Back to Journals » Infection and Drug Resistance » Volume 19
Metagenomic Next-Generation Sequencing for Brain Abscess: Improved Pathogen Detection, Targeted Antimicrobial Therapy, and Association with Fewer Surgical Interventions
Authors Li X ![]() , Fan M
, Fan M ![]() , Yue J, Xie J, Zhang Y, Lu X
, Yue J, Xie J, Zhang Y, Lu X ![]() , Liu L, Li X, Huang Y
, Liu L, Li X, Huang Y ![]()
Received 16 April 2026
Accepted for publication 8 July 2026
Published 14 July 2026 Volume 2026:19 617362
DOI https://doi.org/10.2147/IDR.S617362
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Xiangyun Li,1,* Meixiang Fan,2,* Jiang Yue,3 Jiahui Xie,4 Yutu Zhang,5 Xiaozhe Lu,1 Liangliang Liu,1 Xiantao Li,6 Yanyan Huang1,2
1Department of Geriatrics, Huashan Hospital, Fudan University, Shanghai, 200040, People’s Republic of China; 2Department of General Medicine, Huashan Hospital, Fudan University, Shanghai, 200040, People’s Republic of China; 3Department of Endocrinology and Metabolism, Renji Hospital, School of Medicine, Shanghai Jiao Tong University, Shanghai, 200127, People’s Republic of China; 4International Medical Services & VIP Medical Services, Binzhou People’s Hospital, Shandong First Medical University, Binzhou, 256600, People’s Republic of China; 5Department of General Practice, Jing’an Temple Sub-district Community Health Service Center, Shanghai, 200040, People’s Republic of China; 6Department of Critical Care Medicine, Huashan Hospital, Fudan University, Shanghai, 200040, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yanyan Huang; Xiantao Li, Email [email protected]; [email protected]
Background: Brain abscesses demand prompt, accurate pathogen identification; however, identification using conventional culture is limited, especially for anaerobic and polymicrobial infections. We compared the diagnostic and clinical utility of metagenomic next-generation sequencing (mNGS) with that of conventional culture in patients with brain abscess.
Methods: We retrospectively included 115 patients with confirmed brain abscess pathogens. Seventy-two patients underwent both mNGS and conventional culture, and 43 underwent culture alone. We evaluated diagnostic performance, pathogen profiles, adjustments to antimicrobial regimens, and clinical outcomes.
Results: mNGS detected pathogens in 86.1% of patients versus 44.4% for culture (Cohen’s kappa test p=0.004; McNemar’s test p=0.0001). It identified mixed infections in 53.2% of cases, whereas culture predominantly revealed single pathogens. mNGS produced substantially higher detection rates than culture for anaerobic bacteria (50.0% vs 16.7%) and oral-derived bacteria (77.6% vs 61.1%). Antimicrobial regimens were adjusted in 54.2% of patients based on mNGS results; 61.5% of these adjustments involved de-escalation, and vancomycin was discontinued in 77.8% of patients. mNGS use was associated with a lower surgical intervention rate (47.2% vs 65.1%, P = 0.002). There were no differences in length of hospital stay, fever duration, Glasgow Outcome Scale score, or hospitalization costs. In eight patients without reported dental history, mNGS revealed occult odontogenic foci, enabling source control and potentially reducing recurrence risk.
Conclusion: mNGS outperformed conventional culture for detecting mixed infections, anaerobes, and pathogens of d origin. It may inform targeted antimicrobial therapy and assist in identifying the infection source. In this single‑center retrospective study, which is subject to potential selection bias, mNGS use was associated with a lower rate of surgical intervention; however, this finding should be interpreted as an association rather than causation, and prospective studies are needed to confirm this observation. These findings support the integration of mNGS into diagnostic algorithms for brain abscess.
Keywords: brain abscess, metagenomic next-generation sequencing, pathogen, anaerobic bacteria, precision medicine, surgical intervention
Introduction
Despite improvements in surgical drainage and antibiotic therapy, brain abscesses remain life-threatening infections with high mortality rates and substantial neurological complications.1,2 Clinicians face a fundamental challenge in treating brain abscesses: the delay in receiving conventional culture results often means that appropriate antibiotics are not initiated promptly, and empiric treatments may prove ineffective against polymicrobial or fastidious pathogens.3
Culture-based methods are further constrained by prior antibiotic exposure and the fastidious nature of many intracranial pathogens, especially anaerobes; they often reveal only the “tip of the iceberg” of the infecting community.4 This diagnostic gap can lead to inappropriate antibiotic choice and poor clinical outcomes, thus underscoring the urgent need for more comprehensive and rapid pathogen detection approaches.5,6
The surgical management of brain abscess remains an area of ongoing debate. An analysis of 93 brain abscess cases reported that conservative (medical) management was used in 38.0% of patients, aspiration in 47.6%, and excision in 14.2%.7 A 10‑year retrospective study found that 68% of patients underwent surgery, while 32% received conservative treatment.8 However, a nationwide population‑based cohort study demonstrated that a nonoperative strategy was associated with twice the risks of mortality and abscess rupture, and one‑third of patients (33%) initially managed conservatively ultimately required subsequent neurosurgery.9 Clinical guidelines suggest that for abscesses smaller than 2.5 cm, a trial of antibiotics alone may be attempted with close monitoring, whereas abscesses larger than 2.5 cm generally require surgical intervention.10,11 A UK survey of neurosurgical centres found that 88% of neurosurgeons agree with this 2.5 cm threshold for surgical intervention.12 Reported surgical rates for brain abscess range from 33% to 68%. Because lesion size determines both treatment choice and outcomes, it should be included as a mandatory confounder in multivariable logistic regression to avoid confounding by indication.
In recent years, metagenomic next‑generation sequencing (mNGS) has improved the etiological diagnosis of brain abscesses because it requires no predefined targets, has a short turnaround time, and can detect a broad spectrum of pathogens.13 Wang et al demonstrated that mNGS significantly outperforms conventional culture in brain abscess pus samples (85.0% vs 50.0%, P = 0.0181) and cerebrospinal fluid samples (84.2% vs 7.9%, P < 0.0001), with particular advantages for detecting anaerobic pathogens.14 A 2025 study on cryptogenic brain abscesses further found that surgical resection significantly improves cure rates and reduces recurrence risk, particularly for abscesses larger than 2.5 cm or with mixed infections.15 However, most mNGS studies to date have emphasized its technical strengths—high detection rates, rapid turnaround, and broad pathogen coverage—without systematically characterizing the clinical implications.14 The pathogenic potential of detected organisms and their probable anatomic sources of infection remain underexplored. Moreover, few studies have rigorously evaluated how mNGS influences therapeutic decisions or patient outcomes when used as an etiological diagnostic tool. The rationale is that earlier and more comprehensive pathogen identification could enable timely targeted antibiotics, potentially accelerating infection control, reducing abscess size, and thereby obviating the need for surgical drainage in some patients. Critically, it has not yet been systematically assessed whether mNGS‑guided targeted therapy can reduce the need for surgical intervention by arresting infection progression early and avoiding resection in patients who might otherwise fail medical management. Existing evidence is largely derived from case reports or small series, and the scarcity of real‑world cohort studies limits the generalizability of findings.16,17
Recent evidence suggests that mNGS can reduce antimicrobial expenditure and improve diagnostic efficiency compared with traditional cultures in CNS infections, indicating favorable cost‑effectiveness.18 Nevertheless, the effect of mNGS on surgical rates in brain abscess has not been systematically evaluated, representing a critical knowledge gap that we aimed to address in this study.
