Back to Journals » Journal of Inflammation Research » Volume 19
Low Lymphocyte-to-Monocyte Ratio Predicts Plaque Instability and Stroke Recurrence in Intracranial Atherosclerotic Stenosis
Authors Wu XB ![]() , Guo X, Liu CC, Liu YA, Huang ZR, Huang LX
, Guo X, Liu CC, Liu YA, Huang ZR, Huang LX ![]() , Li QJ, Xu HX, Luo B, Wang SW
, Li QJ, Xu HX, Luo B, Wang SW
Received 5 November 2025
Accepted for publication 27 January 2026
Published 4 February 2026 Volume 2026:19 577715
DOI https://doi.org/10.2147/JIR.S577715
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ning Quan
Xiao-Bing Wu,1,2,* Xin Guo,1,2,* Chi-Chen Liu,1,2,* Yi-Ao Liu,2 Zhong-Run Huang,1 Li-Xin Huang,3 Qing-Jian Li,4 Hui-Xin Xu,4 Bin Luo,2 Sheng-Wen Wang1
1Department of Neurosurgery, Sun Yat-Sen Memorial Hospital, Sun Yat-Sen University, Guangzhou, People’s Republic of China; 2Department of Neurosurgery, The Eighth Affiliated Hospital, Sun Yat-sen University, Shenzhen, People’s Republic of China; 3Department of Neurosurgery, The Third Affiliated Hospital, Sun Yat-Sen University, Guangzhou, People’s Republic of China; 4Department of Oncology, Sun Yat-sen Memorial Hospital, Sun Yat-sen University, Guangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Bin Luo, Department of Neurosurgery, The Eighth Affiliated Hospital, Sun Yat-Sen University, 3025 Shennan Middle Road, Shenzhen, 518033, People’s Republic of China, Email [email protected] Sheng-Wen Wang, Department of Neurosurgery, Sun Yat-sen Memorial Hospital, Sun Yat-sen University, 107 Yanjiang West Road, Guangzhou, Guangdong, 510120, People’s Republic of China, Email [email protected]
Background and Purpose: While our previous cross-sectional study linked the lymphocyte-to-monocyte ratio (LMR) to symptomatic ICAS and plaque inflammation, its prospective value for predicting stroke recurrence remained unexplored. This study aimed to validate the association between LMR and plaque instability in a larger cohort and, critically, to determine whether baseline LMR predicts future ischemic events.
Methods: We prospectively enrolled adult patients with radiologically confirmed ICAS from April 2018 to July 2024 at our tertiary cerebrovascular center. Comprehensive datasets, including clinical characteristics, laboratory markers (LMR and full inflammatory profiles), and neuroimaging features, were systematically collected and analyzed. Hematologic markers were compared between patients with ICAS with and without plaque enhancement and between those with and without symptoms. Receiver operating characteristic analysis was used to assess the discriminative value of LMR for plaque instability and determine optimal cutoff points. A follow-up was conducted to record stroke recurrence and evaluate the predictive role of baseline LMR.
Results: We included 132 patients with confirmed ICAS. LMR emerged as an independent predictor of both plaque enhancement and symptomatic ICAS. An LMR cutoff of 4.0 effectively distinguished symptomatic from asymptomatic plaques. In 120 patients with ICAS with follow-up data, those with LMR of ≤ 4.0 had significantly higher recurrence (32.1% vs 15.6%, P = 0.026) and shorter median recurrence time (P = 0.049) than those with an LMR of > 4.0. Kaplan–Meier analysis showed a significantly lower recurrence-free survival rate in the LMR ≤ 4.0 group than in the LMR > 4.0 group (P = 0.011).
Conclusion: A low LMR is associated with plaque instability in ICAS, and an LMR ≤ 4.0 may serve as a practical and accessible hematologic marker that could help identify patients at increased short-term risk of stroke recurrence.
Keywords: intracranial atherosclerotic stenosis, lymphocyte-to-monocyte ratio, plaque enhancement, plaque instability, follow up, recurrence
Introduction
Intracranial atherosclerotic stenosis (ICAS) is a predominant etiology of ischemic stroke, particularly in China where it accounts for nearly half of all cases.1–3 Neurovascular inflammation is now recognized as a central driver of this disease, promoting plaque destabilization and ultimately precipitating clinical events.4,5 While high-resolution vessel wall imaging (HR-VWI) can directly visualize these unstable, inflamed plaques through gadolinium enhancement—a hallmark of macrophage infiltration and neovascularization6–9—its clinical utility in routine practice is hampered by limited accessibility and high cost.
This diagnostic gap underscores an urgent need for readily available and inexpensive biomarkers. In this context, circulating inflammatory indices derived from routine complete blood counts, such as the lymphocyte-to-monocyte ratio (LMR), offer a promising alternative.10–13 These standardized, low-cost metrics provide a unique window into the systemic inflammatory state.
