Back to Journals » Patient Preference and Adherence » Volume 20
Knowledge, Attitudes, and Practices Among Patients with Multiple Myeloma: A Cross‑Sectional Study Using Structural Equation Modeling in a Single Tertiary Hospital in Wenzhou, China
Authors Zhou Y, Jiang L, Guo H, Zhu R, Tu J, Feng A, Zheng Y
Received 25 February 2026
Accepted for publication 19 June 2026
Published 18 July 2026 Volume 2026:20 605250
DOI https://doi.org/10.2147/PPA.S605250
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Yulei Zhou,1 Lei Jiang,1 Haifei Guo,1 Ruijie Zhu,1 Ji Tu,1 Aimei Feng,1 Yangqin Zheng2
1Department of Hematology, Ruian People’s Hospital, The Third Affiliated Hospital of Wenzhou Medical University, Wenzhou, Zhejiang, People’s Republic of China; 2Department of Hematology, People’s Hospital of Wenzhou, The Third Clinical Institute Affiliated to Wenzhou Medical University, Wenzhou, Zhejiang, People’s Republic of China
Correspondence: Yangqin Zheng, Email [email protected] Aimei Feng, Email [email protected]
Introduction: This study aimed to evaluate the knowledge, attitude, and practice (KAP) of patients with multiple myeloma (MM) regarding the disease.
Methods: This cross-sectional study was conducted among patients with MM at Ruian People’s Hospital in Zhejiang Province, China, between August and November 2024. Data were collected using a structured questionnaire designed to gather demographic information and assess participants’ KAP.
Results: A total of 442 valid questionnaires were analyzed. Among the respondents, 226 (51.1%) were male, and 298 (67.4%) were newly diagnosed with MM. The mean scores for KAP were 13.70 ± 5.69 (range: 0– 22), 32.90 ± 2.89 (range: 10– 50), and 40.12 ± 6.89 (range: 10– 50), respectively. Structural equation modeling revealed that duration of diseases (β = 0.097, P = 0.047) and first-visit department (β = − 0.198, P < 0.001) were directly associated with knowledge. Knowledge (β = − 0.554, P < 0.001) was directly associated with attitude, which deserves cautious interpretation. Knowledge (β = 0.512, P < 0.001), attitude (β = − 0.628, P < 0.001), and education (β = 0.091, P = 0.016) were directly associated with practice. Meanwhile, the first-visit department (β = 0.110, P < 0.001) was indirectly associated with attitude. Knowledge (β = 0.348, P < 0.001), duration of diseases (β = 0.050, P = 0.050), and first-visit department (β = − 0.102, P < 0.001) were indirectly associated with practice. Given the cross-sectional design, the SEM results should be regarded as hypothesis‑generating rather than confirmatory.
Discussion: Patients with MM exhibited insufficient knowledge and slightly negative attitudes. Although mean practice scores were relatively high, important gaps persisted in key behaviors. These findings highlight the need for tailored educational strategies that account for patients’ first‑visit department and disease duration, and suggest that future interventions should address informational gaps alongside the emotional and practical concerns associated with disease awareness.
Keywords: multiple myeloma, knowledge, attitude, practice, cross-sectional study
Introduction
Multiple myeloma (MM) is a hematologic malignancy characterized by the clonal proliferation of plasma cells in the bone marrow, leading to complications such as bone lesions, anemia, renal dysfunction, and hypercalcemia.1,2 In China, the burden of MM has increased, with an estimated 18,793 new cases and 13,421 deaths reported in 2019.3 The age-standardized incidence and mortality rates were 0.93 and 0.67 per 100,000 population, respectively, with a higher burden in males.3 MM progression is driven by interactions between malignant plasma cells and the bone marrow microenvironment, contributing to disease persistence and treatment resistance. Although therapies such as proteasome inhibitors, immunomodulatory agents, and monoclonal antibodies have improved outcomes, MM remains largely incurable and follows a relapsing–remitting course requiring repeated treatment.4–6 Advances in therapy have improved survival, with five-year survival rates exceeding 60% in developed countries.7,8 Nevertheless, patients face ongoing challenges related to treatment complexity, cumulative toxicity, and long-term monitoring.9 As MM increasingly resembles a chronic condition, patients must continuously adapt to evolving treatment strategies while managing symptoms and adverse effects. This dynamic disease trajectory may influence not only patients’ knowledge of MM, but also their attitudes toward therapy and their engagement in recommended health practices.
