Back to Journals » Therapeutics and Clinical Risk Management » Volume 21
Medicinal Plants for Chemotherapy-Induced Nausea and Vomiting: A Systematic Review of Antiemetic, Chemosensitizing, and Immunomodulatory Mechanisms
Authors Sun X, Nie F, Sun J, Zhang J ![]() , Wang Y
, Wang Y ![]()
Received 1 April 2025
Accepted for publication 20 July 2025
Published 31 July 2025 Volume 2025:21 Pages 1187—1218
DOI https://doi.org/10.2147/TCRM.S531645
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor De Yun Wang
Xue Sun,1,2 Fangfang Nie,1,2 Jizhuo Sun,1,2 Jingdong Zhang,2 Yuanhe Wang2
1The First Clinical College, Liaoning University of Traditional Chinese Medicine, Shenyang, Liaoning Province, People’s Republic of China; 2Medical Oncology Department of Gastrointestinal Cancer, Cancer Hospital of Dalian University of Technology, Liaoning Cancer Hospital & Institute, Shenyang, Liaoning Province, People’s Republic of China
Correspondence: Yuanhe Wang, Medical Oncology Department of Gastrointestinal Cancer, Cancer Hospital of Dalian University of Technology, Liaoning Cancer Hospital & Institute, No. 44 Xiaoheyan Road, Dadong District, Shenyang, Liaoning Province, 110042, People’s Republic of China, Tel +8618900918737, Email [email protected]
Background: Chemotherapy-induced nausea and vomiting (CINV) is a major burden for cancer patients, often poorly managed by conventional antiemetics, prompting exploration of medicinal plant therapies for better supportive care.
Objective: This systematic review critically evaluates medicinal plants for CINV, detailing bioactive compounds, diverse antiemetic mechanisms, and promising chemosensitizing and immunomodulatory properties.
Methods: A comprehensive literature search and critical analysis of studies investigating medicinal plants for CINV were performed.
Key Findings: This review synthesizes evidence for 22 botanicals. Ginger (gingerols, shogaols) acts via 5-hydroxytryptamine 3 (5-HT₃) receptor antagonism and substance P/neurokinin-1 (NK-1) inhibition, and offers chemosensitization by downregulating P-glycoprotein. Cannabis (THC, CBD) modulates the endocannabinoid system and 5-HT₃ receptors for CINV relief and may enhance chemotherapy sensitivity. Mint (menthol, menthone) relaxes gastrointestinal smooth muscle and offers anti-inflammatory benefits. Chamomile (apigenin) has antispasmodic/anxiolytic effects; its apigenin also sensitizes cancer cells to chemotherapy. Turmeric (curcumin) acts on neurotransmitter systems, offers potent anti-inflammatory/antioxidant effects, and boosts chemosensitivity via NF-κB/P-gp modulation. Plants like Pinellia ternata, lemon, fennel, and licorice show varied mechanisms (gastrointestinal regulation, anti-inflammatory, neurotransmitter modulation). Many botanicals show chemosensitizing (inhibiting efflux pumps, promoting apoptosis) and immunomodulatory (affecting cytokines, immune cells) properties. Synergistic plant combinations (eg, ginger with P. ternata or turmeric) are noted for enhanced efficacy and safety.
Conclusion: Medicinal plants offer a compelling, multi-targeted approach for CINV management, with potential beyond symptomatic relief via their antiemetic, chemosensitizing, and immunomodulatory actions. Rigorous clinical trials are needed to integrate these botanicals into evidence-based supportive cancer care.
Keywords: cancer, chemotherapy, complementary medicine, herbal medicine, nausea, vomiting
Introduction
Cancer remains a significant global health challenge, with advancements in treatment extending survival but often accompanied by debilitating side effects. CINV is a particularly distressing adverse event, affecting up to 80% of patients and profoundly impairing their quality of life and adherence to treatment regimens.1 CINV is classified based on its onset into acute (within 24 hours post-chemotherapy), delayed (24 hours to 5 days post-chemotherapy), and anticipatory (a conditioned response prior to treatment). The emetogenicity of the chemotherapy agents and individual patient factors significantly influence its severity. Uncontrolled CINV can lead to serious complications such as dehydration, electrolyte imbalances, malnutrition, and esophageal tears (eg, Mallory-Weiss syndrome), thereby increasing healthcare utilization and diminishing overall patient well-being.2 Effective CINV management is therefore a critical component of optimal cancer care.
Current antiemetic prophylaxis, guided by organizations like the Multinational Association of Supportive Care in Cancer/European Society for Medical Oncology (MASCC/ESMO) and the American Society of Clinical Oncology (ASCO), primarily involves 5-HT3RAs (eg, ondansetron, granisetron), NK1RAs (eg, aprepitant), and corticosteroids (eg, dexamethasone).3 While these standard antiemetics form the cornerstone of CINV prevention, particularly for highly and moderately emetogenic chemotherapy, they often provide suboptimal control and are associated with a range of adverse effects, including headache, gastrointestinal discomfort, constipation, and metabolic complications such as hyperglycemia.4 Indeed, even with prophylactic administration, a substantial proportion of patients, approximately 35% and 13% respectively, still report experiencing acute nausea and vomiting.5 This highlights a significant unmet need for safer and more comprehensively effective antiemetic strategies.
Medicinal plants have a long history of use in managing nausea and vomiting and are gaining increasing interest as complementary therapies in oncology. This interest is fueled by an expanding body of scientific evidence suggesting their potential to offer multi-targeted antiemetic actions, often with a more favorable side-effect profile compared to conventional drugs. However, previous reviews in this area have often provided a general overview without a deep, mechanism-based synthesis of how these botanicals exert their effects, particularly concerning their interactions with CINV-specific pathways. Furthermore, there has been a lack of critical evaluation of their potential for synergistic combinations or their capacity to act as chemosensitizers, which could enhance the efficacy of chemotherapy while mitigating its toxicity. For instance, while ginger (Zingiber officinale Roscoe), mint (Mentha spp)., and chamomile (Matricaria recutita) are recognized for their bioactive compounds, a comprehensive understanding of how these compounds modulate CINV pathways, potentially enhance chemosensitivity, or offer immunomodulatory benefits alongside antiemesis is still developing. The potential for synergistic interactions, such as that observed with Pinellia ternata and ginger,6 also remains an underexplored area that could optimize therapeutic outcomes.
This review aims to critically evaluate medicinal plants for CINV management with a specific focus on their underlying mechanistic pathways, their potential for chemosensitization, and the exploration of synergistic plant combinations to enhance integrative cancer care. By synthesizing current knowledge on bioactive constituents, their molecular targets in CINV, and their broader pharmacological effects, this review seeks to provide a robust evidence base to inform future research and the potential integration of phytotherapy into supportive oncology.
Pathophysiology and Treatment Options for CINV
CINV is classified into three distinct stages based on the timing of onset following chemotherapy administration: acute, delayed, and anticipatory. Acute CINV occurs within 24 hours of treatment, with vomiting predominantly mediated by 5-HT3 receptors. Despite the use of antiemetic prophylaxis, up to 35% of patients still experience acute nausea, and approximately 13% suffer from acute vomiting. Delayed CINV arises between 24 hours and 5 days after chemotherapy, primarily mediated by the binding of substance P to NK1 receptors in the central nervous system.7 Following prophylaxis, the incidence of delayed CINV ranges from 20% to 50%.8 Anticipatory CINV refers to nausea and vomiting occurring before chemotherapy, a conditioned response often linked to prior experiences of CINV, and is likely mediated by a combination of physiological and psychological mechanisms. The multifactorial nature of CINV presents a considerable challenge for effective management through conventional pharmaceutical approaches alone.
As illustrated in Figure 1, the mechanisms underlying CINV are multifaceted. CINV arises from a complex interaction of peripheral and central mechanisms, complicating its management. Peripherally, serotonin (5-HT) released from enterochromaffin cells, which produce approximately 80% of the body’s serotonin, is triggered by intestinal irritation or tumor-induced damage. This serotonin binds to 5-HT3 receptors on vagal afferent neurons, initiating signals that reach the chemoreceptor trigger zone (CTZ) in the brain. Subsequently, the CTZ sends signals to the vomiting center, which generates efferent impulses that activate the respiratory and abdominal muscles, leading to emesis. The central mechanism involves substance P, which is concentrated in the CTZ and stimulates NK1 receptors. Substance P also acts on vagal afferents in the gut, amplifying the emetic signal. Additionally, several other receptors contribute to the complexity of CINV, including cannabinoid-1 (CB1), dopamine D2 and D3, histamine H1, muscarinic M3 and M5, and gamma-aminobutyric-B (GABA-B) receptors. This broad receptor involvement underscores the intricate nature of CINV and emphasizes the need for multi-targeted therapeutic strategies.9
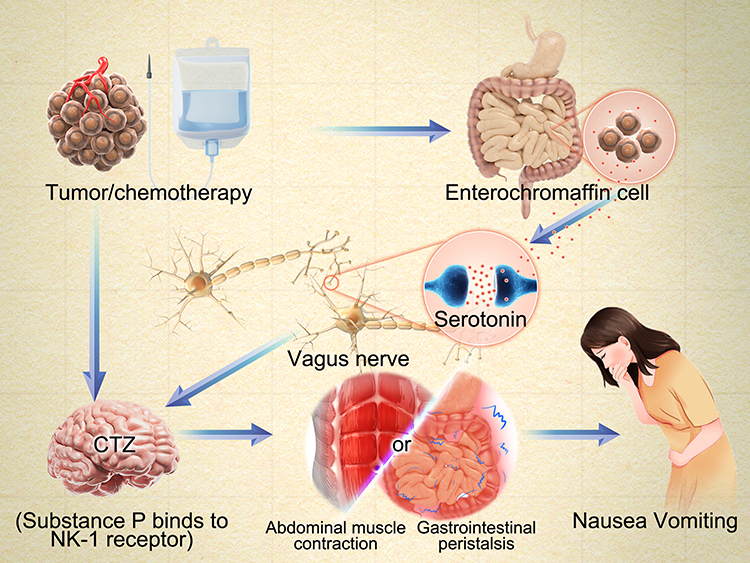 |
Figure 1 Key Peripheral and Central Neurochemical Pathways in Chemotherapy-induced nausea and vomiting (CINV) Targeted by Standard Antiemetic Therapies. This diagram illustrates the primary mechanisms of CINV targeted by conventional antiemetics. Emetogenic signals are initiated via two main routes. Peripheral Pathway: Chemotherapy or tumor factors damage gastrointestinal enterochromaffin cells, releasing serotonin. 5-hydroxytryptamine (5-HT) activates 5-hydroxytryptamine type 3 receptor (5-HT3) on vagal afferents, transmitting emetic signals to the central nervous system. Central Pathway: Signals from the vagus nerve and direct effects of chemotherapy converge on the Chemoreceptor Trigger Zone (CTZ) in the brainstem. Here, substance P activates Neurokinin-1 (NK-1) receptors, further propagating emetic signals. Both pathways relay information to the vomiting center, which coordinates abdominal muscle contractions and altered gastrointestinal peristalsis, leading to nausea and vomiting. |
As shown on the left side of Figure 2, the primary targets of standard antiemetic therapies are key neurochemical pathways involved in the control of vomiting. Antiemetic treatments aim to control vomiting through neurochemical pathways. Antiemetics often exert their effects through competitive blockade of receptors in the CTZ and possibly the vomiting center, thus mitigating peripheral nerve stimulation. Combination antiemetic regimens are now standard practice in CINV management. For patients receiving highly emetogenic chemotherapy (HEC), like cisplatin or anthracycline-cyclophosphamide (AC) combinations (conferring a >90% risk of emesis), major oncology organizations (eg, MASCC/ESMO, NCCN, and ASCO) recommend triple therapy comprising a 5-HT3 receptor antagonist (5-HT3RA), an NK1 receptor antagonist (NK1RA), and dexamethasone. A quadruple regimen, which includes olanzapine in addition to the triple therapy, is also an option. NK1 receptor antagonists used in CINV prevention include aprepitant (oral) and fosaprepitant (IV), which are typically combined with a 5-HT3RA and dexamethasone. The fixed oral combination of netupitant (NK1RA) and palonosetron (5-HT3RA), known as NEPA, can be administered alone or in conjunction with dexamethasone.10 However, these conventional treatments often fall short of providing complete symptom control, particularly in the cases of delayed and anticipatory CINV.
 |
Figure 2 Comparative Overview of Antiemetic Mechanisms: Standard Pharmacological Agents Versus Selected Medicinal Plants and Their Bioactive Components in the Management of Chemotherapy-induced nausea and vomiting (CINV). This figure contrasts mechanistic targets of conventional antiemetics (left) with diverse pathways of medicinal plants (right) in CINV. Standard antiemetics target specific receptors; medicinal plants often use multiple synergistic mechanisms (receptor modulation, anti-inflammatory, GI regulation). Left Panel: Conventional CINV drugs target specific neurochemical pathways. Neurokinin-1 Receptor Antagonist (NK-1RA): aprepitant. Corticosteroids: dexamethasone. 5-hydroxytryptamine type 3 receptors antagonist(5-HT3RA): ondansetron (See Figure 1 for standard CINV pathway details). Right Panel: Medicinal plants offer multi-targeted CINV approaches, grouped by predominant mechanisms. Cannabidiol (CBD) system regulation: CBD. Dopamine (DA) Receptor Inhibition: Zingiber officinale (Z.O.). NK-1RA: Z.O. and Curcumin (CUR). Olfactory Pathway Regulation (Aromatherapy): Citrus limon (C.L.) and Mentha spicata (M.S.). Plant-Based 5-HT3 Receptor Antagonism: Z.O., CBD, C.L., CUR, Glycyrrhiza glabra (G.G.), Pinellia ternata (PPT), Evodia rutaecarpa (E.R.) and Panax ginseng (P.G.). Anti-inflammatory Effects: All (Refers to all medicinal plants mentioned in the article as contributing to this general mechanism). Gastrointestinal (GI) Activity Regulation: All. |
Medicinal Plants Used to Treat CINV
As shown on the right side of Figure 2, medicinal plants target several key mechanisms involved in antiemetic action, including CBD regulation, DA receptor inhibition, NK-1 receptor antagonism, olfactory pathway modulation, 5-HT3 receptor antagonism, anti-inflammatory effects, and regulation of gastrointestinal activity. Table 1 provides a summary of the active compounds, antiemetic mechanisms and Table 2 provides a summary of the chemosensitization, and immunomodulatory mechanisms of 17 medicinal plants. The following outlines the detailed mechanisms of action for specific medicinal plants.
