Back to Journals » Drug Design, Development and Therapy » Volume 20
Lenvatinib in Combination with PD-1 Blockades as Re-Challenging Treatment for Patients with Metastatic Soft Tissue Sarcoma Following TKI Treatment Failure: A Retrospective Study
Authors Song G, Hu J, He W, Deng C, Xu H, Wang A, Feng H, Wu H, Zhu X, Lu J, Tang Q, Wang J
Received 9 December 2025
Accepted for publication 20 March 2026
Published 30 March 2026 Volume 2026:20 587636
DOI https://doi.org/10.2147/DDDT.S587636
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Guohui Song,1,2,* Jinxin Hu,1,2,* Wenqian He,1,2,* Chuangzhong Deng,1,2 Huaiyuan Xu,1,2 Anqi Wang,1,2 Huixiong Feng,1,2 Hao Wu,1,2 Xiaojun Zhu,1,2 Jinchang Lu,1,2 Qinglian Tang,1,2 Jin Wang1,2
1Department of Musculoskeletal Oncology, Sun Yat-Sen University Cancer Center, Guangzhou, 510060, People’s Republic of China; 2State Key Laboratory of Oncology in South China, Guangdong Provincial Clinical Research Center for Cancer, Sun Yat-sen University Cancer Center, Guangzhou, 510060, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jin Wang, Department of Musculoskeletal Oncology, Sun Yat-Sen University Cancer Center, Guangzhou, 510060, People’s Republic of China, Tel +86-20-87340519, Email [email protected] Qinglian Tang, Department of Musculoskeletal Oncology, Sun Yat-Sen University Cancer Center, Guangzhou, 510060, People’s Republic of China, Tel +86-20-87340519, Email [email protected]
Background: Previous research has demonstrated the effectiveness of lenvatinib and programmed death-1 (PD-1) blockades in the treatment of sarcoma. However, there is limited information regarding the efficacy and safety of combining lenvatinib with PD-1 blockades as a re-challenge therapy in patients with metastatic soft tissue sarcoma (STS) following prior treatment failure with tyrosine kinase inhibitors (TKIs).
Methods: Between October 2019 and September 2024, 28 patients with metastatic STS who received rechallenge treatment with lenvatinib in combination with PD-1 blockades following progression on prior TKI treatment were included in this retrospective analysis. The primary endpoint was progression-free survival (PFS). Secondary endpoints included objective response rate (ORR), clinical benefit rate (CBR), overall survival (OS), and safety.
Results: Of the 28 patients, ORR and CBR were 0 and 64.3%, respectively. The median duration of follow-up was 26 months (range, 13.2– 38.8). The median PFS was 4.8 months (95% CI: 2.7– 6.9), while the median OS was 23 months (95% CI: 16.5– 29.5). Approximately 96.4% of patients experienced adverse events of grade 1 or higher. Grade 3 adverse events were reported in 5 patients, accounting for 17.9%.
Conclusion: Our findings indicate that patients with metastatic STS may potentially benefit from the combination of lenvatinib and PD-1 blockades following the failure of prior TKI therapy. The combination of lenvatinib and PD-1 blockade therapy showed encouraging survival results in patients with metastatic STS, with an acceptable and manageable safety profile.
Keywords: metastatic soft tissue sarcoma, tyrosine kinase inhibitor, lenvatinib, PD-1 blockades, rechallenge
Introduction
Soft tissue sarcoma (STS) is a collection of rare mesenchymal tumors representing approximately 1% of adult malignancies and encompasses more than 70 distinct histological subtypes.1,2 Surgery remains the standard primary treatment for most patients with localized soft tissue sarcoma.3 However, despite comprehensive management, approximately 25% of patients diagnosed with high-risk soft tissue sarcomas subsequently develop metastatic disease.4 Patients with metastatic disease are generally treated with anthracycline-based chemotherapy, which typically results in a poor median progression-free survival of 4.2 months.5–7 Currently, therapeutic options for patients with metastatic soft tissue sarcomas who experience disease progression after first-line chemotherapy are quite limited.8–10 Therefore, the development of innovative treatment approaches is essential to improve the prognosis for patients with soft tissue sarcoma.
For patients with metastatic soft tissue sarcomas that fail to benefit from surgical or chemotherapeutic interventions, tyrosine kinase inhibitors (TKIs) have emerged as a significant treatment option.11,12 An increasing number of TKIs have demonstrated favorable clinical efficacy in patients with specific histological subtypes of advanced soft tissue sarcoma.13 However, the development of drug resistance is a common challenge during TKIs therapy, and the limited number of treatment options available to overcome such resistance has negatively impacted the overall survival of sarcoma patients.14 Currently, no validated treatments exist outside of clinical trial settings. Recent literature reports indicate that rechallenge with multi-targeted TKIs may be a viable approach for patients with advanced tumors who have exhausted approved second-line or subsequent treatment options.15,16 However, their use in sarcoma patients is currently limited to clinical trials or off-label applications.
