Back to Journals » Drug Design, Development and Therapy » Volume 19
Low-Dose Esketamine Plus Dexmedetomidine in Patient-Controlled Intravenous Analgesia Improves Post-Cesarean Sleep Quality: A Double-Blind Randomized Trial
Authors Zhang L, He Y, Chen L, Liu X, Zhang T, Zhou X, Mao W, Zhao L ![]() , Li L, Xie Y
, Li L, Xie Y
Received 26 July 2025
Accepted for publication 23 October 2025
Published 4 November 2025 Volume 2025:19 Pages 9789—9796
DOI https://doi.org/10.2147/DDDT.S556396
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Longyi Zhang,* Yunzi He,* Linlin Chen, Xianchun Liu, Ting Zhang, Xuelei Zhou, Wei Mao, Li Zhao, Linji Li, Ying Xie
Department of Anesthesiology, Beijing Anzhen Nanchong Hospital (Nanchong Central Hospital), The Second Clinical Medical College, North Sichuan Medical College, Nanchong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ying Xie, Department of Anesthesiology, Beijing Anzhen Nanchong Hospital (Nanchong Central Hospital), The Second Clinical Medical College, North Sichuan Medical College, Nanchong, People’s Republic of China, Email [email protected]
Purpose: Postoperative sleep disturbance can hinder recovery after cesarean section. Although either esketamine or dexmedetomidine alone has been shown to improve sleep quality, their combined use in patient-controlled intravenous analgesia (PCIA) has not been well studied. This study aimed to evaluate whether adding dexmedetomidine to esketamine in PCIA could further enhance postoperative sleep quality in women after cesarean delivery.
Patients and Methods: In this randomized trial, 105 women receiving PCIA were assigned to control (C), esketamine (E), or esketamine-dexmedetomidine (ED) groups. The primary outcome was the Richards-Campbell Sleep Questionnaire (RCSQ) score on postoperative day 1 (POD1). Secondary outcomes included pain Numerical Rating Scale (NRS) scores, Ramsay sedation scores, RCSQ on POD2– 3, Hospital Anxiety and Depression Scale (HADS) scores, analgesic demands, and adverse events.
Results: On POD1, the RCSQ scores were significantly higher in both the Group E (43.5 ± 17.2; mean difference = 11.6; 95% CI, 4.8– 18.6; P = 0.008) and the Group ED (52.6 ± 11.5; mean difference = 20.7; 95% CI, 13.9– 27.6; P < 0.001) compared with the Group C (31.9 ± 14.2). The Group ED also showed a greater improvement in sleep quality than the Group E (mean difference = 9.1; 95% CI, 2.2– 15.9; P = 0.032). Both intervention groups had lower resting NRS scores and fewer PCIA demands than the control group. No significant differences were found among the three groups regarding adverse events or other secondary outcomes.
Conclusion: Low-dose esketamine combined with dexmedetomidine in PCIA effectively improved postoperative sleep quality and pain relief after cesarean section, proving to be a safe and effective analgesic adjunct.
Keywords: esketamine, cesarean section, patient-controlled intravenous analgesia, dexmedetomidine, sleep quality
Introduction
Cesarean section is among the most frequently performed surgical procedures.1 However, postoperative pain and stress often lead to sleep disturbances—an underrecognized yet critical factor that may impair maternal recovery and quality of life.2–4
Esketamine, an N-methyl-D-aspartate (NMDA) receptor antagonist, has been shown to improve postoperative sleep quality and reduce pain when administered via infusion.5–10 Emerging evidence indicates that its sleep-promoting effects may involve enhancement of slow-wave sleep (N3) and modulation of sleep architecture, potentially mediated through upregulation of brain-derived neurotrophic factor (BDNF), a key regulator of synaptic plasticity also linked to its rapid antidepressant action.11
Dexmedetomidine, a highly selective α2-adrenergic receptor agonist, has been shown in electroencephalographic studies to induce a sleep-like state closely resembling physiological non-rapid eye movement (NREM) sleep.12–14 When administered via patient-controlled intravenous analgesia (PCIA), its stable and continuous delivery enhances sleep quality and alleviates depressive symptoms in postpartum women, outperforming bolus or intraoperative infusions.15 Moreover, dexmedetomidine may mitigate esketamine-induced agitation and neuronal hyperexcitation. Notably, combined administration of esketamine and dexmedetomidine has been reported to further prolong total sleep time, increase the proportion of N3 sleep, and improve the continuity of deep sleep.11
However, the combined use of esketamine and dexmedetomidine in PCIA after cesarean delivery has not been evaluated, despite evidence that each agent independently improves sleep quality. Therefore, this study aimed to assess whether a low-dose PCIA regimen combining esketamine, dexmedetomidine, and sufentanil could enhance postoperative sleep quality and analgesia in women undergoing cesarean section.