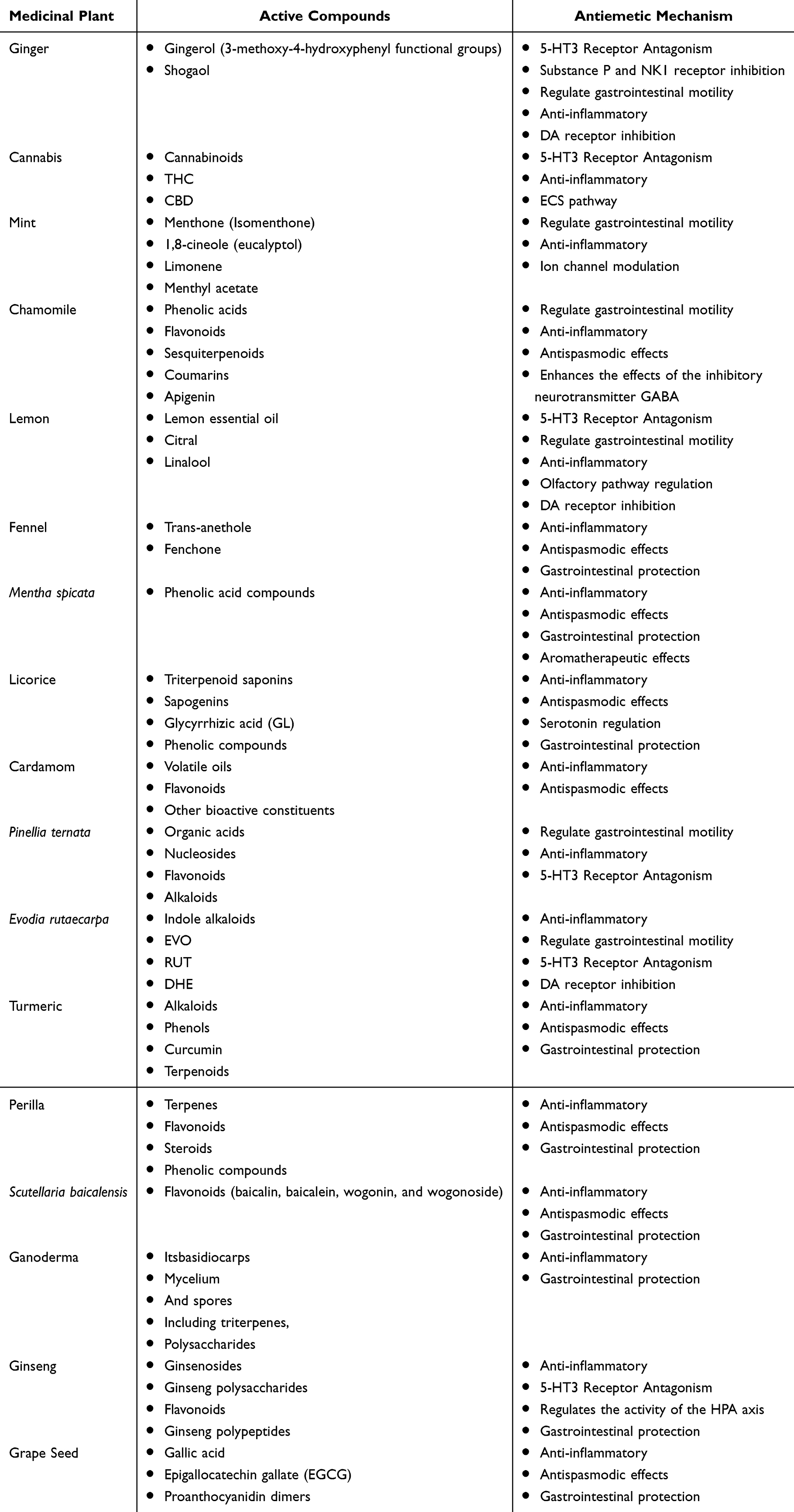 |
Table 1 Active Compounds and Antiemetic Mechanisms of Medicinal Plants |
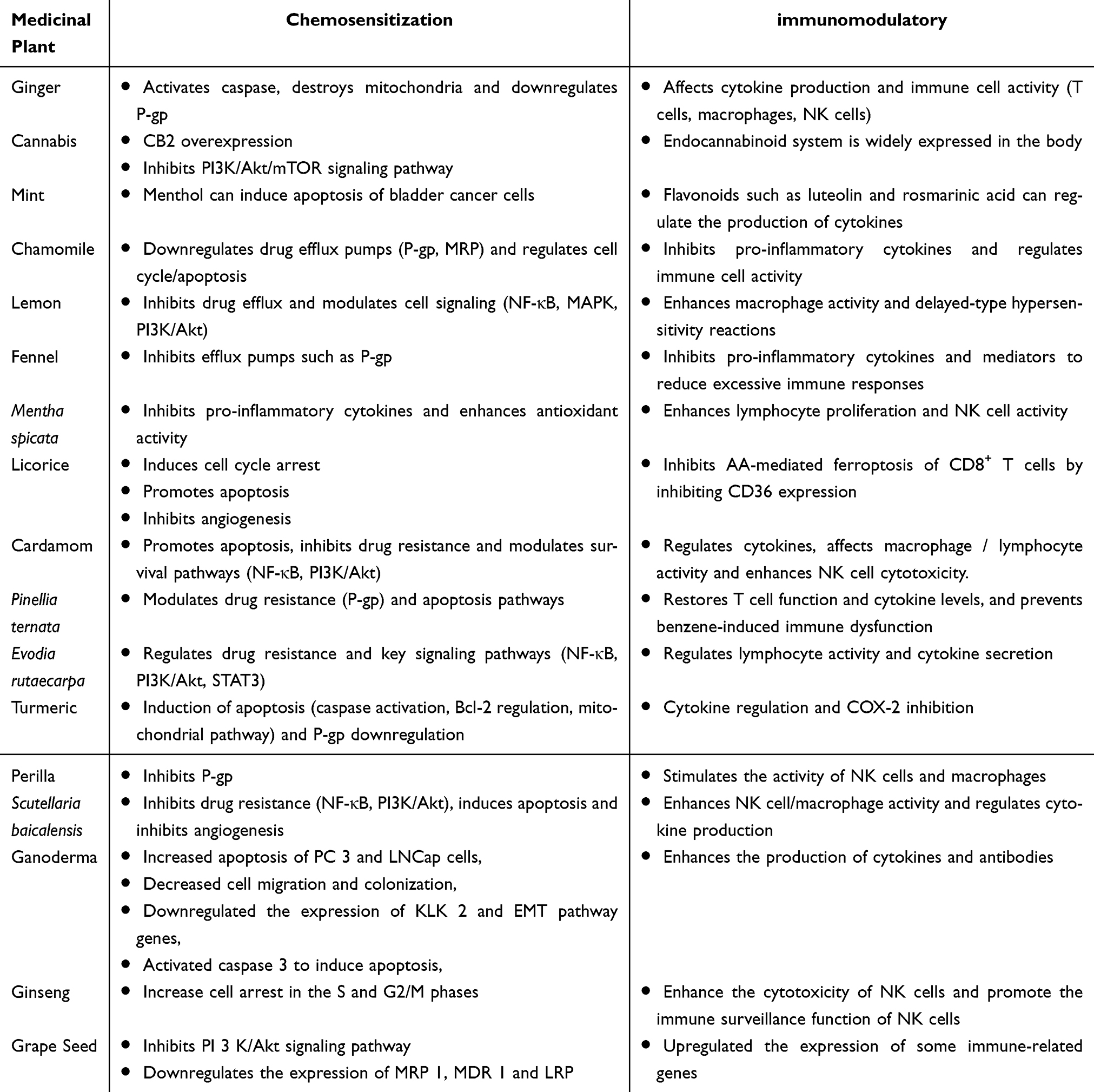 |
Table 2 Chemosensitization, and Immunomodulatory Mechanisms of Medicinal Plants |
Ginger (Zingiber officinale Roscoe)
Ginger is a perennial herb, with the rhizome being the primary medicinal part. Its color ranges from light yellow to gray-brown, and it is characterized by an irregular, thick, branched, fleshy, and scaly structure, accompanied by a fragrant and spicy aroma.11 Ginger has demonstrated efficacy in managing various gastrointestinal disorders, including nausea, vomiting, dyspepsia, and diarrhea. Its therapeutic benefits extend to respiratory ailments and inflammatory conditions such as arthritis. Furthermore, ginger has proven effective in alleviating nausea and vomiting associated with pregnancy, postoperative recovery, and motion sickness.4 Since the early 20th century, numerous bioactive compounds have been isolated from ginger, with gingerol (particularly the 3-methoxy-4-hydroxyphenyl analogs) and shogaol being primarily responsible for its antiemetic effects.12
Antiemetic Mechanism
Serotonin (5-HT₃) Receptor Antagonism
Gingerols, notably 6-gingerol, 8-gingerol, and 8-shogaol, exhibit potent 5-HT3 receptor antagonism, a key mechanism in CINV management. In vitro studies using HEK 293 cells and human colon tissue have demonstrated that 6-gingerol and 6-shogaol effectively inhibit 5-HT-induced calcium influx via 5-HT3 receptors. Furthermore, 6-gingerol has been shown to mitigate cisplatin-induced pica in rats by suppressing the 5-HT system. This suppression is achieved through a reduction in tryptophan hydroxylase (TPH) levels coupled with increased monoamine oxidase A (MAO-A) and serotonin transporter (SERT) levels, ultimately decreasing serotonin levels and inhibiting both central and peripheral 5-HT3 receptor activation. Given the critical role of 5-HT3 receptor activation in CINV, the serotonin-lowering effects of gingerols contribute to their potent antiemetic action by suppressing 5-HT3 receptor activity both centrally and peripherally.13
Substance P and Neurokinin-1 (NK1) Receptor Inhibition
Gingerol also exerts antiemetic effects by modulating substance P and NK-1R activity, which are crucial in the pathophysiology of CINV. Qian et al demonstrated a dose-dependent reduction in vomiting frequency in a cisplatin-treated mink model following gingerol administration. Immunohistochemical analysis revealed that gingerol attenuated the cisplatin-induced upregulation of substance P and NK-1R expression in ileal tissues and the area postrema, suggesting that gingerol’s antiemetic mechanism involves suppression of both central and peripheral substance P/NK-1R signaling.14 In additional studies with rat and mink models, gingerol mitigated cisplatin-induced emesis and the associated damage to the area postrema and ileum, further supporting the involvement of the SP/NK-1R pathway in gingerol’s antiemetic action.15
Regulate Gastrointestinal Motility, Anti-Inflammatory and Antioxidant Effects
Gastric emptying disorder is a recognized pathophysiological factor contributing to gastrointestinal (GI) diseases such as functional dyspepsia and nausea. Ginger has been shown to enhance gastrointestinal motility by increasing the tone and peristalsis of intestinal smooth muscle. By accelerating gastric emptying and shortening transit time, ginger alleviates gastric stasis and indigestion, thereby reducing nausea associated with delayed gastric emptying. Ginger’s gingerols and shogaols act on cholinergic M3 and serotonergic 5-HT3 receptors to promote gastrointestinal motility. A clinical trial demonstrated that ginger extract significantly accelerated gastric emptying and stimulated antral contractions compared to placebo in healthy individuals.16 Ginger also possesses anti-inflammatory properties that may contribute to its antiemetic effects. Bischoff-Kont et al reported that prophylactic ginger extract administration significantly reduced serum pro-inflammatory cytokines, including TNF-α and IL-6, in chemotherapy patients. This reduction in systemic inflammation correlated with decreased CINV frequency and severity, suggesting that ginger’s anti-inflammatory action plays a role in CINV mitigation.17 Additionally, ginger’s potent antioxidant capacity plays a role in its antiemetic effects. Bioactive components, such as 6-shogaol, 6-gingerol, and oleoresins, scavenge reactive oxygen species (ROS) and protect against oxidative stress, which can contribute to nausea. This antioxidant activity, potentially mediated by Nrf2 pathway activation, may help support gastrointestinal health, thus indirectly alleviating nausea and vomiting.18
Dopamine Receptor Inhibition
DA receptor antagonism within the CTZ is a key mechanism for controlling nausea and vomiting, particularly in CINV, postoperative nausea and vomiting (PONV), and motion sickness. Cisplatin disrupts gut dopaminergic signaling, as evidenced by increased ileal levels of DA, dopamine D2 receptor (D2R), and tyrosine hydroxylase (TH), alongside decreased dopamine transporter (DAT) levels in animal models. Critically, gingerol treatment was found to reverse these cisplatin-induced alterations in dopaminergic signaling, suggesting that modulation of the dopamine pathway contributes to gingerol’s antiemetic properties.15
Chemosensitization and Immunomodulatory Effects
Ginger compounds exhibit significant anticancer properties by promoting apoptosis through several mechanisms. These include activating caspases-3 and −9, disrupting mitochondrial membrane potential, and inhibiting the NF-κB signaling pathway, all of which work to suppress cell survival and proliferation. Additionally, ginger compounds downregulate the expression of P-glycoprotein (P-gp), which is responsible for drug efflux. This reduction in P-gp activity enhances the accumulation of chemotherapeutic drugs within cells, thereby increasing the efficacy of chemotherapy.19 The chemosensitizing effect of ginger could allow for lower doses of chemotherapy agents, which may reduce the associated adverse effects, such as nausea and vomiting. Moreover, ginger’s bioactive components—such as 6-gingerol, 6-shogaol, and zingerone—exhibit immunomodulatory effects by influencing both innate and adaptive immune responses. These compounds modulate the production of cytokines and the function of various immune cells, including T cells, macrophages, natural killer (NK) cells, and B cells, impacting cytokine levels such as IL-10, TNF-α, IL-1β, and IL-6.20 Ginger’s ability to modulate immune function not only enhances host defense but may also play a role in mitigating inflammation-mediated nausea, further contributing to its antiemetic effects. These combined actions suggest that ginger can enhance the therapeutic benefits of chemotherapy while potentially reducing side effects. Additionally, ginger’s favorable safety profile, with minimal serious adverse effects, further supports its potential as a valuable adjunct to cancer treatment.21
Cannabis
Cannabis, known by various names such as marijuana, pot, kif, and hemp, is one of the oldest known psychoactive plants. While its origins lie in Central Asia, cannabis is now found globally.22 The plant contains cannabinoids, which mimic the body’s endocannabinoids and activate cannabinoid receptors, primarily CB1 (central nervous system) and CB2 (immune cells). The most well-known and bioactive cannabinoid, Delta-9-tetrahydrocannabinol (THC), is prescribed for the treatment of CINV and AIDS-related anorexia. Cannabidiol (CBD), another key cannabinoid, exhibits anti-epileptic, anti-inflammatory, antiemetic, and neuroprotective properties.23
Antiemetic Mechanism
Endocannabinoid System (ECS) Pathway
The modulation of the ECS has emerged as a promising approach for controlling nausea and vomiting. Cannabinoid agonism at CB1 receptors produces antiemetic effects, whereas CB1 inverse agonism induces emesis. Preclinical studies suggest cannabinoids are particularly effective in controlling intractable and anticipatory nausea, which are often associated with chemotherapy. CBD, a non-psychoactive cannabinoid, also demonstrates antiemetic properties, potentially through indirect activation of somatodendritic 5-HT1A autoreceptors, leading to reduced serotonin release in the forebrain. This effect may enhance its ability to alleviate both chemotherapy-induced and other treatment-related nausea and vomiting.24 The effectiveness of THC-based medications for managing CINV is supported by several meta-analyses. A systematic review by Abrams et al, which included 30 randomized controlled trials involving over 1300 patients, found that cannabinoids (oral nabilone and dronabinol) were superior to placebo and other antiemetics like prochlorperazine, metoclopramide, and chlorpromazine in controlling CINV.25
5-HT3 Receptor Antagonism
Emerging evidence suggests cannabinoids may also exert antiemetic effects by indirectly modulating 5-HT3 receptor activity, mimicking the mechanism of established antiemetics like ondansetron. Both CBD and THC have been shown to attenuate the function of human 5-HT3 receptors expressed in HEK 293 cells.26 Recent research also indicates that CBD may act as an allosteric modulator of 5-HT3 receptors. In Xenopus oocytes, CBD concentration-dependently and reversibly inhibits serotonin-induced currents at 5-HT3 receptors. This allosteric inhibition could contribute to CBD’s effects on nociception and emesis.27
Anti-Inflammatory Pathways
Cannabinoids’ anti-inflammatory properties may also contribute to their antiemetic effects. Activation of cannabinoid receptors has been shown to exert protective effects in animal models of intestinal inflammation, while CB receptor-deficient mice exhibit increased susceptibility to colitis. Strategies aimed at elevating endocannabinoid levels, such as inhibiting their degradation or enhancing cellular uptake, have demonstrated anti-inflammatory effects in the gut. Furthermore, oral administration of THC and palmitoylethanolamide (PEA) has been found to reduce intestinal inflammation.28
Chemosensitization and Immunomodulatory Effects
Recent studies on the interaction between cannabinoids and chemotherapy, particularly in triple-negative breast cancer (TNBC), have shown that chemotherapy can upregulate CB2 receptor expression in TNBC cells. Increased CB2 receptor expression, combined with treatment using CB2 agonists, results in inhibited TNBC cell growth and enhanced sensitivity to chemotherapy agents like cisplatin, doxorubicin, and docetaxel. These anti-proliferative and pro-apoptotic effects of CB2 activation are mediated by inhibition of the PI3K/Akt/mTOR signaling pathway, suggesting that CB2 may serve as a potential therapeutic target in breast cancer.29 In addition to their chemosensitizing effects, cannabinoids play a significant role in modulating immune responses, making them a potential target for immune-related disorders.30
Mint
Peppermint, a perennial herb native to Europe and North America, has long been recognized for its therapeutic applications. Its essential oil, derived through steam distillation of fresh leaves, is widely utilized for alleviating gastrointestinal discomfort. Beyond its digestive benefits, peppermint oil is also known for its antioxidant, antitumor, antibacterial, and analgesic properties. The primary bioactive constituents of peppermint oil include menthol, the most abundant monoterpene, and menthone, which work synergistically to enhance the oil’s therapeutic effects.4
Antiemetic Mechanism
Gastrointestinal Effects
Peppermint oil, with its extensive historical use in treating gastrointestinal disorders, exerts a range of effects on gastrointestinal physiology. These effects include smooth muscle relaxation, achieved through calcium channel blockade or direct action on the enteric nervous system, as well as modulation of visceral sensitivity via transient receptor potential (TRP) cation channels. Moreover, peppermint oil plays a role in managing psychosocial distress. Research demonstrates that peppermint oil influences the physiology of the esophagus, stomach, small intestine, gallbladder, and colon. Its clinical utility extends to facilitating colonoscopies and endoscopic retrograde cholangiopancreatography (ERCP) procedures. Placebo-controlled trials substantiate its effectiveness in managing irritable bowel syndrome (IBS), functional dyspepsia, abdominal pain in pediatric populations, and postoperative nausea. Notably, peppermint oil is considered to have a favorable safety profile.31,32 In vitro studies involving guinea pig and rabbit intestinal smooth muscle further suggest that peppermint oil can mitigate both acetylcholine- and serotonin-induced contractions, potentially through calcium channel blockade.33
Ion Channel Modulation
The transient receptor potential melastatin 8 (TRPM8) channel, a non-selective cation channel permeable to calcium ions, is activated by cold temperatures and cooling agents such as menthol and icilin, with menthol being the primary agonist. Activation of this channel produces a cooling sensation that contributes to the attenuation of nausea signals.34
Anti-Inflammatory Effect
Peppermint oil, particularly menthol, demonstrates notable anti-inflammatory properties that may indirectly enhance its antiemetic effects. Studies have shown that peppermint oil significantly inhibits the secretion of interleukin-1 beta (IL-1β) and tumor necrosis factor-alpha (TNF-α) from porcine alveolar macrophages (PAMs) stimulated with Lipopolysaccharide (LPS). Additionally, peppermint oil exhibits strong antioxidant activity. Furthermore, peppermint oil inhibits the growth of enterotoxigenic Escherichia coli (ETEC) F18+ in a dose-dependent manner. These findings underscore the potential of peppermint oil as an anti-inflammatory, antioxidant, and antimicrobial agent, which may contribute to alleviating nausea and vomiting.35 Further antimicrobial assessments of peppermint oil against Escherichia coli and Staphylococcus aureus have shown that substances such as linalool acetate and carvone possess substantial antimicrobial potency.36
Chemosensitization and Immunomodulatory Effects
Exposure of HepG2 cells to menthol for 24 hours resulted in upregulated MRP2 mRNA expression and a significant decrease in intracellular epirubicin (EPI) concentration. Both EPI and cisplatin (CIS) demonstrated cytotoxicity in HepG2 cells. These findings suggest that menthol-induced MRP2 expression may contribute to the development of anticancer drug resistance in hepatocellular carcinoma.37 Additionally, mint contains flavonoids such as luteolin and rosmarinic acid, which have been documented to modulate cytokine production and exhibit immunomodulatory effects.38 These findings imply that mint and its constituents could serve as adjuncts to cancer treatments, either by improving chemotherapy efficacy or modulating immune responses.
