Back to Journals » Journal of Pain Research » Volume 19
Long-Acting versus Short-Acting Opioids and Opioid-Related Disorders in Chronic Non-Cancer Pain: A Claims Data Analysis in Germany
Authors Brinkmöller S ![]() , Poß-Doering R
, Poß-Doering R ![]() , Straßner C, Laux G
, Straßner C, Laux G ![]()
Received 27 January 2026
Accepted for publication 3 May 2026
Published 3 June 2026 Volume 2026:19 599161
DOI https://doi.org/10.2147/JPR.S599161
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Timothy Atkinson
Sabrina Brinkmöller, Regina Poß-Doering, Cornelia Straßner, Gunter Laux
Department of Primary Care and Health Services Research, Heidelberg University, Medical Faculty, Heidelberg University Hospital, Heidelberg, Germany
Correspondence: Sabrina Brinkmöller, Department of Primary Care and Health Services Research, Heidelberg University, Medical Faculty, Heidelberg University Hospital, Im Neuenheimer Feld 130.3, Heidelberg, 69120, Germany, Email [email protected]
Background: Chronic non-cancer pain is common in primary care and may be managed with long-term opioid therapy. The German guideline “Long-term Use of Opioids for Chronic Non-Cancer Pain” provides recommendations for such treatment. The role of opioid formulation (long-acting vs. short-acting) and the association with opioid-related disorders remains underexplored. This study aims to explore associations between opioid formulation and opioid-related disorders in patients with chronic non-cancer pain receiving long-term opioid therapy in German general practices.
Methods: We conducted a retrospective cross-sectional claims data analysis using data from one statutory health insurer in Baden-Württemberg (AOK), Germany, for the year 2021. The analysis included patients aged ≥ 18 years who received at least one oral or transdermal opioid prescription in all four quarters. Exclusion criteria were malignant diseases or palliative care. The outcome was opioid-related disorder (ICD-10 category F11.-). Multivariable logistic regression analyses were performed to identify predictors.
Results: Multiple models were calculated. The main model included a total of 34,205 patients. The mean age was 70 years, and 65% were female. Overall, 3.1% of patients were diagnosed with an opioid-related disorder. Weak opioids were most frequently prescribed. Long-acting opioids predominated. Higher odds of opioid-related disorders were observed in patients with substance use disorders involving such as sedatives (OR = 5.6, 95% CI: 4.48– 7.01) or alcohol (OR = 2.2, 95% CI: 1.82– 2.66). Short-acting opioids (OR = 2.0, 95% CI: 1.53– 2.48) and combined long- and short-acting therapy (OR = 3.5, 95% CI: 2.38– 5.00) were associated with higher odds of opioid-related disorders compared with long-acting opioids (all p < 0.001).
Conclusion: The results suggest that short-acting opioids, either alone or as part of combination therapy, may be more strongly associated with opioid-related disorders in patients with chronic non-cancer pain and long-term opioid therapy than long-acting opioids alone. Further research is needed to clarify these relationships and their underlying causes.
Keywords: chronic non-cancer pain, primary care, general practice, long-term opioid therapy, opioid-related disorders, opioid formulation, long-acting opioids, short-acting opioids, Germany
Introduction
Chronic pain is commonly defined as pain that persists or recurs for more than three months and extends beyond the expected period of tissue healing.1 It is recognised as a distinct disease entity that is often associated with significant functional limitations and psychosocial distress. It places a high burden of suffering on those affected.1,2 The management of chronic pain typically involves multimodal treatment strategies that integrate both pharmacological and non-pharmacological interventions.2 Opioids can be part of this multimodal approach when prescribed and monitored carefully.3 While considered an essential component in the treatment of cancer-related pain, the use of opioids for chronic non-cancer pain (CNCP) has been the subject of ongoing debate.4 For most patients with CNCP, current evidence shows that opioids are no more effective than non-opioid analgesics or non-pharmacological interventions in improving pain intensity or functional outcomes over a period of more than six months.5,6 In addition to questions of efficacy, potential risks must also be considered, including the development of tolerance, loss of analgesic effect, and the occurrence of opioid-related mental and behavioral disorders (ORD).3 Nevertheless, different guidelines acknowledge that opioid therapy may be considered for certain CNCP conditions when other analgesics or non-pharmacological interventions do not provide adequate pain relief.3,4 However, long-term opioid therapy for CNCP remains controversial.7–11 Definitions of long-term opioid therapy vary internationally. The German “Long-term Use of Opioids for Chronic Non-Cancer Pain” (LONTS) guideline defines long-term treatment durations in studies as 26 weeks or longer (approximately six months), while, from a clinical perspective, long-term opioid therapy is already considered to begin after more than three months of treatment.3 Some long-term opioid therapy patients may develop hyperkatifeia (reduced reward system responsiveness) leading to apathy, depressed mood, irritability, and emotional dysregulation.12 This state can reduce analgesic effect without worsening of the underlying pain, increasing the likelihood of continued opioid use to avoid negative emotions and potentially fostering dose escalation, dependence, and misuse.12 Data from the United States indicate that long-term opioid therapy for certain CNCP conditions does not improve function or return-to-work rates and increases healthcare costs.12 An analysis funded by the Federal Institute for Drugs and Medical Devices (BfArM) of 25 million insured individuals in Germany found that the age- and sex-standardized prevalence of opioid analgesic prescriptions declined by 19% between 2005 and 2020 (from 52.3 to 42.4 per 1,000 individuals). There was only an increase among patients aged 80 years and over, followed by a minor decline after 2020.13 Despite the fall in prescriptions, the total number of oral morphine milligram equivalents (MME) increased by 51% (from 191,987 mg to 290,733 mg per 1,000 person-years) until 2016, particularly among patients aged 60 and over. Thereafter, the total MME declined by 5.3% until 2020. Approximately 18% of new opioid recipients met long-term opioid therapy criteria, most for CNCP.13 No evidence of an opioid crisis exists in Germany, but careful monitoring of long-term opioid therapy patients remains essential.13
General practitioners (GPs) are the primary opioid prescribers in Germany, where around 20% of patients in general practice report pain lasting more than three months.14,15 GPs thus play a central role in assessing suitability, managing risks, and monitoring ORD in patients with CNCP.15–17 In the International Classification of Diseases – 10th Revision – German Modification (ICD-10-GM), ORD are classified under F11.-, encompassing conditions from harmful use (F11.1) and dependence (F11.2) to acute intoxication (F11.0), psychotic disorders (F11.5), and amnesic syndromes (F11.6).18 These conditions reflect the spectrum of opioid-related problems, ranging from misuse to psychiatric complications. Clinical indicators of misuse may include inconsistent pain reports, requests for specific formulations, or obtaining redundant prescriptions from multiple providers.3 The boundary between medically justified use and harmful or non-medical consumption is often fluid, which complicates the timely identification of problematic patterns.3 Due to the complex nature of ORD, it is essential to identify predictors in order to reduce their likelihood and improve patient safety. However, data on the prevalence of ORD in Germany remain limited. According to the German Epidemiological Survey of Substance Abuse of 2018, approximately 5,5 million individuals aged 18–59 are affected by disorders related to analgesic use overall, with a substantial proportion likely attributable to opioids.19 Internationally, significant increases in opioid misuse and transitions to illicit opioid use have been observed, particularly in North America, Australia, and parts of Europe.20 The number of individuals using illicit opioids in Germany is estimated to exceed 200,000, with a considerable degree of underreporting.19
However, data specifically addressing ORD among patients with chronic non-cancer pain in primary care remain scarce, highlighting the need for further investigation in this population. The impact of opioid formulations on ORD remains underexplored and international guidelines differ regarding a preferred formulation.21 While some guidelines recommend the use of long-acting opioids (LAOs),3,22,23 American and Canadian guidelines24,25 take a more cautious stance and emphasize potential risks associated with LAOs. The German LONTS guideline3 recommends the use of LAOs over short-acting opioids (SAOs) in long-term opioid therapy due to their presumed lower potential for misuse, although this recommendation is not supported by high-quality studies.3 This recommendation is based more on considerations such as medication adherence, analgesic effectiveness, and general safety profiles than on robust evidence specifically addressing the relationship between opioid formulations and ORD. Existing studies provide inconsistent findings and are often limited by methodological constraints, leaving uncertainty as to whether formulation type independently influences the risk of ORD. Given these limitations, large-scale routine claims data provide a pragmatic and ecologically valid opportunity to examine real-world prescribing patterns and their association with ORD in primary care.
