Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
A Two-Pronged Educational Intervention for Caregivers to Prevent Residential Pesticide Exposure Among Thai Young Children Living in Agricultural Area
Authors Muenchamnan N, Naksen W, Ong-Artborirak P ![]()
Received 21 May 2023
Accepted for publication 9 August 2023
Published 15 August 2023 Volume 2023:16 Pages 2339—2350
DOI https://doi.org/10.2147/JMDH.S422259
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Nutnichawan Muenchamnan,1 Warangkana Naksen,1 Parichat Ong-Artborirak1,2
1Faculty of Public Health, Chiang Mai University, Chiang Mai, Thailand; 2Department of Research and Medical Innovation, Faculty of Medicine Vajira Hospital, Navamindradhiraj University, Bangkok, Thailand
Correspondence: Warangkana Naksen, Faculty of Public Health, Chiang Mai University, Chiang Mai, 50200, Thailand, Tel +66-53-942507, Fax +66-53-942525, Email [email protected] Parichat Ong-Artborirak, Department of Research and Medical Innovation, Faculty of Medicine Vajira Hospital, Navamindradhiraj University, Bangkok, 10300, Thailand, Tel +66-2244-3522, Email [email protected]
Background: Residential pesticide exposure can be harmful to the health of young children, particularly in agricultural areas. It is critical to educate their caregivers on pesticide exposure prevention. The purpose of this study was to determine the effectiveness of a two-pronged education intervention for caregivers in preventing pesticide exposure among Thai young children living in agricultural areas.
Methods: This was an experimental study with 90 primary caregivers of young children aged 6 months to 5 years. Thirty caregivers each were assigned to one of three groups: booklet plus lecture intervention, only booklet intervention, and control. Caregivers in both interventions received a booklet that educated them on residential pesticide exposure and prevention. The caregivers in the booklet plus lecture group also attended a 2-hour lecture with the same content as the booklet. A questionnaire was developed to assess caregivers’ knowledge, attitudes, intention, and behaviors regarding residential pesticide exposure and prevention in children. Face-to-face interviews were conducted at their homes three times: baseline, post-intervention, and follow-up (three weeks after the end of the intervention).
Results: Linear mixed models showed that, from baseline to post-intervention, the intervention effect on knowledge and attitude in both intervention groups, as well as intention in the booklet plus lecture group, was significant (p< 0.05). From baseline to follow-up, the knowledge, attitude, intention, and behavior scores in both intervention groups increased significantly more than the control group (p< 0.01). Only the attitude score increased more in the booklet plus lecture group than in the booklet group at post-intervention (p=0.009) and follow-up (p=0.003).
Conclusion: Both the booklet plus lecture method and the booklet method alone have a positive effect on improving the caregiver’s knowledge and behaviors regarding pesticide exposure prevention at home. Thus, providing a booklet to caregivers to reduce children’s risk of pesticide exposure is recommended.
Keywords: insecticide, pesticide, education, booklet, lecture, caregiver, children
Introduction
Pesticides are still used extensively in agriculture around the world, particularly in tropical region like Thailand, to protect crops and increase yields. Household insecticides are also commonly used to prevent mosquitos and other insects. These pesticides can be harmful to people’s health, especially children. Pesticide exposure occurs in farming families as a result of pesticide drift and pesticide take-home. Many studies have found that children living in farming communities are at risk of being exposed to pesticides carried home by their parents when they return from farming.1,2 Home pesticide use for insect control may be a significant source of exposure in farmworker homes.3 Household insecticide use leaves residue in residential environments such as food, air, and floor dust.4,5 Young children can be exposed to pesticide residues through ingestion, inhalation, and dermal routes from activities such as crawling, playing on the ground or with toys, and sucking.6,7 In Thailand, studies have found a high risk of residential pesticide exposure from agriculture or household use among young children in both rural and urban areas, depending on caregivers, hygiene habits, and child activities.8–12
Numerous studies have shown that exposure to residential pesticides may have a negative impact on children’s health, including growth, behavioral disorders, neurodevelopment, brain tumors, and cancer.13–19 As a result, young children should be exposed to residential pesticides as little as possible.20,21 Because children are unable to care for themselves, caregivers such as parents should be provided with behavioral intervention to minimize children’s exposure. Education and training are required to promote knowledge and behavior regarding pesticide use among caregivers of children aged 1–6 years.22 Many experimental studies have been conducted to investigate the effects of interventions aimed at protecting children in farming families from pesticide exposure.3,23–31 However, there is little evidence for delivering information about household insecticides, and to date, no intervention study to reduce pesticide exposure among Thai children has been found.
Education via booklet has proven to be a generally effective intervention of behavioral change for parents and guardians in preventing their children from being at risk.32 It is also suggested that multicomponent interventions may be more effective.33,34 When considering a practical and simple format for delivering education with knowledge retention in the Thai rural context, a booklet and lecture via PowerPoint may be appropriate and effective for child caregivers. Therefore, the purpose of this pilot study was to determine the effectiveness of a two-pronged education intervention (booklet and lecture) for caregivers in preventing residential pesticide exposure among Thai young children living in agricultural areas. The findings of this study can be used to educate parents, grandparents, and guardians, as well as the general public, about the effects of household insecticides and prevention. It is also expected to raise awareness and make recommendations for reducing children’s risk of pesticide exposure to individuals, communities, or organizations involved in health policy and planning.
Materials and Methods
Study Design and Subjects
The research is a three-arm experimental study with a pretest-posttest design, two intervention groups and one control group. The study was carried out in agricultural areas in the Wiang Haeng District of Chiang Mai Province, Northern Thailand. In the study area, commercial household insecticide products containing pyrethroids that are widely used include aerosol sprays, electric mosquito repellent liquid vaporizers, mosquito coils, and ant and cockroach killer chalk/powder. The most common names for the active ingredient in these products are cypermethrin, prallethrin, imiprothrin, phenothrin, metofluthrin, permethrin, allethrin, deltamethrin, bifenthrin, and esbiothrin.
To avoid potential contamination, the study areas of three groups were purposively chosen from three villages, each group in one village. The intervention and control groups are separated by 10–15 kilometers. The research project was then publicized in order to recruit subjects for the study using convenience sampling. Village health volunteers visited homes to compile a list of 30 child caregivers in each village. The subjects who met the following inclusion criteria were invited to take part in this study: 1) are Thai primary caregivers living with their children aged 6 months to 5 years; 2) have a history of household pesticide use in the previous six months; and 3) are literate and communicate in Thai.