Materials and Methods
This single-center, randomized, controlled trial was conducted at Nanchong Central Hospital. The study protocol was approved by the Ethics Committee of Nanchong Central Hospital on December 31, 2024 (Approval No. 2024–192) and was registered at the Chinese Clinical Trial Registry on February 6, 2025 (Registration No. ChiCTR2500096770). The trial was conducted in accordance with the ethical principles of the Declaration of Helsinki. Written informed consent was obtained from all participants prior to enrollment.
Study Population
This study enrolled postpartum women who met the following criteria: full-term singleton pregnancy, planned cesarean delivery under spinal anesthesia, ASA physical status I–II, and age 20–45 years. Exclusion criteria included severe systemic disease, gestational diabetes, hypertension, relevant drug allergies or contraindications, psychiatric disorders, communication or cognitive impairment, patient refusal, history of substance abuse (opioids, sedatives, or psychotropic drugs), preoperative heart rate <50 beats/min, or systolic blood pressure <100 mmHg. Participants were withdrawn in cases of inadequate intraoperative analgesia, major intraoperative complications, deviation from the planned anesthetic or surgical procedure, or postoperative loss to follow-up.
Randomization and Masking
An independent physician generated the random allocation sequence via SPSS 25.0 using block randomization with a block size of 6 and a 1:1:1 allocation ratio. Participants were randomly assigned to one of three groups: control (Group C), esketamine (Group E), or esketamine–dexmedetomidine (Group ED). No stratification was applied. Allocation concealment was ensured using sequentially numbered, opaque envelopes prepared by an independent staff member. On the day of surgery, an anesthesiologist opened the envelopes sequentially to prepare the assigned interventions. All study medications were identical in appearance and volume and were uniformly labeled as “intervention drug” to maintain blinding. This anesthesiologist took no part in data collection or postoperative assessments. Patients, surgeons, and outcome assessors remained blinded throughout the study.
Study Intervention
All participants were instructed to fast for 8 hours preoperatively. Upon entering the operating room, they underwent standard electrocardiographic monitoring and received supplemental oxygen via nasal cannula, while an upper limb intravenous line was established. Spinal anesthesia was performed with the patient in the left lateral position. A spinal puncture was conducted at the L2–L3 or L3–L4 intervertebral space, and upon confirmation of cerebrospinal fluid flow, 2 mL of 0.5% bupivacaine was slowly administered. Following drug administration, the patient was placed in the supine position with a 15°–30° leftward tilt of the operating table Surgery commenced once the anesthetic level reached the T6–T8 dermatome. Vasoactive agents, including phenylephrine or ephedrine, were administered as needed to maintain hemodynamic stability.
Following fetal delivery and umbilical cord clamping, PCIA was initiated using the following group-specific regimens, each diluted to 100 mL with normal saline: Group C received sufentanil (2 μg/kg) and ramosetron (0.9 mg); Group E received esketamine (0.5 mg/kg), sufentanil (2 μg/kg), and ramosetron (0.9 mg); and Group ED received esketamine (0.5 mg/kg), dexmedetomidine (1 μg/kg), sufentanil (2 μg/kg), and ramosetron (0.9 mg). The PCIA pump delivered a continuous background infusion at 2 mL/h, with a patient-controlled bolus of 2 mL and a 15-minute lockout interval. Based on this infusion rate and total volume, the continuous dosage approximated 0.01 mg/kg/h of esketamine and 0.02 μg/kg/h of dexmedetomidine in Group ED.
Rescue analgesia (50 mg diclofenac sodium suppository) was administered rectally if participants reported a resting NRS score ≥4 or a movement/coughing NRS score ≥6 with inadequate pain control via PCIA. Repeat administration was permitted at minimum 12-hour intervals. No intraoperative sedatives or analgesics were administered before surgery completion. Requirement for additional sedation or analgesia during the procedure resulted in study exclusion.