Lenvatinib is an orally administered tyrosine kinase inhibitor that selectively targets PDGFR-α, VEGFRs 1–3, RET, FGFRs 1–4, and KIT.17 An increasing body of research indicates that rechallenging with lenvatinib may serve as a viable treatment option for selected patients with advanced malignancies, including sarcoma.18–20 A Phase I dose-escalation studies have demonstrated disease stabilization in some patients with leiomyosarcoma treated with lenvatinib.21 A Phase Ib/II clinical study evaluating the combination of lenvatinib and eribulin was conducted in patients with leiomyosarcoma and liposarcoma.22 The study reported an objective response rate of 19% in the leiomyosarcoma cohort and 20% in the liposarcoma cohort, with a median progression-free survival of 8.56 months.
Immune checkpoint inhibitors (ICIs) targeting programmed death-1 (PD-1) have demonstrated notable success in the treatment of solid tumours, leading to further investigation into their potential role in sarcoma management.23 The specific efficacy of immunotherapy has been observed in certain selected histological subtypes. PD-1 blockades have demonstrated promising results in cases of alveolar soft part sarcoma (ASPS), undifferentiated pleomorphic sarcomas, malignant rhabdoid tumours, and angiosarcoma.24 A systematic review and meta-analysis of clinical trials evaluating ICIs for soft tissue sarcomas indicates that, with ICI monotherapy, the overall objective response rate (ORR) was 16%, and the disease control rate (DCR) was 64%. Compared to monotherapy, combination treatment demonstrates improved efficacy, particularly when incorporating PD-1 blockades and TKIs, which achieves an objective response rate of 28%.25 This indicates that immune checkpoint inhibitors, particularly when combined with tyrosine kinase inhibitors, offer significant therapeutic benefits in the treatment of soft tissue sarcomas.
Preclinical studies using murine tumor models demonstrated that pretreatment with lenvatinib reduces the presence of immunosuppressive tumor-associated macrophages, enhances the activation of cytotoxic T cells, stimulates interferon-γ signaling, and exhibits synergistic effects when combined with PD-1 inhibition.26,27 Recent clinical trials assessing the combination of lenvatinib and PD-1 blockades have demonstrated sustained responses in patients with sarcoma.28 This study identified evidence of activity for lenvatinib and pembrolizumab in synovial sarcoma, MPNST, and osteosarcoma. The overall response rate was 15.2%. Treatment-related adverse events of any grade were observed in 98% of patients, with 57% experiencing Grade 3 or higher events. However, the data concerning the use of lenvatinib in combination with PD-1 blockades for patients with soft tissue sarcoma who have experienced failure of TKI therapy remains limited, and there is insufficient information regarding its effects on patient outcomes, particularly in real-world clinical practice. This retrospective study aims to evaluate real-world experiences with reinitiating lenvatinib in combination with PD-1 blockades in patients with metastatic soft tissue sarcoma following the failure of prior tyrosine kinase inhibitor therapies.
Patients and Methods
Patients and Study Design
This retrospective, single-center study was conducted in a real-world clinical setting to assess the efficacy and safety of lenvatinib in combination with PD-1 blockades in patients with soft tissue sarcoma who have experienced progression following TKIs therapy between October 2019 and September 2024. The inclusion criteria were as follows: (1) histologically-confirmed STS; (2) metastatic tumor lesions unsuitable for curative treatment; (3) at least one measurable lesion in accordance with RECIST 1.1 criteria; (4) A minimum of one treatment cycle with lenvatinib in combination with PD-1 blockades, following the failure of initial tyrosine kinase inhibitor therapy. Patients were excluded from the study if they received treatment with lenvatinib in combination with PD-1 blockades alongside other concurrent therapies, or if their medical records were incomplete.We reviewed patients’ treatment histories within our hospital’s electronic medical records system to identify individuals who meet the inclusion criteria and to exclude those who meet the exclusion criteria.
This study was conducted in accordance with the Declaration of Helsinki and complies with all applicable legal and ethical data protection standards. Ethical approval for this study was obtained from the Ethics Board at Sun Yat-sen University Cancer Center. The ethics review committee granted an exemption from obtaining informed consent from the patients.
