Back to Journals » Advances in Medical Education and Practice » Volume 17
Medical Students’ Perspectives on Inclusivity Within Clinical Environments: A Pilot Study
Authors Haque E ![]() , Lavin JM, Farrington R
, Lavin JM, Farrington R
Received 27 May 2025
Accepted for publication 14 December 2025
Published 23 January 2026 Volume 2026:17 543053
DOI https://doi.org/10.2147/AMEP.S543053
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Enam Haque,1 Jacqueline M Lavin,2 Rebecca Farrington3
1School of Medical Sciences, University of Manchester, Manchester, UK; 2Northern Care Alliance Foundation Trust, Salford, NHS, UK; 3Edge Hill Medical School, Edge Hill University, Ormskirk, UK
Correspondence: Enam Haque, School of Medical Sciences, University of Manchester, Manchester, UK, Email [email protected]
Purpose: Limited resources including staff, technology, and space in United Kingdom National Health Service (NHS) environments present challenges for working teaching and learning. Cumulative pressures impact mental health and prompt medical students to question career choices, leave the profession, or emigrate. There is little understanding of the experience of inclusivity in clinical environments for medical students. This pilot study explores students’ perspectives of these environments, the barriers to formulating change, and possible solutions.
Materials and Methods: Six diverse clinical medical students from the University of Manchester, based at a single NHS Trust, voluntarily participated in one of four recorded focus groups facilitated by a near-peer with protected characteristics. Low participation emphasised the importance of undertaking this pilot study to consider methods for future study design. Transcriptions were independently analysed by two reviewers to generate themes using NVivo.
Results: Key themes included positive experiences with resident doctors; negative interactions with patients; negative attitudes and poor role modelling from some staff; perceived lack of institutional support; and poor learning opportunities. Students suggested staff training and better support structures to improve learning environments.
Conclusion: This study highlights universal issues from the perspectives of minoritised students and emphasises their low participation in research. Authors suggest exploring clinical faculty support and training to improve learning environments, and innovations in study design for wider, more democratic and culturally sensitive participation.
Keywords: equality, diversity, inclusion, medical school, medical student, inclusivity, learning environment, student experience
Introduction
It can be challenging to learn, work, and teach in resource limited United Kingdom (UK) National Health Service (NHS) environments, with pressures on staffing, technology, and physical space. Cumulative pressures lead medical students to question career choices,1 doctors to leave the country or profession1,2 and contribute to a notable deterioration in medical students’ mental health.3
It is known that prioritising inclusivity within clinical environments can improve healthcare workers’ sense of belonging.4 However, little is known about this for medical students. Subsequent knowledge may encourage them to feel valued, to thrive, and to progress their careers and contributions to practice.
Protected characteristics, such as ethnicity and gender, influence the lived experience of students within learning environments. Differences in attainment were reported in a meta-analysis exploring ethnicity and academic performance.5 Ethnic minority students and doctors performed on average worse than white colleagues, despite both groups having high academic ability entering medical school.6 It was concluded that this was not due to learner deficit, neither situating the problem with the student or doctor, nor blaming their personal or social background.6 Brown et al7 conducted qualitative interviews with female medical students who described gender bias dissuading women from surgical careers, pregnancy as a barrier, and disapproval of caring for a baby during training. Students felt physical environments were male dominated with institutional gender bias.
Alongside protected characteristics, factors related to interpersonal learning environments influence student experience. Broad et al8 conducted a questionnaire study of lived experiences of medical students in learning environments. They found 63.3% of students faced harassment, with 43.2% experiencing stereotyping. Only 5% had formally reported incidents and comments suggested students did not think reporting would make a difference.
Social Identity Theory9 suggests that healthcare professionals interpret experiences through the lens of their group identity. Apperception reinforces this, meaning harassment may be underreported if speaking out threatens stigmatisation or risks exclusion from the professional group. Other responses to identity threat may include open or hidden resistance which, discouraged by traditional views of professional identity formation, is increasingly recognised as originating from reinforcement of norms and values that disproportionately reflect the perspectives and priorities of culturally dominant groups.10 Students improved knowledge of diverse student perspectives, cultural humility, and the importance of authenticity, may enable them to become agents of change, through speaking out.
