Back to Journals » Cancer Management and Research » Volume 14
Combination Antiemetic Therapy for Chemotherapy-Induced Nausea and Vomiting in Patients with NSCLC Receiving Carboplatin-Based Chemotherapy
Authors Shimokawa M, Haratake N, Takada K, Toyokawa G, Takamori S, Mizuki F, Takenaka T, Hayashi T ![]()
Received 15 April 2022
Accepted for publication 5 September 2022
Published 9 September 2022 Volume 2022:14 Pages 2673—2680
DOI https://doi.org/10.2147/CMAR.S370961
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Yong Teng
Mototsugu Shimokawa,1,2,* Naoki Haratake,3,* Kazuki Takada,4 Gouji Toyokawa,5 Shinkichi Takamori,6 Fumitaka Mizuki,7 Tomoyoshi Takenaka,3 Toshinobu Hayashi8
1Department of Biostatistics, Graduate School of Medicine, Yamaguchi University, Yamaguchi, Japan; 2Cancer Biostatistics Laboratory, Clinical Research Institute, National Hospital Organization Kyushu Cancer Center, Fukuoka, Japan; 3Department of Surgery and Science, Graduate School of Medical Sciences, Kyushu University, Fukuoka, Japan; 4Department of Surgery, Saiseikai Fukuoka General Hospital, Fukuoka, Japan; 5Department of Surgery, National Hospital Organization Fukuoka National Hospital, Fukuoka, Japan; 6Department of Thoracic Oncology, National Hospital Organization Kyushu Cancer Center, Fukuoka, Japan; 7Center for Clinical Research, Yamaguchi University Hospital, Yamaguchi, Japan; 8Department of Pharmaceutical and Health Care Management, Faculty of Pharmaceutical Sciences, Fukuoka University, Fukuoka, Japan
*These authors contributed equally to this work
Correspondence: Mototsugu Shimokawa, Department of Biostatistics, Graduate School of Medicine, Yamaguchi University, 1-1-1 Minamikogushi, Ube, Yamaguchi, 755-8505, Japan, Tel +81-836-22-2805, Fax +81-836-22-2805, Email [email protected] Toshinobu Hayashi, Department of Pharmaceutical and Health Care Management, Faculty of Pharmaceutical Sciences, Fukuoka University, 8-19-1 Nanakuma, Jonan-ku, Fukuoka, 814-0180, Japan, Tel +81-92-871-6631, Email [email protected]
Purpose: The incidence of delayed chemotherapy-induced nausea and vomiting (CINV) in patients with non-small cell lung cancer (NSCLC) receiving carboplatin (CBDCA)-based chemotherapy (CBDCA + pemetrexed or paclitaxel) has not been clearly described. Therefore, we attempted to evaluate whether delayed CINV could be controlled using a combination of three antiemetics and identify individual risk factors.
Methods: We pooled data from two prospective observational studies, namely a nationwide survey of CINV and a prospective, observational study in Japan, to assess whether delayed CINV could be controlled using a combination of three antiemetics and identified individual risk factors via inverse probability treatment-weighted analysis.
Results: In total, 240 patients were evaluable in this study (median age, 66 years; male, 173; female, 67). The three-antiemetic regimen controlled delayed nausea (31.6% vs 47.3%) and vomiting (5.1% vs 23.1%) better than two antiemetics. Younger age (< 70 years; odds ratio [OR] = 2.233), motion sickness (OR = 3.472), drinking habits (OR = 1.972), receipt of the CBDCA + pemetrexed regimen (OR = 2.041), and the use of two antiemetics (OR = 1.926) were risk factors for delayed nausea. Female sex (OR = 3.372), drinking habits (OR = 2.272), receipt of the CBDCA+ pemetrexed regimen (OR = 2.314), and the use of two antiemetics (OR = 6.830) were risk factors for delayed vomiting.
Conclusion: Female sex, younger age, and receipt of the CBDCA + pemetrexed regimen increased the risk of CINV. Therefore, we recommend additional supportive antiemetics treatment for these patients.
