Back to Journals » Psychology Research and Behavior Management » Volume 19
Measuring Cognitive Flexibility in Chinese Individuals with Obsessive-Compulsive Disorder: Psychometric Validation and Factor Structure of the Chinese Version of the Flexibility in Daily Life Scale
Authors Yan Z ![]() , Chen T, Ma X, Mi S, Wang P
, Chen T, Ma X, Mi S, Wang P ![]() , Li Z
, Li Z
Received 14 February 2026
Accepted for publication 21 May 2026
Published 20 June 2026 Volume 2026:19 598045
DOI https://doi.org/10.2147/PRBM.S598045
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 7
Editor who approved publication: Prof. Dr. Bao-Liang Zhong
Zijun Yan,1,2 Tao Chen,3,4 Xu Ma,1,2 Si Mi,1,2 Pengchong Wang,1,2 Zhanjiang Li1,2
1Beijing Key Laboratory of Mental Disorders, National Clinical Research Center for Mental Disorders & National Center for Mental Disorders, Beijing Anding Hospital, Capital Medical University, Beijing, People’s Republic of China; 2Advanced Innovation Center for Human Brain Protection, Capital Medical University, Beijing, People’s Republic of China; 3Brain and Mind Centre, The University of Sydney, Sydney, Australia; 4School of Psychology, The University of Sydney, Sydney, Australia
Correspondence: Pengchong Wang, Email [email protected] Zhanjiang Li, Email [email protected]
Purpose: Impaired cognitive flexibility is a core feature of obsessive-compulsive disorder (OCD) and may contribute to symptom persistence and variabe therapeutic outcomes. However, traditional measures may adequately capture how cognitive flexibility manifests in daily life. The Flexibility in Daily Life scale (FIDL) is a novel developed self-report instrument assessing multidimensional facets of cognitive flexibility. The present study sought to determine the psychometric structure of the Chinese version of the FIDL and its suitability for individuals within an OCD population.
Patients and Methods: The 37-item FIDL underwent forward-back translation and cross-cultural adaptation. The baseline comprised 157 participants (76 individuals with OCD and 81 healthy controls), with an OCD subsample(N=54) completing a one-month retest. Confirmatory factor analysis (CFA) initially evaluated the established 21-item five-factor model in the full sample. Alternative structures (one-, two-, and correlated three-factor models) were also examined. Given suboptimal model fit indices, exploratory factor analysis (EFA) was subsequently performed in the OCD sample (N=76) to derive a structure more representative of clinical characteristics. Finally, Bayesian exploratory factor analysis (BEFA) was applied to ascertain factor stability.
Results: The established 21-item five-factor model demonstrated suboptimal fit in the Chinese OCD sample (N=157; CFI=0.791, TLI=0.822, RMSEA=0.087, SRMR=0.082). EFA identified a revised 25-item three-factor structure, labeled Contextual Adaptability, Cognitive-Behavioral Rigidity, and Routine/Control, which was corroborated by BEFA. The revised scale exhibited satisfactory internal consistency (Cronbach’s α=0.699– 0.838; McDonald’s ω=0.721– 0.846) and acceptable test-retest reliability (r=0.777– 0.844). The three-factor model failed to demonstrate adequate fit (χ2/df = 2.095, CFI = 0.708, TLI = 0.678, RMSEA = 0.121, SRMR = 0.146), and BEFA further revealed excessive inter-factor overlap, with correlations ranging from 0.969 to 0.987.
Conclusion: The findings provide preliminary evidence that the Chinese FIDL may capture clinically relevant aspects of daily-life cognitive flexibility in OCD populations. The revised three-factor structure offers a potential framework for assessing specific inflexibility profiles and identifying potential intervention targets, including contextual adjustment difficulties, rigid cognitive-behavioral responding, and over-reliance on routine/control. These findings underscore the importance of considering clinical and cultural context when evaluating cognitive flexibility constructs. However, given the exploratory design, limited sample size, and excessive inter-factor overlap, further validation in larger, independent cohorts is warranted.
Keywords: cognitive flexibility, obsessive-compulsive disorder, psychometrics, factor analysis, Bayesian methods
Introduction
Obsessive-compulsive disorder (OCD) is a type of mental illness characterized by persistent, intrusive, and unnecessary obsession and repetitive compulsion.1 It causes marked impairments in social functioning, with a lifetime prevalence rate of 2.43%.2 Patients with OCD struggle to suppress intrusive thoughts and repetitive behaviors, which manifest as cognitive and behavioral inflexibility.3,4 Crucially, this rigidity appears to extend beyond clinical symptoms, also seen in unaffected first-degree relatives, suggesting that inflexibility represents a cognitive phenotype and a potential marker of genetic vulnerability.4–7
Emerging evidence suggests that deficits in cognitive flexibility may not only be linked to greater severity of obsessive-compulsive symptoms (OCS),8–10 but also function as a pivotal prognostic indicator;11 indeed, improvements in flexibility following cognitive behavioral therapy (CBT) or Acceptance and Commitment therapy (ACT) are predictive of meaningful symptom reduction.12,13 Cognitive flexibility is recognized as a multidimensional construct that varies based on executive functioning, default mental states, and personality configurations.14 Clinical evidence further suggests that the inflexibility of OCD presents in multiple aspects, such as excessive adherence to rules, intolerance of uncertainty, and difficulty in interrupting ritualistic behaviors.14,15 However, little is known about the characteristics of these dimensions, which limits a comprehensive understanding of cognitive flexibility.
Current assessment methodologies, however, face significant limitations in capturing the breadth of this construct. While laboratory-based neuropsychological tasks such as the Wisconsin Card Sorting Test (WCST),16,17 the Intra-Extra Dimensional Shift task,18 and the Probabilistic Reversal Learning (PRL) task,19 are widely used to assess cognitive flexibility, they primarily reflect executive control processes and possess limited ecological validity. There is still a relative scarcity of tools that capture this ability in daily life, with only a few available instruments, including the Cognitive Flexibility Inventory (CFI), Cognitive Flexibility Scale (CFS), Behavior Rating Inventory of Executive Function (BRIEF), and Acceptance and Action Questionnaire-II (AAQ-II).20,21 These questionnaires differ in their specific focus. Specifically, CFI, CFS and BRIEF emphasize cognitive and executive functions, whereas AAQ-II is typically used as a measure of generalized psychological flexibility or as a process variable within the framework of ACT. However, existing questionnaires are constrained by their unidimensional focus or a limited scope that fail to capture the broad range of cognitive flexibility exhibited in daily life.22,23
To address the limitation of existing measures, Horne, Chen and Irish23 recently developed the Flexibility in Daily Life scale (FIDL), a multidimensional instrument designed to capture the daily life manifestations of cognitive flexibility, including repetitive and stereotyped behaviors. In its initial validation, the FIDL was refined from an original 37-item pool to a 21-item, five-factor structure comprising Repetition, Switching, Predictability/Control, Routine, and Thoughts/Beliefs. Although initial validation in non-clinical Australian samples has demonstrated good reliability and potential as a promising transdiagnostic tool, its applicability to clinically diagnosed OCD populations remains unclear. This is an important gap, because OCD is characterized by pronounced rigidity, repetitive behavior, and over-reliance on routine,24 which may shape the way daily life flexibility is organized. In addition, the factor structure identified in a Western non-clinical sample may not generalize directly to non-Western cultural contexts, where the expression and interpretation of flexibility-related behaviors may differ.25,26 Therefore, evidence is still lacking as to whether the published FIDL structure can be replicated in Chinese individuals with OCD or whether an alternative structure is specifically suited for this population.
