Back to Journals » International Journal of General Medicine » Volume 19
Knowledge, Attitudes, and Practices Regarding Venous Thromboembolism Among Elderly Chinese Patients: A Cross-Sectional Study
Authors Jin J, Zhang X, Zhao Z, Li J, Hu T, Yuan M, Ke Y, Wang B
Received 10 November 2025
Accepted for publication 16 January 2026
Published 29 January 2026 Volume 2026:19 580403
DOI https://doi.org/10.2147/IJGM.S580403
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Satish Nair
Jun Jin,* Xingliang Zhang,* Zhe Zhao, Jie Li, Tingjun Hu, Meixia Yuan, Yingying Ke, Beiyun Wang
Department of Gerontology, Shanghai Sixth People’s Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai, 200233, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Beiyun Wang, Email [email protected]
Purpose: Venous thromboembolism (VTE) poses a significant health risk for the elderly. This study aims to evaluate the knowledge, attitudes, and practices (KAP) concerning VTE among elderly individuals.
Patients and Methods: This cross-sectional study was conducted between September and October 2024 among elderly inpatients and outpatients at the Department of Gerontology, Shanghai Sixth People’s Hospital in China, involving 540 participants. Demographic characteristics and KAP scores were collected using a self-designed questionnaire. Confirmatory factor analysis demonstrated acceptable construct validity, and a cutoff of 70% of the maximum score was applied to define adequate knowledge, positive attitudes, and proactive practices. Univariate and multivariate regression analyses were used to identify factors associated with KAP scores, and structural equation modeling (SEM) was performed to examine the direct and indirect relationships among knowledge, attitudes, and practices.
Results: Among respondents, 272 (50.4%) were male, and 67 (12.4%) reported a history of VTE. Mean scores were 8.04 ± 5.22 (knowledge), 40.99 ± 4.10 (attitude), and 28.77 ± 5.12 (practice), indicating inadequate knowledge, generally positive attitudes, and moderately proactive practices. SEM revealed that knowledge significantly influenced both attitude (β = 0.365, P < 0.001) and practice (β = 0.306, P < 0.001), while attitude also affected practice (β = 0.219, P < 0.001). Knowledge further had an indirect effect on practice via attitude (β = 0.080, P < 0.001).
Conclusion: These findings highlight critical knowledge gaps among elderly individuals, particularly in mechanical prophylaxis and symptom recognition, underscoring the urgent need for targeted educational interventions to improve VTE prevention strategies.
Keywords: venous thromboembolism, knowledge, attitude, practice, elderly, cross-sectional study
Introduction
Venous thromboembolism (VTE), encompassing deep venous thrombosis (DVT) and pulmonary embolism (PE), presents distinct clinical symptoms depending on the site of thrombosis.1 VTE most commonly occurs in the deep veins of the legs and thighs.2 The global burden of VTE is substantial, with an annual incidence rate of approximately 1.5 per 1000 individuals and a lifetime prevalence of around 5%.3,4 The incidence of VTE increases dramatically with age, reaching up to 1 per 100 annually in older individuals, with advancing age identified as the most critical risk factor.5 Older adults not only face a higher incidence of VTE but also experience more severe outcomes, including significantly higher thirty-day mortality and one-year recurrence rates compared to younger individuals.6 A study has shown that VTE exhibits more severe outcomes in elderly populations, with older patients experiencing significantly higher thirty-day mortality rates of 11.3% compared to 6.6% in younger patients. The elderly also face elevated one-year recurrence rates of 15.8%, notably higher than the 9.1% observed in younger individuals, along with an increased risk of major bleeding complications at 11.3% versus 7.8% in younger patients.7 Additionally, the economic burden of VTE treatment, encompassing hospitalization, anticoagulant therapy, and the management of complications such as post-thrombotic syndrome, represents a challenge for healthcare systems and patients.8
While most existing data are derived from Western populations, emerging studies in China have reported a similar or rising incidence of VTE among elderly hospitalized patients, highlighting the growing clinical relevance of VTE prevention in the Chinese context.9,10 Elderly individuals in China represent a particularly relevant population for VTE prevention research. Compared with younger adults, older adults often have lower health literacy, multiple chronic conditions, and greater dependence on family members for health-related decision-making. In addition, cultural beliefs, limited awareness of preventive care, and variations in access to structured health education may influence their understanding of VTE and engagement in preventive behaviors.11 Within the Chinese healthcare system, geriatric care is frequently delivered through a combination of hospital-based services and family-supported care, making patient knowledge and self-management especially important for effective VTE prevention. Recent systematic reviews examining twelve randomized controlled trials with 2918 participants have demonstrated the significant impact of structured self-management programs among elderly patients. Those engaging in daily moderate physical activity of thirty minutes and following medication adherence protocols showed a forty-two percent reduction in VTE incidence compared to usual care groups, highlighting the crucial role of active self-management in VTE prevention.12 Evidence from comprehensive meta-analyses encompassing nineteen studies with 1681 participants has established the effectiveness of preventive measures. Properly fitted graduated compression stockings reduced VTE risk by sixty-three percent in high-risk elderly patients, while systematic mobilization protocols involving multiple short daily walks decreased VTE incidence by forty-nine percent compared to standard care approaches.13
The knowledge, attitudes, and practices (KAP) framework is widely used to assess health literacy and is based on the premise that knowledge fosters positive attitudes, which in turn shape behavior. In the context of health literacy, KAP surveys operate on the premise that increased knowledge fosters positive attitudes, which in turn shape behaviors.14,15 While previous KAP studies on VTE have primarily focused on nurses.14,16 Understanding the KAP of older adults regarding VTE is crucial. Prolonged immobility and comorbidities increase their vulnerability to VTE, but evidence suggests that active self-management can significantly improve outcomes. However, it is unclear whether elderly individuals are aware of preventive measures or practice them effectively. Recent literature has summarized the current state of KAP regarding VTE prevention among hospitalized patients in China. A narrative review by Pu et al (2024) indicated that most patients exhibited low levels of VTE-related knowledge, while attitudes and behaviors varied from moderate to good depending on education level, clinical department, and exposure to health education. However, the review also highlighted a lack of targeted research focusing specifically on elderly inpatients, who are among the highest-risk groups.15 In line with national clinical consensus, recent Chinese guidelines emphasize the importance of enhancing awareness, prevention, and early intervention for venous thromboembolism among elderly patients, thereby reinforcing the need to assess their knowledge, attitudes, and practices. Therefore, this study aims to explore the current state of KAP regarding VTE among the elderly. Specifically, this study aims to determine the levels of knowledge, attitudes, and practices toward VTE among elderly individuals, and to examine whether attitudes mediate the relationship between knowledge and practices.