Treatment
All patients underwent a minimum of one treatment cycle combining lenvatinib with PD-1 blockades. The initial dose of lenvatinib was prescribed based on patient body weight: patients weighing less than 60 kg received 8 mg once daily, while those weighing more than 60 kg received 12 mg once daily. The discontinuation, suspension, and dosage modifications of lenvatinib were permissible in response to disease progression or the occurrence of adverse events. Simultaneously, PD-1 blockades, including camrelizumab (Jiangsu Hengrui Pharmaceutical Co., Ltd.) and sintilimab (Innovent Biopharmaceuticals (Suzhou) Co., Ltd), were administered intravenously at a dose of 200 mg every three weeks. Both sintilimab and camrelizumab have been approved and launched in China. As domestically produced PD-1 inhibitors, they are extensively utilised in immunotherapy for a range of tumours.29–32 Both medications are included under medical insurance coverage. Each patient received one of these two medications, with the selection made by the clinician based on medication availability and the patient’s overall condition. Only two patients received sintilimab, while the remaining 26 patients were treated with camrelizumab. Treatment was continued until disease progression, development of unacceptable toxicity, or patient or physician decision to discontinue.
Treatment Evaluation
Treatment response was evaluated in accordance with the Response Evaluation Criteria in Solid Tumours (RECIST) version 1.1, utilizing CT or MRI imaging every two treatment cycles or as clinically indicated. The primary endpoint was PFS, defined as the duration from the initiation of lenvatinib in combination with PD-1 blockades therapy to the occurrence of disease progression or death from any cause. Secondary endpoints included ORR, CBR, OS, and safety. The ORR was determined by summing the rates of confirmed CR and PR. A minimum duration of six weeks is required to be classified as SD. The CBR was defined as the proportion of patients achieving complete response, partial response, or stable disease. OS is defined as the duration from the initiation of lenvatinib combined with PD-1 blockades to the time of death from any cause. Safety assessments were conducted by AEs using the Common Terminology Criteria for Adverse Events (CTCAE), version 5.0.3.
Statistical Analysis
The GraphPad Prism version 8.0 and SPSS software (version 26.0) were used for statistical analysis. The Kaplan–Meier method was employed to generate the PFS and OS curves. Univariate analyses were conducted using Cox proportional hazards regression models. Statistical significance was defined as a p-value less than 0.05. Results were expressed as hazard ratios (HR) with 95% confidence intervals (CI).
Results
Patient Characteristics
As detailed in Table 1, a total of 28 eligible patients with metastatic STS were enrolled between October 2019 and September 2024, with a median age of 46 years (range: 16 to 72 years). Of the patients, 14 (50%) identified as male, and 13 patients (46.4%) had an Eastern Cooperative Oncology Group (ECOG) performance status score ranging from 0 to 1. There were five patients diagnosed with malignant peripheral nerve sheath tumor (MPNST), five with alveolar soft part sarcoma (ASPS), three with fibrosarcoma (FS), two with synovial sarcoma (SS), two with dedifferentiated liposarcoma (DDLP), two with clear cell sarcoma (CCS), two with undifferentiated pleomorphic sarcoma (UPS), and seven patients with other subtypes. All patients displayed metastatic lesions, with 6 patients (21.4%) presenting with isolated lung metastasis and 22 patients (78.6%) exhibiting metastases involving multiple organs. Prior to initiating TKI therapy, 23 patients (82.1%) had received first-line chemotherapy, and 12 patients (42.8%) had undergone a minimum of two lines of chemotherapy. 23 patients (82.1%) had received immunotherapy, including three patients who had previously undergone combined treatment with TKI and immunotherapy. Prior to initiating combination therapy with lenvatinib and PD-1 blockades, all patients had previously undergone initial TKIs treatment, including anlotinib, apatinib, and pazopanib, with 9 patients having received two or more different types of TKI therapies.
 |
Table 1 Baseline Characteristics of All Patients |
 |
Table 2 Responses of Lenvatinib and PD-1 Blockade Combination Therapy |
Efficacy
As of the data cutoff date, the median follow-up duration for all patients was 26 months (range: 13.2–38.8), with no patients lost to follow-up. Although none of the 28 patients achieved complete or partial responses, 18 patients maintained stable disease, resulting in a clinical benefit rate of 64.3% (five patients with ASPS, three patients with MPNST, two patients with FS, one patient with SS, one patient with DDLP, one patient with CCS, one patient with UPS, one patient with desmoplastic small round cell tumor (DSRCT), one patient with angiosarcoma (AS) (Table 2). The median PFS was 4.8 months (95% CI: 2.7–6.9), while the median OS was 23 months (95% CI: 16.5–29.5) (Figures 1 and 2). Univariate analysis was conducted to evaluate the relationship between clinical variables (including gender, age, ECOG performance status, primary site, sites of metastasis, prior radiotherapy, prior immunotherapy, and previous TKI categories) and patient outcomes within the entire cohort of 28 patients. The univariable analysis results indicated that the aforementioned variables did not have a significant impact on the progression-free survival of the combined treatment (Table 3).
