Back to Journals » Journal of Asthma and Allergy » Volume 19
Knowledge, Attitudes, and Practices Towards Atopic Dermatitis Among Parents of Children with Atopic Dermatitis: A Cross-Sectional Study
Authors Zheng H, Shen C, Xu D, Ji C, Feng J, Zhou S, Li Y
Received 30 September 2025
Accepted for publication 17 February 2026
Published 2 April 2026 Volume 2026:19 571448
DOI https://doi.org/10.2147/JAA.S571448
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Luis Garcia-Marcos
Huiwen Zheng,1,* Chen Shen,2,* Dan Xu,3 Chai Ji,4 Jia Feng,5 Sha Zhou,1 Yin Li1
1Department of Dermatology, Children’s Hospital, Zhejiang University School of Medicine, National Clinical Research Center for Children and Adolescents, Hangzhou, Zhejiang, People’s Republic of China; 2Information Center, Children’s Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang, People’s Republic of China; 3Department of Pediatric Intensive Care Unit, Children’s Hospital, Zhejiang University School of Medicine, National Clinical Research Center for Child Health, Hangzhou, Zhejiang, People’s Republic of China; 4Department of Children HealthCare, Children’s Hospital, Zhejiang University School of Medicine, National Clinical Research Center for Child Health, Hangzhou, Zhejiang, People’s Republic of China; 5Department of Ophthalmology, Children’s Hospital, Zhejiang University School of Medicine, National Clinical Research Center for Child Health, Hangzhou, Zhejiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Dan Xu, Department of Pediatric Intensive Care Unit, Children’s Hospital, Zhejiang University School of Medicine, National Clinical Research Center for Child Health, Hangzhou, Zhejiang, People’s Republic of China, Tel +86 18268151868, Email [email protected]
Background: Atopic dermatitis (AD) is a common chronic inflammatory skin disease in childhood that imposes substantial physical and psychosocial burdens on children and their families. However, limited evidence is available regarding parents’ knowledge, attitudes, and practices (KAP) toward AD management. This study aimed to investigate the KAP towards AD among parents of children with AD.
Methods: A web-based, cross-sectional study was conducted at a tertiary children’s hospital in China between 17/01/2023 and 30/08/2023. Parents of children diagnosed with AD completed a self-administered questionnaire covering demographics and KAP-related domains. Of 451 valid responses, data were analyzed using descriptive statistics, correlation analysis, and structural equation modeling to examine KAP associations and influencing factors.
Results: Among participants, 364 respondents (80.71%) were women, and 357 (79.16%) of parents had a history of allergic diseases. The mean knowledge, attitude, and practice scores were 12.29± 5.67 (possible range: 0– 24), 30.70± 3.33 (possible range: 9– 45), and 57.02± 8.31 (possible range: 14– 70), respectively. Correlation analysis revealed positive associations between knowledge and practices (r = 0.328, P < 0.001) and between attitudes and practices (r = 0.175, P < 0.001). Structural equation modeling results indicated that higher education level, higher monthly per capita income, and longer time since the child’s diagnosis were positively associated with better knowledge. The number of children in the household was negatively associated with attitudes. Better knowledge, more positive attitudes, higher income, and fewer children in the household were positively associated with more proactive practices.
Conclusion: Parents demonstrated insufficient knowledge, generally positive attitudes, and relatively proactive practices, though many scored below adequacy thresholds. Given the modest strength of the observed associations, these findings should be interpreted cautiously. Efforts may be directed toward enhancing parental education and supporting positive attitudes to potentially improve AD management, while future longitudinal studies are warranted to further clarify causal relationships.
Keywords: atopic dermatitis, parents, knowledge, attitude, practice, cross-sectional study
Corrigendum for this paper has been published.
Introduction
Atopic dermatitis (AD) is a chronic inflammatory skin disease typically beginning in infancy or childhood.1–4 It affects approximately 20% of children, and while the symptoms often improve or disappear as they reach adulthood, some individuals continue to experience symptoms throughout their adult lives.2,5 The primary clinical manifestations of AD include itch, dry skin, and rash.6
AD significantly impacts the quality of life of both patients and caregivers.7 Parents, typically the primary caregivers, face persistent challenges in managing the condition effectively.8 Medication management is a major challenge. Treatment for mild-to-moderate AD typically includes emollients, topical corticosteroids (TCS), and topical calcineurin inhibitors (TCI). Severe or refractory cases may require systemic immunosuppressive agents, phototherapy, or biologics.9–11 TCS are recommended as the first-line treatment for acute flares and for long-term management to prevent relapse.10 However, management of AD can be problematic. For instance, a survey of 300 parents of children with AD in China revealed that 96% harbored concerns about TCS side effects, leading 42% to withhold TCS during AD recurrences.12
The Knowledge, Attitudes, and Practices (KAP) framework posits that knowledge forms the foundation for behavior change, while attitudes and beliefs act as the driving forces behind such changes.13 According to this theory, the evolution of human behavior can be delineated into three phases: acquiring knowledge, forming attitudes and beliefs, and ultimately developing practices or behaviors.14 However, cognitive changes resulting from knowledge acquisition do not necessarily translate into behavior changes. Instead, they should first alter attitudes, which in turn can modify behavior through this new understanding.15 Although some KAP-related studies have been conducted in China, including the recent development of the ADISKAP 1.0 scale,16 research focusing on parents’ knowledge, attitudes, and practices regarding AD remains limited. Recent AD-specific KAP studies have reported persistent gaps in parental knowledge and suboptimal disease management behaviors. A recent national survey in China demonstrated that both adult patients with AD and parents of pediatric AD patients showed inadequate knowledge and inconsistent treatment practices, which were associated with poorer disease control.17 In addition, a cross-sectional study conducted in Thailand revealed that parental misconceptions regarding skincare routines and topical medication use were common and significantly influenced daily management behaviors in children with AD.18 Furthermore, earlier evidence from Europe also indicated that higher parental knowledge and positive attitudes were associated with better treatment adherence and disease outcomes in pediatric AD populations.19 ADISKAP 1.0 scale was designed to assess parental KAP toward AD and infant skincare, but it targets only parents of children under 2 years old. Given that AD can affect children across all age groups, there is a clear gap in understanding parental KAP concerning AD in older children. Consequently, this study aimed to explore the KAP of parents of children with AD.