Against this background, the present study was designed primarily as an exploratory investigation of the factor structure of the Chinese-translated FIDL in a clinical sample of individuals with OCD. Specifically, we first examined whether the previously published 21-item five-factor model could be replicated in the present sample. Given the potential for clinical and cultural variations, we subsequently explored the latent structure of the original 37-item pool within the OCD subsample to identify a framework that is specifically suited for this population. A secondary aim was to evaluate the preliminary reliability and validity of the resulting structure. By addressing these aims, we sought to provide initial evidence for a clinically grounded assessment of multidimensional cognitive flexibility in Chinese individuals with OCD. Such an instrument may eventually help identify distinct patterns of inflexibility, inform the refinement of targeted interventions, and advance our understanding of the mechanisms underlying OCD in diverse clinical contexts.
Materials and Methods
Participants
This study enrolled 76 patients with OCD and 81 healthy controls (HC) between October 2023 and October 2025. A total of 76 patients with OCD were recruited from the outpatient department of Beijing Anding Hospital. All participants met DSM-5 diagnostic criteria for OCD, had a Y-BOCS score > 16, were aged 18–45 years, and provided written informed consent. No comorbid psychiatric disorders were identified based on the clinical evaluation. All clinical assessments were conducted by trained psychiatrists who received consistent training. The OCD group comprised 22 males and 54 females, with an average age of 30.25±6.80 years. Among these patients, 19 were receiving SSRI treatment, whereas 57 were unmedicated. HCs were recruited through advertisement during the same period. The HC group included 81 individuals, including 28 males and 53 females, with an average age of 27.47±5.36 years. Age, level of education, and other demographic characteristics were matched with those of the OCD group. HCs had no self-reported history of psychiatric disorders, severe neurological or organic diseases, substance dependence, or current use of psychoactive substances.
For test-retest reliability, all patients with OCD were invited to complete a follow-up assessment approximately one month after the initial evaluation. Of the 76 patients, 54 completed the follow-up questionnaire, and the test-retest analysis was therefore based on these 54 participants. No item-level missing data were observed among the completed questionnaires. The remaining 22 patients did not complete the follow-up assessment and were excluded from the test-retest analysis.
Measurements
The Flexibility in Daily Life Scale (FIDL)
The Chinese version of the FIDL used in the present study was based on the original 37-item version.23 The translation procedure involved forward translation and back-translation conducted by two bilingual clinical psychologists. After reconciliation of the translated versions, a preliminary Chinese version was generated for use in this study. However, a formal expert committee review, cognitive interviewing, and pilot pretesting in a patient sample were not conducted during the cross-cultural adaptation process. Therefore, the current findings should be interpreted as a preliminary psychometric evaluation of the Chinese FIDL, and further linguistic validation following established cross-cultural adaptation guidelines is warranted.
The Yale-Brown Obsessive-Compulsive Scale (Y-BOCS)
Y-BOCS27,28 is a 10-item scale to measure the severity of OCS. It is divided into two dimensions: obsessive-compulsive thinking and obsessive-compulsive behavior. The higher the score, the more severe the OCS. The Chinese version of Y-BOCS has good inter-rater reliability (r = 0.75), test-retest reliability (r = 0.91).
The Obsessive-Compulsive Inventory-Revised (OCI-R)
OCI-R29,30 is used to measure self-reported OCS. It consists of 18 items, divided into 6 dimensions: washing, obsessing, hoarding, ordering, checking, and neutralizing. The higher the score, the more severe the symptoms. The Chinese version has good internal consistency (Cronbach’s α = 0.84) and test-retest reliability (r = 0.96).
Statistical Analysis
Confirmatory factor analysis (CFA) was first conducted in the full sample to evaluate the fit of the previously reported factor structure of the Chinese version of the FIDL. CFA was conducted using IBM SPSS AMOS 29.0. Parameters were estimated using the maximum likelihood (ML) method. Model fit was evaluated using the chi-square statistic (χ2), comparative fit index (CFI), Tucker-Lewis index (TLI), root mean square error of approximation (RMSEA), and standardized root mean square residual (SRMR). Conventionally, CFI and TLI values of ≥ 0.90 indicate acceptable fit and ≥ 0.95 indicate good fit, whereas RMSEA and SRMR values of ≤ 0.08 indicate acceptable fit.
Given the inadequate fit of the original model, the clinical focus and exploratory nature of the present study, and the limited clinical sample available, exploratory factor analysis (EFA) was subsequently performed in the OCD subsample to examine a potentially more suitable latent structure for this population, although the participant-to-item ratio was below commonly recommended standards. The number of factors retained was determined based on parallel analysis, together with the interpretability of the factor solution. Parallel analysis, EFA and reliability were conducted using JASP.
To examine whether the factor structure suggested by EFA was better represented by a multidimensional solution than by more parsimonious alternatives, we conducted a series of confirmatory factor analyses. Four types of models were tested: a one-factor model, three alternative two-factor models, and a correlated three-factor model. In the one-factor model, all items were specified to load on a single latent factor. In the two-factor models, two of the proposed dimensions were combined into one factor, whereas the remaining dimension was retained as a separate factor. In the correlated three-factor model, Contextual Adaptability, Cognitive-Behavioral Rigidity, and Routine/Control were specified as three distinct but correlated latent factors. Model fit was assessed using χ2/df, CFI, TLI, RMSEA, and SRMR.
To further examine the robustness of the factor structure identified by EFA, Bayesian exploratory factor analysis (BEFA) was performed using the BayesFM package and blavvan packages in R4.4.3. BEFA was used to provide a probabilistic evaluation of the latent structure, particularly with regard to the most plausible number of factors and the allocation of items to factors. In this way, BEFA served as a complementary analytic approach to assess the stability of the EFA-derived solution following the inadequate fit of the original CFA model.
To examine potential attrition bias, baseline demographic and clinical characteristics were compared between patients who completed the follow-up assessment and those who did not. Demographic and clinical characteristics, as well as all reliability and validity analyses, were analyzed using SPSS 27.0.1.
Results
Confirmatory Factor Analysis
The 21-item version showing strong reliability and validity was employed to validate the measure in a Chinese population, including 76 OCD patients and 81 HC participants. The results of CFA showed that χ2/df=2.042, TLI=0.791, CFI=0.822, SRMR=0.087, RMSEA=0.082. The loadings of each item on the corresponding factor ranged from 0.034 to 0.785.
Group Differences in FIDL Between OCD and HC
Except for Routine factor, the other 4 factors and total scores of OCD patients were significantly higher than those of HC, indicating that OCD patients had poor cognitive flexibility (Table 1).