Building on our preliminary findings in a cohort of 86 patients, which linked an LMR ≤ 4.0 to symptomatic ICAS and plaque enhancement on HR-VWI,14 the present study seeks to rigorously validate these associations in a larger sample. Furthermore, we aim to extend these findings by investigating the critical, yet unconfirmed, prognostic utility of a baseline LMR ≤ 4.0 in predicting future ischemic events. We hypothesize that this easily measurable ratio, reflecting a underlying systemic immunoinflammatory imbalance, serves as a surrogate for local plaque instability and a robust predictor of clinical recurrence.
Materials and Methods
Study Population and Data Collection
We identified 186 consecutive patients with ICAS from our institutional database between April 2018 and July 2024. The inclusion criteria were radiographic confirmation of ICAS by either magnetic resonance angiography (MRA) or digital subtraction angiography (DSA). All enrolled patients subsequently underwent HR-VWI as a part of the standardized protocol. We systematically collected comprehensive clinical data, including demographic characteristics (such as age and sex), vascular risk factors (such as hypertension and diabetes mellitus), and lifestyle factors (such as current smoking status and alcohol-consumption patterns).
The participants were required to meet all of the following conditions: (1) age ≥18 years; (2) high-quality HR-VWI images without significant artifacts; (3) radiologically confirmed ICAS by either DSA or MRA. The patients were excluded based on the following considerations: (1) vascular abnormalities: significant extracranial stenosis (>50%) of internal carotid or vertebral arteries; non-atherosclerotic vasculopathies (eg, intracranial arteritis, arterial dissections, moyamoya disease); (2) cardiovascular comorbidities: coronary artery disease and other significant cardiac pathologies; (3) neurological history: as a previous acute ischemic stroke, intracranial arterial occlusion, or intracerebral hemorrhage; (4) systemic conditions: active or chronic infections, malignancies, autoimmune disorders, hematologic diseases, severe systemic illnesses, or renal dysfunction (eGFR <60 mL/min/1.73 m2); (5) Procedural factors: major surgery within the preceding 6 months and incomplete imaging or laboratory data.
Laboratory Measurements
Blood samples were collected via venipuncture within 24 h of hospital admission and processed using standardized protocols. Hematological analysis was performed on the Sysmex XN-9000 automated hematology analyzer (Kobe, Japan). The measured parameters included complete blood count (white blood cells, neutrophils, lymphocytes, monocytes, platelets) and derived inflammatory indices, calculated as follows:
NLR = neutrophil count/lymphocyte count, LMR = lymphocyte count/monocyte count, SII = platelet count × neutrophil count/lymphocyte count. Biochemical analysis was conducted using the Vitros 5,1 FS Clinical Chemistry System (Ortho Clinical Diagnostics). The quantified metabolic markers included lipid profile (total cholesterol, triglycerides, HDL, LDL), apolipoprotein E, and high-sensitivity C-reactive protein (hsCRP).
Imaging Protocol and Analysis
All enrolled patients with ICAS underwent standardized gadolinium-enhanced HR-VWI at baseline using a 3.0 Tesla MRI system. The detailed scanning parameters of VWI are provided in the Supplementary Material 1. Scanning parameters of HR-VWI. DSA was performed on the Philips Allura Xper FD20 machine with a nonionic contrast agent. Raw data were transferred to syngo X Workplace for 3D rotational reconstruction and optimal working angle determination. The degree of stenosis was based on the following formula: [1- (Dstenosis/Dnormal)] × 100%.15
ICAS plaques were radiologically defined by demonstrating focal vessel wall thickening, with consistent visualization on both non-contrast and post-contrast enhanced HR-VWI sequences.16 Plaque enhancement was strictly defined as a visible signal intensity increase on the T1 sequences after 5 min of gadolinium administration (0.1 mmol/kg). Plaque burden was quantified at the site of maximal stenosis using the following standardized formula: Plaque burden (%) = [1 - (lumen area/vessel area)] × 100%.17,18
Diffusion-weighted imaging and FLAIR sequences were utilized to precisely localize acute/subacute infarcts. A plaque was considered symptomatic if it was the only lesion within the ipsilateral territory of the ischemic stroke or it was the most stenotic plaque among multiple plaques within the same territory of an ischemic event, and a transient ischemic attack was not regarded as symptomatic. A plaque was defined as asymptomatic if it was not within the vascular distribution of stroke.19,20
Follow-up Protocol
We implemented a standardized prospective follow-up protocol with scheduled assessments at 3, 6, and 12 months after discharge, followed by annual evaluations thereafter. Follow-up procedures were conducted through either structured telephone interviews or in-person clinical visits during hospital readmissions. Following the acquisition of informed consent from participants or their legal guardians, comprehensive follow-up assessments were performed, including the following: (1) stroke event surveillance: documentation of any new or recurrent ischemic stroke events; precise recording of the symptom onset dates. (2) Treatment adherence monitoring:
Verification of continuous standard medication use (antiplatelet agents and lipid-lowering therapy). (3) Functional status evaluation: Assessment of self-care capacity and formal modified Rankin Scale (mRS) scoring. For patients readmitted with recurrent stroke, complete laboratory data were systematically collected.