Outcomes
Baseline demographic and clinical characteristics were collected, including maternal age, gestational age, height, weight, body mass index (BMI), surgical duration, education level, parity, and neonatal parameters. Preoperative assessment included the Pittsburgh Sleep Quality Index (PSQI) for sleep quality over the preceding month and the Hospital Anxiety and Depression Scale (HADS) for anxiety and depression levels.
The primary outcome was the Richards-Campbell Sleep Questionnaire (RCSQ) score on postoperative day 1 (POD1). Secondary outcomes comprised RCSQ scores on POD2 and POD3; Numerical Rating Scale (NRS) scores for pain at rest and during movement; and Ramsay sedation scores at 6, 12, 24, 48, and 72 hours postoperatively. Additional measures included HADS scores on POD2, counts of effective and total PCIA pump presses, frequency of rescue analgesia, and incidence of adverse events. Prespecified adverse events were nausea, vomiting, dizziness, pruritus, drowsiness, respiratory depression (respiratory rate <8 breaths/min), hypotension (systolic blood pressure <90 mmHg or diastolic blood pressure <60 mmHg), and bradycardia (heart rate <60 beats/min).
Sample Size and Power
The sample size was calculated using PASS 21.0 software. The primary outcome measure was the RCSQ score on POD1. Based on preliminary pilot study results, the expected RCSQ scores were 46.1±5.8 for the Group E, 50.6±10.8 for the Group E, and 40.2±5.0 for the Group C. With a two-sided α = 0.05 and a power of 1-β = 0.9, the sample size ratio was set at 1:1:1. Taking into account a 20% loss to follow-up, 40 participants per group were required, with a total of 120 participants across the three groups.
Statistical Analysis
Data were analyzed using SPSS 25.0. Normally distributed continuous variables are presented as mean ± standard deviation (SD), and non-normally distributed variables as median (interquartile range, IQR). Homogeneity of variance was assessed using Levene’s test. For homogeneous data, one-way analysis of variance (ANOVA) with Bonferroni post-hoc testing was applied; for heterogeneous data, the Kruskal–Wallis H-test was used. Categorical variables are expressed as percentages and compared using the χ2-test or Fisher’s exact test, as appropriate.
The primary endpoint—postoperative sleep quality measured by RCSQ over the first three postoperative days—was analyzed with Bonferroni correction for multiple comparisons. The significance level was set at α = 0.05, and a two-tailed p-value < 0.05 was considered statistically significant. All analyses followed a per-protocol approach, excluding participants who were eliminated after randomization.
Results
Study Participants
The CONSORT flow diagram provides a detailed account of the number of individuals who were contacted, recruited, and randomly assigned (Figure 1). Between February and April 2025, 205 postpartum women were screened for eligibility. Of these, 25 declined to participate and 80 met exclusion criteria. The remaining 120 participants were enrolled and equally allocated to the three groups (n=40 per group). During the study period, 15 participants were excluded: 11 due to inadequate intraoperative analgesia (2 in Group C, 4 in Group E, 5 in Group ED), 1 in Group E due to massive intraoperative bleeding, and 3 in Group C due to surgical plan changes. Consequently, 105 participants completed the study and were included in the final per-protocol analysis.
 |
Figure 1 The flow diagram of the study. |
No significant differences were observed among the three groups in baseline demographic characteristics, preoperative anxiety and depression (HADS scores), sleep quality (PSQI scores), or neonatal parameters and outcomes (Supplementary Table S1).
Maternal Sleep Quality (RCSQ Scores)
On POD1, RCSQ scores were significantly higher in both Group E (43.5 ± 17.2) and Group ED (52.6 ± 11.5) compared to Group C (31.9 ± 14.2), with mean differences of 11.6 (95% CI 4.8–18.6, P = 0.008) and 20.7 (95% CI 13.9–27.6, P < 0.001), respectively. Furthermore, the Group ED demonstrated significantly better outcomes on POD1 relative to Group E, with a mean difference of 9.1 (95% CI 2.2–15.9, P = 0.032). (Figure 2). On POD2, maternal sleep quality showed further improvement in both Group E (61.1 ± 11.6; 95% CI 57.1–65.1; P = 0.02) and Group ED (62.9 ± 13.8; 95% CI 58.1–67.6; P = 0.001) compared to Group C (50.6 ± 16.2). However, no statistically significant difference was observed between Group E and Group ED (Figure 2). By POD3, both intervention groups continued to show numerically higher RCSQ scores than Group C (Group E: 63.8 ± 13.8; Group ED: 66.1 ± 13.9 vs 58.7 ± 11.4). However, these differences no longer reached statistical significance (Figure 2).