Chamomile
Chamomile, a medicinal plant renowned for its antiemetic properties. Research supports its efficacy in managing a variety of conditions, including fever, migraines, headaches, rheumatoid arthritis, and gastrointestinal and dental pain. Chamomile extract is rich in phenolic compounds, notably the flavonoid apigenin, as well as sesquiterpenoids and coumarins.39
Antiemetic Mechanism
Antispasmodic Effects
Chamomile’s ability to relieve gastrointestinal spasms, which often contribute to nausea, is attributed to its high content of flavonoids (eg, apigenin, luteolin, quercetin), coumarins, and volatile oils such as bisabolol and its oxides. These compounds inhibit voltage-dependent calcium channels, thereby reducing intracellular calcium levels in smooth muscle cells, leading to muscle relaxation and alleviation of spasms. Studies have demonstrated that chamomile preparations significantly reduce cisplatin-induced emesis in animal models. Furthermore, chamomile modulates duodenal smooth muscle contractility by affecting calcium channel-mediated contractions and inhibiting those mediated by intracellular calcium release.40
Anti-Inflammatory Properties
Chamomile’s anti-inflammatory effects also contribute to its antiemetic activity by mitigating gastrointestinal irritation and inflammation, which are potential triggers of nausea. Active compounds in chamomile inhibit inflammatory mediators and exhibit antioxidant activity. Notably, studies have shown that chamomile suppresses LPS-induced inflammation in human colorectal adenocarcinoma cells, an effect comparable to that of sulfasalazine.41 Chamomile also modulates the activity of pro-inflammatory and anti-inflammatory mediators released by human macrophages, similar to the action of budesonide. Specifically, it reduces pro-inflammatory TNF-α and CXCL13 while promoting the release of the anti-inflammatory cytokine interleukin-10 (IL-10).42
Central Nervous System Regulation
Chamomile contains apigenin and other flavonoids that interact with benzodiazepine receptors in the brain. Apigenin specifically binds to gamma-aminobutyric acid (GABA-A) receptors, enhancing the effects of the inhibitory neurotransmitter GABA. This interaction reduces neuronal excitability, exerting a sedative effect. By alleviating anxiety and stress, chamomile indirectly mitigates nausea and vomiting associated with psychological factors.43
Chemosensitization and Immunomodulatory Effects
Apigenin, a flavonoid predominantly found in chamomile, has demonstrated significant anticancer properties, including the induction of apoptosis and the inhibition of cancer cell proliferation across various cancer lines. Apigenin also modulates critical cell cycle and apoptotic pathways, thus enhancing the susceptibility of cancer cells to common chemotherapeutic agents such as doxorubicin, cisplatin, and paclitaxel. This is achieved by disrupting cell cycle progression and amplifying apoptotic signaling.44 In liver cancer, apigenin has been shown to enhance the sensitivity of cells to 5-fluorouracil by downregulating NF-κB and P-gp expression. Beyond its effects on cell death pathways, emerging research indicates that apigenin modulates antitumor immune responses. It stimulates immune cells to release death signals to cancer cells and inhibits the secretion of tumor-promoting molecules. Apigenin also influences the activity of macrophages, lymphocytes, and dendritic cells, thereby enhancing immune cell activation and contributing to the broader immune-mediated anticancer effects.45
Lemon
Lemon (Citrus limon), a member of the Rutaceae family, has been historically utilized not only as a culinary and flavoring agent but also as a medicinal remedy. Traditionally, lemon is employed to alleviate gastrointestinal distress, motion sickness, and nausea associated with chemotherapy or postoperative recovery.46 Its sedative effects, which may contribute to its antiemetic properties, are attributed to several bioactive compounds, including flavonoids, limonene, citral, linalool, and other monoterpenes.47,48 These compounds may modulate neurotransmitter activity involved in the emetic reflex.49
Antiemetic Mechanisms
Modulation of Gastrointestinal Motility
Lemon essential oil is rich in limonene, a monoterpene known for its ability to relax gastrointestinal smooth muscle. Limonene has been shown to exert a vasodilatory effect on the superior mesenteric artery in rats. By alleviating muscle spasms, limonene helps reduce discomfort associated with nausea and can prevent the onset of the gag reflex.50
Anti-Inflammatory Effects
Inflammation in the gastrointestinal tract is a known trigger for nausea and vomiting. Limonene’s anti-inflammatory properties contribute to lemon’s antiemetic effects by mitigating inflammation-induced nausea. Limonene modulates several inflammatory pathways, inhibiting pro-inflammatory cytokines and mediators such as nitric oxide (NO) and prostaglandins.51 Research by Yoon et al demonstrated that limonene effectively suppresses LPS-induced production of NO and prostaglandin E2 (PGE2), including a dose-dependent decrease in the expression of inducible nitric oxide synthase (iNOS) and cyclooxygenase-2 (COX-2). Additionally, limonene reduced levels of TNF-α, IL-1β, and IL-6 in the supernatant of LPS-stimulated RAW 264.7 macrophages.52
Modulation of the Central Nervous System Through Olfactory Pathways
Anxiety and stress are key exacerbating factors for nausea and vomiting. Lemon’s anxiolytic properties, attributed to compounds like limonene and linalool, may help reduce stress and anxiety, indirectly alleviating nausea. Studies by Lima NG et al demonstrated that limonene exerts significant anxiolytic-like effects in animal models, comparable to the effects of diazepam, a standard anxiolytic.53 A randomized controlled trial by Yavari Kia P et al showed the efficacy of lemon aromatherapy in reducing nausea and vomiting during pregnancy. The significant improvement observed with inhaled lemon essential oil suggests a central nervous system-mediated mechanism, likely through olfactory pathways.54 Additionally, research by Komiya et al revealed that lemon oil vapor exerts an anti-stress effect in mice, modulating serotonin (5-HT) and DA activity. These findings suggest that exposure to lemon oil vapor can reduce stress-related behaviors and potentially exert antiemetic effects through its influence on these neurotransmitters.55
5-HT3 Receptor Antagonism
Limonene’s antiemetic properties are, in part, attributed to its antagonism of 5-HT3 (serotonin) receptors, which play a pivotal role in mediating nausea and vomiting, particularly in response to chemotherapy and other emetogenic stimuli. Limonene inhibits serotonin-induced nausea by blocking 5-HT3 receptors in both the gastrointestinal tract and the brain.56
Chemosensitization and Immunomodulatory Effects
Flavonoids, abundant in citrus fruits like lemons, are known to inhibit P-gp and other MRP, thereby preventing the efflux of chemotherapeutic drugs from cancer cells and potentially enhancing their efficacy. In a study by Lan et al demonstrated that flavonoids, which induced apoptosis and inhibited non-small cell lung cancer (NSCLC) growth.57 Furthermore, Luetragoon et al examined the immunomodulatory effects of lemon leaf extract components, specifically lupeol, citronellal, and citronellol. These components exhibited high cytotoxicity against the human SCC15 cell line. In co-culture experiments with activated macrophages, lemon leaf extract and its components promoted the development of pro-inflammatory (M1) macrophages and enhanced TNF-α production, leading to apoptosis in SCC15 cells. These findings highlight the potential clinical significance of lemon’s immunomodulatory properties.58
Fennel
Fennel (Foeniculum vulgare Mill., Apiaceae), a versatile herb cultivated as an annual, biennial, or perennial. Extracts and preparations derived from fennel demonstrate a wide array of pharmacological effects, including anti-inflammatory, antispasmodic, antioxidant, antitumor, chemopreventive, and cytoprotective properties. The primary bioactive constituents of fennel include phenolic acids, flavonoids, terpenes, and alkaloids, with trans-anethole and fenchone being the most prominent compounds.59
Antiemetic Mechanism
Antispasmodic Effect
Fennel essential oil, rich in bioactive compounds such as anethole, fenchone, and estragole, exerts a pronounced relaxing effect on gastrointestinal smooth muscle. This relaxation, potentially mediated by calcium channel inhibition, helps alleviate muscle spasms associated with nausea and vomiting. Anise oil, in particular, has demonstrated significant antispasmodic effects by relaxing methacholine-induced contractions in isolated guinea pig tracheal chains, likely through the activation of potassium channels.60
Anti-Inflammatory Properties
The anti-inflammatory effects of fennel are largely attributed to its flavonoid and phenolic content. These compounds help alleviate inflammation-induced nausea by inhibiting pro-inflammatory cytokines and exhibiting antioxidant activity. Fennel essential oil has been shown to significantly inhibit human neutrophil activation, accelerate calcium influx recovery, and suppress the phosphorylation of mitogen-activated protein kinases (p38, JNK, and ERK).61
Gastrointestinal Protection
Fennel also demonstrates gastroprotective effects by enhancing gastric mucus secretion and bolstering antioxidant defenses, thereby protecting the gastric mucosa from irritation and reducing nausea. Its phenolic compounds are particularly effective at scavenging free radicals, preventing mucosal damage. In a mouse model, fennel seed extract was found to significantly improve intestinal epithelial barrier function, as evidenced by increased transepithelial electrical resistance (TEER). Mice treated with fennel seed extract exhibited a lower ulcer index compared to controls, suggesting its potential to enhance gastrointestinal barrier integrity.62
Chemosensitization and Immunomodulatory Effects
Anethole, the primary active compound in fennel, also displays anticancer activity. In a study by W. S. Ramadan et al suggest that combining cisplatin with sweet fennel extract enhances the inhibition of cervical cancer cell growth, potentially allowing for a reduction in the required cisplatin dosage and mitigating its associated side effects.63 Further, Darzi et al explored the immunomodulatory and pro-apoptotic effects of fennel. Their research demonstrated that fennel reduced the proliferation of activated lymphocytes. Specifically, the dichloromethane fraction of fennel induced apoptosis in activated lymphocytes, while the butanol fraction reduced lymphocyte activation and cytokine secretion.64
Mentha Spicata (Spearmint)
Mentha spicata, commonly known as spearmint, is an aromatic plant with a rich history of use in both traditional medicine and culinary practices.65 Spearmint has been a staple in Iranian traditional medicine for centuries, traditionally used to treat diarrhea, detoxify the body, and alleviate symptoms such as indigestion, intestinal weakness, abdominal pain, and gastrointestinal discomfort. Phenolic acids represent some of the key bioactive constituents in spearmint.66
Antiemetic Mechanisms
Antispasmodic Effect
Spearmint essential oil, containing key compounds such as carvone and limonene, has been shown to induce relaxation of gastrointestinal smooth muscle. This action, mediated through calcium channel inhibition, reduces spasms that could trigger nausea and vomiting. Several studies have supported spearmint’s antispasmodic activity. For example, Hashim et al investigated the effects of spearmint essential oil on isolated rabbit jejunum and observed a dose-dependent antispasmodic effect, inhibiting spontaneous contractions. In a similar vein, Hills and Aaronson demonstrated that spearmint oil inhibited acetylcholine and histamine-induced contractions in guinea pig ileum, suggesting a direct relaxant effect on smooth muscle.33,67
Anti-Inflammatory Properties
The anti-inflammatory effects of spearmint, attributed to its flavonoid and phenolic compounds, can help protect the gastrointestinal tract from inflammation-induced nausea. Compounds such as rosmarinic acid have been shown to inhibit the production of inflammatory mediators. In an animal model of colitis, spearmint extract demonstrated significant anti-inflammatory effects by reducing levels of pro-inflammatory cytokines such as TNF-α, IL-1β, and IL-6. These findings further highlight the potential of spearmint in alleviating gastrointestinal inflammation.35
Gastrointestinal Protection
Spearmint is also capable of protecting the gastric mucosa from irritation by enhancing gastric mucus secretion and boosting antioxidant defenses. This protective effect may help shield the stomach and intestines from irritants that induce nausea. Antioxidant compounds found in spearmint neutralize free radicals, preventing mucosal damage. A study by Saeed et al demonstrated that spearmint extract significantly reduced ethanol-induced gastric lesions in rats, providing further evidence of its gastroprotective potential.68
Aromatherapeutic Effects
Inhalation of spearmint essential oil has been shown to alleviate nausea and vomiting, potentially offering a therapeutic alternative through its aromatherapeutic properties. The pleasant scent of spearmint stimulates olfactory receptors, triggering central nervous system responses that may attenuate the sensation of nausea. A clinical study assessing the effects of spearmint oil inhalation on postoperative nausea demonstrated a significant reduction in nausea intensity in patients who inhaled spearmint oil compared to the control group.69
Chemosensitization and Immunomodulatory Effects
The flavonoids and phenolic acids present in spearmint could influence immune responses by inhibiting pro-inflammatory cytokines and enhancing antioxidant defenses. Abdelli et al highlighted the immunomodulatory properties of spearmint extract, showing enhanced lymphocyte proliferation and increased NK cell activity.70 Although spearmint shows promise in supporting immune function, evidence for its chemosensitizing effects in cancer therapy remains limited. Further investigations are warranted to determine whether spearmint can enhance the efficacy of chemotherapy or overcome drug resistance.
