Back to Journals » Therapeutics and Clinical Risk Management » Volume 22
Effect of Dexmedetomidine Combined with Esketamine on Postoperative Fatigue in Patients Undergoing Total Laparoscopic Hysterectomy: A Single-Center Randomized Double-Blinded Controlled Trial
Authors Wu L, Wang Y, Chai Y, Qiu Z, Yin J, Zhang B, Wang G ![]()
Received 21 October 2025
Accepted for publication 30 March 2026
Published 14 April 2026 Volume 2026:22 575704
DOI https://doi.org/10.2147/TCRM.S575704
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Garry Walsh
Lei Wu,* Yuhui Wang,* Yuxin Chai, Zhuang Qiu, Jingwen Yin, Baoshuang Zhang, Guanglei Wang
Department of Anesthesiology, The Affiliated Hospital of Xuzhou Medical University, Xuzhou, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Guanglei Wang, Department of Anesthesiology, The Affiliated Hospital of Xuzhou Medical University, 99 Huaihai Road West, Quanshan District, Xuzhou, Jiangsu, 221006, People’s Republic of China, Tel +86 13852087156, Email [email protected]
Purpose: The purpose of this experiment is to study the impact of dexmedetomidine combined with esketamine on postoperative fatigue in patients who undergo total laparoscopic hysterectomy.
Patients and Methods: A total of 176 patients who received elective total laparoscopic hysterectomy were included in the study and divided into four groups: control group (Group C), dexmedetomidine group (Group D), esketamine group (Group E), and dexmedetomidine combined with esketamine group (Group DE). Group D received dexmedetomidine intervention, Group E received esketamine intervention, and Group DE received the combined intervention of dexmedetomidine and esketamine. The primary outcome was the 10-item Identity-Consequence Fatigue Scale (ICFS-10) scores, which were assessed before surgery and on postoperative days 3, 5, 7, and 30. Secondary outcomes included postoperative Visual Analog Scale (VAS) scores, Pittsburgh Sleep Quality Index (PSQI) scores, extubation time, first postoperative ambulation time, first postoperative flatus time, and nausea and vomiting incidence among four groups.
Results: Compared with Group C, Groups D, E, and DE had lower scores on ICFS-10 and PSQI on postoperative days 3, 5, and 7, as well as lower movement VAS scores at the postoperative 24 and 48 hours (p< 0.05). A lower fatigue incidence was also observed in Group DE on postoperative days 3, 5, and 7. Group DE showed a reduced rate of adverse events (vasoactive drug administration, postoperative nausea and vomiting, and requirement for rescue analgesia) compared with Group C (p< 0.05). No intergroup differences in ICFS-10 scores or fatigue incidence were found on postoperative day 30 (p> 0.05).
Conclusion: For patients undergoing total laparoscopic hysterectomy, the combined use of dexmedetomidine and esketamine enhances early postoperative fatigue levels and lowers the incidence of fatigue. However, this combination has no significant effect on fatigue on postoperative day 30.
Keywords: dexmedetomidine, esketamine, laparoscopic hysterectomy, postoperative fatigue, postoperative pain, sleep quality
Introduction
As a prevalent surgical intervention in gynecology, hysterectomy is commonly administered for the treatment of conditions including uterine fibroids, endometriosis, and abnormal uterine bleeding.1–3 Total laparoscopic hysterectomy (TLH) holds several distinct benefits over total abdominal hysterectomy, including less blood loss during surgery, reduced postoperative pain intensity, fewer wound infection cases, and shorter hospital stays.4 However, postoperative fatigue (POF) remains a common complication after total laparoscopic hysterectomy, presenting symptoms such as persistent weakness, decreased exercise tolerance, reduced interest, poor concentration, sleep disturbances, and low mood.5,6 Research has shown that in minimally invasive hysterectomy, POF is the second most common symptom following postoperative pain; approximately 85% of patients report experiencing this symptom.7 POF not only impairs patients’ postoperative daily activities and reduces their postoperative satisfaction but also may prolong hospital stay and increase medical costs.
The pathogenesis of postoperative fatigue (POF) is complex and remains incompletely understood, and may be associated with fear of disease progression, caregiver status, social support, activities of daily living, nutritional status, postoperative pain, sleep disturbance, anxiety, and depression.8–10 In perioperative anesthetic management, the selection of anesthetic agents, the choice of anesthesia methods, and the precise regulation of anesthetic depth are all important factors influencing the incidence of POF in patients.11–13 Esketamine, which represents the S-enantiomer of ketamine, can suppress the transmission of pain signals through blocking N-Methyl-D-Aspartate (NMDA) receptors, a mechanism contributing to the mitigation of postoperative pain.14 Previous studies have shown that the use of esketamine during gastrointestinal tumor surgery can reduce postoperative fatigue.15,16 Dexmedetomidine, a highly selective α2-adrenergic receptor agonist, has been shown to attenuate inflammatory responses and exert analgesic effects in surgical settings.17,18 In addition, it inhibits the excessive activity of the locus coeruleus, stimulates the occurrence of non-rapid eye movement sleep, and helps shape a sleep architecture that more closely resembles natural sleep.19 Currently, no clinical trial has evaluated the effect of intraoperative dexmedetomidine on postoperative fatigue as a primary endpoint. Nevertheless, the combination of dexmedetomidine and esketamine has been shown to offer distinct advantages over either agent used alone, including superior opioid-sparing effects, improved hemodynamic stability, and enhanced sleep quality.20–22
There is a paucity of evidence regarding the use of dexmedetomidine combined with esketamine for preventing POF in patients undergoing total laparoscopic hysterectomy. This study aims to explore whether the combination of the two drugs can improve POF, thereby providing a new strategy for the clinical rehabilitation of patients.
Materials and Methods
Participants
This study included patients who underwent TLH due to benign lesions at the Affiliated Hospital of Xuzhou Medical University from January 1, 2025 to August 22, 2025. The study set the following inclusion criteria: (1) Age 18–64 years; (2) American Society of Anesthesiologists Physical Status Classification I–II; (3) Body mass index 18–30 kg/m2. For exclusion criteria, they were: (1) refusal to participate by the patient; (2) preexisting preoperative fatigue; (3) contraindications to or allergies to the study drugs; (4) operation duration exceeding 3 hours, or occurrence of severe intraoperative complications requiring emergency treatment; (5) severe preoperative cardiovascular or cerebral dysfunction; (6) severe preoperative hepatic or renal dysfunction; (7) presence of mental or neurological diseases, or communication disorders; (8) conversion from laparoscopic surgery to open laparotomy; (8) postoperative admission to the intensive care unit.