Materials and Methods
Study Design and Participants
This observational cross-sectional study aimed to assess the knowledge, attitudes, and practices (KAP) of parents of children with AD and enrolled parents of outpatient children with AD at Children’s Hospital Affiliated with Zhejiang University School of Medicine between 17/01/2023 and 30/08/2023. The outpatient children met diagnostic criteria based on Hanifin and Rajka (1980),20 and informed consent was provided by their legal guardians. Parents were eligible for inclusion if they were the primary caregivers of children diagnosed with AD, were able to read and complete the online questionnaire independently, and provided informed consent. Parents with cognitive impairment or incomplete questionnaire responses were excluded from the final analysis. This study was approved by the Ethic Committee of Children’s Hospital of Zhejiang University School of Medicine (2022-IRB-160), and all participants provided written informed consent.
Questionnaire
The questionnaire, comprising four dimensions, was developed in accordance with the “Guideline for primary care of atopic dermatitis (2022)” and “Expert consensus for management of itch in atopic dermatitis”.20,21 While the ADISKAP 1.0 scale has been validated for measuring parental KAP regarding AD and infant skincare in Beijing,16 our questionnaire is designed to target parents of children with AD across all pediatric age groups. The initial draft received feedback from 3 experts in the field, each with over 20 years of experience, leading to revisions, that involved the removal of redundant or similar questions and refining ambiguous statements. Then a small-scale distribution (57 copies) was conducted for reliability testing, yielding a Cronbach’s α coefficient of 0.869, demonstrating high internal consistency.
The final questionnaire encompassed the following dimensions: 1) Demographic Information of participants, which included parent’s gender, parent’s age, child’s gender, child’s age, residence, parent’s education, employment status, monthly income per capita, history of allergic diseases in parents, parent’s smoking status, number of children, mother’s age at the birth of the affected child, pet keeping, and time since the child was diagnosed with AD. 2) Knowledge Dimension, with 12 questions scored as follows: 2 points for “very familiar”, 1 point for “heard of”, and 0 points for “uncertain”; 3) Attitude Dimension, comprising 9 questions rated on a five-point Likert scale from “strongly agree” (5 points) to “strongly disagree” (1 point); and 4) Practice Dimension, with 14 questions scored on a five-point Likert scale from “always” (5 points) to “never” (1 point). Higher scores indicate better knowledge, more positive attitudes, and more proactive practices. Attaining scores above 70% of the maximum in each section indicated adequate knowledge, positive attitude, and proactive practice.22
Questionnaire Distribution and Quality Control
An online version of the questionnaire was created using the WeChat-based Questionnaire Star mini-program, with QR codes generated for data collection via WeChat. Participants accessed and completed the questionnaire by scanning the QR code provided to them. Participants were recruited through multiple channels, including posters displayed in the dermatology clinic, direct invitation by attending physicians or nurses, and information shared via the hospital’s WeChat platform. All participation was voluntary.
To ensure quality and completeness, all questions were mandatory. The research team reviewed each questionnaire for completeness, internal coherence, and validity. Questionnaires with abnormal data were considered invalid. Although the data collection period exceeded three months, the questionnaire content, recruitment procedures, and data collection methods were standardized throughout the study period to minimize potential temporal bias.
Sample Size Calculation
A single population proportion formula, 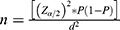 , was used to calculate the sample size. Since there were no KAP studies on AD in the Chinese population, the sample size for this study was calculated based on an expected proportion of participants’ understanding of AD at 50%, with a confidence level of 95% and a margin of error of 5%, requiring a sample size of 384 individuals. In the present study, a total of 451 valid questionnaires were collected and included in the final analysis, exceeding the minimum required sample size.
, was used to calculate the sample size. Since there were no KAP studies on AD in the Chinese population, the sample size for this study was calculated based on an expected proportion of participants’ understanding of AD at 50%, with a confidence level of 95% and a margin of error of 5%, requiring a sample size of 384 individuals. In the present study, a total of 451 valid questionnaires were collected and included in the final analysis, exceeding the minimum required sample size.
Statistical Analysis
Statistical analysis was conducted using Stata 17.0 (Stata Corporation, College Station, TX, USA). Continuous variables were reported as mean ± standard deviation (SD), with intergroup comparisons performed via t-tests or analysis of variance (ANOVA). Categorical variables were described as n (%). Pearson correlation analysis was used to evaluate correlations among knowledge, attitude, and practice scores. Variables with P < 0.05 in the univariate logistic regression analysis were selected for the multivariate regression analysis. Multivariate logistic regression was applied to analyze the independent factors associated with KAP, with scores exceeding 75% of the total score defined as the cutoff value.23 Structural equation modeling (SEM) was used to test the following hypotheses: 1) the duration of diagnosis, educational level, and per capita income directly influence knowledge. These hypotheses were formulated a priori based on prior literature and the conceptual framework of the KAP model. For example, longer disease duration has been associated with greater parental knowledge due to increased medical exposure over time.19 Similarly, higher education and income levels are frequently linked to better health knowledge and behaviors. Factor analysis was not conducted prior to SEM, as the model was designed to test predefined theoretical relationships rather than to explore latent constructs. 2) educational level and number of children directly influence attitude; 3) per capita income, educational level, and number of children directly influence practice; 4) knowledge has a direct effect on attitude and practice; and 5) attitude directly influences practice. Besides, given that AD typically begins in early childhood, with 60% of cases manifesting before the age of two,21 our study conducted a subgroup analysis specifically focusing on parents of children under two years old. All statistical tests were two-tailed, with significance set at P < 0.05.