Huashan Hospital, affiliated to Fudan University, is a national clinical center for both neurological and infectious diseases; it houses leading neurosurgery and infectious disease programs. The hospital has assembled a large cohort of patients with severe, refractory brain abscesses from across China, thereby producing a robust clinical dataset for pathogen‑spectrum analysis. The objectives of the present study were as follows: (1) to delineate the pathogen profile of brain abscesses as revealed by mNGS compared with conventional culture, with particular emphasis on the ability of mNGS to identify anaerobes and mixed infections; and (2) to assess the effects of mNGS results on clinical treatment decisions and to determine whether the integration of mNGS into diagnostic workflows is associated with improved clinical outcomes, particularly regarding the need for surgical intervention.
Materials and Methods
Data Collection
We performed a retrospective analysis of 659 patients diagnosed with brain abscesses at Huashan Hospital, Fudan University from July 2019 to March 2023. Of these, 456 patients were excluded for the following reasons: 288 were hospitalized for routine treatment of recurrent brain abscesses, 126 were transferred from other hospitals with limited available data, 25 refused medical treatment, 13 were suspected cases without confirmed diagnosis, and 2 were confirmed by postoperative pathology to have other brain diseases. The remaining 205 newly defined brain abscess patients were considered for further analysis. Among these, 90 were etiologically negative and were excluded, leaving 115 patients with confirmed pathogens. Samples from 72 of these patients underwent both conventional culture and mNGS and comprised the core analytical cohort; the remaining 43 patients, whose samples underwent conventional culture only, served as the comparator cohort for clinical outcome analyses (Figure 1). Within the core cohort, we compared diagnostic performance, pathogen spectrum, and changes in antimicrobial regimens between mNGS and conventional culture.
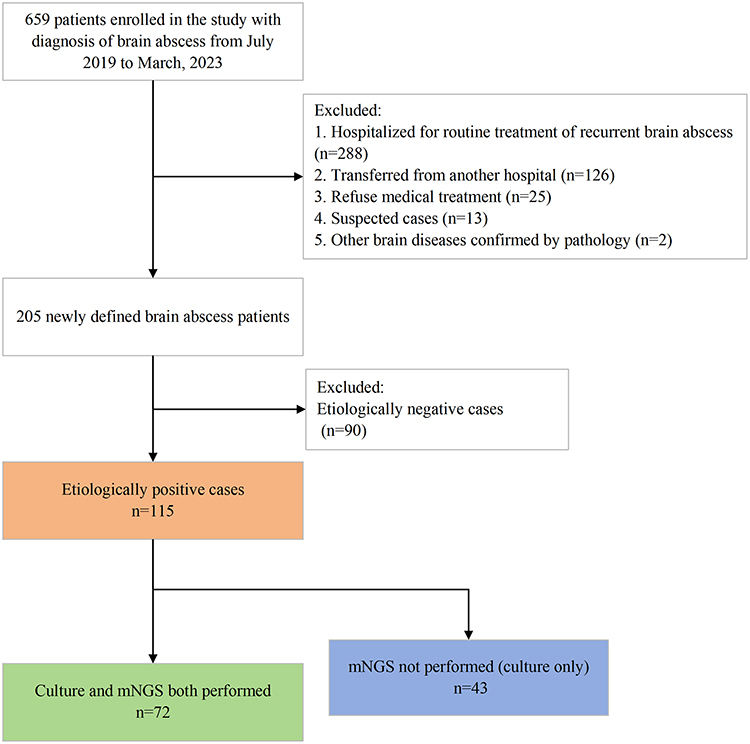 |
Figure 1 The workflow of the study. mNGS, metagenomic next-generation sequencing. |
mNGS was performed at the discretion of the treating physician, typical when empirical antibiotics failed, when anaerobic or fastidious pathogens were suspected, or when the patient was critically ill and required rapid diagnosis. Due to the retrospective nature, the decision was not standardized, which we acknowledge as a limitation. The decision for surgical intervention was made by the treating neurosurgeons based on clinical guidelines, generally for abscesses >2.5 cm in diameter, significant mass effect, or clinical deterioration despite antibiotic therapy. The decision was not blinded to diagnostic methods, reflecting real-world clinical practice. mNGS was introduced at our center during the study period; to account for potential temporal trends in surgical practice and mNGS adoption, year of presentation was included as a covariate in the logistic regression model.
The research was conducted in accordance with the tenets of the Helsinki Declaration and was approved by the Institutional Review Board of Huashan Hospital, Fudan University (IRB Approval No.: KY2024-621).
Microbiological Culture
Conventional microbiological culture was performed on all collected specimens. Samples were inoculated onto blood agar, chocolate agar, and MacConkey agar, and incubated at 37°C under aerobic, anaerobic, and microaerophilic conditions for up to 7 days. Bacterial isolates were identified by standard biochemical tests and matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS). Antimicrobial susceptibility testing was performed using the broth microdilution method according to Clinical and Laboratory Standards Institute (CLSI) guidelines when applicable.
mNGS and Analysis
Sample Collection and Preprocessing
Blood, pus, and cerebrospinal fluid specimens were collected and immediately transferred to 1.5 mL tubes containing 1 g of 0.5 mm glass beads. Tubes were vortexed at 2800–3200 rpm for 30 minutes to achieve complete cell lysis. A 0.3 mL aliquot of each lysate was used for DNA extraction with the TIANamp Micro DNA Kit (DP316, Tiangen Biotech, Beijing, China).
Sequencing Library Preparation
Purified DNA was fragmented to an average size of 150 bp and then underwent end repair, adapter ligation, and polymerase chain reaction amplification. Libraries with 200–300 bp inserts were assessed for quality on an Agilent 2100 Bioanalyzer (Agilent Technologies, Santa Clara, CA, USA) and sequenced on the BGISEQ-200 platform (BGI Group, Guangdong, China).
Bioinformatic Pipeline
Raw sequencing reads were quality-filtered with Trimmomatic v0.39 to remove reads shorter than 35 bp or with average Q-scores below 20. Human-derived reads were removed by aligning to the hg19 and Yanhuang reference genomes using BWA v0.7.17. The remaining reads were aligned to the National Center for Biotechnology Information RefSeq database (downloaded March 2024), which comprised 6,350 bacterial, 4,945 viral, 1,064 fungal, and 234 parasitic genomes.
Interpretation of mNGS Results
Because mNGS cannot distinguish true infection from colonization or from residual nucleic acids from prior therapy,13 we implemented a two-step validation process. First, we applied objective thresholds (≥3 unique reads with relative abundance >1%). Second, two senior attending physicians reviewed the clinical presentations, imaging findings, and treatment outcomes to confirm the pathogenic significance of each detected organism. The two reviewers discussed all discordant cases and reached consensus through joint discussion.
Cost of mNGS Testing
The approximate cost of mNGS testing at our institution was 3,500–4,000 CNY per sample during the study period, which was covered by the patient’s medical insurance or out-of-pocket expenses depending on individual insurance policies.