To explore the role of different opioid formulations, this observational study aims to identify predictors of ORD among patients with CNCP receiving long-term opioid therapy in general practice in Germany.
Methods
Context
This study is part of the RELIEF project (Resource-oriented case management to implement recommendations for patients with chronic pain and frequent analgesic use in general practice),26 funded by the German Federal Ministry of Research, Technology and Space (former BMBF/now BMFTR, funding code 01GY2106). The study was approved by the Ethics Committee of Heidelberg University’s Faculty of Medicine (S-087/2023) and authorised by the German Federal Office for Social Security for the use of claims data. Both institutions reviewed and approved the study methodology, confirming that all procedures comply with the relevant national and institutional guidelines and regulations. All methods were performed in accordance with the relevant guidelines and regulations for claims data. As this was a study involving secondary data analysis, the Ethics Committee of the Medical Faculty of Heidelberg (S-087/2023) waived the need to obtain informed consent, in agreement with the data holder (AOK health insurance). The data holder’s specific decision process is described in detail in the Ethics approval and consent to participate section.
Study Design
This observational study used claims data submitted for reimbursement purposes to AOK Baden-Württemberg, the largest statutory health insurer in Baden-Württemberg.27 The observation period covered one year, from 1 January to 31 December 2021.
Study Population
Data referred to patient cases meeting the following predefined inclusion criteria: patient age 18 years or older; at least one opioid prescription for oral or transdermal opioids from the ATC groups and codes listed in Supplementary Table S1 (see Supplementary Data – Table S1: ATC codes included and excluded for patient case selection based on claims data from AOK Baden-Württemberg, Germany, 2021) in all four quarters of the year 2021; opioid prescription issued by a general practitioner.
Excluded were patients with prescriptions from specialist physicians, patients receiving palliative care or with a diagnosis of malignant disease, as indicated by the following ICD-10-GM Codes: Z51.5 Palliative care; Z51.82 Combined radiotherapy and chemotherapy for malignant neoplasm; Z85.- Personal history of malignant neoplasm; C00-C97 Malignant neoplasm. All patient cases with prescriptions corresponding to excluded ATC codes were removed from the dataset. These included particularly cases with documented specific ATC codes for opioid substitution or misuse therapy and cases with prescription of codeine-containing medications, as codeine is not recommended for CNCP and is mainly used for mild acute pain or cough.
Model A
For a primary multivariable logistic regression, patient cases with an F11.- diagnosis in the first quarter of the observation period were removed from the dataset to enable analysis of incident ORD in CNCP patients undergoing long-term opioid therapy.
Model B
To characterize the subgroup with existing ORD, assess robustness of associations and provide prevalence estimates of F11.- diagnoses, the exploratory Model B included all patient cases, regardless of baseline F11.- diagnosis in the observed population.
Measures
The dependent variable for the regression analyses was the presence of ORD, defined by ICD-10 -GM, F11.- codes for mental and behavioral disorders due to opioid use. The analysis focused on oral and transdermal opioids, as these are most commonly prescribed in general practice. Opioids were classified by release profile into LAOs (oral or transdermal) and SAOs (oral only). Rapid-onset opioids (ROOs) or other release profiles were excluded. The release profiles, which categorize opioids into LAOs and SAOs, were obtained from a summary provided by the German Pharmacy Portal (DAP – German Pharmacy Portal; Abbreviations for dosage forms).28 Based on prescriptions over all four quarters, patients were assigned to one of three groups: 1. LAOs only (reference group), 2. SAOs only 3. Combination of LAOs and SAOs (same potency class). To maintain exposure consistency and reduce confounding, patients with mixed potency combinations (for expamle:, concurrent prescriptions of weak and strong opioids within the observation period) or changes in opioid formulations over time were excluded from the regression analyses, as they could not be clearly assigned to a single opioid formulation exposure group. Opioid formulation groups were therefore defined more strictly for the regression models than in the descriptive analyses. The combination therapy variable included only concurrent LAOs and SAOs within the same potency class within the same quarter, while combinations across potency classes within the same quarter were excluded. As this variable captured treatment patterns across quarters and allowed for changes between potency classes over time, it included a broader patient group than the descriptive analyses.
Data Transfer and Data Storage
Data processing complied with the General Data Protection Regulation, the German Social Code’s data-protection provisions, and applicable national law. Pseudonymised service and claims data were transmitted only after the supervisory authority approved an application under the Social Code (submitted by AOK Baden-Württemberg). As part of the family- doctor centred care evaluation (HZV), AOK Baden-Württemberg compiled the data and provided them to the aQua Institute. Direct identifiers were replaced and data re-pseudonymised; the de-pseudonymization key was accessible only to authorised AOK Baden-Württemberg staff, and linkage only via a project-specific table held by authorised aQua Institute staff. The aQua Institute transferred the data to the Department of Primary Care and Health Services Research, Heidelberg University Hospital, where they were stored in compliance with data-protection requirements. Access was restricted to designated department staff and RELIEF team members (GL, SB, RPD, CS) on a need-to-know basis.
Data Analysis
Data storage and preparation were performed using MySQL (version 10.6.3-MariaDB), and descriptive and regression analyses were performed using SPSS (version 28.0.1.0) and RStudio (R-4.5.1). Descriptive variables included age, sex, nationality, CNCP diagnosis (ICD-10-GM: F45.4, R52.1, R52.2, F62.8), and opioid prescription characteristics by potency class, formulation, and active substance (tramadol, tilidine, tapentadol, morphine, oxycodone, hydromorphone, buprenorphine, fentanyl). Multivariable logistic regression analyses identified factors associated with ORD. Predictors were age, sex, opioid formulation group, MME dose >120 mg/day (the variable was derived based on the Defined Daily Doses (DDD), following the methodology after Schrader et al29), and comorbidities: somatoform pain disorder (F45.40), severe depressive episodes (F32.2, F32.3, F33.2, F33.3), harmful use of non-dependence substances (F55.- e g. nutritional supplements, laxatives), and disorders due to sedatives/hypnotics (F13.-), alcohol (F10.-), or tobacco (F17.-). The daily opioid dose was converted into MME using a multi-step approach based on DDD and established conversion factors. Patients were categorized according to a threshold of >120 mg/day MME. A detailed description of the conversion procedure and calculation steps is provided in the Supplementary Table S2 (see Supplementary Data – Table S2: Included Predictors in the Regression Models, on claims data from AOK Baden-Württemberg, Germany, 2021). Statistical significance was set at p < 0.05 Odds ratios (ORs) with 95% confidence intervals (CIs) were calculated. Model fit was assessed with Nagelkerke’s R2, discriminative performance for predicting ORD by ROC-AUC, and multicollinearity by correlation matrix.