Licorice
Glycyrrhiza glabra, commonly known as licorice, is a medicinal plant whose dried roots and rhizomes have been employed for centuries in traditional medicine to alleviate a range of symptoms, including pain, cough, dyspnea, cramps, and excess phlegm. Licorice contains a complex phytochemical profile, with over 300 identified bioactive compounds contributing to its extensive pharmacological effects. Key constituents include glycyrrhizic acid and flavonoids such as isoliquiritigenin, liquiritigenin, and their derivatives.71
Antiemetic Mechanism
Gastric Protection and Enhanced Mucosal Defense
Licorice flavonoids contribute to gastroprotection by promoting the regeneration of gastric mucosal cells, enhancing mucosal blood flow, and supporting ulcer and erosion healing. Yufan et al demonstrated the gastroprotective effects of licorice flavonoid extract in a rat model of ethanol-induced gastric ulcers. The extract increased the viability of human gastric mucosal epithelial cells, mitigated ethanol-induced damage, reduced histological injury, inhibited inflammation, and promoted the restoration of the gastric mucosal barrier. These findings underscore the capacity of licorice flavonoids to inhibit inflammation and facilitate mucosal repair.72
Anti-Inflammatory and Antioxidant Activity
Licorice flavonoids, particularly liquiritigenin, licoricidin, and glabridin, exhibit potent antioxidant properties, scavenging free radicals and inhibiting lipid peroxidation. Studies have demonstrated their ability to suppress the production of NO, IL-6, and PGE2 in LPS-stimulated macrophages. Notably, licorice coumarin is not typically considered a primary active constituent; the key bioactive compounds are predominantly the flavonoids and chalcones.73
Regulation of Neurotransmitter Systems
Specific licorice compounds, including flavonoids like liquiritigenin and isoliquiritigenin, interact with neurotransmitter receptors and may antagonize serotonin (5-HT3) receptors implicated in the emetic response, thereby reducing nausea and vomiting. Research by Robin et al identified liquiritigenin, glycyrrhizin, and licoricidin (or licorice chalcone A) as potent inhibitors of 5-HT-induced currents. Licoricidin, in particular, may act as a partial antagonist of the 5-HT3A receptor, offering potential relief from CINV.74
Antispasmodic Effect on Gastrointestinal Smooth Muscle
Licorice exhibits antispasmodic properties attributable to several of its active constituents. Glycyrrhetinic acid has shown antispasmodic effects, likely through the inhibition of phosphodiesterase III, which leads to vasodilation and a reduction in carbachol-induced jejunal contractions in mice. Isoliquiritigenin, another licorice compound, also demonstrates antispasmodic activity against contractions induced by KCl, BaCl2, and carbachol. Although isoliquiritigenin concentrations in aqueous licorice extracts are generally low, treatment with naringinase can increase its content and enhance its antispasmodic effects.60
Chemosensitization and Immunomodulatory Effects
Licorice compounds, particularly the flavonoid liquiritigenin, exhibit potent anticancer activity, demonstrating inhibitory effects against various cancer cell types, with minimal toxicity to healthy cells. The anticancer mechanisms of liquiritigenin involve the induction of cell cycle arrest, promotion of apoptosis, and modulation of inflammation-related pathways. Furthermore, liquiritigenin inhibits angiogenesis and has been shown to synergistically enhance the efficacy of conventional chemotherapy and targeted therapies.75 Another licorice-derived compound, 18β-glycyrrhetinic acid (GA), exhibits both anticancer and immunomodulatory properties. Xuan et al attributed GA’s immune-enhancing effects to its ability to inhibit arachidonic acid (AA)-mediated ferroptosis in CD8+ T cells by suppressing CD36 expression.76
Cardamom
Cardamom, a perennial herb from the ginger family native to India and Sri Lanka. It is employed to treat indigestion, stomach cramps, and to alleviate inflammation and pain. Cardamom’s antiemetic effects are attributed to its rich phytochemical composition, which includes volatile oils, flavonoids, and other bioactive constituents.77
Antiemetic Mechanism
Antispasmodic Effect
Cardamom demonstrates antispasmodic properties by relaxing GI smooth muscle, thereby alleviating spasms and hypermotility, both of which contribute to nausea and vomiting. Jamal et al elucidated the antispasmodic effects of cardamom methanol extract in isolated guinea pig ileum, suggesting a potential mechanism involving calcium channel blockade.78
Anti-Inflammatory and Antioxidant Effects
Cardamom mitigates gastrointestinal inflammation, a key trigger for nausea, by inhibiting the production of pro-inflammatory cytokines and enzymes such as COX. Its phenolic compounds and flavonoids function as potent antioxidants, scavenging ROS and protecting the gastrointestinal mucosa from oxidative stress and damage. For instance, a study involving pre-diabetic individuals demonstrated that cardamom improved markers of inflammation and oxidative stress compared to a placebo. Other studies have corroborated these findings, illustrating cardamom’s ability to reduce serum levels of pro-inflammatory cytokines such as TNF-α, IL-6, and CRP.79
Chemosensitization and Immunomodulatory Effects
Several components of cardamom, including 1,8-cineole, α-terpinyl acetate, and limonene, exhibit potential chemosensitizing effects. These constituents may induce apoptosis in cancer cells and enhance the efficacy of chemotherapeutic agents by modulating apoptotic pathways (eg, increasing Bax and decreasing Bcl-2), inhibiting drug resistance mechanisms (such as P-gp expression), and regulating key cell survival pathways (eg, NF-κB and PI3K/Akt).80 Furthermore, its bioactive constituents modulate cytokine production, NF-κB signaling, and COX-2 activity. Research has shown that cardamom water extract enhances splenocyte proliferation and natural killer cell cytotoxicity in a dose-dependent manner, further substantiating its immunomodulatory and antitumor potential.81
Pinellia Ternata
Pinellia ternata (PTT), a member of the Araceae family. In contemporary medical practice, PTT is frequently combined with other herbs as an adjunct therapy for CINV. The tubers of PTT are rich in a variety of phytochemicals, including organic acids, nucleosides, flavonoids, and alkaloids, which contribute to its broad pharmacological profile, encompassing antiemetic, antitumor, and anti-inflammatory effects.82
Antiemetic Mechanism
Gastrointestinal Effects
The cholinergic components of Pinellia ternata can activate muscarinic (M) receptors on gastrointestinal smooth muscle. This activation triggers intracellular signaling cascades that lead to the phosphorylation of smooth muscle contractile proteins, resulting in muscle contraction, enhanced gastrointestinal motility, and improved gastric emptying. Choi et al demonstrated the effectiveness of PTT extract in modulating the pacemaker potentials of interstitial cells of Cajal (ICC) in a mouse model of gastrointestinal dysmotility (GMD). PTT outperformed the control group, both in vivo, by improving GMD symptoms, and in vitro, by modulating ICC pacemaker activity.83
Anti-Inflammatory Effect
Pinellia ternata exhibits notable anti-inflammatory properties, which may help alleviate gastrointestinal inflammation, a key contributor to nausea. Various constituents of PTT have been shown to exhibit anti-inflammatory potential. For instance, the petroleum ether extract of PTT inhibits TNF-α-induced NF-κB activation in vitro and dose-dependently enhances PPAR-α and PPAR-γ activity, suggesting its potential as an anti-inflammatory agent.84 Research by Tao et al further demonstrated that PTT alleviates allergic airway inflammation by modulating Th1 and Th2 cytokine levels. Additionally, PTT can inhibit the TLR4-mediated NF-κB signaling pathway and activate the NLRP3 inflammasome.85
Regulation of Neurotransmitters
Pinellia ternata exerts antiemetic effects, potentially by antagonizing 5-HT3 receptors involved in the vomiting reflex, thereby acting as a 5-HT3 receptor antagonist. It may also modulate the dopamine pathway, possibly by inhibiting dopamine D2 receptors in the CTZ, thereby reducing stimulation of the vomiting center. Studies have shown that Pinellia alkaloids dose-dependently inhibit spontaneous contractions of isolated guinea pig ileum and antagonize the excitatory effects of acetylcholine, 5-HT, and histamine, as well as the relaxant effects of dopamine. A key mechanism by which Pinellia total alkaloids manage CINV may be the antagonism of 5-HT3.86
Chemosensitization and Immunomodulatory Effects
Certain constituents of Pinellia ternata, including alkaloids and polysaccharides, have been shown to modulate the sensitivity of tumor cells to chemotherapeutic agents. These compounds may exert chemosensitizing effects by interacting with drug resistance-related proteins or signaling pathways within tumor cells. In addition, Pinellia exhibits immunomodulatory activity. Studies indicate that Pinellia water extracts positively influence immune function.87 For example, research has demonstrated that Pinellia can protect against benzene-induced immune dysfunction by reducing levels of the immunosuppressive cytokine IL-10 and mitigating structural and functional damage to the thymus and spleen.88
Evodia Rutaecarpa
Evodia rutaecarpa, a well-established medicinal plant, is characterized by its pungent, bitter, and warm properties, and is recognized for its broad spectrum of biological activities and therapeutic applications. It is frequently utilized as a complementary and alternative treatment for abdominal discomfort, bloating, vomiting, and diarrhea.89 The primary bioactive constituents of Evodia rutaecarpa include indole alkaloids, notably evodiamine (EVO), rutaecarpine (RUT), and dehydroevodiamine (DHE), which are believed to mediate many of its pharmacological effects.90
Antiemetic Mechanism
Gastrointestinal Regulation
Evodia rutaecarpa has been shown to enhance gastrointestinal motility, thereby promoting normal peristalsis and facilitating the orderly progression of digestive contents. Several of its constituents may exert regulatory effects on gastrointestinal smooth muscle, potentially through interaction with muscarinic receptors located on smooth muscle cells, which modulate contraction and relaxation. This action helps maintain gastrointestinal stability, alleviating nausea and vomiting. For instance, the flavonoids present in Evodia may exert bidirectional regulatory effects on smooth muscle: reducing excessive contractions during spasms, potentially via allosteric modulation of muscarinic cholinergic receptors, while enhancing contractions when motility is insufficient. Moreover, Evodia may influence the secretion of gastrointestinal hormones, such as motilin and gastrin, thus promoting gastric emptying.91
Anti-Inflammatory Effect
Evodiamine and rutaecarpine, the primary bioactive compounds in Evodia rutaecarpa, exhibit potent anti-inflammatory properties. For example, they suppress iNOS activity and reduce NO production. At the cellular level, these compounds may prevent NF-κB activation and its nuclear translocation, leading to the downregulation of inflammatory mediator gene expression, thereby alleviating the inflammatory responses that contribute to nausea and vomiting.92 Additionally, Evodia constituents have been shown to promote the proliferation and repair of mucosal epithelial cells, possibly through the activation of growth factor receptors like epidermal growth factor receptor (EGFR) and the stimulation of intracellular signaling pathways. This facilitates mucosal healing, reduces gastrointestinal inflammation, and contributes to its antiemetic effects.93
Regulation of the Nervous System
Evodia rutaecarpa contains several alkaloids, which play a crucial role in modulating serotonin 5-HT3 receptors. These alkaloids competitively bind to 5-HT3 receptors, as demonstrated in cellular studies, where they inhibit serotonin-induced increases in intracellular calcium ions, thus effectively blocking 5-HT₃ receptor-mediated signal transduction. This blockade diminishes neurotransmitter release and inhibits the afferent impulses that trigger the vomiting reflex. Furthermore, Experimental studies have demonstrated that Evodia extract can reduce apomorphine-induced vomiting in animal models, likely by competitively binding to D2 receptors, preventing dopamine binding, and thereby inhibiting the activation of the vomiting center.94
Chemosensitization and Immunomodulatory Effects
Emerging research suggests that specific components of Evodia rutaecarpa possess chemosensitizing potential in cancer therapy. In the gastrointestinal tract, Evodia can directly or indirectly inhibit the PI3K/Akt pathway, thereby enhancing the pro-apoptotic effects of gemcitabine on tumor cells. Furthermore, Evodia has been shown to suppress cancer cell proliferation, migration, and invasion by downregulating IL-6-induced STAT3 signaling activation and upregulating SHP-2.95,96 Additionally, Evodia exhibits significant immunomodulatory effects, influencing the activity of immune cells such as T and B lymphocytes and modulating the secretion of immune-related factors. By bolstering immune defenses and promoting immune homeostasis, Evodia may assist the body in combating infections and mitigating chemotherapy-induced side effects, particularly nausea and vomiting.
Turmeric
Turmeric (also known as black turmeric) is a plant with a distinct blue-black rhizome, a pungent and bitter aroma, and a long history of medicinal use. In traditional medicine, both fresh and dried turmeric rhizomes are employed to treat a variety of ailments, including nausea and vomiting, asthma, tumors, hemorrhoids, bronchitis, and bruises. The plant contains active compounds such as alkaloids, phenols, curcumin, and terpenoids.97
Antiemetic Mechanisms
Modulation of Neurotransmitter Systems
The antiemetic effects of turmeric are primarily attributed to its interaction with neurotransmitter systems involved in the vomiting reflex. Curcumin, the principal bioactive compound in turmeric, acts as a competitive antagonist at 5-HT₃ receptors, which are pivotal in CINV. By antagonizing these receptors, curcumin reduces serotonin-mediated activation of vagal afferent nerves, thereby inhibiting the vomiting reflex. Additionally, curcumin modulates dopaminergic signaling in the CTZ and affects substance P levels in both central and peripheral tissues. A study by Ramaholimihaso et al demonstrated that curcumin treatment significantly reduced cisplatin-induced emesis by 58%, primarily through the reduction of serotonin release and the downregulation of substance P levels in brain tissue. Furthermore, the study revealed a substantial reduction in NK1 receptor expression, another key mediator in the emetic response.98
Anti-Inflammatory and Antioxidant Activity
The anti-inflammatory and antioxidant properties of turmeric compounds play a central role in mediating its antiemetic effects. Curcumin, the primary bioactive component of turmeric, effectively inhibits multiple pro-inflammatory signaling pathways, most notably through suppression of NF-κB activation. This modulation reduces the production of key inflammatory mediators such as TNF-α, IL-1β, IL-6, and COX-2. Additionally, curcumin regulates inflammatory enzymes, including lipoxygenase and iNOS. Peng et al demonstrated that curcumin treatment led to a marked reduction in gastric tissue levels of TNF-α and IL-1β. The antioxidant mechanisms of turmeric involve both direct scavenging of free radicals and the enhancement of the cellular antioxidant defense system, primarily through the upregulation of antioxidant enzymes. These actions collectively protect the gastric mucosa from oxidative stress-induced damage, thereby contributing to the antiemetic properties of turmeric.99
Antispasmodic Effect on Gastrointestinal Smooth Muscle
The antispasmodic properties of turmeric compounds significantly contribute to their antiemetic efficacy. Curcumin regulates calcium homeostasis in gastrointestinal smooth muscle cells by inhibiting calcium influx via voltage-dependent calcium channels and reducing intracellular calcium release. This action leads to smooth muscle relaxation and a reduction in gastrointestinal hypermotility. In a study by Kumar et al, curcumin treatment resulted in a 67% reduction in acetylcholine-induced contractions in isolated gastric smooth muscle preparations. Furthermore, histamine-induced gastric contractions were notably inhibited, and gastric emptying disorders were alleviated. These effects are attributed to the reduced expression of muscarinic receptors and altered calcium channel activity within the gastrointestinal smooth muscle tissue.100
Gastric Protection and Enhancement of Mucosal Defense
Curcumin and other curcuminoids present in turmeric (Curcuma longa) play a critical role in enhancing gastric mucosal defense, thereby mitigating the risk of nausea and vomiting. The primary mechanism involves the stimulation of mucus-secreting cells in the gastric epithelium, which increases the production of protective mucus, forming a physical barrier against irritants. Moreover, curcumin modulates gastric acid secretion by inhibiting H+/K+-ATPase activity in parietal cells, thereby helping to maintain an optimal gastric pH. Studies by Kwiecien et al demonstrated that curcumin treatment resulted in a 65% reduction in gastric lesions and a 45% increase in mucus production compared to controls. Additionally, turmeric compounds enhance the expression of growth factors involved in mucosal repair and regeneration, such as EGFR and vascular endothelial growth factor (VEGF).101
Chemosensitization and Immunomodulatory Effects
Curcumin has been shown to enhance the sensitivity of cancer cells to chemotherapeutic agents and to induce apoptosis via multiple mechanisms. These include the regulation of caspase-dependent pathways, upregulation of pro-apoptotic proteins (eg, Bax, Bad), downregulation of anti-apoptotic proteins (eg, Bcl-2, Bcl-xL), and initiation of mitochondrial-mediated death pathways. Research indicates that curcumin also downregulates the expression of P-gp and COX-2. Furthermore, curcumin’s direct interaction with mitochondrial matrix proteins contributes to the chemosensitization of colon cancer cells to doxorubicin.102 A combination treatment of curcumin and 5-fluorouracil (5FU) has been shown to enhance apoptosis and suppress proliferation in both parental and 5FU-resistant (5FUR) cancer cells.103 In addition to its anticancer properties, turmeric also exerts immunomodulatory effects. It modulates cytokine levels by inhibiting pro-inflammatory cytokines and regulating anti-inflammatory cytokines. Curcumin can suppress the expression of inflammatory mediators such as COX-2, reducing PGE2 production. These actions enhance the immune response during chemotherapy, improve treatment efficacy, reduce inflammatory complications, and increase tolerance to chemotherapy regimens.104
Perilla
Perilla (Perilla frutescens), a member of the Lamiaceae family, is a significant medicinal herb widely cultivated in East Asia. Modern research has identified a wide array of bioactive secondary metabolites in various parts of Perilla, including terpenes, flavonoids, alkaloids, steroids, quinones, and phenolic compounds, all of which contribute to its diverse biological activities and medicinal potential. Traditionally, Perilla has been used to treat a variety of conditions, including tumors, vomiting, and gastrointestinal disorders.105
Antiemetic Mechanisms
Antispasmodic Effect on the Smooth Muscle of the Gastrointestinal Tract
The essential oils of Perilla, containing compounds such as perillaldehyde and limonene, exert a direct antispasmodic effect on gastrointestinal smooth muscle. These compounds inhibit calcium influx into smooth muscle cells, leading to muscle relaxation and a reduction in gastrointestinal spasms and contractions. This relaxation relieves discomfort and mitigates nausea associated with gastrointestinal hypermotility. Additionally, Perilla extract may interact with receptors involved in acetylcholine-induced intestinal contraction, further reducing spasms and promoting normal gastrointestinal movement.106
Anti-Inflammatory and Antioxidant Activity
The anti-inflammatory and antioxidant properties of Perilla further enhance its antiemetic potential. Rosmarinic acid, a major phenolic compound found in Perilla, possesses strong antioxidant capabilities, enabling it to neutralize free radicals and prevent oxidative damage in the gastrointestinal tract. Additionally, the flavonoid compounds in Perilla, such as luteolin and apigenin, inhibit the production of pro-inflammatory cytokines such as TNF-α, IL-1β, and IL-6. By suppressing these key inflammatory mediators, Perilla can reduce gastrointestinal inflammation and contribute to its antiemetic effects.107
Gastric Protection and Enhancement of Mucosal Defense
Perilla primarily exerts gastric protection through its essential oil constituents, with perillaldehyde being the most prominent. Perillaldehyde enhances the secretion of gastric mucus, thereby fortifying the protective mucosal barrier against irritants and noxious agents that may provoke nausea and vomiting. Perilla extracts have also demonstrated the ability to inhibit gastric acid secretion, potentially via modulation of proton pump activity or other regulatory mechanisms. The synergistic effect of enhancing the mucosal barrier while reducing gastric acidity significantly contributes to perilla’s antiemetic properties.108
Chemosensitization and Immunomodulatory Effects
Research suggests that perilla components, particularly perillaldehyde, inhibit P-gp, a membrane protein implicated in multidrug resistance by actively effluxing chemotherapy agents from cancer cells. Perilla compounds have also been shown to induce apoptosis across various cancer cell lines, thereby potentially amplifying the anticancer efficacy of chemotherapy. Some studies have revealed synergistic interactions between perilla extracts and chemotherapeutic agents, resulting in enhanced therapeutic outcomes compared to either treatment alone.109 Moreover, perilla possesses immunomodulatory properties, enhancing the activity of immune cells such as NK cells and macrophages, both of which are pivotal in antitumor immunity. Additionally, perilla influences cytokine production, thereby modulating immune responses and potentially bolstering antitumor immunity.110
Scutellaria Baicalensis
Scutellaria baicalensis (Baikal skullcap), a perennial herb from the Lamiaceae family, has been traditionally used to treat a wide array of ailments, including gastrointestinal disorders like dysentery, diarrhea, nausea, and vomiting, as well as various tumors. The root extract is rich in bioactive flavonoids, including baicalin, baicalein, wogonin, and wogonoside.111
Antiemetic Mechanisms
A Gastric Mucosal Protection
Scutellaria baicalensis, particularly through its flavonoid constituents such as baicalin and wogonin, exhibits significant gastroprotective effects. Baicalin elevates the levels of glutathione, a key antioxidant, while simultaneously reducing myeloperoxidase activity. Administration of baicalin via the duodenum notably stimulates gastric mucus production. In pylorus-ligated models, baicalin has been shown to reduce gastric acid secretion and overall acidity, while increasing gastric pH. Moreover, baicalin inhibits histamine-induced gastric acid secretion and demonstrates anti-H+,K+-ATPase activity.112 These findings suggest that Scutellaria baicalensis may help preserve the integrity of the gastric lining and reduce nausea through these mechanisms.