Keywords: NSCLC, aprepitant, carboplatin, nausea, vomiting
Introduction
Lung cancer is the leading cause of cancer-related mortality worldwide.1 Cytotoxic chemotherapy is a key treatment for non-small cell lung cancer (NSCLC), but several new treatment options, such as tyrosine kinase inhibitors and immune checkpoint inhibitors, have been established.2,3 Although cytotoxic chemotherapy is effective against NSCLC, it is often associated with a variety of adverse effects. Chemotherapy-induced nausea and vomiting (CINV) is a relatively common side effect that is well known to have a strong negative effect on patients’ quality of life. For patients with NSCLC receiving cytotoxic chemotherapy, additive effects can be exerted by a combination of different classes of antiemetic medications such as corticosteroids, neurokinin 1 receptor antagonists (NK1RAs), anti-anxiolytics, and 5-hydroxytryptamine-3 receptor antagonists (5-HT3RAs), which are commonly recommended treatments for CINV.4–7
Among cytotoxic chemotherapies for patients with NSCLC, carboplatin (CBDCA)-based chemotherapy is a key option, and the combination of CBDCA-based chemotherapy and immune checkpoint inhibitors is one of the most common standard first-line treatments.8–11 Although CBDCA (area under the concentration–time curve [AUC] > 4) was previously considered to carry a moderate emetic risk, it has been recently re-classified to as having a high emetic risk, and the recommended antiemetic treatment for CBDCA (AUC > 4) was a three-drug combination of a 5-HT3RA, an NK1RA, and dexamethasone (DEX). However, this change was based on results obtained in patients who were treated with CBDCA as a part of a chemotherapy regimen with moderately emetogenicity or from studies with small sample sizes, and the occurrence of delayed CINV has not been well described in patients with NSCLC receiving CBDCA-based chemotherapy.12–17 In addition, detailed data are lacking on the risk factors for CINV.
In the current study, we performed a retrospective analysis of two prospective observational studies, including a nationwide survey of CINV and a prospective, observational study in Japan, to assess whether delayed CINV could be better controlled using a combination of three antiemetics and to identify individual risk factors.
Materials and Methods
Patients and Methods
We analyzed pooled patient-level data from two multicenter, prospective, observational studies. The individual study results were previously published (study A; a nationwide survey of CINV [UMIN000005971]18 and study B; a prospective, observational study with no available registry number).19 The prospective, observational studies enrolled patients in Japan who were scheduled to receive moderately or highly emetogenic chemotherapy regimens. Both studies were approved by the Independent Ethics Committee of National Hospital Organization Kyushu Cancer Center and conducted according to Declaration of Helsinki and the Ethical Guidelines for Medical and Health Research involving Human Subjects. Written informed consent was obtained from all participating patients before any related study procedure was initiated.
Data Collection
In both studies, patients were required to be at least 20 years old and have chemotherapy-naïve NSCLC.18,19 As in a previous study, delayed CINV was defined as any nausea or vomiting that occurred between 24 h and 6–7 days after the first day of anticancer treatment.20 Eligible patients received two antiemetics, namely palonosetron or older 5-HT3RAs (azasetron, ramosetron, or granisetron) and DEX, both of which were administered within 1 h before the scheduled CBDCA-based chemotherapy (CBDCA + pemetrexed [PEM]/CBDCA + paclitaxel [PTX]).18,19 Aprepitant was an optional third antiemetic. The study designs are summarized in Figure 1. Drinking habits are defined as drinking at least several times per week and the history of motion sickness was confirmed either in the medical record or by interviewing individual patients.