Beyond biomedical complexity, MM imposes a considerable psychosocial burden. Patients often report high levels of anxiety, depression, and impaired quality of life, and qualitative work has underscored wide‑ranging supportive‑care needs across the disease trajectory. These psychosocial dimensions, including emotional distress, uncertainty about prognosis, and the cumulative impact of repeated treatment decisions, are central to the lived experience of MM and are likely to shape how patients interpret information and engage with recommended care.10,11 In parallel, health literacy has emerged as a key determinant of how patients with cancer understand their diagnosis and treatment options, participate in decision‑making, and navigate complex care pathways. Systematic reviews indicate that low health literacy is associated with difficulties processing cancer‑related information, poorer quality of life, and less favorable care experiences.12,13 In a chronic malignancy such as MM, where treatment regimens and prognostic information are particularly complex, health literacy may interact with emotional burden to influence both attitudes and day‑to‑day self‑management.
The knowledge, attitude, and practice (KAP) survey serves as a valuable diagnostic tool in healthcare research, operating on the fundamental principle that knowledge influences attitude, which subsequently shapes behaviors.14 The KAP framework has been widely used to assess patient understanding and behaviors in chronic diseases, positing that greater knowledge fosters more favorable attitudes and, in turn, more adaptive health‑related practices. For MM patients, studies have shown that improved disease knowledge and understanding significantly influence treatment decision-making and adherence.15 Patient education has been demonstrated to enhance treatment compliance and self-management behaviors, ultimately leading to better clinical outcomes.1,16 Although KAP research has been conducted in various cancer populations, studies specifically targeting MM patients remain limited. Current evidence is largely derived from investigations of healthcare professionals’ knowledge and practices related to MM, while patient-level understanding and management behaviors have been comparatively underexplored.8 Previous KAP studies among healthcare professionals have provided important insights into their MM-related knowledge, attitudes, and clinical practices.17,18 In the context of MM, however, this linear sequence may be challenged by treatment toxicity, prognostic uncertainty, and the need for repeated therapeutic decisions over a prolonged disease course. Patients who are more informed may also be more aware of relapse risk, adverse effects, and limitations of available therapies, which could engender ambivalence, anxiety, or more critical attitudes despite higher levels of knowledge. Consistently, further clinician-focused research has reported substantial variability in MM awareness and practice patterns, highlighting the need to examine patient perspectives more directly.17,18 For instance, a study in the Enshi Region assessed medical staff’s knowledge, attitude, and practice regarding MM, revealing moderate knowledge, neutral attitudes, and proactive practices among healthcare providers.19 Similarly, a global survey on clinicians’ attitudes and practices toward measurable residual disease (MRD) in MM indicated varied clinical practices and treatment decisions influenced by MRD measurement.20 These studies underline the existing gap in understanding patient-specific perspectives on MM management. The complexity of MM treatment, including combination therapies and potential complications, makes patient education and self-management particularly crucial.21 Given the projected increase in the MM burden in China and the complexity of its management, understanding patients’ KAP becomes increasingly crucial for developing effective patient education and support strategies. Moreover, the prolonged and often expensive nature of contemporary MM therapy exposes many patients to financial toxicity, which has been linked to lower treatment satisfaction and may compromise adherence. The cumulative effects of treatment‑related fatigue, symptom burden, and financial strain may foster ambivalence or negative attitudes toward therapy, even among patients with good informational understanding. These factors suggest that the conventional assumption that greater knowledge uniformly translates into more positive attitudes and behaviors may not hold in this setting.22
Thus, while the KAP framework offers a useful starting point for conceptualizing patient behavior, its assumptions cannot be taken for granted in oncology. The relationships among knowledge, attitudes, and practices in multiple myeloma are likely to be shaped by dynamic factors such as disease stage, prior treatment experience, symptom burden, and perceived prognosis, which may attenuate, modify, or even reverse the expected direction of associations. Therefore, this study aims to assess the knowledge, attitude, and practice of MM patients in China. To move beyond purely descriptive comparisons, we therefore employed structural equation modeling (SEM) to examine how knowledge, attitudes, and practices are interrelated within this complex clinical context, rather than presupposing a simple unidirectional pathway. This approach allows us to test whether higher knowledge is consistently associated with more positive attitudes and practices or whether, as might be expected in a setting marked by therapeutic complexity and prognostic ambiguity, more nuanced and potentially counterintuitive patterns emerge. Specifically, we hypothesized that: (i) knowledge would positively influence attitude; (ii) knowledge would positively influence practice; and (iii) knowledge would exert an indirect positive effect on practice via attitude. Given the biological and psychosocial complexity of multiple myeloma, we also recognized that the canonical KAP sequence might not hold uniformly, and we therefore used structural equation modeling to empirically test both the expected and potentially non‑linear relationships among these constructs.