Results
Characteristics of the Participants
After collecting the questionnaires, the following cases were excluded: 39 cases where the parents’ ages were unreported or under 18 years old and 30 cases of abnormal answer logic. This left 451 valid questionnaires. Among them, 364 respondents (80.71%) were women with a mean age of 32.76±4.93 years and mean childbirth age of 29.58±4.06 years. Among the children, 243 (53.88%) boys were diagnosed with AD, with a mean age of 2.90±3.41 years, and an average age at diagnosis of AD of 18.23±28.42 months. Meanwhile, 224 (49.67%) of parents had a history of allergic rhinitis, and 131 (29.05%) of parents were current smokers.
Knowledge, Attitudes, and Practices
The mean knowledge, attitude, and practice scores were 12.29±5.67 (possible range: 0–24), 30.70±3.33 (possible range: 9–45), and 57.02±8.31 (possible range: 14–70), respectively. Knowledge scores varied by participants’ gender (P = 0.016), residence (P = 0.017), education (P < 0.001), employment status (P = 0.004), and average monthly per capita income (P < 0.001). Attitude scores varied by participants’ education (P = 0.029), smoking status (P = 0.040), and number of children in the household (P = 0.011). Practice scores varied by participants’ gender (P = 0.006), child’s gender (P = 0.013), education (P = 0.003), average monthly per capita income (P < 0.001), and number of children in the household (P < 0.001) (Table 1).
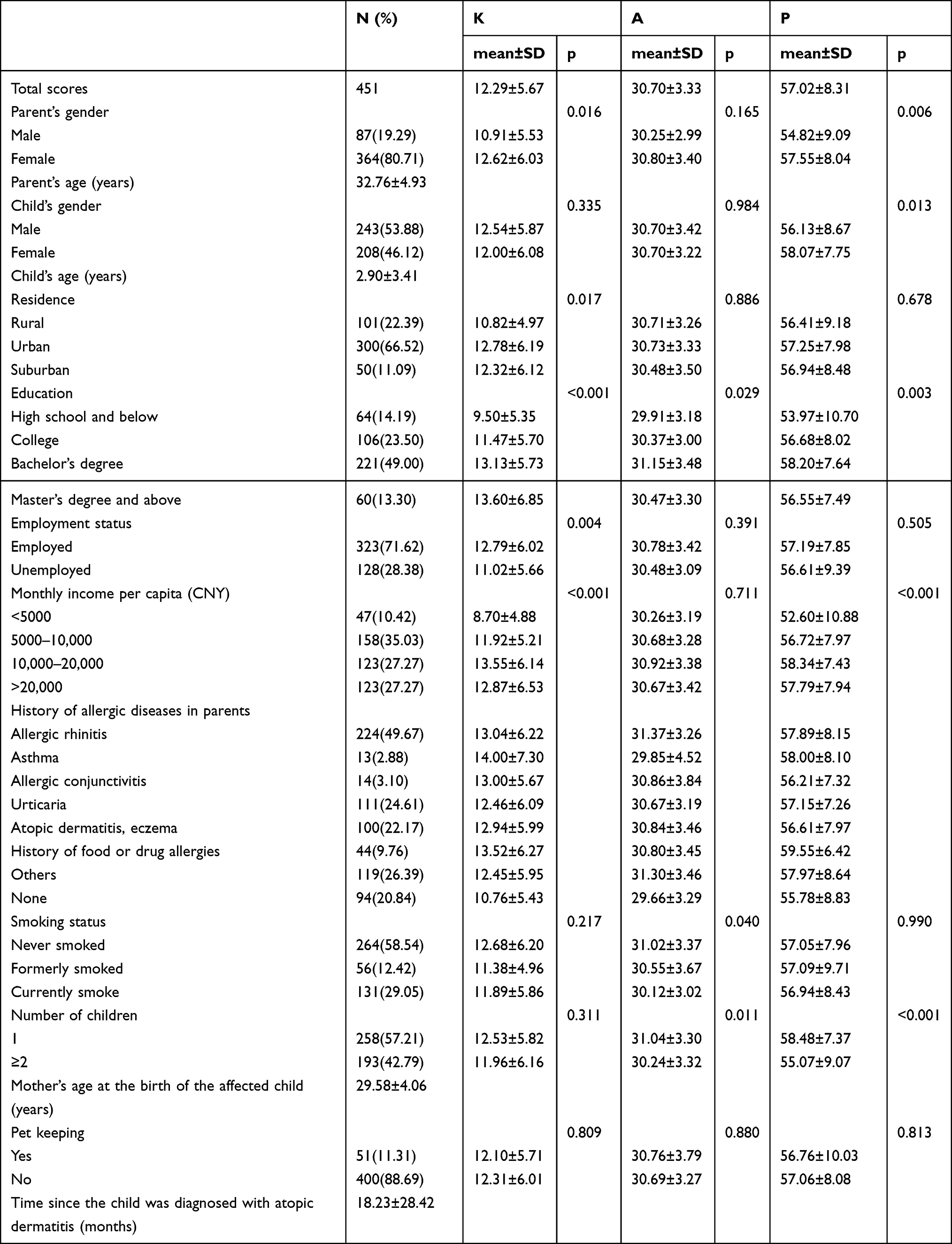 |
Table 1 Basic Characteristics and KAP Scores |
The distribution of knowledge dimensions showed that the three questions with the highest number of participants choosing the “Uncertain” option were “Negative emotions such as stress, anxiety, and depression may contribute to the exacerbation of AD symptoms.” (K4) with 49.00%, “Topical corticosteroids are the first-line drugs for treating AD in China.” (K10) with 35.92%, and “When initiating treatment with topical corticosteroids, formulations with sufficient potency should be chosen to rapidly control inflammation within a few days; after inflammation is controlled, transition to moderate to weak potency corticosteroids or other medications should be gradual.” (K12) with 35.25% (Table 2).