 |
Table 3 Univariate Analyses of Factors Associated with PFS and OS |
 |
Figure 1 Kaplan-Meier estimates of progression-free survival for all the 28 patients with metastatic STS. |
 |
Figure 2 Kaplan-Meier estimates of overall survival for all the 28 patients with metastatic STS. |
Safety
All 28 patients were included in the safety analysis, and the observed toxicities are detailed in Table 4. A total of 27 out of 28 patients (96.4%) experienced adverse events of grade 1 or higher. Treatment-related adverse events resulted in dose reductions for 5 patients (17.9%), treatment suspension for 3 patients (10.7%), and permanent discontinuation of therapy for 2 patients (7.1%). The TRAEs of grade 1–2 that occurred in more than 20% of patients were hypertension (12, 42.9%), proteinuria (12, 42.9%), fatigue (11, 39.3%), hand-foot syndrome (10, 35.7%), hypothyroidism (10, 35.7%), diarrhea (7, 25%), elevated gamma glutamyltransferase (8, 28.6%), AST increased (8, 28.6%), and nausea or vomiting (7, 25%). No grade 4 TRAEs were observed; however, 5 patients (17.9%) experienced grade 3 TRAEs, including hypertension (2 patients, 7.1%), diarrhea (1 patient, 3.6%), pneumothorax (1 patient, 3.6%), and immune-related pneumonia (1 patient, 3.6%).
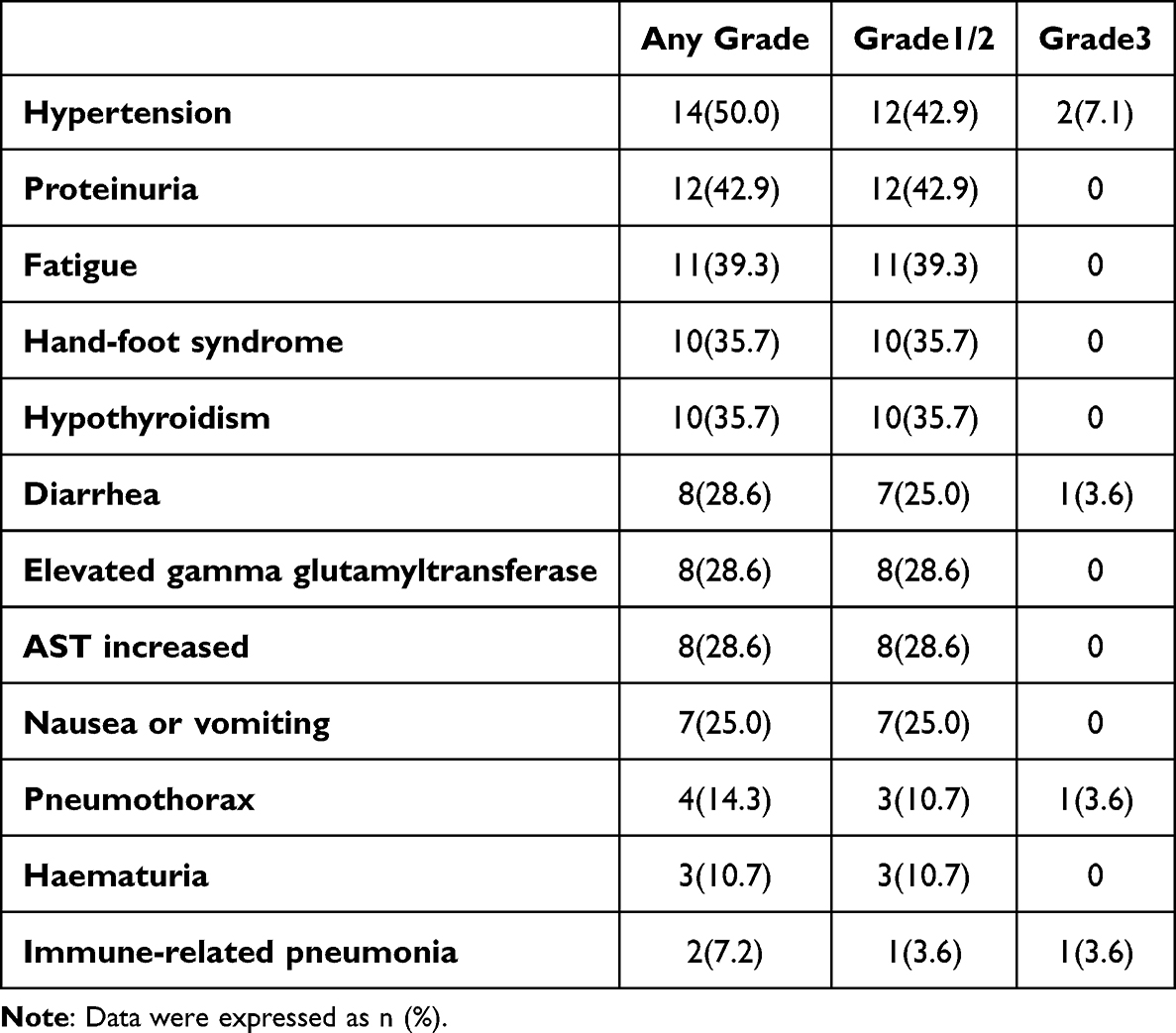 |
Table 4 Summary of Treatment-Related Adverse Events in All Patients |
Discussion
For the majority of soft tissue sarcoma subtypes, palliative anthracycline-based chemotherapy, alone or in combination with other cytotoxic agents, is currently considered the standard first-line treatment for patients with advanced or metastatic disease. However, not all patients with advanced or metastatic soft tissue sarcoma respond to conventional chemotherapy.5 In these instances, TKIs therapy are becoming an increasingly important treatment option, especially for patients who are resistant to or have not experienced satisfactory outcomes with conventional chemotherapy.10 Pazopanib has shown effectiveness in extending progression-free survival in patients with metastatic non-adipocytic soft tissue sarcoma following prior standard chemotherapy, with median PFS of 4.6 months.33 It is the first TKI that is approved for the treatment of patients with advanced soft tissue sarcoma who have undergone prior chemotherapy. Additionally, anlotinib has received approval in China for the treatment of patients with refractory advanced soft tissue sarcoma, demonstrating a median PFS of 5.6 months.34 However, the subsequent treatment after the failure of TKIs remains quite challenging.
Recent studies indicate that re-challenging with multi-targeted tyrosine kinase inhibitors can serve as an effective treatment approach for patients with sarcomas. A randomized Phase II trial showed that regorafenib has modest activity in the treatment of patients with metastatic non-adipocytic soft tissue sarcoma who have received prior chemotherapy and pazopanib.35 The observed median progression-free survival was 2.1 months. A retrospective study revealed that the median PFS for patients with advanced soft tissue sarcoma undergoing multi-targeted TKI rechallenge therapy was 3.3 months.36 The immunomodulatory properties of anti-angiogenic agents indicate that