Methods
Study Design and Participants
This cross-sectional study was conducted at Ruian People’s Hospital between August and November 2024, focusing on patients diagnosed with MM. Ethical approval for the study was granted by the Medical Ethics Committee of Ruian People’s Hospital (Approval Number: YJ2024127), and informed consent was obtained from all participants prior to data collection.
Participants were eligible for inclusion if they met the following criteria: (1) aged 18 years or older; (2) diagnosed with MM according to the Guidelines for the Diagnosis and Management of Multiple Myeloma in China (2022 Revision);23 and (3) fully conscious and possessing adequate cognitive ability to comprehend and complete the questionnaire.
During the study period (August-November 2024), all patients with a confirmed diagnosis of MM who attended the hematology outpatient clinic or were hospitalized in the hematology wards and met the eligibility criteria were approached consecutively by trained research staff. Consecutive recruitment of all eligible patients during the defined period was used to minimize selection bias. A screening log was maintained, recording the number of patients screened, approached, and included, as well as reasons for non‑participation when provided (eg., lack of time, feeling unwell). Patients who refused to participate or withdrew consent at any stage of the study were excluded.
Questionnaire
The questionnaire was developed based on the Guidelines for the Diagnosis and Management of Multiple Myeloma in China (2022 Revision) and the Summary of the Best Evidence for Home Self-Management in Patients with Multiple Myeloma.24 An initial item pool was generated to cover key domains of disease‑related knowledge (diagnosis, complications, treatment, follow‑up), attitudes toward disease and treatment, and self‑management practices. Content relevance and clarity were reviewed by a multidisciplinary expert panel comprising two hematologists, two oncology nurses, and one clinical pharmacist with experience in multiple myeloma care. Panel members independently rated each item for importance and comprehensibility, and items were refined through iterative discussion to improve wording and avoid ambiguity, following established recommendations for content validation of health questionnaires.
A pilot test was conducted in 34 patients with multiple myeloma to evaluate the feasibility, acceptability, and internal consistency of the questionnaire. Participants were asked to comment on item clarity and length, and minor wording adjustments were made to improve comprehensibility based on their feedback. The overall scale demonstrated excellent internal consistency in the pilot (Cronbach’s α = 0.947), supporting the reliability of the instrument for use in the main study, although we acknowledge that internal consistency alone does not establish construct validity.
The finalized questionnaire (Supplementary Questionnaire), presented in Chinese, consisted of four sections: demographic information, knowledge, attitude, and practice dimensions. The demographic section collected data on age, gender, residence, education level, occupation type, household monthly income per capita, duration of MM diagnosis, time from symptom onset to diagnosis, first-visit department, and whether the patient was newly diagnosed or experiencing a recurrence. Residence was classified as rural, urban, and suburban based on the official government categorization of the patients’ primary residence. Education was categorized according to the standard Chinese school system (primary, middle, high/technical, associate, bachelor’s or above) to reflect meaningful gradients in health literacy and socioeconomic status, and to remain comparable with prior Chinese hematologic malignancy and KAP studies that demonstrate better outcomes and knowledge among patients with tertiary education. Monthly household income was grouped into four bands (<2000; 2000–4999; 5000–9999; ≥10,000 RMB), reflecting commonly used thresholds separating very low, lower-middle, middle, and higher income strata in China, and mirroring income categorizations applied in previous Chinese KAP and hematologic malignancy research. Occupation type was categorized as long-term stable employment, temporary work, freelancer, unemployed, retired, or other, reflecting standard and non-standard forms of employment recognized in contemporary Chinese labor research. These categories distinguish levels of job stability, income security, and social protection, which are expected to influence patients’ time availability, financial capacity, and access to health services, and thus their knowledge, attitudes, and practices regarding MM. Disease duration was categorized as <1 year, 1–3 years, 3–5 years, and >5 years to reflect key phases of the multiple myeloma care trajectory in China (ie., newly diagnosed, early post-treatment, intermediate, and long-term survivorship), consistent with contemporary survival patterns reported in Chinese MM cohorts. The first-visit department was the department where the patient was initially referred to for his/her symptoms.
