Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Long-Term Clinical Outcomes and Cost-Effectiveness of Bariatric Surgery for Type 2 Diabetes in Malaysia: A 10-Year Retrospective Cohort Study
Authors Galvan JAA ![]() , Loo GH
, Loo GH ![]() , Kosai NR, Yeong CH, Chinna K, Nordin RB, Lee KKC, Mustafa N
, Kosai NR, Yeong CH, Chinna K, Nordin RB, Lee KKC, Mustafa N ![]()
Received 18 December 2025
Accepted for publication 8 June 2026
Published 8 July 2026 Volume 2026:19 590099
DOI https://doi.org/10.2147/JMDH.S590099
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jacqueline Dunbar-Jacob
Jo Ann Andoy Galvan1, Guo Hou Loo2, Nik Ritza Kosai2, Chai Hong Yeong1, Karuthan Chinna3, Rusli Bin Nordin4, Kenneth Kwing-Chin Lee5, Norlaila Mustafa6
1School of Medicine, Faculty of Health & Medical Sciences, Taylor’s University, Subang Jaya, Malaysia; 2Department of Surgery, Faculty of Medicine, the National University of Malaysia (UKM), Kuala Lumpur, Malaysia; 3Faculty of Business and Management, UCSI University, Kuala Lumpur, Malaysia; 4Faculty of Medicine, Bioscience and Nursing, MAHSA University, Kuala Lumpur, Malaysia; 5School of Pharmacy, Monash University, Subang Jaya, Malaysia; 6Department of Medicine, Faculty of Medicine, The National University of Malaysia (UKM), Kuala Lumpur, Malaysia
Correspondence: Guo Hou Loo, Department of Surgery, Faculty of Medicine, The National University of Malaysia, Kuala Lumpur, Malaysia, Email [email protected]
Background: Malaysia has the highest obesity prevalence in Southeast Asia, driving the burden of type 2 diabetes mellitus (T2DM) and its healthcare costs. Long-term real-world cost-effectiveness data on bariatric surgery from Malaysia are absent. We evaluated the clinical outcomes, safety, and exploratory cost-effectiveness of bariatric surgery in Malaysian patients with obesity and T2DM.
Methods: Retrospective cohort study of 180 patients undergoing laparoscopic sleeve gastrectomy or Roux-en-Y gastric bypass at HCTM, Universiti Kebangsaan Malaysia (2014–2016), with 5-year clinical follow-up. BMI and HbA1c were analysed using generalised estimating equations (GEE) with a Gaussian family, identity link and exchangeable working correlation. An exploratory cost-effectiveness analysis compared 20 surgical patients with 20 matched conventional-management patients (2012–2014) over a 10-year horizon from the healthcare-payer perspective. The incremental cost-effectiveness ratio (ICER) was expressed per 1% HbA1c reduction, with one-way deterministic and probabilistic sensitivity analyses.
Results: Mean BMI decreased from 49.29 ± 8.97 to 25.33 ± 4.25 kg/m2 at 5 years; HbA1c fell from 6.37 ± 1.37% to 5.62 ± 0.68% (both GEE p<0.001). The complication rate was 2.2%, and 76% of patients were discharged ithin 2 days. The base-case ICER was RM 4683 per 1% HbA1c reduction; probabilistic analysis yielded a median ICER of RM 4828 (95% credible interval: cost-saving to RM 32,286) and a 59% probability of cost-effectiveness at a willingness-to-pay threshold of RM 7500 per 1% HbA1c reduction.
Conclusion: In this single-centre Malaysian cohort, bariatric surgery produced durable improvements in BMI and HbA1c with low complication rates and a favourable exploratory ICER. Findings should be interpreted in light of the retrospective design and small economic cohort, and confirmed in multicentre prospective studies.
Keywords: bariatric surgery, cost-effectiveness, type 2 diabetes, obesity, Malaysia, health economics, generalized estimating equations
Introduction
Obesity is a major global driver of non-communicable disease and now affects more than one billion people worldwide. Malaysia records the highest prevalence of obesity in Southeast Asia, with 21.8% of adults classified as obese and an additional 32.6% overweight according to the 2023 National Health and Morbidity Survey.1 This epidemic is closely linked with the rising burden of type 2 diabetes mellitus (T2DM), cardiovascular disease, and certain cancers, all of which contribute to substantial morbidity, premature mortality, and healthcare costs.2 In Malaysia, the economic burden of obesity has been estimated at RM 4.3–8.6 billion annually, representing up to 20% of the national healthcare budget.3
Conventional treatment of obesity and T2DM: lifestyle modification, pharmacotherapy and behavioural interventions often achieve only limited long-term success. Although novel anti-obesity and antidiabetic agents are increasingly available, adherence and affordability remain problematic. The National Diabetes Registry reports that only approximately one-third of Malaysian patients achieve target glycaemic control.4 Suboptimal control drives downstream complications such as nephropathy, cardiovascular disease and retinopathy, which further inflate costs and erode productivity.
Bariatric surgery is the most effective treatment for severe obesity and has demonstrated superior outcomes compared with medical therapy in randomised trials and meta-analyses.5,6 Its metabolic effects extend beyond weight loss, with high rates of T2DM remission and reduction in cardiovascular events. International guidelines, including those of the American Diabetes Association and the International Federation for the Surgery of Obesity and Metabolic Disorders, accordingly recommend metabolic surgery for patients with inadequately controlled T2DM and class II–III obesity, with lower BMI thresholds for Asian populations.7,8
Despite this evidence, bariatric surgery remains markedly underutilised in Malaysia. Only a small fraction of eligible patients undergo surgery annually. Barriers include limited surgical capacity, low public awareness and, most critically, the lack of insurance coverage. Bariatric surgery is excluded from the MySalam national health protection scheme and most private insurance plans, leaving patients to self-fund. This restricts access to higher-income individuals and perpetuates inequities despite the disproportionate burden of obesity and T2DM in lower socioeconomic groups.
Health-economic evaluations are central to shifting such policy barriers. International studies consistently show that bariatric surgery is cost-effective or cost-saving compared with conventional care.9–11 However, cost-effectiveness is highly context-specific and depends on local healthcare costs, epidemiology and financing models. To date, no long-term, real-world cost-effectiveness data are available from Malaysia, limiting evidence-based decision-making by policymakers and insurers.
Against this background, we examined the long-term clinical effectiveness, perioperative safety and exploratory cost-effectiveness of bariatric surgery in Malaysian patients with poorly controlled T2DM using data from a tertiary public hospital. We hypothesised that bariatric surgery would yield superior metabolic outcomes and an incremental cost-effectiveness ratio (ICER) below Malaysia’s willingness-to-pay (WTP) range. These findings would provide the first Malaysian evidence to inform discussions about reimbursement, insurance coverage and national health financing of bariatric surgery.