Ischemic stroke recurrence was rigorously defined as either: worsening of pre-existing neurological deficits or the emergence of new stroke-related symptoms (including but not limited to dysarthria, limb weakness, or visual disturbances), or stroke-related mortality. Patients meeting any predefined exclusion criteria during the follow-up were systematically withdrawn from subsequent analyses so as to maintain cohort integrity.
Statistical Analysis
Continuous variables are presented as the mean ±standard deviation or medians (min-max), which were compared using Student’s t-test or the Mann–Whitney U-test. Categorical variables were expressed as the number of cases and percentages and compared using Fisher’s exact or chi-square test.
Univariate analyses of clinical, laboratory, and imaging data of ICAS patients without and with plaque enhancement, and then between symptomatic ICAS and asymptomatic ICAS, were performed to identify factors associated with plaque enhancement and symptomatic plaques. Factors independently associated with ICAS plaque enhancement and symptomatic plaques were determined by forward multivariate logistic regression analyses after adjusting for variables with P < 0.05 in the univariate comparisons. Furthermore, receiver operating characteristic analysis was performed to determine the optimal cutoff value of the LMR to differentiate symptomatic plaques from asymptomatic plaques. A prospective follow-up analysis was conducted to monitor ischemic stroke recurrence rates and assess LMR’s predictive value for clinical outcomes. SPSS 23.0 software (SPSS Inc., Chicago, Illinois) was used for the statistical analysis of the data. Two-tailed P < 0.05 was considered to indicate statistical significance.
Results
Patient Characteristics
This study included 132 patients with ICAS [mean age: 59.9 ±10.4 years; 77 (58.3%) males and 55 females (41.7%)]. All participants underwent both HR-VWI and diffusion-weighted imaging scans. Of the plaques assessed, 88 showed enhancement and 44 did not; 81 patients had symptomatic ICAS, while 51 were asymptomatic. Follow-up data were obtained for 120 patients, while 12 were lost to follow-up. The median follow-up duration was 22 months (interquartile range: 14–53 months). Detailed baseline characteristics are presented in Tables 1 and 2.