Intervention Measures
This was a single-center prospective, double-blind, randomized controlled trial. A computer-generated random number list was used to randomly allocate eligible patients into four groups in a 1:1:1:1 ratio: dexmedetomidine combined with esketamine group (Group DE), dexmedetomidine group (Group D), esketamine group (Group E), and control group (Group C). Patients were assigned to groups using sealed opaque envelopes. After the patient entered the operating room, an anesthesia nurse who was not involved in perioperative patient management or data collection opened the envelope and prepared the study drugs according to the group assignment: dexmedetomidine (Yichang Renfu Pharmaceutical Co. Ltd). 200 μg diluted to 50 mL, esketamine (Jiangsu Hengrui Medicine Co. Ltd). 50 mg diluted to 50 mL, or normal saline 50 mL. All syringes were identical in appearance. Syringe pump 1 was labeled Study Drug A, containing either dexmedetomidine or normal saline; Syringe pump 2 was labeled Study Drug B, containing either esketamine or normal saline. Drug administration and intraoperative data collection were performed by another attending anesthesiologist who was unaware of the group assignments. In Group DE, dexmedetomidine (0.5µg/kg) was administered via pump infusion over 10 minutes before induction; after induction, esketamine (0.25mg/kg) was given by intravenous injection. During the operation, continuous pump infusion of dexmedetomidine (0.4µg/kg/h) and esketamine (0.125mg/kg/h) was maintained. In Group D, dexmedetomidine was administered via pump infusion, and normal saline in a volume equal to that of esketamine was given by intravenous injection or pump infusion. In Group E, esketamine was administered via intravenous injection and pump infusion, and normal saline in a volume equal to that of dexmedetomidine was given via pump infusion. In Group C, normal saline in volumes equal to those of the two drugs was given by intravenous injection or pump infusion at the same time points. The intervention drugs were continuously administered via pump infusion during the operation until the pneumoperitoneum was released in preparation for abdominal closure. Syringes by the same anesthesia nurse who was excluded from patient follow-up procedures. All operations were performed by the same expert team in our hospital. Patients, gynecologists, data collectors, and statisticians were all unaware of the grouping assignments.
Anesthesia Procedure
All patients were fasting for 2 hours and abstaining from drinking for 8 hours before surgery. Upon entering the operating room, routine monitoring (including electrocardiogram, pulse oxygen saturation, and blood pressure) was initiated for the patient. Baseline blood pressure of the patients was documented after intravenous administration of midazolam 0.02mg/kg. After 3 minutes of preoxygenation, anesthesia induction was conducted with etomidate 0.3mg/kg, sufentanil 0.3–0.5μg/kg, and rocuronium 0.6mg/kg. Following endotracheal intubation, mechanical ventilation was started with settings of 6–8 mL/kg tidal volume, 1:2 inspiratory-to-expiratory ratio, and 60% inspired oxygen concentration. The respiratory rate was adjusted to maintain the end-tidal carbon dioxide pressure within the range of 35–45mmHg. After anesthesia induction was finished, a senior physician gave 20 mL of 0.375% ropivacaine to each side under ultrasound guidance to conduct transversus abdominis plane block. During anesthesia maintenance, all groups received an intravenous infusion of remifentanil (0.1–0.3 µg/kg/min) and propofol (4–6 mg/kg/h) along with inhalation of 1% sevoflurane, while maintaining the bispectral index between 40–60. During the operation, the fluctuation ranges of HR and MAP were restricted to within 20% of their respective baseline values. When MAP reduction surpassed 20% of the baseline value, phenylephrine (50–100μg) or ephedrine (3–6mg) was administered. When MAP elevation surpassed 20% of the baseline value, the depth of anesthesia was increased or urapidil (10–20mg) was used. Sevoflurane and the intervention drugs were discontinued when abdominal closure was initiated. Meanwhile, 2mg tropisetron and 50mg flurbiprofen axetil were administered intravenously for postoperative antiemesis and analgesia. Propofol and remifentanil administration was halted when the surgery ended.
Postoperative Management
Postoperatively, flurbiprofen axetil 50 mg in 100 mL normal saline or tramadol 100 mg in 100 mL normal saline was administered intravenously as needed to maintain a VAS score < 4, with repeated doses permitted every 4–6 hours if required. In cases where a patient developed severe nausea and vomiting, 10mg of metoclopramide was administered intramuscularly. A liquid diet was provided until postoperative flatus occurred, accompanied by appropriate intravenous infusion to supplement electrolytes and vitamin C. Following the passage of flatus and ambulation, the diet was gradually switched to semi-liquid and easily digestible soft foods, with enhanced intake of high‑quality protein. A normal diet was gradually resumed 2–3 days postoperatively.
The Primary and Secondary Outcomes
The primary outcome is the severity of postoperative fatigue, evaluated with the 10-item Identity-Consequence Fatigue Scale (ICFS-10) on postoperative days 3, 5, 7, and 30 (see Supplementary Material 1 for details). The total score of the scale is 60 points, with higher scores indicating more severe fatigue. A score > 24 points is defined as the presence of fatigue.13 The secondary outcomes include the postoperative Visual Analog Scale (VAS) scores and the Pittsburgh Sleep Quality Index (PSQI) scores. Additionally, the following parameters were evaluated: the intraoperative doses of propofol and remifentanil, extubation time, first postoperative ambulation time, first postoperative flatus time. The occurrence of clinical adverse events such as postoperative nausea and vomiting (PONV), bradycardia, tachycardia, hypotension, hypertension, and psychiatric events was also analyzed. All the above outcome measures were assessed and data were collected by a dedicated investigator who was blinded to group allocation. After discharge, postoperative scale assessments were conducted via telephone follow-up. Missing data were handled using complete-case analysis, and only patients with complete data were included in the statistical analysis.
Sample Size Calculation
Sample size calculation was performed using PASS 15.0 (PASS Software, NCSS, LLC, USA, 2017). The primary outcome was the ICFS-10 score on postoperative day 3. A preliminary study including 24 patients (six patients per group) was conducted to estimate the effect size for sample size calculation. The mean ± standard deviation of ICFS-10 scores for Groups DE, D, E, and C were preliminarily estimated as 28.8 ± 5.5, 31.5 ± 5.2, 31.3 ± 6.0, and 34.3 ± 5.6, respectively. These patients were excluded from the final analysis cohort to avoid potential bias. A power analysis was performed with a type I error (α) of 0.05 and a power (1−β) of 0.90. Considering a 20% attrition rate, the total required sample size was determined to be 175 cases.
Statistical Analysis
Statistical analysis was performed using SPSS 28.0 (IBM SPSS, USA, 2022). Data normality was verified via the Shapiro–Wilk test. Normally distributed data were presented as mean ± standard deviation: intergroup comparisons utilized one-way ANOVA with Bonferroni correction for post-hoc pairwise analyses, while intragroup comparisons adopted repeated-measures ANOVA. Non-normally distributed data were presented as median and interquartile range (IQR). Intergroup comparisons among the four groups were performed using the Kruskal–Wallis test, and when a statistically significant difference was detected, Dunn’s post-hoc test with Bonferroni correction was used for multiple comparisons. Categorical variables are reported as numbers (%) and χ2-test or Fisher’s exact test was used when appropriate. Risk factors associated with the incidence of POF were analyzed using binary logistic regression analysis and generalized estimating equation analysis. A p<0.05 was considered statistically significant.
Results
As shown in the study flowchart (Figure 1), 205 female patients planning to undergo elective TLH were invited to participate. Of these, 21 were excluded due to inability, and 8 declined participation, leaving 176 patients who were ultimately enrolled. During the study, 1 patient in Group C was lost to follow-up; 1 patient in Group D and 1 patient in Group E required conversion from laparoscopic to open surgery; and in Group DE, 1 patient underwent conversion from laparoscopy to laparotomy and another was lost to follow-up. Finally, 171 patients were included in the analytical process. No statistically significant disparities were found among the four groups in terms of general characteristics, including age, BMI, preoperative hemoglobin level, educational level, comorbidities, and duration of surgery (p>0.05) (Table 1).
