Back to Journals » Journal of Pain Research » Volume 18
Long Term Effects of Acupuncture for Primary Dysmenorrhea: A Systematic Review and Meta-Analysis
Authors Shen X ![]() , Liu S
, Liu S ![]() , Chen H
, Chen H ![]() , Wang W
, Wang W ![]() , Fang J
, Fang J ![]() , Liu Z
, Liu Z ![]()
Received 13 May 2025
Accepted for publication 1 October 2025
Published 11 October 2025 Volume 2025:18 Pages 5359—5376
DOI https://doi.org/10.2147/JPR.S540073
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Houman Danesh
Xinyu Shen,1,2,* Sixing Liu,3,* He Chen,2 Wei Wang,1,2 Jiufei Fang,2 Zhishun Liu2
1Graduate College, Beijing University of Chinese Medicine, Beijing, People’s Republic of China; 2Department of Acupuncture, Guang’anmen Hospital, China Academy of Chinese Medical Sciences, Beijing, People’s Republic of China; 3School of Acupuncture-Moxibustion and Tuina, Beijing University of Chinese Medicine, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhishun Liu, Department of Acupuncture, Guang’anmen Hospital, China Academy of Chinese Medical Sciences, No. 5 Beixiange St., Xicheng District, Beijing, 100053, People’s Republic of China, Tel +8613651016313, Email [email protected]
Objective: Primary dysmenorrhea (PD) is a recurrent disease. The current treatments for PD often fail to provide long-lasting effects, underscoring the necessity for new treatment options that can offer durable benefits. Previous studies have indicated that the durable effect of acupuncture for PD remains uncertain. In this review, we aimed to evaluate the durable effect after completion of treatment.
Methods: Both English and Chinese literature were comprehensively retrieved from eight databases up to January 24, 2025. Two independent reviewers conducted screening and data extraction. The risk of bias was evaluated using the Cochrane Risk of Bias 2.0 tool. Meta-analysis was conducted where applicable. Pooled continuous data were expressed as mean differences (MD) and the safety outcomes were expressed through odds ratio (OR).
Results: Fourteen randomized controlled trials enrolled 970 patients met the inclusion and exclusion criteria. Acupuncture outperformed no intervention in reducing pain intensity measured by visual analogue scale (VAS) (MD − 47.80; 95% CI − 48.63 to − 46.97; p < 0.0001) and Short-Form McGill Pain Questionnaire (MD − 8.55; 95% CI − 11.46 to − 5.64; p < 0.0001), Cox Menstrual Symptom Scale (CMSS) duration score (MD − 18.24; 95% CI − 22.39 to − 14.09; p < 0.0001) and severity score (MD − 12.96; 95% CI − 16.41 to − 9.51; p < 0.0001) at 3 menstrual cycles post-treatment. Compared to non-steroidal anti-inflammatory drugs (NSAIDs), acupuncture showed superior pain relief measured by VAS (MD − 29.89; 95% CI − 37.63 to − 22.15; p < 0.0001), and symptom amelioration measured by CMSS (MD − 3.00; 95% CI − 5.92 to − 0.08; p = 0.0043) at 3 cycles post-treatment. Acupuncture also enhanced NSAIDs’ analgesic effect measured by VAS (MD − 19.95; 95% CI − 24.23 to − 15.66; p < 0.0001). However, acupuncture presented no superiority over sham acupuncture at 3 menstrual cycles post-treatment.
Conclusion: Acupuncture might provide durable post-treatment effects to primary dysmenorrhea patients up to three menstrual cycles, which was limited by high risk of bias and low certainty evidence.
Keywords: acupuncture, long term effects, meta-analysis, primary dysmenorrhea, systematic review
Introduction
Dysmenorrhea is a prevalent gynecological disease worldwide, classified into primary and secondary forms. Patients with secondary dysmenorrhea are offered a range of appropriate treatments. Hormonal therapy is commonly used to alleviate symptoms and mitigate disease progression, particularly in cases associated with endometriosis or adenomyosis. Additionally, hysteroscopic procedures provide both diagnostic and therapeutic benefits, especially for young women with reproductive aspirations.1,2 Nonetheless, significant gaps remain in the management of primary dysmenorrhea (PD), necessitating further research to optimize treatment strategies.
PD is a type of menstrual pain in the absence of pelvic pathology, necessitating assessment through secondary-level ultrasonography. PD is a prevalent gynecological disease worldwide, affecting an estimated 45% to 90% of women.3 A prior systematic review demonstrated that the prevalence of PD has exceeded 66%.4 A cross-sectional study reported that 51.1% of Chinese college girls experienced PD, with moderate to severe pain occurred in over 30% of these cases.5 Typically, PD occurs for the first time within 6 to 12 months post-menarche.6 Patients may present with recurrent onset within a few hours before and after menstrual bleeding, peaking with the increased of blood flow. The common clinical symptom is spasmodic pain in the lower abdomen or suprapubic area, radiating to the waist or thighs possibly, also including diarrhea, nausea, and vomiting.7 Aside from its PD, featured by recurrent nature and high prevalence, places significant economic repercussions, in addition to negative impacts on psychological well-being and quality of life. Dysmenorrhea may decrease work efficiency and cause absenteeism, resulting in financial burden annually, with an estimated $ 2 billion in the USA.8,9 Therefore, it necessitates the investigation of the management strategy of PD in this situation.
Non-steroidal anti-inflammatory drugs (NSAIDs) for acute pain relief, and hormonal therapies to inhibit ovulation (such as combined hormonal contraceptives) are generally recommended for managing PD by clinical guidance.3,7,9–11 NSAIDs, as first-line analgesic agents, demonstrate limitations in adequately managing patients. Prolonged NSAID administration is associated with gastrointestinal mucosal injury and neuropsychiatric adverse effects. Additionally, approximately 20% of patients report persistent pain despite therapy.12,13 What’s more, medication adherence remains suboptimal, with over 25% of cases involving incorrect dosing.13 Moreover, pharmacokinetic properties of NSAIDs restrict their efficacy to short-term symptom relief, necessitating prophylactic administration prior to pain onset and timely dosing aligned with menstrual cycles. Nonetheless, many patients, particularly adolescents, tend to administer medication post-pain onset, resulting in approximately 90% experiencing pain during each menstruation cycle.14 Hormonal therapies are carefully prescribed for females without contraindications. However, oral contraceptives may induce irregular bleeding in 39%–60% of users and heighten the risk of venous thromboembolism.15,16 Currently, continuous use of contraceptives is recommended, in contrast to the earlier periodic intake, yet accompanied by adherence challenges.17 Little data can be obtained concerning the durable effect after withdrawal. Intrauterine device may be a feasible solution, which, however, is not applicable for young sufferers.18,19 Transcutaneous electrical nerve stimulation (TENS), exercise, behavioral interventions, dietary supplements, topical hot compress and other non-pharmacological interventions are also favored complementary and alternative options. However, it remains an unanswered question of the continuous effect of TENS and exercise, even though they are superior to placebo or no treatment at the end of treatment.20,21 Moreover, the effect of other non-pharmacological interventions described before remains uncertain because of scant and low-quality evidence. At this stage, it is pivotal for seeking a safe and durable treatment.
Even though acupuncture has the following shortcomings, including the financial burden caused by no insurance coverage, the low acceptance of patients with less than 2% of Americans have received acupuncture treatment, and the lack of doctor’s referral, the advantages of its safety and durable effect make it a potential choice for subjects with obstetric and gynecologic diseases, including PD.22–24 Previous studies suggested that acupuncture not only had a similar effect to NSAIDs or sham acupuncture (SA) at the end of treatment, but it might have durable effects as well.25,26 The durable effect refers to the effect still present after the treatment is complete, which may be beneficial in preventing the occurrence of PD, alleviating pain intensity, and avoiding adverse effects from long-term medication use for patients with PD. However, we have no systematic evidence about the long-lasting effect of acupuncture for PD. Therefore, we carried out this review and meta-analysis to investigate whether acupuncture can provide lasting benefits for PD. Our findings might inform gynecologists’ clinical decision-making, guide future research directions for researchers, and offer new treatment options available to patients.
Methods
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines (Table S1), and it was registered on the International Prospective Register of Systematic Reviews (PROSPERO ID: CRD42024603729).27
Search Strategy
From inception to January 24, 2025, we conducted a comprehensive search across PubMed, EMBASE, Web of Science, Cochrane Central Register of Controlled Trials, and Chinese databases including China National Knowledge Infrastructure (CNKI), China Biology Medicine disc (CBM), WanFang Database, and VIP Database. The search strategy employed a combination of free terms and medical Subject Headings (Mesh), integrated through Boolean operators OR and AND. Mesh utilized in the search included “dysmenorrhea” and “acupuncture.” In addition, we reviewed the references of included studies and relevant reviews to avoid omission. The search strategies are detailed in Table S2 of the supplementary material.
Inclusion Criteria
The inclusion criteria for the systematic review followed PICOS principle.
- Participants: Patients with a diagnosis of PD, defined as pain occurring during menstruation without pelvic pathology.
- Intervention: Intervention groups received acupuncture treatment, which refers to the therapy of inserting needles at specific points for stimulation (such as manual acupuncture, electro-acupuncture, auricular acupuncture, dry needling). Studies were both eligible when comparing acupuncture plus another intervention to the intervention alone, and when using different acupuncture techniques.