Methods and Materials
Study Design and Setting
We conducted a retrospective cohort study at Hospital Canselor Tuanku Muhriz (HCTM), Universiti Kebangsaan Malaysia. The study comprised two components: (1) analysis of clinical outcomes and safety in patients undergoing bariatric surgery (Figure 1), and (2) an exploratory cost-effectiveness analysis comparing bariatric surgery with conventional medical management over a 10-year horizon (Figure 2).
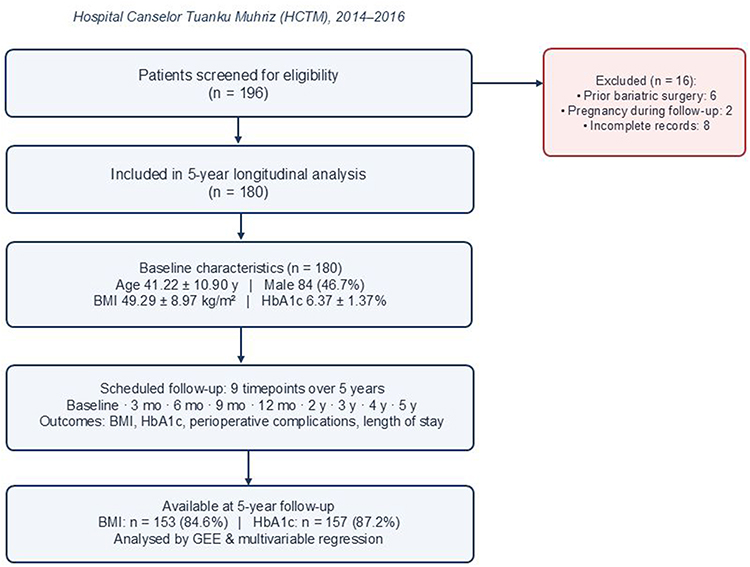 |
Figure 1 Flow diagram for the clinical effectiveness analysis. Of the 196 patients initially screened, 180 met the inclusion criteria for the 5-year longitudinal analysis. Exclusions were prior bariatric surgery (n = 6), pregnancy during follow-up (n = 2) and incomplete records (n = 8). |
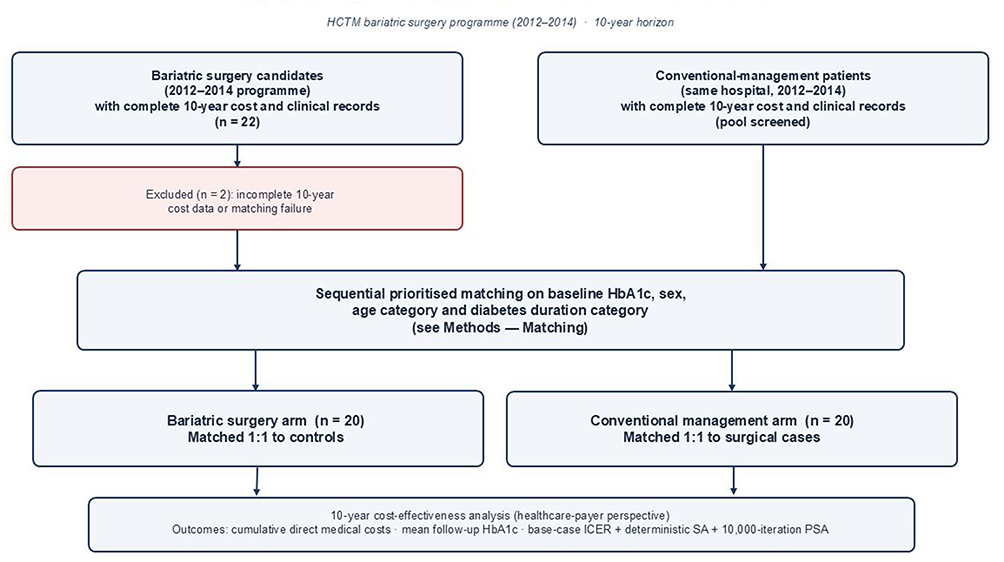 |
Figure 2 Flow diagram for the exploratory cost-effectiveness analysis. From the 2012–2014 surgical programme, 22 candidates had completed 10-year cost and clinical records; 20 were matched to 20 conventionally managed controls drawn from the same hospital cohort and time period. |
Patients
For the clinical cohort, we included 180 adults with obesity and poorly controlled T2DM who underwent laparoscopic sleeve gastrectomy (LSG) or laparoscopic Roux-en-Y gastric bypass (LRYGB) between January 2014 and December 2016. Inclusion criteria were a confirmed diagnosis of T2DM and at least 5 years of follow-up data. Exclusion criteria were prior bariatric surgery, pregnancy during follow-up, secondary causes of obesity and incomplete records. The available retrospective dataset did not record procedure type (LSG vs LRYGB) in a uniform structured form; consequently, outcomes are reported for the combined cohort rather than stratified by procedure (see Limitations).
For the cost-effectiveness cohort, 20 surgical patients were matched to 20 controls managed with conventional therapy between 2012 and 2014. The economic cohort was deliberately restricted to this earlier treatment period because the analysis required a complete 10-year follow-up window. Bariatric surgery at HCTM commenced in 2012, and uptake was gradual during the early years of the programme; consequently, only a limited number of surgical patients had sufficient longitudinal clinical and cost records for inclusion in a 10-year analysis. We acknowledge this as an exploratory analysis (see Sample size justification below).
Sample Size Justification
Because the analysis was retrospective and the eligible pool, with 10-year cost and clinical records, effectively constituted a census of the 2012–2014 surgical programme, a formal a priori power calculation was not feasible. Instead, we performed a post-hoc indicative calculation. For a between-group HbA1c difference of 1.33 percentage points with a pooled standard deviation of approximately 1.7%, a two-sided independent t-test with α = 0.05 has approximately 80% power at n ≈ 26 per group. The available sample of 20 per group, therefore, retains adequate sensitivity for clinically meaningful HbA1c differences but limits precision for cost outcomes. We address this uncertainty explicitly through deterministic and probabilistic sensitivity analyses (see Statistical Analysis).
Matching
Matching variables were selected based on predictors of diabetes remission after bariatric surgery, particularly the ABCD diabetes surgery score (Age, BMI, C-peptide, Duration of T2DM). Because C-peptide was not consistently available in the retrospective dataset, available ABCD-related variables (age, BMI, diabetes duration) were considered, together with baseline HbA1c and sex. Baseline HbA1c was prioritised because it directly reflects glycaemic severity and was the primary effectiveness outcome used in the economic analysis.