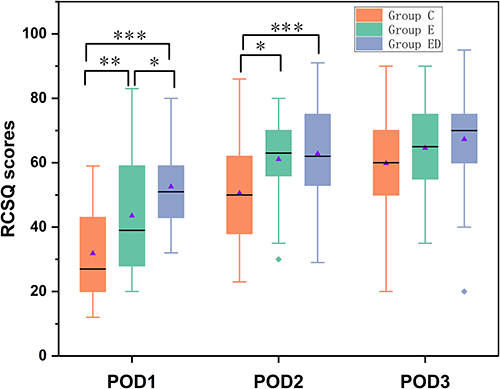 |
Figure 2 RCSQ score three days after operation. The X-axis represents postoperative days (POD1–POD3). The Y-axis represents RCSQ scores (0 = very poor sleep, 100 = excellent sleep). The boxplots display the median (center line), interquartile range (box), and minimum/maximum values (whiskers). The blue triangles represent the mean value for each group. The individual points represent values outside the range of the whiskers. *P < 0.05, **P < 0.01, ***P < 0.001. |
Component Analysis of RCSQ
On POD1, Group E showed significant improvements versus Group C in sleep latency (P = 0.013), number of awakenings (P = 0.028), and perceived sleep quality (p = 0.005). Group ED demonstrated significant enhancements across all five RCSQ domains compared to Group C (all P < 0.001). On POD2, both intervention groups exhibited significantly better sleep latency and perceived sleep quality relative to Group C. Group ED also showed a greater ability to return to sleep than Group E. By POD3, sleep latency remained shorter in both Group E and Group ED compared to Group C. The sole significant difference between Group E and Group ED was observed in sleep depth on POD1, favoring Group ED (P < 0.001) (Supplementary Table S2).
Postoperative Pain (NRS Scores)
Compared to Group C, both Group E and Group ED demonstrated significantly lower median NRS pain scores at rest at 12, 24, and 48 hours postoperatively compared to Group C(P < 0.05). No significant differences were observed among the groups at the remaining time points (Figure 3a). For NRS scores during movement, no significant differences were observed among the three groups (P >0.05) (Figure 3b).
 |
Figure 3 Postoperative pain intensity at rest and during movement over the first three days. (a) Resting pain scores. (b) Movement-evoked pain scores. The X-axis represents postoperative time points (6 h, 12 h, 24 h, 48 h, and 72 h). The Y-axis represents pain intensity assessed using the Numerical Rating Scale (NRS, 0 = no pain, 10 = worst imaginable pain). The boxplots display the median (center line), interquartile range (box), and minimum/maximum values (whiskers). *P < 0.05, **P < 0.01, ***P < 0.001. Abbreviation: NRS, Numerical Rating Scale. |
Analgesic Consumption and Other Outcomes
Compared to Group C, both Group E and Group ED demonstrated a decrease in the total number of PCIA demands and effective presses. However, the difference between Group E and Group ED did not reach statistical significance (Table 1). On POD2, no significant intergroup differences were observed in HADS-A scores, HADS-D scores, Ramsay sedation scores (Supplementary Table S4 and Table 1), or the incidence of adverse events, including nausea and vomiting, pruritus, dizziness, somnolence, respiratory depression, hypotension, and bradycardia (Supplementary Table S3).