- Comparison: Controls included SA, no treatment, NSAIDs, hormonal drugs, and complementary and alternative therapy.
- Outcomes: At least one of pain intensity, pain duration, menstrual related symptoms, quality of life, anxiety and depression, and adverse events should be reported for no less than one menstrual cycle after completion of all treatments.
- Study Design: Only randomized controlled trials (RCTs) were included.
Exclusion Criteria
Studies with following features were excluded: (1) letters, conference papers, and abstracts; (2) studies mixed patients of secondary dysmenorrhea or dysmenorrhea caused by intrauterine device, and the results for PD group could not be extracted separately; (3) interventions involved needle knife therapy, acupoint injection, bee venom acupuncture, thread embedding therapy, or non-penetrating acupuncture (eg laser acupuncture); (4) studies involved Chinese medicine, moxibustion cupping, manipulation and other Chinese treatments excluding acupuncture in any group; (5) studies with unclear follow-up time points.
Outcomes
Data from all available time points after treatment were analyzed. Post-treatment referred to after the last treatment. Other outcomes were assessed based on changes from the baseline, except for the adverse events. The required data from reported statistics would be calculated according to Cochrane guidelines in case of no direct relevant statistics in some researches.28 We extracted pre- and post-intervention means, Standard Deviation (SD), and sample sizes from all included studies. The mean difference (Mean change) was obtained by subtracting the baseline value from the endpoint value as:

If the change of SD (SD change) was not reported, the following formula based on the baseline and final SD can be used to calculate the SD value:

As baseline-endpoint correlation coefficients (Corr) were not reported in these studies, a Corr value of 0.5 was used, which is a value calculated in most articles.29,30
The primary outcome was the change from baseline in pain intensity measured using the Visual Analog Scale (VAS), Numerical Rating Scale (NRS), Brief Pain Inventory (BPI), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), and so on, which have demonstrated high reliability and validity.31 Meanwhile, we also evaluated whether the effects size of VAS reached the minimal clinically important differences (MCIDs). The 0 to 10cm VAS used in some RCTs were converted to 0 to 100mm VAS to facilitate subsequent comparisons. We selected MCIDs of VAS for endometriosis of 10mm as the MCIDs of PD owing to the deficiency of standards in PD.32 The VAS consists of a 100mm line, with one end indicating no pain and the other representing the most severe pain imaginable. Patients ticked their pain level along the line, with distances from “no pain” to the tick mark yielding pain scores. Higher marks mean heavier pain intensity.
Secondary outcomes included the changes from baseline in pain duration, menstrual symptom (measured using CMSS [Cox menstrual symptom scale]/RSS [Cox retrospective symptom scale]/MSS [menstrual symptom score], higher score means worse state), quality of life (measured using SF-36 [36-item Short-Form Health Survey], higher score means better status), and anxiety (measured by HAMA [Hamilton Anxiety Scale], higher score means worse state). Adverse events were also one of the secondary outcomes. What’s more, CMSS had a high degree of validity and reliability in the female population (Cronbach α = 0.833).33
Study Selection and Data Extraction
Literature screening was conducted independently by two researchers in accordance with the aforementioned eligibility criteria. After eliminating the duplicate documents, a preliminary screening was continued by reviewing the title and abstract, and then checking the full text for final screening. We employed Kappa score to evaluate the consistency of two researchers.
Similarly, data were extracted by two researchers independently from the included RCTs using a predesigned table in Excel 2021. Specific data that would be enrolled were first author, publication year, country, sample size, average age, intervention and comparison details, outcomes, follow-up time points, and adverse events. In case of divergence, a consensus would be reached through discussion or by involving a third assessor.
Risk of Bias
The risk of bias of the included studies was also subjected to assessment by two independent researchers in adherence to the Cochrane Risk of Bias 2.0 tool. We evaluated the risk of bias according to the following five domains: randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported results. Each domain was rated as either at “low risk of bias”, “some concerns”, or “high risk of bias”. Differences were settled through discussion, and if necessary, a third investigator intervened to reach a consensus.
Quality of Evidence Assessment
The GRADEpro GDT was used to the GRADE (Grading of Recommendations Assessment, Development, and Evaluation) approach, which was conducted to evaluate the certainty of evidence for outcomes. We evaluated the certainty of evidence according to risk of bias, inconsistency, indirectness, imprecision, and other reasons. The certainty of evidence for each outcome was rated as high, moderate, low, or very low.34
Data Analysis
The Meta package in R (version 4.3.2) was utilized for data analysis.35 Pooled continuous data were expressed as mean differences (MD) with 95% confidence interval (CI). The safety outcomes were expressed through odds ratio (OR), with higher likelihood of acupuncture-related adverse events confirmed when OR>1. I2 was used to evaluate the heterogeneity of meta-analysis. The random effect model was used when significant heterogeneity existed (I2≥50%), and otherwise, the fixed effect model was selected. The leave-one-out way was employed in the sensitivity analysis to evaluate the robustness of the results regarding the long-lasting effect. If the effect size and direction of the results remained consistent with the exception of any single study, the results were considered stable; otherwise, results were considered unstable. Furthermore, a sensitivity analysis was performed using Corr of 0.3 and 0.7 to assess the robustness of the results under these different Corr. If at least 10 studies were included in a meta-analysis with significant heterogeneity, meta-regression was used to explore the source of heterogeneity. VAS-specific subgroup analysis was performed based on the timing of intervention and measurement. The publication bias was clarified using Egger ‘s test and funnel plot if there were at least 10 studies in a meta-analysis.
Results
Study Selection
The details of decision pathway for included studies were summarized at the PRISMA flowchart in Figure 1. As of January 24, 2025, 18530 citation records were returned (PubMed = 426, Embase = 857, Web of science = 345, Cochrane = 590, CNKI = 4126, WanFang = 3682, CBM = 4752, VIP = 3752). After removing duplicates, 9594 studies remained. 306 studies were included for full-text assessment after the title and abstract screening (Kappa score = 0.798). 14 studies met the eligibility criteria and were included in the final analysis (Kappa score = 0.884).36–49
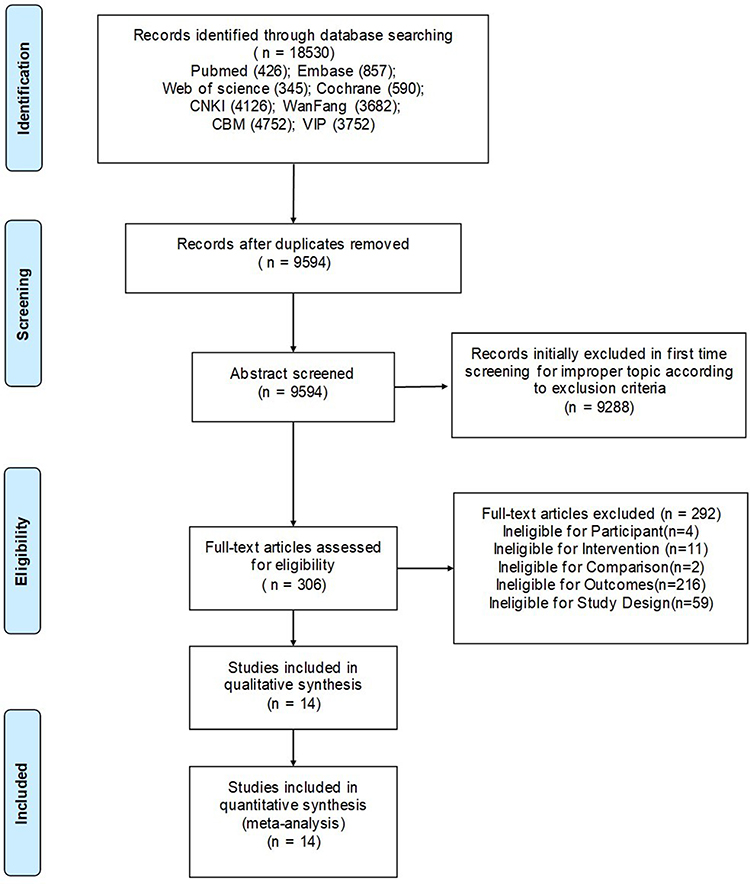 |
Figure 1 Flow diagram of the identification and selection of studies. |
Study Characteristics
For this review, 970 patients were enrolled in the fourteen studies published ranging from 2011 to 2024. The mean age of participants was predominantly around 20 years old. There was no significant difference in baseline characteristics among all studies. Of these, thirteen studies were conducted in China, while one study was executed in Australia by Smith et al36–49 In terms of interventions, ten studies compared acupuncture with NSAIDs,36–39,41,42,44,45,47,48 two studies compared acupuncture with SA,40,49 two studies compared acupuncture with no treatment,43,46 and two studies compared acupuncture plus NSAIDs with NSAIDs alone.41,42 The duration of acupuncture ranged from three to eight sessions every menstrual cycle, spanning three menstrual cycles. Post-treatment follow-up periods varied from one to six menstrual cycles. Regarding the timing for intervention, four studies were performed from 7 days before menstruation,36,39,42,46 three studies from 3–4 days before menstruation,38,40,44 one study from 3 days before menstruation until the fifth day of menstruation,41 two studies from the first day of menstruation or the onset of pain until the third day,37,43 two studies at a frequency of 1–2 times per week including menstruation,45,48 and two studies 1–3 times per week besides menstruation.47,49 Common acupoints included CV4 (Guanyuan), SP6 (Sanyinjiao), SP8 (Diji), ST29 (Guilai), and CV6 (Qihai). In addition, ten studies employed manual acupuncture,37–39,41,43–47,49 one opted for abdominal acupuncture,36 one utilized auricular acupuncture,40 one employed buccal acupuncture,48 and one used manual acupuncture and fire needle jointly.42 Key characteristics and outcomes are summarized in Table 1, while more details of interventions are presented in Table S3.