Given the limited number of eligible patients with complete 10-year follow-up data, full propensity-score-based matching was not feasible. We therefore used a sequential, prioritised matching algorithm: each surgical patient was first matched to a conventional-management patient with the closest baseline HbA1c (within ± 1.5 percentage points where possible) and the same sex; remaining candidates were then assessed for group-level comparability on age category (≤ 50 vs > 50 years) and diabetes duration category (≤ 10 vs > 10 years), thresholds adapted from the ABCD score. The resulting post-matching balance is reported in the Results section. Residual imbalance, particularly for age and diabetes duration, was a consequence of the limited eligible pool and is addressed by the multivariable regression sensitivity analysis described below.
Outcomes
Clinical outcomes were changes in BMI and HbA1c at 3, 6, 9 and 12 months, and annually thereafter up to 5 years. Safety outcomes were perioperative complications graded with the Clavien–Dindo system and length of hospital stay.
Economic outcomes were cumulative direct healthcare costs and the incremental cost-effectiveness ratio (ICER), expressed as cost per 1% HbA1c reduction. We adopted a healthcare-payer perspective and included only direct medical costs (surgical fees, hospitalisation, outpatient follow-up, laboratory tests, medications and management of recorded complications). Indirect costs such as productivity loss, transportation, caregiver costs and out-of-pocket non-medical expenses were not included. Unit costs were derived from hospital billing records, pharmacy records, and Ministry of Health published schedules. All costs are reported in Malaysian Ringgit (RM) in the base year of the cost-effectiveness analysis; given the modest 10-year horizon and Malaysia’s low average inflation rate over the study period, costs were not deflated to a single base year in the primary analysis. Discounting at 3% per annum was applied in sensitivity analyses.
Statistical Analysis
Continuous variables are summarised as mean ± SD (or median and interquartile range if non-normally distributed). Categorical variables are summarised as frequencies and percentages. Changes from baseline at pre-specified time points were assessed with paired t-tests using complete paired observations.
Longitudinal changes in BMI and HbA1c were analysed using generalised estimating equations (GEE), with a Gaussian family, identity link function and an exchangeable working correlation structure, and time specified as a categorical variable. The exchangeable structure was chosen a priori because all patients followed an identical scheduled follow-up. Robust (sandwich) standard errors were used. Overall effects of time were tested with a Wald χ2 statistic, and pairwise comparisons against baseline were Bonferroni-adjusted. As a sensitivity check, models were re-fitted with independence and first-order autoregressive correlation structures; coefficients differed by less than 0.5%, and inferences were unchanged.
Missing follow-up values for BMI or HbA1c were treated as missing-at-random, and the GEE model included available observations under maximum-likelihood-equivalent estimation; no imputation was performed in the primary analysis. The pattern of missingness across follow-up is summarised in the text. Multiple imputation (m = 20) using chained equations was conducted as a sensitivity analysis and produced equivalent point estimates (BMI at 5 years: −24.0 vs −24.0 kg/m2; HbA1c at 5 years: −0.79 vs −0.79 percentage points).
To address potential residual confounding inherent to the retrospective single-arm clinical cohort, we additionally fitted multivariable linear regression models for BMI and HbA1c at 5 years, with baseline BMI, baseline HbA1c, age, sex, hypertension, dyslipidaemia and obstructive sleep apnoea as covariates.
Cost-Effectiveness Measure
The primary economic measure was the ICER, calculated as the ratio of the between-group difference in mean cumulative direct medical costs to the between-group difference in mean HbA1c reduction over the 10-year horizon:

Sensitivity Analyses
We pre-specified two layers of sensitivity analysis. First, one-way deterministic sensitivity analyses varied each key parameter: surgical cost, conventional management cost, mean follow-up HbA1c in each arm and the discount rate (0%, 3%, 5%) within plausible ranges (±20% for costs; ±0.3 percentage points for HbA1c). Results are displayed as a tornado diagram. Second, probabilistic sensitivity analysis (PSA) was performed with 10,000 Monte Carlo simulations, sampling surgical and conventional costs from gamma distributions and follow-up HbA1c values from normal distributions parameterised by their observed means and standard errors. PSA results are displayed as a cost-effectiveness plane and cost-effectiveness acceptability curve. Probabilities of cost-effectiveness were calculated against willingness-to-pay (WTP) thresholds ranging from RM 0 to RM 30,000 per 1% HbA1c reduction.
Ethics
The study was approved by the institutional ethics review committee (UKMREC; JEP-2022-545). Patient data were anonymised and analysed in accordance with the Declaration of Helsinki. The requirement for individual informed consent was waived in view of the retrospective design and use of anonymised records.
Results
Baseline Characteristics
A total of 180 patients (84 males, 96 females; mean age 41.22 ± 10.90 years) underwent bariatric surgery between 2014 and 2016. Mean baseline BMI was 49.29 ± 8.97 kg/m2, and mean baseline HbA1c was 6.37 ± 1.37%. The most prevalent comorbidities were dyslipidaemia (46.1%) and hypertension (27.2%); obstructive sleep apnoea was present in 8.9% (Table 1).