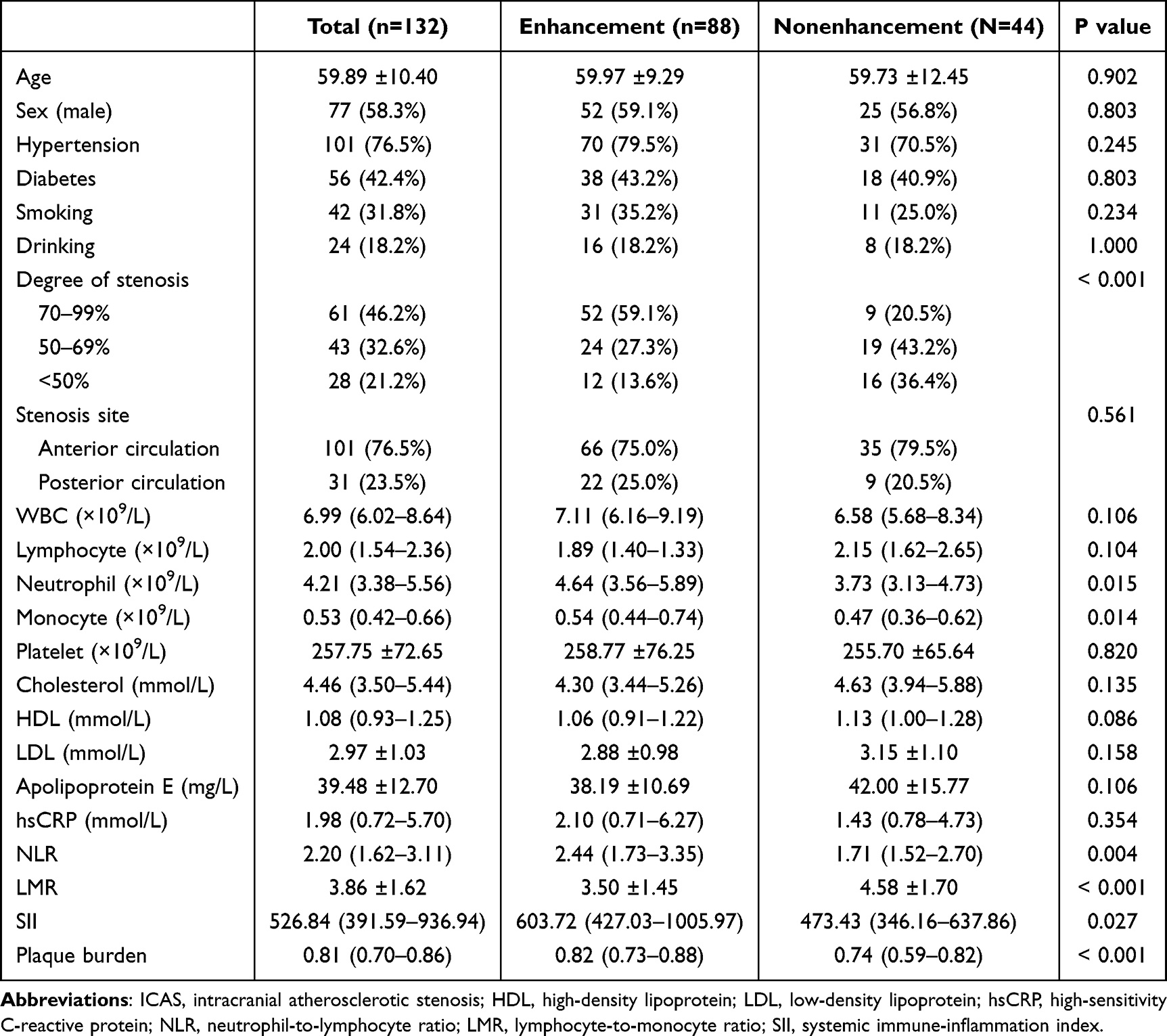 |
Table 1 Characteristics of ICAS Atherosclerotic Plaques Without and with Enhancement |
 |
Table 2 Characteristics of ICAS Plaques Without and with Symptoms |
LMR as an Independent Predictor of Plaque Enhancement and Symptomatic ICAS
Plaque enhancement was significantly associated with greater stenosis severity, increased plaque burden, and elevated levels of NLR and SII (Table 1). Symptomatic ICAS was more frequent in patients with hypertension, higher plaque enhancement rates, more severe stenosis, and elevated high-sensitivity C-reactive protein and NLR levels (Table 2). Multivariate logistic regression analysis identified LMR as an independent risk factor for both symptomatic ICAS (odds ratio: 0.718; 95% confidence interval: 0.546–0.944; P = 0.018) (Table 3) and plaque enhancement (odds ratio: 0.703; 95% confidence interval: 0.539–0.918; P = 0.010) (Supplementary Table 1).
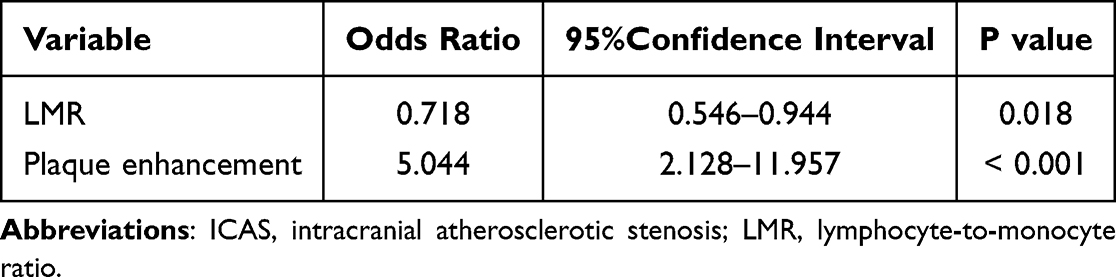 |
Table 3 Forward Multiple Logistic Regression Analysis of Symptomatic ICAS |
Prognostic Utility of LMR ≤ 4.0 for Plaque Instability
The receiver operating characteristic curve revealed that an LMR cutoff of 4.0 distinguished symptomatic from asymptomatic ICAS, with a sensitivity of 72.8%, a specificity of 60.8%, and an area under the curve of 0.698 (P = 0.001) (Figure 1). Among the 120 patients with complete follow-up, those with an LMR of ≤4.0, an independent predictor of stroke recurrence (Supplementary Table 2), experienced significantly higher stroke recurrence (32.1% vs 15.6%, P = 0.026) and a shorter median recurrence interval (P = 0.049) than those with an LMR of >4.0 (Table 4). In addition, positive correlation between baseline LMR and HDL was showed (Supplementary Table 3). The sensitivity and specificity of baseline LMR of ≤ 4.0 for identifying symptomatic ICAS were 74.6% and 57.1%, respectively. For predicting recurrent stroke during follow-up, the sensitivity and specificity were 26.8% and 89.8%, respectively (Supplementary Table 4). Kaplan–Meier survival analysis (Figure 2) demonstrated significantly reduced recurrence-free survival in the LMR ≤ 4.0 group compared with the LMR > 4.0 group (P = 0.011).