Statistical Methods
Data collection and charting were performed using Microsoft Excel spreadsheets (Microsoft, Redmond, WA, USA). Sample size determination and power analysis were performed using G*Power software (version 3.1.9.7). The detection rate of conventional culture was approximately 50%, whereas mNGS showed a detection rate of 85%. These values were used for sample size calculation (α = 0.05, power = 0.80, allocation ratio 1:1), yielding a minimum of 27 patients per group (54 total). Accounting for a 15% attrition rate, at least 34 patients per group were required. Baseline characteristics were compared using independent two-sample t-tests, Mann–Whitney U-tests, chi-square tests and Fisher exact test as appropriate. The diagnostic performance of mNGS was compared with conventional culture using McNemar’s test and Cohen’s kappa test. Variables with p < 0.1 were selected as independent variables in a logistic regression model to assess factors associated with surgical intervention. Clinical outcomes were analyzed using t-tests or Mann–Whitney U-tests as appropriate. For secondary outcomes (length of hospital stay, fever duration, Glasgow Outcome Scale score, and hospitalization costs), no adjustment for multiple comparisons was made; these analyses should be considered exploratory. All analyses were performed using SPSS 23.0 (IBM Corp., Armonk, NY, USA). P < 0.05 was considered statistically significant.
Results
General Characteristics
The core cohort comprised 72 patients: 55 men (76.4%) and 17 women (23.6%). The median age was 59 years (IQR 48.5–68). The mean fever duration after admission was 7 days. The most common symptoms were headache (41 patients, 56.9%) and fever (40 patients, 55.6%); however, combined headache and fever (18 patients, 25.0%) was less frequent. Among the underlying diseases, diabetes (22 patients, 30.6%) was the most common, followed by hypertension (19 patients, 26.4%) and tumor (7 patients, 9.7%) in the mNGS + culture group (Table 1). Baseline characteristics of the two groups are summarized in Table 1. Two variables showed possible differences between the groups: alcohol consumption (P=0.082) and deep-seated abscess (P=0.001). Among the 72 patients in the core cohort, specimens included pus (n=38), cerebrospinal fluid (n=52), and blood (n=9). Among the 43 patients in the core cohort, specimens included pus (n=35), cerebrospinal fluid (n=40), and blood (n=3).
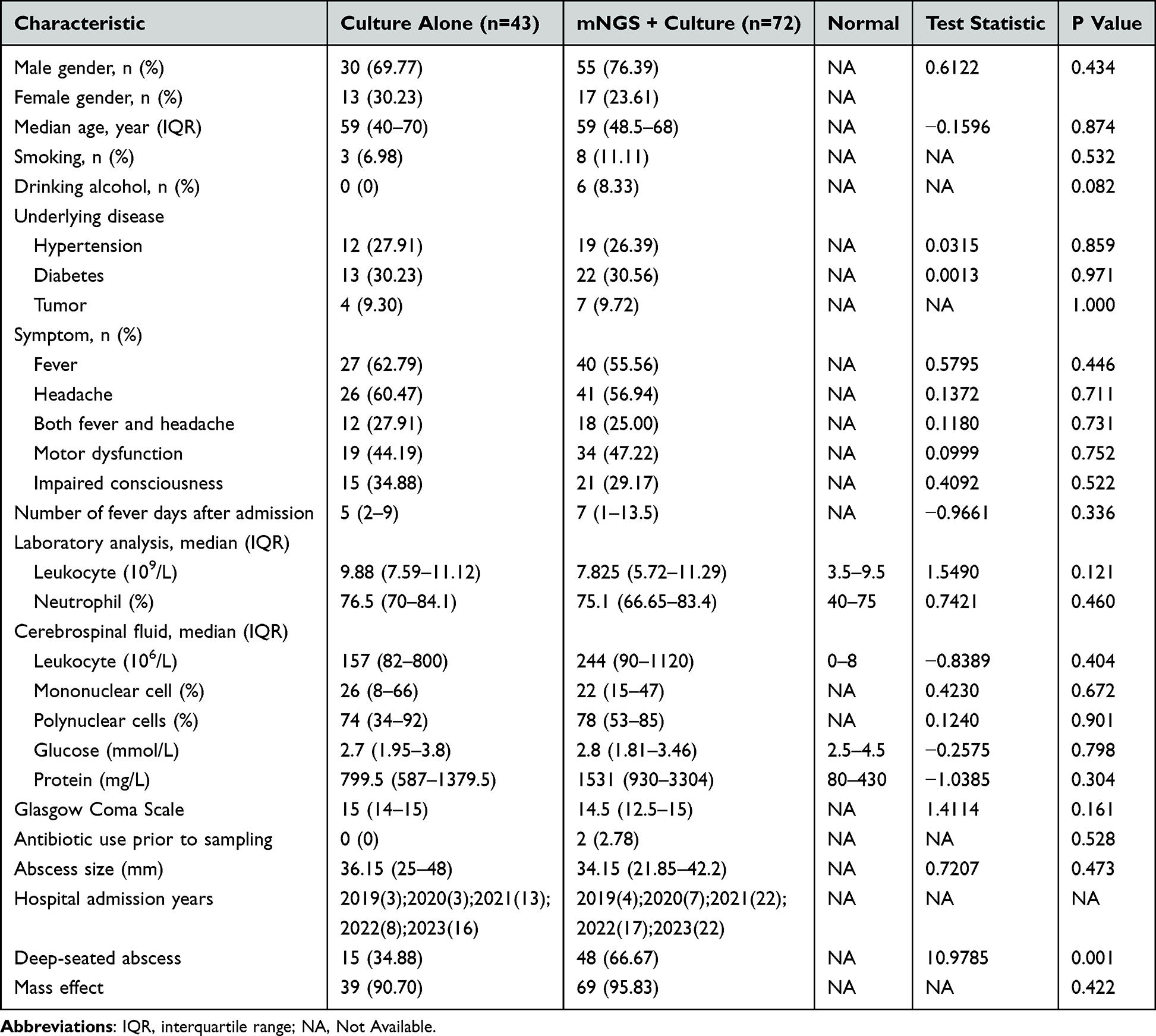 |
Table 1 The General Characteristics of Patients |
Diagnostic Efficiency of mNGS Compared with Conventional Culture Methods for Brain Abscess
In the core cohort of 72 patients, 22 had positive results by both mNGS and conventional culture. Only mNGS detection was positive in 40 cases, and 10 cases showed positive results solely from culture. Consequently, mNGS demonstrated a significantly higher pathogen detection rate (86.1%; 62/72 cases) than conventional culture (44.4%; 32/72 cases; Cohen’s kappa test p=0.004; McNemar’s test p=0.0001) (Figure 2).