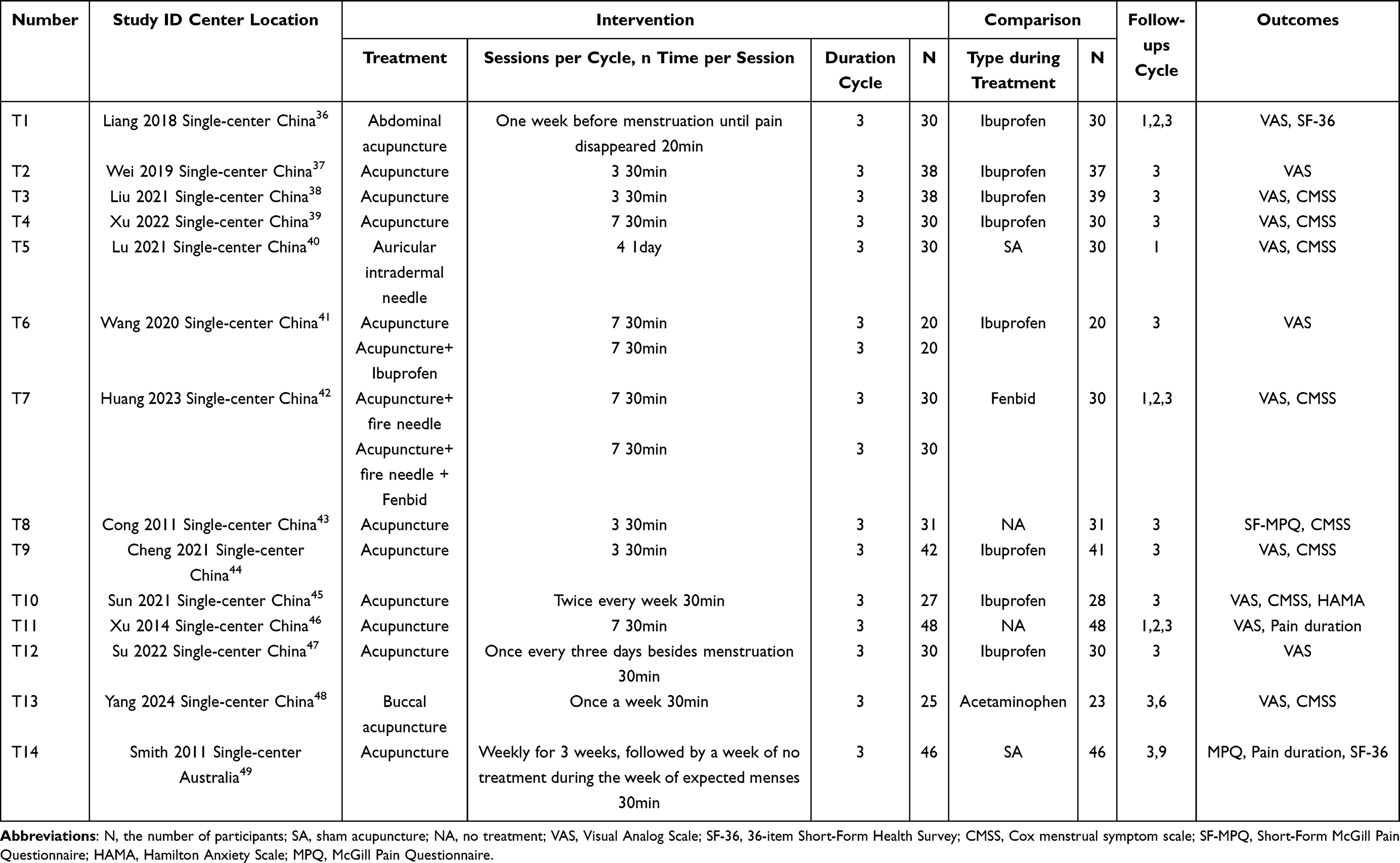 |
Table 1 Characteristics of Included Trials |
Risk of Bias
Five studies were rated as having a high risk of bias, and nine studies as having some concerns, as presented in Figures 2 and 3. With regard to the randomization process, one study was classified as having high risk of bias due to inappropriate random way,36 nine studies as having some concerns because the information allocation sequence concealed was missing.37–39,41–44,46,47 All studies were judged to have some concerns owing to the lack of sufficient description of the intervention deviation and appropriate analysis.36–49 For missing outcome data, three studies were evaluated in some concerns considering that more than 5% of loss to follow up might influence true value.36,45,48 The study by Smith et al was rated as of high risk due to the insufficient reasons for missing outcome data.49 As for outcome measurement, in consideration of patients might be influenced by knowledge of intervention received, ten studies comparing acupuncture with NSAIDs were rated as some concerns,36–39,41,42,44,45,47,48 two studies comparing acupuncture with no treatment and one study in which patient personally pressed the needle were rated as high risk.40,43,46 The risk of bias from selective reporting was determined to be some concern in ten studies due to the absence of registration information.36,37,41–43,45–47
 |
Figure 2 Risk of bias summary. |
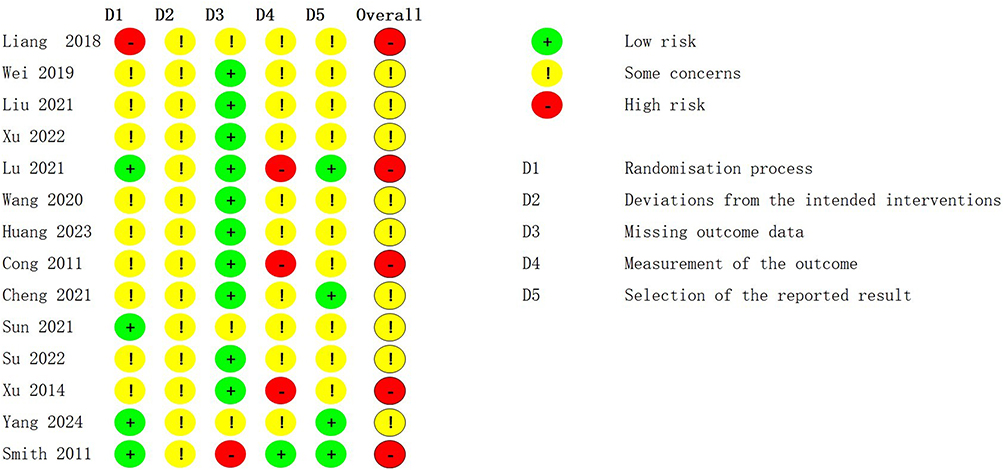 |
Figure 3 Risk of bias of each included study. |
Acupuncture Versus No Treatment
Two trials, with 158 participants, compared acupuncture with no treatment, suggesting that acupuncture might provide sustainable effect for 3 menstrual cycles.43,46
For primary outcomes, the two trials, conducted by Cong et al and Xu et al, assessed pain intensity using SF-MPQ and VAS scales separately.43,46 Both of trials revealed notable alleviation (p < 0.0001) from immediately after the last treatment to 3 menstrual cycles post-treatment (Figure 4, Figure S1–S6).43,46 The reduction of VAS achieved the MCID of 10mm up to 3 menstrual cycles after treatment.46
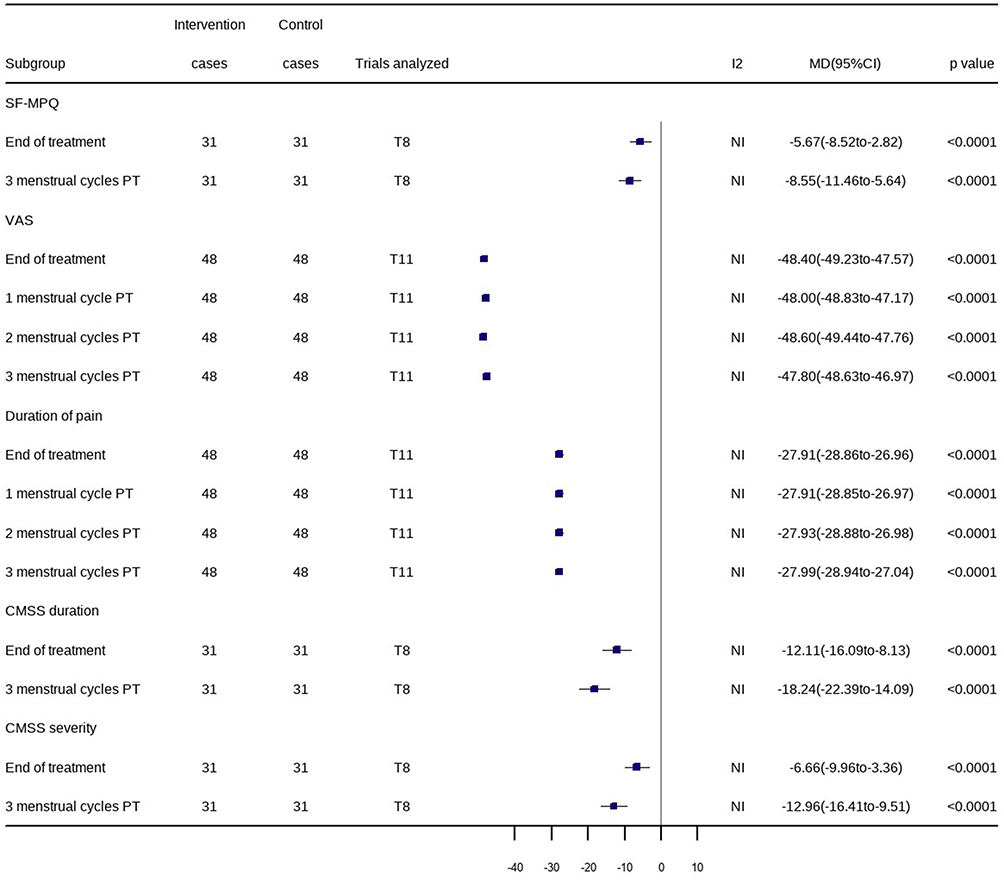 |
Figure 4 Acupuncture versus no treatment: changes from baseline in SF-MPQ, VAS, duration of pain, CMSS duration, and CMSS severity. |
As for secondary outcomes, the pain duration of patients receiving acupuncture was significantly reduced at 1 menstrual cycle (MD −27.91; 95% CI −28.85 to −26.97; p < 0.0001), 2 menstrual cycles (MD −27.93; 95% CI −28.88 to −26.98; p < 0.0001), and 3 menstrual cycles (MD −27.99; 95% CI −28.94 to −27.04; p < 0.0001) post-treatment (Figure 4, Figures S7–S10).46
For menstrual symptoms, acupuncture resulted in obviously declined CMSS duration score (MD −18.24; 95% CI −22.39 to −14.09; p < 0.0001) and severity score (MD −12.96; 95% CI −16.41 to −9.51; p < 0.0001) at the three-menstrual cycles post-treatment (Figure 4, Figures S11–S14).43
Acupuncture Versus SA