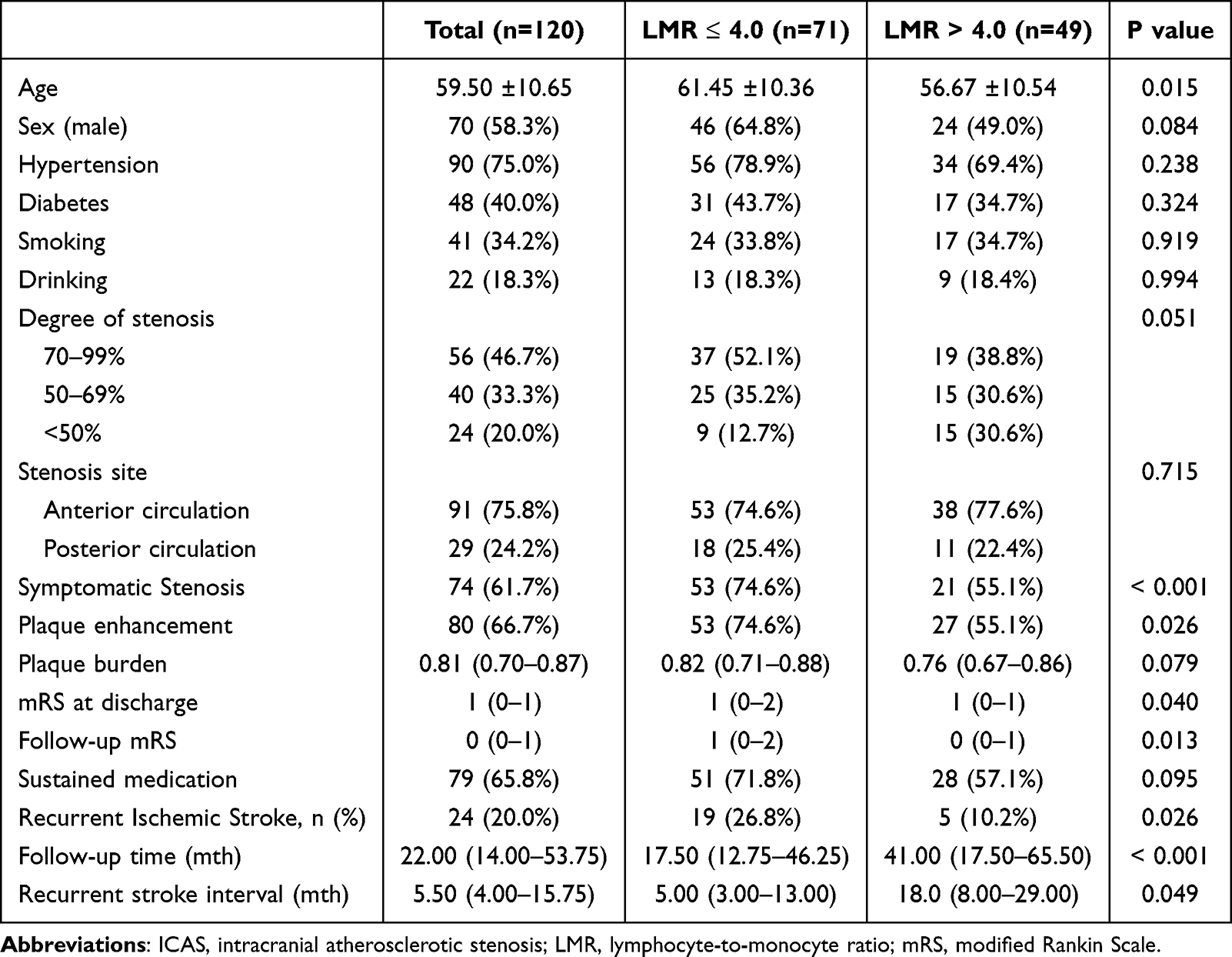 |
Table 4 Characteristics of ICAS Patients with LMR ≤ 4.0 and LMR > 4.0 |
 |
Figure 1 ROC curve for determining the presence of symptomatic stenosis. The AUC of LMR was 0.698 (95% CI: 0.604–0.793, P < 0.001). The sensitivity was 72.8%, and the specificity was 60.8%. |
 |
Figure 2 Kaplan–Meier estimate for recurrence of ischemic stroke according to LMR ≤ 4.0 evolution over time. ICAS patients presenting with LMR ≤ 4.0 (blue line) have a greater risk of recurrence than those with LMR > 4.0 (red line) (P = 0.011). |
Discussion
For the first time, our longitudinal data confirm that baseline LMR, a convenient indicator of systemic immune-inflammatory balance, independently predicts stroke recurrence in ICAS patients. This discovery provides a novel clinical evidence for targeting neurovascular inflammation in secondary stroke prevention.