Anti-Inflammatory and Antioxidant Activities
Scutellaria baicalensis is renowned for its potent anti-inflammatory and antioxidant properties. The flavonoids baicalin and wogonin exhibit strong antioxidant activity by scavenging free radicals and inhibiting lipid peroxidation. These compounds can directly modulate immune cells leading to the suppression of pro-inflammatory cytokines such as IL-1β, IL-6, IL-8, and TNF-α, along with other inflammatory mediators like nitric oxide, prostaglandins, and reactive oxygen species. The underlying molecular mechanisms include downregulation of Toll-like receptors, activation of Nrf2 and PPAR pathways, and inhibition of inflammation-related signaling cascades. In light of its antiviral and antibacterial properties, Scutellaria baicalensis may offer promising potential as a therapeutic agent to mitigate infection-associated cytokine storms, surpassing conventional treatments that target only inflammatory or bacterial pathways.113,114
Potential Antispasmodic Effects on Gastrointestinal Smooth Muscle
Certain flavonoids in Scutellaria baicalensis have been shown to exhibit smooth muscle relaxant properties in experimental models, suggesting that the herb may possess antispasmodic effects on gastrointestinal smooth muscle. This action could be beneficial in reducing nausea associated with gastrointestinal spasms or contractions.115
Chemosensitization and Immunomodulatory Effects
Scutellaria baicalensis has demonstrated significant chemosensitizing and immunomodulatory effects in preclinical studies. Baicalin, the primary active component, has been shown to inhibit several pathways associated with drug resistance in cancer cells, including the NF-κB and PI3K/Akt signaling pathways. This modulation makes cancer cells more susceptible to chemotherapy. In addition, baicalin and other flavonoids in Scutellaria baicalensis can induce apoptosis in cancer cells, potentially enhancing the efficacy of chemotherapy. The herb also displays anti-angiogenic activity, inhibiting the formation of blood vessels that supply tumors, thus restricting tumor growth and further augmenting chemotherapy’s therapeutic effects.116,117 Furthermore, Scutellaria baicalensis can enhance immune cell activity, particularly NK cells and macrophages, which are integral to anti-cancer immunity. It also modulates cytokine production, influencing immune responses and potentially promoting antitumor immunity.118
Ganoderma
Ganoderma lucidum (commonly known as Reishi or Lingzhi) is a basidiomycete fungus from the Polyporaceae family. It is a renowned medicinal mushroom used extensively in traditional Chinese, Japanese, and other East Asian medical systems. Phytochemical investigations have identified numerous bioactive compounds in its basidiocarps, mycelium, and spores, including triterpenes, polysaccharides, nucleotides, sterols, steroids, fatty acids, proteins, and trace elements. Ganoderma is believed to exert a variety of therapeutic effects, including inhibiting tumor growth, reducing hypertension, modulating immune responses, and mitigating nausea and vomiting, especially as an adjuvant to chemotherapy.9
Antiemetic Mechanisms
Anti-Inflammatory and Antioxidant Activity of Gastrointestinal Tract
Ganoderma lucidum (Reishi mushroom) contains a wide range of bioactive compounds, including polysaccharides, triterpenoids, and peptides, some of which exhibit remarkable anti-inflammatory and antioxidant properties in various experimental models. These effects likely contribute to its gastroprotective action by mitigating inflammation and oxidative stress within the gastric mucosa. Research by Kamra et al demonstrated substantial antioxidant activity in various Ganoderma lucidum extracts.119 For instance, Ganoderma lucidum polysaccharides (GLPs) have demonstrated efficacy in preventing induced gastric ulcers in animal models. Pre-treatment with various GLP fractions has been shown to alleviate gastric mucosal congestion and bleeding, reduce serum myeloperoxidase levels and inflammatory markers, and enhance antioxidant activity. Additionally, GLPs increase the levels of protective factors, such as NO and epidermal growth factor EGFR. These findings suggest that GLPs hold promise as a natural source for functional foods aimed at preventing ethanol-induced gastric damage.120
Chemical Sensitivity and Immune Regulation
GLPs are widely used as adjuvants in cancer therapy, exhibiting promising anticancer properties. Ramin’s investigation into the synergistic effects of GLPs combined with docetaxel and flutamide on prostate cancer cells revealed that GLP, both independently and in combination with these chemotherapeutic agents, significantly promoted apoptosis while inhibiting cell migration and colony formation in PC3 and LNCaP cell lines. Furthermore, GLPs downregulated the expression of KLK2 and genes involved in the epithelial-mesenchymal transition (EMT) pathway, suggesting that GLPs enhance the sensitivity of prostate cancer cells to chemotherapy.121 Zhao et al demonstrated that Ganoderma lucidum effectively suppressed the growth of both chemotherapy-sensitive and chemotherapy-resistant epithelial ovarian cancer (EOC) cells, augmenting the cytotoxic effects of cisplatin.122 Additionally, research by Li Ren et al has shown that GLPs play a crucial role in modulating immune responses, including enhancing antitumor immunity, and supporting antiviral, antibacterial, and antifungal responses mediated by lymphocytes and bone marrow cells. GLPs can also amplify cytokine and antibody production, even when other stimuli, such as LPS and inflammatory factors, are present. These findings underscore the potential of GLPs to regulate various facets of the host immune system, including innate, cellular, and humoral immunity.123
Ginseng
Panax ginseng (PG), derived from the dried root and rhizome of Panax ginseng C.A. Mey. (Araliaceae), is renowned for its wide-ranging pharmacological effects, which are utilized to treat conditions such as inflammation, cancer, metabolic syndrome, and autoimmune diseases. The primary active constituents of ginseng include ginsenosides, ginseng polysaccharides, polyacetylenes, and peptides.124 Clinical studies have demonstrated the efficacy of ginseng-based compounds in mitigating chemotherapy-induced side effects.125
Antiemetic Mechanisms
Anti-Inflammatory and Antioxidant Activity of Gastrointestinal Tract
Ginseng’s bioactive constituents, particularly ginsenosides such as Rb1, Rg1, and Rd, exhibit notable anti-inflammatory and antioxidant properties, which have been corroborated in various experimental models. The well-established anti-inflammatory and antioxidant properties of ginseng may play a crucial role in its potential antiemetic effects. Ginsenosides have been shown to modulate key inflammatory pathways such as NF-κB and MAPK, as well as to decrease the production of pro-inflammatory cytokines, including TNF-α, IL-1β, and IL-6. Moreover, ginseng exhibits robust antioxidant activity by scavenging free radicals and protecting various tissues, including the GI tract, from oxidative damage. Research by Wu Yuqing et al demonstrated that pretreatment with ginsenoside Rh4 significantly reduced the extent of gastric lesions and the percentage of mucosal injury, reinforcing the gastroprotective effects of ginsenosides.126,127
Potential Regulation of Neurotransmitting System
Ginseng has been implicated in the modulation of the hypothalamic-pituitary-adrenal (HPA) axis, which governs stress responses and plays a role in the regulation of nausea. Additionally, certain ginsenosides exhibit potential effects on serotonergic and dopaminergic systems. Alkaloids and flavonoids found in various plants, including ginseng (Radix) and Flom, have demonstrated significant potential in regulating the 5-HT3 receptor, a mechanism that may contribute to the treatment of various chronic conditions. Recent studies have shown that these plant extracts exert effective antagonistic effects on the 5-HT3 receptor, suggesting their potential therapeutic utility in managing nausea.128
Chemical Sensitivity and Immune Regulation
Ginseng, often heralded as the “king of herbs”, has shown promise in enhancing the efficacy of chemotherapeutic agents while mitigating their adverse effects. Rich in anticancer compounds, particularly ginsenosides, ginseng has been the subject of extensive research, with findings indicating that it can both sensitize tumors to chemotherapy and reduce treatment-related side effects. For example, Fishbein et al demonstrated that Asian ginseng could enhance the anticancer activity of 5-FU against human colorectal cancer (CRC) cells. Studies have revealed that the combination of Protopanaxadiol and 5-FU elicits stronger antiproliferative and pro-apoptotic responses in human CRC cell lines.129 Furthermore, ginseng demonstrates immunomodulatory effects. Research by Yang Chunmei et al highlighted that ginsenoside Rh2 (GRh2) exhibits significant antitumor activity, primarily by enhancing NK cell cytotoxicity and improving immune surveillance, which may further contribute to its therapeutic potential in cancer treatment.130
Grape Seed
Grapes (Vitis vinifera) have long been cultivated for their medicinal, nutritional, and economic value. Grape seeds are particularly rich in polyphenolic compounds, most notably flavonoids such as catechins, gallic acid and proanthocyanidins. Studies have demonstrated the cardioprotective, anticancer, and anti-inflammatory properties of grape seed extract (GSE). Proanthocyanidins are believed to confer multiple health benefits.9
Antiemetic Mechanism
Gastric Protection and Support
Grape seed extract, abundant in proanthocyanidins (PACs), which are oligomeric and polymeric flavonoids, is renowned for its potent antioxidant properties. These PACs scavenge free radicals and prevent oxidative damage, potentially contributing to gastric mucosal protection. Furthermore, PACs may influence the digestion, absorption, and bioavailability of nutrients by interacting with carbohydrates, proteins, lipids, and their respective enzymes and transporters. Additionally, PACs exhibit prebiotic-like effects by modulating the gut microbiota, promoting the growth of beneficial bacteria such as Bifidobacterium. These diverse actions collectively underscore the potential of PACs in the prevention and management of gastrointestinal diseases.131
Anti-Inflammatory and Antioxidant Activity in the Gastrointestinal Tract
GSE is renowned for its potent antioxidant properties, primarily attributed to its rich content of proanthocyanidins, which are among the most powerful plant-derived antioxidants. These proanthocyanidins effectively scavenge a variety of free radicals and inhibit lipid peroxidation, thereby reducing oxidative stress. In addition to its antioxidant effects, GSE exhibits notable anti-inflammatory properties, which may help mitigate nausea associated with gastrointestinal inflammation. Research by Rameshprabu et al demonstrated the protective effects of GSE against LPS-induced oxidative stress, inflammation, and barrier dysfunction in human Caco-2 colonocytes.132
Antispasmodic Effect on Gastrointestinal Smooth Muscle
GSE has been shown to modulate gastrointestinal smooth muscle contractility, a mechanism that may help relieve nausea associated with muscular spasms. Studies indicate that GSE significantly reduces histamine-induced contractions in the ileum of guinea pigs, potentially through the inhibition of H1 histamine receptors. Further investigations are needed to explore the potential effects of grape seed extract on smooth muscle relaxation in human subjects.133
Chemosensitization and Immunomodulatory Effects
MDR remains a formidable challenge in cancer therapy. Lin et al investigated the potential of GSE to overcome MDR in human leukemia cell lines (HL-60 and HL-60/ADR). Their study demonstrated that GSPE, when combined with cytarabine (Ara-C), significantly reduced the IC50 of both Ara-C and doxorubicin (ADR) in resistant HL-60/ADR cells. GSE was found to downregulate the expression of multidrug resistance-associated proteins (MRP1, MDR1, and LRP) and to induce apoptosis, indicating its potential as a promising adjuvant for enhancing chemotherapy efficacy in MDR leukemia.134 Moreover, Mousavi S et al demonstrated that a proprietary GSE containing proanthocyanidins upregulated the expression of several immune-related genes in the mucosal tissues of rainbow trout. These genes included complement component 3 (C3), lysozyme (lys), omDB-3, interferon-gamma (IFN-γ), and TNF-α.135
Other Complementary Medicinal Plants
While the preceding sections have focused on medicinal plants with strong empirical evidence supporting their use in CINV management, several other botanicals with a more limited research base also warrant consideration. These plants, although less extensively studied, show preliminary efficacy or have traditional uses that suggest they may be beneficial in treating CINV. Further research is needed to fully elucidate their mechanisms of action and clinical effectiveness.
Holy Basil
Holy basil has long been used in traditional medicine to alleviate digestive discomfort, including nausea. Holy basil may exert several indirect mechanisms that complement the actions of other antiemetic agents, such as its anti-inflammatory properties. Holy basil’s antioxidant effects may help prevent oxidative stress, which is often implicated in nausea. Additionally, as an adaptogen, holy basil may enhance the body’s ability to cope with stress, a known exacerbating factor for nausea. While holy basil holds promise as a natural remedy for nausea, further studies are required to confirm its efficacy and determine optimal dosages and formulations.136
Saffron
Saffron is primarily known for its effects on cardiovascular health, inflammation, and menstrual pain. However, some of its properties may indirectly reduce nausea or vomiting, particularly through its anti-inflammatory effects. Saffron contains bioactive compounds with anti-inflammatory properties that may alleviate nausea associated with gastrointestinal inflammation. Furthermore, certain studies suggest that saffron may influence serotonin levels, a neurotransmitter implicated in nausea and vomiting. Although this mechanism warrants further exploration, additional research is needed to specifically assess saffron’s potential as an antiemetic agent.137
Purslane
Purslane has a long history of medicinal use, and its pharmacological properties suggest it may hold potential for alleviating nausea and vomiting. Purslane contains a variety of compounds with anti-inflammatory activity, and inflammation within the digestive system can sometimes lead to nausea. Additionally, purslane is rich in antioxidants that may protect against oxidative stress, a potential contributor to nausea. These mechanisms, however, remain indirect and require further investigation to confirm their role in purslane’s potential antiemetic action.138
Garlic and Onion
Garlic and onions possess a diverse array of medicinal and biological properties, primarily attributed to their rich spectrum of soluble bioactive compounds. While onions are primarily recognized for their characteristic flavor compounds, garlic is distinguished by its broader and more varied range of bioactive substances. These include lectins, prostaglandins, fructans, pectins, adenosine, a suite of B vitamins (B1, B2, B6), vitamin E, niacin, fatty acids, glycolipids, phosphatidic acid, essential amino acids, and saponins such as chlorogenic acid. These components contribute to their well-documented antifungal, antibacterial, antitumor, antithrombotic, and cholesterol-lowering effects. Beyond these established pharmacological activities, emerging evidence suggests that aged garlic extract (AGE) may offer protective benefits against the side effects of antitumor therapies, including nausea, vomiting, gastritis, gastric ulcers, bleeding, and intestinal ulcers. Additionally, onion consumption has been shown to stimulate gastrointestinal processes, enhancing nutrient absorption and reducing gastrointestinal transit time, which may help alleviate nausea and vomiting. However, further studies are needed to substantiate these claims, especially regarding the protective role of AGE in mitigating chemotherapy-induced side effects.139
Medicinal Plants That Can Be Used in Combination
Although individual medicinal plants have demonstrated efficacy in the management of CINV, traditional medicine often emphasizes the synergistic potential of plant combinations to enhance therapeutic outcomes. This section explores several promising combinations, underscoring their potential for synergistic effects in alleviating CINV while calling for further research to validate and optimize their clinical application.
Ginger and Pinellia
The combination of these two herbs is believed to offer a potent antiemetic effect. Due to the inherent toxicity of Pinellia, it is typically used in conjunction with ginger to enhance safety and broaden its therapeutic application. Ginger is thought to mitigate Pinellia’s toxic effects, making this combination particularly suitable for treating vomiting. Modern pharmacological studies support this notion, indicating that gingerol, the active compound in ginger, may inhibit the release of inflammatory factors and the production of ROS, potentially elucidating its protective role. A study by Cai Honglin, in which pregnant mice were administered a ginger-Pinellia decoction, found no adverse effects on the mothers or embryos, further validating the traditional claim of ginger’s ability to mitigate the toxicity of Pinellia.6
Ginger and Mint
The combination of these two herbs targets multiple pathways implicated in nausea and vomiting. For instance, ginger is often more effective in addressing motion sickness, pregnancy-related nausea, and chemotherapy-induced nausea, while mint is traditionally used to alleviate indigestion and nausea associated with bloating and gastrointestinal discomfort. This combination thus offers a broader spectrum of antiemetic action. Additionally, the refreshing taste of the ginger-mint combination may make it more palatable for individuals experiencing nausea, potentially improving tolerance. The synergistic effects of this combination not only enhance efficacy but also minimize the need for high doses of either herb, reducing the risk of adverse effects associated with excessive ginger or mint consumption.140
Ginger and Turmeric
The synergistic interaction between ginger and turmeric has been demonstrated in various studies, particularly in the context of inflammation inhibition. Xian Zhou et al explored the effects of combined ginger and turmeric extracts in attenuating inflammation. The ginger-turmeric combination, at a specific ratio, optimally suppressed the production of NO, TNF, and IL-6. This synergistic effect on TNF inhibition was confirmed in human THP-1 monocytes. Moreover, the combination upregulated the activity of nuclear factor erythroid 2-related factor 2 (Nrf2) and increased heme oxygenase-1 (HO-1) protein expression. Given that inflammation can provoke nausea and vomiting through various mechanisms, including direct stimulation of the vomiting center and gastric dysfunction, the anti-inflammatory properties of this ginger-turmeric combination make it a promising therapeutic strategy for managing nausea and vomiting.141
Ginger and Lemon
Al-Ataby et al investigated the anticancer and immunomodulatory properties of a combined lemon and ginger extract. In a mouse model of breast cancer, oral administration of the combined aqueous extract over 14 days resulted in significant apoptosis induction and inhibition of angiogenesis. Notably, 50% of the treated mice exhibited complete tumor regression, with an overall tumor reduction of 32.8%. Analysis of the extract revealed high concentrations of α-pinene and α-terpineol. These findings suggest that the combination of lemon and ginger extracts holds promise as a potential anticancer agent, warranting further investigation for its role as an adjunct to conventional cancer therapies.142
Ginger and Cloves
Ginger and cloves offer complementary pharmacological activities that may act synergistically in the management of CINV. Cloves are known for their ability to alleviate gastrointestinal discomfort, such as gas and bloating, which can exacerbate nausea. They also possess mild anesthetic and anti-inflammatory properties, with clove tea traditionally used to ease nausea. Ginger, with its well-established anti-inflammatory, antioxidant, and antiemetic properties, further enhances the therapeutic effects of cloves. A published patent highlights the synergistic potential of gingerol (from ginger) and eugenol (from cloves) in effectively managing CINV associated with cancer treatment. This combination warrants further exploration to validate its clinical efficacy.143
Additionally, Table 3 categorizes each plant according to the level of evidence (preclinical, clinical, traditional only). Although this review synthesizes the extensive evidence for medicinal plants in the management of CINV, several gaps and research priorities must be acknowledged in order to enhance the scientific rigor and clinical applicability of these findings. Many botanicals, such as turmeric, perilla, and cardamom, have encouraging evidence for their antiemetic effects but are currently still primarily preclinical or derived from traditional use, highlighting the need for well-designed clinical trials to validate these preliminary observations in cancer patients. More intensively studied plants, such as ginger and cannabis, have a broader evidence base.