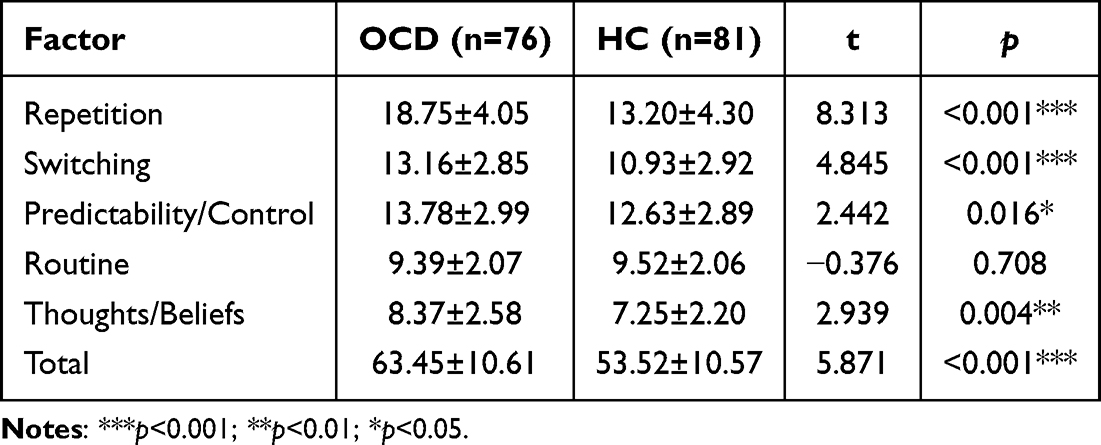 |
Table 1 Comparison of FIDL Scores Between the OCD and HC Groups |
Exploratory Factor Analysis
Given that the initial CFA of the 21-item version yielded suboptimal fit indices, we deemed it necessary to further investigate the potential underlying structure within this clinical population. Consequently, we performed EFA using the original 37-item FIDL in OCD population to develop a more appropriate construct. The results of the feasibility test for factor analysis indicated that the KMO value was 0.732, and Bartlett’s test of Sphericity was significant (p<0.001), as shown in Table 2, suggesting that the data were suitable for factor analysis. Based on the parallel analysis and scree plot, three common factors were extracted. Principal axis factoring was applied, followed by Promax oblique rotation. Items with factor loadings below 0.40 or with substantial cross-loadings were removed, resulting in a final set of 25 items (see Supplementary Material Table S1).
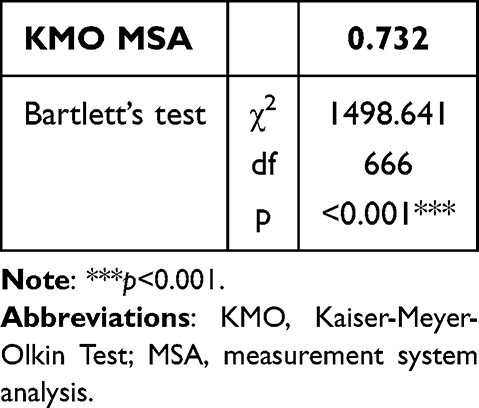 |
Table 2 The Results of KMO Test and Bartlett’s Test |
After rotation, the factor structure became clearly delineated. As illustrated in Figure 1, Factor 1 comprised items 7, 10, 11, 28, 32, 36, and 37, and was labeled “Contextual Adaptability”. This factor reflects the capacity for attentional control and task switching in response to contextual cues within a situation. Factor 2 consisted of items 1, 15, 16, 17, 18, 19, 21, 23, 30, and 31, labeled “Cognitive-Behavioral Rigidity”, capturing automatic thought processes and habitual behavioral patterns. Factor 3 included items 2, 8, 9, 13, 20, 22, 33, and 34, labeled “Routine/Control”, representing a preference for specific routines and a strong need for order in daily situations. The detailed content of each factor is provided in Supplementary Table S2. Notably, item 8 showed a negative loading on Factor 3, whereas the other items loading on this factor showed positive loadings. This pattern is theoretically consistent with the wording of item 8, which reflects the opposite pole of the construct represented by Factor 3. Accordingly, item 8 was treated as a reverse-scored item when calculating the routine/control subscale, so that higher scores consistently reflected a stronger preference for routine and repetitive daily behavior.
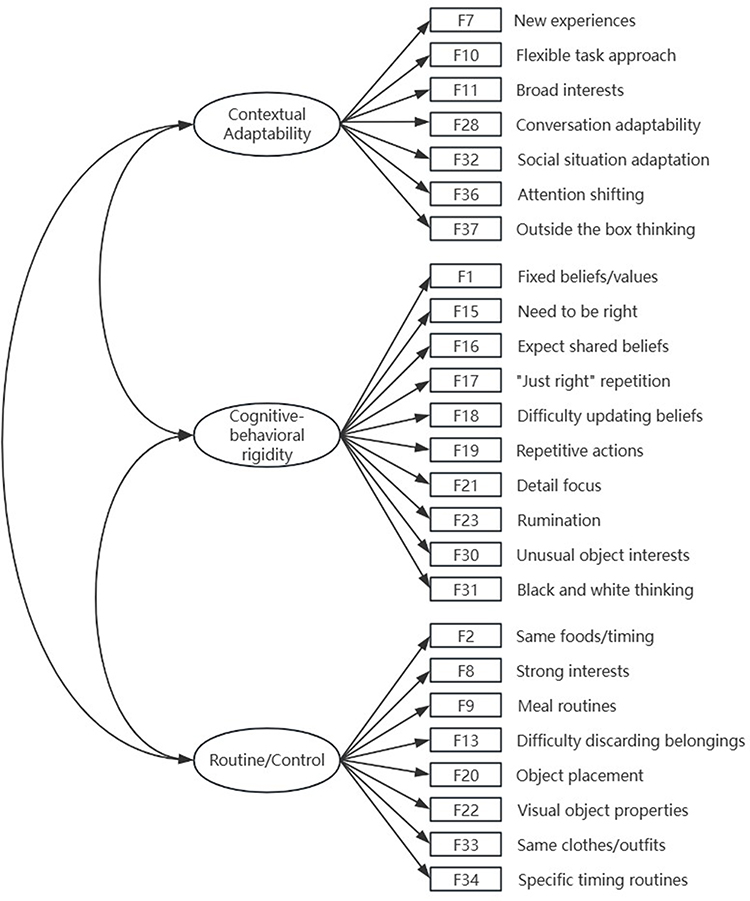 |
Figure 1 The structure diagram of three factors from exploratory factor analysis. |
The squared loadings of the three factors were 5.232, 4.881, and 3.788, accounting for 14.1%, 13.2%, and 10.2% of the variance, respectively. In total, the three-factor solution explained 37.6% of the overall variance (Table 3).
 |
Table 3 Factor Characteristics |
Comparison of Alternative Factor Structures
Following the EFA, we compared the extracted three-factor solution with more parsimonious alternatives using CFA. Specifically, a one-factor model, three alternative two-factor models, and the original correlated three-factor model were tested.
The correlated three-factor model provided the best relative fit among the tested models, whereas the one-factor model showed the poorest fit. Specifically, the one-factor model demonstrated poor fit to the data (χ2/df = 2.578, CFI = 0.575, TLI = 0.536, RMSEA = 0.145, SRMR = 0.171). The three alternative two-factor models showed some improvement over the one-factor solution. The least favorable two-factor model was the model combining Contextual Adaptability and Cognitive-Behavioral Rigidity while retaining Routine/Control as a separate factor (χ2/df = 2.529, CFI = 0.589, TLI = 0.550, RMSEA = 0.143, SRMR = 0.168). Better performance was observed for the two-factor model combining Contextual Adaptability and Routine/Control (χ2/df = 2.200, CFI = 0.678, TLI = 0.647, RMSEA = 0.126, SRMR = 0.156), and for the two-factor model combining Cognitive-Behavioral Rigidity and Routine/Control (χ2/df = 2.189, CFI = 0.681, TLI = 0.650, RMSEA = 0.126, SRMR = 0.152). Among all candidate models, the correlated three-factor model yielded the best fit (χ2/df = 2.095, CFI = 0.708, TLI = 0.678, RMSEA = 0.121, SRMR = 0.146). However, although this model outperformed the one-factor and two-factor alternatives, its absolute fit remained unsatisfactory. Thus, the CFA provided only limited support for the proposed three-factor structure.