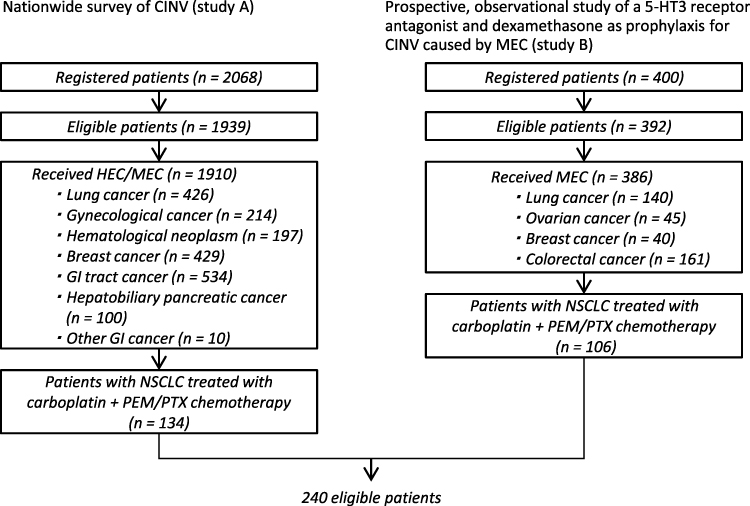 |
Figure 1 Patient selection diagram. Pooled data from 240 patients with non-small cell lung cancer (NSCLC) who received carboplatin (CBDCA)-based chemotherapy regimens (CBDCA + pemetrexed [PEM]/CBDCA + paclitaxel [PTX]) were selected among 2468 patients from two prospective observational studies. Abbreviations: CINV, chemotherapy-induced nausea and vomiting; HEC, highly emetogenic chemotherapy; MEC, moderately emetogenic chemotherapy; GI, gastrointestinal; PEM, pemetrexed; PTX, paclitaxel. |
Statistical Analysis
Patient demographics and the incidence of delayed nausea and vomiting were summarized using descriptive statistics or contingency tables and compared using Student’s t-test or the chi-squared test. We used an inverse probability treatment-weighted (IPTW) model derived from a logistic regression model to balance observable characteristics among the administered antiemetics.21,22 Independent risk factors for delayed nausea and vomiting were also evaluated using logistic regression analysis with a backward elimination method. The observed incidence of efficacy outcomes was compared between the two-antiemetic and three-antiemetic groups using the chi-squared test. p < 0.05 (two-sided) was considered significant. All statistical analyses were performed using SAS 9.4 (SAS Institute, Cary, NC, USA).
Results
Patient Characteristics
We included 240 patients with NSCLC in this analysis (nationwide survey of CINV: n = 134 [55.8%], prospective, observational study: n = 106 [44.2%]; two antiemetics: n = 186, three antiemetics: n = 54). Baseline characteristics, including age, sex, drinking habits, the incidence of motion sickness, the CBDCA-based regimen used, and the number of antiemetics, are presented in Table 1. Table 2 lists the unweighted and weighted patient characteristics stratified by the number of antiemetics.
 |
Table 1 Patients’ Baseline Characteristics |
 |
Table 2 Unweighted and Weighted Baseline Characteristics of Patients with NSCLC Treated with CBDCA Categorized by the Number of Antiemetic Regimens |
The percentages of female patients (unweighted) were 25.3% in the two-antiemetic group and 37.0% in the three-antiemetic group. There were also more patients with drinking habits (p = 0.0025) and more patients who received CBDCA + PTX (p = 0.0027) in the two-antiemetic group than in the three-antiemetic group.
The propensity scores were adequately balanced between the groups after IPTW adjustment, with no differences in age (p = 0.4193), sex (p = 0.1854), drinking habits (p = 0.8909), the incidence of motion sickness (p = 0.7205), and the CBDCA-based regimen used (p = 0.8531) between the groups.
Control of Delayed CINV
The incidence of CINV after IPTW adjustment is presented in Figure 2. Although the whole cohort had a high incidence of delayed nausea (45.4%), the rate was significantly lower in the three-antiemetic group (31.6%) than in the two-antiemetic group (47.3%, p = 0.0019). The overall incidence of delayed vomiting was low (20.4%), but it was significantly lower in the three-antiemetic group (5.1% vs 23.1%; p < 0.0001).
 |
Figure 2 Incidence of delayed nausea and vomiting. The incidence of delayed nausea and vomiting was significantly higher in the two-antiemetic group than that in the three-antiemetic group. |
Risk Factors for Delayed CINV
Univariate and multivariate logistic regression analyses were performed using age, sex, motion sickness, drinking habits, CBDCA-based regimens, and antiemetic regimens as risk factors for delayed CINV (Table 3).
 |
Table 3 Risk Factors for Delayed Nausea and Delayed Vomiting |
As presented in Table 3, the risk factors for delayed nausea included younger age (<70 years, odds ratio [OR] = 2.233; p = 0.0013), motion sickness (OR = 3.472; p = 0.0073), drinking habits (OR = 1.972; p = 0.0065), receipt of the CBDCA + PEM regimen (OR = 2.041; p = 0.0034), and the use of two antiemetics (OR = 1.926; p = 0.0045), whereas female sex (OR = 3.372; p = 0.0010), drinking habits (OR = 2.272; p = 0.0272), receipt of the CBDCA + PEM regimen (OR = 2.314; p = 0.0209), and the use of two antiemetics (OR = 6.830; p < 0.0001) were risk factors for delayed vomiting.