Results
From a total dataset of N=2,540,716 insured individuals, n=33,505 patients were included in Model A and n=34,205 patients in Model B based on the predefined inclusion criteria. Patient characteristics observed over all four quarters in 2021 are summarized in Table 1 The mean age of the cohort was 71.7 years in Model A and 71.4 years in Model B. Female patients accounted for 65.7% in Model A and 65.2% in Model B. A diagnosis of CNCP was recorded in 62.6% of patients in Model A and 63.0% in Model B. Among the CNCP diagnoses, the most frequently coded condition was “other chronic pain” (ICD-10-GM: R52.2), which was present in 79.2% of patients in Model A and 79.4% in Model B. An ORD was identified in 1.0% of patients in Model A and 3.1% in Model B.
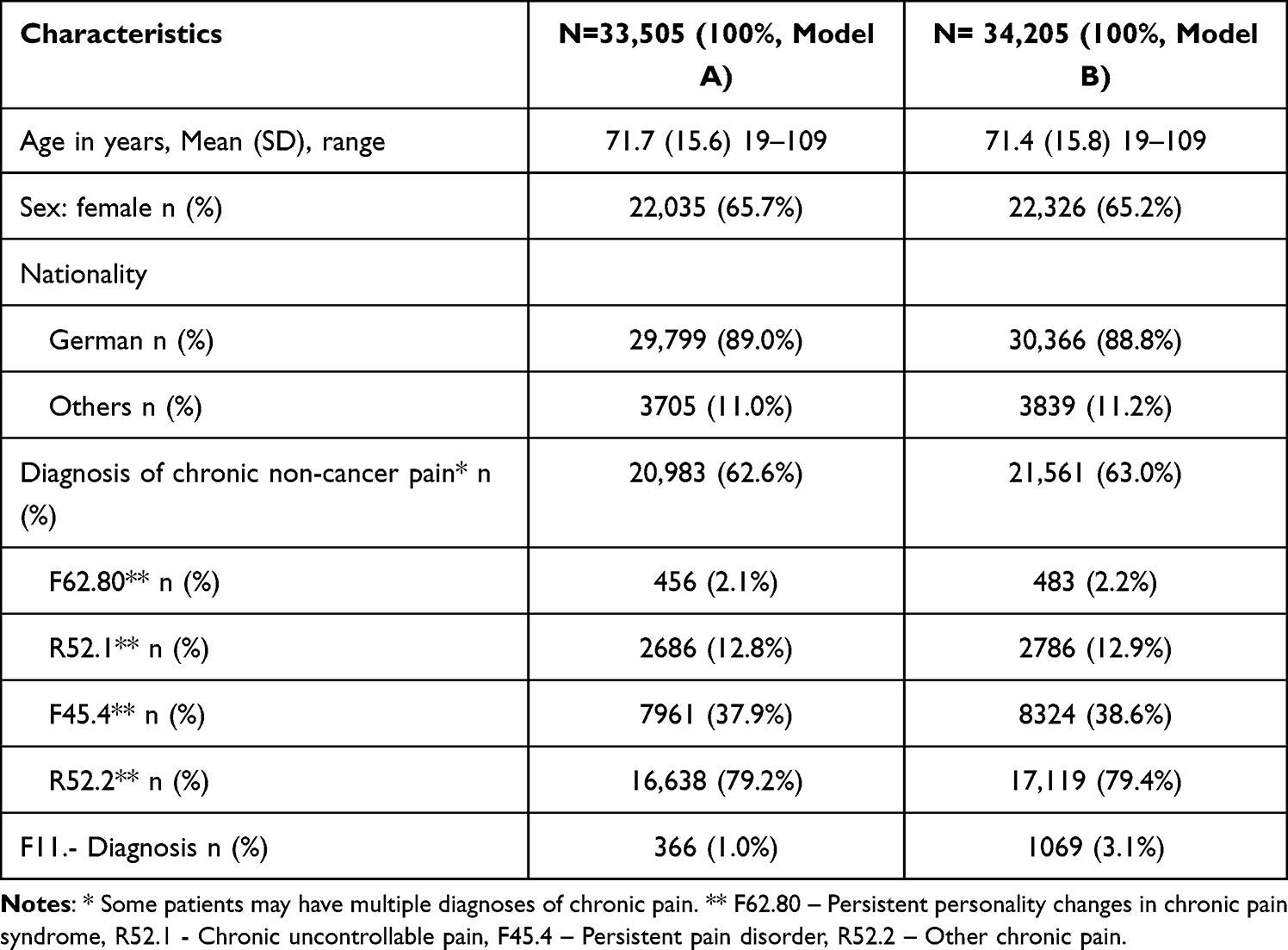 |
Table 1 Patients with Opioid Prescription Issued by General Practitioners in All Four Quarters of 2021 |
All patients included in the analysis received at least one opioid prescription in all four quarters. A majority of patients —57.4% in Model A and 57.1% in Model B— were consistently treated with weak opioids throughout the observation period. Within this subgroup, weak LAOs predominated, accounting for 89.6% (Model A) and 89.5% (Model B) of prescriptions. Among patients treated with strong opioids, strong LAOs were similarly the most commonly prescribed formulation, representing 96.1% in Model A and 96.0% in Model B. Within this group, transdermal opioids represented a substantial proportion, comprising 40.4% in Model A and 40.0% in Model B. At the active substance level, tilidine emerged as the most frequently prescribed opioid, accounting for 45.6% (Model A) and 45.3% (Model B) of all prescriptions, followed by oxycodone (15.9% and 16.0%, respectively), while tramadol and fentanyl were prescribed in approximately equal numbers of case, each representing approximately 14.0% across both models. The distribution of prescription patterns is presented in Table 2.