The G*power program was used to calculate the sample size for three groups using the formula for comparing more than two independent means with an effect size of 0.4, a 95% confidence level, and an 80% power. The minimum sample size for each group in this study was 22 caregivers. To account for possible loss to follow-up, this number was increased to 30 individuals for each group: 1) booklet plus lecture group, 2) booklet group, and 3) control group (no intervention). The study was approved by the Committee of Research Ethics, Faculty of Public Health, Chiang Mai University (No. ET026/2564). All caregivers who participated in the study provided written informed consent.
Intervention
A two-pronged intervention consisted of a booklet and a lecture to educate caregivers in order to prevent pesticide exposure of their children. The booklet was designed to deliver a guide and details about pesticides through text and images. Many research findings have been referenced to support many of the statements in the booklet. Its contents included knowledge about household insecticides, sources of pesticide exposure (agriculture, home, and public health), factors related to pesticide exposure (eg, take-home pathway, child behaviors and activities, and characteristics of insecticide use), routes of pesticide exposure (oral, dermal, and inhalation) via various media (food and water, surfaces, air, and soil), effects of pesticide exposure (acute and chronic), and preventing pesticide exposure (eg, using less toxic substances, home cleaning, washing vegetables and fruits, hygiene habits, safe use, storage, and disposal). Before printing, the booklet was reviewed by experts for suitability and validity and revised based on their recommendations. The second prong was an onsite lecture with PowerPoint that covered the same information as the booklet. This activity lasted about two hours and only 30 caregivers from the booklet plus lecture group attended in a community room. During this session, the caregivers can ask for clarification and the researcher can check for understanding.
Questionnaire
A five-part questionnaire for child caregivers was developed based on literature reviews. In the first part, the questionnaire was designed to collect general information about caregivers and their young children (eg, gender, age, marital status, education, occupation, perceived income sufficiency, relationship to the child, and duration of child care), as well as information about household insecticide use (the need for household insecticide training or education, frequency and duration of using household insecticides, and having other family members who use household insecticides). The second part, knowledge about residential pesticide exposure, included 17 questions about sources of exposure, risk factors, route of exposure, health effects, and prevention. Each item was scored 1 for the correct answer and 0 for the incorrect or unsure answer, for a total possible score of 17. Examples of these questions were “Household insecticides can be absorbed through the skin of young children”, “Household pesticides can leave residues on toys for young children” and “Residential pesticide exposure may have an impact on the nervous system and brain development of young children”. The third part, attitude regarding residential pesticide exposure, included 12 questions. Each item was a positive or negative question with five rating scales ranging from strongly disagree to strongly agree. There were 12 to 60 points in total possible. Examples of these questions were “You think that household insecticides are only harmful to mosquitoes and bugs, not to young children”, “You think that household pesticides can only harm weak children” and “You think that young children should be exposed to as little pesticide residue as possible”.
The fourth part, intention to prevent child exposure to residential pesticides, included 10 questions. Each item was a positive question with five rating scales ranging from lowest to highest level. The total score was between 10 and 50 points. Examples of these questions were “I intend to reduce my use of household insecticides”, “I intend to stop using household insecticides or instead use safer alternatives such as natural insect repellents” and “I intend to clean my children’s toys more frequently”. The last part, behaviors to prevent child exposure to residential pesticides, included 10 questions. Each item was either a positive or negative question with a five-point rating scale ranging from never to always. The final score ranged from 10 to 50 points. Examples of these questions were “You used household insecticides while there were young children nearby”, “You clean your home with a damp or wet cloth after using household insecticides” and “You wash your children’s hands or remind them to wash their hands”. All parts were reviewed and validated by a panel of three experts in community, environmental, and occupational health. The questionnaire was pilot tested for reliability with 20 child caregivers who lived in a nearby area and shared the same characteristics as the participants in this study. In terms of knowledge, the Kuder-Richardson (KR-20) coefficient was 0.79. Cronbach’s alpha coefficients for attitude, intention, and behavior were 0.88, 0.96, and 0.92, respectively.
Data Collection
Face-to-face interviews with caregivers were conducted at their homes three times: pre-intervention (baseline), immediately after intervention (post-intervention), and three weeks after the end of the intervention (follow-up). Caregivers with multiple children in the age range of interest were notified to provide information on their youngest children. At the beginning, all participants were asked about general information and household insecticide use, as well as their knowledge, attitudes, intentions, and behaviors about pesticide exposure and prevention. The booklet was then distributed at home to both intervention groups, including the booklet plus lecture group and the booklet group. One week after receiving the booklet, the researcher delivered a two-hour oral community lecture to the booklet plus lecture group to provide knowledge focused on the first prong intervention. Immediately after the end of the intervention, all three groups were interviewed to assess changes in knowledge, attitudes, and intentions. Similarly, the same questionnaire with behavioral questions was used to assess the effectiveness of educational interventions at the follow-up period (Figure 1). Two research assistants were trained in the interviewer-administered questionnaire. This study was carried out between March and April of 2022.