Materials and Methods
Study Design and Subjects
This cross-sectional study was conducted on the elderly between September and October 2024 in the Department of Gerontology, Shanghai Sixth People’s Hospital Affiliated with Shanghai Jiao Tong University School of Medicine. The study received ethical approval from the Ethics Committee of Shanghai Sixth People’s Hospital (Approval No: 2024–171), and informed consent was obtained from all participants prior to enrollment. Participants were eligible for inclusion if they were aged 60 years or older, capable of understanding the study’s purpose, and willing to voluntarily provide informed consent. Individuals with serious medical conditions, including advanced malignancy, severe cardiopulmonary diseases (eg, New York Heart Association class IV heart failure, severe chronic obstructive pulmonary disease, or severe hearing and visual impairments), or other conditions that could significantly impair cognitive function or communication ability, were excluded to ensure the reliability of questionnaire responses. Cognitive screening is routinely conducted for elderly inpatients in our institution. Cognitive normality was determined using the Montreal Cognitive Assessment–Basic (MoCA-B), with education-adjusted scores within the normal range, together with intact activities of daily living.
Questionnaire
The questionnaire was developed based on the relevant clinical guidelines, including the “Chinese expert consensus on the prevention and treatment of venous thromboembolism in the elderly”17 and the “Expert consensus on the prevention of venous thromboembolism for elderly patients with critical illness in China (2023)”18 The initial draft underwent expert review by two geriatric specialists with over three decades of clinical experience. Their feedback led to refinements in terminology and the addition of lifestyle modification components, such as recommendations regarding prolonged immobility. A pilot study (n=31) was conducted to assess reliability, yielding an overall Cronbach’s alpha coefficient of 0.768, which indicated good internal consistency. To assess construct validity, confirmatory factor analysis (CFA) was performed. The CFA results indicated an acceptable model fit, with all key indices falling within recommended thresholds. These results suggest that the questionnaire has acceptable construct validity and that the factor structure adequately represents the theoretical dimensions of knowledge, attitudes, and practices (Figure S1).
The questionnaire comprehensively collected demographic, socioeconomic, anthropometric, clinical, and VTE-related information, and assessed knowledge, attitudes, and practices using structured scales comprising 10 knowledge items, 10 attitude items, and 8 practice items with predefined scoring systems (detailed in Supplementary materials; Questionnaire Introduction section). A validation trap item of common knowledge was incorporated to identify non-attentive responses. The questionnaire was originally developed and administered in Chinese; therefore, no translation or back-translation procedures were required (the Chinese and English versions of the questionnaire are provided in the Supplementary Materials). Thresholds for adequate knowledge, positive attitudes, and proactive practices were established at 70% of the possible maximum scores. This cut-point is widely used in KAP research when no validated or unified standard exists, including studies involving elderly lay populations. In the context of older adults without professional medical training, a 70% threshold is commonly considered to reflect a meaningful level of understanding or engagement rather than expert-level mastery, thereby supporting interpretability and comparability across studies.19,20
Questionnaire Distribution and Quality Control
A mixed-mode survey design incorporating both digital and paper-based administration was implemented using convenience sampling. The digital questionnaire was hosted on the Wenjuanxing platform (https://www.wjx.cn/) and distributed via QR codes displayed in geriatric outpatient and inpatient departments. Additional digital distribution occurred through the hospital’s geriatric medicine department’s WeChat public account. For paper-based administration, researchers conducted face-to-face survey distribution in clinical settings, providing clarification of questionnaire items as needed. Two designated research assistants summarized the data and performed data quality control, with each assistant cross-checking the other’s work. Quality control measures included the exclusion of digital responses completed in less than 90 seconds, incorrect responses to validation trap items, and submissions exhibiting response patterns indicative of inattentive completion or logical inconsistencies. The time threshold of 90 seconds was determined based on pilot testing and the average completion time required to read and answer all items, and was used to identify responses likely completed without adequate consideration.
Sample Size
The required sample size was estimated using the standard formula for cross-sectional studies,21,22 with a significance level of α = 0.05:

where  . To obtain a conservative estimate, the expected proportion
. To obtain a conservative estimate, the expected proportion  was set at 0.5, which yields the maximum sample size, and the admissible error
was set at 0.5, which yields the maximum sample size, and the admissible error  was defined as 5%. Based on this calculation, the minimum required sample size was 400, and after accounting for an anticipated 20% attrition rate, the final target sample size was 480.
was defined as 5%. Based on this calculation, the minimum required sample size was 400, and after accounting for an anticipated 20% attrition rate, the final target sample size was 480.
Statistical Analysis
Data analysis was performed using SPSS 26.0 (IBM, Armonk, NY, USA) and AMOS 24.0 (IBM, Armonk, NY, USA). Normality tests were conducted to assess the distribution of scores across each dimension. For normally distributed continuous variables, means and standard deviations (SD) were reported, and independent t-tests or analysis of variance (ANOVA) were employed to compare. For skewed distributed continuous variables, medians with interquartile ranges (25th and 75th percentiles) were presented, and the Wilcoxon-Mann–Whitney test and the Kruskal–Wallis test was applied for comparison. Correlations between the scores of knowledge, attitude, and practice dimensions were examined using the Spearman correlation coefficient. To identify factors associated with KAP dimension scores, univariate and multivariate regression analyses were conducted. Variables with a P-value < 0.1 in the univariate analyses were included in the multivariate regression models. Median scores for each dimension were used to classify participants for regression analysis. Structural equation modeling (SEM), grounded in the KAP theoretical framework, was utilized to test whether attitudes mediate the relationship between knowledge and practice. The hypothesized model included direct paths from knowledge to attitude and practice, and from attitude to practice, based on the conceptual KAP framework. Prior to SEM, potential confounders identified through univariate analyses (eg, age, education level, prior VTE education) were considered during model interpretation. Model fit was assessed using root mean square error of approximation (RMSEA), standardized root mean square residual (SRMR), Tucker-Lewis index (TLI), and comparative fit index (CFI). SEM was used to test the following hypotheses: (H1) knowledge has a direct effect on attitude and practice, (H2) attitude has a direct effect on practice, and (H3) knowledge indirectly affects practice through attitude. Following verification of these assumptions, the model examined both direct pathways and mediating effects. Model fit was evaluated using the following criteria: root mean square error of approximation (RMSEA) < 0.08, standardized root mean square residual (SRMR) < 0.08, Tucker-Lewis index (TLI) > 0.8, and comparative fit index (CFI) > 0.8. A two-tailed P-value < 0.05 was considered statistically significant.