combining anti-angiogenic therapy with immunotherapy may constitute an effective approach for the treatment of sarcomas.37,38 In this study, we observed that following failure of initial TKI therapy, 64.3% of patients with metastatic STS experienced clinical benefit from treatment with lenvatinib combined with PD-1 blockades. The median PFS was 4.8 months, and the median OS was 23 months. Based on these findings, reinitiating treatment with lenvatinib in combination with PD-1 blockades may offer a beneficial approach in managing refractory soft tissue sarcoma. To the best of our knowledge, this represents the first documented report assessing the potential efficacy of rechallenge with lenvatinib and PD-1 blockades in metastatic soft tissue sarcoma patients following the development of resistance to initial TKI therapy.
When compared to their respective monotherapies, the combination of lenvatinib and PD-1 inhibitors demonstrated enhanced antitumor activity, leading to higher objective response rates and significant improvements in survival outcomes for patients with solid tumors.39 Previous studies have provided preliminary evidence suggesting the potential benefits of combining lenvatinib with PD-1 inhibitors in patients with advanced STS. A case report documents tumor regression following treatment with pembrolizumab and lenvatinib in a patient with recurrent leiomyosarcoma.40 Sujana Movva et al subsequently documented the effectiveness of combining lenvatinib with pembrolizumab in patients with sarcoma in a prospective, open-label, single-institution, non-randomized study.28 Participants in the study had not received any previous treatment with TKIs or immunomodulatory agents. This study identified evidence of activity for lenvatinib and pembrolizumab in synovial sarcoma, MPNST, and osteosarcoma. In the UPS and MPNST/synovial cohorts, the best overall response rates at 27 weeks were 25% and 30%, respectively. Additional responses were observed in angiosarcoma and UPS. The overall response rate was 15.2%. The median PFS varied from 9.8 weeks in the LMS cohort to 34 weeks in the vascular cohort. In our study, none of the 28 patients achieved complete or partial responses; however, 18 patients demonstrated stable disease. The median PFS was 4.8 months, while the median OS was 23 months. The reduction in ORR may be attributable to multiple factors. First, in our study, all patients had previously experienced failure with TKIs therapy prior to receiving lenvatinib and PD-1 blockades, and 80% of the cohort had also undergone immunotherapy with PD-1 blockades. Second, in the present study, patients with diminished performance status were included; notably, those with an ECOG score of 2 or higher comprised 53.6% of the study population. Third, the initial dosage of lenvatinib in our study was set at a lower level, determined based on the patient’s body weight: either 8 mg or 12 mg once daily. Finally, our study encompassed a broader range of histological subtypes, including five cases of ASPS and 3 cases of fibrosarcoma. The antitumour efficacy of TKI rechallenge remains poorly understood. One potential explanation is the variation in targets and affinities among multi-targeted TKIs.