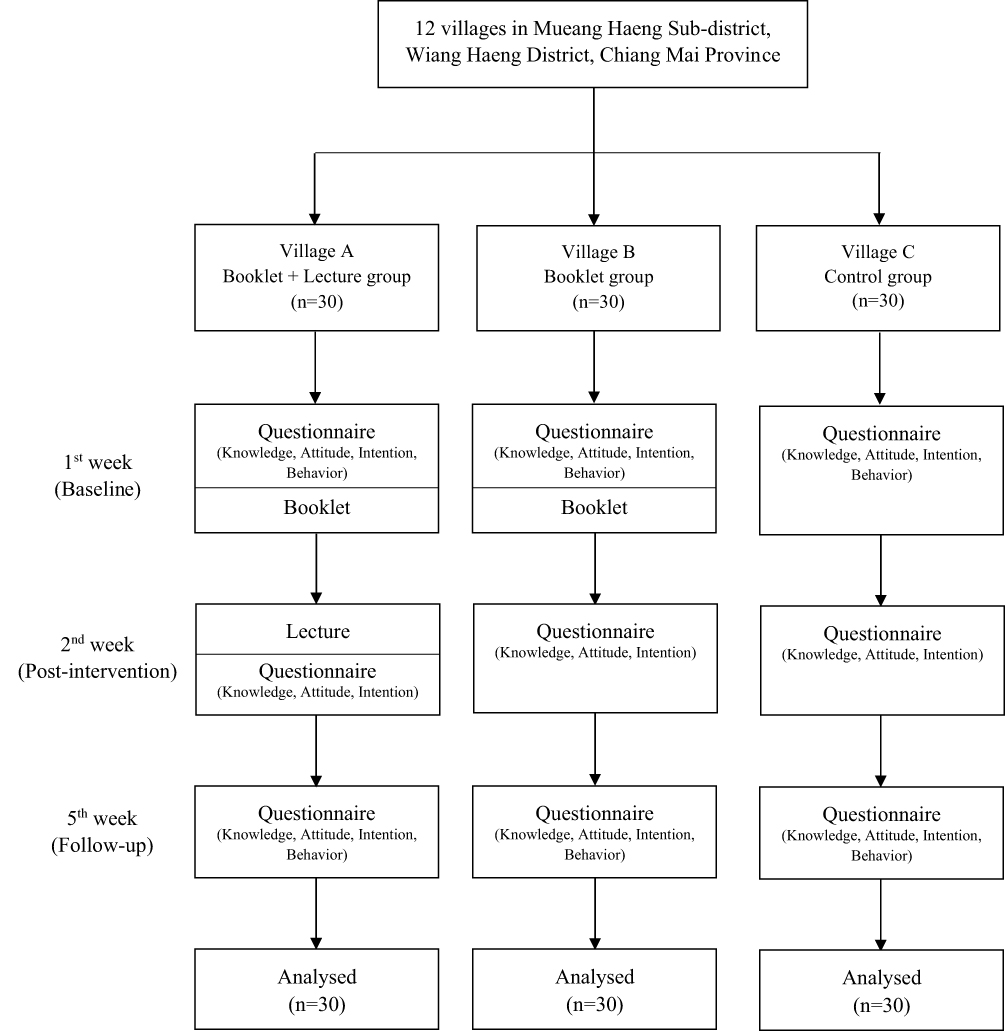 |
Figure 1 Data collection flowchart. |
Statistical Analysis
Data were analyzed using Stata/IC version 16.0 for Windows (StataCorp LP, College Station, TX, USA) and the level of significance for all statistical tests was set at 0.05. The general information about caregivers and their young children as well as the use of household insecticides among the three groups was compared using the chi-square test. The mean differences in knowledge, attitude, intention, and behavior about pesticide exposure and prevention among different groups at each measurement time were tested using one-way analysis of variance (ANOVA). A difference-in-difference analysis was performed using a linear mixed model with interaction between intervention and time to assess the magnitude of the intervention effect at post-intervention and follow-up compared to baseline.
Results
General information for 90 participants divided into three groups (booklet plus lecture group, booklet group, and control group) are shown in Table 1. The mean age of caregivers in the booklet plus lecture group was 36.8 years (SD=12.7), 38.4 years (SD=12.4) in the booklet group, and 39.9 years (SD=11.3) in the control group. The chi-square test revealed no statistically significant differences among the three groups in general information about caregivers such as gender, age, marital status, education, occupation, perceived income sufficiency, relationship to the child, and duration of child care, as well as general information about their young children such as gender and age. In terms of household insecticide use, there were no statistically significant differences among three groups in the need for training or education on household insecticides, frequency of using household insecticides, duration of using household insecticides, and having other family members who use household insecticides.
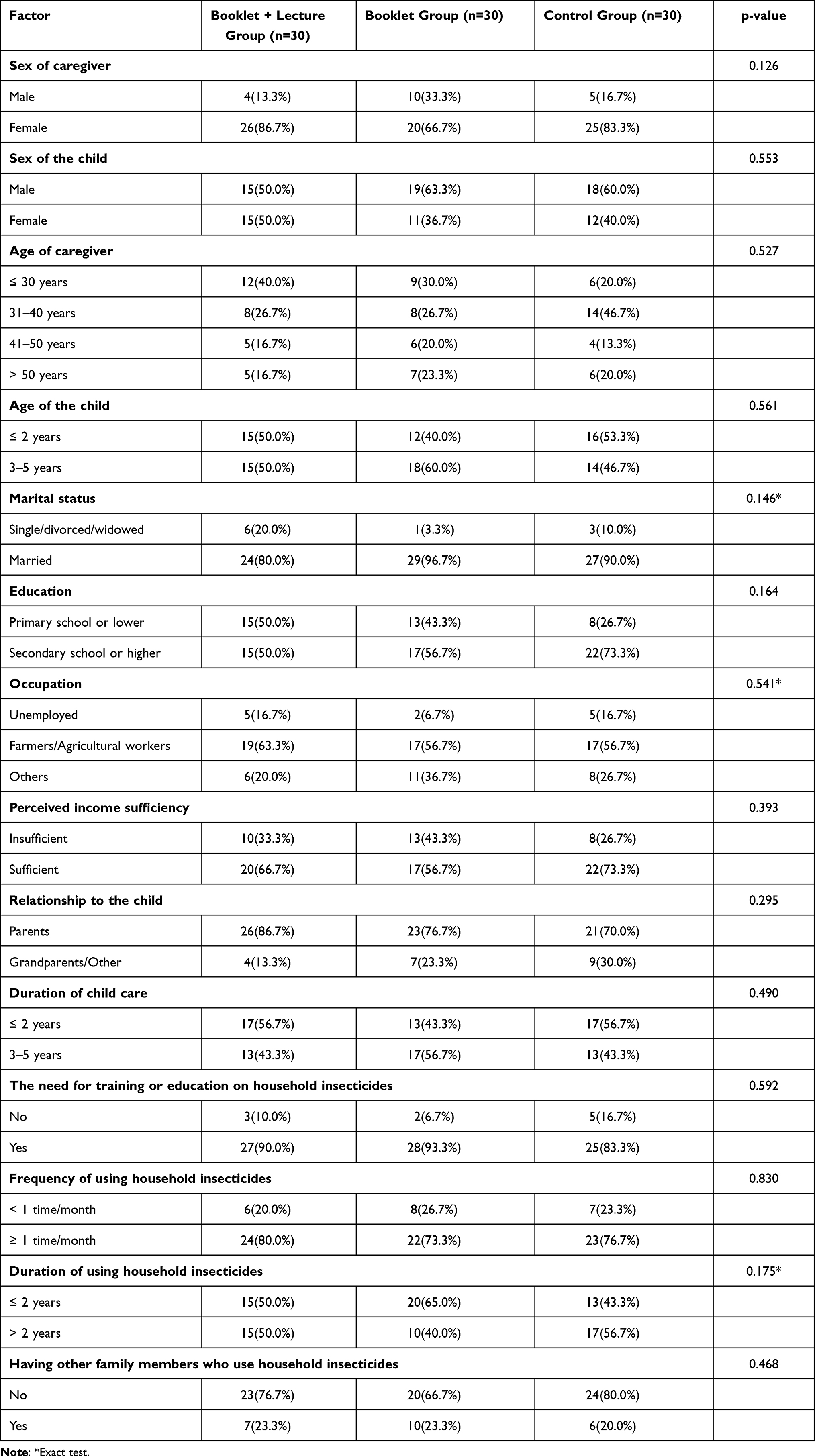 |
Table 1 General Information About Caregivers and Their Young Children as Well as the Use of Household Insecticides from Different Groups |
Table 2 compares caregivers’ knowledge, attitude, intention, and behavior regarding residential pesticide exposure and prevention at each time point in different groups. At baseline, there were no statistically significant differences in mean knowledge, attitude, intention, and behavior scores among the three groups. At post-intervention, post hoc tests using Bonferroni revealed that mean scores of knowledge, attitude, and intention in the two-pronged intervention group were significantly higher when compared to the control group (p<0.05), whereas only mean scores of knowledge and attitude in the booklet group were significantly higher when compared to the control group (p<0.05). At follow-up, the mean scores of knowledge, attitude, intention and behavior in both intervention groups were significantly higher than those in the control group (p<0.05).