Logistic regression analysis illustrated that drinking habits, receipt of the CBDCA + PEM regimen, and the use of two antiemetics were common risk factors for delayed CINV.
Discussion
The current analysis confirmed that a three-antiemetic combination is the optimal treatment for patients with NSCLC treated with CBDCA-based chemotherapy to alleviate delayed vomiting. In addition, some risk factors for CINV during CBDCA-based chemotherapy were identified. Younger age, motion sickness, drinking habits, receipt of the CBDCA + PEM regimen, and the use of two antiemetics were risk factors for delayed nausea, and female sex, drinking habits, receipt of the CBDCA + PEM regimen, and the use of two antiemetics were risk factors for delayed vomiting. Drinking habits, receipt of the CBDCA + PEM regimen, and the use of two antiemetics were independent risk factors for delayed CINV in logistic regression analysis. These results might facilitate the personalization of antiemetic treatment for patients with NSCLC treated with CBDCA-based chemotherapy.
A three-drug combination of a 5-HT3RA, an NK1RA, and DEX has been recently recommended for antiemetic treatment during CBDCA-based chemotherapy. However, the evidence supporting the use of a three-antiemetic combination in patients with NSCLC treated with CBDCA-based chemotherapy is not sufficient.12–17 In the current study, which was performed before the current recommendation was issued, the incidence of both delayed nausea and vomiting after IPTW adjustment was significantly lower in the three-antiemetic group than in the two-antiemetic group. These results support the current recommendation, and a three-antiemetic combination might be the optimal supportive treatment for patients with NSCLC treated with CBDCA-based chemotherapy.
Identifying risk factors for CINV is important to improve the quality of life of patients with NSCLC and ensure the continuity of chemotherapy. Common risk factors for CINV include female sex, a history of motion sickness, and younger age.17–19,23,24 However, a few reports identified receipt of the CBDCA + PEM regimen as an independent risk factor for delayed nausea compared with other CBDCA-based regimens. In the current study, logistic regression analysis identified receiving the CBDCA + PEM regimen as an independent risk factor for delayed CINV, along with the aforementioned well-known patient-related risk factors. Hayashi et al previously reported that patients receiving PEM had a significantly higher rate of CINV than those receiving taxanes,24 and the CBDCA + PEM regimen was associated with a higher risk of delayed nausea than the CBDCA + PTX regimen.25 Therefore, because antiemetics have limited efficacy, even when using a three-drug combination, the optimal antiemetic regimen must be determined carefully for each patient treated with the CBDCA + PEM regimen, especially for female patients, younger patients, or patients with drinking habits or histories of motion sickness.
A Phase III trial revealed the efficacy and safety of olanzapine plus a three-antiemetic combination in patients who received highly emetogenic chemotherapy regimens including anthracycline/cyclophosphamide and cisplatin.26 Recently, a phase III trial (J FORCE) demonstrated that the addition of olanzapine to DEX, an NK1RA, and palonosetron improved CINV control in patients receiving cisplatin-based highly emetogenic chemotherapy.27 Furthermore, it was reported that adding olanzapine to antiemetic therapy with aprepitant, a 5-HT3RA, and DEX improved CINV control in patients receiving CBDCA-based chemotherapy.28 These results suggest that the addition of olanzapine to standard triplet antiemetic therapy is a promising option to improve the control of delayed nausea in patients at high risk of CINV who receive CBDCA + PEM. Concerning DEX, a phase III study reported at ESMO202129 aimed to clarify the non-inferiority of DEX on day 1 to DEX on days 1–4 when combined with an NK1RA, palonosetron, and olanzapine in patients receiving cisplatin-based highly emetogenic chemotherapy. In that trial, the primary endpoint of the complete response rate in the delayed phase was statistically met, and DEX on day 1 was non-inferior to DEX on days 1–4. However, patients who received DEX on day 1 had a significantly higher incidence of nausea and appetite loss. Therefore, it might be better to evaluate the optimal period for DEX administration among patients at high risk of CINV who are treated with CBDCA + PEM in prospective studies.