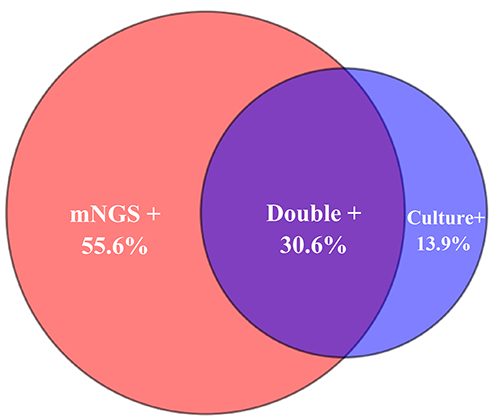 |
Figure 2 The positive rates of pathogen detection by mNGS and conventional culture (n=72). |
Number of Pathogens Isolated of mNGS and Conventional Culture in Brain Abscess Cases
Of the 32 culture-positive patients, 28 had a single pathogen isolated, 4 had two pathogens detected, and none had three or more pathogens identified. By contrast, among the 62 mNGS-positive patients, 27 had one pathogen detected, 12 had two pathogens identified, and 21 had three or more pathogens isolated. Thus, mNGS identified 33 cases of mixed infection, representing 53.2% of the total infections, whereas conventional culture mostly detected only single-pathogen infections. Together, these findings indicate the potential advantages of mNGS for diagnosing mixed infections in brain abscesses (Figure 3).
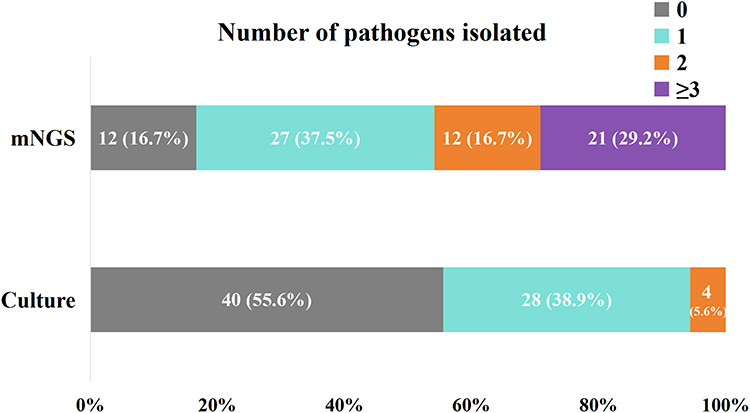 |
Figure 3 Number of pathogen species detected by mNGS and conventional culture (n=72). |
Pathogen Profiles Detected by mNGS and Conventional Culture
The pathogen profiles detected by conventional culture and mNGS are summarized in Table 2, with detailed species lists provided in Tables S1 and S2. Conventional culture identified 36 isolates, comprising 33 bacteria (21 Gram-positive and 12 Gram-negative), 2 fungi, and 1 acid-fast bacillus. The predominant Gram-positive bacteria included Streptococcus spp. (14 isolates, 38.9%) and Staphylococcus spp. (4 isolates, 11.1%). By contrast, the most frequently observed Gram-negative bacteria were Fusobacterium spp. (3 isolates, 8.3%), Aggregatibacter spp. (3 isolates, 8.3%), and Klebsiella spp. (2 isolates, 5.6%). These findings from conventional culture suggest the overwhelming prevalence of Streptococcus spp. and Staphylococcus spp. within the pathogenic spectrum of brain abscesses, despite the detection of other pathogens (Supplementary Table S1).
 |
Table 2 Summary of Pathogen Species Detected by Conventional Culture and mNGS |
mNGS detected a substantially broader range of pathogens than conventional culture, identifying 134 isolates: 129 bacteria (52 Gram-positive and 77 Gram-negative), 2 fungi, 2 viruses, and 1 mycoplasma. The most common Gram-positive bacteria were Streptococcus spp. (28 isolates, 20.9%), Parvimonas spp. (9 isolates, 6.7%), and Actinomyces spp. (5 isolates, 3.7%). Predominant Gram-negative bacteria were Fusobacterium spp. (18 isolates, 13.4%), Porphyromonas spp. (11 isolates, 8.2%), Campylobacter spp. (9 isolates, 6.7%), and Prevotella spp. (7 isolates, 5.2%) (Supplementary Table S2).
Notably, in our study, mNGS and conventional culture yielded markedly different pathogen spectra. Conventional culture mainly recovered Gram-positive bacteria (58.3%, 21/36) rather than Gram-negative bacteria (33.3%, 12/36). By contrast, mNGS detected a higher proportion of Gram-negative bacteria (57.5%, 77/134) than Gram-positive bacteria (38.8%, 52/134) (Figure 4).
 |
Figure 4 Differences in bacterial species distribution between mNGS and conventional culture (n=72). |
Compared to Conventional Culture, mNGS Detected More Anaerobes
Compared with conventional culture, mNGS showed a markedly higher detection rate for anaerobic bacteria (50.0% vs 16.7%). Conventional culture identified anaerobes in 6 of 36 isolates (16.7%), comprising four species: Fusobacterium nucleatum (3 cases), Porphyromonas gingivalis (1 case), Parvimonas micra (1 case), and Bacteroides pyogenes (1 case). By contrast, mNGS detected anaerobes in 67 of 134 isolates (50.0%), spanning 13 species. The top five anaerobic species detected by mNGS were F. nucleatum (18 cases), P. gingivalis (11 cases), P. micra (9 cases), Campylobacter rectus (9 cases), and Tannerella forsythia (6 cases) (Figure 5).
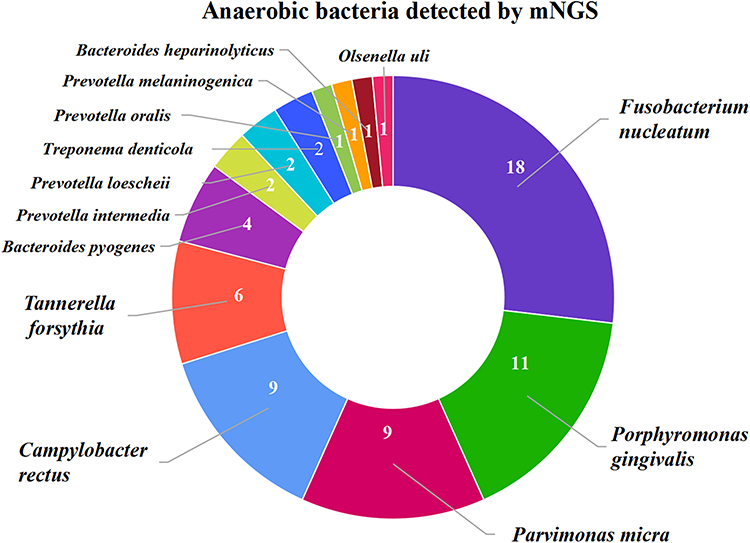 |
Figure 5 Anaerobic bacteria detected by mNGS in brain abscess patients (n=72). |
Analysis of Oral-Derived Pathogens in Brain Abscesses
Conventional culture identified oral-derived bacteria in 22 of 36 isolates (61.1%), representing 10 species. The most frequently detected species by conventional culture were Streptococcus intermedius (7 cases), Streptococcus constellatus (3 cases), F. nucleatum (3 cases), Streptococcus sanguinis (2 cases), and Staphylococcus epidermidis (2 cases). By contrast, mNGS detected oral-derived bacteria in 104 of 134 isolates (104/134, 77.6%), revealing 24 species. The most frequently detected species using mNGS were F. nucleatum (18 cases), S. intermedius (15 cases), P. gingivalis (11 cases), P. micra (9 cases), and C. rectus (9 cases). In addition, in eight patients without reported dental history, mNGS revealed occult odontogenic foci. Overall, both mNGS and conventional culture show that a high proportion of oral-origin bacteria are detected in patients with brain abscesses.