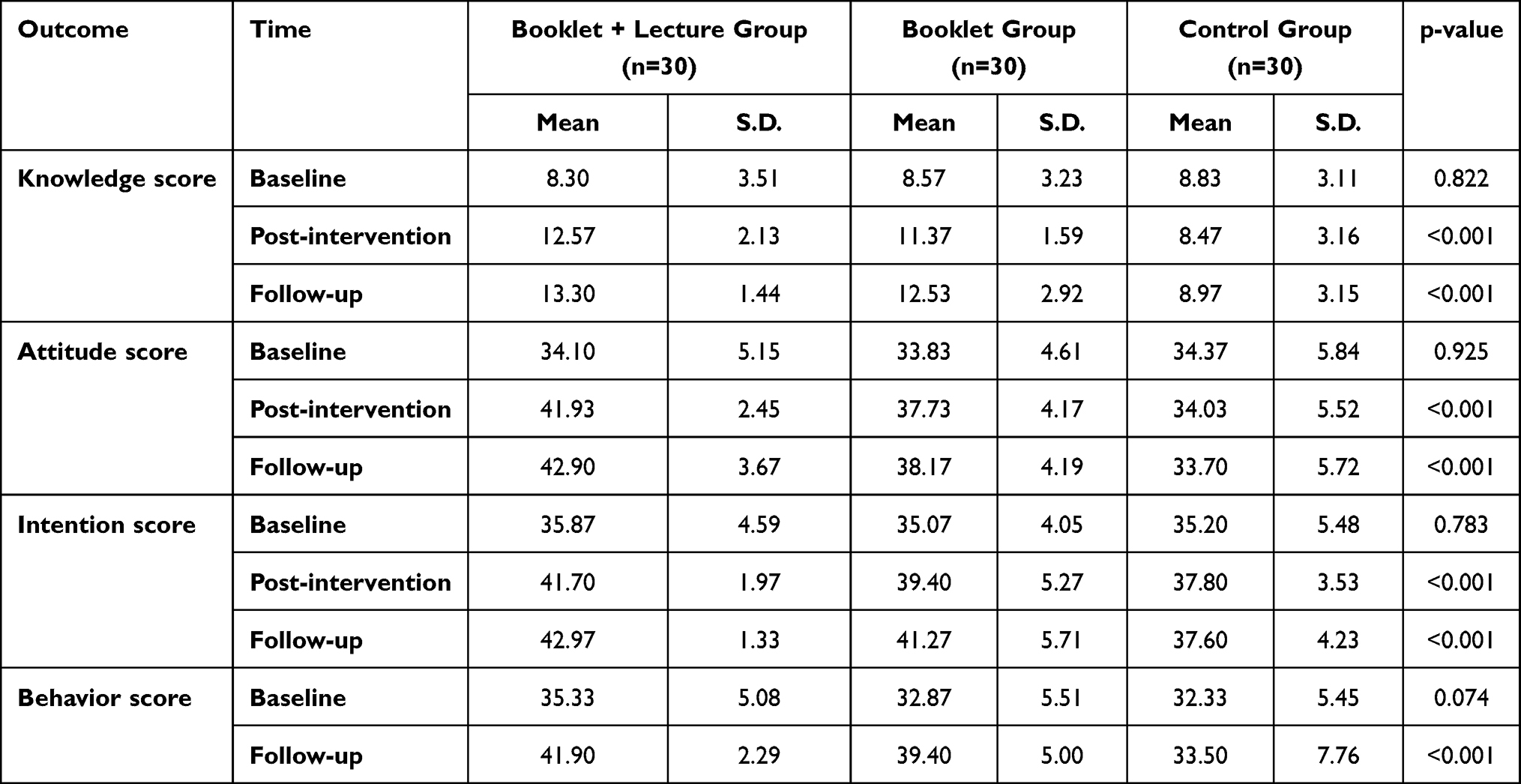 |
Table 2 Mean Score Comparison of Variables Studied Among Different Groups at Each Point of Measurement |
Table 3 shows the magnitude of the overall intervention effect by linear mixed models. From baseline to post-intervention, intention to prevent pesticide exposure in young children increased more in the booklet plus lecture group and the booklet group than in the control group by 3.23 points (p = 0.020) and 1.73 points (p = 0.212), respectively. From baseline to follow-up, the absolute effect of the booklet plus lecture group was 4.70 points for intention (p = 0.001), and 5.40 points for behavior (p = 0.006). Whereas the absolute effect of the booklet group was 3.80 points for intention (p = 0.002), and 5.37 points for behavior (p = 0.002). At post-intervention and follow-up, the intervention effect on knowledge and attitude in both groups was found to be significant (p < 0.01). In addition, attitude increased more in the booklet plus lecture group than in the booklet group by 3.93 points at post-intervention (p = 0.009) and 4.47 points at follow-up (p = 0.003), whereas there was no statistically significant difference in knowledge, intention, and behavior between the two interventions (Table 4).