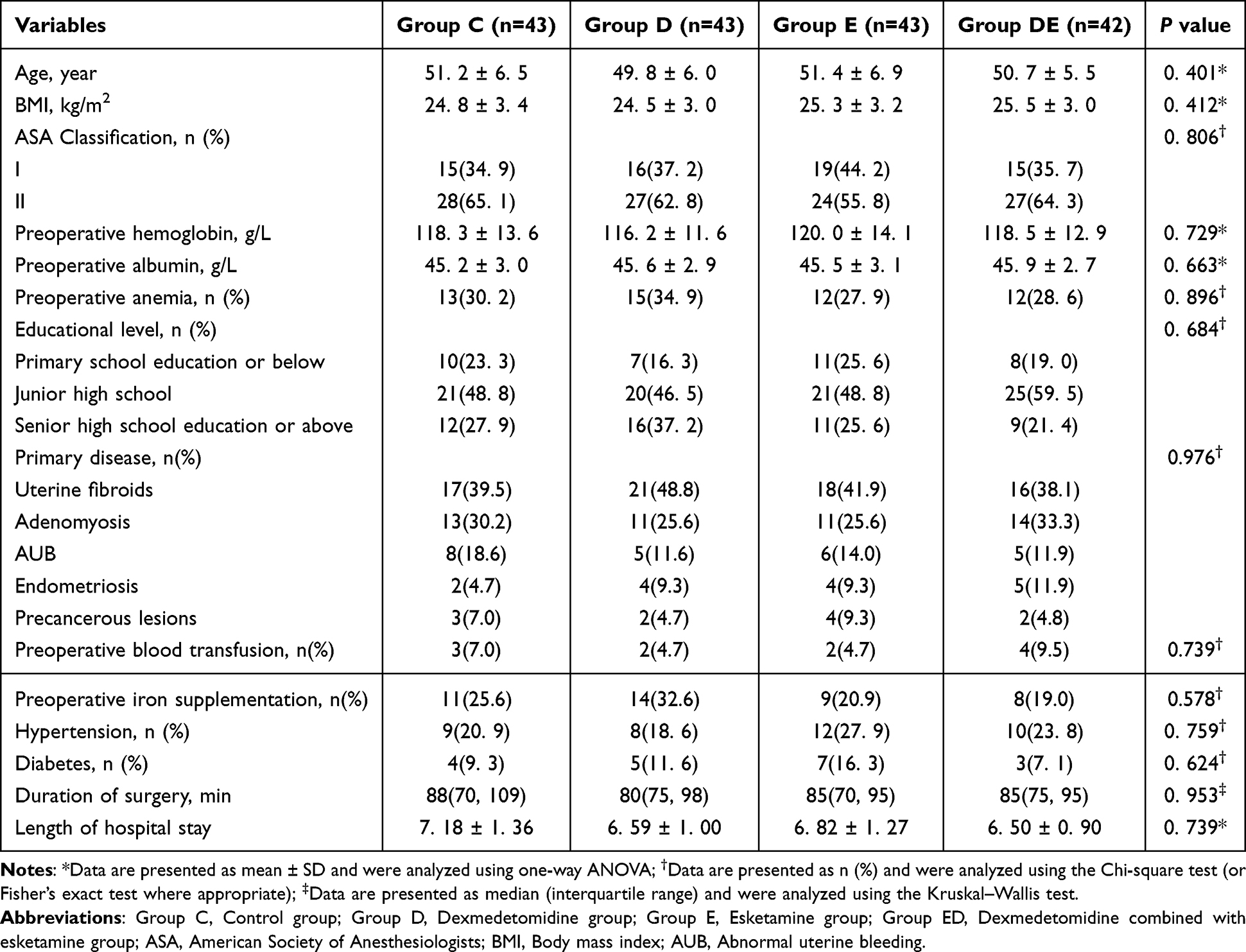 |
Table 1 Baseline Demographic and Clinical Characteristics of Patients |
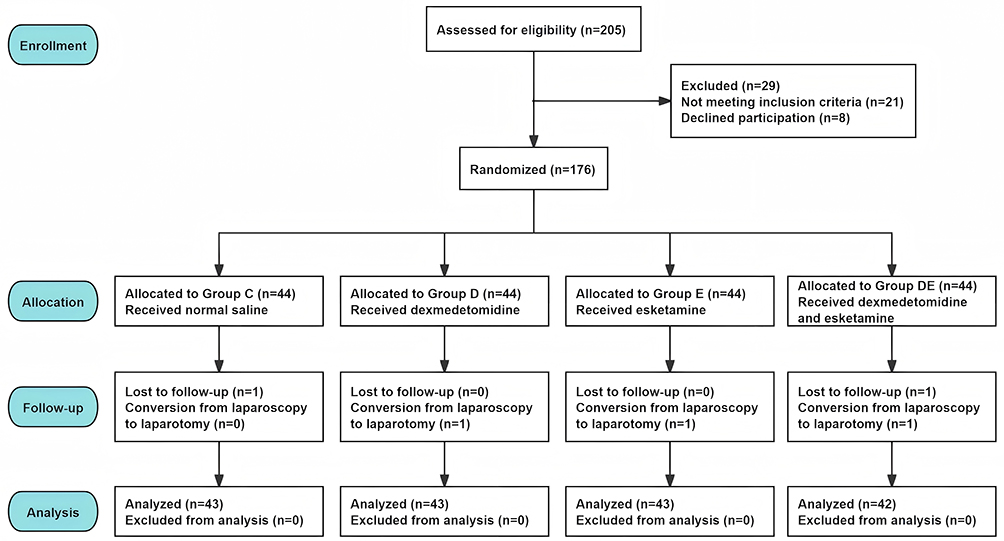 |
Figure 1 Study flowchart. |
Primary Outcomes
No significant statistical discrepancy was found regarding preoperative ICFS-10 scores among the four groups (p=0.825). Compared with Group C, Groups D, E, and DE had significantly lower ICFS-10 scores on postoperative days 3, 5, and 7 (p<0.05); notably, Group DE also exhibited a significantly lower fatigue incidence on these three time points (p<0.05). At each postoperative time point, ICFS-10 scores in all four groups were significantly higher than their respective preoperative scores (p<0.05). By postoperative day 30, however, the four groups showed no significant disparities in ICFS-10 scores or fatigue incidence (p>0.05) (Table 2).