The knowledge dimension comprised 11 items, each rated on a three-point scale: “Understand” (2 points), “Partially understand” (1 point), and “Do not understand” (0 points), with a total possible score ranging from 0 to 22. The attitude dimension included 10 items measured on a five-point Likert scale, with positively worded items scored from “Strongly agree” (5 points) to “Strongly disagree” (1 point). Negatively worded items were reverse-scored to maintain consistency. After reverse scoring, higher attitude scores represented more positive attitudes toward disease management. This section had a total score range of 10 to 50. The practice dimension contained 10 items, assessed on a scale from “Never” (1 point) to “Always” (5 points), yielding a total score range of 10 to 50. Participants scoring above 70% of the total possible points in the KAP dimensions were classified as demonstrating good knowledge, positive attitude, and effective practice, respectively.25 In addition, a trap question, “20+20=50,” was included, and those who answered incorrectly were considered to have submitted invalid questionnaires.
Questionnaire Distribution
To enhance accessibility and reduce non‑response, a mixed‑mode administration strategy was employed, including paper‑based, online self‑administered, and interviewer‑assisted completion. The content, question order, and response options were identical across paper and online formats, and the same instruction script was used for all participants to ensure procedural consistency across modes. A standardized written instruction sheet was provided for all modes, and research staff used a uniform verbal script to introduce the study and explain how to complete the questionnaire. For patients with limited literacy or visual difficulties, trained research staff or accompanying family members read each item verbatim and provided neutral clarification of wording when necessary, without rephrasing questions or suggesting answers. They were instructed not to offer examples, interpretations, or opinions that could influence responses, in line with recommendations to minimize interviewer bias in survey research. Once participants fully comprehended the content, they were given the option to complete the survey online by scanning a QR code via the WeChat platform. For other patients, the questionnaire was distributed online by sharing the survey link through WeChat and official institutional WeChat accounts. This approach enabled participants to conveniently access and complete the questionnaire through the provided link. Questionnaires containing abnormal information, such as age below 18 or above 100 years, or exhibiting logical inconsistencies, were considered invalid. Participants with missing data on any KAP item or key covariate were excluded from the corresponding analysis.
Sample Size Calculation
The sample size for this cross-sectional study was calculated using the standard formula for estimating proportions:26 n = (Z2 × p × (1 - p)) / d2, where n represents the required sample size, Z is the Z-score for a 95% confidence level (1.96), p is the estimated prevalence of the outcome of interest (assumed to be 0.5 to maximize variability), and d is the margin of error, set at 0.05. Substituting these values into the formula, the minimum required sample size was determined to be 384 participants. To account for a potential 10% non-response or invalid data rate, the final target sample size was set at 427 participants to ensure sufficient statistical power.
In addition to the proportion‑based calculation for descriptive analyses, we considered the suitability of the achieved sample size (N = 442) for SEM. The specified model included three latent constructs (knowledge, attitude, and practice) indicated by 31 observed items, along with several exogenous observed variables (eg., disease duration, first‑visit department, education). This yields a ratio of cases to estimated parameters and to indicator variables that is consistent with commonly cited guidelines for SEM, which generally recommend total samples of at least 200 participants and ratios of approximately 5–10 participants per estimated parameter or ≥ 10 participants per indicator variable for models of moderate complexity. Simulation studies also suggest that, under conditions of reasonably strong factor loadings and reliable indicators, sample sizes in the range of 300–450 can provide adequate power and stable solutions for models of similar complexity.27 Nevertheless, we acknowledge that these rules of thumb do not replace an a priori SEM‑specific power analysis and that our ability to detect very small effects may be limited.