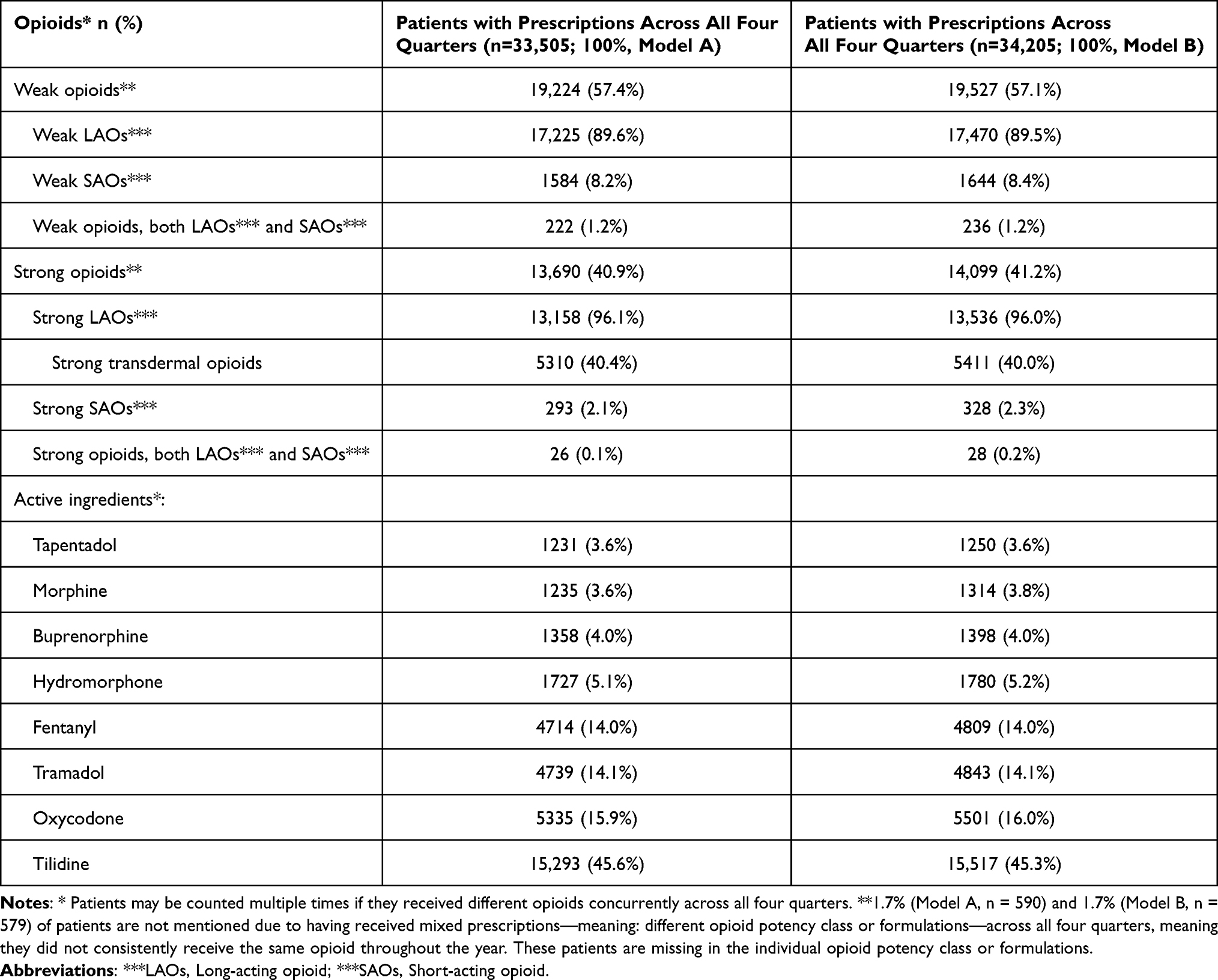 |
Table 2 Distribution Opioid Prescriptions Issued by General Practitioners in Germany, 2021 |
Predictors of Opioid-Related Disorders
In both models, age was inversely associated with the odds of an ORD, with each additional year of age decreasing the odds by 5.1% in Model A (OR = 0.949, 95% CI 0.94–0.95, p < 0.001) and by 4.9% in Model B (OR = 0.951, 95% CI 0.94–0.95, p < 0.001). Male sex (reference: female) was in Model A (OR = 1.14, 95% CI 0.91–1.43, p = 0.250) not significant. In Model B, male sex was significantly associated with 23% higher odds compared to female sex (OR = 1.23, 95% CI 1.12–1.49, p < 0.001). Opioid formulations were a central determinant of ORD occurrence. Compared to patients receiving only LAOs, those prescribed exclusively SAOs had 80% higher odds in Model A (OR = 1.8, 95% CI 1.24–2.71, p = 0.002) and 100% higher odds in Model B (OR = 2.0, 95% CI 1.53–2.48, p < 0.001). The highest odds were observed among patients receiving both LAOs and SAOs formulations, with an 210% increase in Model A (OR = 3.1, 95% CI 1.74–5.71, p = 0.001) and 250% increase in Model B (OR = 3.5, 95% CI 2.38–5.00, p < 0.001). High opioid dosage (>120 MME on average over 365 days) was associated with a 270% increase in Model A (OR = 3.7, 95% CI 2.98–4.83, p < 0.001) and a 310% increase in Model B (OR = 4.1, 95% CI 3.52–4.74, p < 0.001). Regarding comorbid diagnoses, severe depressive episodes were associated with 90% higher odds in Model A (OR = 1.9, 95% CI 1.42–2.55, p < 0.001) and with a 80% increase in Model B (OR = 1.8, 95% CI 1.56–2.26, p < 0.001). Pain in somatoform disorders was not significant in Model A (OR = 1.3, 95% CI 0.97–1.88, p = 0.073) and a significant increase of 50% in Model B (OR = 1.5, 95% CI 1.26–1.88, p < 0.001). Harmful non-dependence use of substances was associated with a 160% increase in Model A (OR = 2.6, 95% CI 1.72–3.95, p < 0.001) and a 220% increase in Model B (OR = 3.2, 95% CI 2.50–4.20, p < 0.001). Disorders due to sedatives/hypnotics use was associated with nearly threefold higher odds (290% increase) in Model A (OR = 3.9, 95% CI 2.72–5.66, p < 0.001) and almost sixfold higher odds (460% increase) in Model B (OR = 5.6, 95% CI 4.48–7.01, p < 0.001). Disorders due to alcohol use was linked to a 130% increase in Model A (OR = 2.3, 95% CI 1.71–3.10, p < 0.001) and a 120% increase in Model B (OR = 2.2, 95% CI 1.82–2.66, p < 0.001). Tobacco-related disorders were also significant, with an 80% increase in Model A (OR = 1.8, 95% CI 1.45–2.32, p < 0.001) and a 60% increase in Model B (OR = 1.6, 95% CI 1.38–1.86, p < 0.001).
Goodness-of-fit statistics indicated adequate model performance, with Nagelkerke’s R2 = 0.189 for Model A and 0.251 for Model B. The AUC was 0.845 for Model A and 0.850 for Model B, reflecting excellent discrimination for the dependent variable (ORD) in both models. Multicollinearity between predictors was ruled out using a correlation matrix. The results of the logistic regression analyses are shown in Table 3.