Following the expansion of the sample size, our analysis confirmed that low LMR consistently retained its independent predictive value for both plaque enhancement and symptomatic patients with ICAS. In addition, baseline LMR was negatively correlated with plaque burden and the degree of stenosis. A low LMR, characterized by lymphopenia and monocytosis, signifies a pro-inflammatory state. In this state, increased monocytes infiltrate the vascular wall and differentiate into macrophages, driving local inflammation, while concurrent lymphocytopenia—particularly the loss of regulatory T cells—compromises anti-inflammatory responses and immune stability. The observed correlation between low LMR and plaque enhancement serves as a validating link, strongly supporting the notion that peripheral immune cell ratios can faithfully reflect the local inflammatory activity of intracranial plaques. Notably, the optimal cutoff of LMR ≤ 4.0 for distinguishing symptomatic ICAS aligned with our earlier findings,14 reinforcing the reproducibility of this marker across patient populations. The prognostic relevance of LMR also extends beyond ICAS. LMR is an independent predictor of unfavorable short-term outcomes in acute ischemic stroke;21 an LMR of < 3.24 correlates with early neurological deterioration in acute ischemic stroke.22 Additionally, an LMR of ≤ 4.8 has been linked to the presence and burden of coronary artery disease.23 The combined cross-sectional and longitudinal analyses suggest that an LMR ≤ 4.0 may serve as a practical and inexpensive hematologic marker linked to ICAS plaque instability. Although it offers only moderate predictive accuracy, this easily obtained ratio could aid in identifying a subset of patients at elevated risk of recurrent ischemic stroke. Its value may be enhanced when combined with other biomarkers and imaging parameters in future predictive models.
A growing body of evidence highlights the central role of inflammation in ICAS plaque formation and destabilization. HR-VWI studies demonstrate that plaques enhanced with gadolinium typically exhibit histopathological features of local inflammation, including macrophage accumulation and neovascularization.24 These enhancement patterns are now established as reliable imaging markers of unstable plaques.25,26 In our study, patients with symptomatic ICAS exhibited significantly higher levels of peripheral inflammatory markers than their asymptomatic counterparts (P < 0.01), supporting the systemic inflammatory contribution to plaque progression. Furthermore, both HR-VWI plaque enhancement and low LMR were identified as independent predictors of symptomatic ICAS. This imbalance of immune cells leads to the instability of plaques, resulting in an increased proportion of ischemic strokes. Additional circulating biomarker, like IL-6, was also reported to be associated with plaque instability.27 This is consistent with the core findings of previous study.28 Findings from the CANTOS trial29 further strengthen this perspective, showing that anti-inflammatory therapy significantly reduced cardiovascular event rates independently of lipid-lowering interventions. These results suggest that elevated local and systemic inflammatory activity underlies plaque instability and we contend that identifying these high-risk immunoinflammatory phenotypes in ICAS patients should therefore be a priority for guiding future trials of personalized anti-inflammatory treatment.
This study found a significant positive correlation between baseline LMR and HDL. Contrary to previous reports linking dyslipidemia to ICAS plaque enhancement,30 our findings revealed no significant association between dyslipidemia and either plaque enhancement or symptomatic ICAS. This discrepancy may reflect stricter exclusion criteria in our study design, statin use among certain patients before enrollment, or ethnic variation among study populations.
Therefore, our findings should be interpreted as preliminary and hypothesis-generating, and the possible mechanism diagram of stroke recurrence is shown in Supplementary Figure 1. This study serves as a stepping stone toward larger, multicenter studies that will be needed to validate the LMR threshold and to develop integrated multiparameter risk-prediction models.
Nonetheless, our study has several methodological limitations. First, as a single-center study, it is subject to selection bias and wide CIs, and this may limit external generalizability. Second, despite stringent exclusion criteria, unrecognized subclinical infections at baseline may have influenced inflammatory marker values. Third, only baseline LMR was used to evaluate recurrent events, although inflammation is clearly implicated in plaque instability, the precise biological mechanisms underlying LMR’s independent association remain unclear. Inconsistent significance among inflammatory markers may reflect differences in biomarker sensitivity, involvement of distinct immune pathways, or immune cell ratio threshold effects. Lastly, the study did not assess dynamic changes in LMR during follow-up in relation to stroke recurrence, which warrants exploration in future research.
Conclusion
This study provides preliminary evidence that a low LMR, particularly when ≤ 4.0, is associated with plaque instability and an increased risk of stroke recurrence in patients with ICAS. It suggests that LMR may serve as a readily accessible biomarker for identifying high-risk individuals, Future studies should investigate dynamic changes in LMR over time and its integration with other clinical and imaging markers to better stratify recurrence risk.
Data Sharing Statement
The data supporting the funding of this study are available from the corresponding author upon request.
Ethics Approval and Consent to Participate
The studies involving human participants were in accordance with the Declaration of Helsinki and reviewed and approved by Sun Yat-sen Memorial Hospital (SYSKY-2025-784-01). The patients/participants provided their written informed consent to participate in this study.