The present study had some limitations. For example, its design was neither randomized nor blinded. Therefore, these findings should be interpreted within the limitations of the observational study design. Furthermore, the possibility of selection bias between patients treated with two or three antiemetics cannot be dismissed. Further research is needed to verify these results. Despite these limitations, the findings described the risk factors for CBDCA-based regimens in clinical practice.
Conclusion
In the current study, a three-antiemetic combination was associated with a lower risk of CINV than a two-antiemetic combination specifically in patients with NSCLC treated with CBDCA-based chemotherapy, and drinking habits, receipt of the CBDCA + PEM regimen, and the use of two antiemetics were independent risk factors for delayed CINV, which corresponded to the current antiemetic guidelines and previous studies,30,31 and the result of the current study demonstrated important findings in support of those guidelines. The optimal antiemetic therapy for each CBDCA-based chemotherapy regimen should be carefully selected because CINV is not sufficiently controlled in some patients at high risk of CINV. Female patients, younger patients, and patients receiving CBDCA + PEM have a high risk of CINV. Therefore, we recommended that additional antiemetics for delayed CINV (eg, olanzapine) be considered for these patients.
Abbreviations
CINV, chemotherapy-induced nausea and vomiting; NSCLC, non-small cell lung cancer; CBDCA, carboplatin; NK1RAs, neurokinin 1 receptor antagonists; 5-HT3RAs, 5-hydroxytryptamine-3 receptor antagonists; AUC, area under the concentration–time curve; DEX, dexamethasone; PEM, pemetrexed; PTX, paclitaxel; IPTW, inverse probability treatment-weighted; OR, odds ratio; CI, confidence interval.
Data Sharing Statement
The data that support the findings of this study are available from two prospective observational studies, but restrictions apply to the availability of these data, which were used under license for the current study. Therefore, the data are not publicly available. However, data are available from the authors upon reasonable request and with permission of all study groups.
Acknowledgments
We are grateful to Kazuo Tamura, Keisuke Aiba, and Toshiaki Saeki for their helpful advice. We thank Joe Barber Jr., PhD, from Edanz for editing a draft of this manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2021. CA Cancer J Clin. 2021;71(1):7–33. doi:10.3322/caac.21654
2. Hirsch FR, Scagliotti GV, Mulshine JL, et al. Lung cancer: current therapies and new targeted treatments. Lancet Lond Engl. 2017;389(10066):299–311. doi:10.1016/S0140-6736(16)30958-8
3. Grant MJ, Herbst RS, Goldberg SB. Selecting the optimal immunotherapy regimen in driver-negative metastatic NSCLC. Nat Rev Clin Oncol. 2021;18(10):625–644. doi:10.1038/s41571-021-00520-1
4. Berger MJ, Ettinger DS, Aston J, et al. NCCN guidelines insights: antiemesis, version 2.2017. J Natl Compr Cancer Netw. 2017;15(7):883–893. doi:10.6004/jnccn.2017.0117
5. Hesketh PJ, Kris MG, Basch E, et al. Antiemetics: American Society of Clinical Oncology Clinical Practice Guideline Update. J Clin Oncol. 2017;35(28):3240–3261. doi:10.1200/JCO.2017.74.4789
6. Roila F, Warr D, Hesketh PJ, et al. 2016 updated MASCC/ESMO consensus recommendations: prevention of nausea and vomiting following moderately emetogenic chemotherapy. Support Care Cancer. 2017;25(1):289–294. doi:10.1007/s00520-016-3365-1
7. Aogi K, Takeuchi H, Saeki T, et al. Optimizing antiemetic treatment for chemotherapy-induced nausea and vomiting in Japan: update summary of the 2015 Japan Society of Clinical Oncology Clinical Practice Guidelines for Antiemesis. Int J Clin Oncol. 2021;26(1):1–17. doi:10.1007/s10147-020-01818-3