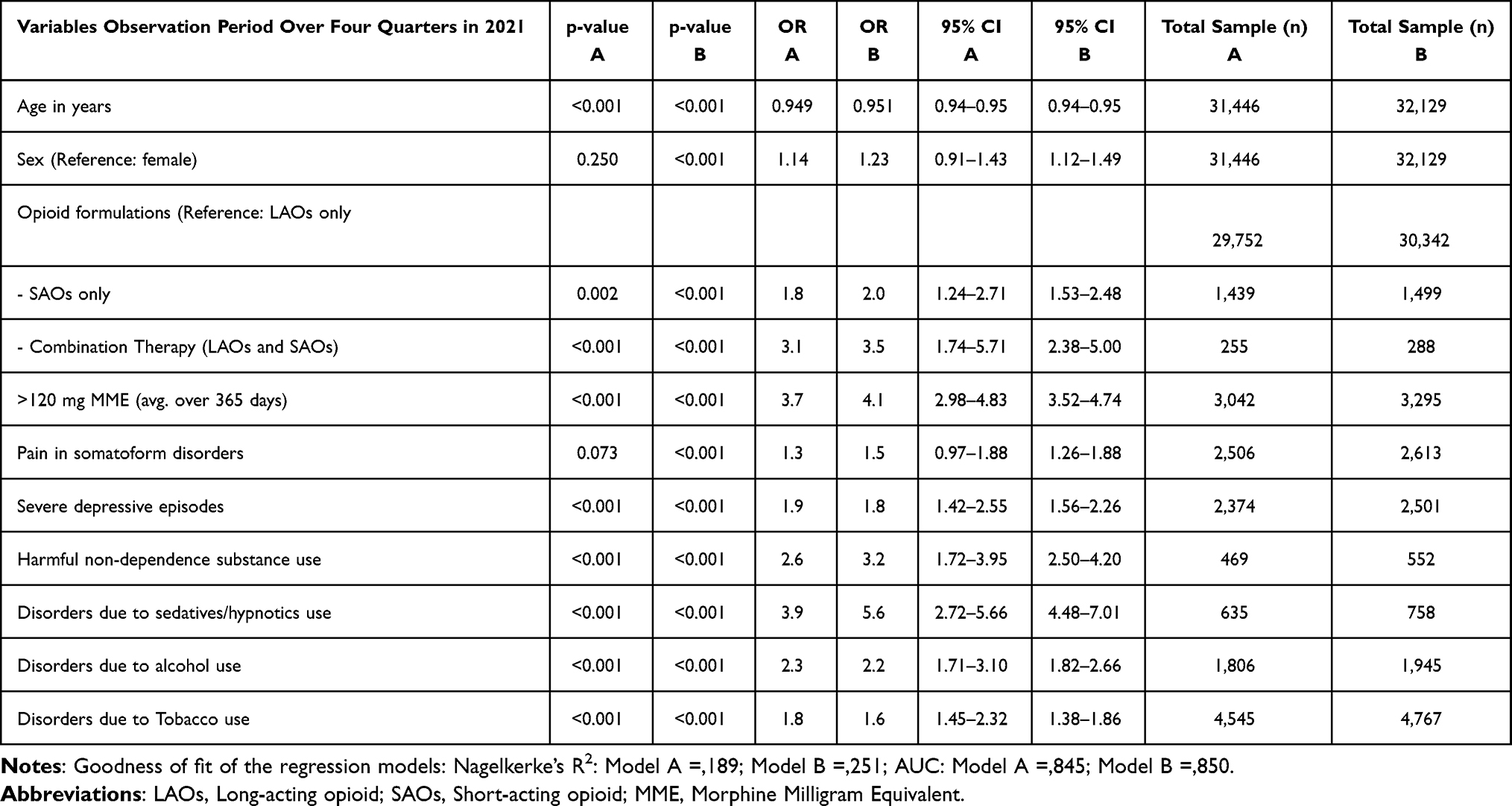 |
Table 3 Predictors of Opioid-Related Disorders in Patients with Opioid Prescriptions from General Practitioners in Germany (Model A: n = 33,505; Model B: n = 34,205), Calculated with Logistic Regression |
Discussion
This study confirms established predictors of ORD and suggests that SAOs, either alone or as part of combination therapy, may be more strongly associated with ORD in patients with CNCP and long-term opioid therapy than LAOs alone. To our knowledge, this is the first German study to examine opioid formulation in relation to ORD during long-term therapy in CNCP in general practice. These findings require confirmation in further studies to improve understanding of the underlying mechanisms and clinical implications. The cohort predominantly comprised of older adults and women. Despite continuous opioid prescribing, a substantial proportion of patients had no recorded diagnosis of CNCP. As patients with cancer-related pain were excluded from the study, it can reasonably be assumed that opioid prescriptions were not issued for cancer-related pain. The most common were weak opioids, followed by strong opioids. LAOs were the most frequently prescribed. Multivariable regression analyses identified robust predictors of ORD: younger age, higher opioid dosage, exclusive SAOs therapy, combined LAOs and SAOs therapy, severe depressive episodes and selected substance use disorders. An association with male sex was evident only when prevalent cases were included. Larger observed effect estimates for sedative or hypnotic use disorders in these models likely reflect differences in baseline patient characteristics. The fact that the confidence intervals overlap suggests that convergence is possible with a larger sample size. These findings should be interpreted with caution when extrapolating to prescribing patterns in Germany, as study-specific inclusion criteria have excluded certain patient groups and also influence the representation of combination therapy and SAOs.
Opioid Formulations
Exclusive SAOs therapy and combined LAOs and SAOs therapy were associated with higher odds of ORD compared with exclusive LAOs therapy. In the context of a German patient population, which is not characterized by an opioid crisis, these findings provide initial evidence consistent with the recommendations of the LONTS guideline. While the fixed dosing schedules recommended by LONTS could not be assessed using claims data, our results offer first indications that the choice of opioid formulation may be relevant in long-term opioid therapy for CNCP. However, given the one-year observation period, the findings should be interpreted as reflecting associations within a limited time frame rather than long-term trajectories of opioid use, dose escalation, or changes in prescribing patterns. In addition, the smaller number of patients in the exclusive SAO and combination therapy groups resulted in wider confidence intervals, which should be considered when interpreting these estimates.
Earlier literature (2003–2014), including several systematic reviews, found no meaningful differences in efficacy or safety between LAOs and SAOs in CNCP,30–32 with most studies of low methodological quality. Consequently, earlier recommendations emphasized tailoring therapy to individual needs, goals, and functioning rather than to opioid formulation.30–32 More recent meta-analyses confirmed comparable effects of LAOs and SAOs on functional outcomes and side effects.33 High-quality evidence favoring one formulation remains lacking, and few studies have specifically examined long-term opioid therapy.
The most recent guideline (2023) from the American Society of Interventional Pain Physicians (ASIPP)34 stated that LAOs and SAOs are similarly effective, but LAOs are associated with a higher incidence and prevalence of adverse events. The rational cites Dowell et al,35 who—preparing the CDC guidelines—found no evidence that LAOs are more effective or safer than intermittent SAOs use, or that they reduce misuse or addiction risk. In fact, LAOs use was associated with higher total average daily opioid doses compared with SAOs taken as needed.34,35 This contrasts sharply with the German LONTS guideline,3 which preferentially recommends LAOs, arguing that fixed dosing schedules may improve pain control, adherence, and reduce fall and addiction risk. While acknowledging the lack of high-quality evidence, LONTS emphasizes fixed dosing schedules more than opioid formulation type.3 When examining the impact of combination therapy in patients with CNCP receiving long-term opioid therapy, one study from the United States likewise reported an association between combination therapy and higher odds of opioid-related adverse events.36 However, in contrast to our results, this study found that LAOs alone were associated with increased odds of opioid-related adverse events compared to SAOs. It should also be noted that several estimates were not statistically significant in a consistent manner, and some confidence intervals were extremely wide (extending into triple digits), which substantially limited their interpretability.36 As these findings are based on patient data from the United States opioid crisis, they must be interpreted with caution, a point elaborated in the following section.