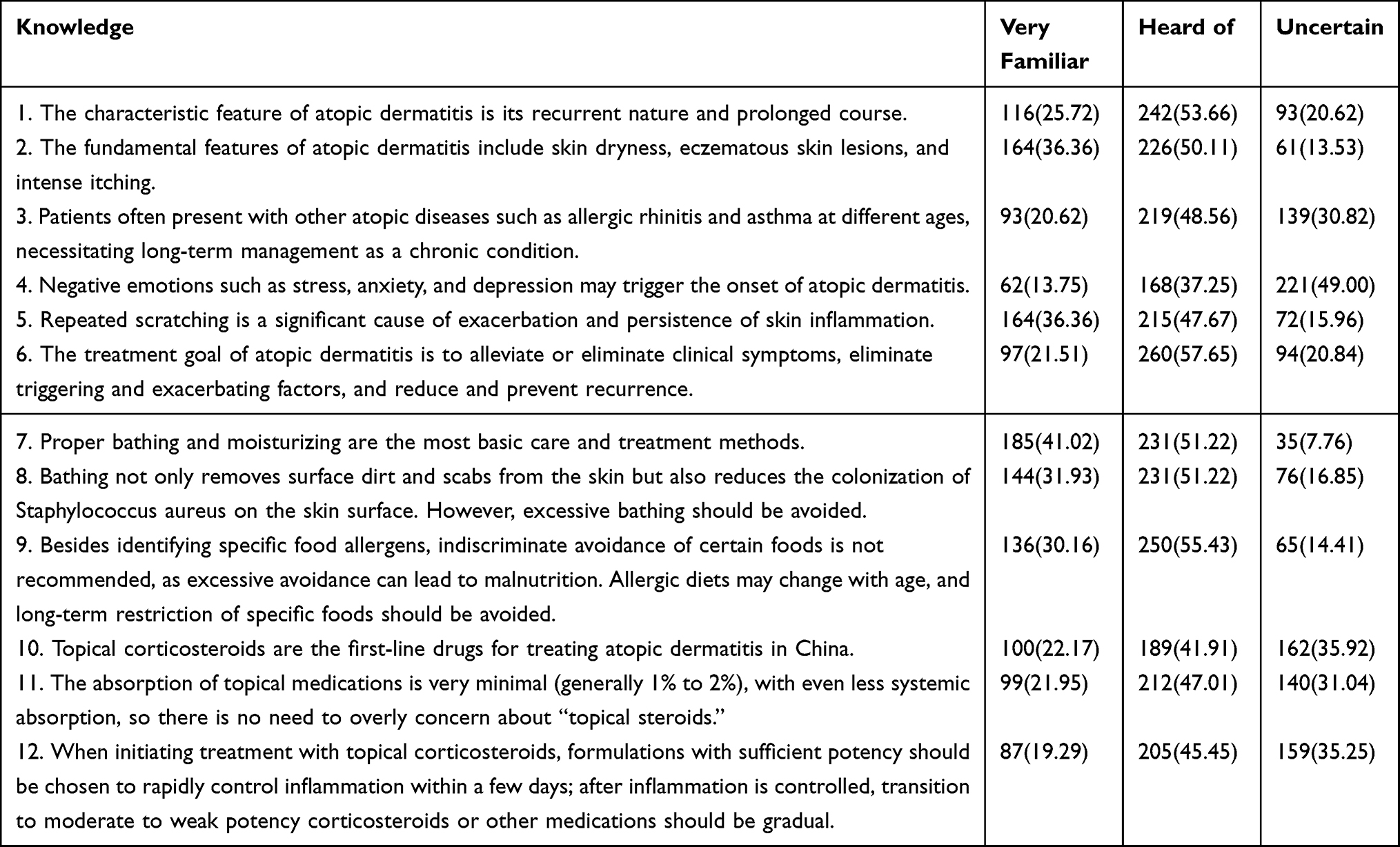 |
Table 2 Distribution of Knowledge |
Regarding relevant attitudes, 49.89% strongly agreed that itching and rash significantly disrupt the child’s social life, education, and daily activities (A2), and 35.48% strongly agreed that, although AD is not contagious, discrimination from others leads to social anxiety and concerns about appearance (A3). Another 21.51% strongly agreed that their children had a higher incidence of food allergies than the general child population and thus strict avoidance should be continued (A6) (Table 3).
 |
Table 3 Distribution of Attitudes |
In the practice section, 44.35% consistently limited bathing time to 5–10 minutes (P1), 60.53% consistently applied skincare products immediately after bathing (P2), 62.97% consistently chose soft, cotton, loose-fitting clothing (P3), and 62.53% consistently followed the doctor’s medication prescription (P8) (Table 4).