Governing bodies and medical associations have produced guidelines, reports, and pledges to highlight the importance of tackling such challenges and increase professional awareness. The British Medical Association (BMA) Anti-Sexism Pledge sets standards for clinical learning environments.11 It includes ending sexual harassment in medicine, ensuring safe and known reporting processes for discrimination and harassment, nurturing a safe environment for pregnant students and doctors, and eliminating sexism from career progression. The Medical Schools Council (MSC) guidance, Active Inclusion: Challenging Exclusions, sets the Equality, Diversity, Inclusion (EDI) strategy for medical schools.12 It suggests making student events inclusive and implementing robust reporting processes for harassment. The General Medical Council (GMC) supplemental section on EDI in Selecting for Excellence13 advocates: “The learning environment is safe for patients and supportive for learners and educators. The culture is caring, compassionate and provides a good standard of care and experience for patients, carers, and families”. It endorses better support and role modelling; improving equality, diversity, and inclusion (EDI) training for staff; and implementing EDI activities in the curriculum. However, whilst under-reporting remains a challenge, it is finding ways to sustainably implement these guidelines that is central to tackling the issues.
Existing literature fails to report medical students’ perspectives on how their protected characteristics affect their learning experiences. It is not known how aware students are of the available support and resources, or how to raise concerns about difficulties in their learning environments.
This study was based in a single sector that included both primary and care settings. It aimed to describe the challenges arising for diverse medical students in clinical learning environments, as well as the support available to them. It also aimed to explore medical student suggestions for improvement, to inform strategies for engagement in clinical placements and ultimately motivate individuals to continue in practice.
Materials and Methods
Study Design
A small pilot study was chosen because of known difficulties enabling representation from diverse students in medical education feedback.14
The authors concentrated on depth and relevance of data rather than quantity, in anticipation of low participation. The research questions centred on:
What are the perceived experiences of medical students with protected characteristics within their clinical learning environments? What are their perceived challenges?
Focus groups were initially deemed best suited to gain rich descriptions from the perspectives of medical students, in an environment where students might feel supported by peers to disclose sensitive information. The focus group interviews were facilitated by the local EDI student representative for the sector, a medical student with intersectional protected characteristics who received training for this role. This near-peer approach aimed to foster a psychologically safe space, minimising hierarchy and power differentials. To avoid tokenism and in line with Fischer’s participatory governance theory,15 the research included the students’ suggested ideas for improvements.
Study Participants and Recruitment
The study was set in a northern UK medical school. Participants were recruited from approximately 450 students in years 3–5 of the medical programme through online adverts on the student portal, email, and social media. Those who expressed interest and met inclusion criteria were emailed further information, including the study background, how the data would be collected and analysed, and a consent form. Medical students included in the study had experienced clinical placements and belonged to at least one of the following protected characteristics: disability, gender reassignment, pregnant, ethnic minority, minority religious group, female, and LGBTQI. Participants self-identified and did not need to disclose their protected characteristic(s). Respondents signed consent forms and were allocated to focus groups depending on availability. All participants were advised of their right to withdraw and reassured that data would be anonymised. Six students participated in total, each attending one of four focus group interview sessions. Due to small numbers, demographic data was not collected to assuage fears around confidentiality and maintain anonymity.
Data Collection
The focus group topic guide was pre-determined by the research team who were experienced educators with an EDI focus. It used prompts and questions created in line with the aims of the study and existing literature. The focus group guide was semi-structured with flexibility for the order and prominence of questions to maintain the conversation flow and allow for new areas of exploration to be followed should they arise. Focus groups each lasted one hour and were securely conducted using the online Zoom platform over a 4-week period. The discussions were audio recorded and transcribed verbatim by a university approved transcription service. The text was anonymised and reviewed by two members of the research team. The recordings were deleted, and transcriptions stored in the university secure research data repository.
Data Analysis
Using NVivo software version 11, two researchers independently analysed data using Thematic Analysis methodology proposed by Braun and Clark.16 Researchers initially read the transcripts multiple times to understand the nuances of students’ experiences. Key features of initial codes reflected both positive and negative experiences, challenges, and solutions. Grouping these into broader themes highlighted supportive relationships, barriers to inclusion, institutional issues, and recommendations for change. These were checked against the data and then named before linking to the literature and producing the report.
Discrepancies between the two researchers’ coding were discussed to reach consensus. The final themes were reflected upon then discussed with the collective research team.
Ethics
The University of Manchester Proportionate Ethics Committee approved the study. [Approval date: 10.04.22, Review Reference: 2022–13,955-22918] Participants’ informed consent included publication of anonymised responses/direct quotes. This paper complies with the Declaration of Helsinki.