Author Contributions
Xiao-Bing Wu: Conceptualization, Data curation, Formal analysis, and Writing – original draft. Xin Guo: Data curation, Investigation, Writing – original draft. Chi-Chen Liu: Methodology, Visualization, Writing – original draft. Yi-Ao Liu: Investigation, Resources, Writing – review & editing. Zhong-Run Huang: Validation, Project administration, Writing – review & editing. Li-Xin Huang: Resources, Supervision, Writing – review & editing. Qing-Jian Li: Software, Validation, Writing – review & editing. Hui-Xin Xu: Conceptualization, Supervision, Writing – review & editing. Bin Luo: Conceptualization, Funding acquisition, Supervision, Writing – review & editing. Sheng-Wen Wang: Conceptualization, Methodology, Funding acquisition, Supervision, Writing – review & editing. All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the National Administration of Traditional Chinese Medicine Foundation of China (No. CXZH202404015), the National Administration of Traditional Chinese Medicine Foundation of China (ZXYXTMBGLA3-4), the National Natural Science Foundation of China project (81901339), the National Natural Science Foundation of China project (82203086), and the Guangdong Basic and Applied Basic Research Foundation, project (2023A1515010916).
Disclosure
The authors declare that they have no competing interests.
References
1. Gutierrez J, Turan TN, Hoh BL, et al. Intracranial atherosclerotic stenosis: risk factors, diagnosis, and treatment. Lancet Neurol. 2022;21(4):355–10. doi:10.1016/S1474-4422(21)00376-8
2. Tjoumakaris SI, Roy JM, Amin-Hanjani S, et al. ARISE II consensus on the management of intracranial atherosclerotic disease. Stroke. 2025;56(6):1636–1641. doi:10.1161/STROKEAHA.124.050336
3. Wang Y, Zhao X, Liu L, et al. Prevalence and outcomes of symptomatic intracranial large artery stenoses and occlusions in China: the Chinese intracranial atherosclerosis (CICAS) study. Stroke. 2014;45(3):663–669. doi:10.1161/STROKEAHA.113.003508
4. Mo J, Liu X, Zhang H, et al. Inflammatory burden index and one-year clinical outcomes in large artery atherosclerosis ischemic stroke: a multicenter prospective study. Eur J Neurol. 2025;32(6):e70242. doi:10.1111/ene.70242
5. Wu XB, Liu YA, Huang LX, et al. Hemodynamics combined with inflammatory indicators exploring relationships between ischemic stroke and symptomatic middle cerebral artery atherosclerotic stenosis. Eur J Med Res. 2023;28(1):378. doi:10.1186/s40001-023-01344-8
6. Huang LX, Wu XB, Liu YA, et al. Qualitative and quantitative plaque enhancement on high-resolution vessel wall imaging predicts symptomatic intracranial atherosclerotic stenosis. Brain Behav. 2023;13(6):e3032. doi:10.1002/brb3.3032
7. Yu Y, Cui R, He X, et al. Residual inflammatory risk and intracranial atherosclerosis plaque vulnerability: insights from high-resolution magnetic resonance imaging. J Stroke. 2025;27(2):207–216. doi:10.5853/jos.2024.03251
8. Zheng W, Yan H, Tian D, et al. Plaque enhancement of middle cerebral artery and pre-stroke diet are associated with prognosis of subacute ischemic stroke: a prospective high-resolution MR vessel wall imaging study. Eur J Radiol. 2024;180:111693. doi:10.1016/j.ejrad.2024.111693
9. Hur J, Park J, Kim YJ, et al. Use of contrast enhancement and high-resolution 3D black-blood MRI to identify inflammation in atherosclerosis. JACC Cardiovasc Imaging. 2010;3(11):1127–1135. doi:10.1016/j.jcmg.2010.08.012
10. Aly M, Abdalla RN, Batra A, et al. Follow-up neutrophil-lymphocyte ratio after stroke thrombectomy is an independent biomarker of clinical outcome. J Neurointerv Surg. 2021;13(7):609–613. doi:10.1136/neurintsurg-2020-016342
11. Li S, Liu K, Zhang R, et al. Lower lymphocyte to monocyte ratio is a potential predictor of poor outcome in patients with cerebral venous sinus thrombosis. Stroke Vasc Neurol. 2018;4(3):148–153. doi:10.1136/svn-2018-000180
12. Gong P, Liu Y, Gong Y, et al. The association of neutrophil to lymphocyte ratio, platelet to lymphocyte ratio, and lymphocyte to monocyte ratio with post-thrombolysis early neurological outcomes in patients with acute ischemic stroke. J Neuroinflammation. 2021;18(1):51. doi:10.1186/s12974-021-02090-6
13. Liao B, Xu Q, Lu P, Zhang Y. The prognostic value of systemic immune-inflammation index in patients with aneurysmal subarachnoid hemorrhage: a systematic review. Neurosurg Rev. 2023;46(1):219. doi:10.1007/s10143-023-02133-x
14. Wu XB, Huang LX, Huang ZR, et al. The lymphocyte-to-monocyte ratio predicts intracranial atherosclerotic stenosis plaque instability. Front Immunol. 2022;13:915126. doi:10.3389/fimmu.2022.915126
15. Samuels OB, Joseph GJ, Lynn MJ, Smith HA, Chimowitz MI. A standardized method for measuring intracranial arterial stenosis. AJNR Am J Neuroradiol. 2000;21(4):643–646.