Adjustment of Antibiotic Therapy Based on mNGS Results
mNGS led to changes in antibiotic treatment for 39 patients (54.2%). Among these modifications, 24 patients (61.5%) underwent de-escalation, 12 patients (30.8%) required escalation, and 3 patients (7.7%) received other adjustments, including the addition of antifungal agents (Table 3).
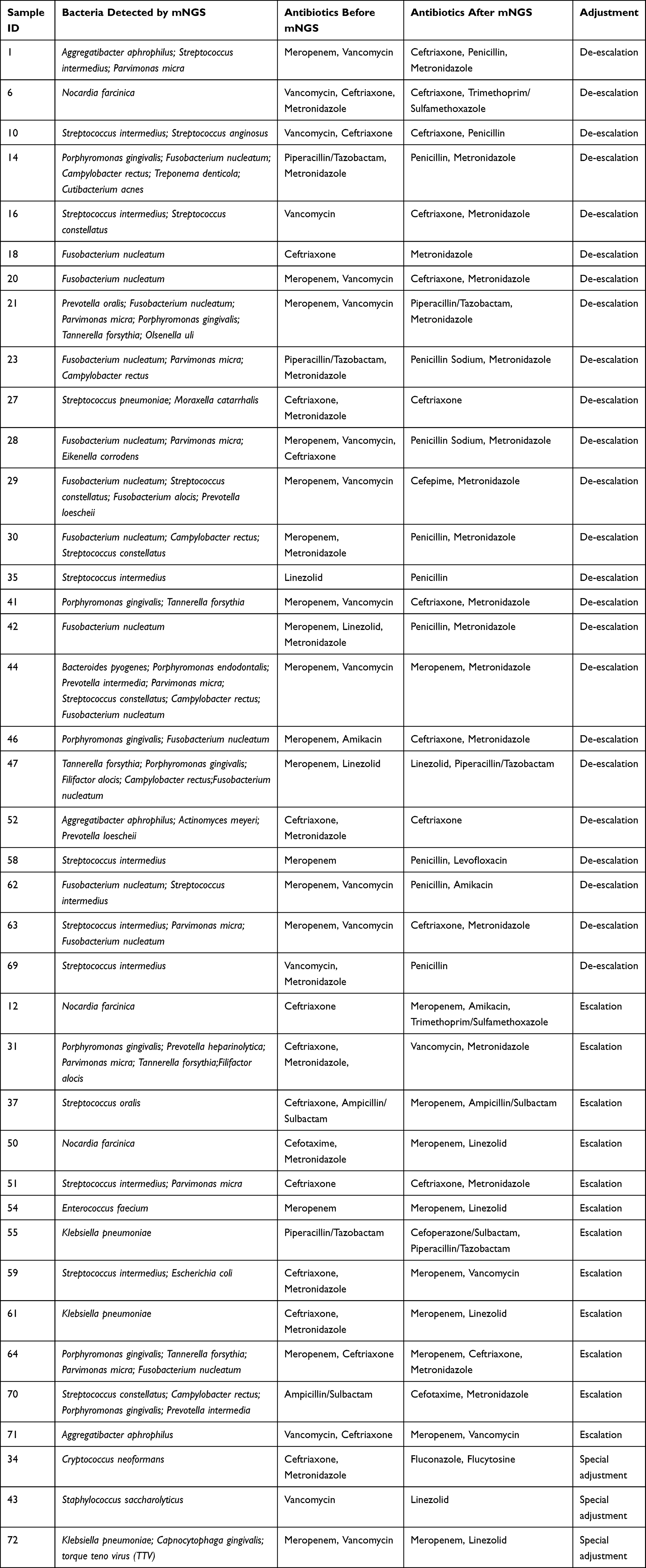 |
Table 3 mNGS-Guided Modifications to Antibiotic Therapy |
A notable pattern emerged in 15 cases underwent de-escalation (15/24, 62.5%): initial broad-spectrum empirical therapy consisting of vancomycin and meropenem was de-escalated to penicillin with or without metronidazole. Among 18 patients who were initially treated with vancomycin, 14 no longer continued vancomycin therapy. None of the 24 patients who underwent de-escalation experienced recurrence or clinical deterioration during the follow-up period.
Among the 12 patients whose therapy was escalated following mNGS, the predominant reason was the detection of pathogens not covered by the initial empirical regimens. Four cases were escalated owing to potentially resistant organisms, including Enterococcus spp. and Klebsiella pneumoniae. Two cases required escalation because Nocardia spp. were identified; these two patients received combination therapy with meropenem, amikacin, and trimethoprim-sulfamethoxazole.
The remaining 33 mNGS-positive patients (45.8%) did not undergo antibiotic regimen changes, because the mNGS results confirmed that the empirical regimen was already appropriate for the detected pathogens, or because the detected organisms were considered contaminants rather than true pathogens after clinical review.
Follow-Up Outcomes
The median follow-up duration for the entire cohort was 24 months (IQR 12–30 months). No recurrence of brain abscess was observed in either the mNGS-guided treatment group or the culture-alone group during the follow-up period.
mNGS-Guided Precision Antibiotic Therapy May Reduce Surgical Intervention in Brain Abscesses
Among the 115 patients with confirmed pathogens, 28 patients in the culture-only group (28/43, 65.1%) underwent surgical intervention, compared with 34 patients in the mNGS-plus-culture group (34/72, 47.2%). In a multivariable logistic regression model adjusting for alcohol consumption and deep-seated abscess, mNGS use remained independently associated with a lower likelihood of surgical intervention (OR = 0.321, 95% CI: 0.125–0.823, P = 0.018) (Table 4).
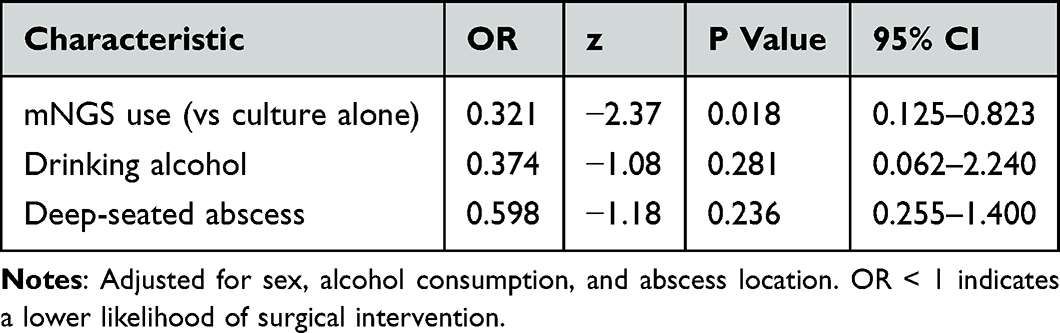 |
Table 4 Multivariable Logistic Regression Analysis of Factors Associated with Surgical Intervention (n = 115) |
Discussion
This study demonstrates that mNGS can detect a broader range of pathogens--with particular advantages in identifying anaerobic bacteria, fastidious organisms, and mixed infections--and further supports antimicrobial stewardship. In the present retrospective study of brain abscesses, mNGS markedly improved pathogen detection rates compared with conventional culture (86.1% vs 44.4%, Cohen’s kappa test p=0.004; McNemar’s test p=0.0001), with particularly large gains for identifying anaerobic bacteria (50.0% vs 16.7%). mNGS-guided antimicrobial therapy may also be associated with a significant reduction in surgical intervention (47.2% vs 65.1%, P = 0.002) and did not worsen clinical outcomes, including length of hospital stay, fever duration, Glasgow Outcome Scale scores, or hospitalization costs.