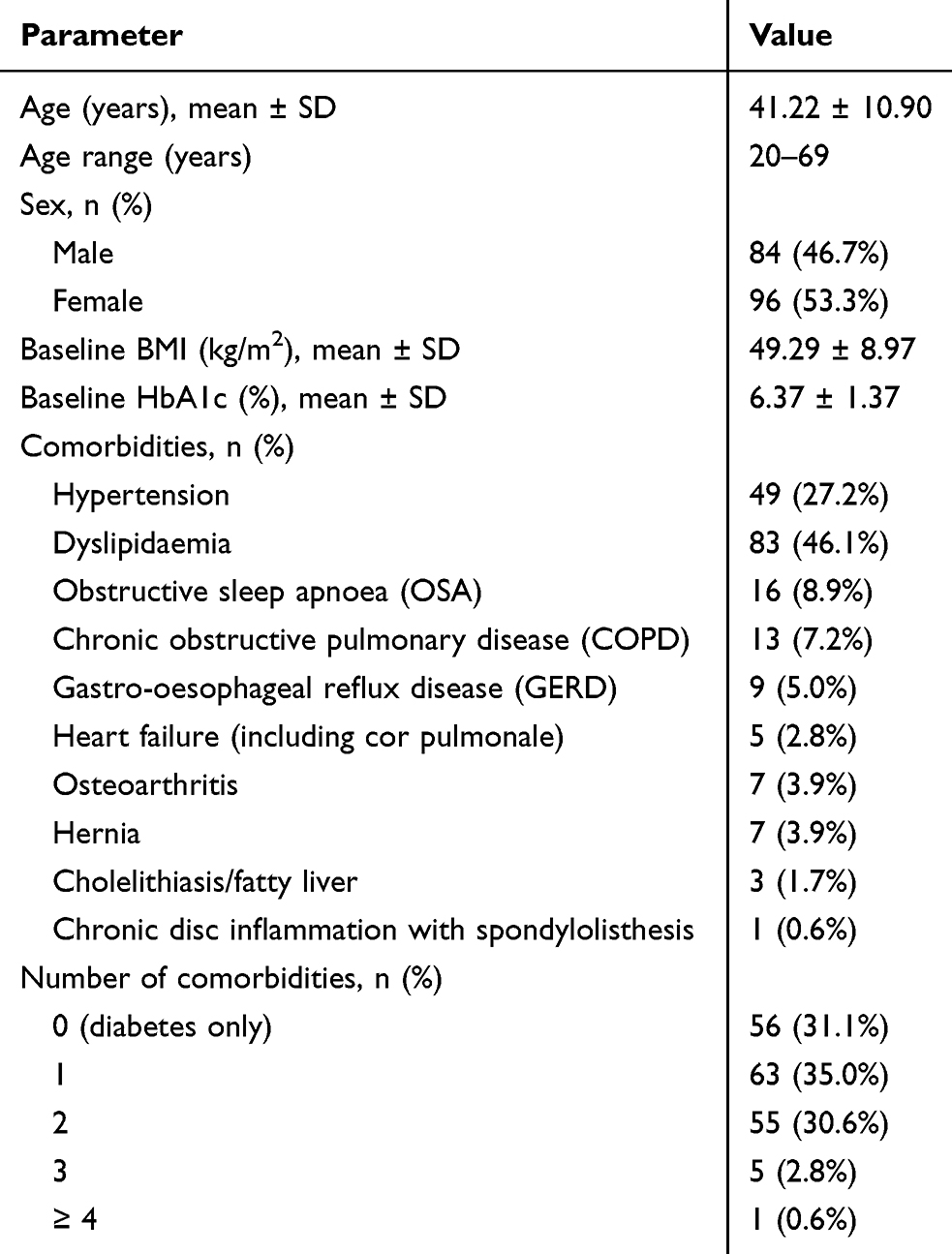 |
Table 1 Baseline Sociodemographic and Clinical Characteristics of the Clinical Cohort (n = 180) |
Clinical Outcomes
At 3 months, mean BMI decreased by 4.23 kg/m2 (95% CI 3.95–4.52; t = 29.6) and HbA1c by 0.42 percentage points (95% CI 0.36–0.49; t = 13.5; both p < 0.001). At 12 months, mean BMI had fallen to 31.63 ± 6.31 kg/m2 (mean difference vs baseline 17.85; 95% CI 17.01–18.68; t = 42.3) and mean HbA1c to 5.58 ± 0.81% (mean difference 0.79; 95% CI 0.67–0.92; t = 12.7; both p < 0.001) (Table 2).
 |
Table 2 Short-Term Clinical Outcomes Following Bariatric Surgery (n = 180) |
Long-term outcomes were sustained. At 5 years, mean BMI was 25.33 ± 4.25 kg/m2 and mean HbA1c 5.62 ± 0.68%. Among patients with follow-up data at 5 years, 131 of 157 (83.4%) had HbA1c < 6.0% and 127 of 153 (83.0%) maintained a BMI < 30 kg/m2. GEE confirmed a significant overall effect of time on both BMI (Wald χ2 = 2340.78, df = 8, p < 0.001) and HbA1c (Wald χ2 = 282.35, df = 8, p < 0.001), with significant reductions from baseline at every follow-up time point after Bonferroni correction (Table 3, Figures 3 and 4). Sensitivity analyses using independence and autoregressive correlation structures produced essentially identical estimates (5-year BMI coefficient = −23.99 vs −23.96 and −23.91, respectively).
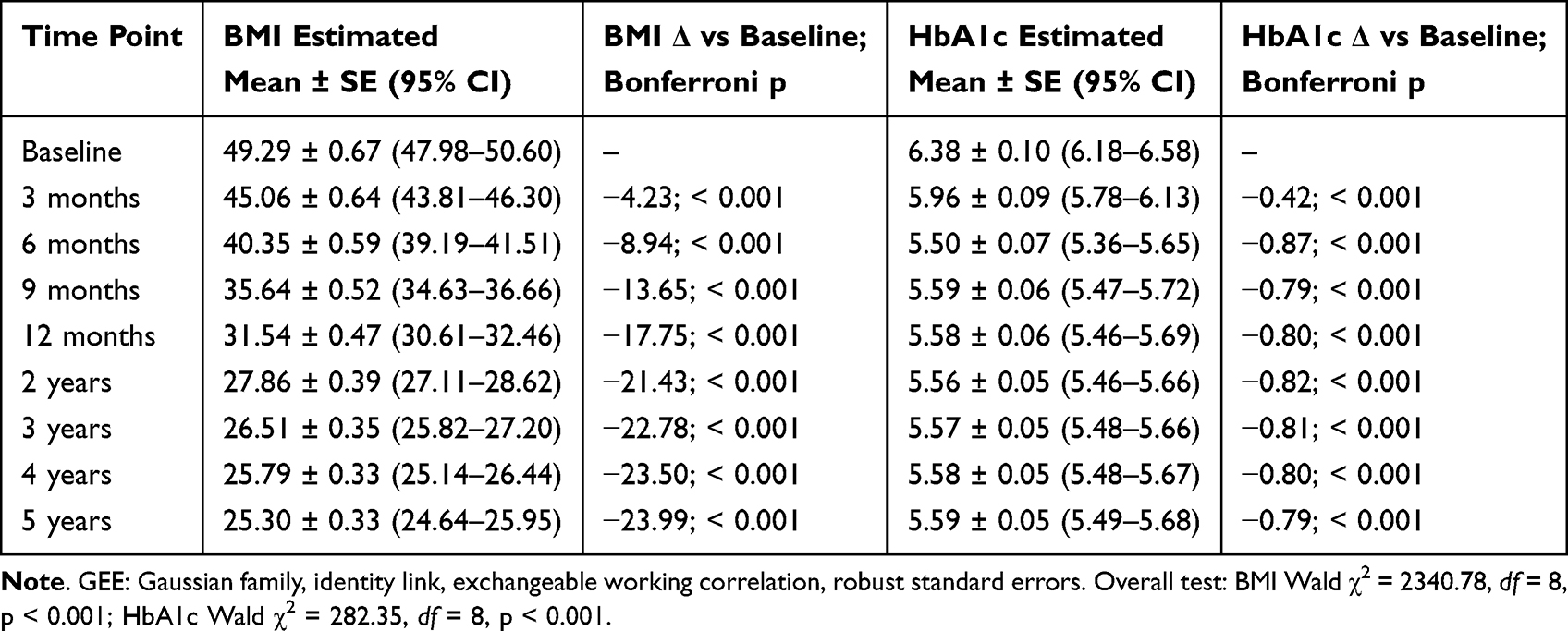 |
Table 3 GEE-Estimated Marginal Means and Pairwise Comparisons of BMI and HbA1c Across Follow-Up |
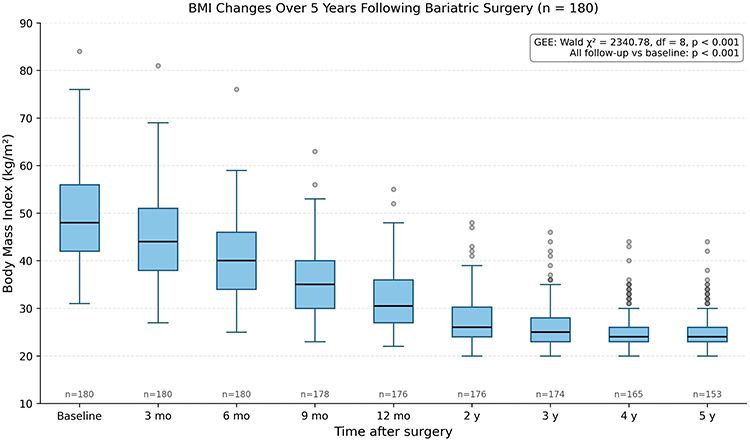 |
Figure 3 Distribution of BMI (kg/m2) at each follow-up time point in the clinical cohort (n = 180). Boxes show the interquartile range with the median line; whiskers extend to 1.5 × IQR; circles denote observations beyond 1.5 × IQR. Sample sizes are annotated below each box. The inset statistic gives the GEE overall test of time and the Bonferroni-adjusted p-value for each follow-up vs baseline. |
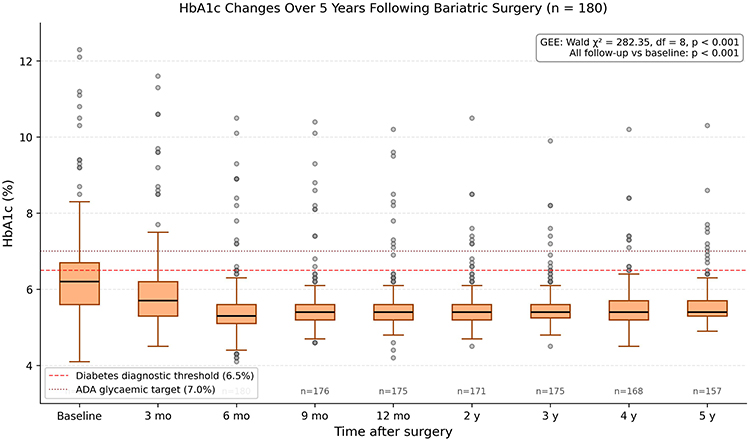 |