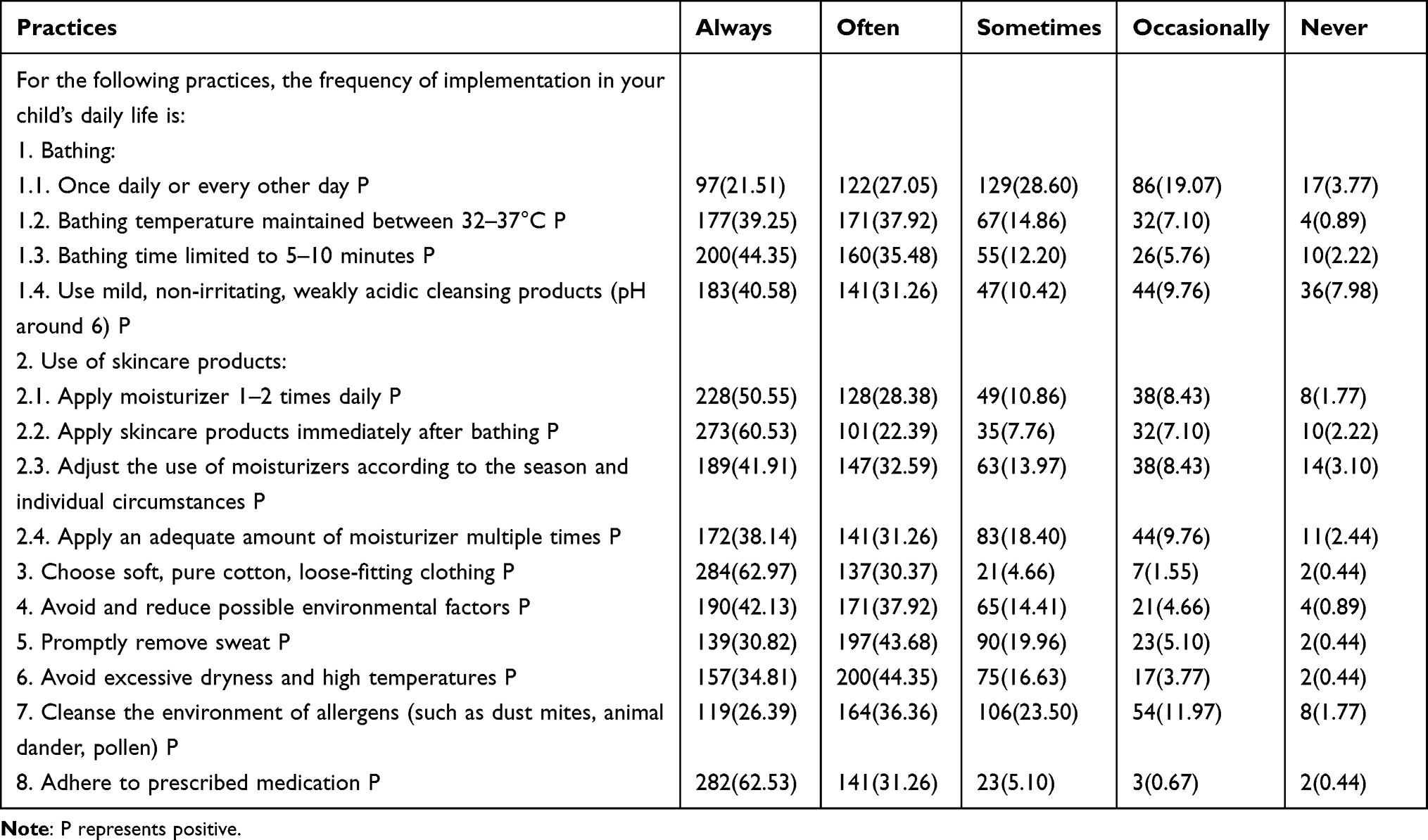 |
Table 4 Distribution of Practices |
Correlation and Multivariable Analysis
Correlation analysis revealed significant correlations between knowledge and practices (r = 0.328, P < 0.001) and between attitudes and practices (r = 0.175, P < 0.001), but no significant correlation between knowledge and attitudes (r = 0.056, P = 0.235) (Tables S1-S4).
Multivariate logistic regression showed that an average monthly per capita income of 10,000–20,000 yuan (OR = 4.739, 95% CI: [1.015, 22.124], P = 0.048) and time since the child’s AD diagnosis (OR = 1.017, 95% CI: [1.006, 1.028], P = 0.002) were independently associated with good knowledge (Table S1). Additionally, knowledge (OR = 1.047, 95% CI: [1.006, 1.089], P = 0.024) and current smoking (OR = 0.488, 95% CI: [0.268, 0.889], P = 0.019) were independently associated with attitude (Table S2). Furthermore, knowledge (OR = 1.127, 95% CI: [1.074, 1.181], P < 0.001), having a male child (OR = 0.528, 95% CI: [0.323, 0.863], P = 0.011), and the child’s age (OR = 0.841, 95% CI: [0.774, 0.914], P < 0.001) were independently associated with practices (Table S3).
SEM Analysis
SEM results indicated that education (β = 0.820, P < 0.001), monthly per capita income (β = 0.596, P = 0.009), and the time since the child’s diagnosis (β = 0.065, P < 0.001) directly affected knowledge. The number of children in the household directly impacted attitudes (β = −0.711, P = 0.025). Knowledge (β = −0.711, P < 0.001), attitudes (β = 0.338, P = 0.002), monthly per capita income (β = 0.735, P = 0.022), and number of children in the household (β = −2.857, P < 0.001) directly influenced practice (Table S5 and Figure 1). The SEM showed favorable model fit indices, indicating a well-fitting model (Table S6).
 |
Figure 1 Structural Equation Modeling. |
Subgroup Analysis
Subgroup analysis of participants with children under two years old showed that the knowledge score (OR = 1.136, 95% CI: [1.055, 1.224], P = 0.001) and having a male child (OR = 0.413, 95% CI: [0.196, 0.872], P = 0.020) were independently associated with practice, while for knowledge and attitude scores, no factors were independently associated with them (Tables S7–S9). SEM results revealed that education (β = 0.599, P = 0.043) and the time since the child’s diagnosis (β = 0.203, P < 0.001) directly influenced knowledge. The number of children in the household directly affected attitudes (β = −1.035, P = 0.016). Knowledge (β = 0.433, P < 0.001) and attitudes (β = 0.282, P = 0.032) directly influenced practice (Table S10 and Figure S1). The SEM showed favorable model fit indices, indicating a well-fitting model (Table S11).
Discussion
Parents of children with AD exhibited insufficient knowledge, generally positive attitudes, and relatively proactive practices, although many did not meet the predefined threshold for adequacy. It should be noted that the observed associations were modest in magnitude and reflect statistical correlations rather than causal relationships. Therefore, while our findings suggest a potential need for targeted educational interventions aimed at improving parental knowledge and fostering positive attitudes regarding AD in children, longitudinal studies are warranted to further validate these relationships and assess their long-term impact on parental behavior and disease management outcomes.
Compared to the ADISKAP 1.0 scale developed in Beijing,16 our study reveals both similarities and important differences in parental KAP patterns. Both studies identified significant knowledge gaps among parents, particularly regarding topical corticosteroid use, with our study showing 35.92% of parents uncertain about corticosteroids as first-line treatment, which aligns with the corticosteroid phobia documented in ADISKAP 1.0. However, our findings extend beyond the infant-focused scope of ADISKAP 1.0 by demonstrating that knowledge and practice patterns vary significantly with child age and time since diagnosis. Our study found that parents with children under 2 years showed different KAP patterns compared to those with older children, suggesting that the developmental stage-specific needs identified in ADISKAP 1.0 continue to evolve as children grow. Furthermore, our regional analysis revealed urban-rural disparities in knowledge scores that were not addressed in the ADISKAP 1.0 study, highlighting the importance of regional context in understanding parental KAP patterns across different healthcare settings in China.