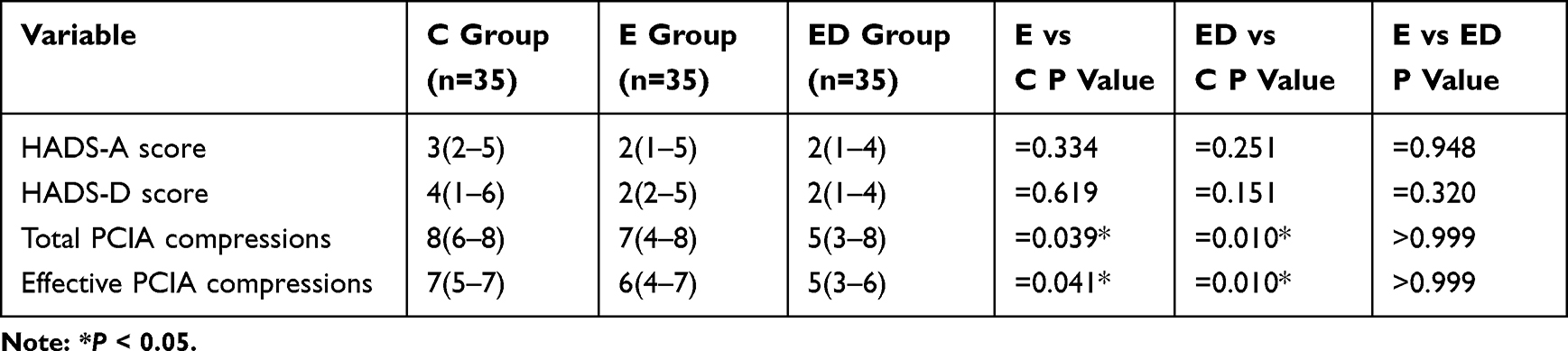 |
Table 1 Comparison of Postoperative Anxiety and Depression Scores and the Number of Pressing Times of Analges Ic Pump Among the Three Groups |
Discussion
This study demonstrates that both Group E and Group ED significantly improved maternal RCSQ scores on POD1 and POD2 compared with Group C, with Group ED showing greater improvement on POD1. These results indicate that low-dose esketamine enhances postoperative sleep quality after cesarean section, and co-administration with dexmedetomidine may further augment this effect. Both regimens also reduced resting pain scores.
Postoperative sleep disturbance is common after cesarean section.16,17 Previous studies have shown that esketamine and dexmedetomidine individually improve sleep quality, but evidence on their combined use in PCIA has been limited.12,18,19 We employed a low-dose esketamine regimen (0.5 mg/kg total; continuous infusion, 0.01 mg/kg/h), previously established as safe for mothers and neonates,20–22 combined with a low-dose dexmedetomidine infusion (0.02 μg/kg/h) to enhance analgesia and sleep quality without excessive sedation.23,24 The observed synergy may stem from complementary mechanisms. Esketamine’s NMDA receptor antagonism provides foundational analgesia and anti-inflammatory effects,25–27 potentially mitigating postoperative sleep disruption. While preclinical studies suggest esketamine can influence circadian regulators like CLOCK and BMAL1,28,29 we acknowledge this remains a hypothesis in our clinical context. Dexmedetomidine likely contributes through its α2-adrenergic agonist effects, enhancing analgesia and inducing natural sleep states.10,12,30 This pharmacodynamic profile may also counter esketamine-related neuropsychiatric side effects, supporting the safety of the combination.31
Although no significant difference in movement-evoked pain was observed versus controls, both esketamine and dexmedetomidine demonstrate dose-dependent analgesia. The relatively low doses used here may have been adequate for resting pain but suboptimal for movement-related pain.32–35 Nevertheless, both Group E and Group ED demonstrated a reduction in the number of presses on the analgesia pump, suggesting that these interventions were effective in managing postoperative pain in parturients.
We observed no significant changes in anxiety and depression scores, likely due to low preoperative baselines and the brief observation period.18,36 Future studies with extended follow-up are needed to evaluate long-term psychological outcomes.
From a clinical perspective, these findings suggest that incorporating low-dose esketamine, either alone or in combination with dexmedetomidine, into routine PCIA protocols may represent a feasible strategy to enhance postoperative sleep quality and improve maternal recovery after cesarean section. In particular, the addition of dexmedetomidine appears to further optimize the balance between analgesia, sleep promotion, and safety, while potentially reducing esketamine-related adverse effects. Therefore, adapting current PCIA regimens to include these agents could provide a practical and evidence-based approach to support enhanced recovery after surgery pathways in obstetric anesthesia.
This study has limitations. First, no validated minimal clinically important difference (MCID) exists for RCSQ, so the clinical relevance of our findings should be interpreted cautiously. Second, we did not include a dexmedetomidine-only group, although its sleep benefits are well established; further studies are needed to clarify whether combined therapy offers a true advantage over monotherapy. Third, objective sleep monitoring was not performed, limiting precision. Finally, the follow-up was restricted to the first three postoperative days, and long-term outcomes remain to be determined.
Conclusion
In conclusion, adding low-dose esketamine and dexmedetomidine to PCIA improved postoperative sleep quality and reduced resting pain after cesarean section, with a favorable safety profile. Future studies should optimize dosing strategies and assess dexmedetomidine monotherapy to further refine PCIA protocols in obstetric anesthesia.