16. Yang H, Ji C, Wang H, et al. Characterisation of symptomatic intracranial plaque without substantial stenosis using high-resolution vessel wall MRI. Clin Radiol. 2021;76(5):392.e21–e26. doi:10.1016/j.crad.2021.01.008
17. Yuan W, Liu X, Yan Z, et al. Association between high-resolution magnetic resonance vessel wall imaging characteristics and recurrent stroke in patients with intracranial atherosclerotic steno-occlusive disease: a prospective multicenter study. Int J Stroke. 2024;19(5):569–576. doi:10.1177/17474930241228203
18. Sanchez S, Raghuram A, Fakih R, et al. 3D enhancement color maps in the characterization of intracranial atherosclerotic plaques. AJNR Am J Neuroradiol. 2022;43(9):1252–1258. doi:10.3174/ajnr.A7605
19. Shi Z, Li J, Zhao M, et al. Quantitative histogram analysis on intracranial atherosclerotic plaques: a high-resolution magnetic resonance imaging study. Stroke. 2020;51(7):2161–2169. doi:10.1161/STROKEAHA.120.029062
20. Tian X, Shi Z, Wang Z, et al. Characteristics of culprit intracranial plaque without substantial stenosis in ischemic stroke using three-dimensional high-resolution vessel wall magnetic resonance imaging. Front Neurosci. 2023;17:1160018. doi:10.3389/fnins.2023.1160018
21. Zhang YX, Shen ZY, Jia YC, et al. The association of the neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio, lymphocyte-to-monocyte ratio and systemic inflammation response index with short-term functional outcome in patients with acute ischemic stroke. J Inflamm Res. 2023;16:3619–3630. doi:10.2147/JIR.S418106
22. Sun L, Ye X, Yu J, et al. Peripheral lymphocyte-to-monocyte ratio as a predictive factor for early neurological deterioration in patients with acute ischemic stroke. Int J Gen Med. 2024;17:4397–4405. doi:10.2147/IJGM.S483064
23. Si Y, Liu J, Shan W, et al. Association of lymphocyte-to-monocyte ratio with total coronary plaque burden in patients with coronary artery disease. Coron Artery Dis. 2020;31(7):650–655. doi:10.1097/MCA.0000000000000857
24. Millon A, Boussel L, Brevet M, et al. Clinical and histological significance of gadolinium enhancement in carotid atherosclerotic plaque. Stroke. 2012;43(11):3023–3028. doi:10.1161/STROKEAHA.112.662692
25. Shi X, Tao T, Ling H, et al. High-risk plaque characteristics associated with recurrent stroke in patients with intracranial stenosis: a systematic review and meta-analysis. J Neurol. 2025;272(2):173. doi:10.1007/s00415-025-12924-5
26. Huang J, Liu C, Jiao S, et al. Application of high-resolution MRI in evaluating statin efficacy on symptomatic intracranial atherosclerosis. Eur Radiol. 2025;35(1):441–452. doi:10.1007/s00330-024-10968-1
27. Schieffer B, Schieffer E, Hilfiker-Kleiner D, et al. Expression of angiotensin II and interleukin 6 in human coronary atherosclerotic plaques: potential implications for inflammation and plaque instability. Circulation. 2000;101(12):1372–1378. doi:10.1161/01.cir.101.12.1372
28. Sharma M, Schlegel MP, Afonso MS, et al. Regulatory T cells license macrophage pro-resolving functions during atherosclerosis regression. Circ Res. 2020;127(3):335–353. doi:10.1161/CIRCRESAHA.119.316461
29. Ridker PM, Everett BM, Thuren T, et al. Antiinflammatory therapy with Canakinumab for atherosclerotic disease. N. Engl J Med. 2017;377(12):1119–1131. doi:10.1056/NEJMoa1707914
30. Woo NE, Na HK, Heo JH, et al. Factors for enhancement of intracranial atherosclerosis in high resolution vessel wall MRI in ischemic stroke patients. Front Neurol. 2020;11:580. doi:10.3389/fneur.2020.00580
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Preoperative Inflammation-Associated Blood Cell Markers in Patients with Non-Metastatic Clear Cell Renal Cell Carcinoma: A Retrospective Study
Cheng Y, Kou W, Zhu Y
International Journal of General Medicine 2023, 16:3067-3080
Published Date: 19 July 2023