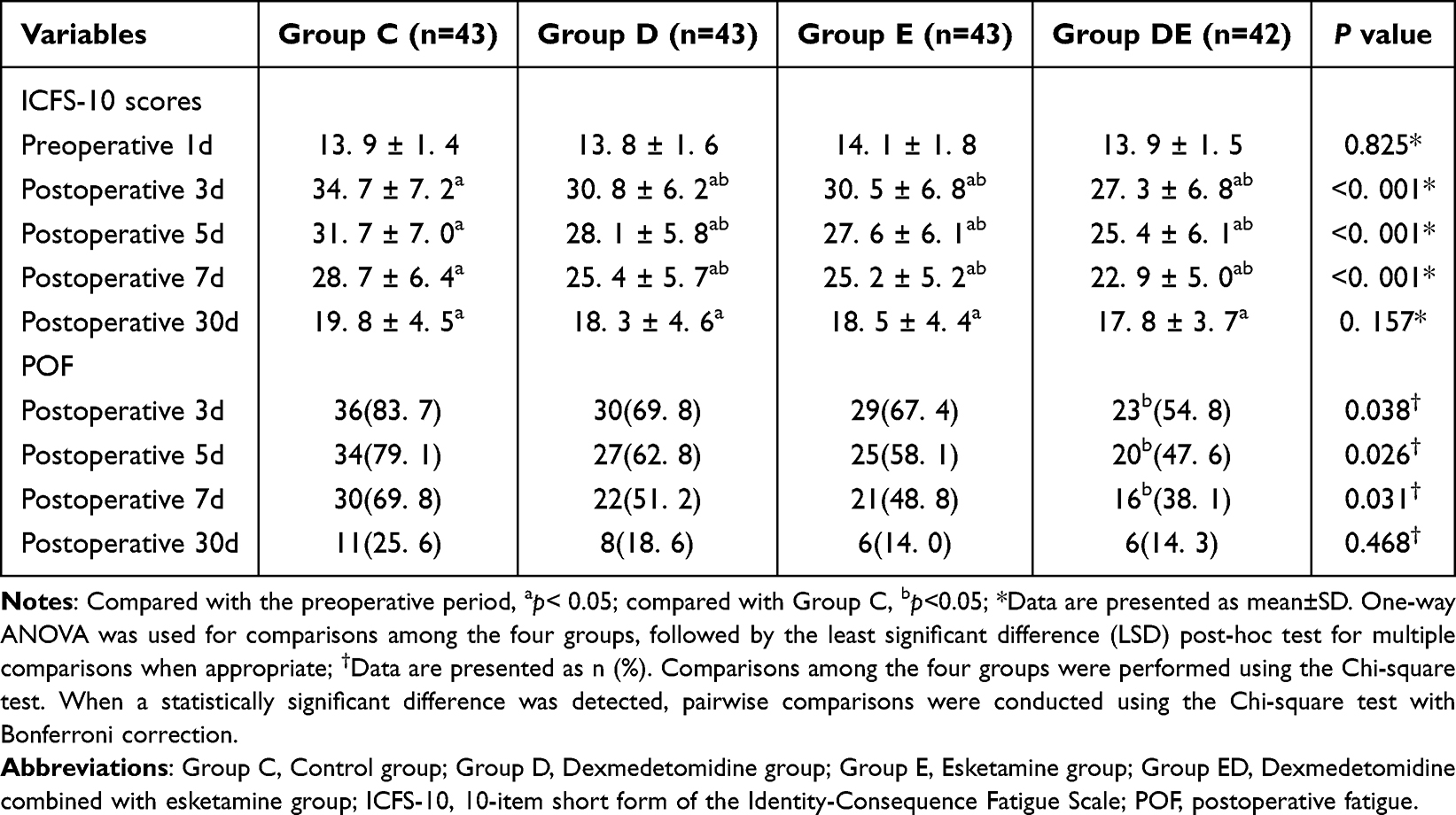 |
Table 2 Comparison of ICFS-10 Scores and POF Incidence at Multiple Time Points |
Secondary Outcomes
As shown in Table 3, compared with Group C, Group DE had a remarkably lower resting VAS score at 24 hours postoperatively (p<0.05). Additionally, at 24 and 48 hours postoperatively, Groups D, E, and DE had notably lower movement VAS scores (p<0.05). At 48 hours postoperatively, no statistically significant difference in resting VAS scores was observed among the four groups (p=0.460) (Table 3).
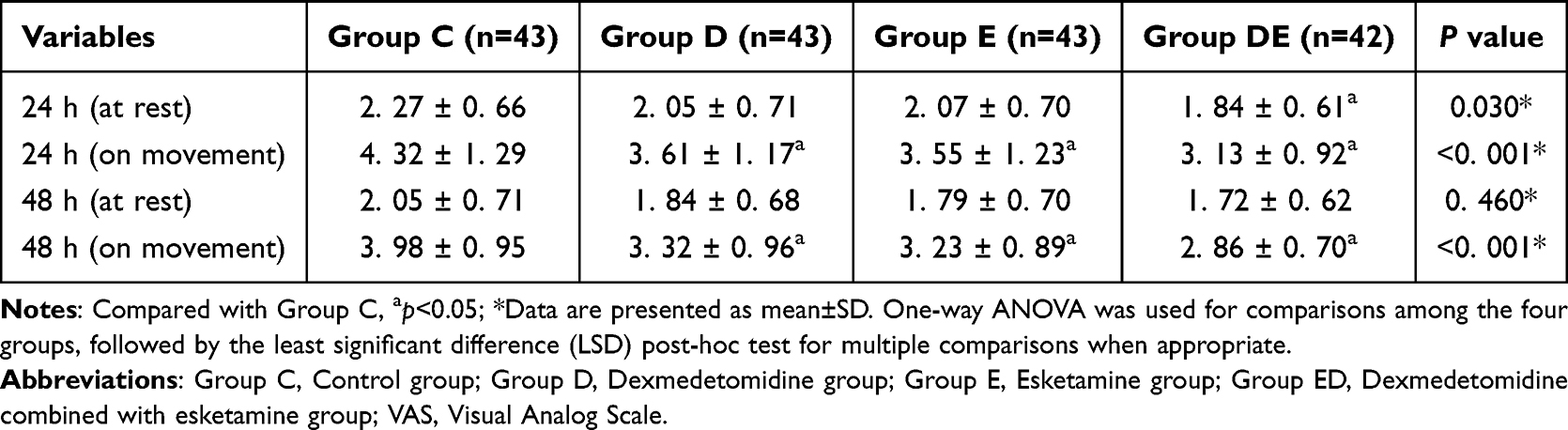 |
Table 3 Comparison of VAS Scores at Multiple Time Points |
Among the four groups, no notably statistical difference showed in preoperative PSQI scores (p>0.05). PSQI scores in Groups D, E, and DE were significantly lower than those in Group C on postoperative days 3, 5, and 7 (p<0.05). At all three postoperative time points, PSQI scores in all four groups were significantly higher than their respective preoperative scores (p<0.05). However, on postoperative day 30, the four groups showed no significant disparities in PSQI scores (p>0.05) (Table 4).
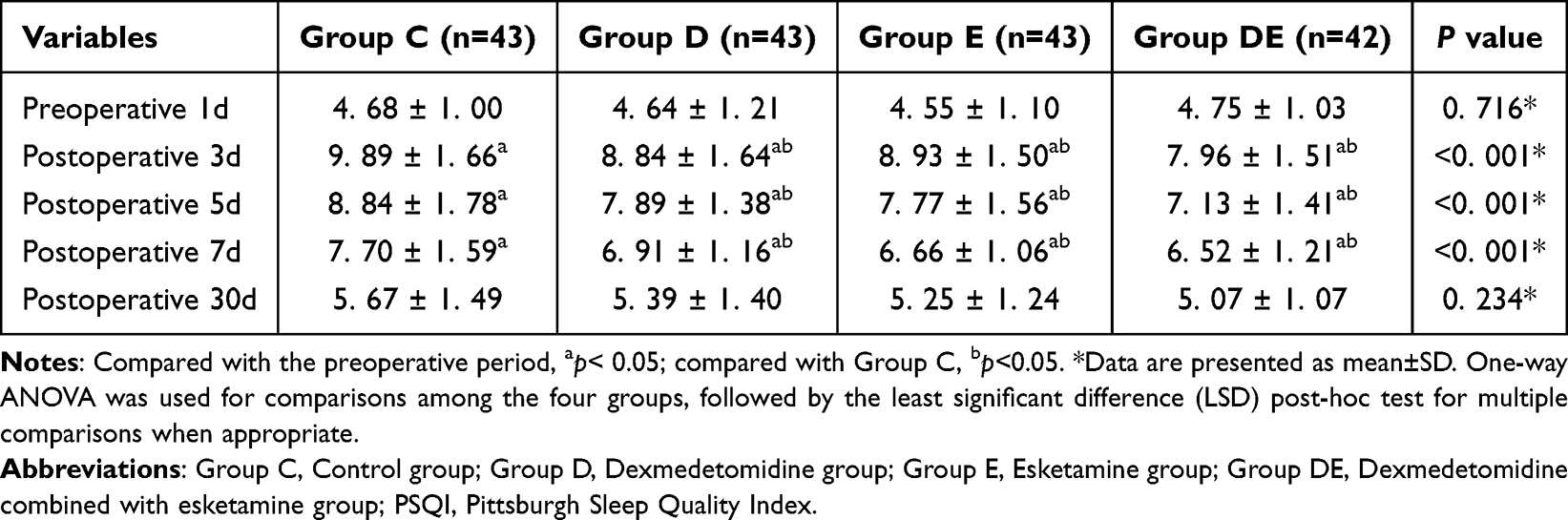 |
Table 4 Comparison of PSQI Scores at Multiple Time Points |
Moreover, compared with Group C, Group DE required significantly less propofol than Group C (p<0.05), while remifentanil dosages were significantly lower in Groups E and DE (p<0.05). Additionally, Group DE had a lower incidence of vasoactive drug use, PONV, and rescue analgesia than Group C (p<0.05). It is noteworthy that no psychiatric adverse events attributed to esketamine were recorded in the groups receiving esketamine. No significant differences in other clinical adverse reactions were observed across the four groups (p>0.05) (Table 5).