Figure 4 Distribution of HbA1c (%) at each follow-up time point in the clinical cohort (n = 180). Boxes show the interquartile range with the median line; whiskers extend to 1.5 × IQR; circles denote observations beyond 1.5 × IQR. The dashed red horizontal line marks the diabetes diagnostic threshold of 6.5% HbA1c, and the dotted dark-red line marks the American Diabetes Association glycaemic target of 7.0% HbA1c. Sample sizes are annotated below each box. |
In the multivariable linear regression for HbA1c at 5 years (n = 156; R2 = 0.565), baseline HbA1c was the strongest independent predictor (β = 0.35, 95% CI 0.30–0.40, p < 0.001) and older age was modestly associated with lower 5-year HbA1c (β = −0.008 per year, p = 0.020); baseline BMI, sex and comorbidities were not significant. For BMI at 5 years (n = 153; R2 = 0.413), baseline BMI was the dominant predictor (β = 0.31, 95% CI 0.24–0.37, p < 0.001). These findings indicate that the observed long-term reductions were not driven by selected confounders.
Safety
Surgical safety was favourable. The overall complication rate was 2.2% (four events: three short-term Clavien–Dindo grade I dumping syndrome cases managed by dietary modification and one long-term grade I incisional hernia managed conservatively). No mortality occurred during follow-up. Hospital stay was short: 76% of patients were discharged within 2 days, and 21% were managed as day cases without overnight admission. Because procedure type was not consistently recorded in the retrospective dataset, we were unable to stratify complication rates by LSG vs LRYGB, and longer-term complications such as nutritional deficiencies and weight regain were not systematically captured (see Limitations) (Table 4).
 |
Table 4 Procedure-Related Complications (n = 180) |
Economic Evaluation
The exploratory cost-effectiveness cohort comprised 20 surgical and 20 conventionally managed patients. Baseline HbA1c and sex distribution were broadly comparable between groups, with no statistically significant difference in baseline HbA1c (Mann–Whitney U, p = 0.267) or sex (Fisher’s exact, p = 0.311). The conventional-management group, however, had a higher proportion of older patients (90% vs 70% aged > 50 years) and longer diabetes duration (95% vs 60% > 10 years). This residual imbalance is reported transparently in Table 5 and was addressed by the multivariable regression sensitivity analysis.