The occurrence of adverse events observed in our study was noteworthy; however, the majority of these events were manageable, consistent with previously reported data for the combination. A systematic review has confirmed the safety and efficacy of pembrolizumab in combination with lenvatinib for patients with advanced solid tumors.39 The combination therapy has demonstrated greater effectiveness compared to pembrolizumab or lenvatinib monotherapy across multiple cancer types, with manageable adverse effects.
The present study has some limitations. First, this study is retrospective and involves a limited sample size, which may introduce selection bias. Additionally, this study does not include a control group, which limits the ability to directly compare the efficacy of lenvatinib combined with PD-1 blockades to that of each monotherapy individually. Nonetheless, this study remains a valuable reference for future research.
Conclusion
Our findings indicate that patients with metastatic STS may potentially benefit from the combination of lenvatinib and PD-1 blockades following the failure of prior TKI therapy. The effectiveness of this combination treatment in STS patients with resistance to TKI therapies warrants further investigation through larger cohort studies.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author Jin Wang ([email protected]). The data are not publicly available due to privacy or ethical restrictions.
Patient Consent and Ethics Approval
The need for patient informed consent was waivered due to the retrospective nature of the study, and ethical approval was obtained from the ethics committee of our hospital.
Funding
This study did not receive any funding or financial support.
Disclosure
There is no conflict of interest.
References
1. Sbaraglia M, Bellan E, Dei Tos AP. The 2020 WHO classification of soft tissue tumours: news and perspectives. Pathologica. 2021;113(2):70–11. doi:10.32074/1591-951X-213
2. Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2022. Ca A Cancer J Clin. 2022;72(1):7–33. doi:10.3322/caac.21708
3. Coindre JM, Terrier P, Bui NB, et al. Prognostic factors in adult patients with locally controlled soft tissue sarcoma. A study of 546 patients from the French Federation of Cancer Centers Sarcoma Group. J Clin Oncol. 1996;14(3):869–877. doi:10.1200/JCO.1996.14.3.869
4. von Mehren M, Kane JM, Agulnik M, et al. Soft tissue sarcoma, version 2.2022, NCCN clinical practice guidelines in oncology. J Nat Comprehensive Cancer Network. 2022;20(7):815–833. doi:10.6004/jnccn.2022.0035
5. Judson I, Verweij J, Gelderblom H, et al. Doxorubicin alone versus intensified doxorubicin plus ifosfamide for first-line treatment of advanced or metastatic soft-tissue sarcoma: a randomised controlled Phase 3 trial. Lancet Oncol. 2014;15(4):415–423. doi:10.1016/S1470-2045(14)70063-4
6. Italiano A, Mathoulin-Pelissier S, Cesne AL, et al. Trends in survival for patients with metastatic soft-tissue sarcoma. Cancer. 2011;117(5):1049–1054. doi:10.1002/cncr.25538
7. Gamboa AC, Gronchi A, Cardona K. Soft-tissue sarcoma in adults: an update on the current state of histiotype-specific management in an era of personalized medicine. Ca A Cancer J Clin. 2020;70(3):200–229. doi:10.3322/caac.21605
8. Gronchi A, Miah AB, Dei Tos AP, et al. Soft tissue and visceral sarcomas: ESMO-EURACAN-GENTURIS Clinical Practice Guidelines for diagnosis, treatment and follow-up(☆). Annals Oncol. 2021;32(11):1348–1365. doi:10.1016/j.annonc.2021.07.006
9. Pautier P, Italiano A, Piperno-Neumann S, et al. Doxorubicin alone versus doxorubicin with trabectedin followed by trabectedin alone as first-line therapy for metastatic or unresectable leiomyosarcoma (LMS-04): a randomised, multicentre, open-label phase 3 trial. Lancet Oncol. 2022;23(8):1044–1054. doi:10.1016/S1470-2045(22)00380-1
10. Spalato-Ceruso M, Ghazzi NE, Italiano A. New strategies in soft tissue sarcoma treatment. J Hematol Oncol. 2024;17(1):76. doi:10.1186/s13045-024-01580-3