Results
The interviews explored the perceived experiences of medical students in clinical learning environments and found these were split into two broad categories. The first highlighted positive experiences with resident (formerly named “junior” doctors) particularly Clinical Educational Fellows (CEFs). The CEF position is a near peer role for early career doctors, that splits workload between teaching and clinical delivery, with responsibility to medical students, the undergraduate support team, fellow healthcare professionals, and patients. Table 1 provides a description of the perceived positive and negative experiences for students, with corresponding quotes. Students described positive experiences of being provided with good learning opportunities. Conversely, negative experiences were reported in interactions with patients.
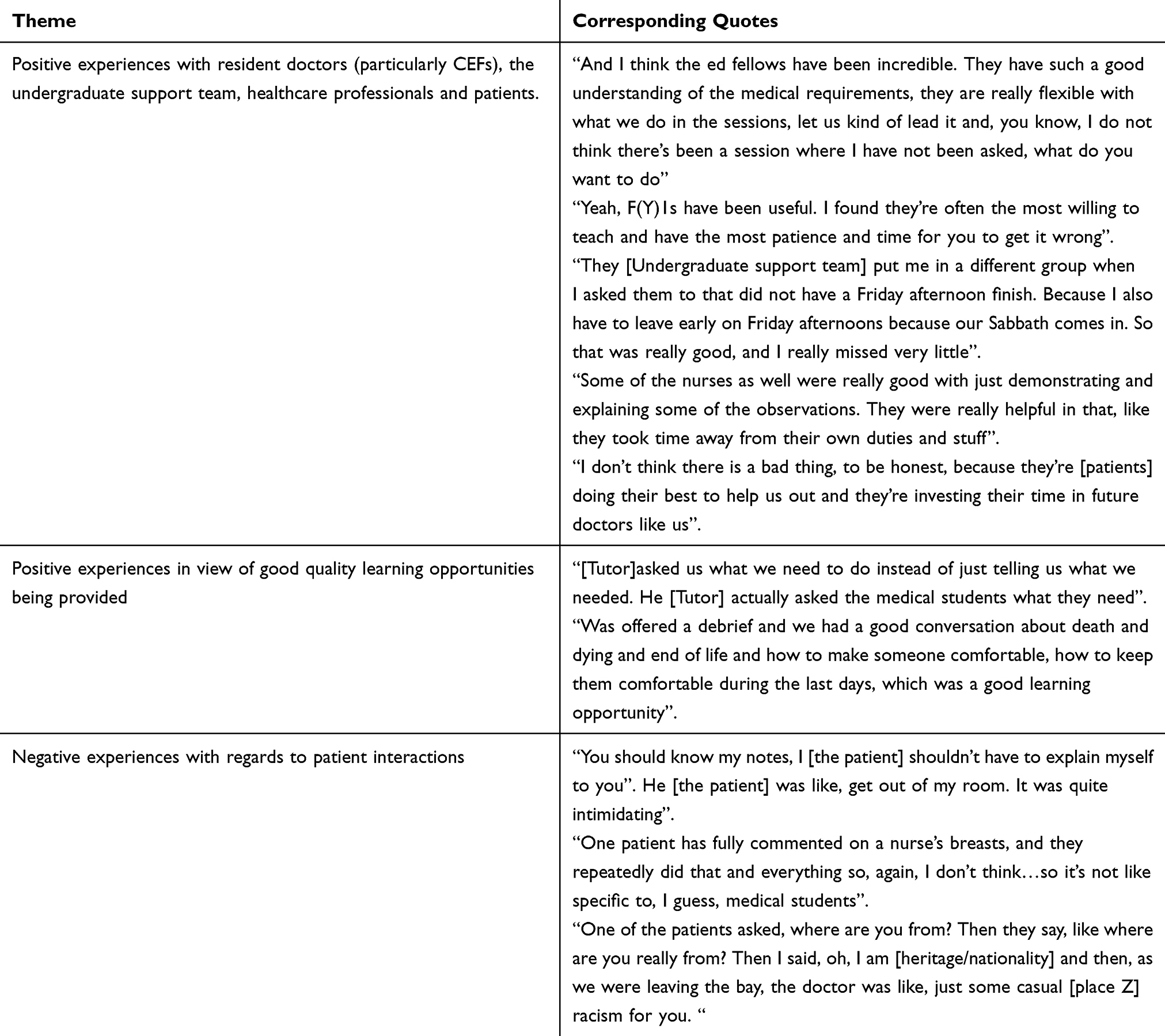 |
Table 1 Perceived Positive and Negative Experiences of Medical Students with Protected Characteristics in Clinical Learning Environments |
Table 2, provides a description of the perceived challenges faced by students, with corresponding quotes. Four challenges identified within the learning environments included perceived stigma and negative attitudes from staff, poor role models, lack of support from the institution and poor learning opportunities.