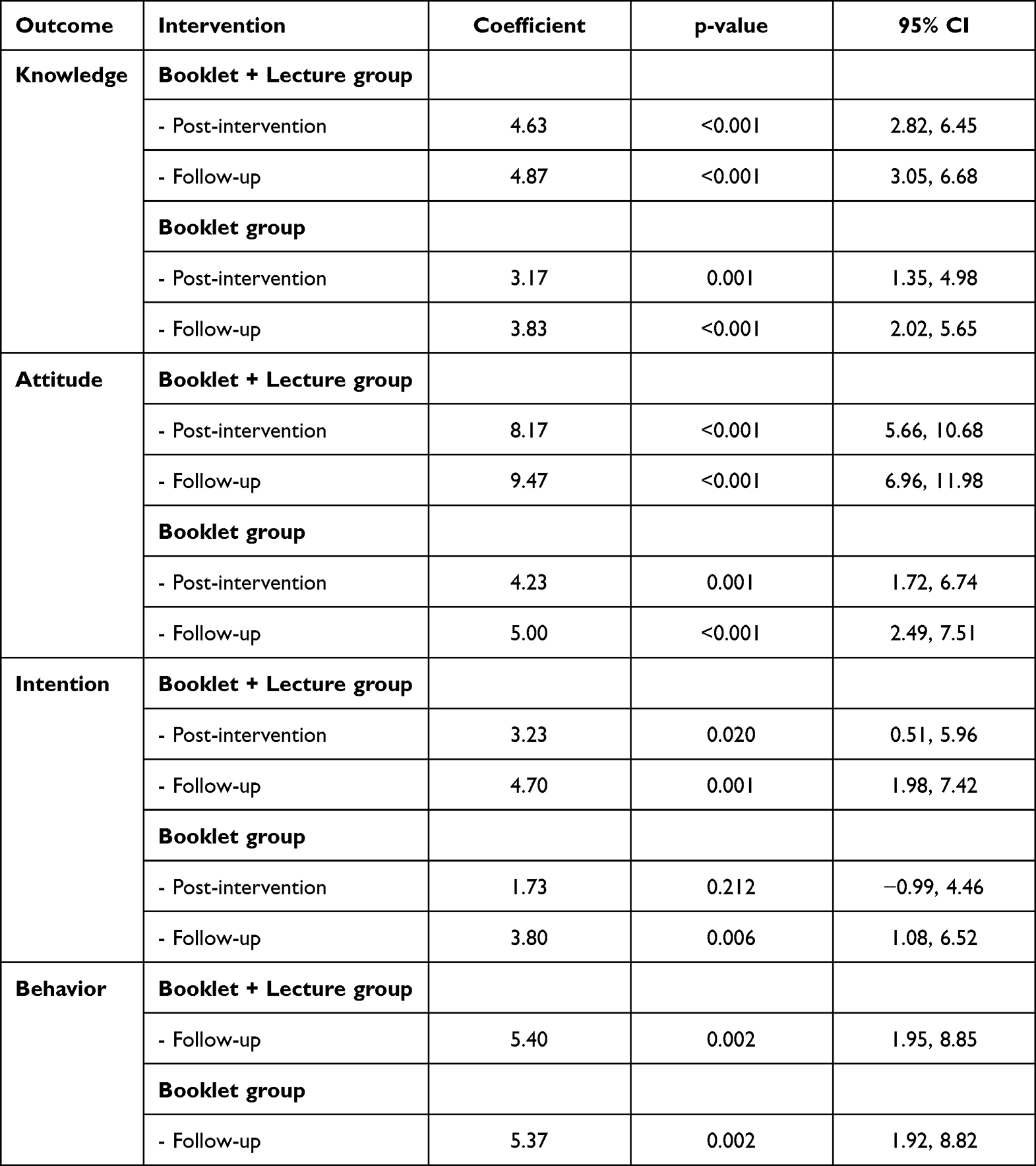 |
Table 3 Effects of the Program for Caregivers on Variables Studied at Post-Intervention and Follow-Up Compared to Baseline by Mixed Effects Model |
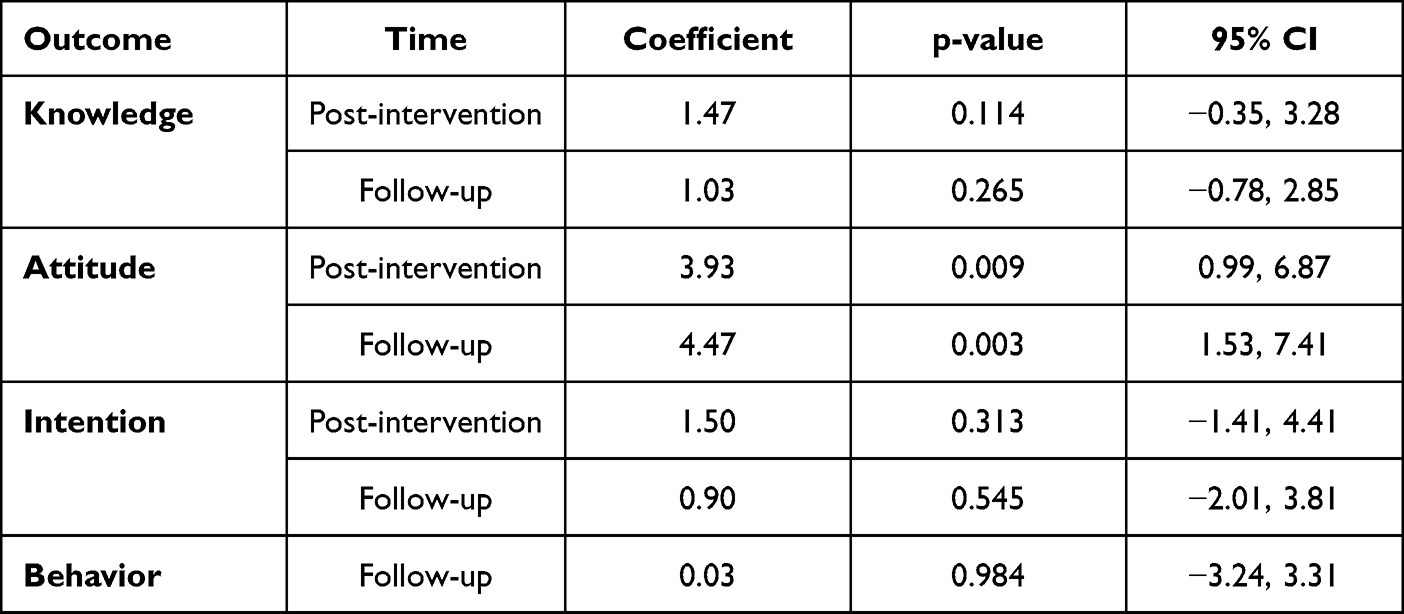 |
Table 4 Effects of a Two-Pronged Educational Intervention for Caregivers (vs Booklet Group) on Variables Studied at Post-Intervention and Follow-Up Compared to Baseline Using a Mixed Effects Model |
Discussion
This study examined the distribution of a booklet and onsite lecture intervention to educate Thai caregivers about pesticide exposure at home and improve pesticide preventive behaviors for their young children living in agricultural communities. Given that the booklet plus lecture was hypothesized to be the highest-intensity intervention for promoting preventive behaviors among caregivers, the increasing score in knowledge, attitude, and intention for the two-pronged intervention group was higher, as expected. However, there was only a statistically significant difference in attitude between the two intervention groups. This could be because caregivers in both intervention groups can access the booklet whenever they need information. The slightly higher increase in knowledge score may be due to participants being motivated again by an onsite lecture prior to data collection after the immediate end of intervention. Interaction from the lecture session may allow caregivers to concentrate and gain a deeper understanding and learning, as well as possibly improve knowledge retention. It may then encourage a positive attitude, resulting in a slightly higher than intention score in the two-pronged intervention group. According to a previous study, the most effective media used is a combination of print media such as booklets and electronic media such as power point presentations.35
Whereas behavior scores between two intervention groups may be comparable, implying that a booklet intervention alone may be sufficient to promote pesticide exposure prevention. Considered in terms of benefit, while reading a booklet is restricted to caregivers who are Thai literate, viewing a presentation may be suitable for illiterate people. This study may be limited by the short time frame (one month) for looking at behavior outcomes, which normally take time to change. Therefore, the study evaluating intervention effectiveness in the short term and long-term follow-up should be investigated further. A lecture intervention should also be considered.
In terms of booklet intervention, it has a significant impact on promoting caregivers’ good behavior for their children. Because the booklet provided evidence-based information, it may convince caregivers of the effectiveness of a health intervention.36 This study does not report having seen the booklets, which should be asked in the next study. The distribution of booklets is recommended as a low-cost effective method that has proven the effectiveness of an educational booklet suitable for knowledge dissemination in Thai rural communities. This is consistent with some studies that found a positive effect of booklet intervention on caregivers for child health care.32,37,38 Overall, the study revealed a significant intervention effect on knowledge, attitudes, intentions, and behaviors over time, with the exception of the intention score at post-intervention in the booklet group. More sessions of educational intervention to retain knowledge may be required for greater improvements as well as a greater likelihood of ensuring the continued existence of the gained knowledge and practice.