Two studies compared acupuncture with SA, including 152 participants.40,49 Regarding pain intensity, acupuncture provided significant improvement compared with SA only at 1 menstrual cycle (MD −19.79; 95% CI −25.60 to −13.98; p < 0.0001) post-treatment (Figures S15 and S16).40 Conversely, the MPQ by Smith et al suggested that acupuncture was not superior to SA at 3 and 9 menstrual cycles post-treatment (Figure 5, Figures S17–S19).49
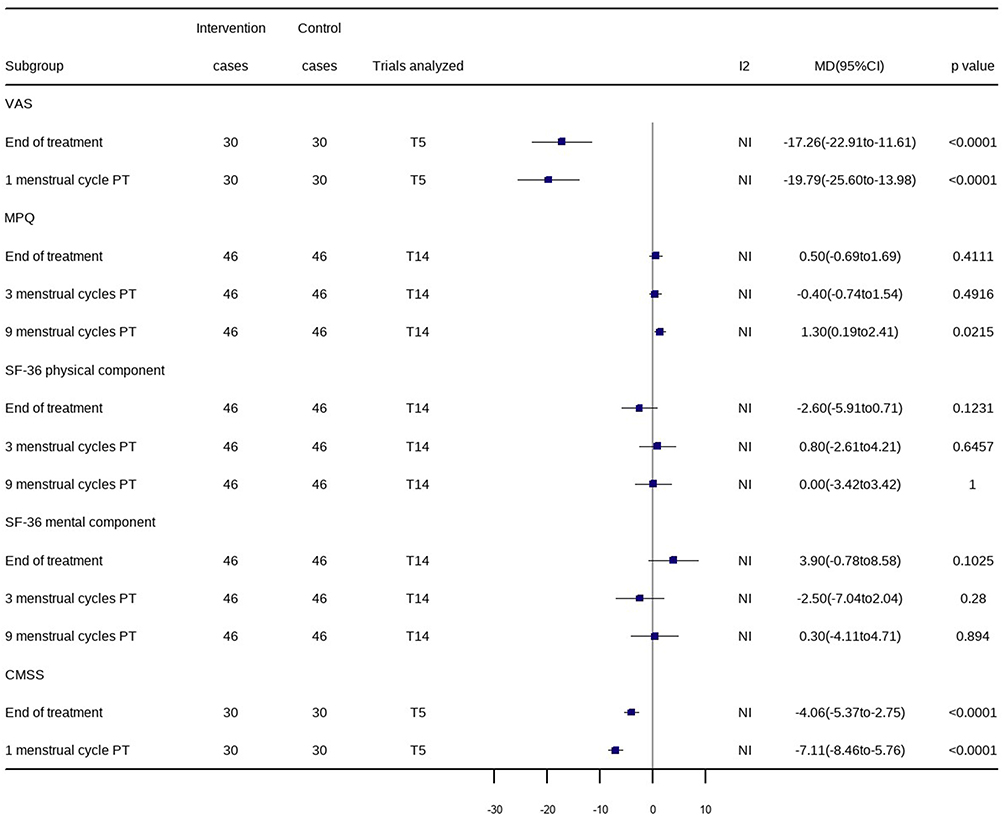 |
Figure 5 Acupuncture versus SA: changes from baseline in VAS, MPQ, SF-36 physical component, SF-36 mental component, and CMSS. |
As for the quality of life, no significant differences (p > 0.05) were observed in either physical or mental dimensions between the two groups at any of the follow-up points (Figure 5, Figures S20–S25).49
Acupuncture resulted in profound improvements in CMSS compared with SA at 1 menstrual cycle post-treatment (MD −7.11; 95% CI −8.46 to −5.76; p < 0.0001) (Figure 5, Figure S26 and S27).40
Smith et al also compared acupuncture with SA regarding pain duration, yet without data reported at baseline, precluding the calculation of pooled effect size estimates.49 Participants with acupuncture suffered shorter period of pain than those with SA at 3 menstrual cycles post-treatment (p < 0.05), while no benefits in pain duration were found immediately and at 9 menstrual cycles.49
Acupuncture Versus NSAIDs
Ten trials compared acupuncture with NSAIDs, with a total of 618 participants.36–39,41,42,44,45,47,48 The findings indicated that acupuncture might provide a lasting effect for PD for a minimum of six menstrual cycles. As for primary outcomes, obvious differences were found in pain intensity between two groups at 1 menstrual cycle (MD −30.08; 95% CI −49.29 to −10.88; p = 0.0021), 2 menstrual cycles (MD −29.59; 95% CI −48.41 to −10.78; p = 0.0021), 3 menstrual cycles (MD −29.89; 95% CI −37.63 to −22.15; p < 0.0001), and 6 menstrual cycles (MD −45.00; 95% CI −53.06 to −36.94; p < 0.0001) after treatment termination, and the difference exceeded the MCID of 10mm (Figure 6, Figures S28–S32).36–39,41,42,44,45,47,48
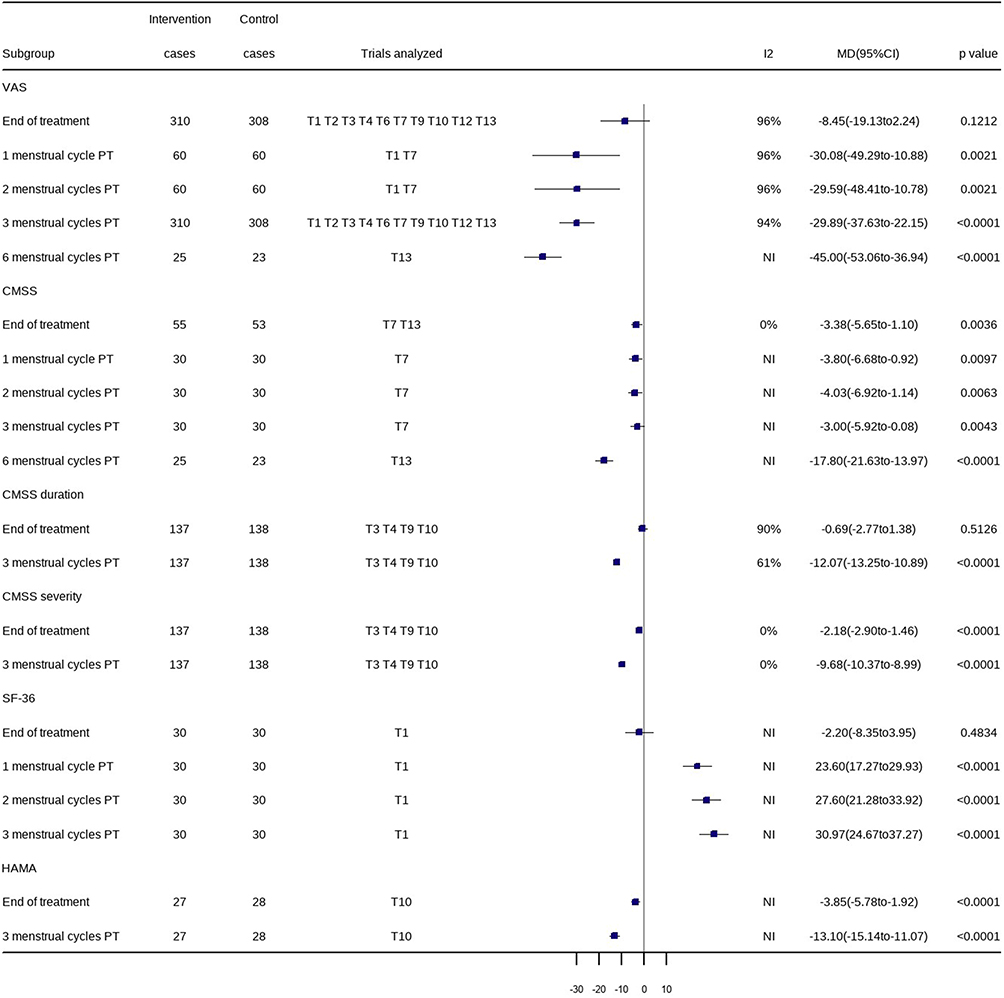 |
Figure 6 Acupuncture versus NSAIDs: changes from baseline in VAS, CMSS, CMSS duration, CMSS severity, SF-36, and HAMA. |
Because of the significant heterogeneity in the result of VAS at 3 menstrual cycles post-treatment (I2=94%), we used year, age and course of disease as covariates for meta-regression analysis. The result of meta-regression did not reveal association between year, age and course of disease effect size (p > 0.05). Thus, year, age and course of disease failed to explain the significant heterogeneity across studies. More details of meta-regression are presented in Table S4.36–39,41,42,44,45,47,48
Moreover, six studies evaluated the current pain during the visiting,36,39,42,44,47,48 two assessed the average intensity of menstrual pain,37,45 and two valued the maximum pain intensity during menstruation.38,41 All three types of measurements consistently showed that compared to NSAIDs, acupuncture reduced pain intensity up to 3 menstrual cycles after completion of treatment (Figure 7). Subgroup analysis based on the timing of intervention revealed significant improvement (p < 0.0001) across all groups in 3 menstrual cycles post-treatment (Figure 7).