In the three-factor model, standardized loadings for Contextual Adaptability ranged from 0.522 to 0.888. Standardized loadings for Cognitive-Behavioral Rigidity ranged from 0.367 to 0.746, and standardized loadings for Routine/Control ranged from 0.454 to 0.618. The latent factor correlations in the correlated three-factor model were moderate in magnitude. Contextual Adaptability was correlated with Cognitive-Behavioral Rigidity at r = 0.386 and with Routine/Control at r = 0.604. Cognitive-Behavioral Rigidity and Routine/Control were correlated at r = 0.627. These values indicate that the three dimensions were related, but they were not empirically redundant within the confirmatory framework.
Bayesian Exploratory Factor Analysis
To control for the potential influence of sample size and to further evaluate the robustness of the factor structure, we performed a BEFA. The reversible-jump MCMC algorithm explored models with up to three factors. In total, we ran 7000 MCMC iterations, including 2000 burn-in iterations and 5000 iterations retained for posterior estimation. The posterior distribution of the number of factors strongly supported a three-factor solution, with 99.66% of posterior samples assigning the model to three latent factors, as shown in Figure 2.
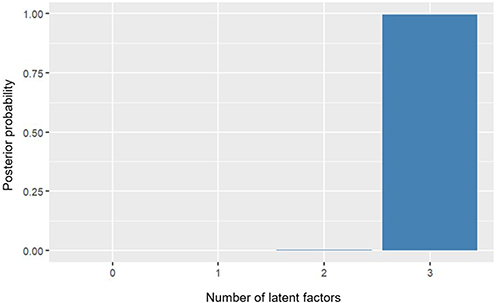 |
Figure 2 Posterior distribution of the number of latent factors. Notes: The figure shows the posterior probability associated with each candidate factor solution. The three-factor solution had the highest posterior probability, supporting the retention of three latent factors. |
Model estimation demonstrated excellent MCMC performance, with a Metropolis-Hastings acceptance rate of 0.998 and stable posterior summaries across iterations. Item-factor assignments were evaluated using the posterior mode of the iteration parameter. Most items showed high posterior probabilities for their assigned factor (generally>0.70), indicating stable and well-identified item-factor associations (see Supplementary Material Table S3). Posterior loading summaries further confirmed this structure. Each item displayed its strongest loading within its assigned factor, and only minimal cross-loading tendencies were observed (see Supplementary Material Table S4).
The model showed acceptable information criteria values (DIC=1947.924; WAIC=2062.247; LOOIC=2062.906), suggesting that the estimated factor structure provided a reasonable balance between model fit and complexity. Posterior predictive checking indicated acceptable model fit. The posterior predictive p-value (PPP=0.10) fell within the commonly accepted range (0.10–0.90), suggesting no substantial discrepancy between the model-implied and observed data. As shown in Figure 3, the observed SRMR was well captured by the posterior predictive distribution, and there was no visual evidence of systematic model misfit.
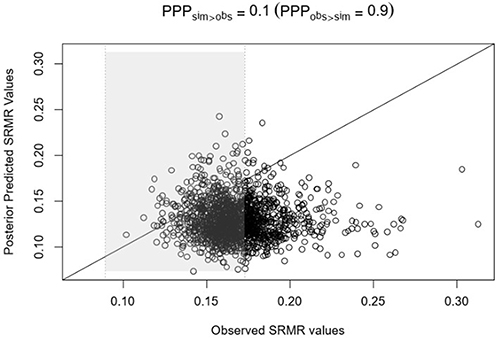 |
Figure 3 Posterior Predictive Check based on SRMR. Notes: Each point represents one posterior draw. The x-axis shows the SRMR value from the observed data, and the y-axis shows the SRMR value from a dataset replicated under the fitted Bayesian model. The diagonal line indicates equality between observed and replicated values. The posterior predictive p-value summarizes the model’s fit by comparing discrepancies in the observed and replicated data. |
Despite the clear three-factor allocation, the estimated latent factors were extremely highly correlated. Posterior means of factor correlations ranged from 0.97 to 0.99, with narrow 95% HPD intervals (Table 4). It suggested that the three dimensions are strongly overlapping and may reflect closely related aspects of a common underlying construct.
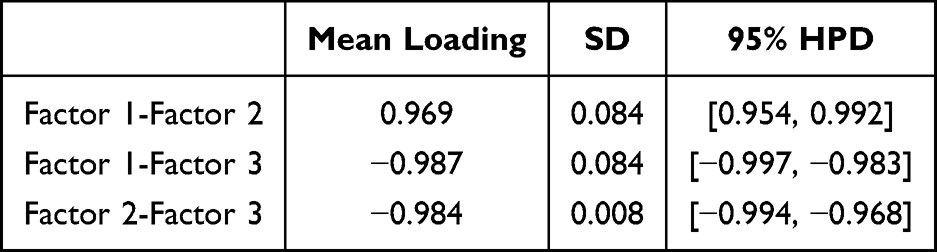 |
Table 4 Factor Correlation Matrix |
Reliability of Revised 25-Item Scale
Coefficient of Internal Consistency
The overall Cronbach’s α coefficient of the Chinese version of the 25-item FIDL scale for OCD patients was 0.838, and for the Contextual Adaptability, Cognitive-behavioral rigidity, Routine/Control factors were 0.832, 0.817, and 0.699, respectively (Table 5). After removing anyone of the items, the Cronbach’s α coefficient ranged from 0.824 to 0.856.
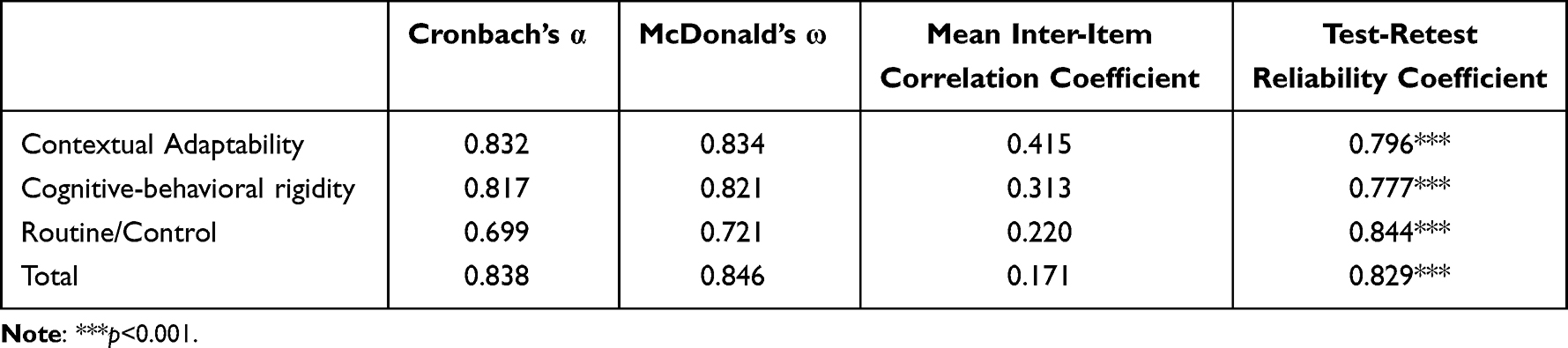 |
Table 5 The Reliability Indicators of the Revised 25-Item FIDL |
The overall McDonald’s ω coefficient of the Chinese version of the 25-item FIDL total scale and for the Contextual Adaptability, Cognitive-behavioral rigidity, Routine/Control factors were 0.846, 0.834, 0.821, and 0.721, respectively (Table 5).