8. Rajeswaran A, Trojan A, Burnand B, Giannelli M. Efficacy and side effects of cisplatin- and carboplatin-based doublet chemotherapeutic regimens versus non-platinum-based doublet chemotherapeutic regimens as first line treatment of metastatic non-small cell lung carcinoma: a systematic review of randomized controlled trials. Lung Cancer Amst Neth. 2008;59(1):1–11. doi:10.1016/j.lungcan.2007.07.012
9. Rossi A, Chiodini P, Sun JM, et al. Six versus fewer planned cycles of first-line platinum-based chemotherapy for non-small-cell lung cancer: a systematic review and meta-analysis of individual patient data. Lancet Oncol. 2014;15(11):1254–1262. doi:10.1016/S1470-2045(14)70402-4
10. DeRemer DL, Clemmons AB, Orr J, Clark SM, Gandhi AS. Emerging role of olanzapine for prevention and treatment of chemotherapy-induced nausea and vomiting. Pharmacotherapy. 2016;36(2):218–229. doi:10.1002/phar.1703
11. Reck M, Rodríguez-Abreu D, Robinson AG, et al. Pembrolizumab versus chemotherapy for PD-L1-positive non-small-cell lung cancer. N Engl J Med. 2016;375(19):1823–1833. doi:10.1056/NEJMoa1606774
12. Hesketh PJ, Schnadig ID, Schwartzberg LS, et al. Efficacy of the neurokinin-1 receptor antagonist rolapitant in preventing nausea and vomiting in patients receiving carboplatin-based chemotherapy. Cancer. 2016;122(15):2418–2425. doi:10.1002/cncr.30054
13. Weinstein C, Jordan K, Green SA, et al. Evaluation of factors contributing to the response to fosaprepitant in a heterogeneous, moderately emetogenic chemotherapy population: an exploratory analysis of a randomized phase III trial. Support Care Cancer. 2018;26(11):3773–3780. doi:10.1007/s00520-018-4242-x
14. Ito Y, Karayama M, Inui N, et al. Aprepitant in patients with advanced non-small-cell lung cancer receiving carboplatin-based chemotherapy. Lung Cancer Amst Neth. 2014;84(3):259–264. doi:10.1016/j.lungcan.2014.03.017
15. Kusagaya H, Inui N, Karayama M, et al. Evaluation of palonosetron and dexamethasone with or without aprepitant to prevent carboplatin-induced nausea and vomiting in patients with advanced non-small-cell lung cancer. Lung Cancer Amst Neth. 2015;90(3):410–416. doi:10.1016/j.lungcan.2015.11.009
16. Tanioka M, Kitao A, Matsumoto K, et al. A randomised, placebo-controlled, double-blind study of aprepitant in nondrinking women younger than 70 years receiving moderately emetogenic chemotherapy. Br J Cancer. 2013;109(4):859–865. doi:10.1038/bjc.2013.400
17. Yahata H, Kobayashi H, Sonoda K, et al. Efficacy of aprepitant for the prevention of chemotherapy-induced nausea and vomiting with a moderately emetogenic chemotherapy regimen: a multicenter, placebo-controlled, double-blind, randomized study in patients with gynecologic cancer receiving paclitaxel and carboplatin. Int J Clin Oncol. 2016;21(3):491–497. doi:10.1007/s10147-015-0928-y
18. Tsuji Y, Baba H, Takeda K, et al. Chemotherapy-induced nausea and vomiting (CINV) in 190 colorectal cancer patients: a prospective registration study by the CINV study group of Japan. Expert Opin Pharmacother. 2017;18(8):753–758. doi:10.1080/14656566.2017.1317746
19. Matsui R, Suzuki K, Takiguchi T, et al. 5-Hydroxytryptamine-3 receptor antagonist and dexamethasone as prophylaxis for chemotherapy-induced nausea and vomiting during moderately emetic chemotherapy for solid tumors: a multicenter, prospective, observational study. BMC Pharmacol Toxicol. 2020;21(1):72. doi:10.1186/s40360-020-00445-y
20. Shimokawa M, Hayashi T, Nishimura J, et al. Pooled analysis of combination antiemetic therapy for chemotherapy-induced nausea and vomiting in patients with colorectal cancer treated with oxaliplatin-based chemotherapy of moderate emetic risk. BMC Cancer. 2021;21(1):1111. doi:10.1186/s12885-021-08860-y