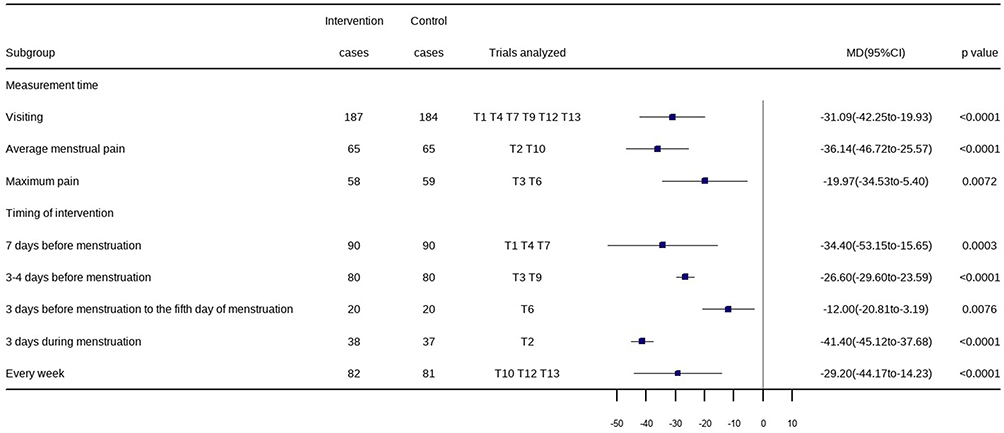 |
Figure 7 Subgroup analysis of acupuncture versus NSAIDs: changes from baseline in VAS at 3 menstrual cycles post-treatment. |
As for secondary outcomes, acupuncture led to evident improvement (p < 0.05) in total CMSS scale up to 6 menstrual cycles after completing the treatment (Figure 6, Figures S33–S37).42,48 Meanwhile, both CMSS duration score (MD −12.07; 95% CI −13.25 to −10.89; p < 0.0001) and severity score (MD −9.68; 95% CI −10.37 to −8.99; p < 0.0001) were reduced significantly at the three-menstrual cycles post-treatment, without evident improvement in CMSS duration at the end of treatment (Figure 6, Figures S38–S41).38,39,44,45
Analyses based on data in the study of Liang et al indicated that substantial enhancement in the quality of life for patients receiving acupuncture compared to NSAIDs at 1 menstrual cycle (MD 23.60; 95% CI 17.27 to 29.93; p < 0.0001), 2 menstrual cycles (MD 27.60; 95% CI 21.28 to 33.92; p < 0.0001), and 3 menstrual cycles (MD 30.97; 95% CI 24.67 to 37.27; p < 0.0001) post-treatment (Figure 6, Figures S42–S45).36
A study by Sun et al evaluated the long-lasting effect of HAMA, showing that acupuncture outperformed NSAIDs significantly in three menstrual cycles post-treatment (MD −13.10; 95% CI −15.14 to −11.07; p < 0.0001) (Figure 6, Figures S46 and S47).45
Acupuncture Plus NSAIDs Versus NSAIDs Alone
Two trials, with 100 patients, evaluated acupuncture plus NSAIDs versus NSAIDs alone.41,42 The pooled data indicated significant reduction in pain intensity in patients using acupuncture as an adjunct to NSAIDs at 1 menstrual cycle (MD −21.70; 95% CI −26.59 to −16.81; p < 0.0001), 2 menstrual cycles (MD −22.00; 95% CI −26.94 to −17.06; p < 0.0001), and 3 menstrual cycles post-treatment (MD −19.95; 95% CI −24.23 to −15.66; p < 0.0001) (Figure 8, Figure S48–S51).41,42 Each of these reductions met the MCID of 10mm.
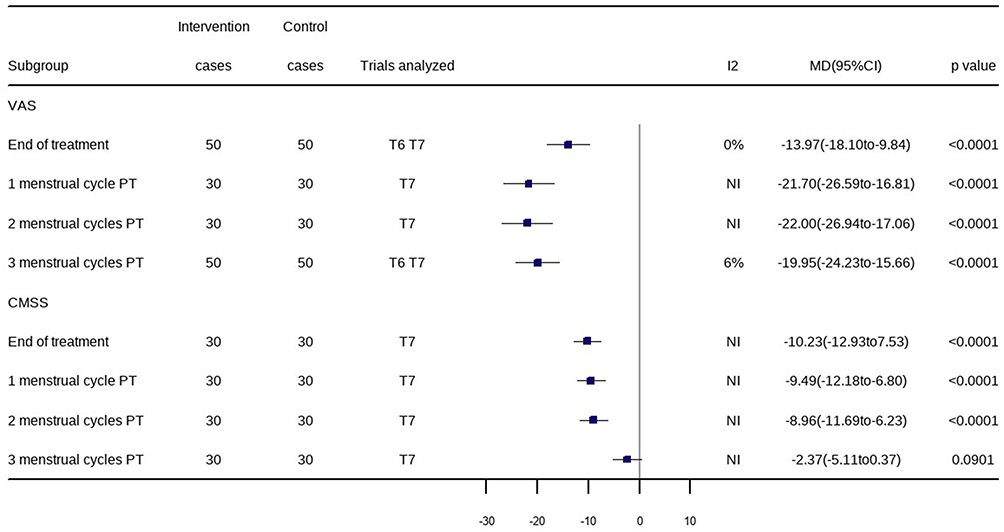 |
Figure 8 Acupuncture plus NSAIDs versus NSAIDs alone: changes from baseline in VAS, and CMSS. |
As for CMSS, acupuncture plus NSAIDs appeared to provide significant improvement up to 2 menstrual cycles post-treatment (p < 0.05), but the advantage was not maintained at 3 menstrual cycles post-treatment (Figure 8, Figure S52–S55).42
Adverse Events
Adverse events were reported in three trails.36,37,42 The main type of adverse events in acupuncture groups was subcutaneous hemorrhage. For the groups using NASID, gastrointestinal discomfort and dizzy were the primary problem. The pooled data showed that acupuncture was a safe treatment (OR: 0.62; 95% CI 0.16 to 2.44; p = 0.4922).