Mean Inter-Item Correlation Coefficient
The mean inter-item correlation coefficient among the items of the FIDL total scale and the factors of Contextual Adaptability, Cognitive-behavioral rigidity, Routine/Control were 0.171, 0.415, 0.313, and 0.220, respectively (Table 5).
Test-Retest Reliability Coefficient
To assess potential attrition bias, baseline age, gender, and Y-BOCS scores were compared between patients who completed the one-month retest and those who did not. No significant differences were found between the two groups (age: t=−0.389, p=0.698; gender: χ2=0.124, p=0.725; Y-BOCS: t=0.406, p=0.686).
The initial test scores of the 25-item FIDL total scale and its factors of Contextual Adaptability, Cognitive-behavioral rigidity, Routine/Control were 72.82±11.59, 18.87±4.52, 32.30±6.39, 21.64±4.97. The retest scores were 75.11±10.69, 19.24±4.28, 33.04±5.36, 22.83±5.29. The retest scores of total and the 3 factors were all positively correlated with the initial scores (p<0.001). The test-retest reliability coefficients were 0.829, 0.796, 0.777, and 0.844, respectively (Table 5).
Group Differences in 25-Items FIDL Between OCD and HC
Except for Routine/Control factor, other factors and total scores of OCD patients were significantly higher than those of HC, indicating that OCD patients had poor cognitive flexibility (Table 6).
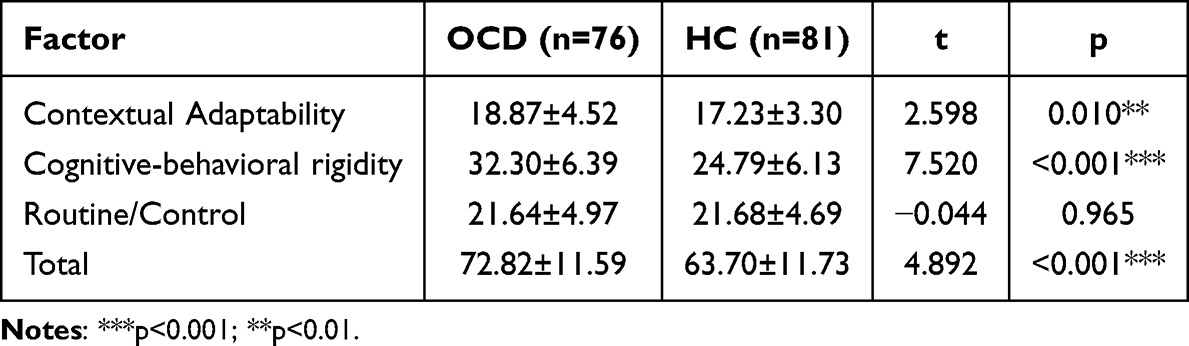 |
Table 6 Comparison of 25-Items FIDL Scores Between the OCD and HC Groups |
Correlation Between Three Factors and Clinical Symptoms
The mean total Y-BOCS score for the sample was 23.13±3.79, and the mean total OCI-R score was 25.58±13.39. Correlation analyses were conducted for both the total score of the revised 25-item FIDL and its three factor scores. The total score and the Cognitive-behavioral rigidity factor were positively correlated with both Y-BOCS and OCI-R scores (p<0.01). Routine/Control factor showed a positive correlation with the OCI-R total score (r=0.400, p<0.001). In contrast, the Contextual Adaptability factor was not significantly associated with either Y-BOCS or OCI-R scores (p>0.05) (Table 7).
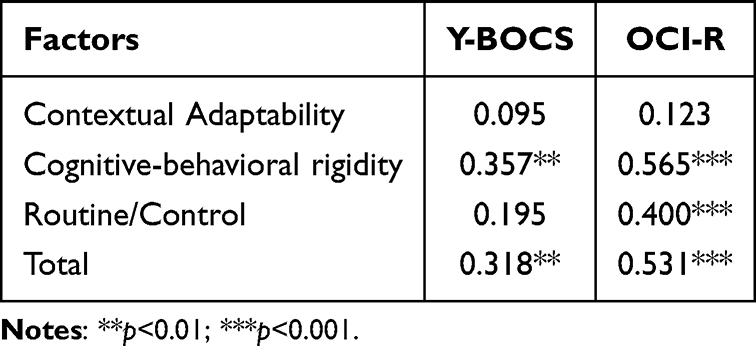 |
Table 7 The Correlation Between Three Factors and OCS |
Discussion
Cognitive flexibility is a core cognitive characteristic of OCD and may play an important role in the maintenance and treatment. Despite its clinical relevance, the psychometric performance of cognitive flexibility measures has received limited attention in OCD populations. In this study, we administered the multidimensional FIDL, which provides a more comprehensive assessment of daily life cognitive flexibility, to a clinical sample of OCD patients in China. A renewed EFA identified a revised 25-item version with a three-factor structure, which was further examined using BEFA and reliability testing. The results provide preliminary support for the internal structure and reliability of the Chinese FIDL. However, because the analyses were exploratory and further evidence is needed regarding cross-cultural equivalence, discriminant validity, and replication in independent samples, this structure should be interpreted as an initial empirical framework rather than a definitive validation of the scale. These findings offer a foundation for future research on the assessment of daily-life cognitive flexibility in Chinese OCD populations.
The CFA indicated that the five-factor structure of the FIDL was suboptimal within the Chinese OCD population. This discrepancy might reflect a complex interplay of population-specific, cultural, and methodological factors. First, the five-factor FIDL was developed and validated in a western, predominantly healthy adult sample,23 and its utility in clinical population featured with inflexibility needs to be further examined. The rigidity profile of healthy individuals shows limited overlap with that of OCD populations, who consistently demonstrate marked rigid thinking and behavior.31 Moreover, cultural and contextual factors may partly explain the incomplete replication of the original FIDL structure, although this interpretation remains tentative. Previous cross-cultural research suggests that flexibility-related constructs, such as emotion regulation and expressive flexibility, may show both shared and culture-specific patterns in their meaning and psychological correlates.32,33 However, because the present study did not directly compare Chinese and original-language samples or test measurement invariance across cultural groups, cultural specificity cannot be established as a direct explanation. Future studies should therefore use cross-cultural comparison and measurement invariance testing to determine whether the observed factor structure reflects cultural adaptation effects, OCD-specific characteristics, or sample-specific instability.
To elucidate a latent structure better aligned with the clinical profile of Chinese patients with OCD, we conducted an EFA and yield a 25-item version of the FIDL with a three-factor structure: Contextual adaptability, Cognitive-behavioral rigidity, and Routine/Control. BEFA was subsequently used to scrutinize this structure. Taken together, the posterior factor distribution, item-factor allocation patterns, and loading estimates provide robust supported for a three-factor structure. Psychometric evaluations further demonstrated that the revised version exhibits good internal consistency reliability and test-retest reliability. These findings preliminarily verified that the new revised version was applicable to Chinese patients with OCD.