Results
Basic Information on the Population
A total of 568 participants were initially enrolled in the study. After excluding 2 participants due to lack of informed consent, 8 due to abnormal height or weight entries, 1 for logical errors in multiple-choice questions, and 17 for incorrect answers to trap questions, 540 valid datasets were analyzed, yielding a validity rate of 95.1%. Among these, 272 (50.4%) were male, 254 (47.0%) were aged 60–69 years, 214 (39.6%) had a household per capita monthly income of 5000–10,000 yuan, 335 (62.0%) had a BMI within the normal range, 379 (70.2%) had other medical conditions, 67 (12.4%) had been diagnosed with VTE, and 111 (20.6%) had received relevant education (Table 1).
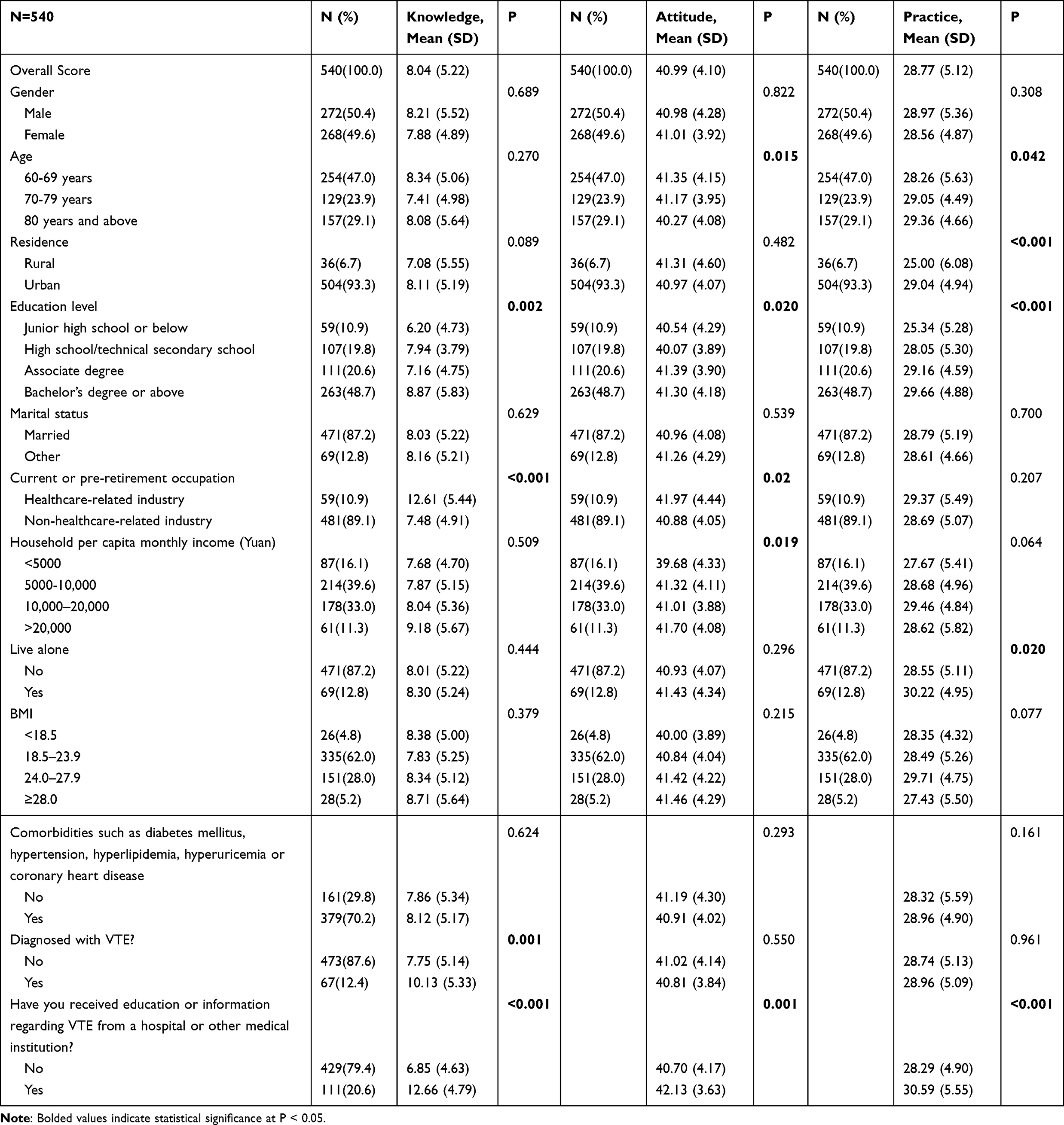 |
Table 1 Baseline Characteristics and KAP Scores of Study Participants |
The mean scores for knowledge, attitude, and practice were 8.04±5.22 (of a possible 20 points), 40.99±4.10 (of a possible 50 points), and 28.77±5.12 (of a possible 40 points), respectively. Using the threshold of 70% of the maximum possible score as the cutoff value (14 points for knowledge, 35 points for attitude, and 28 points for practice), 21.3% (115/540) of participants demonstrated adequate knowledge, 89.4% (483/540) showed positive attitudes, and 52.8% (285/540) exhibited proactive practices regarding VTE. Analysis of demographic characteristics revealed that knowledge scores were significantly associated with education level (P < 0.010), current or pre-retirement occupation (P < 0.001), VTE diagnosis (P = 0.001), and relevant education received (P < 0.001). Attitude scores were associated with age (P = 0.015), education level (P = 0.020), current or pre-retirement occupation (P = 0.020), household per capita monthly income (P = 0.019), and relevant education received (P = 0.001). Practice scores were associated with age (P = 0.042), residence (P < 0.001), education level (P < 0.001), living alone (P = 0.020), and relevant education received (P < 0.001) (Table 1).