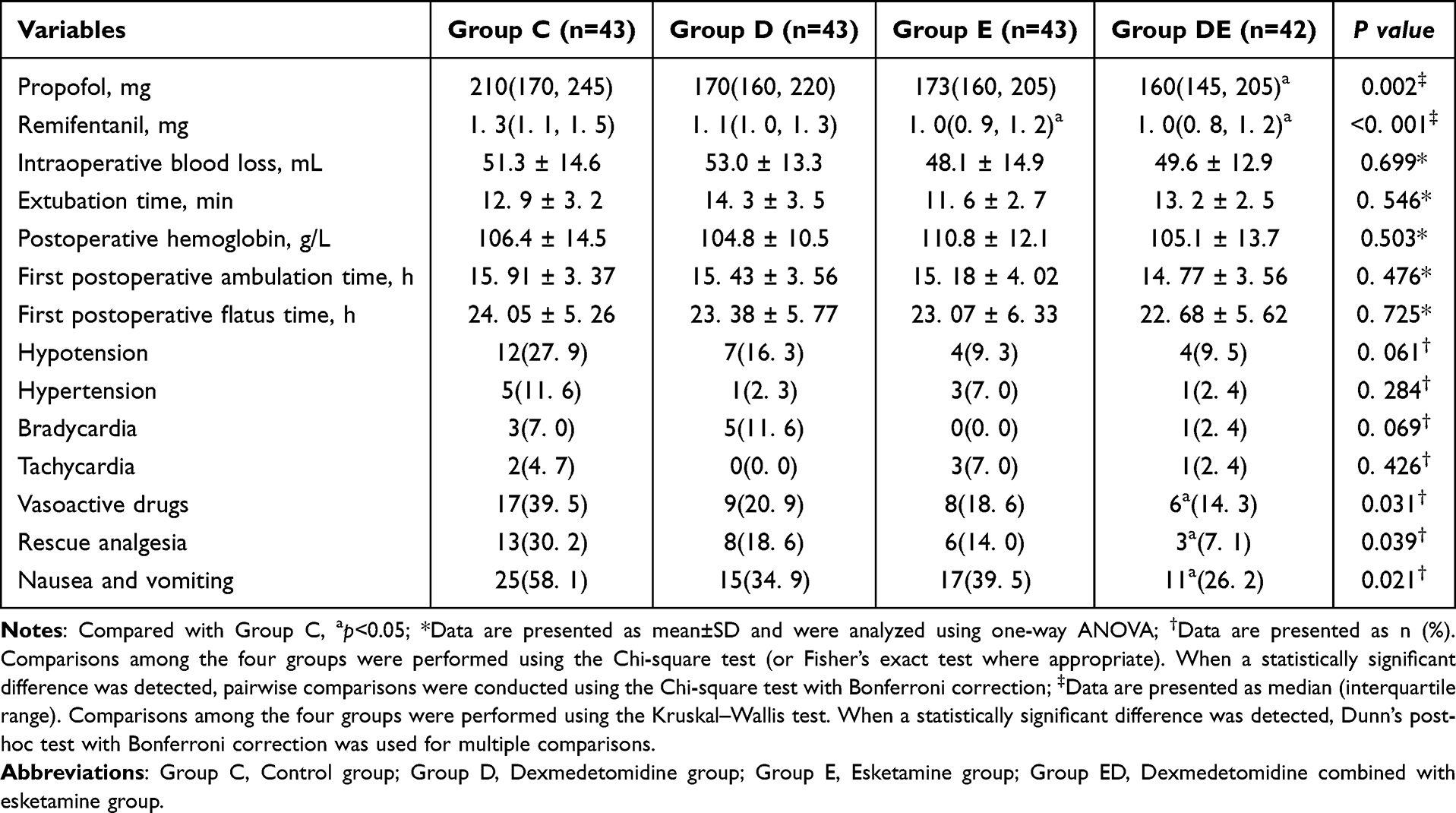 |
Table 5 Comparison of Intraoperative and Postoperative Conditions |
Univariate analysis was performed to screen for potential influencing factors of POF. For non-repeated measures data, binary logistic regression was used; for repeated measures data, the generalized estimating equation (GEE) was applied. The results showed that age, operation duration, postoperative hemoglobin level, and postoperative PSQI score were identified as potential factors associated with POF by binary logistic regression (p<0.05), while the GEE revealed that the VAS score during postoperative activity was also correlated with POF (p<0.05). These variables were then included in a multivariate generalized estimating equation model. After adjustment, age, postoperative hemoglobin level, operation duration, propofol dosage, postoperative PSQI score, and VAS score during postoperative activity were identified as independent risk factors for POF (Table 6).