Our findings underscore gender-based discrepancies, with females exhibiting better knowledge and practice scores compared to males. These findings are consistent with previous AD-focused studies conducted in different regions. Reljić et al reported that mothers of children with AD generally demonstrated higher disease-related knowledge and greater engagement in treatment-related decision-making compared with fathers, which was associated with improved disease management outcomes.19 Similarly, Nie et al observed that female caregivers exhibited significantly higher KAP scores in a Chinese multicenter survey, suggesting that gender-related caregiving roles may influence information acquisition and health behaviors in pediatric AD management.17 This observation aligns with studies suggesting that mothers, who typically assume the role of primary caregivers, acquire more health-related information and engage more actively in managing the health conditions of their children.24,25 This gender difference underscores the need for targeted educational efforts that cater to the specific informational needs of fathers, who may be less involved in daily management but equally essential in a supportive role.
Specifically, our findings underscored a direct relationship between parental education, income, and KAP, which parallels observations from a Serbian study that indicated better knowledge and attitudes among more educated and employed parents.19 Higher education often equips parents with better information-seeking skills and critical thinking, allowing them to interpret medical advice more accurately. Urban residents scored higher in knowledge than rural residents, likely due to better access to healthcare resources in urban areas. This urban-rural disparity has been recognized in the literature, emphasizing the need for community-based education and support programs tailored to rural populations.26 Employed parents scored higher in knowledge compared to their unemployed counterparts, possibly due to increased exposure to health information at workplaces or through healthcare benefits provided by employers. Furthermore, employment might also correlate with income, which directly influences access to healthcare.
Interestingly, our study also noted a significant impact of the child’s age and the time since diagnosis on parental practices. As children grow and develop, their care needs evolve, requiring adjustments in management strategies. Over time, parents also gain more experience and knowledge, which enhances their ability to effectively manage the condition. This finding underscores the importance of continuous education for parents throughout the child’s growth and the evolution of AD.27 Besides, participants with only one child scored higher in attitudes and practices, which could be because they can dedicate more time and resources to one child’s care. Conversely, families with multiple children might face challenges dividing attention and finances among all children.28 Besides, relationships between knowledge-practice and attitude-practice were revealed, which aligns with prior findings that a well-informed and positive approach often translates into proactive management.19
Our subgroup analysis revealed that the influence of education on knowledge scores appears to be weaker in the subgroup of parents with children under two years old. This finding is inconsistent with the literature, indicating that parents of younger children are often more engaged in seeking information immediately following diagnosis.29 Additionally, the role of attitudes in influencing practices is observed to be lesser in the subgroup. This could be due to the practical challenges and stress associated with caring for younger children, where immediate concerns and daily demands may override the influence of attitudes on practice.30 Interestingly, the negative impact of having more children in the household on practices is less pronounced in the subgroup. This might be due to the concentrated care and attention often required by infants, which necessitates more active management practices from parents. Additionally, having more children might lead to a more experienced approach to childcare among parents, enhancing their ability to manage the condition more effectively through accumulated knowledge and practical skills.31,32 Nevertheless, these findings suggest that targeted educational strategies focusing on daily skincare routines, treatment adherence, and psychosocial support may still be beneficial for improving parental engagement in AD management.
Overall, the findings across the knowledge, attitude, and practice dimensions highlight several important gaps and opportunities for intervention. Although many respondents were familiar with the characteristic features and chronic course of AD, awareness of psychological triggers, particularly the role of negative emotions, was relatively limited. Educational programs should therefore emphasize the multifactorial nature of AD and integrate discussions of stress management and mental health support into routine care.33 Attitudinally, while most caregivers expressed trust in physicians and recognized the importance of skin barrier protection, concerns about treatment modalities—especially corticosteroid use—and the burden of daily care routines persisted. Such misconceptions, including corticophobia reported in previous studies,34 underscore the need for open communication, personalized education, and shared decision-making to improve confidence and adherence.35 In practice, although key behaviors such as maintaining skin hydration were commonly adopted, inconsistencies remained in bathing routines and environmental control. Targeted, practical education and the use of digital tools to support daily management and adherence monitoring may help reinforce recommended behaviors and promote sustained improvements in AD care.36
Several limitations should be acknowledged. Firstly, the study’s reliance on a web-based self-administered questionnaire may introduce selection bias, as it could exclude participants without internet access or those less inclined to participate in online surveys. Secondly, the cross-sectional design limits the ability to establish causal relationships between variables, merely capturing a snapshot of the participants’ KAP at a single point in time. The data collection period spanned seven months, which is longer than the typical 1–3 month period for cross-sectional studies. This extended timeframe raises the possibility of temporal bias, as seasonal variations, public health campaigns, or other external events during this period could have influenced parental KAP, potentially distorting the data and affecting the consistency of the “snapshot” in time. Although we standardized procedures to minimize this risk, its potential influence cannot be entirely excluded. Thirdly, the study was conducted in a single tertiary hospital, and the focus on a specific hospital setting may restrict the generalizability of findings to broader populations, as healthcare access, socioeconomic status, and cultural factors may vary across different regions or healthcare settings. Lastly, while the knowledge dimension in this study was measured using a 3-point Likert scale, which reflects participants’ self-perceived understanding, this method may not fully capture objective knowledge. Self-assessment could lead to overestimation or underestimation of actual knowledge levels. Nevertheless, in our context, perceived knowledge remains valuable, as it may influence attitudes and behavioral decisions. Moreover, certain questionnaire items were designed based on Chinese clinical guidelines, which may differ from international recommendations. These differences in clinical practice may influence the interpretation of some items, and should be considered when applying the findings to broader or non-domestic contexts. In addition, certain questionnaire items have addressed topics that may be perceived as controversial, such as corticosteroid use and the role of psychological stress in disease exacerbation. While these items were included to reflect real-world misconceptions and beliefs, their interpretation may vary among respondents, which could influence the accuracy and consistency of the results. In addition, as the survey was conducted in a tertiary hospital setting and relied on voluntary participation, parents who were more health-conscious, better educated, or had greater access to digital platforms may have been more likely to respond. This potential selection bias should be considered when interpreting the generalizability of the findings to the overall population of caregivers for children with AD.