Distribution of Responses to Knowledge, Attitude, and Practice
In the knowledge dimension, the three items most frequently answered as “Unclear” were: “Mechanical preventive methods, such as the use of medical compression stockings and intermittent pneumatic compression devices, can aid in the prevention of VTE” (K8, 49.1%), “Pulmonary embolism primarily manifests as dyspnea” (K5, 37.4%), and “Common treatment methods for VTE include anticoagulant medications, thrombolytic therapy, and surgical thrombectomy” (K10, 37.4%) (Table 2). In the attitude dimension, 20.7% of respondents were very concerned, and 35.4% were concerned about developing VTE (A3). However, 8.3% indicated they would not take active preventive measures (A8), and 36.5% held a neutral stance (Table 3). For practice-related responses, 50.7% reported never using medical compression stockings or other mechanical preventive measures (P6), 8.5% never paid attention to weight management to reduce the risk of VTE (P8), and 6.1% never attempted to avoid smoking or exposure to secondhand smoke (P7) (Table 4). Regarding the sources of awareness about VTE, the majority of patients (301, 55.7%) reported obtaining information through new media platforms, including WeChat, Weibo, Douyin, and Xiaohongshu. Additionally, 277 respondents (51.3%) acquired knowledge from medical sources, such as supervising doctors, hospital lectures, and educational campaigns.
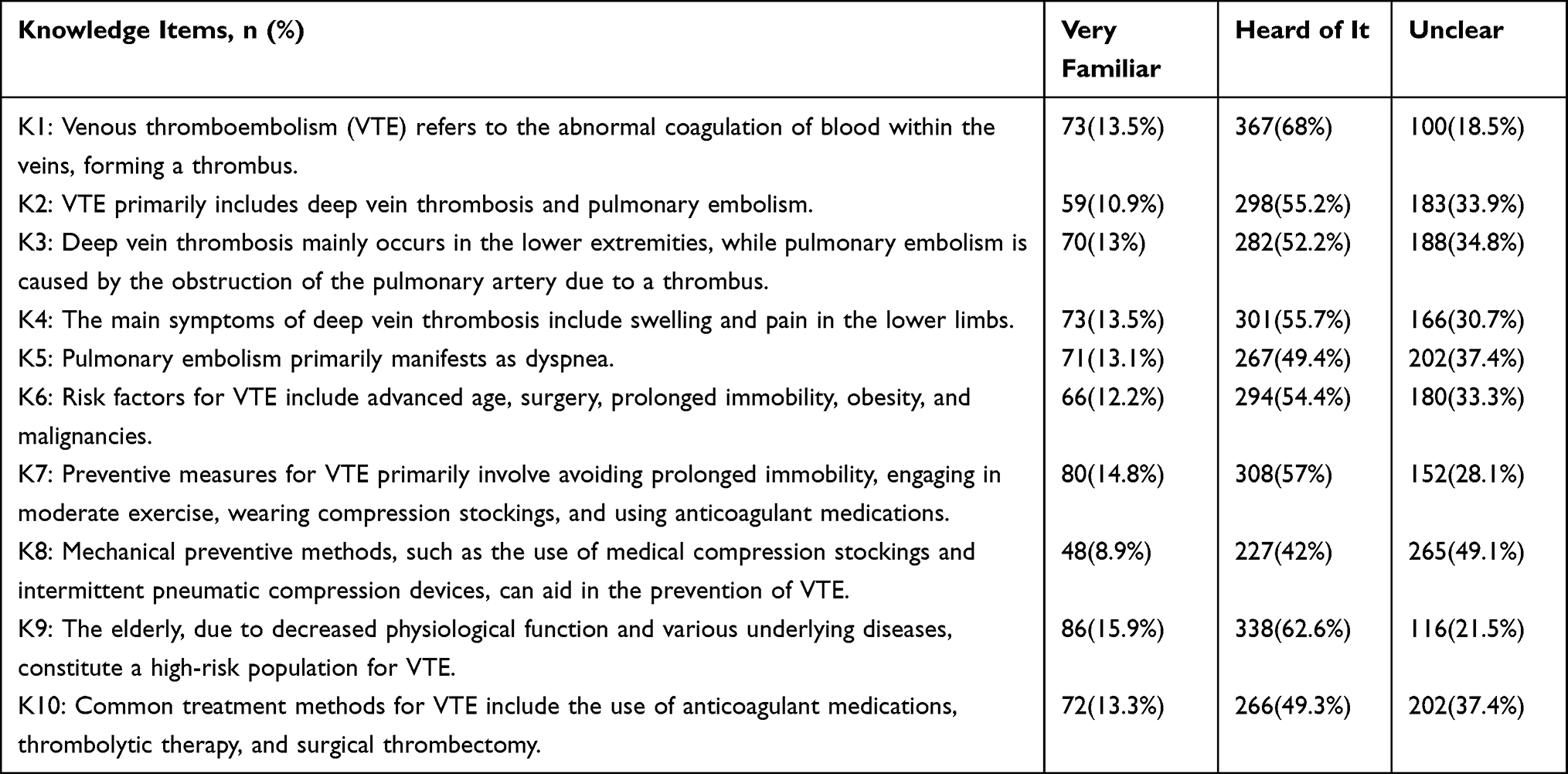 |
Table 2 Distribution of Responses in the Knowledge Dimension |
 |
Table 3 Distribution of Responses in the Attitude Dimension |
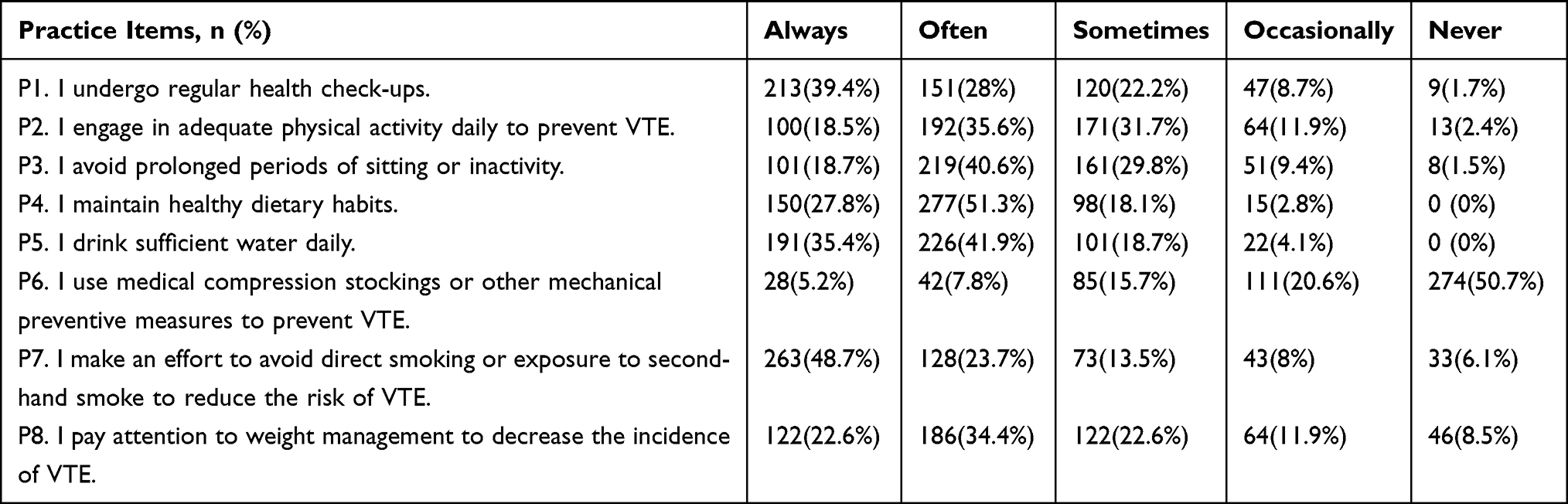 |
Table 4 Distribution of Responses in the Practice Dimension and Behavioral Insights |
Correlations Between KAP
Correlation analysis revealed significant positive relationships between knowledge and attitude scores (r = 0.325, P < 0.001), knowledge and practice scores (r = 0.355, P < 0.001), and attitude and practice scores (r = 0.339, P < 0.001) (Table 5).
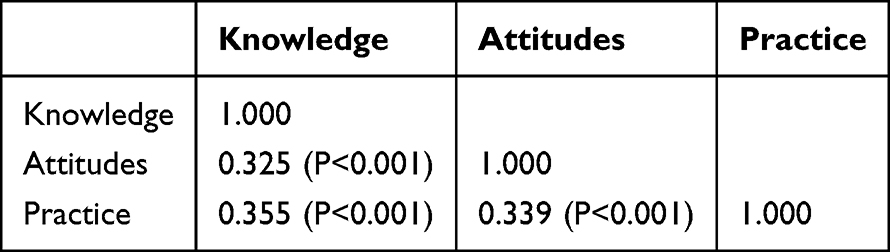 |
Table 5 Correlation Analysis Among Knowledge, Attitudes, and Practices Dimensions |
Univariate and Multivariate Analysis of Knowledge, Attitude, and Practice Dimensions
The multivariate regression analysis showed that knowledge significantly influenced attitudes (OR = 1.129, 95% CI: [1.082, 1.178], P < 0.001) and practices (OR = 1.121, 95% CI: [1.071, 1.172], P < 0.001), with attitudes also positively influencing practices (OR = 1.102, 95% CI: [1.048, 1.158], P < 0.001). Higher education levels, specifically high school/technical secondary school (OR = 2.616, 95% CI: [1.180, 5.796], P = 0.018) and Bachelor’s degree or above (OR = 2.410, 95% CI: [1.115, 5.210], P = 0.025), were independently associated with proactive practices. The detailed results, adjusted for confounding factors, are available in the supplementary materials (Tables S1–S3).