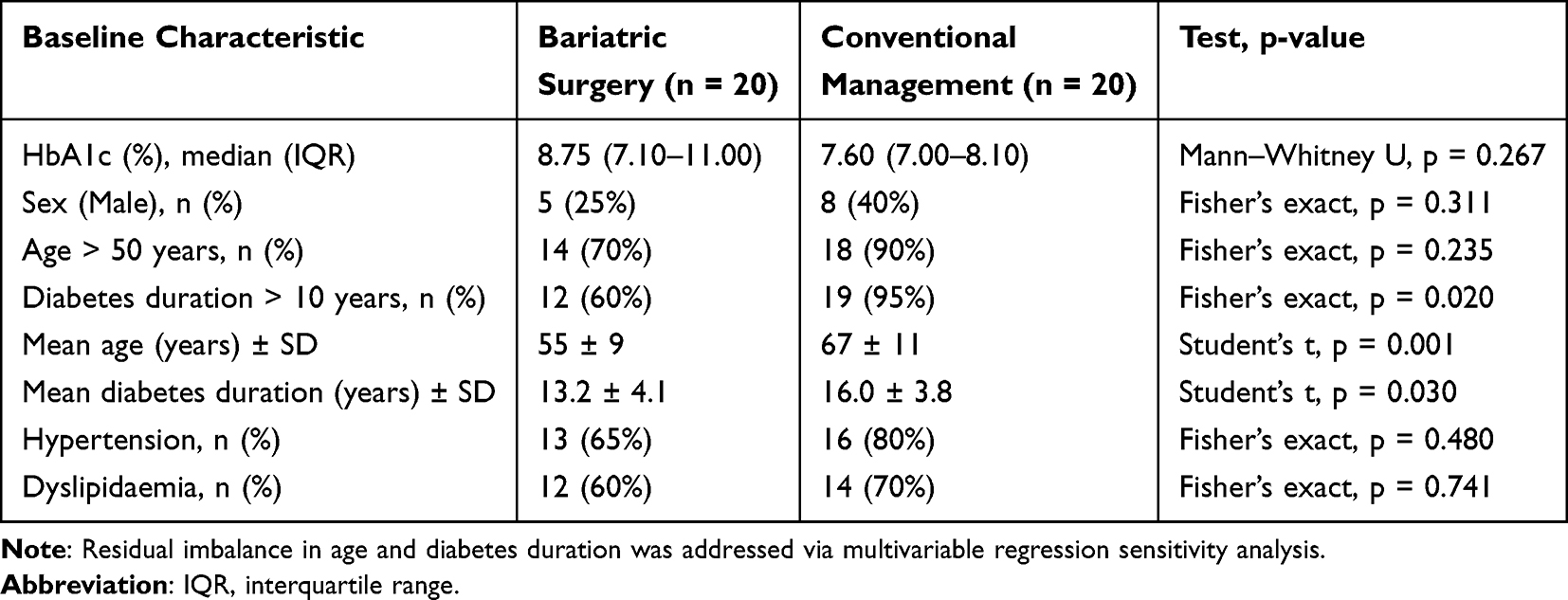 |
Table 5 Post-Matching Baseline Balance in the Exploratory Cost-Effectiveness Cohort (n = 20 per Arm) |
Over 10 years, total direct medical costs were RM 256,240 in the surgical group and RM 250,012 in the conventional group, yielding an incremental cost of RM 6228 (per patient RM 311). Mean follow-up HbA1c was 6.42% vs 7.75% (incremental HbA1c reduction 1.33 percentage points in favour of surgery). The base-case ICER was RM 4683 per 1% HbA1c reduction (Tables 6 and 7).
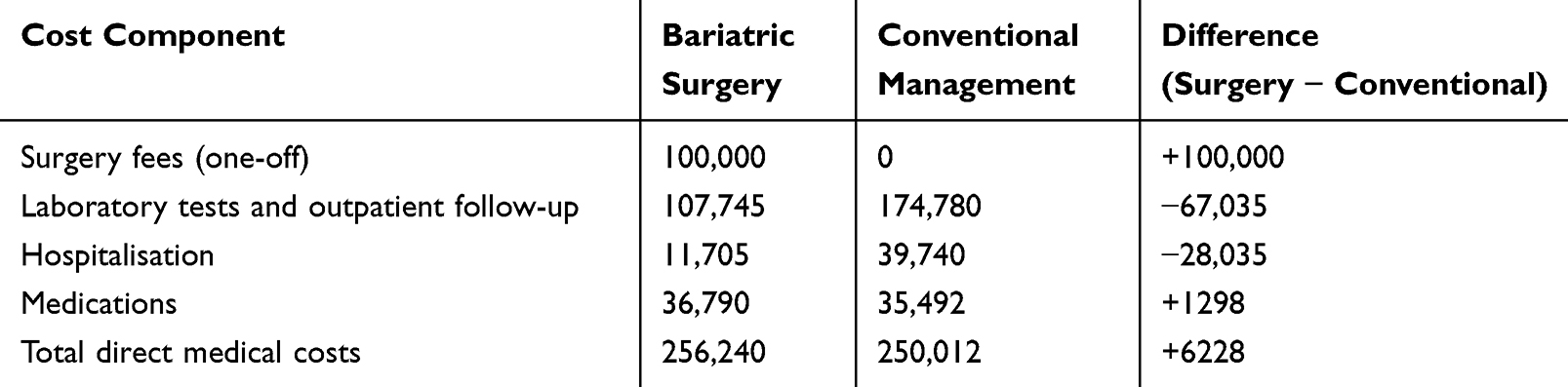 |
Table 6 Ten-Year Direct Medical Cost Composition (Exploratory Matched Cohort, n = 20 per Arm; All Values in RM) |
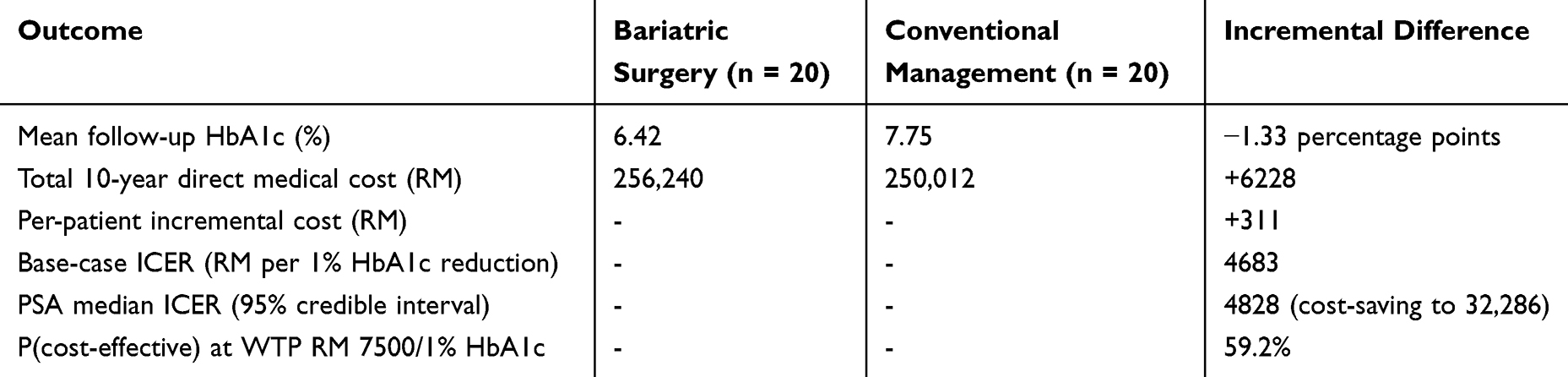 |
Table 7 Cost-Effectiveness Summary (10-Year Horizon, Exploratory Matched Cohort) |
One-way sensitivity analyses showed that the ICER was most sensitive to surgical and conventional management costs. Within ± 20% variation, the ICER ranged from cost-saving (negative ICER, indicating surgery dominated) to RM 43,215 per 1% HbA1c reduction. Discount rates of 3% and 5% increased the ICER to RM 15,321 and RM 21,173, respectively, reflecting the front-loading of surgical costs (Figure 5).