Conclusions
In conclusion, parents of children with AD exhibited insufficient knowledge, generally positive attitudes, and relatively proactive practices regarding AD. Given the modest strength of the observed correlations, these findings should be interpreted as associative rather than causal. Therefore, efforts may be directed toward enhancing parental education and supporting positive attitudes to potentially improve disease management, while future longitudinal studies are warranted to further clarify the causal relationships between knowledge, attitudes, and practices.
Abbreviations
KAP, Knowledge, attitudes, and practices; AD, Atopic dermatitis; TCS, Topical corticosteroids; TCI, Topical calcineurin inhibitors; SD, Standard deviation; ANOVA, Analysis of variance; SEM, Structural equation modeling.
Data Sharing Statement
All data generated or analysed during this study are included in this published article.
Ethics Approval and Informed Consent
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Ethic Committee of Children’s Hospital of Zhejiang University School of Medicine (2022-IRB-160). All participants were informed about the study protocol and provided written informed consent to participate in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests.
References
1. Sarama R, Matharu PK, Abduldaiem Y, Corrêa MP, Gil CD, Greco KV. In vitro disease models for understanding psoriasis and atopic dermatitis. Front Bioeng Biotechnol. 2022;10:803218. doi:10.3389/fbioe.2022.803218
2. Schmidt SAJ, Mailhac A, Darvalics B, et al. Association between atopic dermatitis and educational attainment in Denmark. JAMA Dermatol. 2021;157(6):1–12. doi:10.1001/jamadermatol.2021.0009
3. Cooper KD. Atopic dermatitis: recent trends in pathogenesis and therapy. J Invest Dermatol. 1994;102(1):128–137. doi:10.1111/1523-1747.ep12371746
4. Leung DY, Bieber T. Atopic dermatitis. Lancet. 2003;361(9352):151–160. doi:10.1016/S0140-6736(03)12193-9
5. Simpson EL, Guttman-Yassky E, Margolis DJ, et al. Association of inadequately controlled disease and disease severity with patient-reported disease burden in adults with atopic dermatitis. JAMA Dermatol. 2018;154(8):903–912. doi:10.1001/jamadermatol.2018.1572
6. Drucker AM, Wang AR, Li WQ, Sevetson E, Block JK, Qureshi AA. The burden of atopic dermatitis: summary of a report for the National Eczema Association. J Invest Dermatol. 2017;137(1):26–30. doi:10.1016/j.jid.2016.07.012
7. Feng LJ, Chen AW, Luo XY, Wang H. Increased attention deficit/hyperactivity and oppositional defiance symptoms of 6–12 years old Chinese children with atopic dermatitis. Medicine. 2020;99(25):e20801. doi:10.1097/MD.0000000000020801
8. Epifanio MS, Genna V, De Luca C, Roccella M, La Grutta S. Paternal and maternal transition to parenthood: the risk of postpartum depression and parenting stress. Pediatr Rep. 2015;7(2):5872. doi:10.4081/pr.2015.5872
9. Patrizi A, Raone B, Ravaioli GM. Management of atopic dermatitis: safety and efficacy of phototherapy. Clin Cosmet Invest Dermatol. 2015;8:511–520. doi:10.2147/CCID.S87987
10. Wollenberg A, Barbarot S, Bieber T, et al. Consensus-based European guidelines for treatment of atopic eczema (atopic dermatitis) in adults and children: part I. J Eur Acad Dermatol Venereol. 2018;32(5):657–682. doi:10.1111/jdv.14891
11. Wollenberg A, Barbarot S, Bieber T, et al. Consensus-based European guidelines for treatment of atopic eczema (atopic dermatitis) in adults and children: part II. J Eur Acad Dermatol Venereol. 2018;32(6):850–878. doi:10.1111/jdv.14888
12. Li Y, Han T, Li W, Li Y, Guo X, Zheng L. Awareness of and phobias about topical corticosteroids in parents of infants with eczema in Hangzhou, China. Pediatr Dermatol. 2018;35(4):463–467. doi:10.1111/pde.13527
13. Gao L, Su S, Du N, et al. Medical and non-medical students’ knowledge, attitude and willingness towards the COVID-19 vaccine in China: a cross-sectional online survey. Hum Vaccin Immunother. 2022;18(5):2073757. doi:10.1080/21645515.2022.2073757
14. Twinamasiko N, Olum R, Gwokyalya AM, Nakityo I, Wasswa E, Sserunjogi E. Assessing knowledge, attitudes and practices towards COVID-19 public health preventive measures among patients at Mulago National Referral Hospital. Risk Manag Healthc Policy. 2021;14:221–230. doi:10.2147/RMHP.S287379
15. Wang J, Chen L, Yu M, He J. Impact of knowledge, attitude, and practice (KAP)-based rehabilitation education on the KAP of patients with intervertebral disc herniation. Ann Palliat Med. 2020;9(2):388–393. doi:10.21037/apm.2020.03.01
16. Sun X, Zhao M, Wu Q, et al. Development and validation of the atopic dermatitis and infant skincare knowledge, attitude, and practice (ADISKAP 1.0) scale. Pediatr Investig. 2023;7(3):153–162. doi:10.1002/ped4.12374
17. Nie Z, Fan P, Zhou Y, Han S. Knowledge, attitudes, and practices in adult patients and parents of pediatric atopic dermatitis patients: a cross-sectional study. Front Public Health. 2024;12:1460044. doi:10.3389/fpubh.2024.1460044
18. Nummak P, Techasatian L, Uppala R, Sitthikarnkha P, Saengnipanthkul S, Sirikarn P. Parental attitudes and practices regarding atopic dermatitis: a cross-sectional study among a Thai Population. Children. 2024;11(7):870. doi:10.3390/children11070870
19. Reljić V, Gazibara T, Nikolić M, Zarić M, Maksimović N. Parental knowledge, attitude, and behavior toward children with atopic dermatitis. Int J Dermatol. 2017;56(3):314–323. doi:10.1111/ijd.13529
20. Chinese Medical Association, Journal of Chinese Medical Association, Chinese Society of Dermatology and venereology, Chinese Medical Association Branch of General Practice, Editorial Board of Chinese Journal of General Practice-Chinese Medical Association, group. Davdbdatgtpe. Guideline for primary care of atopic dermatitis (2022). Chin J General Pract. 2022;21:609–619.