SEM Analysis
The SEM analysis demonstrated good model fit (RMSEA = 0.068, SRMR = 0.064, TLI = 0.894, and CFI = 0.903) (Table S4). Direct effects were observed for knowledge on attitude (β = 0.365, P < 0.001) and practice (β = 0.306, P < 0.001), as well as for attitude on practice (β = 0.219, P < 0.001). Knowledge also had an indirect effect on practice mediated by attitude (β = 0.080, P < 0.001) (Table S5 and Figure 1).
 |
Figure 1 Structured equation modeling. Ellipses represent latent variables (unobserved constructs), including overall knowledge, attitude, and practice. Rectangles represent observed variables (measured questionnaire items) that serve as indicators of the latent variables. Circles represent error terms or residuals associated with the observed variables. Single-headed arrows indicate hypothesized directional relationships (pathways) between latent variables and from latent variables to observed variables, with standardized path coefficients labeled on the arrows. |
Discussion
Elderly individuals demonstrated inadequate knowledge but generally positive attitudes and proactive practices toward VTE. While the observed patterns are consistent with those reported in previous KAP studies, the present findings provide population-specific evidence among elderly Chinese patients, offering valuable local data to inform targeted prevention strategies in this setting. Efforts to improve educational initiatives, particularly targeting knowledge gaps through tailored interventions, may enhance VTE prevention and management among this population.
Poor knowledge of VTE, a condition with significant morbidity and mortality risks, may contribute to suboptimal prevention and delayed treatment, underscoring the need for targeted educational interventions. The results of this study identified three major knowledge gaps among elderly participants: limited understanding of mechanical prophylaxis methods, poor recognition of key symptoms of pulmonary embolism, and inadequate awareness of available treatment options for VTE. These deficiencies mirror previous research showing that elderly individuals are often less familiar with newer or specialized preventive techniques, like medical compression stockings or intermittent pneumatic compression devices.23,24 Additionally, low awareness of critical symptoms such as dyspnea for pulmonary embolism may lead to delayed recognition and postponed medical intervention, which in turn increases the risk of severe complications, higher short-term mortality, and disease progression in elderly patients. Compared to studies conducted in Western populations, where health literacy initiatives have improved general awareness of VTE,25,26 the observed gaps in our study suggest that current health education efforts in China may not be adequately addressing these specific topics.