Based on prescribing trends and epidemiological data,37 leading German pain medicine experts conclude that Germany has not experienced and is unlikely to experience an opioid crisis. This context is essential for interpreting differences in international guidelines. The ASIPP’s34 restrictive stance reflects the United States opioid crisis, where LAOs—particularly oxycodone—were heavily implicated in misuse and overdose, driven by liberal prescribing and aggressive marketing rather than appropriately monitored chronic pain care.37 United States data therefore disproportionately capture LAOs-related harms in high-risk populations.34 In contrast, our claims data analysis directly examined the association between opioid formulation and ORD in German primary care, in a context not affected by an opioid crisis.
Patient Characteristics and Comorbidities
Existing evidence suggests that patients with CNCP and psychiatric comorbidities are particularly susceptible to opioid misuse. This risk is notably elevated in younger individuals and those receiving high-dose regimens exceeding 120 mg MME per day, especially in the presence of depressive or somatoform disorders.38,39 A history of benzodiazepine dependence or the concurrent use also increases vulnerability to opioid-related risks, as confirmed by national and international studies.40,41 A German claims data analysis identified GPs as the main opioid prescribers to primarily older, multimorbid patients.42 Consistent with European43 and German data,44 older female patients with CNCP were observed in this present study than male patients. National and international evidence confirms that long-term opioid therapy in primary care is most often prescribed to older female patients, with weak opioids being most common.44 However, prescribing of strong opioids, particularly fentanyl, as also found in our data, warrants continued monitoring.44
Our regression model incorporated variables already known to be associated with an increased likelihood of ORD. Consistent with the prior evidence,29,45–47 younger age, male sex, psychiatric comorbidities—specifically severe depressive episodes—and opioid dosages exceeding 120 mg MME were strongly associated with higher odds of developing an ORD. This aligns with the German guideline on “Medication-Related Disorders”,48 which advises caution when prescribing opioids to younger patients (20–40 years), males, and those with psychiatric disorders.48
Evidence indicates that the concurrent prescription of opioids and tranquilizers in patients with CNCP receiving long-term opioid therapy is associated with an increased likelihood of hospitalization.47 This is consistent with our findings for substance use disorders involving sedatives or hypnotics—which belong to the same pharmacological class as tranquilizers—and which demonstrated an association with higher odds of ORD. Certain diagnoses within the ICD-10 category F11.- frequently necessitate inpatient treatment, further underscoring the plausibility of this association. Notably, our models also identified associations for harmful use of non-dependence substances (eg, nutritional supplements, laxatives) and for alcohol-related disorders—associations which, to our knowledge and according to Just et al,38 previously have not been reported in a German population. By contrast, disorders due to tobacco use showed also an association, though it still contributed to the broader profile of substance use disorders in this group. Overall, these results underscore that substance use disorders are relevant in patients with CNCP receiving long-term opioid therapy. Clinical monitoring should therefore encompass not only the well-established associations with sedatives and hypnotics,47 but also alcohol misuse38 and harmful use of non-dependence substances, as these may represent underrecognised yet clinically relevant factors contributing to ORD in patients with CNCP.
Strengths and Limitations
A major strength of this study is the large patient cohort, enabling robust regression analyses. Claims data provide valuable insight into healthcare delivery and allow precise cohort definition through strict inclusion and exclusion criteria. However, unlike prospective controlled trials, patient allocation occurs retrospectively, requiring cautious interpretation. Several limitations should be considered. First, the analyses were based on claims data from a single statutory health insurance provider in one federal state in Germany and covered a one-year observation period, which may limit generalizability to other regions, healthcare settings, or longer time periods. In addition, the restriction to patients receiving opioid prescriptions in general practice may exclude individuals with more severe or complex conditions managed in specialist care, who may have a different risk profile for ORD. Furthermore, study-specific inclusion criteria, such as the focus on oral and transdermal opioids, may have excluded patients receiving other opioid formulations, which also affect the representation of combination therapy and SAOs. Second, inherent limitations of claims data must be acknowledged. Actual medication intake cannot be confirmed; prescription redemption reflects intent but does not capture adherence or reasons for non-adherence. Involvement of multiple prescribers could not be assessed. Moreover, ORD were identified using ICD-10-GM F11.- codes, which may lead to underestimation, as such diagnoses may not be consistently documented in routine primary care practice. Third, methodological aspects of variable definition should be considered. The categorization of opioid dose into a binary variable (>120 mg/day vs. ≤120 mg/day MME) may obscure differences across the full dose range. In addition, MME estimates were based on DDD, which represent an approximation of actual exposure and should be interpreted with caution. In our regression models, relatively wide confidence intervals, particularly for SAOs and combination therapies, indicate some uncertainty in the estimates. Finally, the study design limits the assessment of temporal dynamics. The observation period was restricted to one year, precluding analysis of long-term trajectories, dose escalation, or changes in prescribing patterns. Although long-term opioid therapy was defined as continuous prescriptions across four quarters, international studies often apply shorter definitions, which may limit comparability. In addition, a substantial proportion of patients had no recorded diagnosis of CNCP, which may reflect under documentation in routine care.
Conclusion
To our knowledge, this is the first study to examine opioid formulations in relation to ORD among patients with CNCP and long-term opioid therapy in general practice using German claims data. Our results confirm previously reported associations between CNCP and ORD and provide further indications regarding the role of opioid formulation. Given that GPs provide the majority of opioid prescriptions and ongoing care for this patient population in Germany, these observations are particularly relevant to primary care. Generalizability and underlying mechanisms warrant further investigation, particularly given the modest prevalence of ORD and the limited size of some subgroups.
Abbreviations
CNCP, chronic non-cancer pain; ORD, opioid-related mental and behavioral disorders; LONTS, Long-term use of opioids for chronic non-cancer pain (German guideline); MME, oral morphine milligram equivalents; GPs, General practitioners; ICD-10-GM, International Classification of Diseases – 10th Revision – German Modification; LAOs, long-acting opioids SAOs, short-acting opioids; RELIEF, Resource-oriented case management to implement recommendations for patients with chronic pain and frequent use of analgesics in general practices; BMBF, German Federal Ministry of Education and Research; BMFTR, German Federal Ministry of Research, Technology and Space; ASIPP, American Society of Interventional Pain Physicians; CDC, Center of Disease and Prevention.
Data Sharing Statement
The AOK Baden-Wuerttemberg can be contacted for access to the claims data. Data are available on reasonable request.
Ethics Approval and Consent to Participate
This study did not involve human participants. The analysis was based on claims data. The legal basis for the transfer of social data for research and planning purposes is Section 75 of the German Social Code, Book X (SGB X). The requirements of Section 75 (1) sentence 1 SGB X are met. As the project funded by the German Federal Ministry of Education and Research serves a research purpose in the public interest, the transfer of secondary data does not require individual informed consent in accordance with Article 9 (2)(j) GDPR. The pseudonymised claims data were made available following approval by the competent supervisory authority, based on an application submitted by AOK Baden-Württemberg pursuant to Section 75 SGB X.