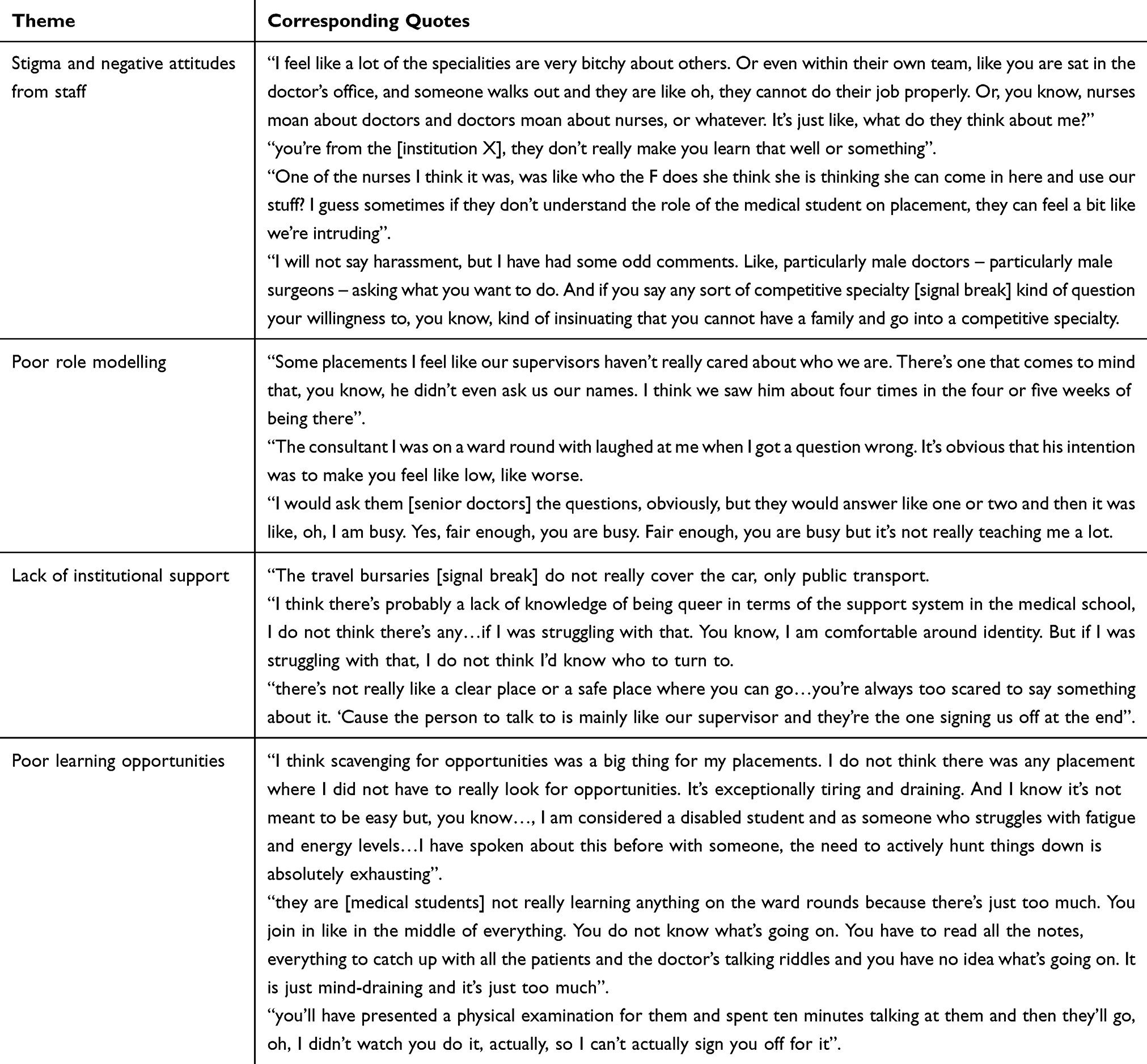 |
Table 2 Perceived Challenges of Medical Students with Protected Characteristics Within Their Clinical Learning Environments |
Table 3 provides a description of the students’ ideas for improvements. Suggested improvements from students included staff training, development of staff advocates for protected characteristics and having improved support structures.