To address the gaps in VTE prevention awareness, education should focus on three aspects: mechanical prevention, symptom recognition, and treatment knowledge. Practical sessions, such as demonstrations of compression device use, can enhance understanding and compliance. Educational materials using real-life scenarios can further aid symptom identification. Cultural and social factors, such as reliance on family members for health-related decision-making and traditional health beliefs, may influence health behaviors among some older adults in China, as suggested by previous studies.27,28 Although platforms like WeChat and Douyin are popular, limited digital literacy in some elderly patients hinders access to online information. Therefore, education should combine digital and traditional formats, including printed brochures, community lectures, and involvement of family members and community leaders.
Healthcare providers should integrate VTE education into routine care using simple language and visual tools. As prior research suggests,29 new media are important for information dissemination among the elderly. Thus, combining digital platforms with offline strategies ensures broader coverage. Despite positive attitudes, many patients were neutral toward preventive behaviors like compression stocking use and exercise. This may stem from unclear guidance or low perceived relevance. Personalized action plans and regular follow-ups by community health workers may improve adherence. Highlighting benefits such as independence and reduced caregiver burden may further motivate engagement.30,31 Campaigns should leverage trusted media platforms to enhance reach across diverse populations.32,33
In terms of practices, the low uptake of mechanical preventive measures and inadequate attention to weight management were notable concerns. These results are consistent with previous findings, where practical barriers such as cost, accessibility, or cultural perceptions of these interventions often limit adherence.34,35 To overcome these challenges, policymakers should consider subsidizing compression stockings for low-income groups and increasing their availability through community pharmacies or clinics. Cultural perceptions of aging, preventive care, and reliance on traditional practices may influence VTE awareness and behaviors.36 These factors could limit engagement with formal education or preventive strategies, underscoring the need for culturally sensitive interventions. Additionally, integrating weight management counseling into routine geriatric care and providing free or low-cost exercise programs tailored for the elderly could foster long-term behavioral changes. Programs could include group activities such as tai chi, walking clubs, or guided stretching sessions to improve both adherence and social support.8,37
The significant correlations between knowledge, attitudes, and practices observed in this study are consistent with existing literature, which underscores the interdependence of these dimensions in shaping health behaviors.38,39 These moderate correlations indicate that while knowledge and attitudes are important, they only partially explain behavioral practices, suggesting the need for comprehensive interventions. Structural equation modeling results further confirmed that attitudes mediate the relationship between knowledge and practice. This suggests that while improving knowledge is critical, fostering positive attitudes is equally important for translating knowledge into sustained behavior changes. Importantly, the structural equation modeling results provide practical implications for intervention design. The demonstrated direct and indirect pathways indicate that knowledge alone is insufficient to drive preventive behaviors unless it is accompanied by supportive attitudes. Therefore, educational interventions for elderly populations should not only focus on disseminating factual information about VTE but also aim to strengthen risk perception, perceived benefits of prevention, and confidence in self-management. Multicomponent programs that integrate knowledge delivery with attitude-oriented strategies, such as motivational counseling, case-based education, and peer support, may be more effective in promoting sustained preventive practices. For example, incorporating peer-led testimonials or real-world success stories may help reinforce motivation and self-efficacy among elderly individuals.
The multivariate analysis identified several demographic and socioeconomic factors influencing KAP outcomes. Higher education levels were consistently associated with better knowledge and practices, likely reflecting greater access to health information and higher health literacy. Similar trends have been reported in studies on hypertension management, where individuals with higher education are more likely to engage in preventive health behaviors.40,41 Interventions targeting individuals with lower educational attainment should use simple, visually engaging materials and focus on actionable steps rather than technical explanations. Our analysis revealed an interesting age-related pattern: adults aged 80 and above demonstrated significantly better practices yet showed poorer attitudes compared to their younger counterparts aged 60–69 years. This discrepancy between attitudes and practices among the oldest age group suggests a need for tailored interventions that address generational differences in health perceptions while reinforcing the importance of maintaining their existing preventive practices.
Notably, our analysis revealed that prior VTE-related education from medical institutions was one of the strongest predictors of KAP outcomes. In both univariate and multivariate analyses, participants with previous educational exposure consistently showed better performance across all three dimensions, with the strongest association observed in the knowledge domain. These findings align with previous research demonstrating the effectiveness of structured educational programs in improving health outcomes.42,43 The robust association between prior education and improved KAP scores underscores the critical role of healthcare providers in delivering targeted education. Based on these findings, we recommend that hospitals incorporate VTE prevention into routine health check-ups, with nurses or allied health professionals offering brief, tailored educational sessions. Healthcare providers play a central role in VTE education and prevention. Targeted training programs focusing on updated clinical guidelines and effective patient communication strategies may enhance their capacity to deliver consistent and impactful health education. For rural populations with limited access to hospitals, telehealth platforms or mobile health units could be considered as alternative delivery methods for educational programs.
This study has several limitations. First, due to its cross-sectional design, causal relationships between knowledge, attitudes, and practices related to VTE cannot be established. Second, the use of convenience sampling may have introduced selection bias, as individuals who were more accessible or willing to participate may differ systematically from those who were not, potentially limiting the representativeness and generalizability of the findings. In particular, the overrepresentation of participants with higher educational attainment may have contributed to selection bias, as such individuals are more likely to engage in health surveys and possess higher baseline health literacy. Third, the absence of random sampling further reduces the external validity of the study, making it difficult to extrapolate the results to the broader elderly population in Shanghai. Fourth, data were collected from a single hospital, which may further limit generalizability to other settings or populations. Fifth, reliance on self-reported data may introduce reporting bias, as participants could overestimate their knowledge or practices due to social desirability. In addition, some practice items reflected general health or wellness behaviors rather than VTE-specific preventive actions, which may have reduced the specificity of the practice dimension. Furthermore, because of the anonymous nature of the online survey, test–retest reliability could not be assessed, limiting evaluation of the questionnaire’s temporal stability. Together, the reliance on self-reported data and the inability to assess test–retest reliability may introduce measurement bias. Finally, although regression analyses adjusted for key demographic and educational variables, some VTE-related clinical factors, such as recent surgery or medication use, were not included, which may have influenced the observed associations. These limitations should be considered when interpreting the results and designing future research.
Conclusion
In conclusion, these findings highlight critical knowledge gaps among elderly individuals, particularly in mechanical prophylaxis and symptom recognition, despite generally positive attitudes and moderate preventive practices. Knowledge was shown to play a central role in shaping both attitudes and practices, with attitudes partially mediating the relationship between knowledge and preventive behaviors. These results underscore the urgent need for targeted, population-appropriate educational interventions to strengthen VTE-related knowledge and translate awareness into effective preventive practices among elderly individuals.