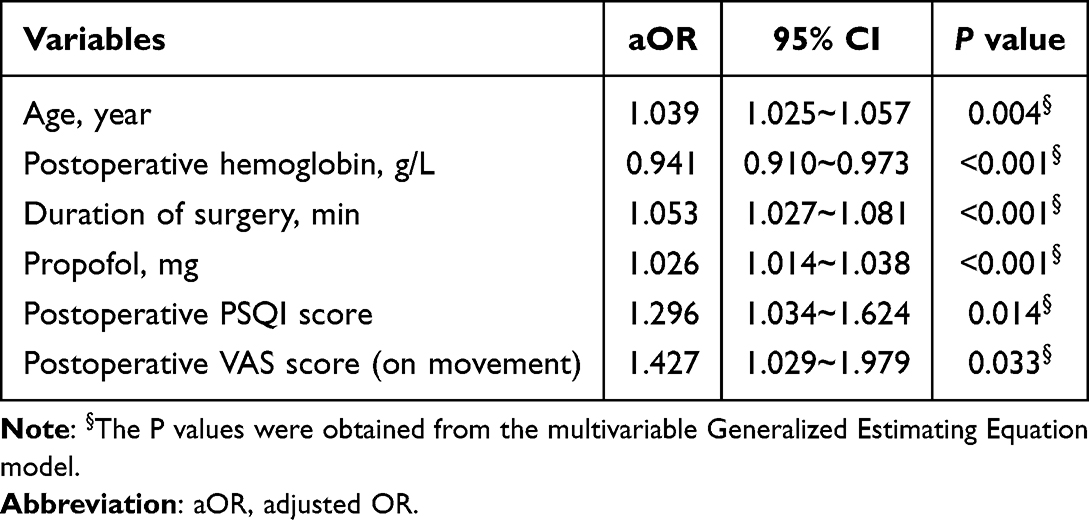 |
Table 6 Analysis of Risk Factors for POF |
Discussion
Postoperative fatigue, a common yet underrecognized complication, significantly impairs the recovery process of surgical patients.23,24 Previous studies have shown that hysterectomy can impair ovarian reserve, leading to hormonal secretion disorders and thus the early onset of menopausal symptoms.25 This phenomenon is more pronounced in patients over 40 years old, which is roughly consistent with the population included in this trial. Previous studies have shown a broad link between women’s psychological well-being and their social stressors.26 Furthermore, in the specific context of hysterectomy, the uterus is central to female identity; the surgery may cause psychological distress and self-perception disturbance, further contributing to postoperative fatigue.27,28 Nøstdahl et al selected 10 items from the 31 questions of the Perioperative Fatigue Assessment Scale to develop the ICFS-10 This scale evaluates multiple characteristics and manifestations of fatigue, with high internal consistency; it reflects patients’ fatigue status over the previous two days, and assessments at multiple time points can comprehensively capture the severity of perioperative fatigue.29 Fatigue incidence in Group C was as high as 83.7% in this study, and the incidence remained at 69.8% on the 7th day after surgery, which was consistent with the findings of previous study.7
Evidence from studies suggests that postoperative pain is closely associated with the occurrence of fatigue, and optimized pain management can alleviate the severity of postoperative fatigue.9 Dexmedetomidine can act on α2 receptors in the presynaptic membrane, inhibit the descending pain pathway, and reduce the release of norepinephrine. Meanwhile, it induces hyperpolarization of peripheral neurons and attenuates the firing of nociceptive neurons triggered by Aδ and C fibers, exerting an analgesic effect.30 Previous studies have revealed that administering low dose esketamine (0.25 mg/kg) preoperatively can relieve early postoperative pain in gynecological surgery.31 In the current study, Group D, E, and DE had a significantly lower pain score during postoperative activity, and Group DE required less postoperative rescue analgesia. This is conducive to the patients’ early postoperative ambulation, improves systemic blood circulation, and helps them recover energy and physical strength. Sleep disturbance is another key factor influencing the development of POF.9,32 The decline in sleep quality and changes in sleep patterns will exacerbate patients’ fatigue. Dexmedetomidine facilitates rapid eye movement sleep by promoting the suppression of norepinephrine release, while supporting a more physiological sleep pattern and improving sleep structure.33 The study by Qiu et al has shown that intraoperative infusion of esketamine can enhance sleep quality after gynecological surgery, with no significant adverse reactions34 In this study, both dexmedetomidine and esketamine have demonstrated the ability to improve postoperative sleep quality scores on postoperative days 3, 5, and 7, which is consistent with the findings reported by Zhang et al35 However, no significant differences in these scores among the four groups were detected on postoperative day 30. This finding may be associated with the metabolic clearance of the two drugs and the recovery of patients’ sleep structure. On postoperative day 30, no significant variations in PSQI scores were observed when each group’s postoperative scores were compared with their own preoperative measurements; This suggests that sleep disturbances induced by TLH may primarily occur during the early postoperative phase.
The beneficial effects of the combination regimen on reducing postoperative fatigue may also be attributed to the complementary effects of the two drugs. Dexmedetomidine likely curbs the systemic inflammatory response and provides neuroprotection, thereby reducing the physiological burden that contributes to fatigue.36 Concurrently, esketamine modulates the affective components of postoperative recovery. Sun et al reported that continuous intraoperative infusion of low-dose esketamine improved patients’ mood and reduced fatigue on postoperative days 3 and 716 Additionally, esketamine has been shown to induce alpha-spindle oscillations, thereby enhancing postoperative sleep quality.37 Both of these effects are crucial for psychological resilience following surgery. This multimodal approach-simultaneously dampening peripheral inflammation and bolstering central emotional recovery-represents a more holistic strategy. It is this synergistic interplay that enables the combination to outperform single-agent administration in lowering the incidence and severity of postoperative fatigue, thereby facilitating enhanced recovery.
However, comparisons among the four groups revealed no significant disparities in either ICFS-10 scores or POF incidence at 30 days postoperatively. This finding suggests that the fatigue-improving effects of dexmedetomidine and esketamine are primarily evident during the early stage after surgery—when postoperative pain, sleep disturbances, and surgical trauma responses are most prominent. Furthermore, the ICFS-10 scores on postoperative day 30 were still significantly higher than those preoperatively, and the incidence of fatigue in each group remained between 14.3% and 25.6%. Preoperatively comorbidities, as well as pelvic adhesions and pelvic floor dysfunction induced by surgery, may lead to the persistent presence of fatigue. Thus, more studies are necessary to examine the impacts of extra intervention strategies, such as psychological interventions and rehabilitation exercises, on chronic fatigue after surgery.
In this study, a loading dose combined with continuous intraoperative infusion was administered to maintain stable plasma concentrations and avoid fluctuations, thereby facilitating hemodynamic stability and reducing adverse reactions. Common adverse effects of dexmedetomidine include hypotension, bradycardia, and prolonged emergence time, whereas esketamine tends to induce hypertension, tachycardia, and neurological adverse reactions.38,39 The results showed no statistically significant difference in the incidence of the above adverse reactions between the four groups. Dexmedetomidine effectively alleviates sympathetic activation induced by esketamine, contributing to more stable intraoperative hemodynamics and reduced vasoactive agent requirements. Our results demonstrated that the administration of vasoactive agents was significantly decreased in Group DE, which is in line with previous findings by Ye et al22 Previous studies have demonstrated that propofol can promote glucagon-mediated gluconeogenesis and accelerate fatty acid β-oxidation, thereby attenuating acute postoperative fatigue.40 This study found that a higher dose of propofol was a mild risk factor for postoperative acute fatigue (adjusted OR = 1.026), which is inconsistent with previous studies reporting anti-fatigue properties of propofol. On the one hand, propofol dosage may largely serve as a surrogate marker for surgical duration and complexity; prolonged surgery is associated with greater tissue injury and stress responses, thereby increasing the risk of fatigue. On the other hand, the concurrent administration of dexmedetomidine and esketamine may exert more potent anti-inflammatory and analgesic effects, which could partially mask or offset the potential anti-fatigue benefits of propofol. Consequently, the net effect presented as a slight elevation in fatigue risk. Meanwhile, postoperative nausea and vomiting (PONV) is a common complication of gynecological laparoscopic surgery, which is associated with pneumoperitoneum, opioid administration, Trendelenburg position, and postoperative pain.41,42 The combination of these two agents can reduce intraoperative opioid consumption and postoperative rescue analgesic requirements. The results of the present study demonstrated that intraoperative remifentanil consumption was significantly decreased in Group D and Group DE. Furthermore, the incidence of PONV in Group DE was significantly lower than that in Group C. These findings are consistent with those reported in previous studies.43
The present study has certain limitations, which are as follows: First, controversy persists regarding the dose selection for dexmedetomidine and esketamine. Although the administration regimen employed in the present trial has been proven effective, it may not represent the optimal dosing strategy. Second, as the sample size of the present study was computed based on ICFS-10 scores from postoperative day 3, it may therefore lack adequate statistical power for assessing secondary endpoints. The sole administration of dexmedetomidine or esketamine can mitigate POF severity but fails to decrease the incidence of POF. Future studies will need to adjust drug dosing, and multi-center randomized controlled trials with expanded sample sizes should be performed to explore this area. Third, this study did not collect biological samples such as blood that could help analyze the mechanism by which dexmedetomidine and esketamine affect POF.