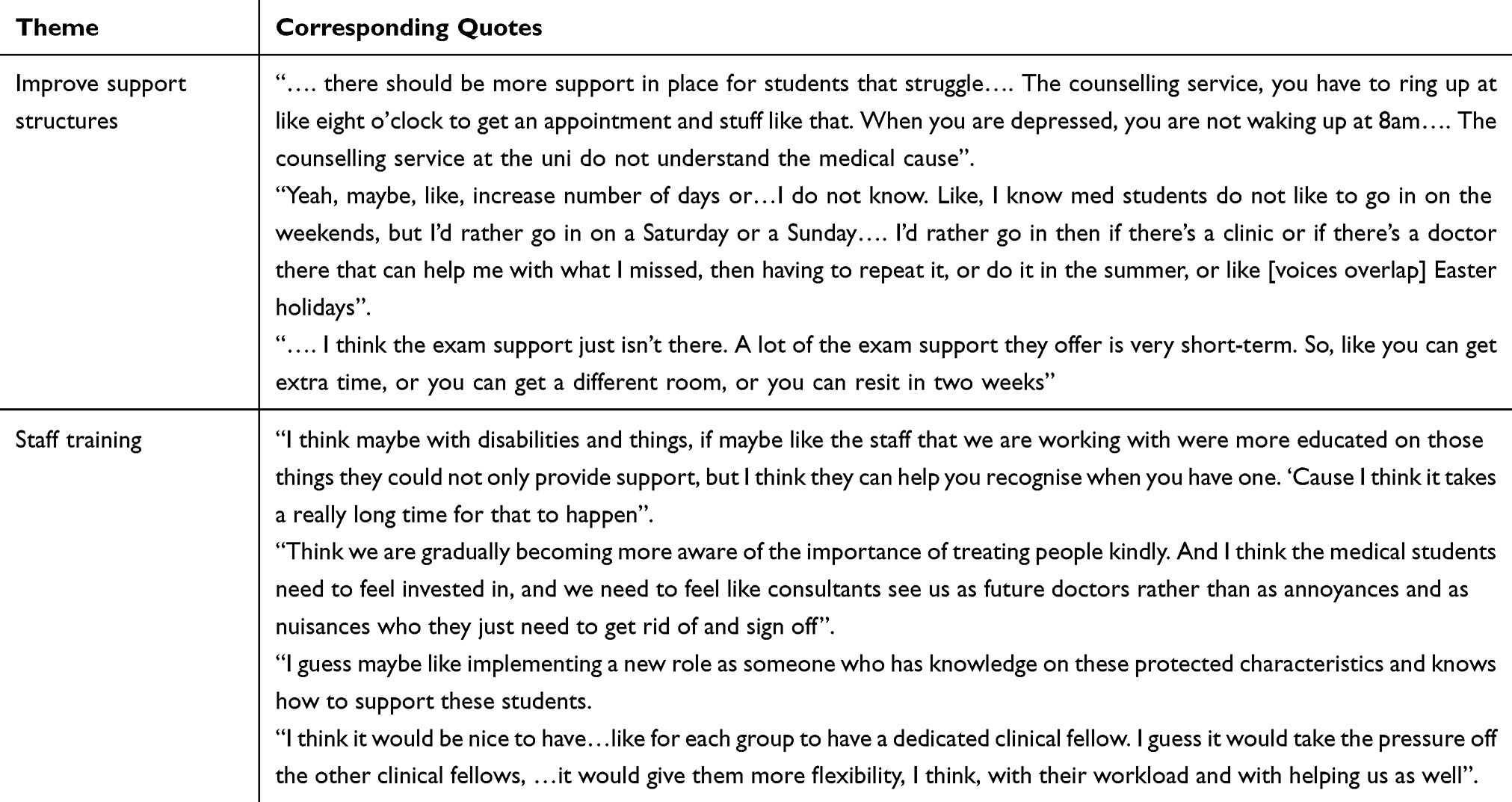 |
Table 3 Student Suggestions for Improvement |
Discussion
This study aimed to address two research questions: the perceived experiences of medical students with protected characteristics within their clinical learning environments and the challenges they faced. It also explored the students’ suggested ideas for improvement. It was interesting that a broad range of issues were identified, despite the small number of participants. Students expressed positive aspects of experiential learning on placement, the highlight being contact with Clinical Educational Fellows (CEFs) as near peers. This aligns with current literature. Hossain et al17 explored the impact of a structured teaching programme for final-year medical students led by Clinical Teaching Fellows (equivalent to CEFs in the study). Students commented positively on the teaching being reliable, relevant and varied, and the fellows being a familiar face during their placement. This suggests it would be worthwhile to consider a similar more structured intervention for this student body.