Statistical Methods
Data analysis was performed using SPSS version 22.0 (IBM Corp., Armonk, NY, USA) and STATA version 18.0 (StataCorp, College Station, TX, USA). Continuous variables were presented as mean ± standard deviation (SD), and the normality of continuous variables was assessed using the Shapiro–Wilk test. For normally distributed data, independent sample t-tests and one-way analysis of variance (ANOVA) were employed, while for non-normally distributed data, the Mann–Whitney U-test and Kruskal–Wallis test were utilized. Categorical variables were expressed as frequencies and percentages (n [%]). Spearman correlation analysis was conducted to examine the correlation among KAP scores. Because all variables were measured at a single time point in this cross‑sectional study, the SEM was used to evaluate the plausibility of these hypothesized directional relationships and to explore potential direct and indirect pathways within the KAP framework, rather than to establish causal effects or temporal ordering among the constructs. SEM was utilized to test the following hypotheses: (H1) knowledge directly influences attitude, (H2) knowledge directly influences practice, and (H3) knowledge indirectly influences practice through attitude. The model was estimated using maximum likelihood (ML) applied to the covariance matrix. We acknowledge that the underlying KAP items are ordinal Likert‑type measures and that ML estimation under multivariate normality assumptions may be suboptimal for strictly ordinal data; accordingly, the SEM results should be interpreted as approximate and exploratory. Model fit was assessed using the Root Mean Square Error of Approximation (RMSEA), Standardized Root Mean Square Residual (SRMR), Tucker-Lewis Index (TLI), and Comparative Fit Index (CFI). To minimize model overfitting, a theoretically specified model was first tried and then compared with more parsimonious alternative models by removing non‑significant paths and re‑estimating the model. Model selection was based on theoretical plausibility and global fit indices (CFI, TLI, RMSEA, and SRMR), with particular attention to avoiding overly complex models relative to the sample size. Sensitivity analyses were conducted by testing alternative path structures and reduced models to assess the robustness of key associations. A two-sided p-value of less than 0.05 was considered statistically significant.
Results
A total of 502 questionnaires were collected. The following cases were excluded: 4 cases without informed consent, 5 cases with outlier age values (17, 100, 108, 108, 117), and 51 cases with logical errors, including incorrect responses to the trap question, resulting in 442 valid responses for analysis. The internal consistency was high across the total scale and its subscales, with Cronbach’s α coefficients of 0.9104 for the total scale. The total scale’s KMO value was 0.9346.
Basic Information
Among the 442 patients with MM who participated in this study, 222 (50.2%) were aged 65 years and above, 226 (51.1%) were male, 259 (58.6%) resided in rural areas, 131 (29.6%) were retired, 151 (34.2%) had the disease for 1–3 years, 247 (55.9%) had their first visit in the hematology department, and 298 (67.4%) were newly diagnosed. Following their diagnosis with MM, 337 (76.24%) received MM medication (including chemotherapy). Regarding complications, 197 (44.57%) had been diagnosed by a doctor as having an infection (including herpes zoster virus infection), and 148 (33.48%) had been diagnosed by a doctor as having a bone disease (fracture, etc). The mean KAP scores were 13.70 ± 5.69 (range: 0–22), 32.90 ± 2.89 (range: 10–50), and 40.12 ± 6.89 (range: 10–50), respectively. Based on the predefined 70% threshold, the mean knowledge score was 62.3%, attitude 65.8%, and practice 80.2%, indicating insufficient knowledge, slightly negative attitudes, and generally active practices overall (Table 1).