According to the KAP model, which is widely used to change behavior, knowledge is an important factor that leads to attitude and practice. It can be explained that when caregivers gain knowledge, they will consider the importance of caring for and protecting the health of young children, resulting in a shift in attitudes and an increased intention to perform good behaviors for children. Additionally, attitude plays an important role in the Theory of Planned Behavior (TPB), which contributes to behavioral intention and actual behavior.39 A change in intention can partially lead to a change in behavior. A study found that small-to-medium change in behavior results from a medium-to-large change in intention.40 However, this study showed the influence of the two interventions on the enhancement of caregiver intentions. The actual practice of caregivers in preventing pesticide exposure in children should be investigated and monitored. Biomonitoring of pesticides in children is suggested for future research.
The educational intervention that covered various aspects of residential pesticide exposure and prevention to children may have resulted in a higher knowledge score for both intervention groups. Because household insecticides are commonly used in Thailand, many caregivers may be unaware of the potential negative consequences of exposure in children. Concerningly, daily household insecticide use in Thai urban areas was reported at 79% for households that used insecticide products.9 At the pre-intervention, the caregivers had a low knowledge score for children’s health effects of pesticide exposure (eg behavioral disorders, neurodevelopment, brain tumors, blood cancer), pesticide exposure from flea and tick prevention pet products, pesticide residue contamination on children’s body skin, dermal route of pesticide exposure, pesticide exposure prevention, and pesticide drift and take-home for children in agricultural communities. As a result, education has enabled them to gain new and different perspectives on household insecticides. The intervention also highlighted the importance of knowledge for exposure prevention in promoting good caregiver behaviors and lowering the risks of young children. In line with previous research, some caregivers are unaware of the route of exposure and the negative effects of pesticides on children’s health.22,25
Regarding attitude, the caregivers scored low on questions at baseline about the effects of pesticide exposure; some incorrectly believed that insecticide use in the home could not be dangerous for children and could only harm weak children, as well as increasing resistance in the body for children who are exposed on a regular basis. Some caregivers thought that household insecticides decompose in the air after use, that cleaning the house after use is unnecessary, that young children’s clothes should not be washed separately from those who used agricultural pesticides, and that reading the package label before using household insecticides is a waste of time. Additionally, they had low scores on many intention questions at baseline, including stopping the use of household insecticides or using other safer substances, reducing the use of household insecticides to less, cleaning children’s toys more often, frequently washing children’s hands and feet or reminding them to wash their hands and feet, and reading the package label before using household insecticides. On many behavior questions at baseline, they also received low scores, including reading and following instructions on packaging labels of household insecticide products, using household insecticides while young children are nearby, reducing the frequency of use of household insecticides, using herbal insect repellents instead of, and cleaning the house with a damp or wet cloth after using household insecticides. At the post-intervention and follow-up, scores on attitudes, intentions, and behaviors among caregivers in both intervention groups increased in all items.