Sensitivity Analysis
In comparison of acupuncture and NSAIDs, the results of VAS, CMSS duration and CMSS severity at 3 menstrual cycles post-treatment were conducted sensitivity analysis by leave-one-out way. No single study altered the direction or statistical significance of the overall effect, which confirmed the robustness of results (Figures 9–11).36–39,41,42,44,45,47,48
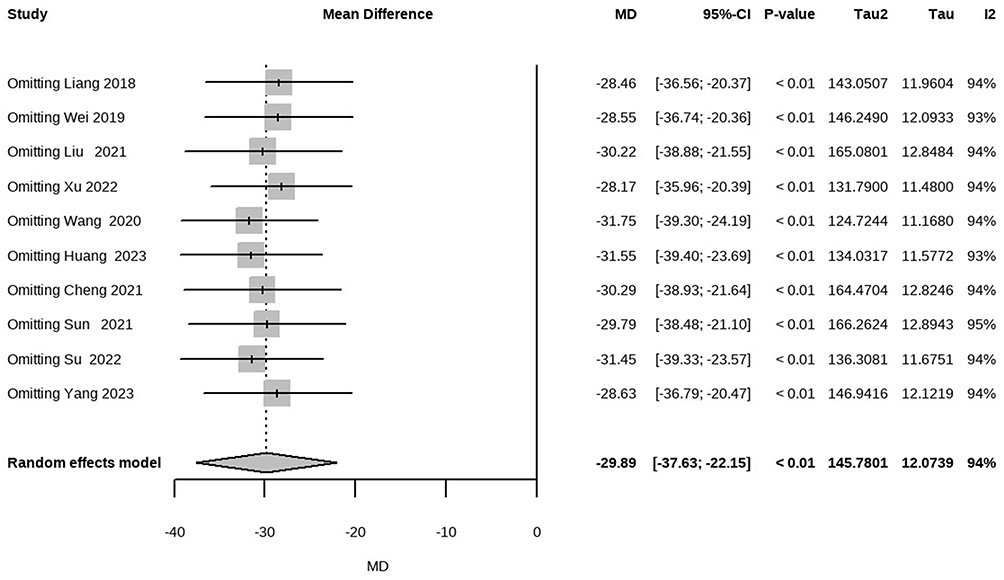 |
Figure 9 Sensitivity analysis of acupuncture versus NSAIDs: changes from baseline in VAS at 3 menstrual cycles post-treatment. |
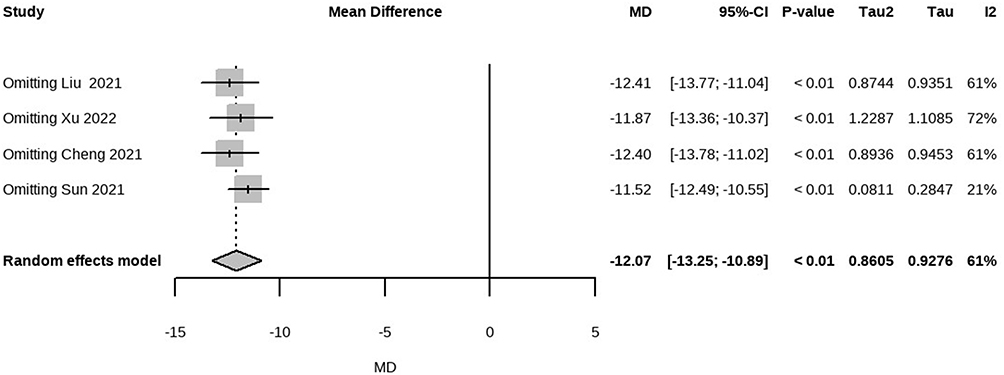 |
Figure 10 Sensitivity analysis of acupuncture versus NSAIDs: changes from baseline in CMSS duration at 3 menstrual cycles post-treatment. |
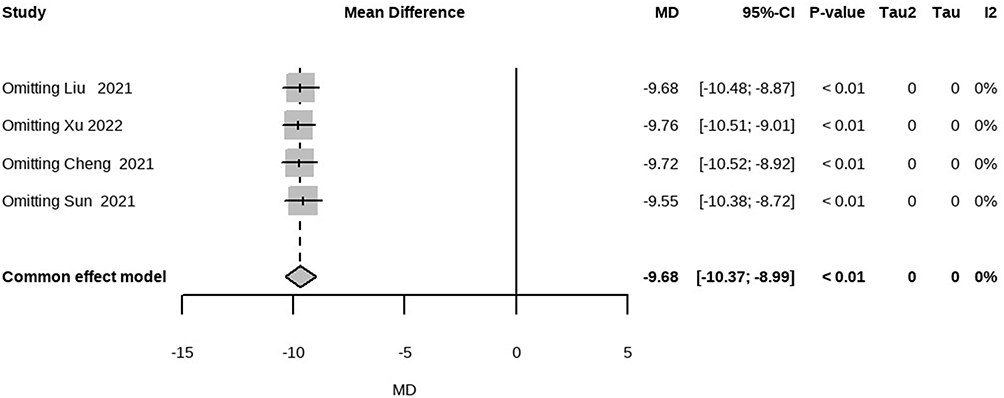 |
Figure 11 Sensitivity analysis of acupuncture versus NSAIDs: changes from baseline in CMSS severity at 3 menstrual cycles post-treatment. |
The sensitivity analysis, which employed different Corr (0.3 and 0.7), demonstrated that the overall effect size and heterogeneity varied only marginally, indicated that varying Corr did not influence the robustness of the results. More details of sensitivity analysis are presented in Figure S56 and S57.36–39,41,42,44,45,47,48
Publication Bias
Ten studies were included to analysis the difference in pain intensity between acupuncture and NSAIDs.36–39,41,42,44,45,47,48 According to the symmetric funnel diagram and result in Egger’ test (p = 0.4944), the authenticity of the results remained unaffected by publication bias (Figure 12).
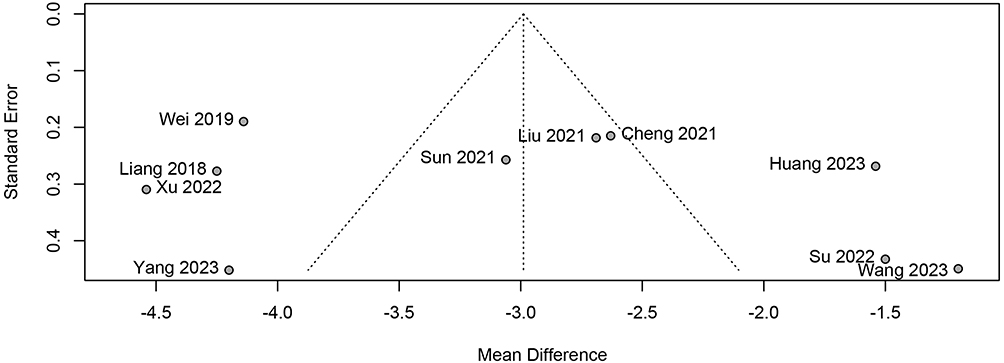 |
Figure 12 Funnel plot of VAS score in the comparison between acupuncture and NSAIDs at 3 menstrual cycles post-treatment. |
Quality of Evidence
The certainty of the evidence primarily ranged from very low to low, downgraded attributable to risk of bias, high heterogeneity, and inadequate sample sizes. More details of interventions are presented in Tables S5–S8.
Discussion
In this meta-analysis, we summarized the data to observe the durable effect of acupuncture for primary dysmenorrhea. According to above results, acupuncture presented a significant reduction in pain intensity, no matter compared with NSAIDs, no treatment and as complementary treatment at 3 menstrual cycles post-treatment. In addition, acupuncture outperformed NSAIDs and no treatment in alleviating menstrual symptoms at least 3 menstrual cycles after treatment. However, there was insufficient superiority of acupuncture compared with SA.
Globally, a substantial proportion of women may experience recurrent PD, necessitating treatments that offer long-lasting effect with minimal side effects. We conducted this systematic review and meta-analysis to examine the durable effects of acupuncture for PD on pain intensity, pain duration, menstrual symptom, quality of life and anxiety. In total, 14 studies with 970 participants were included in this meta-analysis.
Compared with no treatment, acupuncture revealed clinical improvement in pain intensity and considerable benefits in shortening pain duration and alleviating dysmenorrhea symptoms. Furthermore, comparing our research findings with those of conventional medications provided valuable insights. A meta-analysis on dysmenorrhea revealed that NSAIDs could reduce VAS scores by 34–65 points compared with placebo.12 In contrast, acupuncture emerged as a convenient and potentially widespread treatment option, as short-term acupuncture could provide relief for at least 3 menstrual cycles, and its effect was equivalent to that of regular use of NSAIDs.
The comparison of acupuncture versus NSAIDs provided further evidence for the above. During 3 cycles of follow-up periods after intervention, acupuncture provided significantly better relief of pain than NSAIDs, unaffected by publication bias and the difference of intervention and measurement. Additionally, acupuncture demonstrated a potential improvement in alleviating menstrual symptoms, enhancing quality of life, and mitigating psychological issues. However, these findings should be accepted with caution due to the presence of significant heterogeneity, which might be ascribed to the type of acupuncture, selection of acupoints, timing of interventions, and so on.
Meanwhile, acupuncture as adjunct to NSIADs, compared to NSAIDs alone, achieved more obvious pain relief for up to 3 menstrual cycles post-treatment, with improved menstrual symptoms for up to 2 menstrual cycles post-treatment.
The exploration of acupuncture versus SA was thought-provoking. Lu et al in China revealed that acupuncture significantly reduced VAS and CMSS scores in PD patients, demonstrating sustained benefits after one menstrual cycle.40 Conversely, Smith et al found no notable advantages of acupuncture over SA in alleviating pain intensity or enhancing quality of life, except for a reduction in pain duration at three cycles post-treatment.49 They proposed that the placebo effect was a potential factor associated with pain-alleviating effect of acupuncture. More importantly, pain alleviation was generally assessed based on the self-reported information, and this type of subjective data might be more susceptible to the impact of the placebo effect and the effectiveness of blindness. Similarly, a prior meta-analysis enrolled 1,270 patients to explore the placebo effect of SA on PD, and showed that placebo response was significant in pain intensity (SMD −0.99; 95% CI −1.31 to −0.68; p < 0.05), symptom scale (total frequency rating score: SMD −0.20; 95% CI −0.80 to −0.39; and average severity score: SMD −0.35; 95% CI −0.90 to −0.20; both p < 0.05).50 The analysis of the fundamental mechanisms underlying the placebo response substantiated our hypothesis. This review demonstrated that placebo induces therapeutic effects via activation of endogenous opioid and dopaminergic neurochemical pathways. The placebo effect size in randomized controlled trials was approximately 40% in functional neurological disorders, including PD.51 In view of the above, the role of placebo effect cannot be directly excluded in the above positive results of acupuncture. Therefore, acupuncture exhibits comprehensive clinical effect for PD, involving the placebo effect possibly. Furthermore, the disparity between the two interventions may serve as a confounding variable influencing the outcomes. Specifically, LU et al employed auricular acupuncture, whereas Smith et al utilized conventional acupuncture. Additionally, the intervention protocols differed in terms of frequency and treatment duration. LU et al administered four consecutive sessions prior to menstruation, with each stimulation lasting one day, while Smith et al conducted shorter duration and lower frequency with weekly sessions lasting 30 minutes. Therefore, future research necessitates more rigorous experimental studies to further investigate the differential therapeutic efficacy between acupuncture and sham acupuncture.