11. Casali PG, Abecassis N, Aro HT, et al. Soft tissue and visceral sarcomas: ESMO-EURACAN Clinical Practice Guidelines for diagnosis, treatment and follow-up. Annals Oncol. 2018;29(Suppl 4):iv51–iv67. doi:10.1093/annonc/mdy096
12. Yuan J, Li X, Yu S. Molecular targeted therapy for advanced or metastatic soft tissue sarcoma. Cancer Contr. 2021;28:10732748211038424. doi:10.1177/10732748211038424
13. Kyriazoglou A, Gkaralea LE, Kotsantis I, et al. Tyrosine kinase inhibitors in sarcoma treatment. Oncol Lett. 2022;23(6):183. doi:10.3892/ol.2022.13303
14. Smolle MA, Szkandera J, Andreou D, Palmerini E, Bergovec M, Leithner A. Treatment options in unresectable soft tissue and bone sarcoma of the extremities and pelvis - a systematic literature review. EFORT Open Rev. 2020;5(11):799–814. doi:10.1302/2058-5241.5.200069
15. Flippot R, Biondani P, Auclin E, et al. Activity of EGFR tyrosine kinase inhibitors in NSCLC with refractory leptomeningeal metastases. J Thoracic Oncol. 2019;14(8):1400–1407. doi:10.1016/j.jtho.2019.05.007
16. Elaidi R, Harbaoui A, Beuselinck B, et al. Outcomes from second-line therapy in long-term responders to first-line tyrosine kinase inhibitor in clear-cell metastatic renal cell carcinoma. Annals Oncol. 2015;26(2):378–385. doi:10.1093/annonc/mdu552
17. Scott LJ. Lenvatinib: first global approval. Drugs. 2015;75(5):553–560. doi:10.1007/s40265-015-0383-0
18. Felicetti F, Nervo A, Piovesan A, et al. Tyrosine kinase inhibitors rechallenge in solid tumors: a review of literature and a case description with lenvatinib in thyroid cancer. Expert Rev Anticancer Ther. 2017;17(12):1093–1098. doi:10.1080/14737140.2017.1390432
19. Song G, Tang Q, Lu J, et al. Lenvatinib monotherapy versus lenvatinib in combination with PD-1 blockades as re-challenging treatment for patients with metastatic osteosarcoma: a real-world study. Drug Des Devel Ther. 2025;19:1119–1128. doi:10.2147/DDDT.S501742
20. Kosaka Y, Kawaoka T, Kosaka M, et al. Successful lenvatinib re-challenge following atezolizumab plus bevacizumab combination therapy failure for unresectable hepatocellular carcinoma. Internal Med. 2023;62(12):1771–1774. doi:10.2169/internalmedicine.9581-22
21. Nakamichi S, Nokihara H, Yamamoto N, et al. A Phase 1 study of lenvatinib, multiple receptor tyrosine kinase inhibitor, in Japanese patients with advanced solid tumors. Cancer Chemother Pharmacol. 2015;76(6):1153–1161. doi:10.1007/s00280-015-2899-0
22. Chen TW, Hsu CL, Hong RL, et al. A single-arm phase Ib/II study of lenvatinib plus eribulin in advanced liposarcoma and leiomyosarcoma. Clin Cancer Res. 2022;28(23):5058–5065. doi:10.1158/1078-0432.CCR-22-2092
23. Fazel M, Dufresne A, Vanacker H, Waissi W, Blay JY, Brahmi M. Immunotherapy for soft tissue sarcomas: anti-PD1/PDL1 and beyond. Cancers. 2023;15(6):1643. doi:10.3390/cancers15061643
24. Anastasiou M, Kyriazoglou A, Kotsantis I, et al. Immune checkpoint inhibitors in sarcomas: a systematic review. Immuno-Oncol Technol. 2023;20:100407. doi:10.1016/j.iotech.2023.100407
25. Cao Y, Wang W, Xu H, et al. Efficacy of immune checkpoint inhibitors in the treatment of soft tissue sarcoma: a systematic review and meta-analysis of clinical trials. Int Immunopharmacol. 2025;148:114070. doi:10.1016/j.intimp.2025.114070
26. Adachi Y, Kamiyama H, Ichikawa K, et al. Inhibition of FGFR reactivates IFNγ signaling in tumor cells to enhance the combined antitumor activity of lenvatinib with Anti-PD-1 antibodies. Cancer Res. 2022;82(2):292–306. doi:10.1158/0008-5472.CAN-20-2426
27. Kato Y. Lenvatinib enhances antitumor immunity of anti-PD-1 antibody. Int J Clin Oncol. 2025;30(4):666–673. doi:10.1007/s10147-025-02721-5
28. Movva S, Seier K, Avutu V, et al. Histology-specific clinical trial of lenvatinib and pembrolizumab in patients with sarcoma. Clin Cancer Res. 2024;30(24):5612–5619. doi:10.1158/1078-0432.CCR-24-2519