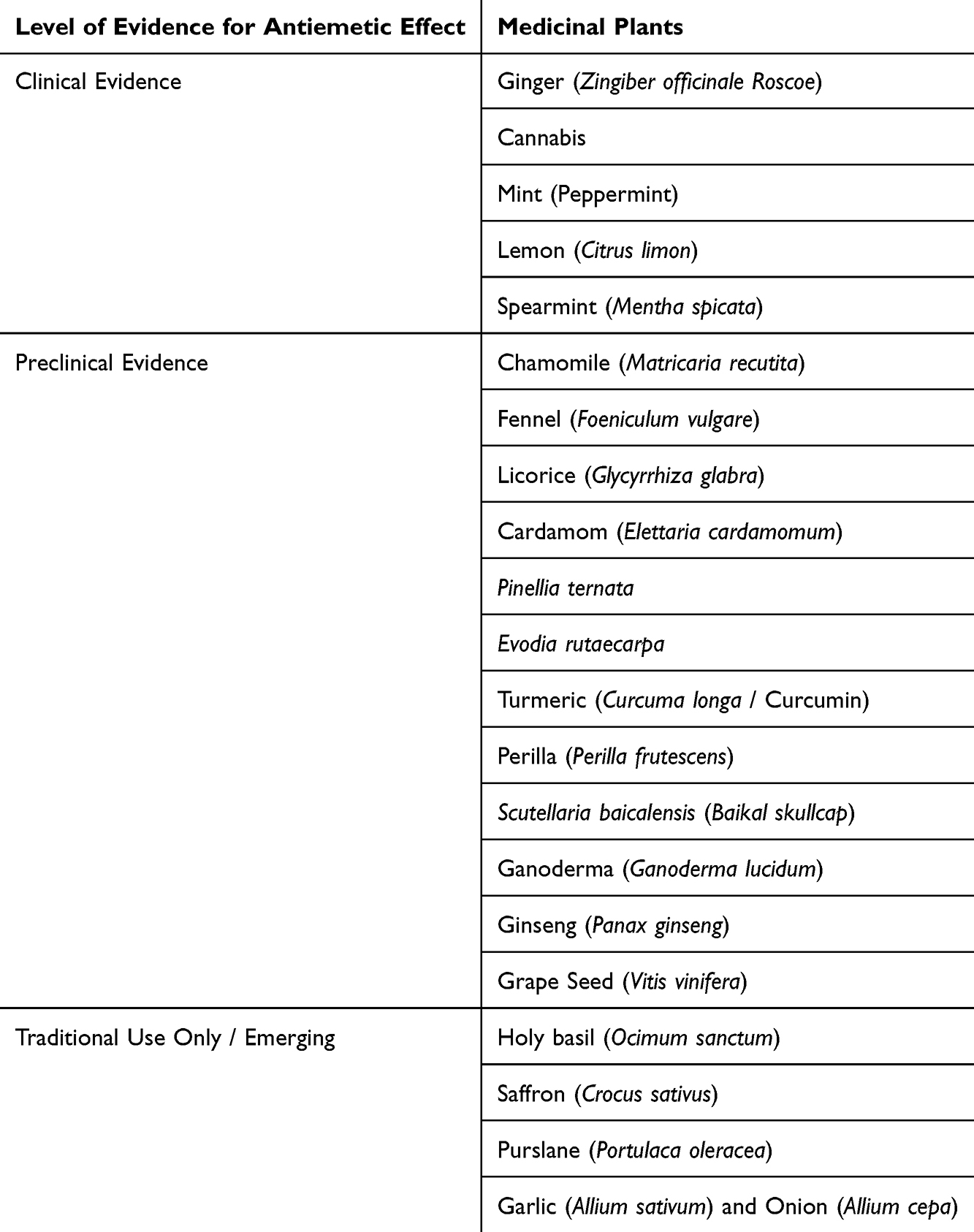 |
Table 3 Classification of Medicinal Plants by Level of Evidence for Antiemetic Effects |
Discussion
This systematic review provides a comprehensive analysis of medicinal plants utilized in the management of CINV. We identified numerous plants with robust evidence supporting their antiemetic efficacy, often through multiple mechanisms, including 5-HT3 receptor antagonism, modulation of the substance P/NK1 pathway, and anti-inflammatory activity. This multi-target approach offers distinct advantages over conventional single-target antiemetics. Furthermore, many of these plants exhibit pleiotropic effects, demonstrating not only CINV control but also chemosensitizing and immunomodulatory properties. This multifaceted therapeutic potential may represent a paradigm shift in supportive cancer care, enhancing patient outcomes and improving quality of life. Importantly, our analysis highlights the superior efficacy observed with plant combinations compared to monotherapy, further emphasizing their potential for optimizing CINV management.
In terms of antiemetic efficacy, although 5-HT3receptor antagonists (eg, ondansetron) and NK1receptor antagonists (eg, aprepitant) remain the cornerstone of CINV management, their limitations—such as incomplete efficacy and the potential for adverse effects—are well-documented.4 This review highlights the promising potential of medicinal plants to address these unmet needs. For example, ginger has shown comparable efficacy to pharmaceutical agents in alleviating both acute and delayed CINV, while also offering additional systemic benefits.144 Furthermore, while cannabinoids are known for their psychoactive properties, they have demonstrated superior efficacy over certain standard antiemetics in specific contexts, such as refractory or anticipatory CINV. These observations suggest that medicinal plants could serve as complementary therapies to conventional pharmacotherapy by targeting mechanisms not addressed by standard antiemetics. For instance, peppermint and chamomile exhibit relaxant effects on gastrointestinal smooth muscle, providing an additional layer of symptom relief not currently available through traditional antiemetic regimens. Additionally, the immunomodulatory and chemosensitizing properties of plants like ginger and cannabis present novel opportunities for enhancing the therapeutic index of chemotherapy.
Regarding clinical safety, standard antiemetics are often associated with adverse effects, including headache, constipation, diarrhea, and cardiac events. Dopamine antagonists, in particular, may also induce sedation and orthostatic hypotension.145,146 In contrast, the medicinal plants reviewed in this paper generally exhibit a favorable safety profile, particularly when compared to conventional antiemetics. Many of these plants, such as ginger, turmeric, and chamomile, have a long history of traditional use and demonstrate remarkable safety in contemporary clinical trials. This safety profile enhances their appeal as adjunctive therapies alongside standard antiemetics. Furthermore, the review identifies promising synergistic combinations—such as ginger with Pinellia or turmeric—where the combined therapeutic effects exceed the sum of their individual contributions. These findings suggest the potential for developing optimized combination therapies that maximize therapeutic efficacy while maintaining a favorable safety profile.147
Integrating medicinal plants with conventional antiemetic therapy offers several advantages, including enhanced antiemetic efficacy, reduced dosages of standard medications (and potentially fewer side effects), and a more holistic approach to patient care. Medicinal plants target complementary biological pathways not addressed by standard antiemetics, facilitating synergistic effects. This synergy may allow for lower doses of conventional medications while preserving therapeutic efficacy, thereby minimizing adverse events. Furthermore, this integrative approach could address multiple symptoms associated with chemotherapy, such as fatigue and anxiety. For example, studies have shown that supplementing a standard antiemetic regimen with ginger can further alleviate nausea severity in chemotherapy patients.148 However, integrating medicinal plants into standard oncology care presents several challenges. Healthcare providers require evidence-based guidelines to optimize patient selection, dosage, and monitoring. Additionally, potential herb-drug interactions must be rigorously evaluated, particularly considering the complex polypharmacy often encountered in cancer patients.
Future research priorities should include expanding clinical trials to investigate medicinal plants for CINV management and optimizing extraction and preparation methods to ensure consistent efficacy. Standardized techniques, such as high-performance liquid chromatography (HPLC), could be employed to quantify active constituents—such as gingerol in ginger or cannabinoids in cannabis—enabling precise dosing in clinical studies. While some antiemetic mechanisms of these plants are partially understood, further research is needed to fully elucidate their molecular and cellular pathways. For instance, investigating the interaction between gingerol and specific serotonin (5-HT3) receptor subtypes could provide insights into its antiemetic efficacy. Similarly, exploring the role of cannabinoids in modulating central and peripheral nervous system activity may reveal novel therapeutic targets for refractory CINV. Comparative trials evaluating medicinal plants against standard antiemetics, as well as studies investigating combination therapies, are essential to inform clinical decision-making.
Despite the promising findings, several limitations must be acknowledged. Standardization remains a significant challenge, as the concentration of active compounds in medicinal plants can vary considerably based on factors such as geographic origin, cultivation practices, and processing methods. This variability complicates both the interpretation of research findings and the establishment of consistent clinical efficacy. Future research should strategically prioritize rigorous clinical trials, standardization and quality control, and comparative and integrative studies to improve objectivity. Addressing these research priorities will help build a more solid evidence base to objectively evaluate the efficacy and safety of phytotherapy interventions and potentially incorporate them into comprehensive cancer supportive care strategies.
Conclusion
Medicinal plants present a compelling, multi-targeted therapeutic option that may enhance current strategies for CINV management, offering potential beyond symptomatic relief. Among the 22 plants studied, ginger, cannabis, and turmeric show the strongest evidence and more prominent antiemetic efficacy in clinical and preclinical models and exert anti-inflammatory effects. Their documented antiemetic, chemosensitizing, and immunomodulatory actions strongly support their further investigation. Future research should prioritize dose standardization, comprehensive safety profiling, and large-scale clinical trials to guide their evidence-based integration into oncology care.
Abbreviations
5-HT3, 5-Hydroxytryptamine Type 3; 5-HT3RA, 5-HT3 Receptor Antagonist; CB1, Cannabinoid-1; CBD, Cannabidiol; CINV, Chemotherapy-Induced Nausea and Vomiting; CIS, Cisplatin; COX-2, Cyclooxygenase-2; CTZ, Chemoreceptor Trigger Zone; DA, Dopamine; ECS, Endocannabinoid System; GABA, Gamma-Aminobutyric acid; GI, Gastrointestinal; IL-10, Interleukin-10; IL-1β, Interleukin-1 beta; IL-6, Interleukin-6; LPS, Lipopolysaccharide; MRP, Multidrug Resistance-associated Protein; NF-κB, Nuclear Factor kappa-light-chain-enhancer of activated B cells; NK cells, Natural Killer cells; NK-1, Neurokinin-1; NK1RA, NK1 Receptor Antagonist; NO, Nitric Oxide; PGE, Prostaglandin E; P-gp, P-glycoprotein; ROS, Reactive Oxygen Species; TNF-α, Tumor Necrosis Factor-alpha.
Data Sharing Statement
The data for this study are available from the corresponding author on reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Sisco-Qilu Oncology Research Fund (2019) [Grant No. Y-QL2019-0380], the Sisco-Hutchison MediPharma Oncology Research Fund (2021) [Grant No. Y-HH202101-0194], the Liaoning Province Science and Technology Joint Planning (Fund) Project (2023) [Grant No. 2023-MSLH-165], the Spark Program - Clinical Research Innovation and Development Fund for Cancer Treatment (2023) and 2024 Medical Research Project of China Health & Medical Development Foundation.
Disclosure
The authors declare that they have no conflicts of interest to disclose.
References
1. Piechotta V, Adams A, Haque M, et al. Antiemetics for adults for prevention of nausea and vomiting caused by moderately or highly emetogenic chemotherapy: a network meta-analysis. Cochrane Database Syst Rev. 2021;11(11):CD012775.
2. Zhou J-G, Huang L, Jin S-H, et al. Olanzapine combined with 5-hydroxytryptamine type 3 receptor antagonist (5-HT3 RA) plus dexamethasone for prevention and treatment of chemotherapy-induced nausea and vomiting in high and moderate emetogenic chemotherapy: a systematic review and meta-analysis of randomised controlled trials. ESMO Open. 2020;5(1). doi:10.1136/esmoopen-2019-000621
3. Jordan K, Gralla R, Jahn F, Molassiotis A. International antiemetic guidelines on chemotherapy induced nausea and vomiting (CINV): content and implementation in daily routine practice. Eur J Pharmacol. 2014;722:197–202. doi:10.1016/j.ejphar.2013.09.073
4. Rajabalizadeh R, Ghasemzadeh Rahbardar M, Hosseinzadeh H. Medicinal herbs in treating chemotherapy‐induced nausea and vomiting: a review. Phytother Res. 2022;36(10):3691–3708. doi:10.1002/ptr.7563
5. Antonarakis ES, Hain RD. Nausea and vomiting associated with cancer chemotherapy: drug management in theory and in practice. Arch Dis Child. 2004;89(9):877–880. doi:10.1136/adc.2003.037341
6. Li Ang CL. Research progress on the efficacy and compatibility of pinellia ternata. Front Med Sci Res. 2022;4(12):28–34. doi:10.25236/fmsr.2022.041205
7. Aapro M. CINV: still troubling patients after all these years. Support Care Cancer. 2018;26(Suppl 1):5–9. doi:10.1007/s00520-018-4131-3
8. Escobar Y, Cajaraville G, Virizuela JA, et al. Incidence of chemotherapy-induced nausea and vomiting with moderately emetogenic chemotherapy: ADVICE (Actual Data of Vomiting Incidence by Chemotherapy Evaluation) study. Support Care Cancer. 2015;23(9):2833–2840. doi:10.1007/s00520-015-2809-3
9. Haniadka R, Popouri S, Palatty PL, Arora R, Baliga MS. Medicinal plants as antiemetics in the treatment of cancer. Integr Cancer Ther. 2011;11(1):18–28. doi:10.1177/1534735411413266
10. Escobar Alvarez Y, De Castro Carpeno J, Bell D, Drago A, Franceschetti A. Prevention of chemotherapy-induced nausea and vomiting in the real-world setting in Spain. Clin Transl Oncol. 2021;23(10):2155–2162. doi:10.1007/s12094-021-02623-8
11. Zhang M, Zhao R, Wang D, et al. Ginger (Zingiber officinale Rosc.) and its bioactive components are potential resources for health beneficial agents. Phytother Res. 2021;35(2):711–742. doi:10.1002/ptr.6858
12. Semwal RB, Semwal DK, Combrinck S, Viljoen AM. Gingerols and shogaols: important nutraceutical principles from ginger. Phytochemistry. 2015;117:554–568. doi:10.1016/j.phytochem.2015.07.012
13. Dai Y, Zhao Y, Nie K, Di Sotto A. The antiemetic mechanisms of gingerols against chemotherapy-induced nausea and vomiting. Evid Based Complement Alternat Med. 2022;2022:1–14. doi:10.1155/2022/1753430
14. Wang YU. Effect of gingerol on substance P and NK1 receptor expression in a vomiting model of mink. Chin Med J. 2010;123(4):478–484.