21. Committee on Allergic Diseases, China Dermatologist Association, Atopic Dermatitis Research Center, Chinese Society of Dermatology, Healthcare DBoCIEaPAfMa. Expert consensus for management of itch in atopic dermatitis. Chin Jl of Dermatology. 2021;54:319–396.
22. Lee F, Suryohusodo AA. Knowledge, attitude, and practice assessment toward COVID-19 among communities in East Nusa Tenggara, Indonesia: a cross-sectional study. Front Public Health. 2022;10:957630. doi:10.3389/fpubh.2022.957630
23. Malaeb D, Sallam M, Younes S, et al. Knowledge, attitude, and practice in a sample of the Lebanese Population Regarding Cholera. Int J Environ Res Public Health. 2022;19(23):16243. doi:10.3390/ijerph192316243
24. Shrestha S, Arora S, Hunter A, Debesay J. Changing dynamics of caregiving: a meta-ethnography study of informal caregivers’ experiences with older immigrant family members in Europe. BMC Health Serv Res. 2023;23(1):43. doi:10.1186/s12913-023-09023-4
25. Pourghaznein T, Heydari A, Manzari Z, MousaviBazaz S. Designing a supportive program based on the real needs of mothers with children undergoing hemodialysis: a qualitative study. Iran J Nurs Midwifery Res. 2022;27(1):60–66. doi:10.4103/ijnmr.IJNMR_430_20
26. Wang S, Lai J, Wu R, et al. Grocott methenamine silver staining is the optimal approach to histological diagnosis of pulmonary cryptococcosis. Front Microbiol. 2022;13:885511. doi:10.3389/fmicb.2022.885511
27. Kim SS, Kim NK, Seo SR. Cynanchi atrati and its phenolic constituent sinapic acid target regulator of calcineurin 1 (RCAN1) to control skin inflammation. Antioxidants. 2022;11(2):205.
28. Thomas JR, Hanson D, Chinnan-Pothen A, Freaney C, Silverman J. Packed school lunch food consumption: a childhood plate waste nutrient analysis. Nutrients. 2023;15(5):1116. doi:10.3390/nu15051116
29. Song H. Longitudinal investigations of autoregressive cross-lagged path models among internet use, executive function problems, and maternal control in young Korean children. Front Psychiatry. 2022;13:846995. doi:10.3389/fpsyt.2022.846995
30. Bayer DK. A practical approach to caring for atopic dermatitis in children. Curr Opin Pediatr. 2023;35(6):686–691. doi:10.1097/MOP.0000000000001293
31. Neri I, Galli E, Baiardini I, et al. Implications of atopic dermatitis on the quality of life of 6–11 years old children and caregivers (PEDI-BURDEN). J Asthma Allergy. 2023;16:383–396. doi:10.2147/JAA.S404350
32. Sandhu JK, Salame N, Ehsani-Chimeh N, Armstrong AW. Economic burden of cutaneous infections in children and adults with atopic dermatitis. Pediatr Dermatol. 2019;36(3):303–310. doi:10.1111/pde.13828
33. Courtney A, Su JC. The psychology of atopic dermatitis. J Clin Med. 2024;13(6):1602. doi:10.3390/jcm13061602
34. Kotrulja L, Milavić T, Bulić SO, et al. Importance of educational intervention and parental knowledge on atopic dermatitis in children. Acta Clin Croat. 2016;55(1):29–34. doi:10.20471/acc.2016.55.01.5
35. Roustán G, Loro M, Rosell Á, et al. Development of a patient journey map for improving patient experience and quality of atopic dermatitis care. Dermatol Ther. 2024;14(2):505–519. doi:10.1007/s13555-024-01100-8
36. Zvulunov A, Lenevich S, Migacheva N. A mobile health app for facilitating disease management in children with atopic dermatitis: feasibility and impact study. JMIR Dermatol. 2023;6:e49278. doi:10.2196/49278
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Knowledge, Attitudes and Practices Towards Psoriasis Among Patients and Their Family Members
Zhang X, Du H, Liu X, Liu L, Zhang T
Clinical, Cosmetic and Investigational Dermatology 2024, 17:769-782
Published Date: 3 April 2024
Knowledge, Attitudes and Practices Toward Physical Literacy Among the College Students During COVID-19 School Closure
Ma C, Yue M, Zhu X
Journal of Multidisciplinary Healthcare 2024, 17:1629-1640
Published Date: 15 April 2024
Knowledge, Attitude and Practice of Radiologists Regarding Artificial Intelligence in Medical Imaging
Huang W, Li Y, Bao Z, Ye J, Xia W, Lv Y, Lu J, Wang C, Zhu X
Journal of Multidisciplinary Healthcare 2024, 17:3109-3119
Published Date: 4 July 2024
Knowledge, Attitude, and Practice Toward Varicocele in Patients with Varicoceles: A Cross-Sectional Study in Chinese Patients
Gong P, Shen J, Yang Y, Xue D, Lu H, Zhuang Q, Wang X, Tian Z, Chen Y, Chen C, Cao Y
International Journal of General Medicine 2024, 17:3423-3432
Published Date: 7 August 2024
Knowledge, Attitude, and Practice Towards Rehabilitation in Patients with Breast Cancer: A Cross-Sectional Study
Zhou Y, Lu Q, Yu X
Journal of Multidisciplinary Healthcare 2025, 18:1483-1492
Published Date: 12 March 2025