29. Fang W, Yang Y, Ma Y, et al. Camrelizumab (SHR-1210) alone or in combination with gemcitabine plus cisplatin for nasopharyngeal carcinoma: results from two single-arm, phase 1 trials. Lancet Oncol. 2018;19(10):1338–1350. doi:10.1016/S1470-2045(18)30495-9
30. Xu J, Zhang Y, Jia R, et al. Anti-PD-1 antibody SHR-1210 combined with apatinib for advanced hepatocellular carcinoma, gastric, or esophagogastric junction cancer: an open-label, dose escalation and expansion study. Clin Cancer Res. 2019;25(2):515–523. doi:10.1158/1078-0432.CCR-18-2484
31. Shi Y, Su H, Song Y, et al. Safety and activity of sintilimab in patients with relapsed or refractory classical Hodgkin lymphoma (ORIENT-1): a multicentre, single-arm, Phase 2 trial. Lancet Haematol. 2019;6(1):e12–e9. doi:10.1016/S2352-3026(18)30192-3
32. Ansell SM. Sintilimab: another effective immune checkpoint inhibitor in classical Hodgkin lymphoma. Lancet Haematol. 2019;6(1):e2–e3. doi:10.1016/S2352-3026(18)30210-2
33. van der Graaf WT, Blay JY, Chawla SP, et al. Pazopanib for metastatic soft-tissue sarcoma (PALETTE): a randomised, double-blind, placebo-controlled phase 3 trial. Lancet. 2012;379(9829):1879–1886. doi:10.1016/S0140-6736(12)60651-5
34. Shen G, Zheng F, Ren D, et al. Anlotinib: a novel multi-targeting tyrosine kinase inhibitor in clinical development. J Hematol Oncol. 2018;11(1):120. doi:10.1186/s13045-018-0664-7
35. Penel N, Mir O, Wallet J, et al. A double-blind placebo-controlled randomized phase II trial assessing the activity and safety of regorafenib in non-adipocytic sarcoma patients previously treated with both chemotherapy and pazopanib. Eur J Cancer. 2020;126:45–55. doi:10.1016/j.ejca.2019.12.001
36. Liu J, Deng YT, Wu X, Jiang Y. Rechallenge with multi-targeted tyrosine kinase inhibitors in patients with advanced soft tissue sarcoma: a single-center experience. Cancer Manage Res. 2021;13:2595–2601. doi:10.2147/CMAR.S300430
37. Tian L, Goldstein A, Wang H, et al. Mutual regulation of tumour vessel normalization and immunostimulatory reprogramming. Nature. 2017;544(7649):250–254. doi:10.1038/nature21724
38. Nuti M, Zizzari IG, Botticelli A, Rughetti A, Marchetti P. The ambitious role of anti angiogenesis molecules: turning a cold tumor into a hot one. Cancer Treat Rev. 2018;70:41–46. doi:10.1016/j.ctrv.2018.07.016
39. Mo DC, Luo PH, Huang SX, Wang HL, Huang JF. Safety and efficacy of pembrolizumab plus lenvatinib versus pembrolizumab and lenvatinib monotherapies in cancers: a systematic review. Int Immunopharmacol. 2021;91:107281. doi:10.1016/j.intimp.2020.107281
40. Mehta N, Lee SS, Salame G. A case of pembrolizumab and lenvatinib as an alternative therapy for leiomyosarcoma. Gynecol Oncol Rep. 2023;45:101145. doi:10.1016/j.gore.2023.101145
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Feasibility and Tolerability of Lenvatinib, Plus PD-1 Blockades for Patients with Unresectable Hepatocellular Carcinoma: A Retrospective Exploratory Study
Jia M, Jia JK, Xu J, Xue HZ
Cancer Management and Research 2022, 14:2625-2638
Published Date: 2 September 2022
Significance of Physical Status and Liver Function Reserve for Outcome of Patients with Advanced Hepatocellular Carcinoma Receiving Lenvatinib Treatment
Chan KM, Lai Y, Hung HC, Lee JC, Cheng CH, Wang YC, Wu TH, Lee CF, Wu TJ, Chou HS, Wang CT, Chai PM, Lien HY, Lee WC
Journal of Hepatocellular Carcinoma 2023, 10:281-290
Published Date: 18 February 2023
Feasibility and Safety of the Clinical Outcomes of TACE Combined with Lenvatinib and PD-1 Blockades in the Treatment of Hepatocellular Carcinoma with Portal Vein Tumor Thrombus: A Retrospective Exploratory Study
Sun W, Liu Y, Wang L
International Journal of General Medicine 2024, 17:3627-3640
Published Date: 21 August 2024
Lenvatinib Monotherapy Versus Lenvatinib in Combination with PD-1 Blockades as Re-Challenging Treatment for Patients with Metastatic Osteosarcoma: A Real-World Study
Song G, Tang Q, Lu J, Xu H, Wang A, Deng C, Wu H, Hu J, Zhu X, Wang J
Drug Design, Development and Therapy 2025, 19:1119-1128
Published Date: 18 February 2025