Conclusions
The combined administration of dexmedetomidine and esketamine significantly alleviated the severity and reduced the incidence of early postoperative fatigue in patients undergoing total laparoscopic hysterectomy. This intervention yielded lower fatigue scores, effective pain relief, and improved sleep quality in the early postoperative period. Importantly, this enhanced recovery profile was achieved without increasing adverse reactions, underscoring its clinical value as a safe and effective strategy for the prevention and management of POF.
Data Sharing Statement
Individual deidentified participant data collected during the trial will be fully shared, together with the study protocol and statistical analysis plan. Data access requests may be submitted to the corresponding author and will be approved after signing a data access agreement. Data will be available immediately upon publication for a period of 5 years.
Ethics and Registration
This study was approved by the Ethics Committee for Clinical Trials of the Affiliated Hospital of Xuzhou Medical University (ethics approval number: XYFY2024-KL561-01), and registered at the Chinese Clinical Trial Registry (ethics approval number: ChiCTR2400094406). Written informed consent was obtained from all enrolled patients. The trial is being carried out in compliance with the ethical principles of the Declaration of Helsinki.
Consent for Publication
All data and materials may be published, and the people providing consent have reviewed the entire content of the article to be published.
Acknowledgments
We thank the Department of Gynecology for their help with data collection.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest related to this work.
References
1. Pickett CM, Seeratan DD, mol BWJ, et al. Surgical approach to hysterectomy for benign gynaecological disease. Cochrane Database Syst Rev. 2023;8(8):CD003677. doi:10.1002/14651858.CD003677.pub6
2. Orhan A, Ozerkan K, Kasapoglu I, et al. Laparoscopic hysterectomy trends in challenging cases (1995-2018). J Gynecol Obstet Hum Reprod. 2019;48(10):791–12. doi:10.1016/j.jogoh.2019.06.007
3. Nguyen PN, Nguyen VT. Evaluating clinical features in intracavitary uterine pathologies among vietnamese women presenting with peri-and postmenopausal bleeding: a bicentric observational descriptive analysis. J Midlife Health. 2022;13(3):225–232. doi:10.4103/jmh.jmh_81_22
4. Madhok B, Nanayakkara K, Mahawar K. Safety considerations in laparoscopic surgery: a narrative review. World J Gastrointest Endosc. 2022;14(1):1–16. doi:10.4253/wjge.v14.i1.1
5. Schroeder D, Hill GL. Predicting postoperative fatigue: importance of preoperative factors. World J Surg. 1993;17(2):226–231. doi:10.1007/BF01658931
6. Maisel P, Baum E, Donner-Banzhoff N. Fatigue as the chief complaint–epidemiology, causes, diagnosis, and treatment. Dtsch Arztebl Int. 2021;118(33–34):566–576. doi:10.3238/arztebl.m2021.0192
7. Feinberg J, Zivanovic O, Hannon M, et al. Patient-reported symptoms after minimally invasive hysterectomy and association with postoperative complications. Gynecol Oncol. 2023;175:163–168. doi:10.1016/j.ygyno.2023.06.011
8. Cai Y, Zhou L. Risk stratification using a nomogram model for postoperative cancer-related fatigue in elderly survivors following early-stage non-small cell lung cancer resection. BMC Pulm Med. 2025;26(1):15. doi:10.1186/s12890-025-04046-5
9. Mendy N, Moriceau J, Sacuto Y, et al. Postoperative fatigue after day surgery: prevalence and risk factors. A prospective observational study. Minerva Anestesiol. 2020;86(12):1269–1276. doi:10.23736/S0375-9393.20.14358-X
10. She S, Wu Y, Mu A, Cui F, Zhao X, Shen M. Fatigue, sleep and physical activity in postoperative patients with pituitary adenomas: a survey. Int J Nurs Pract. 2024;30(3):e13237. doi:10.1111/ijn.13237
11. Guo S, Sun B, Wang X, et al. Effect of intravenous lidocaine on postoperative fatigue syndrome in patients undergoing laparoscopic radical colorectal cancer surgery: a randomized clinical trial. Sci Rep. 2025;15(1):18146. doi:10.1038/s41598-025-01892-5
12. Yin X, Qiao S, Zhang L, et al. New intervention strategy for postoperative fatigue syndrome in elderly patients with colorectal cancer: a clinical hypothesis study based on vagus nerve stimulation. Front Med Lausanne. 2025;12:1588850. doi:10.3389/fmed.2025.1588850
13. Wang X, Zhou M, Liu Q, et al. Impact of pecto-intercostal fascial block on postoperative fatigue in elderly patients undergoing off-pump coronary artery bypass grafting: a randomized clinical trial. Int J Surg. 2025;111(5):3323–3330. doi:10.1097/JS9.0000000000002353
14. Chen HZ, Gao Y, Li KK, et al. Effect of intraoperative injection of esketamine on postoperative analgesia and postoperative rehabilitation after cesarean section. World J Clin Cases. 2024;12(28):6195–6203. doi:10.12998/wjcc.v12.i28.6195
15. Lin X, Feng X, Sun L, et al. Effects of esketamine on postoperative fatigue syndrome in patients after laparoscopic resection of gastric carcinoma: a randomized controlled trial. BMC Anesthesiol. 2024;24(1):185. doi:10.1186/s12871-024-02513-w
16. Sun L, Zhao Y, Li Y, et al. Effect of continuous subanesthetic esketamine infusion on postoperative fatigue in patients undergoing laparoscopic radical resection for colorectal cancer: a randomized controlled study. Am J Cancer Res. 2023;13(6):2554–2563.