15. Tian L, Qian W, Qian Q, Zhang W, Cai X. Gingerol inhibits cisplatin-induced acute and delayed emesis in rats and minks by regulating the central and peripheral 5-HT, SP, and DA systems. J Nat Med. 2020;74(2):353–370. doi:10.1007/s11418-019-01372-x
16. Nikkhah Bodagh M, Maleki I, Hekmatdoost A. Ginger in gastrointestinal disorders: a systematic review of clinical trials. Food Sci Nutr. 2019;7(1):96–108. doi:10.1002/fsn3.807
17. Bischoff-Kont I, Fürst R. Benefits of ginger and its constituent 6-shogaol in inhibiting inflammatory processes. Pharmaceuticals. 2021;14(6):571. doi:10.3390/ph14060571
18. Mao QQ, Xu XY, Cao SY, et al. Bioactive compounds and bioactivities of ginger (Zingiber officinale Roscoe). Foods. 2019;8(6):185. doi:10.3390/foods8060185
19. de Lima RMT, Dos Reis AC, de Menezes AAPM, et al. Protective and therapeutic potential of ginger (Zingiber officinale) extract and [6]‐gingerol in cancer: a comprehensive review. Phytother Res. 2018;32(10):1885–1907. doi:10.1002/ptr.6134
20. Mahomoodally MF, Aumeeruddy MZ, Rengasamy KRR, et al. Ginger and its active compounds in cancer therapy: from folk uses to nano-therapeutic applications. Semin Cancer Biol. 2021;69:140–149. doi:10.1016/j.semcancer.2019.08.009
21. Kim SD, Kwag EB, Yang MX, Yoo HS. Efficacy and safety of ginger on the side effects of chemotherapy in breast cancer patients: systematic review and meta-analysis. Int J Mol Sci. 2022;23(19). doi:10.3390/ijms231911267
22. Zaami S, Di Luca A, Di Luca NM, Montanari Vergallo G. Medical use of cannabis: Italian and European legislation. Eur Rev Med Pharmacol Sci. 2018;22(4):1161–1167. doi:10.26355/eurrev_201802_14405
23. Amin MR, Ali DW. Pharmacology of medical cannabis. Adv Exp Med Biol. 2019;1162:151–165.
24. Parker LA, Rock EM, Limebeer CL. Regulation of nausea and vomiting by cannabinoids. Br J Pharmacol. 2011;163(7):1411–1422. doi:10.1111/j.1476-5381.2010.01176.x
25. Abrams DI, Guzman M. Cannabis in cancer care. Clin. Pharmacol. Ther. 2015;97(6):575–586. doi:10.1002/cpt.108
26. Xiong W, Koo BN, Morton R, Zhang L. Psychotropic and nonpsychotropic cannabis derivatives inhibit human 5-HT3A receptors through a receptor desensitization-dependent mechanism. Neuroscience. 2011;184:28–37. doi:10.1016/j.neuroscience.2011.03.066
27. Yang KH, Galadari S, Isaev D, Petroianu G, Shippenberg TS, Oz M. The nonpsychoactive cannabinoid cannabidiol inhibits 5-hydroxytryptamine3A receptor-mediated currents in Xenopus laevis oocytes. J Pharmacol Exp Ther. 2010;333(2):547–554. doi:10.1124/jpet.109.162594
28. Uranga JA, Vera G, Abalo R. Cannabinoid pharmacology and therapy in gut disorders. Biochem Pharmacol. 2018;157:134–147. doi:10.1016/j.bcp.2018.07.048
29. Song Q, Zhang W, Shi D, et al. Overexpression of cannabinoid receptor 2 is associated with human breast cancer proliferation, apoptosis, chemosensitivity and prognosis via the PI3K/Akt/mTOR signaling pathway. Cancer Med. 2023;12(12):13538–13550. doi:10.1002/cam4.6037
30. Almogi-Hazan O, Or R. Cannabis, the Endocannabinoid System and Immunity-the Journey from the Bedside to the Bench and Back. Int J Mol Sci. 2020;21(12):4448. doi:10.3390/ijms21124448
31. Scarpellini E, Broeders B, Schol J, et al. The use of peppermint oil in gastroenterology. Curr Pharm Des. 2023;29(8):576–583. doi:10.2174/1381612829666230328163449
32. Chumpitazi BP, Kearns GL, Shulman RJ. Review article: the physiological effects and safety of peppermint oil and its efficacy in irritable bowel syndrome and other functional disorders. Aliment Pharmacol Ther. 2018;47(6):738–752. doi:10.1111/apt.14519
33. Hills JM, Aaronson PI. The mechanism of action of peppermint oil on gastrointestinal smooth muscle. An analysis using patch clamp electrophysiology and isolated tissue pharmacology in rabbit and Guinea pig. Gastroenterology. 1991;101(1):55–65. doi:10.1016/0016-5085(91)90459-x
34. Yin Y, Lee SY. Current view of ligand and lipid recognition by the menthol receptor TRPM8. Trends Biochem Sci. 2020;45(9):806–819. doi:10.1016/j.tibs.2020.05.008
35. Hejna M, Kovanda L, Rossi L, Liu Y. Mint oils: in vitro ability to perform anti-inflammatory, antioxidant, and antimicrobial activities and to enhance intestinal barrier integrity. Antioxidants. 2021;10(7):1004. doi:10.3390/antiox10071004
36. Kapp K, Orav A, Roasto M, et al. Composition and antibacterial effect of mint flavorings in candies and food supplements. Planta Med. 2020;86(15):1089–1096. doi:10.1055/a-1158-1699
37. Nagai K, Tamura M, Murayama R, Fukuno S, Ito T, Konishi H. Development of multi-drug resistance to anticancer drugs in HepG2 cells due to MRP2 upregulation on exposure to menthol. PLoS One. 2023;18(9):e0291822. doi:10.1371/journal.pone.0291822
38. Ciliberti MG, Albenzio M, Sevi A, Frabboni L, Marino R, Caroprese M. Immunomodulatory role of Rosmarinus officinalis L. Mentha x piperita L. and Lavandula angustifolia L. Essential oils in sheep peripheral blood mononuclear cells. Vet Sci. 2024;11(4). doi:10.3390/vetsci11040157
39. Dai YL, Li Y, Wang Q, et al. Chamomile: a review of its traditional uses, chemical constituents, pharmacological activities and quality control studies. Molecules. 2022;28(1):133. doi:10.3390/molecules28010133
40. Silveira ES, Bezerra SB, Ávila KS, et al. Gastrointestinal effects of standardized Brazilian phytomedicine (Arthur de Carvalho Drops®) containing Matricaria recutita, Gentiana lutea and Foeniculum vulgare. Pathophysiology. 2019;26(3–4):349–359. doi:10.1016/j.pathophys.2019.09.002
41. Menghini L, Ferrante C, Leporini L, et al. An hydroalcoholic chamomile extract modulates inflammatory and immune response in HT29 cells and isolated rat colon. Phytother Res. 2016;30(9):1513–1518. doi:10.1002/ptr.5655
42. Vissiennon C, Hammoud D, Rodewald S, et al. Chamomile flower, myrrh, and coffee charcoal, components of a traditional herbal medicinal product, diminish proinflammatory activation in human macrophages. Planta med. 2017;83(10):846–854. doi:10.1055/s-0043-104391
43. Johnston GA. Flavonoid nutraceuticals and ionotropic receptors for the inhibitory neurotransmitter GABA. Neurochem Int. 2015;89:120–125. doi:10.1016/j.neuint.2015.07.013
44. Farhan M. Insights on the role of polyphenols in combating cancer drug resistance. Biomedicines. 2023;11(6):1709. doi:10.3390/biomedicines11061709
45. Huang J, Chen X, Chang Z, Xiao C, Najafi M. Boosting. Anti-tumour immunity using adjuvant apigenin. Anticancer Agents Med Chem. 2023;23(3):266–277. doi:10.2174/1871520622666220523151409
46. Rahayu M, Kalima T, Martgrita MM, et al. Ethnobotany and diversity of Citrus spp. (Rutaceae) as a source of “Kem-kem” traditional medicine used among the Karo sub-ethnic in North Sumatra, Indonesia. Heliyon. 2024;10(9):e29721. doi:10.1016/j.heliyon.2024.e29721
47. Kathem SH, Nasrawi YS, Mutlag SH, Nauli SM. Limonene exerts anti-inflammatory effect on LPS-induced jejunal injury in mice by inhibiting NF-kappaB/AP-1 pathway. Biomolecules. 2024;14(3):334. doi:10.3390/biom14030334
48. Denkova-Kostova R, Teneva D, Tomova T, et al. Chemical composition, antioxidant and antimicrobial activity of essential oils from tangerine (Citrus reticulata L.), grapefruit (Citrus paradisi L.), lemon (Citrus lemon L.) and cinnamon (Cinnamomum zeylanicum Blume). Z Naturforsch C J Biosci. 2021;76(5–6):175–185. doi:10.1515/znc-2020-0126
49. Das S, Gazdag Z, Szente L, et al. Antioxidant and antimicrobial properties of randomly methylated beta cyclodextrin - captured essential oils. Food Chem. 2019;278:305–313. doi:10.1016/j.foodchem.2018.11.047
50. de Sousa DPMR, de Araújo Ribeiro LA, de Lima JT. Spasmolytic activity of carvone and limonene enantiomers. Nat Prod Commun. 2015;10(11):1893–1896.
51. de Cassia da Silveira e Sa R, Andrade LN, De Sousa DP. A review on anti-inflammatory activity of monoterpenes. Molecules. 2013;18(1):1227–1254. doi:10.3390/molecules18011227
52. Yoon WJ, Lee NH, Hyun CG. Limonene suppresses lipopolysaccharide-induced production of nitric oxide, prostaglandin E2, and pro-inflammatory cytokines in RAW 264.7 macrophages. J Oleo Sci. 2010;59(8):415–421. doi:10.5650/jos.59.415
53. Lima NG, De Sousa DP, Pimenta FC, et al. Anxiolytic-like activity and GC-MS analysis of (R)-(+)-limonene fragrance, a natural compound found in foods and plants. Pharmacol Biochem Behav. 2013;103(3):450–454. doi:10.1016/j.pbb.2012.09.005
54. Yavari Kia P, Safajou F, Shahnazi M, Nazemiyeh H. The effect of lemon inhalation aromatherapy on nausea and vomiting of pregnancy: a double-blinded, randomized, controlled clinical trial. Iran Red Crescent Med J. 2014;16(3):e14360. doi:10.5812/ircmj.14360
55. Komiya M, Takeuchi T, Harada E. Lemon oil vapor causes an anti-stress effect via modulating the 5-HT and DA activities in mice. Behav. Brain Res. 2006;172(2):240–249. doi:10.1016/j.bbr.2006.05.006
56. Yun J. Limonene inhibits methamphetamine-induced locomotor activity via regulation of 5-HT neuronal function and dopamine release. Phytomedicine. 2014;21(6):883–887. doi:10.1016/j.phymed.2013.12.004
57. Lan T, Luo X, Pi Z, et al. Disruption of NADPH homeostasis by total flavonoids from Adinandra nitida Merr. ex Li leaves triggers ROS-dependent p53 activation leading to apoptosis in non-small cell lung cancer cells. J Ethnopharmacol. 2024;332:118340.
58. Luetragoon T, Thongsri Y, Daotak K, Potup P, Usuwanthim K. Anti-proliferative and immunomodulatory properties of kaffir lime leaves and bioactive compounds on macrophages co-cultured with squamous cell carcinoma. PLoS One. 2023;18(2):e0281378. doi:10.1371/journal.pone.0281378
59. Vella FM, Pignone D, Laratta B. The Mediterranean species calendula officinalis and foeniculum vulgare as valuable source of bioactive compounds. Molecules. 2024;29(15):3594. doi:10.3390/molecules29153594
60. Rauf A, Akram M, Semwal P, et al. Antispasmodic potential of medicinal plants: a comprehensive review. Oxid Med Cell Longev. 2021;2021(1). doi:10.1155/2021/4889719
61. Korinek M, Handoussa H, Tsai YH, et al. Anti-$$um and MAPKs. Front Pharmacol. 2021;12:674095. doi:10.3389/fphar.2021.674095
62. Das B, Rabalais J, Kozan P, et al. The effect of a fennel seed extract on the STAT signaling and intestinal barrier function. PLoS One. 2022;17(7):e0271045. doi:10.1371/journal.pone.0271045
63. Ramadan WS, Sait KH, Anfinan NM, Sait H. The chemosensitizing effect of aqueous extract of sweet fennel on cisplatin treated HeLa cells. Clin Exp Obstet Gynecol. 2016;43(3):358–364. doi:10.12891/ceog2125.2016
64. Darzi S, Khazraei S, Amirghofran Z. The immunoinhibitory and apoptosis-inducing activities of Foeniculum vulgare on human peripheral blood lymphocytes. Res Pharm Sci. 2018;13(2):103–110. doi:10.4103/1735-5362.223792
65. Souza FV, da Rocha MB, de Souza DP, Marcal RM. (-)-Carvone: antispasmodic effect and mode of action. Fitoterapia. 2013;85:20–24. doi:10.1016/j.fitote.2012.10.012
66. Mahendran G, Verma SK, Rahman LU. The traditional uses, phytochemistry and pharmacology of spearmint (Mentha spicata L.): a review. J Ethnopharmacol. 2021;278:114266. doi:10.1016/j.jep.2021.114266
67. Hashim MS, Lincy S, Remya V, Teena M, Anila L. Anti-spasmodic effect of Mentha spicata and its effect on calcium channels in the gut. Int J Pharm Sci Res. 2013;4(3):1020–1024.
68. Saeed SA, Khan I, Hameed A, Qureshi NA, Gilani AH. Protective effect of Mentha spicata and its major constituents against ethanol-induced gastric mucosal injury in rats: underlying mechanisms. Evid Based Complement Alternat Med. 2015. doi:10.1155/2015/183527
69. Hunt R, Dienemann J, Norton HJ, et al. Aromatherapy as treatment for postoperative nausea: a randomized trial. Anesth Analg. 2013;117(3):597–604. doi:10.1213/ANE.0b013e31824a0b1c
70. Abdelli N, Bouchez-Mahiout I, Yahia M, Sekkal FZ, Djaziri R. Immunomodulatory activity of Mentha spicata L. from Algeria. IntJ Pharmacogn Phytochem Res. 2017;9(4):529–535.
71. Wang KL, Yu YC, Chen HY, et al. Recent advances in Glycyrrhiza glabra (Licorice)-containing herbs alleviating radiotherapy- and chemotherapy-induced adverse reactions in cancer treatment. Metabolites. 2022;12(6). doi:10.3390/metabo12060535
72. Wu Y, Guo Y, Huang T, et al. Licorice flavonoid alleviates gastric ulcers by producing changes in gut microbiota and promoting mucus cell regeneration. Biomed Pharmacother. 2023;169(7):115868. doi:10.1016/j.biopha.2023.115868
73. Fu Y, Chen J, Li YJ, Zheng YF, Li P. Antioxidant and anti-inflammatory activities of six flavonoids separated from licorice. Food Chem. 2013;141(2):1063–1071. doi:10.1016/j.foodchem.2013.03.089
74. Herbrechter R, Ziemba PM, Hoffmann KM, Hatt H, Werner M, Gisselmann G. Identification of Glycyrrhiza as the rikkunshito constituent with the highest antagonistic potential on heterologously expressed 5-HT3A receptors due to the action of flavonoids. Front Pharmacol. 2015;6(2):226–234. doi:10.3389/fphar.2015.00130
75. Bhat AA, Moglad E, Afzal M, et al. The anticancer journey of liquiritin: insights into its mechanisms and therapeutic prospects. Curr Med Chem. 2024;39(3):1333–1342. doi:10.2174/0109298673315699240805111122
76. Ma X, Sun Z, Chen H, et al. 18beta-glycyrrhetinic acid suppresses Lewis lung cancer growth through protecting immune cells from ferroptosis. Cancer Chemother Pharmacol. 2024;93(6):575–585. doi:10.1007/s00280-024-04639-7
77. Ashokkumar K, Murugan M, Dhanya MK, Warkentin TD. Botany, traditional uses, phytochemistry and biological activities of cardamom [Elettaria cardamomum (L.) Maton] - A critical review. J Ethnopharmacol. 2020;246:112244. doi:10.1016/j.jep.2019.112244
78. Jamal A, Javed K, Aslam M, Jafri MA. Gastroprotective effect of cardamom, Elettaria cardamomum Maton. fruits in rats. J Ethnopharmacol. 2006;103(2):149–153. doi:10.1016/j.jep.2005.07.016
79. Ballester P, Cerdá B, Arcusa R, García-Muñoz AM, Marhuenda J, Zafrilla P. Antioxidant activity in extracts from Zingiberaceae family: cardamom, turmeric, and ginger. Molecules. 2023;28(10):4024. doi:10.3390/molecules28104024
80. Qiblawi S, Al-Hazimi A, Al-Mogbel M, Hossain A, Bagchi D. Chemopreventive effects of cardamom (Elettaria cardamomum L.) on chemically induced skin carcinogenesis in Swiss albino mice. J Med Food. 2012;15(6):576–580. doi:10.1089/jmf.2011.0266
81. Majdalawieh AF, Carr RI. In vitro investigation of the potential immunomodulatory and anti-cancer activities of black pepper (Piper nigrum) and cardamom (Elettaria cardamomum). J Med Food. 2010;13(2):371–381. doi:10.1089/jmf.2009.1131
82. Bai J, Qi J, Yang L, Wang Z, Wang R, Shi Y. A comprehensive review on ethnopharmacological, phytochemical, pharmacological and toxicological evaluation, and quality control of Pinellia ternata (Thunb.) Breit. J Ethnopharmacol. 2022;298:115650. doi:10.1016/j.jep.2022.115650
83. Choi NR, Park J, Ko SJ, et al. Prediction of the medicinal mechanisms of pinellia ternata breitenbach, a traditional medicine for gastrointestinal motility disorders, through network pharmacology. Plants. 2022;11(10):1348. doi:10.3390/plants11101348
84. Rozema E, Atanasov AG, Fakhrudin N, et al. Selected extracts of Chinese herbal medicines: their effect on NF-kappaB, PPARalpha and PPARgamma and the respective bioactive compounds. Evid Based Complement Alternat Med. 2012;2012:983023. doi:10.1155/2012/983023
85. Tao X, Li J, He J, et al. Pinellia ternata (Thunb.) Breit. attenuates the allergic airway inflammation of cold asthma via inhibiting the activation of TLR4-medicated NF-kB and NLRP3 signaling pathway. J Ethnopharmacol. 2023;28(315):1116720.
86. Zhang QL, Gong LL, Li GS, Du J, Nie K. Effects of Alkaloids of Pinellia Ternata on 5-HT3 receptor and NK1 receptor in isolated Guinea-pig Ileum. J ShandongUniv Tradit Chin Med. 2017;41(05):466–468.
87. W Y. Comparative study on the immune function of five kinds of Gansu authentic Chinese herbal medicines in aging mice. J Beijing Union Univ. 2016;30(2):77–82.