Our study confirms the diagnostic value of mNGS in central nervous system infections, consistent with recent reports. Wang et al reported a positive detection rate of 85.0% for mNGS in brain abscess pus samples, which was markedly higher than the 50.0% rate achieved by culture.14 Similarly, Qu et al noted that mNGS improved pathogen identification in 77% of brain abscess cases and enabled targeted therapy.19 We further show that mNGS not only enhances diagnostic accuracy but also reveals a pathogen spectrum distinctly different from that of conventional culture. Both methods most frequently identified Streptococcus spp., but mNGS detected a higher proportion of Gram-negative bacteria (57.5% vs 33.3%) and was superior in capturing anaerobic, rare, and fastidious organisms.20,21 Specifically, mNGS identified 13 anaerobic species, whereas culture recovered only four in our study.
Critically, mNGS uncovered that polymicrobial infections are far more common than previously recognized. In our cohort, mNGS identified mixed infections in 33 patients (53.2% of mNGS-positive cases), including 21 patients with three or more pathogens. By contrast, conventional culture detected only four cases with two pathogens and none with three or more. This discrepancy has direct clinical implications: polymicrobial infections tend to follow more complex courses and have higher treatment failure rates when not fully covered, potentially leading to persistent infection, recurrence, or surgical intervention.17,22,23 The ability to resolve complex microbial communities—especially the diverse anaerobic and oral-derived bacteria—allows clinicians to refine antimicrobial regimens with greater precision.4,24
mNGS is valuable for antimicrobial stewardship. Notably, mNGS-guided therapy enabled de-escalation in 61.5% of cases without compromising outcomes, indicating that precise pathogen identification allows rational narrowing of the antimicrobial spectrum.25,26 For example, in 15 patients, empirical vancomycin plus meropenem was de-escalated to penicillin ± metronidazole, reflecting the predominance of anaerobic and streptococcal pathogens.27 Among 18 patients who received empirical vancomycin, 14 (77.8%) discontinued it after mNGS ruled out methicillin-resistant Staphylococcus aureus and other resistant Gram-positive organisms, reducing unnecessary broad-spectrum exposure in line with stewardship principles and potentially lowering the risk of adverse events and resistance.28 Of the 39 patients whose regimens were modified, 22 (56.4%) had metronidazole initiated or optimized after mNGS detected anaerobes (eg, Fusobacterium spp., Prevotella spp., Porphyromonas spp)., underscoring the need for targeted anaerobic coverage in brain abscess management.28 Furthermore, 77.6% of isolates identified by mNGS were oral-derived pathogens, supporting the hypothesis that many brain abscesses originate from oral flora—consistent with previous microbiological studies—and reinforcing the rationale for empirical coverage of oral anaerobes in suspected brain abscess.29–31 The absence of recurrence in 24 patients is underpowered to detect rare events, and that larger studies are needed to confirm the safety of this approach.
A key finding of our study was that mNGS-guided therapy may also be associated with a reduction in surgical interventions. The surgical rate was lower in the mNGS‑plus‑culture group than in the culture‑only group (47.2% vs 65.1%, P = 0.002). In the core cohort, 54.2% of patients had their antimicrobial regimens adjusted based on mNGS results. These data indicate that mNGS allows clinicians to tailor therapies to specific pathogens and potentially control infection without surgical drainage, especially in patients with small abscesses or without significant mass effect.32 In the culture‑only group, the absence of comprehensive and rapid pathogen identification—and thus the inability to guide precise antibiotic therapy—may have lowered the threshold for surgery as a diagnostic or therapeutic measure.
Although mNGS testing incurred additional diagnostic costs (3,500–4,000 CNY per sample at our institution), the lack of significant difference in total hospitalization costs between the two groups may be explained by offsetting savings elsewhere. These could include reduced antibiotic expenditures resulting from early de-escalation, fewer surgical procedures, or shorter durations of intensive care in patients who avoided surgery.
Despite the improved pathogen detection and targeted therapy enabled by mNGS, we did not observe significant differences in length of hospital stay, fever duration, Glasgow Outcome Scale scores, or total hospitalization costs. This apparent paradox warrants careful consideration. Several factors may explain this finding. First, our study may have been underpowered to detect differences in these secondary outcomes, which are influenced by a wide range of confounders not fully captured in this retrospective analysis. Second, for many patients, empirical broad-spectrum antibiotic regimens may have been adequate to cover the most common pathogens (eg, streptococci and anaerobes), such that the incremental clinical benefit of mNGS-guided targeted therapy was modest rather than dramatic. Third, clinical recovery in brain abscess patients is determined by multiple factors beyond infection control, including baseline neurological status, underlying comorbidities, and the extent of mass effect, which may overshadow the impact of earlier pathogen identification. Fourth, although mNGS incurred additional diagnostic costs, these appeared to be offset by savings from antibiotic de-escalation and avoidance of unnecessary procedures, resulting in comparable total costs. These observations suggest that the primary value of mNGS in brain abscess management may lie not in shortening hospital stays or reducing costs, but in enabling precise antimicrobial selection, avoiding unnecessary broad-spectrum exposure, and potentially reducing surgical interventions—benefits that may have longer-term implications for antimicrobial stewardship and patient outcomes. Prospective studies with larger sample sizes are needed to further evaluate the clinical and economic impact of mNGS-guided therapy.
Beyond diagnosis and treatment guidance, mNGS proved valuable for identifying infection sources and preventing recurrence. In our cohort, eight patients without reported dental abscess or periodontitis at presentation had mNGS profiles dominated by periodontal pathogens (eg, F. nucleatum, P. gingivalis, or Prevotella spp). After multidisciplinary consultation with the Department of Stomatology, focused oral examination revealed previously unrecognized dental caries or occult gingival abscesses. Targeted dental interventions—such as the extraction of carious teeth and periodontitis treatment—were then performed. Addressing the primary focus in this way may reduce the risk of brain abscess recurrence. These findings indicate that mNGS not only yields accurate pathogen identification but also aids source tracing via the characteristic microbial signatures of oral-derived pathogens.33,34 Because odontogenic brain abscesses are often clinically silent or overlooked, mNGS may be a critical tool for revealing occult oral foci and enabling the complete eradication of the infectious source, thereby improving long-term outcomes.35,36 We acknowledge that these eight cases represent an anecdotal observation, as systematic dental evaluation was not performed in all patients. This underscores the need for prospective studies with standardized dental screening protocols to determine the true prevalence of odontogenic foci in brain abscess patients.