Data Sharing Statement
Data are available to researchers on request for the purpose of reproducing the results or replicating the procedure by directly contacting the corresponding author.
Ethics Approval
The study protocol was approved by the Ethics Committee of Nanchong Central Hospital, Affiliated Hospital of Capital Medical University Beijing Anzhen Hospital (Approval No. 2024-192).
Consent Statement
All study participants or their legally authorized representative provided informed consent.
Supplementary Materials
The Supplementary File S1 contains the following supporting information: maternal demographics and general parameters of the newborns, a detailed comparison of the five components of the RCSQ over the first three postoperative days, and data on adverse reactions and Ramsay Sedation Scores.
Funding
Research Project of Sichuan Medical Science and Technology Innovation Research Association(2025HXKT013).
Disclosure
The authors report no other conflicts of interest in this work.
References
1. Eisenach JC, Pan PH, Smiley R, Lavand’homme P, Landau R, Houle TT. Severity of acute pain after childbirth, but not type of delivery, predicts persistent pain and postpartum depression. Pain. 2008;140(1):87–94. doi:10.1016/j.pain.2008.07.011
2. Parsaei M, Hasehmi SM, Seyedmirzaei H, et al. Perioperative esketamine administration for prevention of postpartum depression after the cesarean section: a systematic review and meta-analysis. J Affect Disord. 2024;361:564–580. doi:10.1016/j.jad.2024.06.080
3. Libretti A, Bracci B, De Pedrini A, Surico D, Troìa L, Remorgida V. The dermabond prineo skin closure system: benefits and complications. J Gynecologic Surg. 2023;40(2):123–131. doi:10.1089/gyn.2023.0038
4. Peltonen H, Paavonen EJ, Saarenpää-Heikkilä O, Vahlberg T, Paunio T, Polo-Kantola P. Sleep disturbances and depressive and anxiety symptoms during pregnancy: associations with delivery and newborn health. Arch Gynecol Obstet. 2023;307(3):715–728. doi:10.1007/s00404-022-06560-x
5. Jiang M, Xu J. A study on the effects of esketamine combined with comprehensive nursing intervention on postoperative pain, postpartum depression, and quality of life in women undergoing cesarean section. Altern Ther Health Med. 2024;30(10):70–77.
6. Li S, Zhuo Z, Li R, Guo K. Efficacy of esketamine for the treatment of postpartum depression and pain control following cesarean section: a randomized, double-blind, controlled clinical trial. Bmc Anesthesiol. 2024;24(1):52. doi:10.1186/s12871-024-02436-6
7. Xu LL, Wang C, Deng CM, et al. Efficacy and safety of esketamine for supplemental analgesia during elective cesarean delivery: a randomized clinical trial. JAMA Network Open. 2023;6(4):e239321. doi:10.1001/jamanetworkopen.2023.9321
8. Groetzinger LM, Rivosecchi RM, Bain W, et al. Ketamine infusion for adjunct sedation in mechanically ventilated adults. Pharmacotherapy. 2018;38(2):181–188. doi:10.1002/phar.2065
9. Bryant JE, Frölich M, Tran S, Reid MA, Lahti AC, Kraguljac NV. Ketamine induced changes in regional cerebral blood flow, interregional connectivity patterns, and glutamate metabolism. J Psychiatr Res. 2019;117:108–115. doi:10.1016/j.jpsychires.2019.07.008
10. Zhang Y, Cui F, Ma JH, Wang DX. Mini-dose esketamine-dexmedetomidine combination to supplement analgesia for patients after scoliosis correction surgery: a double-blind randomised trial. Br J Anaesth. 2023;131(2):385–396. doi:10.1016/j.bja.2023.05.001
11. Ding Y, Wang Z, Huang J, Yi Y, Wu Z. Esketamine optimized the efficacy of dexmedetomidine in treating sleep disorders with comorbid depression. Neuropsychiatr Dis Treat. 2025;21:1409–1423. doi:10.2147/ndt.S530265
12. Mei B, Yang X, Yang YY, et al. Intraoperative dexmedetomidine infusion improved postoperative sleep quality and melatonin secretion in patients undergoing elective thoracoscopic lung surgery: a prospective, randomized study. Nat Sci Sleep. 2024;16:2009–2020. doi:10.2147/nss.S491084