Our study included 14 RCTs for investigation, which was an improvement compared with previous reviews, providing more evidence of the long-lasting effect of acupuncture on PD. In the systematic review conducted by Smith et al, the comparative analysis encompassed acupuncture versus sham acupuncture, NSAIDs, and no treatment. This was different from our review. Primarily, our review emphasized the sustained effects of acupuncture across multiple control groups, including sham acupuncture, no treatment, and NSAIDs. Conversely, Smith et al focused solely on the long-term efficacy of acupuncture relative to sham acupuncture. Additionally, our analysis incorporated more studies and provided detailed assessments of pain duration in the acupuncture versus sham acupuncture comparison, which were absent in Smith et al’ s review. Consequently, our findings supported the conclusion that acupuncture exerts a durable analgesic effect, a conclusion that conflicts with Smith et al.26 The review by Woo et al enrolled 60 trails with 5,901 participants in 2018, and focused on assessment of immediate effect on pain reduction of PD sufferers.
The acupuncture is a potential treatment for dysmenorrhea in clinic, but the mechanism of acupuncture to relieve dysmenorrhea remains incomplete. It is considered to be related to the increase of endogenous opioid peptide content and the anti-inflammatory effect mediated by hypothalamus-pituitary-adrenal axis.52
There are several limitations in this study. First, the sample size was insufficient, comprising only 970 participants. Second, all included trails exhibited high or considerable risk of bias. Third, the effect evaluations were mainly based on subjective scales. Moreover, the outcome measurement was not standardized in different articles, possibly reducing accuracy. Additionally, some of the results were highly heterogeneous and unexplained. Thus, the results should be interpreted with caution. High-quality randomized trials with standardized outcome measures and longer follow-up are urgently needed.
Conclusion
Acupuncture might offer sustained analgesic and symptomatic benefits for primary dysmenorrhea patients for up to three menstrual cycles after treatment completion. However, these results were limited by high risk of bias and low certainty evidence. Future studies with rigorous design and extended follow-up are urgently needed to further investigate the long-lasting effect of acupuncture.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Abbreviations
PD, primary dysmenorrhea; NSAIDs, non-steroidal anti-inflammatory drugs; TENS, transcutaneous electrical nerve stimulation; SA, sham acupuncture; PRISMA, Preferred Reporting Items for Systematic Review and Meta-Analysis; PROSPERO, the International Prospective Register of Systematic Reviews; CNKI, China National Knowledge Infrastructure; CBM, China Biology Medicine disc; Mesh, medical Subject Headings; RCTs, randomized controlled trials; SD, Standard Deviation; Corr, correlation coefficients; VAS, Visual Analog Scale; NRS, Numerical Rating Scale; BPI, Brief Pain Inventory; MPQ, McGill Pain Questionnaire; SF-MPQ, Short-Form McGill Pain Questionnaire; MCIDs, minimal clinically important differences; CMSS, Cox menstrual symptom scale; RSS, Cox retrospective symptom scale; MSS, menstrual symptom score; SF-36, 36-item Short-Form Health Survey; HAMA, Hamilton Anxiety Scale; GRADE, Grading of Recommendations Assessment, Development, and Evaluation; MD, mean differences; CI, confidence interval; OR, odds ratio; PT, post-treatment.
Data Sharing Statement
All data generated in this review are available from the corresponding author upon reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the High Level Chinese Medical Hospital Promotion Project [Grant numbers HLCMHPP2023089] and Self-designed project of Guang ‘anmen Hospital [Grant numbers 137].
Disclosure
The authors have declared that no competing interests exist in this work.
References
1. Martire FG, d’Abate C, Schettini G, et al. Adenomyosis and adolescence: a challenging diagnosis and complex management. Diagnostics. 2024;14(21):2344. doi:10.3390/diagnostics14212344
2. D’Urso V, Gulino FA, Incognito GG, et al. Hysteroscopic findings and operative treatment: all at once? J Clin Med. 2023;12(13):4232. doi:10.3390/jcm12134232
3. Kho KA, Shields JK. Diagnosis and management of primary dysmenorrhea. JAMA. 2020;323(3):268. doi:10.1001/jama.2019.16921
4. Wang L, Yan Y, Qiu H, et al. Prevalence and risk factors of primary dysmenorrhea in students: a meta-analysis. Value Health. 2022;25(10):1678–1684. doi:10.1016/j.jval.2022.03.023
5. Chen L, Tang L, Guo S, Kaminga AC, Xu H. Primary dysmenorrhea and self-care strategies among Chinese college girls: a cross-sectional study. BMJ open. 2019;9(9). doi:10.1136/bmjopen-2018-026813
6. ACOG Committee Opinion No 760.Dysmenorrhea and endometriosis in the adolescent. Obstetrics Gynecol. 2018;132(6):e249. doi:10.1097/AOG.0000000000002978
7. Burnett M, Lemyre MN. 345-primary dysmenorrhea consensus guideline. J Obstet Gynaecol Canada. 2017;39(7):585–595. doi:10.1016/j.jogc.2016.12.023
8. Schoep ME, Nieboer TE, van der Zanden M, Braat DDM, Nap AW. The impact of menstrual symptoms on everyday life: a survey among 42,879 women. Am J Obstet Gynecol. 2019;220(6):569.e1–569.e7. doi:10.1016/j.ajog.2019.02.048
9. Ferries-Rowe E, Corey E, Archer JS. Primary dysmenorrhea: diagnosis and therapy. Obstet Gynecol. 2020;136(5):1047–1058. doi:10.1097/AOG.0000000000004096
10. Barcikowska Z, Rajkowska-Labon E, Grzybowska ME, Hansdorfer-Korzon R, Zorena K. Inflammatory markers in dysmenorrhea and therapeutic options. Int J Environ Res Public Health. 2020;17(4):1191. doi:10.3390/ijerph17041191
11. Kirsch E, Rahman S, Kerolus K, et al. Dysmenorrhea, a narrative review of therapeutic options. J Pain Res. 2024;17:2657–2666. doi:10.2147/JPR.S459584
12. Marjoribanks J, Ayeleke RO, Farquhar C, Proctor M. Nonsteroidal anti-inflammatory drugs for dysmenorrhoea. Cochrane Database Syst Rev. 2015;2015(7):CD001751. doi:10.1002/14651858.CD001751.pub3
13. Oladosu FA, Tu FF, Hellman KM. Nonsteroidal antiinflammatory drug resistance in dysmenorrhea: epidemiology, causes. and Treatment Am J Obstet Gynecol. 2018;218(4):390–400. doi:10.1016/j.ajog.2017.08.108
14. O’Connell K, Davis AR, Westhoff C. Self-treatment patterns among adolescent girls with dysmenorrhea. J Pediatr Adolesc Gynecol. 2006;19(4):285–289. doi:10.1016/j.jpag.2006.05.004
15. Manzoli L, De Vito C, Marzuillo C, Boccia A, Villari P. Oral contraceptives and venous thromboembolism: a systematic review and meta-analysis. Drug Saf. 2012;35(3):191–205. doi:10.2165/11598050-000000000-00000
16. Schroll JB, Black AY, Farquhar C, Chen I. Combined oral contraceptive pill for primary dysmenorrhoea. Cochrane Database Syst Rev. 2023;7(7):CD002120. doi:10.1002/14651858.CD002120.pub4
17. Damm T, Lamvu G, Carrillo J, Ouyang C, Feranec J. Continuous vs. cyclic combined hormonal contraceptives for treatment of dysmenorrhea: a systematic review. Contracept X. 2019;1:100002. doi:10.1016/j.conx.2019.100002
18. Ekelund M, Melander M, Gemzell-Danielsson K. Intrauterine contraception: attitudes, practice, and knowledge among Swedish health care providers. Contraception. 2014;89(5):407–412. doi:10.1016/j.contraception.2013.12.014
19. Wemrell M, Gunnarsson L. Attitudes toward the copper IUD in Sweden: a survey study. Front Glob Womens Health. 2022;3:920298. doi:10.3389/fgwh.2022.920298
20. Armour M, Ee CC, Naidoo D, et al. Exercise for dysmenorrhoea. Cochrane Database Syst Rev. 2019;9(9):CD004142. doi:10.1002/14651858.CD004142.pub4
21. Han S, Park KS, Lee H, et al. Transcutaneous electrical nerve stimulation (TENS) for pain control in women with primary dysmenorrhoea. Cochrane Database Syst Rev. 2024;7(7):CD013331. doi:10.1002/14651858.CD013331.pub2
22. Bleck R, Marquez E, Gold MA, Westhoff CL. A scoping review of acupuncture insurance coverage in the United States. Acupunct Med. 2021;39(5):461–470. doi:10.1177/0964528420964214
23. Robinson N, Lorenc A, Ding W, Jia J, Bovey M, Wang XM. Exploring practice characteristics and research priorities of practitioners of traditional acupuncture in China and the EU-A survey. J Ethnopharmacol. 2012;140(3):604–613. doi:10.1016/j.jep.2012.01.052
24. Smith CA, Armour M, Betts D. Treatment of women’s reproductive health conditions by Australian and New Zealand acupuncturists. Complement Ther Med. 2014;22(4):710–718. doi:10.1016/j.ctim.2014.06.001
25. Woo HL, Ji HR, Pak YK, et al. The efficacy and safety of acupuncture in women with primary dysmenorrhea: a systematic review and meta-analysis. Medicine. 2018;97(23):e11007. doi:10.1097/MD.0000000000011007
26. Smith CA, Armour M, Zhu X, Li X, Lu ZY, Song J. Acupuncture for dysmenorrhoea. Cochrane Database Syst Rev. 2016;4(4):CD007854. doi:10.1002/14651858.CD007854.pub3
27. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. J Clin Epidemiol. 2021;134:178–189. doi:10.1016/j.jclinepi.2021.03.001
28. Cochrane Handbook for Systematic Reviews of Interventions. Available from: https://training.cochrane.org/handbook/current.