Practical Considerations for mNGS Implementation
Based on our findings, we suggest that mNGS may be considered in the following scenarios: (1) empirically, in critically ill patients requiring urgent pathogen identification, in immunocompromised patients, or when atypical or polymicrobial infections are suspected; and (2) sequentially, when conventional cultures remain negative after 3–5 days, when culture results are discordant with clinical presentation, or when fastidious or anaerobic pathogens are suspected. For result interpretation, we advocate a hierarchical approach integrating: (a) clinical correlation — match with clinical presentation; (b) abundance assessment — higher read counts and relative abundance (>1%) in sterile sites suggest true infection, whereas low-abundance reads or typical skin flora (eg, Cutibacterium acnes, coagulase-negative Staphylococci) suggest contamination; (c) confirmatory testing — correlation with Gram stain, histopathology, or repeat testing; and (d) treatment response — does the patient respond to targeted therapy? mNGS results should be interpreted by a multidisciplinary team (infectious disease specialists, microbiologists, and neurosurgeons) to guide therapeutic decisions.
Study Limitations
Several limitations merit acknowledgment. First, this was a single-center retrospective study, which may introduce selection bias. Second, mNGS testing was not performed in all patients (72/115), reflecting real-world clinical practice but limiting direct head-to-head comparisons. Third, the modest sample size precluded subgroup analyses by abscess location, size, severity (eg, Glasgow Coma Scale score, neurological deficits, or mass effect), underlying comorbidities, or specimen type (eg, pus, cerebrospinal fluid, or blood). Fourth, interpreting mNGS results requires clinical expertise, meaning that the generalizability of our findings to settings without such expertise may be limited. Fifth, although we observed a lower rate of surgical intervention in patients who received mNGS-guided therapy compared with those managed with culture alone, the retrospective design precludes any causal inference. Whether mNGS directly reduces the need for surgery, or whether the observed difference is attributable to unmeasured confounding (eg, differences in abscess characteristics, clinician judgment, or selection bias), cannot be determined from this study. Prospective randomized trials are required to establish causality. Despite these limitations, the differences in surgical rates and treatment modifications reached significance, and the consistency of our findings across multiple clinical outcomes supports the robustness of our conclusions. The observed difference in surgical rates should be interpreted as an association only.
Conclusion
mNGS markedly enhanced pathogen detection in brain abscesses, particularly for anaerobic, and enabled targeted antimicrobial therapy that may be correlated with fewer surgical interventions without compromising clinical outcomes. The pathogen profiles revealed by mNGS demonstrated a more complex microbial landscape than conventional culture suggested, with mixed infections and anaerobes contributing more substantially than previously appreciated. By identifying oral-derived pathogens, mNGS supports source tracing and permits the detection and management of occult odontogenic foci that might otherwise remain undiagnosed, thereby potentially reducing the recurrence risk. These findings highlight that mNGS is an important diagnostic tool deserving attention for brain abscesses, helping to strengthen antimicrobial stewardship, improve source control, and decrease reliance on invasive procedures. Nonetheless, multicenter prospective studies are warranted to validate our observations and define the optimal role of mNGS in brain abscess management, including evaluations of cost-effectiveness and the effects of mNGS on long-term functional outcomes.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Waiver of Informed Consent
This retrospective observational study was approved by the Institutional Review Board of Huashan Hospital, Fudan University (IRB Approval No.: KY2024-621). All data were derived from de-identified, routinely collected medical records from previous clinical practice. No additional interventions were performed, and the study posed no more than minimal risk to participants.Owing to the long study period, large sample size, and the fact that most patients had been discharged, lost to follow-up, or deceased, it was impracticable to obtain written informed consent from every individual participant.Patient confidentiality was strictly protected; all data were anonymized. The study was conducted in accordance with the Declaration of Helsinki and relevant Chinese ethical regulations. A waiver of informed consent was granted by the ethics committee.
Consent for Publication
Not applicable. This manuscript contains no individual person’s data in any form.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
Xiangyun Li and Meixiang Fan are co-first authors for this study. The authors declare that they have no competing interests in this work.
References
1. Brouwer MC, Tunkel AR, McKhann II GM, van de Beek D. Brain abscess. N Engl J Med. 2014;371(5):447–16. doi:10.1056/NEJMra1301635
2. Bodilsen J, Dalager-Pedersen M, van de Beek D, Brouwer MC, Nielsen H. Long-term mortality and epilepsy in patients after brain abscess: a nationwide population-based matched cohort study. Clin Infect Dis. 2020;71(11):2825–2832. doi:10.1093/cid/ciz1153
3. Widdrington JD, Bond H, Schwab U, et al. Pyogenic brain abscess and subdural empyema: presentation, management, and factors predicting outcome. Infection. 2018;46(6):785–792. doi:10.1007/s15010-018-1182-9
4. Al Masalma M, Armougom F, Scheld WM, et al. The expansion of the microbiological spectrum of brain abscesses with use of multiple 16S ribosomal DNA sequencing. Clin Infect Dis. 2009;48(9):1169–1178. doi:10.1086/597578
5. Hu J, Yu W, Cui J, Zhang L, Yu W. Recent advances in diagnostic technologies for postoperative central nervous system infections: a review. Neurol Sci. 2025;46(9):4279–4291. doi:10.1007/s10072-025-08279-4
6. Darlow CA, McGlashan N, Kerr R, et al. Microbial aetiology of brain abscess in a UK cohort: prominent role of Streptococcus intermedius. J Infect. 2020;80(6):623–629. doi:10.1016/j.jinf.2020.03.011
7. Dhar S, Pal B. Analysis of 93 Brain Abscess Cases to Review the Effect of Intervention to Determine the Feasibility of the Management Protocol: a Tertiary Care Perspective. Asian J Neurosurg. 2021;16(3):483–487. doi:10.4103/ajns.AJNS_467_20
8. Park JS, Sin EG. Clinical Characteristics, Risk Factor and Outcome of Brain Abscess: a Retrospective Analysis During a 10-year Period. J Neurointens Care. 2023;6(2):114–122. doi:10.32587/jnic.2023.00675
9. Eriksen EM, Larsen L, Storgaard M, et al. Nonoperative Versus Neurosurgical Treatment of Brain Abscess: an Emulated Trial Nested Within a Nationwide, Population-Based Cohort. Clin Infect Dis. 2026;82(2):219–227. doi:10.1093/cid/ciaf304
10. NHS. Brain abscess - Treatment. Available from: https://www.nhs.uk/content-widgets/health-a-to-z/brain-abscess/treatment.
11. Brook I. Brain Abscess Treatment & Management. 2025. Available from: https://emedicine.medscape.com/article/212946-treatment.