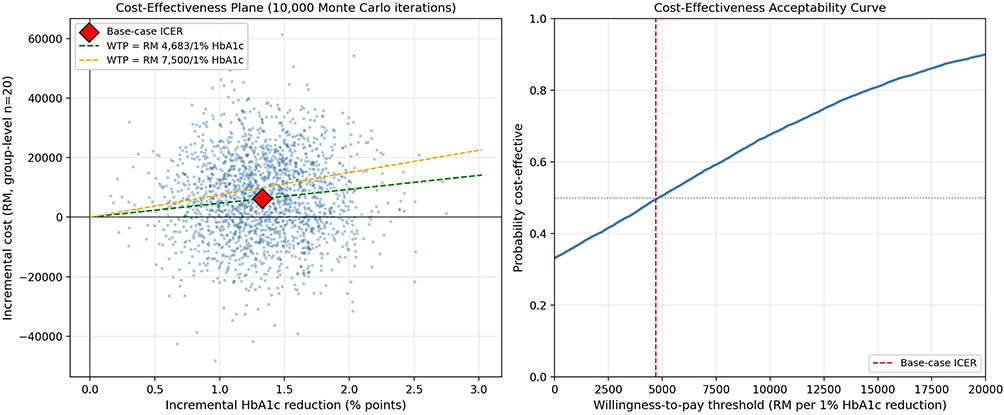 |
Figure 5 Tornado diagram showing one-way deterministic sensitivity of the ICER to ±20% variation in costs, ±0.3 percentage points in mean follow-up HbA1c, and discount rates of 0%, 3% and 5%. The vertical black line indicates the base-case ICER of RM 4683 per 1% HbA1c reduction. |
Probabilistic sensitivity analysis (10,000 iterations) produced a mean ICER of RM 5391 and a median of RM 4828, with a 95% credible interval ranging from cost-saving (negative ICER) to RM 32,286 per 1% HbA1c reduction. The probability that bariatric surgery was cost-effective was 50.6% at a WTP threshold of RM 5000 per 1% HbA1c reduction, 59.2% at RM 7500, 67.6% at RM 10,000 and 89.9% at RM 20,000 (Figure 6). These wide credible intervals reflect the small sample of the matched cohort and reinforce that the economic component should be regarded as exploratory.
 |
Figure 6 Probabilistic sensitivity analysis. Left panel: cost-effectiveness plane showing 2000 representative iterations from a 10,000-iteration Monte Carlo simulation. Each blue dot represents one simulated pair-difference (incremental cost vs incremental HbA1c reduction); the red diamond marks the base-case ICER. The green dashed line is the willingness-to-pay (WTP) threshold of RM 4683 per 1% HbA1c reduction; the Orange dashed line is WTP = RM 7500 per 1% HbA1c reduction. Right panel: cost-effectiveness acceptability curve plotting the probability that bariatric surgery is cost-effective against a range of WTP thresholds. The vertical red dashed line indicates the base-case ICER. |
Discussion
In this single-centre Malaysian cohort, bariatric surgery was associated with substantial and durable reductions in BMI and HbA1c over 5 years, a low rate of perioperative complications, and an exploratory ICER of RM 4683 per 1% HbA1c reduction over 10 years. To our knowledge, this is the first study to report both long-term clinical outcomes and a real-world cost-effectiveness analysis of bariatric surgery in Malaysia.
The clinical findings are consistent with the international literature. Buchwald et al reported high rates of diabetes remission and sustained weight reduction across procedures,5 and the Swedish Obese Subjects (SOS) study demonstrated long-term improvements in weight, glycaemic control and survival.6 A recent meta-analysis by Mirghani et al confirmed that surgery remains superior to medical therapy for T2DM remission.12 Asian populations develop metabolic complications at lower BMI thresholds than Western populations,7,8 and our results align with Li et al, who reported significant metabolic benefits of bariatric surgery in Asian patients with BMI < 35 kg/m2.13 This supports the lower BMI thresholds in Asian guidelines, including the Malaysian Clinical Practice Guidelines on Obesity.
The relatively low mean baseline HbA1c (6.37%) in our cohort warrants explanation. Most patients had been managed in a specialist diabetes service before referral and were typically on intensive antidiabetic regimens, including insulin, at the time of surgical workup; consequently, baseline HbA1c values reflect treated rather than untreated diabetes. This contextualises the modest absolute HbA1c reduction (0.79 percentage points at 12 months) alongside the much larger reduction in pharmacotherapy intensity observed at follow-up.
Our cost-effectiveness findings should be interpreted with caution, given the small economic cohort. The base-case ICER (RM 4683 per 1% HbA1c reduction) sits within the lower portion of plausible willingness-to-pay ranges, but probabilistic analysis revealed considerable uncertainty: at a threshold of RM 7500 per 1% HbA1c reduction, the probability of cost-effectiveness was 59%. The ICER was particularly sensitive to assumptions about discount rate and unit costs, reflecting the front-loaded nature of surgical expenditure. These results are nonetheless broadly consistent with the international literature. Hoerger et al reported that bariatric surgery for severely obese adults with diabetes was highly cost-effective in the United States,9 Picot et al found surgery economically favourable in the United Kingdom,10 and Borisenko et al demonstrated net cost savings across European settings.11 Lester et al also reported real-world cost-effectiveness of bariatric surgery in Canada over a 10-year and lifetime horizon.14 Importantly, Noparatayaporn et al reported that bariatric surgery was cost-effective in Thailand, a middle-income Asian setting comparable to Malaysia.15
Placing these findings in the Malaysian healthcare context, the Ministry of Health has previously commissioned health technology assessments of glucose-lowering therapies. Newer agents such as GLP-1 receptor agonists and SGLT2 inhibitors have been associated with ICERs in the order of RM 30,000–60,000 per QALY relative to standard care in regional analyses, and intensive multidisciplinary diabetes management programmes have reported per-patient annual costs ranging from RM 1800 to RM 3000 for patients with multiple complications. Against this background, an ICER of RM 4683 per 1% HbA1c reduction, even with its wide credible interval, suggests bariatric surgery is in a similar or more favourable cost-effectiveness range than several emerging pharmacological interventions for poorly controlled T2DM. We acknowledge that direct comparison is limited by the use of HbA1c (rather than QALYs) as the effectiveness measure, and that a formal cost-utility analysis is a priority for future work.
Despite strong global and regional evidence, bariatric surgery remains underutilised in Malaysia. Only a few hundred procedures are performed annually, and access is restricted by a lack of insurance coverage. Surgery is excluded from the MySalam national protection scheme and is rarely reimbursed by private insurers. Our findings provide local economic evidence that may inform such reimbursement decisions, though the small economic sample means policy translation must proceed cautiously and ideally be supported by larger, multicentre evaluations.
Strengths and Limitations
Strengths include the real-world cohort, the 5-year clinical follow-up and the 10-year economic horizon, the use of GEE and multivariable regression to handle clustered data and residual confounding, and the addition of deterministic and probabilistic sensitivity analyses around the ICER. Costs were derived from actual hospital billing records and Ministry of Health schedules.