13. He J, Zhang X, Li C, Fu B, Huang Y, Li H. Dexmedetomidine nasal administration improves perioperative sleep quality and neurocognitive deficits in elderly patients undergoing general anesthesia. Bmc Anesthesiol. 2024;24(1):42. doi:10.1186/s12871-024-02417-9
14. Liu H, Wei H, Qian S, et al. Effects of dexmedetomidine on postoperative sleep quality: a systematic review and meta-analysis of randomized controlled trials. Bmc Anesthesiol. 2023;23(1):88. doi:10.1186/s12871-023-02048-6
15. Xu S, Zhou Y, Wang S, et al. Perioperative intravenous infusion of dexmedetomidine for alleviating postpartum depression after cesarean section: a meta-analysis and systematic review. Eur J Obstet Gynecol Reprod Biol. 2024;296:333–341. doi:10.1016/j.ejogrb.2024.03.024
16. Duran S, Vural G. Problems experienced by the mothers in post-cesarean period: a narrative review. Iran J Public Health. 2023;52(10):2036–2041. doi:10.18502/ijph.v52i10.13841
17. Kiliçli Id A, Zeyneloglu Id S. Effect of reflexology on pain, fatigue, sleep quality, and lactation in postpartum primiparous women after cesarean delivery: a randomized controlled trial. J Hum Lact. 2024;40(2):221–236. doi:10.1177/08903344241232982
18. Qiu D, Wang XM, Yang JJ, et al. Effect of intraoperative esketamine infusion on postoperative sleep disturbance after gynecological laparoscopy: a randomized clinical trial. JAMA Network Open. 2022;5(12):e2244514. doi:10.1001/jamanetworkopen.2022.44514
19. Zhai Q, Zhang Y, Ye M, et al. Reducing complement activation during sleep deprivation yields cognitive improvement by dexmedetomidine. Br J Anaesth. 2023;131(3):542–555. doi:10.1016/j.bja.2023.04.044
20. Singh JB, Fedgchin M, Daly E, et al. Intravenous esketamine in adult treatment-resistant depression: a double-blind, double-randomization, placebo-controlled study. Biol Psychiatry. 2016;80(6):424–431. doi:10.1016/j.biopsych.2015.10.018
21. Lei Y, Liu H, Xia F, et al. Effects of esketamine on acute and chronic pain after thoracoscopy pulmonary surgery under general anesthesia: a multicenter-prospective, randomized, double-blind, and controlled trial. Study Protocol. Front Med. 2021;8. doi:10.3389/fmed.2021.693594
22. Han T, Chen Q, Huang J, et al. Low-dose esketamine with sufentanil for postcesarean analgesia in women with gestational diabetes mellitus: a prospective, randomized, double-blind study. Front Endocrinol. 2023;14:1202734. doi:10.3389/fendo.2023.1202734
23. Zhang ZF, Su X, Zhao Y, et al. Effect of mini-dose dexmedetomidine supplemented intravenous analgesia on sleep structure in older patients after major noncardiac surgery: a randomized trial. Sleep Med. 2023;102:9–18. doi:10.1016/j.sleep.2022.12.006
24. Hong H, Zhang DZ, Li M, et al. Impact of dexmedetomidine supplemented analgesia on delirium in patients recovering from orthopedic surgery: a randomized controlled trial. BMC Anesthesiol. 2021;21(1):223. doi:10.1186/s12871-021-01441-3
25. Wang S, Deng C-M, Zeng Y, et al. Efficacy of a single low dose of esketamine after childbirth for mothers with symptoms of prenatal depression: randomised clinical trial. BMJ. 2024:385:e078218. doi:10.1136/bmj-2023-078218
26. Welters ID, Feurer MK, Preiss V, et al. Continuous s-(+)-ketamine administration during elective coronary artery bypass graft surgery attenuates pro-inflammatory cytokine response during and after cardiopulmonary bypass. Br J Anaesth. 2011;106(2):172–179. doi:10.1093/bja/aeq341
27. Yang Y, Zhang Y, Zhou G, Yang Z, Yan H, Zhang J. Efficacy of epidural esketamine on postoperative sleep quality after laparoscopic and robotic lower abdominal surgeries: a study protocol for randomised, double-blind, controlled trial. BMJ Open. 2024;14(2):e081589. doi:10.1136/bmjopen-2023-081589