29. Li H, Wang L, Feng J, Jiang L, Wu J. Effects of oral intake fruit or fruit extract on skin aging in healthy adults: a systematic review and meta-analysis of randomized controlled trials. Front Nutr. 2023;10:1232229. doi:10.3389/fnut.2023.1232229
30. Yu J, Xia J, Yang C, et al. Effects of oat beta-glucan intake on lipid profiles in hypercholesterolemic adults: a systematic review and meta-analysis of randomized controlled trials. Nutrients. 2022;14(10):2043. doi:10.3390/nu14102043
31. de Arruda GT, Driusso P, Rodrigues JC, de Godoy AG, Avila MA. Numerical rating scale for dysmenorrhea-related pain: a clinimetric study. Gynecol Endocrinol. 2022;38(8):661–665. doi:10.1080/09513590.2022.2099831
32. Bourdel N, Alves J, Pickering G, Ramilo I, Roman H, Canis M. Systematic review of endometriosis pain assessment: how to choose a scale? Hum Reprod Update. 2015;21(1):136–152. doi:10.1093/humupd/dmu046
33. Wang YL, Zhu HL. The prevalence and associated risk factors of primary dysmenorrhea among women in Beijing: a cross-sectional study. Sci Rep. 2025;15(1):5003. doi:10.1038/s41598-025-89038-5
34. Xiang XN, Wang ZZ, Hu J, et al. Telehealth-supported exercise or physical activity programs for knee osteoarthritis: systematic review and meta-analysis. J Med Internet Res. 2024;26:e54876. doi:10.2196/54876
35. Balduzzi S, Rücker G, Schwarzer G. How to perform a meta-analysis with R: a practical tutorial. Evid Based Ment Health. 2019;22(4):153–160. doi:10.1136/ebmental-2019-300117
36. Liang RL, Wang LN, Wang LP, et al. Clinical observation of abdominal acupuncture treating primary dysmenorrhea. J Clin Acupun Moxibus. 2018;34(02):16–19.
37. Wei YH, Li WJ, Fan HX. Immediate and long-term analgesic effect of baliao points daoqi method in treating primary dysmenorrhea. Acta Chinese Medicine. 2019;34(12):2687–2691. doi:10.16368/j.issn.1674-8999.2019.12.616
38. Liu RP, Cheng XM, Wang YJ. Observation on the curative effect of the method of “ tonifying the spleen and stomach, regulating Ren Meridian” on primary dysmenorrhea with Qi-blood deficiency. Mod J Integr Traditional Chin Western Med. 2021;30(29):3218–3221+3256. doi:10.3969/j.issn.1008-8849.2021.29.006
39. Xu XQ, Yuan Q. Clinical study on Jin’s three-needle acupuncture therapy for the treatment of primary dysmenorrhea of cold accumulation causing blood stasis type. J Guangzhou Univ Traditional Chin Med. 2022;39(08):1836–1840. doi:10.13359/j.cnki.gzxbtcm.2022.08.022
40. Lu CX, Deng XJ, Chen M, et al. Different stimulation methods on auricular points for primary dysmenorrhea: a randomized controlled trial. Zhongguo Zhen Jiu. 2021;41(7):737–741. doi:10.13703/j.0255-2930.20200531-k0002
41. Wang XH, Huang F, Zhao Y. Clinical study of Dong’s Qi acupoint combined with ibuprofen in treatment of dysmenorrhea of cold coagulation and stasis type. Hubei J Traditional Chin Med. 2020;42(01):10–13.
42. Huang LY, Liu RQ, Shen MX. Clinical observation on the treatment of primary dysmenorrhea with Hershey’s acupuncture and moxibustion combined with Fenbid. J Emerge Traditional Chin Med. 2023;32(02):288–290. doi:10.3969/j.issn.1004-745X.2023.02.026
43. Cong X, Liu GX, Lin XY, et al. Analgesic effects of primary dysmenorrhea treated with acupuncture. J Shandong Univ Traditiona Chin Med. 2011;35(03):224–225+257. doi:10.16294/j.cnki.1007-659x.2011.03.001
44. Cheng XM, Liu RP, Wang YJ. Clinical Study on Acupuncture for Treatment of Primary Dysmenorrhea of Cold Coagulation and Blood Stasis by “Tonifying Spleen and Stomach, Regulating Ren Meridian”. Chin J Inf Traditional Chin Med. 2021;28(02):102–106. doi:10.19879/j.cnki.1005-5304.202008133
45. Sun T, Wang SL, Zhu SP. Therapeutic effects of sequential-acupuncture therapy on pain and anxiety of patients with primary dysmenorrhea. J Zhejiang Chin Med Univ. 2021;45(01):70–74. doi:10.16466/j.issn1005-5509.2021.01.014
46. Xu SW, Yu C, Zhao JP, et al. Observation on analgesic effect and curative effect of premenstrual acupuncture on primary dysmenorrhea. Beijing J Tradit Chinese Med. 2014;33(01):41–43. doi:10.16025/j.1674-1307.2014.01.019
47. Su JP, Lin C. Observation on the effect of “ S” ring acupuncture of Zhuang medicine in the treatment of Gingin disease (primary dysmenorrhea). J Guangxi Univ Chin. 2022;25(03):23–25.
48. Yi Y, Huijun Y, Huiling Z, Lihua J. Clinical observation on 90 cases of primary dysmenorrhea treated by buccal acupuncture therapy: a randomized controlled study. J Traditional Chin Med. 2024;44(1):172–181. doi:10.19852/j.cnki.jtcm.20231110.001
49. Smith CA, Crowther CA, Petrucco O, Beilby J, Dent H. Acupuncture to treat primary dysmenorrhea in women: a randomized controlled trial. Evid Bsed Compl Alternat Med. 2011;2011(1):612464. doi:10.1093/ecam/nep239
50. Sun CY, Xiong ZY, Sun CY, et al. Placebo response of sham acupuncture in patients with primary dysmenorrhea: a meta-analysis. J Integr Med. 2023;21(5):455–463. doi:10.1016/j.joim.2023.08.005
51. Enck P, Benedetti F, Schedlowski M. New insights into the placebo and nocebo responses. Neuron. 2008;59(2):195–206. doi:10.1016/j.neuron.2008.06.030
52. Qiao L, Guo M, Qian J, Xu B, Gu C, Yang Y. Research advances on acupuncture analgesia. Am J Chin Med. 2020;48(2):245–258. doi:10.1142/S0192415X20500135
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Efficacy and Safety of Acupuncture for Tinnitus-Associated Insomnia: A Protocol for a Systematic Review and Meta-Analysis
Fan L, Gao Y, Zhou J, Hu H, Gao H
Journal of Pain Research 2022, 15:2957-2965
Published Date: 21 September 2022
The Analgesic Effect and Potential Mechanisms of Acupuncture for Migraine Rats: A Systematic Review and Meta-Analysis
Sun S, Liu L, Zhou M, Liu Y, Sun M, Zhao L
Journal of Pain Research 2023, 16:2525-2542
Published Date: 24 July 2023
Efficacy of Acupuncture in Acute Exacerbation of Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis
Yang C, Tian H, Xu G, Luo Q, Sun M, Liang F
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:707-720
Published Date: 11 March 2024
Manual Therapy in Primary Dysmenorrhea: A Systematic Review and Meta-Analysis
Li X, Sun Y, Wang Y, Wang X, Yu C
Journal of Pain Research 2024, 17:1663-1681
Published Date: 6 May 2024
Acupuncture and Moxibustion in the Treatment of Gynecological Perioperative Anxiety: A Systematic Review and Meta-Analysis
Wang X, Yu Q, Zhu J, Liu J, Gao X, Wang X, Wang L, Xu X
Journal of Pain Research 2024, 17:3515-3538
Published Date: 31 October 2024