Our findings are consistent with previous research, which found that an education intervention (lecture and video) for farmer families to protect their children can significantly increase knowledge scores.24,25 A community-based education program for farmworkers and farmworker family members on reducing pesticide exposures at home and at work, with a focus on protecting children, resulted in a significant increase in knowledge about the routes of exposure, the vulnerability of children, and ways to minimize pesticide exposures, as well as improved behaviors.27 Significant improvements in pesticide-related knowledge and practices related to para-occupational exposure and residential pest control were observed among farmworker families after intervention.26 Another study found a significant increase in overall pesticide knowledge and increased protective behaviors at home after watching a pesticide exposure video intended for protecting children for migrant and seasonal farmworkers.28 According to a study in children, knowledge, attitude, and practice about pesticides improved significantly after receiving educational intervention among children aged 13 to 15 years working in agriculture.23 A home-based intervention to reduce pesticide exposures to farmworkers’ children reduced insecticide levels in their home from floor wipe samples.3
To our knowledge, this is the first study to look at the effects of delivering an educational intervention to reduce children’s residential pesticide exposure in Thailand. Despite the small sample size, statistical significance can be found in this study. These findings may not be generalizable to other child caregivers as participants were chosen using non-probability sampling. Using a questionnaire to assess changes in caregiver behaviors, social desirability bias may occur. Measurements of biomarkers for evaluating internal exposure in children, such as insecticide metabolites, are required to confirm the effectiveness of this intervention, as well as the adequacy of recommended prevention behaviors for reducing the children’s health risk.
Conclusion
This study demonstrates that a two-pronged educational intervention, consisting of a booklet and an onsite lecture, can be effective in providing caregiver knowledge about residential pesticide exposure and improving behaviors in exposure prevention of children living in agricultural areas. Implementing only the booklet showed that it is a simple design and efficient method. As a result, delivering a booklet to caregivers to reduce children’s risk of pesticide exposure is recommended for practical reasons. It is also anticipated that the booklet will be useful to caregivers in both agricultural and non-agricultural communities where child caregivers used household insecticides because the details particularly emphasized household insecticide exposure and prevention. More intervention studies are needed to evaluate approaches to minimizing child pesticide exposure.
Ethical Approval and Consent
The study was approved by the Committee of Research Ethics, Faculty of Public Health, Chiang Mai University (No. ET026/2564). All participants who participated in the study provided written informed consent. This study was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
The authors would like to thank all of the caregivers for their participation, as well as the village health volunteers for their assistance.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bradman A, Whitaker D, Quiro L, et al. Pesticides and their metabolites in the homes and urine of farmworker children living in the Salinas Valley, CA. J Expo Anal Environ Epidemiol. 2007;17(4):331–349. doi:10.1038/sj.jes.7500507
2. Lu C, Fenske RA, Simcox NJ, Kalman D. Pesticide exposure of children in an agricultural community: evidence of household proximity to farmland and take home exposure pathways. Environ Res. 2000;84(3):290–302. doi:10.1006/enrs.2000.4076
3. Salvatore AL, Castorina R, Camacho J, et al. Home-based community health worker intervention to reduce pesticide exposures to farmworkers’ children: a randomized-controlled trial. J Expo Sci Environ Epidemiol. 2015;25(6):608–615. doi:10.1038/jes.2015.39
4. Glorennec P, Serrano T, Fravallo M, et al. Determinants of children’s exposure to pyrethroid insecticides in western France. Environ Int. 2017;104:76–82. doi:10.1016/j.envint.2017.04.007
5. Morgan MK. Children’s exposures to pyrethroid insecticides at home: a review of data collected in published exposure measurement studies conducted in the United States. Int J Environ Res Public Health. 2012;9(8):2964–2985. doi:10.3390/ijerph9082964
6. Landrigan PJ, Claudio L, Markowitz SB, et al. Pesticides and inner-city children: exposures, risks, and prevention. Environ Health Perspect. 1999;107(Suppl 3):431–437. doi:10.1289/ehp.99107s3431
7. Saillenfait A-M, Ndiaye D, Sabaté J-P. Pyrethroids: exposure and health effects – an update. Int J Hyg Environ Health. 2015;218(3):281–292. doi:10.1016/j.ijheh.2015.01.002
8. Kunno J, Ong-Artborirak P, Taneepanichskul N, et al. Effect of pyrethroid insecticides exposure in relation to pyrethroid metabolite and GABA concentration of young children, Bangkok Thailand. Hum Ecol Risk Assess. 2019;25:1–14. doi:10.1080/10807039.2019.1615828
9. Kunno J, Ong-Artborirak P, Panicharoen P, et al. Pyrethroid insecticides in households from urban areas: an association of the 3-PBA metabolite and hand wipes. Ann Global Health. 2020;86(1):55. doi:10.5334/aogh.2746
10. Siriwat S, Ong-Artborirak P, Nganchamung T, et al. Health risk assessment of residential exposure to cypermethrin among young children in agricultural communities in northeastern Thailand. Hum Ecol Risk Assess. 2019;25(3):614–623. doi:10.1080/10807039.2018.1539635
11. Siriwat S, Rohitrattana J, Nganchamung T, et al. Exposure of chlorpyrifos in toddlers living in an agricultural area in Sakon Nakhon province, North-East Thailand. J Health Res. 2019;33(2):151–161. doi:10.1108/JHR-07-2018-0057
12. Siriwat S, Ong-Artborirak P, Ponrachom C, et al. Non-carcinogenic health risk from carbamate pesticide exposure of toddlers living in agricultural areas of Thailand. Int J Environ Health Res;2022:1–11. doi:10.1080/09603123.2022.2123456