Data Sharing Statement
All data generated or analysed during this study are included in this published article.
Ethics Approval and Informed Consent
The study was approved by the Ethics Committee of Shanghai Sixth People’s Hospital (2024-171). All participants were informed about the study protocol and provided written informed consent to participate in the study. I confirm that all methods were performed in accordance with the relevant guidelines. All procedures were performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. McLendon K, Goyal A, Attia M. Deep venous thrombosis risk factors. In: StatPearls. Treasure Island (FL): StatPearls Publishing Copyright © 2024, StatPearls Publishing LLC.; 2024.
2. Kraft CT, Janis JE. Deep venous thrombosis prophylaxis. Clin Plast Surg. 2020;47(3):409–13. doi:10.1016/j.cps.2020.03.002
3. Heit JA. Epidemiology of venous thromboembolism. Nat Rev Cardiol. 2015;12(8):464–474. doi:10.1038/nrcardio.2015.83
4. Stevens H, Tran H, Gibbs H. Venous thromboembolism: current management. Aust Prescr. 2019;42(4):123–126. doi:10.18773/austprescr.2019.039
5. Naess IA, Christiansen SC, Romundstad P, Cannegieter SC, Rosendaal FR, Hammerstrøm J. Incidence and mortality of venous thrombosis: a population-based study. J Thromb Haemost. 2007;5(4):692–699. doi:10.1111/j.1538-7836.2007.02450.x
6. Hong J, Lee JH, Yhim HY, et al. Incidence of venous thromboembolism in Korea from 2009 to 2013. PLoS One. 2018;13(1):e0191897. doi:10.1371/journal.pone.0191897
7. Spencer FA, Gore JM, Lessard D, et al. Venous thromboembolism in the elderly. Thrombosis Haemostasis. 2008;100(05):780–788. doi:10.1160/TH08-04-0255
8. Gregson J, Kaptoge S, Bolton T, et al. Cardiovascular risk factors associated with venous thromboembolism. JAMA Cardiol. 2019;4(2):163–173. doi:10.1001/jamacardio.2018.4537
9. Chen X, Huang J, Liu J, Deng H, Pan L. Venous thromboembolism risk factors and prophylaxis of elderly intensive care unit patients in a Chinese general hospital. Ann Palliat Med. 2021;10(4):4453–4462. doi:10.21037/apm-21-464
10. Jin F, Cheng Y-Q, Yan W, Chen Y, Zhong N-S, Zhong N-S. Incidence and prevention of venous thromboembolism in acutely ill hospitalized elderly Chinese. Chinese Med J. 2011;124(3):335–340.
11. Lee JA, Donaldson J, Drake D, et al. Venous thromboembolism knowledge among older post-Hip fracture patients and their caregivers. Geriatr Nurs. 2014;35(5):374–380. doi:10.1016/j.gerinurse.2014.05.004
12. Kahn SR, Morrison DR, Cohen JM, et al. Interventions for implementation of thromboprophylaxis in hospitalized medical and surgical patients at risk for venous thromboembolism. Cochrane Database Syst Rev. 2013; 7. doi:10.1002/14651858.CD008201.pub2
13. Clarke MJ, Broderick C, Hopewell S, Juszczak E, Eisinga A. Compression stockings for preventing deep vein thrombosis in airline passengers. Cochrane Database Syst Rev. 2021;4(4). doi:10.1002/14651858.CD004002.pub4
14. Al-Mugheed K, Bayraktar N. Knowledge, risk assessment, practices, self-efficacy, attitudes, and behaviour’s towards venous thromboembolism among nurses: a systematic review. Nurs Open. 2023;10(9):6033–6044. doi:10.1002/nop2.1914
15. Pu Z, Jia P, Chen J, et al. Research progress on knowledge-attitude-practice of VTE prevention in hospitalized patients: a review. Medicine. 2024;103(27):e38714. doi:10.1097/MD.0000000000038714
16. Lee J-A, Grochow D, Drake D, Johnson L, Reed P, van Servellen G. Evaluation of hospital nurses’ perceived knowledge and practices of venous thromboembolism assessment and prevention. J Vasc Nurs. 2014;32(1):18–24. doi:10.1016/j.jvn.2013.06.001
17. Society PVDMBotCG; Jichun Z, Yuzhen Z. Chinese expert consensus on the prevention and treatment of venous thromboembolism in the elderly. Chin J Bases Clin General Surg. 2023;30(10):1173–1187
18. Society CCMDo CG, Medicine ZPCRCf CC; Jing Y. Expert consensus on the prevention of venous thromboembolism for elderly patients with critical illness in China (2023. Chin Crit Care Med. 2023;35(6):561–572
19. Hebo HJ, Gemeda DH, Abdusemed KA. Hepatitis B and C viral infection: prevalence, knowledge, attitude, practice, and occupational exposure among healthcare workers of Jimma university medical center, Southwest Ethiopia. Scientific World J. 2019;2019:9482607. doi:10.1155/2019/9482607
20. He D, Shen X, Wang L, Pan Z. Knowledge, attitude and practice of the community general practice teams on dysphagia complicated with aspiration pneumonia after stroke. Healthcare. 2023;11(23). doi:10.3390/healthcare11233073
21. Chen Q, Zhang Y, Li H. Knowledge, attitude, and practice toward non-nutritive sweeteners among the population with reduced sugar intake requirement. Front Nutr. 2023;10:1268599. doi:10.3389/fnut.2023.1268599
22. Zhi X, Chen J, Yang L, et al. Knowledge, attitudes, and practices toward nutritional management among patients with gastrointestinal cancer: a cross-sectional study. Asia Pac J Oncol Nurs. 2025;12:100688. doi:10.1016/j.apjon.2025.100688
23. Dahm KT, Myrhaug HT, Strømme H, Fure B, Brurberg KG. Effects of preventive use of compression stockings for elderly with chronic venous insufficiency and swollen legs: a systematic review and meta-analysis. BMC Geriatr. 2019;19(1):76. doi:10.1186/s12877-019-1087-1