Acknowledgments
We thank AOK Baden-Württemberg for providing the claims data and the aQua Institute (Institute for Applied Quality Improvement and Research in Health Care, Göttingen, Germany) for their initial data processing and their collaboration in developing the data protection concept. For the publication fee we acknowledge financial support by Heidelberg University.
Author Contributions
CS and RPD applied for the claims data and developed the required data protection concept. They also submitted the application for claims data analysis to the Federal Office for Social Security. SB prepared the ethics application for the use of claims data, supported by RPD and CS. SB and GL designed and planned the study. GL contributed substantial expertise and provided methodological and operational guidance during data selection, processing, and analysis. SB performed the data selection, preparation, and analysis. SB drafted the manuscript and was responsible for all subsequent revisions.
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The RELIEF project is funded by the German Federal Ministry of Research, Technology and Space (BMFTR) within the framework of the call for proposals “Junior Research Groups in Health Services Research” (funding reference: 01GY2106). This funding has had no influence on the study’s design, conduction, evaluation, or the drafting of the paper.
Disclosure
RELIEF is a publicly funded research project (funding code: 01GY2106). CS and RPD share the project management, SB is a doctoral student in the project. CS is currently contributing to a revision of the S3-LONTS guideline. GL declares no competing interests. The authors report no other conflicts of interest in this work.
References
1. Treede RD, Rief W, Barke A, et al. A classification of chronic pain for ICD-11. Pain. 2015;156:1003–12. doi:10.1097/j.pain.0000000000000160
2. Cohen SP, Vase L, Hooten WM. Chronic pain: an update on burden, best practices, and new advances. Lancet. 2021;397:2082–2097. doi:10.1016/S0140-6736(21)00393-7
3. Häuser W, Bock F, Hüppe M, et al. Recommendations of the second update of the LONTS guideline. Schmerz. 2020;34(3):204–244. doi:10.1007/s00482-020-00472-y
4. Häuser W, Schug S, Furlan AD. The opioid epidemic and national guidelines for opioid therapy for chronic noncancer pain: a perspective from different continents. Pain Rep. 2017;2(3):e599. doi:10.1097/PR9.0000000000000599
5. Krebs EE, Gravely A, Nugent S, et al. Effect of opioid vs nonopioid medications on pain-related function in patients with chronic back pain or Hip or knee osteoarthritis pain: the SPACE randomized clinical trial. JAMA. 2018;9:872–882. doi:10.1001/jama.2018.0899
6. Chou R, Hartung D, Turner J, et al. Opioid Treatments for Chronic Pain
7. Bialas P, Maier C, Klose P, Häuser W. Effectiveness and harms of long-term opioid therapy in chronic non-cancer pain: systematic review and meta-analysis of open-label extension studies lasting ≥26 weeks. Eur J Pain. 2020;25(2):265–278. doi:10.1002/ejp.1496
8. Trescot AM, Glaser SE, Hansen H, Benyamin R, Patel S, Manchikanti L. Effectiveness of opioids in the treatment of chronic non-cancer pain. Pain Phys. 2008;11(Suppl 2):S181–S200. doi:10.36076/ppj.2008/11/s181
9. Chou R, Deyo R, Devine B, et al. The effectiveness and risks of long-term opioid treatment of chronic pain. Evid Rep Technol Assess. 2014;218:1–219 doi:10.23970/AHRQEPCERTA218.
10. O’Brien MDC, Wand APF. A systematic review of the evidence for the efficacy of opioids for chronic non-cancer pain in community-dwelling older adults. Age Ageing. 2020;49(2):175–183. doi:10.1093/ageing/afz175
11. Vowles KE, McEntee ML, Julnes PS, Frohe T, Ney JP, van der Goes DN. Rates of opioid misuse, abuse, and addiction in chronic pain: a systematic review and data synthesis. Pain. 2015;156(4):569–576. doi:10.1097/01.j.pain.0000460357.01998.f1
12. Davis MP, Digwood G, Mehta Z, McPherson ML. Tapering opioids: a comprehensive qualitative review. Ann Palliat Med. 2020;9(2):586–610. doi:10.21037/apm.2019.12.10
13. Scholle OHF, Jobski K, Vierbrock J, et al. Prescribing of opioid analgesics in Germany: opposite trends when different quantification measures are used. Clin Epidemiol. 2026; 18:580510. doi:10.2147/CLEP.S580510.
14. Glaeske G. Opioid report 2022. SOCIUM Research Center on Inequality and Social Policy, University of Bremen. 2022. Available from: https://www.hkk.de/fileadmin/dateien/allgemeines_uebergeordnet/reports/gesundheitsreports/2022_hkk_gesundheitsreport_opioide_web.pdf.
15. Hensler S, Heinemann D, Becker MT. Chronic pain in German general practice. Pain Med. 2009;10(8):1408–1415. doi:10.1111/j.1526-4637.2009.00735.x
16. Dupont D, Brinkmöller S, Carter S, et al. Exploring physician and patient perspectives on expectations and role models towards chronic pain treatment in general practice: a qualitative cross-sectional study. Healthcare. 2025;2:187. doi:10.3390/healthcare13020187
17. Chronic non-tumor-related pain: explanations and implementation guidance. DEGAM S1 recommendations for action. AWMF Register No. 053-036. 2025. Available from: https://register.awmf.org/assets/guidelines/053-036l_S1_Chronischer_Schmerz_2025-02.pdf.
18. F11: mental and behavioural disorders due to opioids. gesund.bund.de – reliable information for your health. 2025. Available from: https://gesund.bund.de/icd-code-suche/f11.
19. Atzendorf J, Rauschert C, Seitz NN, Lochbühler K, Kraus L. The use of alcohol, tobacco, illegal drugs and medicines: an estimate of consumption and substance-related disorders in Germany. Dtsch Arztebl Int. 2019;116(35–36):577–584. doi:10.3238/arztebl.2019.0577
20. German Society for Addiction Research and Therapy (DG-Sucht), German Society for Psychiatry and Psychotherapy, Psychosomatics, and Neurology (DGPPN), et al. S3 Guideline: opioid-Use Disorders. AWMF Registry No. 076-012. 2025. Available from: https://register.awmf.org/assets/guidelines/076-012m_S3_Opioidbezogene-Stoerungen_2025-11.pdf.
21. Krčevski Škvarč N, Morlion B, Vowles KE, et al. European clinical practice recommendations on opioids for chronic non-cancer pain – part 2: special situations. Eur J Pain. 2021;25:969–985. doi:10.1002/ejp.1744
22. Faculty of Pain Medicine, Australian and New Zealand College of Anaesthetists. Recommendations regarding the use of opioid analgesics in patients with chronic non-cancer pain. Faculty of Pain Medicine website. 2025. Available from: https://www.anzca.edu.au/getContentAsset/a852b656-b043-458d-9951-aa81f259f4e6/80feb437-d24d-46b8-a858-4a2a28b9b970/PS01(PM)_-Statement-regarding-the-use-of-opioid-analgesics-in-patients-with-chronic-non-cancer-pain.PDF. Accessed
23. Chou R, Fanciullo GJ, Fine PG, et al. Clinical guidelines for the use of chronic opioid therapy in chronic non-cancer pain. J Pain. 2009;10(2):113–130. doi:10.1016/j.jpain.2008.10.008
24. Dowell D, Ragan KR, Jones CM, et al. CDC Clinical Practice guideline for prescribing opioids for pain—United States. MMWR Recomm Rep. 2022;71(3):1–95. doi:10.15585/mmwr.rr7103a1
25. Busse JW, Craigie S, Juurlink DN, et al. Guideline for opioid therapy and chronic non-cancer pain. Can Med Assoc J. 2017;189(E666):E659. doi:10.1503/cmaj.170363
26. RELIEF – resource-oriented case management for implementing recommendations for patients with chronic pain and frequent analgesic use in general practice. 2022. Available from: https://www.relief-amed.de/.