Students encountered many challenges, with some concerning experiences, such as bullying and discrimination. Worryingly, the students did not feel able to challenge such behaviours within the hierarchy and believed any attempt to do so would be futile. Some incidents had created cognitive dissonance for students, and they welcomed more opportunities to debrief their confusing experiences of interacting with staff and patients. Incidents of sexism were challenging within learning environments, which aligns with current literature. Ibrahim et al18 conducted a qualitative study of female medical students, to explore their experiences of sexism whilst in their clinical work. There was evidence of sexual harassment, stereotyping, and microaggressions, all of which negatively impacted students’ mental health and their participation on placement. They also felt multiple factors hindered reporting. Recent campaigns and reports in the literature and medical press highlight that these issues are not local to the study setting but need to be addressed at scale in medical education. Interventions may include the instigation of better staff training and user-friendly reporting systems or online platforms for anonymously raising concerns.
There was a widespread feeling among students that they were unwelcome and burdensome in the clinical environment; senior staff did not understand their needs; and the NHS working environment was not a happy one. This is in keeping with previous studies. Ravalier et al19 conducted a survey and semi-structured interviews with NHS staff, exploring work stress. These mixed methods elicited issues with workload and the work environment. Their data also unearthed that half of respondents felt poorly supported by their manager. It is worrying that students are entering potentially troubled clinical work environments, and it would be helpful to address this early in preparation for practice.
Stigma and negative attitudes were challenges within clinical learning environments, particularly around racism. This had an impact on students’ sense of belonging and on career hesitancy. Morrison et al20 explored racial microaggressions on graduate medical students. They found this to be a regular experience with negative impact on their wellbeing, experience, and performance. To counter this, students felt that role-modelling was particularly important.
Ward rounds were not considered valuable learning opportunities by students and could be stressful. This is supported by a systematic review, which noted the negative experience of ward rounds as learning opportunities for postgraduate trainees.21 In Gray et al,22 a structured framework and tool was deemed to have educational value for trainees and be acceptable to preceptors for adding educational opportunities during ward rounds. This approach may address the concerns felt by students, particularly if it is deliberately and intentionally inclusive in design.
As expected, students were stressed by summative assessments. Students with health problems wished longer term support around preparation for assessments and flexibility to manage workloads. de Oliveira et al23 explored the experience of medical students with disability. They noted multiple challenges, including educators’ poor awareness of disabilities, and lack of teaching adaptations and adjustments to the physical learning space. Students with disability suggested student collective advocacy to improve access, and for faculty to determine requirements of individual students with disability throughout their time in medical school.23
Placement signoffs caused anxiety and, paradoxically, distracted students from learning. They wanted more clarity on who was responsible for completion and on how to manage this. Al-Mously et al24 highlighted the lack of supervisor engagement in feedback, with over 50% of year 5 medical students reporting they rarely received feedback on their clinical performance. Burgess & Mellis25 emphasised the risk to medical students of lack of direct observation of clinical performance, including lack of achieving clinical competence and a feeling of being lost in the clinical environment.
Staff development was considered crucial by students to help teachers understand their learning and pastoral needs. They felt that staff training on induction requirements and Equality, Diversity, and Inclusion were important. Bilal et al26 conducted a meta-analysis and systematic review looking at staff development, noting that professional competence and knowledge significantly improved with different interventions. Students in the study also suggested improved IT access and stronger bespoke support structures. Weiss et al27 highlighted that 17.7% medical students in their study felt that staff did not respect protected characteristics, particularly those who were from ethnic minority, female, or LGBTQ backgrounds.
Strengths and Limitations
The qualitative data was rich, varied, and informative, despite the limited responses with a modest sample size. Whilst small numbers preclude working towards data saturation, we felt that information power was more important for this seldom-heard group.28 This topic is sensitive and gaining the nuanced viewpoints of even small numbers of students generated data and perspectives which are insightful and not well-described in existing literature. Self-selection by students meant hearing from those with more specific issues, but only those with the confidence to speak out. The pilot study was designed to address anxieties around confidentiality that students with protected characteristics and intersectional issues face in speaking out through using self-identification and not collecting demographic data. However, using this strategy, along with facilitation by a near peer with diverse characteristics to facilitate the focus groups, did not result in high participation. This shows the importance of such pilot studies and will result in further research to optimise future design, including mixed methods, individual interviews, reflective narratives, and arts-based research.
Suggestions for the Future
This study has highlighted the key issues facing diverse students in a clinical sector of a large medical school. The authors suggest piloting interventions to amplify the positive findings and minimise the challenging ones. Aiming to make systems more responsive and equitable through reasoned dialogue rather than rather than passive feedback could improve trust from minoritised groups.