24. Nickles MA, Ennis WJ, O’Donnell TF, Altman IA. Compression therapy in peripheral artery disease: a literature review. J Wound Care. 2023;32(Sup5):S25–s30. doi:10.12968/jowc.2023.32.Sup5.S25
25. Pelikan JM, Straßmayr C, Ganahl K. Health literacy measurement in general and other populations: further initiatives and lessons learned in Europe (and Beyond). Stud Health Technol Inform. 2020;269:170–191. doi:10.3233/SHTI200031
26. Alvarado-Little W. Health literacy initiatives and lessons learned within public health agencies. Stud Health Technol Inform. 2020;269:294–302. doi:10.3233/SHTI200044
27. Key NS, Khorana AA, Kuderer NM, et al. Venous thromboembolism prophylaxis and treatment in patients with cancer: ASCO clinical practice guideline update. J Clin Oncol. 2020;38(5):496–520. doi:10.1200/JCO.19.01461
28. Speth J. Guidelines in practice: prevention of venous thromboembolism. Aorn J. 2023;118(5):321–328. doi:10.1002/aorn.14019
29. Ratcliff CL, Krakow M, Greenberg-Worisek A, Hesse BW. Digital health engagement in the US population: insights from the 2018 health information national trends survey. Am J Public Health. 2021;111(7):1348–1351. doi:10.2105/AJPH.2021.306282
30. Joslin EP. The prevention of diabetes mellitus. JAMA. 2021;325(2):190. doi:10.1001/jama.2020.17738
31. Schaper NC, van Netten JJ, Apelqvist J, et al. Practical guidelines on the prevention and management of diabetes-related foot disease (IWGDF 2023 update). Diabetes Metab Res Rev. 2024;40(3):e3657. doi:10.1002/dmrr.3657
32. Campello E, Spiezia L, Adamo A, Simioni P. Thrombophilia, risk factors and prevention. Expert Rev Hematol. 2019;12(3):147–158. doi:10.1080/17474086.2019.1583555
33. O’Rourke E, Faryal R, Blondon M, Middeldorp S, Ná F. VTE risk assessment and prevention in pregnancy. Hamostaseologie. 2024;44(3):218–225. doi:10.1055/a-2238-4681
34. Bukhsh A, Goh BH, Zimbudzi E, et al. Type 2 diabetes patients’ perspectives, experiences, and barriers toward diabetes-related self-care: a qualitative study from Pakistan. Front Endocrinol. 2020;11:534873. doi:10.3389/fendo.2020.534873
35. Owens-Gary MD, Zhang X, Jawanda S, Bullard KM, Allweiss P, Smith BD. The importance of addressing depression and diabetes distress in adults with type 2 diabetes. J Gen Intern Med. 2019;34(2):320–324. doi:10.1007/s11606-018-4705-2
36. Dong J, Yu S, Qin Y, Jin X, Xing Y, Wang H. Knowledge and health beliefs about dementia prevention among Chinese older adults: a qualitative study. Qualitative Health Res. 2025;10497323251324127. doi:10.1177/10497323251324127
37. Partridge JA, Anton PM, Wallace JP, Lake LL. Exercise social support, barriers, and instructions in venous thromboembolism survivors: a descriptive study. Res Pract Thromb Haemost. 2023;7(5):102147. doi:10.1016/j.rpth.2023.102147
38. Davies C, Stoney T, Hutton H, et al. School-based HPV vaccination positively impacts parents’ attitudes toward adolescent vaccination. Vaccine. 2021;39(30):4190–4198. doi:10.1016/j.vaccine.2021.05.051
39. Yılmaz G, Riad A, Krsek M, Kurt H, Attia S. Oral health-related knowledge, attitudes and behaviours of elementary school teachers. Int J Environ Res Public Health. 2021;18(11):6028. doi:10.3390/ijerph18116028
40. Przezak A, Bielka W, Pawlik A. Hypertension and type 2 diabetes-the novel treatment possibilities. Int J Mol Sci. 2022;23(12):6500. doi:10.3390/ijms23126500
41. Wang Y, Ye C, Kong L, et al. Independent associations of education, intelligence, and cognition with hypertension and the mediating effects of cardiometabolic risk factors: a Mendelian randomization study. Hypertension. 2023;80(1):192–203. doi:10.1161/HYPERTENSIONAHA.122.20286
42. Fasolino T, Koci A, Huggins J, Lindell K. A rapid review of uses and outcomes of telehealth care in rural and remote regions in the United States. J Hosp Palliat Nurs. 2023;25(5):239–248. doi:10.1097/NJH.0000000000000964
43. Janjua S, Carter D, Threapleton CJ, Prigmore S, Disler RT. Telehealth interventions: remote monitoring and consultations for people with chronic obstructive pulmonary disease (COPD). Cochrane Database Syst Rev. 2021;7(7):Cd013196. doi:10.1002/14651858.CD013196.pub2
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Knowledge, Attitudes and Practices Towards Psoriasis Among Patients and Their Family Members
Zhang X, Du H, Liu X, Liu L, Zhang T
Clinical, Cosmetic and Investigational Dermatology 2024, 17:769-782
Published Date: 3 April 2024
Knowledge, Attitudes and Practices Toward Physical Literacy Among the College Students During COVID-19 School Closure
Ma C, Yue M, Zhu X
Journal of Multidisciplinary Healthcare 2024, 17:1629-1640
Published Date: 15 April 2024
Knowledge, Attitude and Practice of Radiologists Regarding Artificial Intelligence in Medical Imaging
Huang W, Li Y, Bao Z, Ye J, Xia W, Lv Y, Lu J, Wang C, Zhu X
Journal of Multidisciplinary Healthcare 2024, 17:3109-3119
Published Date: 4 July 2024
Knowledge, Attitude, and Practice Toward Varicocele in Patients with Varicoceles: A Cross-Sectional Study in Chinese Patients
Gong P, Shen J, Yang Y, Xue D, Lu H, Zhuang Q, Wang X, Tian Z, Chen Y, Chen C, Cao Y
International Journal of General Medicine 2024, 17:3423-3432
Published Date: 7 August 2024
Knowledge, Attitude, and Practice Towards Rehabilitation in Patients with Breast Cancer: A Cross-Sectional Study
Zhou Y, Lu Q, Yu X
Journal of Multidisciplinary Healthcare 2025, 18:1483-1492
Published Date: 12 March 2025