12. Perea CT, Roy H, Hatcher J, et al. Management of community-acquired brain abscess and intracranial empyema: a survey of UK neurosurgical centres. Eur J Clin Microbiol Infect Dis. 2026. doi:10.1007/s10096-026-05522-4
13. Simner PJ, Miller S, Carroll KC. Understanding the promises and hurdles of metagenomic next-generation sequencing as a diagnostic tool for infectious diseases. Clin Infect Dis. 2018;66(5):778–788. doi:10.1093/cid/cix881
14. Wang X, Guo X, Liu H, et al. Augmented pathogen detection in brain abscess using metagenomic next-generation sequencing: a retrospective cohort study. Microbiol Spectr. 2024;12(10):e0032524. doi:10.1128/spectrum.00325-24
15. Zheng XY, Li DY, Li MH, et al. Precision Treatment of Cryptogenic Brain Abscesses: metagenomic Next-generation Sequencing and Imaging for Recurrence Control. World Neurosurg. 2025;201:124288. doi:10.1016/j.wneu.2025.124288
16. Liu Y, Zhu W, Jiao M, Guo W, Luo Y. Clinical application value of metagenomic next-generation sequencing in the diagnosis of central nervous system infections. Front Bioeng Biotechnol. 2023;11:885877. doi:10.3389/fbioe.2023.885877
17. Yu H, Liang D, Ding X, et al. Comparison of microbial culture, metagenomic next-generation sequencing and droplet digital polymerase chain reaction methods for pathogen detection in patients with neurosurgical central nervous system infection. Front Cell Infect Microbiol. 2025;15:1606283. doi:10.3389/fcimb.2025.1606283
18. Tian Y, Xu N, Chen Y, et al. Cost-effectiveness analysis of metagenomic next-generation sequencing versus traditional bacterial cultures for postoperative central nervous system infections in critical care settings: a prospective pilot study. Front Cell Infect Microbiol. 2025;15:1710412. doi:10.3389/fcimb.2025.1710412
19. Qu C, Chen Y, Ouyang Y, et al. Metagenomics next-generation sequencing for the diagnosis of central nervous system infection: a systematic review and meta-analysis. Front Neurol. 2022;13:989280. doi:10.3389/fneur.2022.989280
20. Liang Y, Lin M, Qiu L, et al. Clinical characteristics of hospitalized patients with Nocardia genus detection by metagenomic next generation sequencing in a tertiary hospital from southern China. BMC Infect Dis. 2023;23(1):772. doi:10.1186/s12879-023-08615-z
21. Lan ZW, Xiao MJ, Guan YL, Zhan YJ, Tang XQ. Detection of Listeria monocytogenes in a patient with meningoencephalitis using next-generation sequencing: a case report. BMC Infect Dis. 2020;20(1):721. doi:10.1186/s12879-020-05447-z
22. Stebner A, Ensser A, Geißdörfer W, Bozhkov Y, Lang R. Molecular diagnosis of polymicrobial brain abscesses with 16S-rDNA-based next-generation sequencing. Clin Microbiol Infect. 2021;27(1):76–82. doi:10.1016/j.cmi.2020.03.028
23. Kommedal Ø, Wilhelmsen MT, Skrede S, et al. Massive parallel sequencing provides new perspectives on bacterial brain abscesses. J Clin Microbiol. 2014;52(6):1990–1997. doi:10.1128/JCM.00346-14
24. Zhu XM, Dong CX, Xie L, Liu HX, Hu HQ. Brain abscess from oral microbiota approached by metagenomic next-generation sequencing: a case report and review of literature. World J Clin Cases. 2024;12(3):616–622. doi:10.12998/wjcc.v12.i3.616
25. Hu HL, Guo LY, Wu HL, Feng WY, Chen TM, Liu G. Evaluation of next-generation sequencing for the pathogenic diagnosis of children brain abscesses. J Infect. 2019;78(4):323–337. doi:10.1016/j.jinf.2019.01.003
26. Yang H, Xu N, Yan M, et al. Comparison of metagenomic next-generation sequencing and conventional culture for the diagnostic performance in febrile patients with suspected infections. BMC Infect Dis. 2024;24(1):350. doi:10.1186/s12879-024-09236-w
27. Al Masalma M, Lonjon M, Richet H, et al. Metagenomic analysis of brain abscesses identifies specific bacterial associations. Clin Infect Dis. 2012;54(2):202–210. doi:10.1093/cid/cir797
28. Dyar OJ, Huttner B, Schouten J, Pulcini C. What is antimicrobial stewardship? Clin Microbiol Infect. 2017;23(11):793–798. doi:10.1016/j.cmi.2017.08.026
29. Omland LH, Nielsen H, Bodilsen J. Update and approach to patients with brain abscess. Curr Opin Infect Dis. 2024;37(3):211–219. doi:10.1097/QCO.0000000000001014
30. Roy H, Bescos R, McColl E, et al. Oral microbes and the formation of cerebral abscesses: a single-centre retrospective study. J Dent. 2023;128:104366. doi:10.1016/j.jdent.2022.104366
31. Bodilsen J, Mariager T, Duerlund LS, et al. Brain abscess caused by oral cavity bacteria: a nationwide, population-based cohort study. Clin Infect Dis. 2024;78(3):544–553. doi:10.1093/cid/ciad678
32. Thy M, Gaudemer A, d’Humières C, Sonneville R. Brain abscess in immunocompetent patients: recent findings. Curr Opin Infect Dis. 2022;35(3):238–245. doi:10.1097/QCO.0000000000000833
33. Tian C, Liu J, Chen Z, Li L. Case report: analysis of the efficacy and safety of anti-infectious treatment for brain abscess caused by oral anaerobes. Front Pharmacol. 2025;16:1506879. doi:10.3389/fphar.2025.1506879
34. Sun S, He R, Chen S, Ren J, Ma X, Yang J. Odontogenic brain abscess caused by Porphyromonas gingivalis and Streptococcus constellatus: a case report and review article. J Oral Microbiol. 2025;17(1):2485197. doi:10.1080/20002297.2025.2485197
35. Heintz E, Pettengill MA, Gangat MA, Hardy DJ, Bonnez W, Sobhanie MM. Oral flora meningoencephalitis diagnosis by next-generation DNA sequencing. Access Microbiol. 2019;1(9):e000056. doi:10.1099/acmi.0.000056
36. Wei J, Zhong F, Sun L, Huang CY. Brain abscess of odontogenic origin: a case report and literature review. Medicine. 2023;102(48):e36248. doi:10.1097/MD.0000000000036248
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Clinical Evaluation of Metagenomic Next-Generation Sequencing and Identification of Risk Factors in Patients with Severe Community-Acquired Pneumonia
Lu D, Abudouaini M, Kerimu M, Leng Q, Wu H, Aynazar A, Zhong Z
Infection and Drug Resistance 2023, 16:5135-5147
Published Date: 9 August 2023
Awareness and Predictors of the Use of Bioinformatics in Genome Research in Saudi Arabia
Alomair L, Abolfotouh MA
International Journal of General Medicine 2023, 16:3413-3425
Published Date: 11 August 2023
Clinical Utility and Therapeutic Strategy Value of Metagenomic Next-Generation Sequencing in Pulmonary Infection Among Cancer Patients
Cao Y, Huang J, Wu W, Xu Z, Wang C, Wu X, Zhan C, Xing J, Liu J, Zhu M, Ma S
Infection and Drug Resistance 2026, 19:568562
Published Date: 13 February 2026
Detection Blind Spots in Microbial Culture, tNGS, and mNGS: Anaerobic Bacterial Infections in the Lung—A Retrospective Analysis of Two Cases
Zhuang J, Yu Z, Jin C, Qiu H, Wu Y, Feng Q, Zheng S, Wang J
Infection and Drug Resistance 2026, 19:611567
Published Date: 9 July 2026