The exploratory three-factor structure of the 25-item FIDL may be broadly consistent with multidimensional perspectives in the flexibility literature. For example, Kashdan and Rottenberg’s14 conceptualization of psychological flexibility highlights multiple components of adaptive functioning, which includes executive functioning, default mental states, and personality configurations. While psychological flexibility and cognitive flexibility in daily life are conceptually distinct, both concern adaptive responses to changing demands. In this sense, the former may provide a useful comparative framework for understanding the multidimensional pattern observed in the FIDL, although it should not be taken as conceptually equivalent to the construct measured here. Specifically, the Cognitive-Behavioral Rigidity factor reflect various forms of “stereotyping and habits” of default mental states, including adherence to existing beliefs, difficulty in adopting others’ perspectives, a preference for fixed ways of managing tasks, dichotomous (“black and white”) thinking, and repetitive behaviors, excessive attention to detail, a tendency to insist that others follow established rules. Overall, the factor captures the difficulties patients experience in altering entrenched patterns of thinking and behavior. Importantly, this dimension was incorporated into the FIDL to provide a more comprehensive assessment of the multidimensional nature of cognitive flexibility by including additional cognitive and behavioral characteristics. The Contextual Adaptability factor corresponds to the executive functioning of “refocus or rapidly shift cognitive sets and thereby shift attention”. It reflects ability to adjust attention and behavior across different social contexts, respond smoothly when the topic of conversation or ongoing activity shifts. The content of this dimension parallels constructs commonly assessed in prior flexibility measures, such as the Shift subscale of the BRIEF, representing a disposition toward effective adaptation to changing circumstances and situational demands. Finally, Routine/Control factors correspond to personality configurations that reflect a preference for specific routines and need for order in situations. It is conceptually related to “Routines and Rituals” dimension of the flexibility scale,34 in that both concern perceived control and order under changing conditions. It represents relatively stable, trait-like tendencies—such as high conscientiousness or strong needs for structure—that constrain flexibility in daily functioning.35 However, this interpretation remains tentative. Because the present analyses were exploratory and the extracted factors showed high intercorrelations, the findings do not yet demonstrate that the three factors are clearly distinct or that they closely correspond to established theoretical dimensions of flexibility. Thus, the proposed structure should be regarded as a preliminary framework that requires further validation in independent samples, with additional evidence from confirmatory factor analysis, exploratory structural equation modeling, and convergent and discriminant validity testing.
Moreover, OCD is characterized by rigid patterns of thinking and behavior, often accompanied by ritualized routines.3,4,36,37 Researchers believed that intolerance of uncertainty and a heightened need for control are central cognitive vulnerabilities of OCD.38 The three factors identified in the revised structure align closely with the core pathology of OCD. The factors we labeled “Cognitive-behavioral rigidity” and “Routine/Control” consolidate the most clinically relevant elements of the original five-factor model and map directly onto these hallmark features of OCD. The non-significant difference between OCD and HC on the Routine/Control dimension may indicate that this dimension captures relatively common preferences for order, routine, and predictability rather than OCD-specific impairment. Previous study has suggested that rituals and routines are common in non-clinical populations, whereas OCD-related rituals are distinguished by distress, loss of control, functional interference, and considerable symptom heterogeneity across dimensions.39,40 Although the present study did not find a significant association between the “Contextual Adaptability” dimension and clinical symptom severity, this finding should be interpreted with caution. Given that individuals with OCD frequently exhibit executive dysfunction, particularly in attentional control and cognitive shifting, their reduced capacity to adjust to changing contextual cues or task demands may reflect subtle executive impairments that were not fully captured in the current sample. Future research is needed to further explore the characteristics of this dimension and its relationship with symptom presentation in OCD populations. These findings suggest that the Chinese FIDL may provide clinically relevant information beyond conventional OCS measures. The Chinese FIDL may also be useful in future OCD treatment studies, including CBT/ACT and pharmacological trials for treatment-resistant OCD, by assessing cognitive and behavioral flexibility as a complementary treatment-response indicator beyond symptom severity.41,42 An additional issue worthy of future investigation is whether digital-era compulsive phenomena, such as obsession-driven repetitive scrolling, online checking, or other technology-mediated reassurance-seeking behaviors, constitute a clinically meaningful extension of the current construct. Because the present study did not include items specifically designed to assess such behaviors, this possibility could not be examined here and should be addressed in future scale development research.
Taken together, the revised 25-item, three-factor Chinese version provides a preliminary and exploratory representation of daily life flexibility in Chinese individuals with OCD. Notably, the present findings provide only limited support for the proposed three-factor structure. Although the correlated three-factor CFA model demonstrated better relative fit than the one-factor and two-factor alternatives, its absolute fit remained unsatisfactory, indicating that the superiority of the three-factor model should be interpreted cautiously rather than as clear confirmation of the hypothesized structure. This cautious interpretation is further supported by the BEFA results. The three-factor solution accounted for only 37.6% of the total variance, suggesting that the extracted factors provided a relatively modest explanation of the item covariance. Moreover, the inter-factor correlations were extremely high, indicating that the three dimensions shared substantial common variance and were only weakly differentiated. Taken together, these findings suggest that although a three-factor representation may capture more information than more parsimonious alternatives, the factors do not appear to represent clearly distinct latent constructs. Rather, the scale may be better understood as assessing a broad underlying construct with partially differentiated but highly overlapping subdomains. This interpretation is consistent with methodological discussions emphasizing that comparative model superiority should be evaluated alongside absolute model fit, explained variance, and discriminant validity concerns. Future research should therefore examine whether a more flexible measurement model, such as ESEM model,43 better represents the data, and should refine item content to improve both overall explanatory power and dimensional distinctiveness.
Beyond these findings, several limitations of the present study should be acknowledged. First, the proposed three-factor structure should be regarded as preliminary. The EFA and BEFA were conducted in a relatively small clinical sample without an a priori power analysis, and the model was not fully cross-validated in an independent OCD sample. Given that sample size and factor-retention decisions can affect the stability and replicability of exploratory factor solutions, future studies should validate the Chinese FIDL in larger, independent, and preferably multicenter OCD samples.44,45 Second, the sample predominantly consisted of individuals with compulsive washing symptoms, which may limit the generalizability of the findings to the broader OCD population, given the heterogeneous symptom dimensions of OCD.46 Third, construct validity was only partially examined. Although correlations with the Y-BOCS and OCI-R provided preliminary evidence of convergent validity, these measures assess OCS severity rather than flexibility itself. Future studies should examine convergence with other flexibility-related instruments, such as the CFI, CFS, as well as neuropsychological tasks such as WCST and PRL task.23 Fourth, discriminant validity was not formally assessed, which is particularly relevant given the high inter-factor correlations observed in the BEFA. Future research should examine whether the FIDL subscales are distinguishable from each other and from related constructs such as OCD severity, anxiety, depression, rumination, intolerance of uncertainty, and cognitive rigidity. Finally, medication status, psychiatric comorbidities, and several recommended cross-cultural adaptation procedures, such as expert review, cognitive interviewing, and pilot testing, were not fully addressed, which may have influenced self-reported flexibility and limited semantic or conceptual equivalence with the original scale.47,48
Conclusion
This study evaluated the factorial validity and preliminary applicability of the Chinese version FIDL in a clinical OCD population. Findings indicated that the original five-factor structure yielded suboptimal fit in this population. Based on the EFA, we propose a revised 25-item, three-factor model as a viable alternative for evaluating self-reported daily life cognitive flexibility among Chinese patients. However, these findings should be interpreted with caution in light of several limitations, including the modest sample size for the EFA, the incomplete assessment of construct validity, and the unresolved issue of factor distinctiveness. Consequently, the revised Chinese FIDL should be considered a preliminary and promising measurement framework rather than a fully validated instrument. Future research involving larger, multi-center, and more diverse samples, coupled with more rigorous psychometric evaluations, is needed to confirm the robustness of this structure. If supported by future evidence, this framework may contribute to the assessment of multidimensional inflexibility in OCD and foster a more refined understanding of cognitive features relevant to clinical evaluation and intervention.