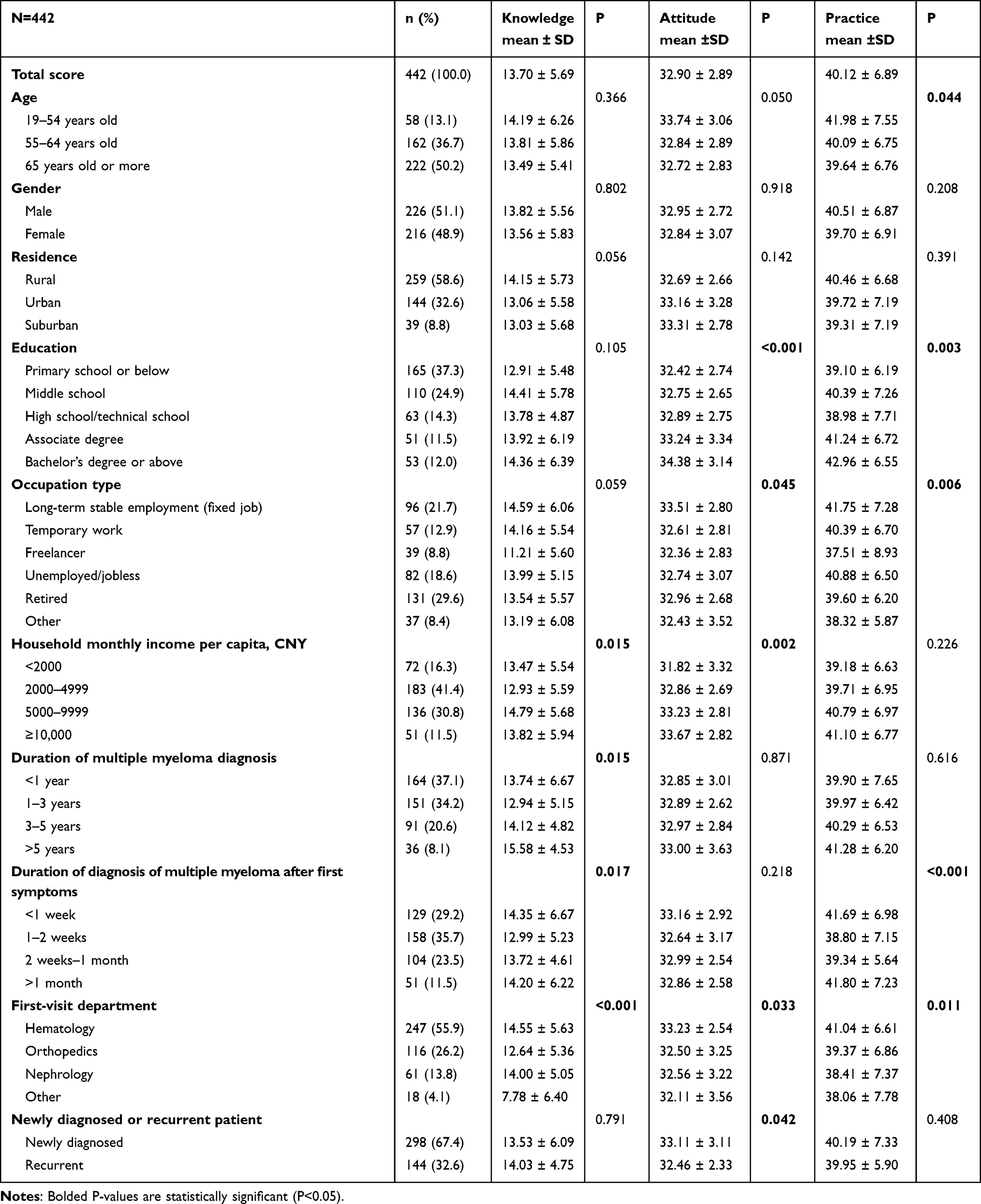 |
Table 1 Basic Characteristics |
Distribution of Responses to KAP
Inspection of item‑level distributions showed no evidence of complete floor or ceiling effects for the knowledge and attitude items; although mean practice scores were relatively high, several practice items (eg., participation in MM management courses, daily monitoring of symptoms, engagement in physical exercise) demonstrated substantial variability, indicating that important gaps remained despite overall favorable practice levels.
The distribution of knowledge dimensions showed that the three questions with the highest percentage of participants choosing the “Do not understand” option were “Venous thromboembolism is one of the major complications of MM.” (K4) with 20.1%, “Patients with MM should have regular follow-ups, and remote consultations through the internet can be utilized.” (K11) with 19.9%, and “Autologous hematopoietic stem cell transplantation is a common treatment method for multiple myeloma.” (K5) with 19.5% (Table 2).
