australian health system. Pharmacoeconomics. 2018;36(2):239–252. doi:10.1007/s40273-017-0585-2
24. Harris AH, Hill SR, Chin G, Li JJ, Walkom E. The role of value for money in public insurance coverage decisions for drugs in Australia: a retrospective analysis 1994-2004. Med Decis Making. 2008;28(5):713–722. doi:10.1177/0272989X08315247
25. Figarella A, Chau C, Loundou A, d’Ercole C, Bretelle F. The introduction of a universal transvaginal cervical length screening program is associated with a reduced preterm birth rate. Am J Obstet Gynecol. 2023;228(2):219e1–219e14. doi:10.1016/j.ajog.2022.07.046
26. Temming LA, Durst JK, Tuuli MG, et al. Universal cervical length screening: implementation and outcomes. Am J Obstet Gynecol. 2016;214(4):523e1–523e8. doi:10.1016/j.ajog.2016.02.002
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prominent Mutation of Intron 22 Inversion in Sporadic Hemophilia: Is It Worth the Antenatal Screening?
Sasanakul W, Chuansumrit A, Sirachainan N, Kadegasem P
The Application of Clinical Genetics 2022, 15:49-54
Published Date: 19 May 2022
Economic Evaluation of Mepolizumab as Add-on Therapy to Standard Care in Severe Eosinophilic Asthma: A Cost-Effectiveness Analysis in Colombia
Buendia JA, Acuna-Cordero R, Rodriguez-Martinez CE
Journal of Asthma and Allergy 2025, 18:211-218
Published Date: 17 February 2025
Cost-Utility Analyses of Hemodialysis, Peritoneal Dialysis, and Kidney Transplantation in Patients with End-Stage Kidney Disease: A Systematic Review
Wulandari W, Alfaqeeh M, Zakiyah N, Shafie AA, Suwantika AA
ClinicoEconomics and Outcomes Research 2025, 17:883-895
Published Date: 5 December 2025
Long-Term Clinical Outcomes and Cost-Effectiveness of Bariatric Surgery for Type 2 Diabetes in Malaysia: A 10-Year Retrospective Cohort Study
Galvan JAA, Loo GH, Kosai NR, Yeong CH, Chinna K, Nordin RB, Lee KKC, Mustafa N
Journal of Multidisciplinary Healthcare 2026, 19:590099
Published Date: 8 July 2026