An example would be to design, implement, and evaluate a structured supportive programme co-produced with near peer resident doctors or Clinical Educational Fellows (CEF). The authors have obtained institutional support and aim for the initiative to be led by a CEF. Staff development can improve the learning environment, particularly if EDI is incorporated into the training. The medical school has created a standardised EDI training package for clinical placement supervisors, and this could be delivered to all educators in the sector.
The authors suggest evaluation of these further interventions through a mixed methods approach, incorporating qualitative and quantitative data analysis. This pilot study illustrates that future study design to reach students from communities who lack trust in research is about more than power differentials. Campbell et al29 quip “do not think that skin gets you in” and go on to describe their experiences as scholars of colour where building respectful relationships and foregrounding cultural sensitivities to improve access requires much more consideration and reflexivity.
Conclusion
This study aimed to explore how inclusive the clinical learning environment was for medical students with protected characteristics. It elicited challenges that were universal, such as bullying and discrimination, navigating unhappy environments, and feeling devalued. Positive experiences were linked to contact with Clinical Education Fellows, and students were keen for their greater involvement in undergraduate education. A key intervention stressed by students was improved staff training, particularly around EDI. The authors aim to implement change by highlighting the issues facing medical students and through being transparent about deficits. They propose development of interventions to address the barriers facing students from protected characteristics and more nuanced evaluation of their impact and effectiveness.
Acknowledgments
The authors would like to thank Dr Imelda Vitenu for her excellent work as a medical student interviewer, facilitating all the focus groups for the study. They would also like to thank the Northern Care Alliance undergraduate education manager, Kate Fowles, for her support in advertising the study for recruitment of participants. Also, Dr Sai Ram, Teaching Fellow at the NCA, for her support and review of the article draft.
Funding
Funding was obtained from the Office for Students Access and Participation Plan, to pay for transcription costs with an approved transcription service.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ferreira T, Collins AM, Feng O, et al. Career intentions of medical students in the UK: a national, cross-sectional study (AIMS study). BMJ Open. 2023;13(9):e075598. doi:10.1136/bmjopen-2023-075598
2. Brennan N, Langdon N, Bryce M, et al. Drivers of international migration of doctors to and from the United Kingdom. General Medical Council; 2021. Available from: https://www.gmc-uk.org/about/what-we-do-and-why/data-and-research/research-and-insight-archive/drivers-of-international-migration-of-doctors-to-and-from-the-united-kingdom.
3. British Medical Association. Medical student mental health and wellbeing survey report. 2024. Available from: https://www.bma.org.uk/media/7125/bma-medical-student-mental-health-survey-report-march-2024.pdf.
4. Woods A, Zajac SA, Middleton ED, et al. Doing the work: the role of inclusive leadership in promoting psychological safety and openness to diversity through diversity, equity, and inclusion practices. Psychol Leaders Leadership. 2024;27(1):115–9. doi:10.1037/mgr0000158
5. Woolf K, W.w PH, McManus IC. Ethnicity and academic performance in UK trained doctors and medical students: systematic review and meta-analysis. BMJ. 2011;342:d901. doi:10.1136/bmj.d901
6. Woolf K. Editorials: differential attainment in medical education and training. BMJ. 2020;368:m339. doi:10.1136/bmj.m339
7. Brown MEL, Hunt GEG, Hughes F, et al. Too male, too pale, too stale’: a qualitative exploration of student experiences of gender bias within medical education. BMJ Open. 2020;10:e039092. doi:10.1136/bmjopen-2020-039092
8. Broad J, Matheson M, Verrall F, et al. Discrimination, harassment, and non-reporting in UK medical education. Med Educ. 2018;52:414–426. doi:10.1111/medu.13529
9. Tajfel H, Turner JC. The social identity theory of intergroup behavior. In: Worchel S, Austin WG, editors. Psychology of Intergroup Relations.
10. Sternszus R, Steinert Y, Razack S, et al. Being, becoming, and belonging: reconceptualizing professional identity formation in medicine. Front Med. 2024;11:1438082. doi:10.3389/fmed.2024.1438082
11. BMA Pledge on ending Sexism in Medicine. 2023. Available from: https://www.bma.org.uk/media/6823/joint-pledge-on-ending-sexism-in-medicine.pdf.
12. Medical Schools Council. Active Inclusion. Challenging Exclusions in Medical Education. 2021. Available from: https://www.medschools.ac.uk/media/2918/active-inclusion-challenging-exclusions-in-medical-education.pdf.
13. General Medical Council. Promoting Excellence- Equality & Diversity Considerations. 2017. Available from: https://www.gmc-uk.org/-/media/documents/promoting-excellence-equality-and-diversity-considerations_pdf-72709944.pdf.