88. Guo JiaYu GJ, Meng Juan MJ, Du JinHui DJ. Effects of Gancao Xiexin Decoction on main intestinal flora and sIgA in mice with intestinal flora disorder induced by antibiotics. J Chin J Microecol. 2019;31(11):1246–1259.
89. Xu CCL. Research progress of Wuzhuyu decoction. ChiMed. 2022;37(10):5853–5856.
90. Gao YX, Jiang LL, Zhang Q, Zuo DZ, Li XW. Rutaecarpine protects against bleomycin-induced pulmonary fibrosis through inhibiting Notch1/eIF3a signaling pathway in rats. China J Chin Mater Med. 2018;43(17):3530–3538.
91. Huang M, Li J, Huang W, Zhou Y, Cai L, Liu M. The effectiveness of Evodia rutaecarpa hot compress on the recovery of gastrointestinal function after laparoscopic surgery for colorectal cancer: a propensity score-matched retrospective cohort study. medRxiv. 2024. doi:10.1101/2024.05.07.24306986
92. Liao JF, Chiou WF, Shen YC, Wang GJ, Chen CF. Anti-inflammatory and anti-infectious effects of Evodia rutaecarpa (Wuzhuyu) and its major bioactive components. ChinMed. 2011;6:1–8.
93. Chen L, Hu Y, Ye Z, et al. Major indole alkaloids in evodia rutaecarpa: the latest insights and review of their impact on gastrointestinal diseases. Biomed Pharmacother. 2023;167:115495. doi:10.1016/j.biopha.2023.115495
94. Wang QS, Ding SL, Mao HP, Cui YL, Qi XJ. Antidepressant-like effect of ethanol extract from Zuojin Pill, containing two herbal drugs of Rhizoma Coptidis and Fructus Evodiae, is explained by modulating the monoaminergic neurotransmitter system in mice. J Ethnopharmacol. 2013;148(2):603–609. doi:10.1016/j.jep.2013.05.011
95. Zhu B, Zhao L, Liu Y, et al. Induction of phosphatase shatterproof 2 by evodiamine suppresses the proliferation and invasion of human cholangiocarcinoma. Int J Biochem Cell Biol. 2019;108:98–110. doi:10.1016/j.biocel.2019.01.012
96. Wei WT, Chen H, Wang ZH, et al. Enhanced antitumor efficacy of gemcitabine by evodiamine on pancreatic cancer via regulating PI3K/Akt pathway. Int J Biol Sci. 2012;8(1):1–14. doi:10.7150/ijbs.8.1
97. Bhupendra S, Rameshroo K, Shashikant C. Medicinal value of Curcuma cassia Roxb: an overview. Pharmaceut Biosci J. 2016;69–74. doi:10.20510/ukjpb/4/i6/134671
98. Ramaholimihaso T, Bouazzaoui F, Kaladjian A. Curcumin in depression: potential mechanisms of action and current evidence-a narrative review. Front Psychiatry. 2020;11:572533. doi:10.3389/fpsyt.2020.572533
99. Peng Y, Ao M, Dong B, et al. Anti-inflammatory effects of curcumin in the inflammatory diseases: status, limitations and countermeasures. Drug Des Devel Ther. 2021;15:4503–4525. doi:10.2147/DDDT.S327378
100. Purwar B, Shrivastava A, Arora N, Kumar A, Saxena Y. Effects of curcumin on the gastric emptying of albino rats. Indian J Physiol Pharmacol. 2012;56(2):168–173.
101. Kwiecien S, Magierowski M, Majka J, et al. Curcumin: a potent protectant against esophageal and gastric disorders. Int J Mol Sci. 2019;20(6):1477. doi:10.3390/ijms20061477
102. Jayarajan J, Angandoor S, Vedulla SH, et al. Curcumin induces chemosensitization to doxorubicin in Duke’s type B coloadenocarcinoma cell line. Mol Biol Rep. 2020;47(10):7883–7892. doi:10.1007/s11033-020-05866-w
103. Toden S, Okugawa Y, Jascur T, et al. Curcumin mediates chemosensitization to 5-fluorouracil through miRNA-induced suppression of epithelial-to-mesenchymal transition in chemoresistant colorectal cancer. Carcinogenesis. 2015;36(3):355–367. doi:10.1093/carcin/bgv006
104. Shafei A, Ramzy MM, Hegazy AI, et al. The molecular mechanisms of action of the endocrine disrupting chemical bisphenol A in the development of cancer. Gene. 2018;647:235–243. doi:10.1016/j.gene.2018.01.016
105. Hou T, Netala VR, Zhang H, Xing Y, Li H, Zhang Z. Perilla frutescens: a rich source of pharmacological active compounds. Molecules. 2022;27(11):3578. doi:10.3390/molecules27113578
106. Adam G, Robu S, Flutur MM, et al. Applications of perilla frutescens extracts in clinical practice. Antioxidants. 2023;12(3):727. doi:10.3390/antiox12030727
107. Ahmed HM. Ethnomedicinal, phytochemical and pharmacological investigations of Perilla frutescens (l.) Britt. Molecules. 2018;24(1):102. doi:10.3390/molecules24010102
108. Kangwan N, Pintha K, Lekawanvijit S, Suttajit M. Rosmarinic acid enriched fraction from perilla frutescens leaves strongly protects indomethacin-induced gastric ulcer in rats. Biomed Res Int. 2019;2019:9514703. doi:10.1155/2019/9514703
109. Abd El-Hafeez AA, Fujimura T, Kamei R, et al. Synergistic tumor suppression by a Perilla frutescens-derived methoxyflavanone and anti-cancer tyrosine kinase inhibitors in A549 human lung adenocarcinoma. Cytotechnology. 2018;70(3):913–919. doi:10.1007/s10616-017-0124-1
110. Jung SJ, Baek HI, Park EO, et al. Immunomodulatory effects of supercritical CO(2) extracted oils from Portulaca oleracea and Perilla frutescens (PPCE) in healthy individuals: a randomized double-blind clinical trial. Food Funct. 2024. doi:10.1039/d4fo03361b
111. Shen J, Li P, Liu S, et al. Traditional uses, ten-years research progress on phytochemistry and pharmacology, and clinical studies of the genus Scutellaria. J Ethnopharmacol. 2021;265:113198. doi:10.1016/j.jep.2020.113198
112. Ribeiro ARS, Do Nascimento Valença JD, da Silva Santos J, et al. The effects of baicalein on gastric mucosal ulcerations in mice: protective pathways and anti-secretory mechanisms. Chem. Biol. Interact. 2016;260:33–41. doi:10.1016/j.cbi.2016.10.016
113. Wen Y, Wang Y, Zhao C, Zhao B, Wang J. The pharmacological efficacy of baicalin in inflammatory diseases. Int J Mol Sci. 2023;24(11):9317. doi:10.3390/ijms24119317
114. Liao H, Ye J, Gao L, Liu Y. The main bioactive compounds of Scutellaria baicalensis Georgi. for alleviation of inflammatory cytokines: a comprehensive review. Biomed Pharmacother. 2021;133(6):110917. doi:10.1016/j.biopha.2020.110917
115. Sripathi R, Ravi S. Ethnopharmacology, phytoconstituents, essential oil composition and biological activities of the genus Scutellaria. J Pharm Sci Res. 2017;9(3):275.
116. Wu X, Zhang H, Salmani JM, Fu R, Chen B. Advances of wogonin, an extract from Scutellaria baicalensis, for the treatment of multiple tumors. Onco Targets Ther. 2016;9:2935–2943. doi:10.2147/OTT.S105586
117. Zeng A, Liang X, Zhu S, et al. Baicalin, a potent inhibitor of NF-kappaB signaling pathway, enhances chemosensitivity of breast cancer cells to docetaxel and inhibits tumor growth and metastasis both in vitro and in vivo. Front Pharmacol. 2020;11:879. doi:10.3389/fphar.2020.00879
118. Wang R, Wang C, Lu L, Yuan F, He F. Baicalin and baicalein in modulating tumor microenvironment for cancer treatment: a comprehensive review with future perspectives. Pharmacol Res. 2024;199(107032).
119. Kamra A, Bhatt AB. Evaluation of antimicrobial and antioxidant activity of Ganoderma lucidum extracts against human pathogenic bacteria. Int J Pharm Pharm Sci. 2012;4(2):359–362.
120. Tian B, Zhao Q, Xing H, et al. Gastroprotective effects of ganoderma lucidum polysaccharides with different molecular weights on ethanol-induced acute gastric injury in rats. Nutrients. 2022;14(7):1476. doi:10.3390/nu14071476
121. Rahimnia R, Akbari MR, Yasseri AF, et al. The effect of ganoderma lucidum polysaccharide extract on sensitizing prostate cancer cells to flutamide and docetaxel: an in vitro study. Sci Rep. 2023;13(1):18940. doi:10.1038/s41598-023-46118-8
122. Zhao S, Ye G, Fu G, Cheng JX, Yang BB, Peng C. Ganoderma lucidum exerts anti-tumor effects on ovarian cancer cells and enhances their sensitivity to cisplatin. Int J Oncol. 2011;38(5):1319–1327. doi:10.3892/ijo.2011.965
123. Ren L, Zhang J, Zhang T. Immunomodulatory activities of polysaccharides from Ganoderma on immune effector cells. Food Chem. 2021;340:127933. doi:10.1016/j.foodchem.2020.127933
124. Liu L, Xu FR, Wang YZ. Traditional uses, chemical diversity and biological activities of Panax L. (Araliaceae): a review. J Ethnopharmacol. 2020;263:112792. doi:10.1016/j.jep.2020.112792
125. Kim HS, Kim MK, Lee M, Kwon BS, Suh DH, Song YS. Effect of red ginseng on genotoxicity and health-related quality of life after adjuvant chemotherapy in patients with epithelial ovarian cancer: a randomized, double blind, placebo-controlled trial. Nutrients. 2017;9(7):772. doi:10.3390/nu9070772
126. Lee S, Kim MG, Ko SK, Kim HK, Leem KH, Kim YJ. Protective effect of ginsenoside Re on acute gastric mucosal lesion induced by compound 48/80. J Ginseng Res. 2014;38(2):89–96. doi:10.1016/j.jgr.2013.10.001
127. Wu Y, Duan Z, Qu L, Zhang Y, Zhu C, Fan D. Gastroprotective effects of ginsenoside Rh4 against ethanol-induced gastric mucosal injury by inhibiting the MAPK/NF-κB signaling pathway. Food Funct. 2023;14(11):5167–5181. doi:10.1039/D2FO03693B
128. Akotkar L, Aswar U, Ganeshpurkar A, Rathod K, Bagad P, Gurav S. Phytoconstituents targeting the serotonin 5-HT(3) receptor: promising therapeutic strategies for neurological disorders. ACS Pharmacol Transl Sci. 2024;7(6):1694–1710. doi:10.1021/acsptsci.4c00084
129. Zhao L, Zhao H, Zhao Y, et al. Role of ginseng, quercetin, and tea in enhancing chemotherapeutic efficacy of colorectal cancer. Front Med. 2022;9:939424. doi:10.3389/fmed.2022.939424
130. Yang C, Qian C, Zheng W, et al. Ginsenoside Rh2 enhances immune surveillance of natural killer (NK) cells via inhibition of ERp5 in breast cancer. Phytomedicine. 2024;123:155180. doi:10.1016/j.phymed.2023.155180
131. Chen Y, Wang J, Zou L, Cao H, Ni X, Xiao J. Dietary proanthocyanidins on gastrointestinal health and the interactions with gut microbiota. Crit Rev Food Sci Nutr. 2023;63(23):6285–6308. doi:10.1080/10408398.2022.2030296
132. Nallathambi R, Poulev A, Zuk JB, Raskin I. Proanthocyanidin-rich grape seed extract reduces inflammation and oxidative stress and restores tight junction barrier function in Caco-2 colon cells. Nutrients. 2020;12(6):1623. doi:10.3390/nu12061623
133. Glensk M, Hurst WJ, Glinski VB, Bednarski M, Glinski JA. Isolation of 1-(3’,4’-Dihydroxyphenyl)-3-(2”,4”,6”-trihydroxyphenyl)-propan-2-ol from grape seed extract and evaluation of its antioxidant and antispasmodic potential. Molecules. 2019;24(13):2466. doi:10.3390/molecules24132466
134. Lin KN, Jiang YL, Zhang SG, Huang SY, Li H. Grape seed proanthocyanidin extract reverses multidrug resistance in HL-60/ADR cells via inhibition of the PI3K/Akt signaling pathway. Biomed Pharmacother. 2020;125:109885. doi:10.1016/j.biopha.2020.109885
135. Mousavi S, Sheikhzadeh N, Hamidian G, et al. Changes in rainbow trout (Oncorhynchus mykiss) growth and mucosal immune parameters after dietary administration of grape (Vitis vinifera) seed extract. Fish Physiol Biochem. 2021;47(2):547–563. doi:10.1007/s10695-021-00930-z
136. Jahanger MA, Patra KK, Kumari S. A glance at the phytochemical and ethno-pharmacological understanding of four Ocimum species. Curr Pharm Biotechnol. 2023;24(9):1094–1107. doi:10.2174/1389201023666221003102423
137. Zeinali M, Zirak MR, Rezaee SA, Karimi G, Hosseinzadeh H. Immunoregulatory and anti-inflammatory properties of Crocus sativus (Saffron) and its main active constituents: a review. Iran J Basic Med Sci. 2019;22(4):334–344. doi:10.22038/ijbms.2019.34365.8158
138. Zhou YX, Xin HL, Rahman K, Wang SJ, Peng C, Zhang H. Portulaca oleracea L.: a review of phytochemistry and pharmacological effects. Biomed Res Int. 2015;2015:925631. doi:10.1155/2015/925631
139. Fakhar MMM, Darabinia M, Bani Mostafavi E, Rafiei A. A review of the therapeutic properties of garlic and onion in the traditions of traditional medicine and traditions of religion and health. Religion and Health. 2017;5(1):70–81.
140. Agus Y, Hidayat R. The effect of ginger water and mint leaves for reduce nausea and vomiting in the 1st trimester of pregnancy.
141. Zhou X, Afzal S, Wohlmuth H, et al. Synergistic anti-inflammatory activity of ginger and turmeric extracts in inhibiting lipopolysaccharide and interferon-gamma-induced proinflammatory mediators. Molecules. 2022;27(12). doi:10.3390/molecules27123877
142. Al-Ataby IA, Talib WH. Daily consumption of lemon and ginger herbal infusion caused tumor regression and activation of the immune system in a mouse model of breast cancer. Front Nutr. 2022;9:829101. doi:10.3389/fnut.2022.829101
143. Mann A. Biopotency role of culinary spices and herbs and their chemical constituents in health and commonly used spices in Nigerian dishes and snacks. Afr J Food Sci. 2011;5(3):111–124.
144. Marx WM, Teleni L, McCarthy AL, et al. Ginger (Zingiber officinale) and chemotherapy-induced nausea and vomiting: a systematic literature review. Nutr Rev. 2013;71(4):245–254. doi:10.1111/nure.12016
145. Orhan A, Nguyen C, Chan A, Herrstedt J. Pharmacokinetics, pharmacodynamics, safety, and tolerability of dopamine-receptor antagonists for the prevention of chemotherapy-induced nausea and vomiting. Expert Opin Drug Metab Toxicol. 2024;20(6):473–489. doi:10.1080/17425255.2024.2367593
146. Brygger L, Herrstedt J. Academy of Geriatric Cancer R. 5-Hydroxytryptamine3 receptor antagonists and cardiac side effects. Expert Opin Drug Saf. 2014;13(10):1407–1422. doi:10.1517/14740338.2014.954546
147. Zhou X, Munch G, Wohlmuth H, et al. Synergistic inhibition of pro-inflammatory pathways by ginger and turmeric extracts in RAW 264.7 cells. Front Pharmacol. 2022;13:818166. doi:10.3389/fphar.2022.818166
148. Ryan JL, Heckler CE, Roscoe JA, et al. Ginger (Zingiber officinale) reduces acute chemotherapy-induced nausea: a URCC CCOP study of 576 patients. Support Care Cancer. 2012;20(7):1479–1489. doi:10.1007/s00520-011-1236-3
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Combination Antiemetic Therapy for Chemotherapy-Induced Nausea and Vomiting in Patients with NSCLC Receiving Carboplatin-Based Chemotherapy
Shimokawa M, Haratake N, Takada K, Toyokawa G, Takamori S, Mizuki F, Takenaka T, Hayashi T
Cancer Management and Research 2022, 14:2673-2680
Published Date: 9 September 2022
Chemotherapy Induced Neutropenia, Febrile-Neutropenia and Determinants Among Solid Cancer Patients Attending Oncology Unit of a Tertiary Care Teaching Hospital in Ethiopia
Dessalegn M, Fantahun M, Yesufe AA, Hussein M, Tsegaye A
Cancer Management and Research 2023, 15:185-195
Published Date: 22 February 2023
Frailty and Cancer: Current Perspectives on Assessment and Monitoring
Goede V
Clinical Interventions in Aging 2023, 18:505-521
Published Date: 28 March 2023
Gastroparesis: Myths, Misconceptions, and Management
Cangemi DJ, Lacy BE
Clinical and Experimental Gastroenterology 2023, 16:65-78
Published Date: 6 June 2023
The Effect of Oral Care Intervention in Mucositis Management Among Pediatric Cancer Patients: An Updated Systematic Review
Nurhidayah I, Nurhaeni N, Allenidekania A, Gayatri D, Mediani HS
Journal of Multidisciplinary Healthcare 2024, 17:3497-3515
Published Date: 17 July 2024