27. AOK – The Health Insurance Fund. Care levels. 2025. Available from: https://www.aok.de/pk/pflege-im-alltag/pflegegrade/.
28. DAP – German Pharmacy Portal. Abbreviations for dosage forms and their meanings. Available from: https://www.deutschesapothekenportal.de/download/public/arbeitshilfen/dap_arbeitshilfe_123.pdf.
29. Schrader NF, Niemann A, Weitzel M, et al. Exceeding the guideline-recommended maximum daily dose of opioids for long-term treatment of non-cancer pain in Germany: a large retrospective observational study. BMC Public Health. 2024;24:2580. doi:10.1186/s12889-024-20141-4
30. Chou R, Clark E, Helfand M. Comparative efficacy and safety of long-acting oral opioids for chronic non-cancer pain: a systematic review. J Pain Symptom Manage. 2003;26(5):1026–1048. doi:10.1016/j.jpainsymman.2003.03.003
31. Pedersen L, Borchgrevink PC, Riphagen II, Fredheim OMS. Long- or short-acting opioids for chronic non-malignant pain? A qualitative systematic review. Acta Anaesthesiol Scand. 2014;58(4):390–401. doi:10.1111/aas.12279
32. Fine PG, Mahajan G, McPherson ML. Long-acting opioids and short-acting opioids: appropriate use in chronic pain management. Pain Med. 2009;10 Suppl 2:S79–88. doi:10.1111/j.1526-4637.2009.00666.x
33. Noori A, Sadeghirad B, Wang L, et al. Comparative benefits and harms of individual opioids for chronic non-cancer pain: systematic review and network meta-analysis of randomised trials. Br J Anaesth. 2022;129(3):394–406. doi:10.1016/j.bja.2022.05.031
34. Manchikanti L, Kaye AM, Knezevic NN, et al. Comprehensive, evidence-based, consensus guidelines for prescription of opioids for chronic non-cancer pain from the American Society of Interventional Pain Physicians (ASIPP). Pain Phys. 2023;26(7S):S7–S126. doi:10.36076/ppj.2023.26.S7
35. Dowell D, Haegerich TM, Chou R. CDC guideline for prescribing opioids for chronic pain—United States, 2016. MMWR Recomm Rep. 2016;65:1–49. doi:10.15585/mmwr.rr6501e1
36. Salkar M, Ramachandran S, Bentley JP, et al. Do formulation and dose of long-term opioid therapy contribute to risk of adverse events among older adults? J Gen Intern Med. 2022;37(2):367–374. doi:10.1007/s11606-021-06792-8
37. Häuser W, Petzke F, Radbruch L. The U.S. opioid epidemic threatens Germany. Schmerz. 2020;34:1–3. doi:10.1007/s00482-019-00441-0
38. Just J, Petzke F, Scherbaum N, Radbruch L, Weckbecker K, Häuser W. Critical discussion of new data regarding prevalence of opioid use disorder in patients with chronic pain in Germany. Schmerz. 2022;36:13–18. doi:10.1007/s00482-021-00582-1
39. Campbell G, Nielsen S, Larance B, et al. Pharmaceutical opioid use and dependence among people living with chronic pain: associations observed within the POINT cohort. Pain Med. 2015;16:1745–1758. doi:10.1111/pme.12773
40. Cochran BN, Flentje A, Heck NC, et al. Factors predicting development of opioid use disorders among individuals receiving an initial opioid prescription: modelling using a database of commercially insured individuals. Drug Alcohol Depend. 2014;138:202–208. doi:10.1016/j.drugalcdep.2014.02.701
41. Fredheim OM, Mahic M, Skurtveit S, Dale O, Romundstad P, Borchgrevink PC. Chronic pain and use of opioids: a population-based pharmacoepidemiological study from the Norwegian Prescription Database and the Nord-Trøndelag Health Study. Pain. 2014;155:1213–1221. doi:10.1016/j.pain.2014.03.009
42. Lappe V, Grandt D, Marschall U, et al. Opioid prescriptions for insured persons without cancer in Germany: data from BARMER. Schmerz. 2025;39:359–369. doi:10.1007/s00482-024-00852-8
43. Bimpong K, Thomson K, McNamara CL, et al. The gender pain gap: gender inequalities in pain across 19 European countries. Scand J Public Health. 2022;50(2):287–294. doi:10.1177/1403494820987466
44. Rosner B, Neicun J, Yang JC, Roman-Urrestarazu A. Opioid prescription patterns in Germany and the global opioid epidemic: systematic review of available evidence. PLoS One. 2019;14(8):e0221153. doi:10.1371/journal.pone.0221153
45. Marschall U, L’hoest H, Radbruch L, Häuser W. Long-term opioid therapy for chronic non-cancer pain in Germany. Eur J Pain. 2016;20:767–776. doi:10.1002/ejp.802
46. García-Sempere A, Hurtado I, Robles C, et al. Initial opioid prescription characteristics and risk of opioid misuse, poisoning and dependence: retrospective cohort study. BMJ Qual Saf. 2024;33:13–23. doi:10.1136/bmjqs-2022-015833
47. Capaldi DM, Kerr DCR, Tiberio SS, Owen LD. Men’s misuse of prescription opioids from early to middle adulthood: examination of developmental and concurrent prediction models. J Consult Clin Psychol. 2019;87(10):893–903. doi:10.1037/ccp0000442
48. German Society for Psychiatry and Psychotherapy, Psychosomatics, and Neurology (DGPPN); German Society for Addiction Research and Addiction Therapy (DG-Sucht). S3 guideline on medication-related disorders, 1st edition. Version 01. 2020. Available from: https://register.awmf.org/de/leitlinien/detail/038-025.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Nurse-Led Model of Care with Telemonitoring to Manage Patients with Heart Failure in Primary Health Care: A Mixed-Method Feasibility Study
Longhini J, Canzan F, Zambiasi P, Toccoli S, Gios L, Del Greco M, Sforzin S, Moz M, Fracchetti M, Saiani L, Brolis R, Guarnier A, Soverini M, Maines M, Ambrosi E
Patient Preference and Adherence 2023, 17:2579-2594
Published Date: 20 October 2023
Follow-Up in Primary Care After Ischemic Stroke – Insights From the Nor-COAST Study

Sande IS, Helgheim KL, Saltvedt I, Røsstad TG, Spigset O, Ellekjær H, Gynnild MN
International Journal of General Medicine 2025, 18:2141-2150
Published Date: 15 April 2025