21. Xie J, Liu C. Adjusted Kaplan-Meier estimator and log-rank test with inverse probability of treatment weighting for survival data. Stat Med. 2005;24(20):3089–3110. doi:10.1002/sim.2174
22. Sugihara M. Survival analysis using inverse probability of treatment weighted methods based on the generalized propensity score. Pharm Stat. 2010;9(1):21–34. doi:10.1002/pst.365
23. Shimokawa M, Hayashi T, Kogawa T, et al. Evaluation of combination antiemetic therapy on CINV in patients with gynecologic cancer receiving TC chemotherapy. Anticancer Res. 2019;39(1):225–230. doi:10.21873/anticanres.13101
24. Hayashi T, Shimokawa M, Miyoshi T, et al. A prospective, observational, multicenter study on risk factors and prophylaxis for low emetic risk chemotherapy-induced nausea and vomiting. Support Care Cancer. 2017;25(9):2707–2714. doi:10.1007/s00520-017-3679-7
25. Hayashi T, Shimokawa M, Matsuo K, et al. Chemotherapy-induced nausea and vomiting (CINV) with carboplatin plus pemetrexed or carboplatin plus paclitaxel in patients with lung cancer: a propensity score-matched analysis. BMC Cancer. 2021;21(1):74. doi:10.1186/s12885-021-07802-y
26. Navari RM, Qin R, Ruddy KJ, et al. Olanzapine for the prevention of chemotherapy-induced nausea and vomiting. N Engl J Med. 2016;375(2):134–142. doi:10.1056/NEJMoa1515725
27. Hashimoto H, Abe M, Tokuyama O, et al. Olanzapine 5 mg plus standard antiemetic therapy for the prevention of chemotherapy-induced nausea and vomiting (J-FORCE): a multicentre, randomised, double-blind, placebo-controlled, Phase 3 trial. Lancet Oncol. 2020;21(2):242–249. doi:10.1016/S1470-2045(19)30678-3
28. Tanaka K, Inui N, Karayama M, et al. Olanzapine-containing antiemetic therapy for the prevention of carboplatin-induced nausea and vomiting. Cancer Chemother Pharmacol. 2019;84(1):147–153. doi:10.1007/s00280-019-03868-5
29. Shimomura K, Minatogawa H, Mashiko T, et al. LBA63 Placebo-controlled, double-blinded phase III study comparing dexamethasone on day 1 with dexamethasone on days 1 to 4, with combined neurokinin-1 receptor antagonist, palonosetron, and olanzapine in patients receiving cisplatin-containing highly emetogenic chemotherapy: SPARED trial. Ann Oncol. 2021;32:S1339–S1340. doi:10.1016/j.annonc.2021.08.2144
30. Razvi Y, Chan S, McFarlane T, et al. ASCO, NCCN, MASCC/ESMO: a comparison of antiemetic guidelines for the treatment of chemotherapy-induced nausea and vomiting in adult patients. Support Care Cancer. 2019;27(1):87–95. doi:10.1007/s00520-018-4464-y
31. Giuliani J, Bonetti A. Cost-effectiveness of newer regimens for the prophylaxis of chemotherapy-induced nausea and vomiting: review of the literature and real-world data. Curr Opin Oncol. 2020;32(4):269–273. doi:10.1097/CCO.0000000000000634
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Gastroparesis: Myths, Misconceptions, and Management
Cangemi DJ, Lacy BE
Clinical and Experimental Gastroenterology 2023, 16:65-78
Published Date: 6 June 2023
Medicinal Plants for Chemotherapy-Induced Nausea and Vomiting: A Systematic Review of Antiemetic, Chemosensitizing, and Immunomodulatory Mechanisms
Sun X, Nie F, Sun J, Zhang J, Wang Y
Therapeutics and Clinical Risk Management 2025, 21:1187-1218
Published Date: 31 July 2025
Promethazine Combined with Metoclopramide for the Prevention of Postoperative Nausea and Vomiting in Patients Undergoing Laparoscopic Colorectal Cancer Surgery: A Randomized Controlled Trial
Liu R, Bi R, Zhang J, Li X, Tian B, Yan W
Drug Design, Development and Therapy 2025, 19:9029-9039
Published Date: 4 October 2025