Abbreviations
OCD, Obsessive-compulsive disorder; OCS, Obsessive-compulsive symptoms; CBT, Cognitive behavioral therapy; ACT, Acceptance and commitment therapy; WCST, Wisconsin Card Sorting Test; PRL, Probabilistic Reversal Learning; CFI, Cognitive Flexibility Inventory; CFS, Cognitive Flexibility Scale; BRIEF, Behavior Rating Inventory of Executive Function; AAQ-II, Acceptance and Action Questionnaire-II; FIDL, Flexibility in Daily Life Scale; HC, Healthy control; Y-BOCS, Yale-Brown Obsessive-Compulsive Scale; OCI-R, Obsessive-compulsive Inventory-Revised; CFA, Confirmatory factor analysis; ML, maximum likelihood; χ2, the chi-square statistic; CFI, comparative fit index; TLI, Tucker-Lewis index; RMSEA, root mean square error of approximation; SRMR, standardized root mean square residual; EFA, exploratory factor analysis; BEFA, Bayesian exploratory factor analysis; KMO, Kaiser-Meyer-Olkin Test; MSA, Measurement system analysis.
Data Sharing Statement
The data presented in this study are available from corresponding author (Dr Pengchong Wang, [email protected]) on reasonable request.
Ethics Approval and Informed Consent
This study involving human participants were reviewed and approved by Research Ethics Committee of Beijing Anding Hospital. All participants provided their written informed consent to participate in this study.
Acknowledgments
We thank the members of the Cognitive Behavioral Therapy research group at Beijing Anding Hospital, Capital Medical University, for their participation and support in this study, and the Neuropsychological Platform for providing equipment and facilities for the research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by National Natural Science Foundation of China (No. 82171542), Beijing Anding Hospital Obsessive-Compulsive Disorder Prospective Cohort Study (Grant No.3-1-55), and Beijing Municipal Administration of Hospitals Clinical Medicine Development of Special Funding Support (code: XMLX202129).
Disclosure
The authors report no conflicts of interest in this work.
References
1. American Psychiatric Association. Desk Reference to the Diagnostic Criteria From DSM-V. Vols. 24–26. American Psychiatric Publishing; 2013.
2. Liu B, Cheng J, Liu Z, et al. Prevalence of obsessive-compulsive disorder and related healthcare utilisation in China: a cross-sectional epidemiological survey. Gen Psychiatr. 2025;38(6):e102013. doi:10.1136/gpsych-2024-102013
3. Eichholz A, Schwartz C, Meule A, Heese J, Neumüller J, Voderholzer U. Self-compassion and emotion regulation difficulties in obsessive-compulsive disorder. Clin Psychol Psychother. 2020;27(5):630–14. doi:10.1002/cpp.2451
4. Rosa-Alcázar AI, Rosa-Alcázar Á, Martínez-Esparza IC, Storch EA, Olivares-Olivares PJ. Response inhibition, cognitive flexibility and working memory in obsessive-compulsive disorder, generalized anxiety disorder and social anxiety disorder. Int J Environ Res Public Health. 2021;18(7):3642. doi:10.3390/ijerph18073642
5. Abramovitch A, Abramowitz JS, Mittelman A. The neuropsychology of adult obsessive-compulsive disorder: a meta-analysis. Clin Psychol Rev. 2013;33(8):1163–1171. doi:10.1016/j.cpr.2013.09.004
6. Bora E. Meta-analysis of neurocognitive deficits in unaffected relatives of obsessive-compulsive disorder (OCD): comparison with healthy controls and patients with OCD. Psychol Med. 2020;50(8):1257–1266. doi:10.1017/s0033291720001634
7. Martínez-Esparza IC, Olivares-Olivares PJ, Rosa-Alcázar Á, Rosa-Alcázar AI, Storch EA. Executive functioning and clinical variables in patients with obsessive-compulsive disorder. Brain Sci. 2021;11(2):267. doi:10.3390/brainsci11020267
8. Snyder HR, Kaiser RH, Warren SL, Heller W. Obsessive-compulsive disorder is associated with broad impairments in executive function: a meta-analysis. Clin Psychol Sci. 2015;3(2):301–330. doi:10.1177/2167702614534210
9. Whiting DL, Deane FP, Simpson GK, McLeod HJ, Ciarrochi J. Cognitive and psychological flexibility after a traumatic brain injury and the implications for treatment in acceptance-based therapies: a conceptual review. Neuropsychol Rehabil. 2017;27(2):263–299. doi:10.1080/09602011.2015.1062115
10. Ramakrishnan S, Robbins TW, Zmigrod L. Cognitive rigidity, habitual tendencies, and obsessive-compulsive symptoms: individual differences and compensatory interactions. Front Psychiatry. 2022;13:865896. doi:10.3389/fpsyt.2022.865896
11. Elsner B, Beucke JC, Kathmann N, Reuter B. Pavlovian fear reversal learning predicts outcome of exposure-based cognitive behavioral therapy for adult obsessive-compulsive disorder. J Psychiatr Res. 2025;191:23–29. doi:10.1016/j.jpsychires.2025.09.012
12. Twohig MP, Vilardaga JCP, Levin ME, Hayes SC. Changes in psychological flexibility during acceptance and commitment therapy for obsessive compulsive disorder. J Contextual Behav Sci. 2015;4(3):196–202. doi:10.1016/j.jcbs.2015.07.001
13. Schubert C, Hilbert S, Favreau M, Wolstein J, Voderholzer U. Psychological flexibility as a potential change factor in cognitive behavioural therapy of OCD. Behav Cogn Psychother. 2022;50(4):381–391. doi:10.1017/s1352465822000091
14. Kashdan TB, Rottenberg J. Psychological flexibility as a fundamental aspect of health. Clin Psychol Rev. 2010;30(7):865–878. doi:10.1016/j.cpr.2010.03.001
15. Dajani DR, Uddin LQ. Demystifying cognitive flexibility: implications for clinical and developmental neuroscience. Trends Neurosci. 2015;38(9):571–578. doi:10.1016/j.tins.2015.07.003
16. Berg EA. A simple objective technique for measuring flexibility in thinking. J Gen Psychol. 1948;39:15–22. doi:10.1080/00221309.1948.9918159
17. Grant DA, Berg EA. A behavioral analysis of degree of reinforcement and ease of shifting to new responses in a Weigl-type card-sorting problem. J Exp Psychol. 1948;38(4):404–411. doi:10.1037/h0059831
18. Robbins TW, James M, Owen AM, et al. A study of performance on tests from the CANTAB battery sensitive to frontal lobe dysfunction in a large sample of normal volunteers: implications for theories of executive functioning and cognitive aging. J Int Neuropsychol Soc. 1998;4(5):474–490. doi:10.1017/s1355617798455073
19. Cools R, Clark L, Owen AM, Robbins TW. Defining the neural mechanisms of probabilistic reversal learning using event-related functional magnetic resonance imaging. J Neurosci. 2002;22(11):4563–4567. doi:10.1523/jneurosci.22-11-04563.2002
20. Miles S, Gnatt I, Phillipou A, Nedeljkovic M. Cognitive flexibility in acute anorexia nervosa and after recovery: a systematic review. Clin Psychol Rev. 2020;81:101905. doi:10.1016/j.cpr.2020.101905
21. Uddin LQ. Cognitive and behavioural flexibility: neural mechanisms and clinical considerations. Nat Rev Neurosci. 2021;22(3):167–179. doi:10.1038/s41583-021-00428-w
22. Strang JF, Anthony LG, Yerys BE, et al. The flexibility scale: development and preliminary validation of a cognitive flexibility measure in children with autism spectrum disorders. J Autism Dev Disord. 2017;47(8):2502–2518. doi:10.1007/s10803-017-3152-y
23. Horne K, Chen T, Irish M. Development of the Flexibility in Daily Life scale to measure multidimensional cognitive and behavioural flexibility in health and disease. Br J Clin Psychol. 2025;64(2):315–329. doi:10.1111/bjc.12505
24. Gruner P, Pittenger C. Cognitive inflexibility in obsessive-compulsive disorder. Neuroscience. 2017;345:243–255. doi:10.1016/j.neuroscience.2016.07.030
25. Feng B, Sheehan R, Utama P, et al. Cross-cultural differences on affective, cognitive, and psychiatric measures: evidence from a British-Chinese comparison. Ment Health Sci. 2025;3(2):e70020. doi:10.1002/mhs2.70020
26. Schirmbeck K, Rao N, Maehler C. Similarities and differences across countries in the development of executive functions in children: a systematic review. Infant Child Dev. 2020;29(1):e2164. doi:10.1002/icd.2164
27. Goodman WK, Price LH, Rasmussen SA, et al. The yale-brown obsessive compulsive scale. II. Validity. Arch Gen Psychiatry. 1989;46(11):1012–1016. doi:10.1001/archpsyc.1989.01810110054008
28. Zhang Y, Meng F, Cui Y, Gan X, Guo W. Study on clinical reliability and validity of Yale-Brown Obsessive Compulsive Scale. Chin Mental Health. 1996;10(5):205–207.