13. Babina K, Dollard M, Pilotto L, et al. Environmental exposure to organophosphorus and pyrethroid pesticides in South Australian preschool children: a cross sectional study. Environ Int. 2012;48:109–120. doi:10.1016/j.envint.2012.07.007
14. Chen M, Chang CH, Tao L, et al. Residential exposure to pesticide during childhood and childhood cancers: a meta-analysis. Pediatrics. 2015;136(4):719–729. doi:10.1542/peds.2015-0006
15. Chen S, Gu S, Wang Y, et al. Exposure to pyrethroid pesticides and the risk of childhood brain tumors in East China. Environ Pollut. 2016;218:1128–1134. doi:10.1016/j.envpol.2016.08.066
16. Van Maele-Fabry G, Gamet-Payrastre L, Lison D. Residential exposure to pesticides as risk factor for childhood and young adult brain tumors: a systematic review and meta-analysis. Environ Int. 2017;106:69–90. doi:10.1016/j.envint.2017.05.018
17. Viel JF, Rouget F, Warembourg C, et al. Behavioural disorders in 6-year-old children and pyrethroid insecticide exposure: the PELAGIE mother-child cohort. Occup Environ Med. 2017;74(4):275–281. doi:10.1136/oemed-2016-104035
18. Wang N, Huang M, Guo X, et al. Urinary metabolites of organophosphate and pyrethroid pesticides and neurobehavioral effects in Chinese children. Environ Sci Technol. 2016;50(17):9627–9635. doi:10.1021/acs.est.6b01219
19. Wu XM, Bennett DH, Ritz B, et al. Residential insecticide usage in northern California homes with young children. J Expo Sci Environ Epidemiol. 2011;21(4):427–436. doi:10.1038/jes.2010.36
20. Ding G, Bao Y. Revisiting pesticide exposure and children’s health: focus on China. Sci Total Environ. 2014;472:289–295. doi:10.1016/j.scitotenv.2013.11.067
21. Roberts JR, Karr CJ, Paulson JA. Pesticide exposure in children. Pediatrics. 2012;130(6):e1765–e1788. doi:10.1542/peds.2012-2758
22. Deng Y, Dai H, Zeng M, et al. Knowledge and behavior regarding pesticide use: a survey among caregivers of children aged 1–6 years from rural China. Environ Sci Pollut Res Int. 2019;26(22):23037–23043. doi:10.1007/s11356-019-05560-w
23. Fathy EG, Elkarmlawy EM, Mohamed HE, et al. Effect of educational program on prevention of pesticides hazards among children working in agriculture. Am J Nurs Res. 2020;8(2):199–210. doi:10.12691/ajnr-8-2-9
24. Farahat TM, Farahat FM, Michael AA. Behavioral-based educational intervention directed toward Egyptian agricultural families to protect children from pesticide exposure. Int Q Community Health Educ. 2008;28(2):97–108. doi:10.2190/IQ.28.2.b
25. Farahat TM, Farahat FM, Michael AA. Evaluation of an educational intervention for farming families to protect their children from pesticide exposure. East Mediterr Health J. 2009;15(1):47–56. doi:10.26719/2009.15.1.47
26. Quandt SA, Grzywacz JG, Talton JW, et al. Evaluating the effectiveness of a lay health promoter-led, community-based participatory pesticide safety intervention with farmworker families. Health Promot Pract. 2013;14(3):425–432. doi:10.1177/1524839912459652
27. Liebman AK, Juárez PM, Leyva C, Corona A. A pilot program using promotoras de salud to educate farmworker families about the risk from pesticide exposure. J Agromedicine. 2007;12(2):33–43. doi:10.1300/J096v12n02_04
28. Napolitano M, Lasarev M, Beltran M, Philips J, Bryan C, McCauley L. Un lugar seguro para sus ninos: development and evaluation of a pesticide education video. J Immigr Health. 2002;4(1):35–45. doi:10.1023/A:1013059211540
29. Thompson B, Coronado GD, Vigoren EM, et al. Para Niños Saludables: a community intervention trial to reduce organophosphate pesticide exposure in children of farmworkers. Environ Health Perspect. 2008;116(5):687–694. doi:10.1289/ehp.10882
30. Salvatore AL, Chevrier J, Bradman A, et al. A community-based participatory worksite intervention to reduce pesticide exposures to farmworkers and their families. Am J Public Health. 2009;99(Suppl 3):S578–S581. doi:10.2105/AJPH.2008.149146
31. Strong LL, Thompson B, Koepsell TD, et al. Reducing the take-home pathway of pesticide exposure: behavioral outcomes from the para Niños Saludables Study. J Occup Environ Med. 2009;51(8):922–933. doi:10.1097/JOM.0b013e3181ad4995
32. Farizan NH, Sutan R, Mani KK. Effectiveness of “Be SAFE drowning prevention and water safety booklet” intervention for parents and guardians. Iran J Public Health. 2020;49(10):1921–1930. doi:10.18502/ijph.v49i10.4695
33. Wensing M, van der Weijden T, Grol R. Implementing guidelines and innovations in general practice: which interventions are effective? Br J Gen Pract. 1998;48(427):991–997.
34. Davis D, Davis N. Selecting educational interventions for knowledge translation. CMAJ. 2010;182(2):E89–E93. doi:10.1503/cmaj.081241
35. Azmi GN, Mamuroh L, Hendrawati S. Educational media to increase mother’s knowledge of exclusive breastfeeding: a literature review. J Mater Care Reprod Health. 2022;5(3):136–147.
36. Cusack L, Del Mar CB, Chalmers I, Gibson E, Hoffmann TC. Educational interventions to improve people’s understanding of key concepts in assessing the effects of health interventions: a systematic review. Syst Rev. 2018;7(1):68. doi:10.1186/s13643-018-0719-4
37. Hansen MB, Rasmussen IS, Marloth T, et al. A pre-post intervention study: knowledge among parents about child infections and antibiotic use facilitated by maternal and child health nurses. Nurs Open. 2023;10(2):641–648. doi:10.1002/nop2.1330
38. Vijayarani M, Mukesh YP, Balamurugan G. Effectiveness of an information booklet on opinion among caregivers of children with Autism. RJNS. 2022;12(1):1444–1448.
39. Ajzen I. The theory of planned behavior. Organ Behav Hum Decis Process. 1991;50(2):179–211. doi:10.1016/0749-5978(91)90020-T
40. Webb TL, Sheeran P. Does changing behavioral intentions engender behavior change? A meta-analysis of the experimental evidence. Psychol Bull. 2006;132(2):249–268. doi:10.1037/0033-2909.132.2.249
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparison Between Game-Based Learning and Traditional Learning Methods in Traumatic Dental Management Among Dental Interns at KAUFD
Dardeer FM, Areesh RM, Alnafisi AA, Alzain I, Andijani BM, Abudawood SN, Abdullah AM, Ainousa AM, Alulaiyan M
Clinical, Cosmetic and Investigational Dentistry 2025, 17:381-390
Published Date: 25 August 2025
Learning Needs in Heart Failure Care Across Patients, Caregivers, and Healthcare Professionals: A Scoping Review of Asian Studies
Sugiharto F, Trisyani Y, Nuraeni A, Abdullah KL
Patient Preference and Adherence 2026, 20:577045
Published Date: 4 February 2026