17. Zhong S, Sun Q, Wen J, et al. Dexmedetomidine attenuates inflammatory response and chronic pain following video-assisted thoracoscopic surgery for lung cancer. Surgery. 2024;176(4):1263–1272. doi:10.1016/j.surg.2024.06.001
18. Zeng H, Yin F, Fan L, et al. Combination of dexamethasone and dexmedetomidine as adjuvants of transversus abdominis plane block for postoperative analgesia in gastric cancer patients: a double-blinded randomized controlled trial. J Clin Anesth. 2024;97:111543. doi:10.1016/j.jclinane.2024.111543
19. Valli K, Radek L, Kallionpää RE, et al. Subjective experiences during dexmedetomidine- or propofol-induced unresponsiveness and non-rapid eye movement sleep in healthy male subjects. Br J Anaesth. 2023;131(2):348–359. doi:10.1016/j.bja.2023.04.026
20. Zhang Y, Cui F, Ma JH, Wang DX. Mini-dose esketamine-dexmedetomidine combination to supplement analgesia for patients after scoliosis correction surgery: a double-blind randomised trial. Br J Anaesth. 2023;131(2):385–396. doi:10.1016/j.bja.2023.05.001
21. Zhang XQ, Liu Y, Xie WX, et al. Effects of esketamine combined with dexmedetomidine on oxidative stress and lung function during one-lung ventilation in patients with mild to moderate COPD undergoing thoracoscopic surgery. Int Immunopharmacol. 2026;168(Pt 2):115860. doi:10.1016/j.intimp.2025.115860
22. Ye X, Xie B, Li Y, Zhong R, Li Y. Effect of dexmedetomidine-assisted esketamine on hemodynamics and stress level in patients undergoing total laparoscopic hysterectomy under general anesthesia. J Formos Med Assoc. 2025;2025:1
23. De Biase G, Otamendi-Lopez A, Chen S, et al. Impact of postoperative fatigue following minimally invasive lumbar spine surgery. J Clin Neurosci. 2023;112:64–67. doi:10.1016/j.jocn.2023.04.013
24. Tuveri M, Perri G, Marinelli V, et al. The prognostic role of fatigue, depression and anxiety on postoperative outcomes after pancreatectomy for pancreatic cancer. A prospective observational study (FAT-PRO study). Pancreatology. 2022;22(7):1035–1040. doi:10.1016/j.pan.2022.10.001
25. Huang Y, Wu M, Wu C, et al. Effect of hysterectomy on ovarian function: a systematic review and meta-analysis. J Ovarian Res. 2023;16(1):35. doi:10.1186/s13048-023-01117-1
26. Pham TH, Vo MT, Nguyen PN. Burnout syndrome and sexual disorders among vietnamese female nurses and midwives at Tu Du Hospital: A Frontline hospital-based cross-sectional study. Womens Health Rep. 2025;6(1):660–670. doi:10.1089/whr.2024.0193
27. Hare AM, Tappy E, Schaffer JI, et al. Effects of social determinants of health and social support on surgical outcomes among patients undergoing hysterectomy. Obstet Gynecol. 2025;145(1):115–123. doi:10.1097/AOG.0000000000005771
28. Blümel JE, Chedraui P, Vallejo MS, et al. Impact of hysterectomy without oophorectomy on the health of postmenopausal women: assessment of physical, psychological, and cognitive factors. Maturitas. 2025;196:108229. doi:10.1016/j.maturitas.2025.108229
29. Nøstdahl T, Bernklev T, Raeder J, Sandvik L, Fredheim O. Postoperative fatigue; translation and validation of a revised 10-item short form of the Identity-Consequence Fatigue Scale (ICFS). J Psychosom Res. 2016;84:1–7. doi:10.1016/j.jpsychores.2016.03.002
30. Chen Z, Liu Z, Feng C, Jin Y, Zhao X. Dexmedetomidine as an adjuvant in peripheral nerve block. Drug Des Devel Ther. 2023;17:1463–1484. doi:10.2147/DDDT.S405294
31. Li T, Han L, Wu Z, Chen Y, Wang Y. Effect of different doses of esketamine on postoperative recovery in patients undergoing gynecologic laparoscopic surgery, a randomized, double-blind, single-center clinical study. Drug Des Devel Ther. 2025;19:2833–2843. doi:10.2147/DDDT.S513571
32. Shen X, Jin M, Wang Y, et al. Fatigue trajectory and its associated factors in patients after pituitary adenoma surgery: a longitudinal study. Support Care Cancer. 2025;33(8):702. doi:10.1007/s00520-025-09745-7
33. Liu H, Wei H, Qian S, et al. Effects of dexmedetomidine on postoperative sleep quality: a systematic review and meta-analysis of randomized controlled trials. BMC Anesthesiol. 2023;23(1):88. doi:10.1186/s12871-023-02048-6
34. Qiu D, Wang XM, Yang JJ, et al. Effect of intraoperative esketamine infusion on postoperative sleep disturbance after gynecological laparoscopy: a randomized clinical trial. JAMA Network Open. 2022;5(12):e2244514. doi:10.1001/jamanetworkopen.2022.44514
35. Zhang L, He Y, Chen L, et al. Low-dose esketamine plus dexmedetomidine in patient-controlled intravenous analgesia improves post-cesarean sleep quality: a double-blind randomized trial. Drug Des Devel Ther. 2025;19:9789–9796. doi:10.2147/DDDT.S556396
36. Hu Y, Zhou H, Zhang H, et al. The neuroprotective effect of dexmedetomidine and its mechanism. Front Pharmacol. 2022;13:965661. doi:10.3389/fphar.2022.965661
37. Zhou YH, Li L, Gao R, et al. Effect of low-dose supplemental esketamine infusion on the intraoperative frontal electroencephalography dynamics and postoperative sleep disturbance during gynecological laparoscopic surgery: a double-blind, randomized clinical trial. Int J Surg. 2025;111(10):6988–7000. doi:10.1097/JS9.0000000000002836
38. Al-Hassan A, Weissman B, Chowdhury S, Sawires J, Soti V. Comparative efficacy of dexmedetomidine and remifentanil in reducing postoperative pain and opioid use: a systematic review. Cureus. 2025;17(2):e79759. doi:10.7759/cureus.79759
39. Suleiman A, Wongtangman K, Eikermann M, Stucke AG. Neuroanatomical and pharmaco-physiological effects of hypoxia and esketamine on breathing, the sympathetic nerve system, and cortical function. Br J Anaesth. 2025;134(2):277–280. doi:10.1016/j.bja.2024.11.011
40. Zhang WW, Xue R, Mi TY, et al. Propofol ameliorates acute postoperative fatigue and promotes glucagon-regulated hepatic gluconeogenesis by activating CREB/PGC-1α and accelerating fatty acids beta-oxidation. Biochem Biophys Res Commun. 2022;586:121–128. doi:10.1016/j.bbrc.2021.11.073
41. Wu X, Xing Y, Pan L, Chai M. Effect of perioperative application of dexmedetomidine on post-operative stress reaction, pain and prognostic adverse effects in patients undergoing gynaecological laparoscopy. J Minim Access Surg. 2024;20(4):373–379. doi:10.4103/jmas.jmas_47_23
42. Elvir-Lazo OL, White PF, Yumul R, Cruz Eng H. Management strategies for the treatment and prevention of postoperative/postdischarge nausea and vomiting: an updated review. F1000Res. 2020;9:F1000FacultyRev–983. doi:10.12688/f1000research.21832.1
43. Zhang CL, Yan Y, Zhang Y, et al. Effects of esketamine combined with dexmedetomidine on postoperative delirium and quality of recovery in elderly patients undergoing thoracoscopic radical lung cancer surgery: a randomized controlled trial. CNS Spectr. 2024;(20):1–10. doi:10.1017/S1092852924002177
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effect of Dexmedetomidine and Two Different Doses of Esketamine Combined Infusion on the Quality of Recovery in Patients Undergoing Modified Radical Mastectomy for Breast Cancer - A Randomised Controlled Study
Huang Z, Liu N, Hu S, Ju X, Xu S, Wang S
Drug Design, Development and Therapy 2023, 17:2613-2621
Published Date: 28 August 2023
Opioid-Free Anesthesia for Pain Relief After Laparoscopic Cholecystectomy: A Prospective Randomized Controlled Trial
Yu JM, Tao QY, He Y, Liu D, Niu JY, Zhang Y
Journal of Pain Research 2023, 16:3625-3632
Published Date: 30 October 2023
Intranasal Dexmedetomidine-Esketamine Combination Premedication versus Monotherapy for Reducing Emergence Delirium and Postoperative Behavioral Changes in Pediatric Tonsillectomy and/or Adenoidectomy: A Randomized Controlled Trial

Liao Y, Xie S, Zhuo Y, Chen S, Luo Y, Wei Y, Yao Y
Drug Design, Development and Therapy 2024, 18:4693-4703
Published Date: 23 October 2024
The Effects of Opioid-Free Anesthesia with Dexmedetomidine and Esketamine on Postoperative Anesthetic-Related Complications for Hip Surgery in the Elderly
Ye Q, Hu Y, Xing Q, Wu Y, Zhang Y
International Journal of General Medicine 2024, 17:6291-6302
Published Date: 17 December 2024
Effect of Intraoperative Intravenous Infusion of Esketamine Combined with Dexmedetomidine on Postoperative Sleep Disturbance in Patients Undergoing Radical Mastectomy
Geng X, Pu Y, Hu Z, Zhang H, Wang M, Fang C, Lv G, Li W, Zhang X, Fan X, Liu S, Chen X, Wu J
Drug Design, Development and Therapy 2025, 19:4629-4640
Published Date: 31 May 2025