Several limitations warrant emphasis. First, the economic cohort comprised only 20 matched pairs, which yields wide credible intervals around the ICER and limits generalisability; this is reflected in the explicit “exploratory” framing of the cost-effectiveness analysis. Second, the dataset did not allow stratification of clinical outcomes or complications by procedure type (LSG vs LRYGB); given documented differences in efficacy and safety, this is a meaningful gap that future studies should address with prospective data capture. Third, longer-term complications such as nutritional deficiencies, weight regain, gastro-oesophageal reflux and re-operation rates were not systematically recorded. Fourth, the retrospective single-centre design carries inherent risks of residual confounding and limited external validity. Fifth, indirect costs (productivity, transport, caregiver burden) were not captured, meaning that societal benefits are likely underestimated. Sixth, the use of HbA1c rather than QALYs as the effectiveness denominator means our results should be interpreted as exploratory economic evidence rather than as a definitive cost-utility analysis.
Conclusion
In this single-centre Malaysian cohort, bariatric surgery produced durable and clinically meaningful reductions in BMI and HbA1c over 5 years, with low complication rates and short hospital stays. The exploratory 10-year cost-effectiveness analysis suggested a base-case ICER of RM 4683 per 1% HbA1c reduction, with probabilistic sensitivity analysis indicating a moderate probability of cost-effectiveness at conventional willingness-to-pay thresholds. While these findings are encouraging and broadly consistent with international evidence, the small economic cohort and retrospective design preclude definitive policy conclusions. The results provide a foundation and motivation for larger, prospective, multicentre evaluations that can inform decisions about reimbursement and access to bariatric surgery for Malaysian patients with poorly controlled T2DM.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Institute for Public Health. National health and morbidity survey 2023. Kuala Lumpur: Ministry of Health Malaysia; 2024.
2. World Health Organization. Noncommunicable diseases country profiles 2022. Geneva: World Health Organization; 2022.
3. CodeBlue. Economic burden of obesity in Malaysia. CodeBlue News. 2023. Available from: https://codeblue.galencentre.org.
4. Ministry of Health Malaysia. National diabetes registry report 2023. Putrajaya: MOH; 2023.
5. Buchwald H, Avidor Y, Braunwald E, et al. Bariatric surgery: a systematic review and meta-analysis. JAMA. 2004;292(14):1724–12. doi:10.1001/jama.292.14.1724
6. Sjöström L, Narbro K, Sjöström CD, et al. Effects of bariatric surgery on mortality in Swedish obese subjects. N Engl J Med. 2007;357(8):741–752. doi:10.1056/NEJMoa066254
7. ElSayed NA, Aleppo G, Aroda VR, et al; on behalf of the American Diabetes Association. Introduction and methodology: standards of care in diabetes-2023. Diabetes Care. 2023;46(Supplement_1):S1–S4. doi:10.2337/dc23-Sint
8. Rubino F, Nathan DM, Eckel RH, et al. Metabolic surgery in the treatment algorithm for type 2 diabetes: a joint statement. Diabetes Care. 2016;39(6):861–877. doi:10.2337/dc16-0236
9. Hoerger TJ, Zhang P, Segel JE, Kahn HS, Barker LE, Couper S. Cost-effectiveness of bariatric surgery for severely obese adults with diabetes. Diabetes Care. 2010;33(9):1933–1939. doi:10.2337/dc10-0554
10. Picot J, Jones J, Colquitt JL, et al. The clinical effectiveness and cost-effectiveness of bariatric surgery for obesity: a systematic review and economic evaluation. Health Technol Assess. 2009;13(41):1–190. doi:10.3310/hta13410
11. Borisenko O, Adam D, Funch-Jensen P, et al. Bariatric surgery can lead to net cost savings to health care systems: results from a comprehensive European decision analytic model. Obes Surg. 2015;25(9):1559–1568. doi:10.1007/s11695-014-1567-5
12. Mirghani H, Altedlawi Albalawi I. Metabolic surgery versus usual care effects on diabetes remission: a systematic review and meta-analysis. Diabetol Metab Syndr. 2023;15(1):31. doi:10.1186/s13098-023-01001-4
13. Li Q, Chen L, Yang Z, et al. Metabolic effects of bariatric surgery in type 2 diabetic patients with body mass index <35 kg/m2. Diabetes Obes Metab. 2012;14(3):262–270. doi:10.1111/j.1463-1326.2011.01524.x
14. Lester ELW, Padwal RS, Birch DW, et al. The real-world cost-effectiveness of bariatric surgery for the treatment of severe obesity: a cost-utility analysis. CMAJ Open. 2021;9(2):E673–E679. doi:10.9778/cmajo.20200188
15. Noparatayaporn P, Thavorncharoensap M, Chaikledkaew U, et al. Cost-utility and budget impact analysis of laparoscopic bariatric surgery for obesity with type II diabetes mellitus in Thailand. PLoS One. 2024;19(12):e0315336. doi:10.1371/journal.pone.0315336
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Retrospective Evaluation of Pregnancy Outcomes Following Bariatric Surgery: A Single-Center Experience
Wang X, Liu J, He A, Dong Z, Chen X, Yu S, Gao L, Wang H, Chen W, Hu R, Jiang S, Wang J, Chen Y, Wang C, Yang W, Li R
Diabetes, Metabolic Syndrome and Obesity 2022, 15:3669-3678
Published Date: 25 November 2022
CELESTIA: Cost-Effectiveness Analysis of Empagliflozin Versus Sitagliptin in Patients with Type 2 Diabetes in Greece
Ghetti G, Pradelli L, Papageorgiou G, Karpouzos G, Arikan Y
ClinicoEconomics and Outcomes Research 2023, 15:97-109
Published Date: 17 February 2023
Association of Serum Leptin and Adiponectin Concentrations with Type 2 Diabetes Biomarkers and Complications Among Saudi Women
Mohammed Saeed W, Nasser Binjawhar D
Diabetes, Metabolic Syndrome and Obesity 2023, 16:2129-2140
Published Date: 13 July 2023
The Regulation of Metabolic Homeostasis by Incretins and the Metabolic Hormones Produced by Pancreatic Islets
Reed J, Bain SC, Kanamarlapudi V
Diabetes, Metabolic Syndrome and Obesity 2024, 17:2419-2456
Published Date: 13 June 2024
Relative Effectiveness and Safety of the GLP-1 (Glucagon-Like Peptide 1) Receptor Agonists, Semaglutide and Liraglutide in the Treatment of Obese Type 2 Diabetics: A Prospective Observational Cohort Study in Poland
Hoffmann K, Michalak M, Paczkowska A
Diabetes, Metabolic Syndrome and Obesity 2025, 18:2723-2738
Published Date: 7 August 2025