29. Peng ZW, Yang WH, Miao GD, Jing J, Chan RC. The Chinese version of the Obsessive-Compulsive Inventory-Revised scale: replication and extension to non-clinical and clinical individuals with OCD symptoms. BMC Psychiatry. 2011;11:129. doi:10.1186/1471-244x-11-129
30. Foa EB, Huppert JD, Leiberg S, et al. The Obsessive-Compulsive Inventory: development and validation of a short version. Psychol Assess. 2002;14(4):485–496. doi:10.1037/1040-3590.14.4.485
31. Chamberlain SR, Solly JE, Hook RW, Vaghi MM, Robbins TW. Cognitive inflexibility in OCD and related disorders. Curr Topics Behav Neurosci. 2021;49:125–145. doi:10.1007/7854_2020_198
32. Ang JYZ, Tsai W. Cultural differences in the relations between expressive flexibility and life satisfaction over time. Front Psychol. 2023;14:1204256. doi:10.3389/fpsyg.2023.1204256
33. Chen MS, Bi K, Han X, Sun P, Bonanno GA. Emotion regulation flexibility and momentary affect in two cultures. Nat Ment Health. 2024;2:450–459. doi:10.1038/s44220-024-00215-3
34. Hollocks MJ, McQuaid GA, Yerys BE, et al. Measuring flexibility in autistic adults: exploring the factor structure of the flexibility scale self report. Autism Res. 2023;16(11):2208–2219. doi:10.1002/aur.3025
35. Roberts BW, Lejuez C, Krueger RF, Richards JM, Hill PL. What is conscientiousness and how can it be assessed? Dev Psychol. 2014;50(5):1315–1330. doi:10.1037/a0031109
36. Calkins AW, Berman NC, Wilhelm S. Recent advances in research on cognition and emotion in OCD: a review. Curr Psychiatry Rep. 2013;15(5):357. doi:10.1007/s11920-013-0357-4
37. Chamberlain SR, Fineberg NA, Menzies LA, et al. Impaired cognitive flexibility and motor inhibition in unaffected first-degree relatives of patients with obsessive-compulsive disorder. Am J Psychiatry. 2007;164(2):335–338. doi:10.1176/ajp.2007.164.2.335
38. Pinciotti CM, Riemann BC, Abramowitz JS. Intolerance of uncertainty and obsessive-compulsive disorder dimensions. J Anxiety Disord. 2021;81:102417. doi:10.1016/j.janxdis.2021.102417
39. Wairauch Y, Siev J, Hasdai U, Dar R. Compulsive rituals in Obsessive-Compulsive Disorder - A qualitative exploration of thoughts, feelings and behavioral patterns. J Behav Ther Exp Psychiatry. 2024;84:101960. doi:10.1016/j.jbtep.2024.101960
40. Mataix-Cols D, Rosario-Campos MC, Leckman JF. A multidimensional model of obsessive-compulsive disorder. Am J Psychiatry. 2005;162(2):228–238. doi:10.1176/appi.ajp.162.2.228
41. Martiadis V, Pessina E, Martini A, et al. Brexpiprazole augmentation in treatment resistant OCD: safety and efficacy in an Italian sample. Psychiatr Danubina. 2024;36(Suppl 2):396–401.
42. Martiadis V, Pessina E, Cattaneo CI, et al. Efficacy and tolerability of vortioxetine monotherapy in SSRI-resistant OCD: a retrospective multicenter study. Front Psychiatry. 2025;16:1617345. doi:10.3389/fpsyt.2025.1617345
43. Afolabi KT, Konold T. The circle of methods for evaluating latent variable measurement models: EFA, CFA, and ESEM. Pract Assess Res Eval. 2024;29(1):15. doi:10.7275/pare.2061
44. Goretzko D, Bühner M. Robustness of factor solutions in exploratory factor analysis. Behaviormetrika. 2022;49:131–148. doi:10.1007/s41237-021-00152-w
45. Lorenzo-Seva U, Ferrando PJ. Determining Sample Size Requirements in EFA Solutions: a Simple Empirical Proposal. Multivariate Behav Res. 2024;59(5):899–912. doi:10.1080/00273171.2024.2342324
46. Zhou Y, Cao X, Wang J, et al. Association between miscellaneous symptoms and primary symptom dimensions among Chinese adults with obsessive-compulsive disorder. Psychiatry Res. 2019;274:274–279. doi:10.1016/j.psychres.2019.02.042
47. Sharma E, Sharma LP, Balachander S, et al. Comorbidities in obsessive-compulsive disorder across the lifespan: a systematic review and meta-analysis. Front Psychiatry. 2021;12:703701. doi:10.3389/fpsyt.2021.703701
48. Cruchinho P, López-Franco MD, Capelas ML, et al. Translation, cross-cultural adaptation, and validation of measurement instruments: a practical guideline for novice researchers. J Multidiscip Healthc. 2024;17:2701–2728. doi:10.2147/jmdh.S419714
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Psychometric Evaluation of the Grit Psychological Resources Scale (GPRS)
Schimschal SE, Cleary M, Kornhaber RA, Barnett T, Visentin DC
Journal of Multidisciplinary Healthcare 2023, 16:913-925
Published Date: 5 April 2023
Measuring Maternal Resilience in the Context of Parenting Challenges: A Korean Adaptation of the Maternal Resilience Scale
Jang HJ, Nam SH, Lee K, Lee J
International Journal of Women's Health 2026, 18:574491
Published Date: 10 February 2026