14. Sethi I, Dine CJ. Exploring the landscape of student representation in medical curriculum development across U.S. MD schools: a comparative analysis. BMC Med Educ. 2025;25:747. doi:10.1186/s12909-025-07114-w
15. Fischer F. Participatory governance: from theory to practice. In: Levi-Faur D editor. The Oxford Handbook of Governance. Oxford University Press; 2012:457–471. doi:10.1093/oxfordhb/9780199560530.013.0032.
16. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
17. Hossain S, Shah S, Scott J, et al. Reinventing undergraduate clinical placements with a switch to delivery by clinical teaching fellows. Adv Med Educ Pract. 2021;12:1429–1438. PMID: 34924780; PMCID: PMC8674148. doi:10.2147/AMEP.S336912
18. Ibrahim D, Riley R. Female medical students’ experiences of sexism during clinical placements: a qualitative study. Healthcare. 2023;(7):1002. doi:10.3390/healthcare11071002
19. Ravalier JM, McVicar A, Boichat C. Work stress in NHS employees: a mixed-methods study. Int J Environ Res Public Health. 2020;17(18):6464. doi:10.3390/ijerph17186464
20. Morrison N, Zaman T, Webster G, et al. Where are you really from?’: a qualitative study of racial microaggressions and the impact on medical students in the UK. BMJ Open. 2023;13:e069009. doi:10.1136/bmjopen-2022-069009
21. Khalaf Z, Khan S. Education during ward rounds: systematic review. Interact J Med Res. 2022;11(2):e40580. PMID: 36285742; PMCID: PMC9685505. doi:10.2196/40580
22. Gray AZ, Modak M, Connell T, Enright H. Structuring ward rounds to enhance education. Clin Teacher. 2020;17(3):286–291. PMID: 31452336. doi:10.1111/tct.13086
23. de Oliveira E, Dantas RG, Amaral GA, Barreto Giaxa RR, de Góis AFT. Experiences of disabled students in undergraduate medical education. Med Teach. 2021;44(3):294–299. doi:10.1080/0142159X.2021.1985098
24. Al-Mously N, Nabil NM, Al-Babtain SA, Fouad Abbas MA. Undergraduate medical students’ perceptions on the quality of feedback received during clinical rotations. Med Teach. 2014;36(sup1):S17–S23. doi:10.3109/0142159X.2014.886009
25. Burgess A, Mellis C. Feedback and assessment for clinical placements: achieving the right balance. Adv Med Educ Prac. 2015;6:373–381. doi:10.2147/AMEP.S77890
26. Bilal, Guraya SY, Chen, S. The impact and effectiveness of faculty development program in fostering the faculty’s knowledge, skills, and professional competence: a systematic review and meta-analysis. Saudi J Biol Sci. 2019;26(4).
27. Weiss J, Balasuriya L, Cramer LD, et al. Medical students’ demographic characteristics and their perceptions of faculty role modeling of respect for diversity. JAMA Network Open. 2021;4(6):e2112795. doi:10.1001/jamanetworkopen.12795
28. Malterud K, Siersma VD, Guassora AD. Sample size in qualitative interview studies: guided by information power. Qual Health Res. 2016;26(13):1753–1760. doi:10.1177/1049732315617444
29. Campbell RD, Dennis MK, Lopez K, Matthew R, Choi YJ. Qualitative research in communities of color: challenges, strategies, and lessons. J Soc Work Res. 2021;12(1):177–200. doi:10.1086/712234
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Medical Professionalism in the Provision of Clinical Care in Healthcare Organizations
Bhardwaj A
Journal of Healthcare Leadership 2022, 14:183-189
Published Date: 26 October 2022
Peer Teaching in Undergraduate Medical Education: What are the Learning Outputs for the Student-Teachers? A Systematic Review
Tanveer MA, Mildestvedt T, Skjærseth IG, Arntzen HH, Kenne E, Bonnevier A, Stenfors T, Kvernenes M
Advances in Medical Education and Practice 2023, 14:723-739
Published Date: 11 July 2023
Reporting of Demographics & Subgroup Analyses in Premarketing Studies of FDA Approved High-Risk Cardiovascular Devices, 2014–2022
Swanson MJ, Uyeki CL, Yoder SR, Dhruva SS, Miller JE, Ross JS
Medical Devices: Evidence and Research 2024, 17:165-172
Published Date: 29 April 2024
Reporting of Race and Ethnicity in SLE Studies in High-Impact Rheumatology Journals
Eroglu I, Suter LG, Baker H
Open Access Rheumatology: Research and Reviews 2026, 18:526618
Published Date: 25 April 2026