28. Sato S, Bunney B, Mendoza-Viveros L, et al. Rapid-acting antidepressants and the circadian clock. Neuropsychopharmacology. 2022;47(4):805–816. doi:10.1038/s41386-021-01241-w
29. Orozco-Solis R, Montellier E, Aguilar-Arnal L, et al. A circadian genomic signature common to ketamine and sleep deprivation in the anterior cingulate cortex. Biol. Psychiatry. 2017;82(5):351–360. doi:10.1016/j.biopsych.2017.02.1176
30. Ji C, Su X, Gao C, et al. Advances in the use of dexmedetomidine during the perioperative period to improve postoperative sleep quality in patients undergoing surgery. J Int Med Res. 2024;52(11):3000605241290715. doi:10.1177/03000605241290715
31. Zhang CL, Yan Y, Zhang Y, et al. Effects of esketamine combined with dexmedetomidine on postoperative delirium and quality of recovery in elderly patients undergoing thoracoscopic radical lung cancer surgery: a randomized controlled trial. CNS Spectr. 2024:1–10. doi:10.1017/s1092852924002177
32. Liu QR, Zong QK, Ding LL, et al. Effects of perioperative use of esketamine on postpartum depression risk in patients undergoing cesarean section: a randomized controlled trial. J Affect Disord. 2023;339:815–822. doi:10.1016/j.jad.2023.07.103
33. Yang SQ, Zhou YY, Yang ST, et al. Effects of different doses of esketamine intervention on postpartum depressive symptoms in cesarean section women: a randomized, double-blind, controlled clinical study. J Affect Disord. 2023;339:333–341. doi:10.1016/j.jad.2023.07.007
34. Bellon M, Le Bot A, Michelet D, et al. Efficacy of intraoperative dexmedetomidine compared with placebo for postoperative pain management: a meta-analysis of published studies. Pain Ther. 2016;5:63–80. doi:10.1007/s40122-016-0045-2
35. Brinck ECV, Virtanen T, Mäkelä S, et al. S-ketamine in patient-controlled analgesia reduces opioid consumption in a dose-dependent manner after major lumbar fusion surgery: a randomized, double-blind, placebo-controlled clinical trial. PLoS One. 2021;16(6):e0252626. doi:10.1371/journal.pone.0252626
36. Chen Y, Guo Y, Wu H, et al. Perioperative adjunctive esketamine for postpartum depression among women undergoing elective cesarean delivery: a randomized clinical trial. JAMA Network Open. 2024;7(3):e240953. doi:10.1001/jamanetworkopen.2024.0953
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Sufentanil Combined with Nalbuphine via Patient-Controlled Intravenous Analgesia After Cesarean Section: A Retrospective Evaluation
Wang L, Wang Y, Ma Y, Mu X, Zhang Z, Wang H, Zheng Z, Nie H
Drug Design, Development and Therapy 2022, 16:3711-3721
Published Date: 21 October 2022
Analgesic Effect of Esketamine Combined with Tramadol for Patient-Controlled Intravenous Analgesia After Cesarean Section: A Randomized Controlled Trial
Guo Y, Ding X, Wang S, Wang F, Zheng Z, Zou L
Journal of Pain Research 2023, 16:3519-3528
Published Date: 20 October 2023
Effects of Intraoperative Esketamine–Dexmedetomidine Combination on Postpartum Depressive Symptoms and Neuropsychiatric Events Following Cesarean Delivery: A Randomized Controlled Trial
Li MM, Wei QF, Zhu QY, Qing X, Liu XS, Fang PP
Drug Design, Development and Therapy 2026, 20:587487
Published Date: 3 March 2026
Effect of Dexmedetomidine Combined with Esketamine on Postoperative Fatigue in Patients Undergoing Total Laparoscopic Hysterectomy: A Single-Center Randomized Double-Blinded Controlled Trial
Wu L, Wang Y, Chai Y, Qiu Z, Yin J, Zhang B, Wang G
Therapeutics and Clinical Risk Management 2026, 22:575704
Published Date: 14 April 2026
Postpartum Sleep Quality and Early Blood Pressure Levels After Cesarean Delivery in Women with Hypertensive Disorders of Pregnancy: A Prospective Cohort Study
Liu Y, Liu B, You J, Zhang L, Miao W, Ma F, He C, Liu G, Huang Y
International Journal of Women's Health 2026, 18:606769
Published Date: 9 May 2026