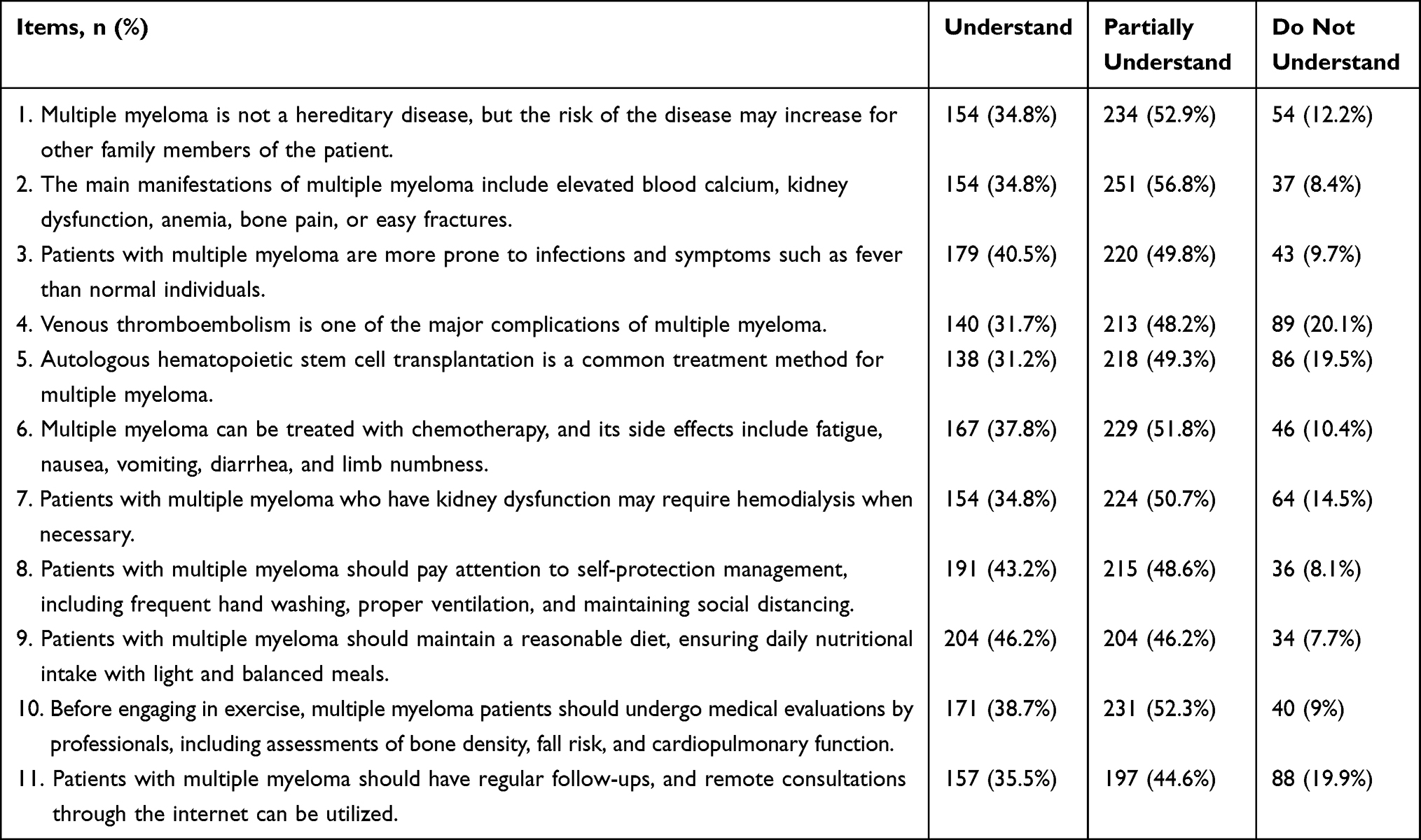 |
Table 2 Distribution of Knowledge Dimension Responses |
Responses to the attitude dimension showed that 38% strongly agreed and 52.9% agreed that MM has caused a significant negative impact on their life (A1), 34.8% strongly agreed and 53.8% agreed that they feel anxious about the economic burden caused by the disease (A8), and 21.9% strongly agreed and 48.2% agreed that they find it difficult to accept chemotherapy during the course of the disease (A6) (Table 3).
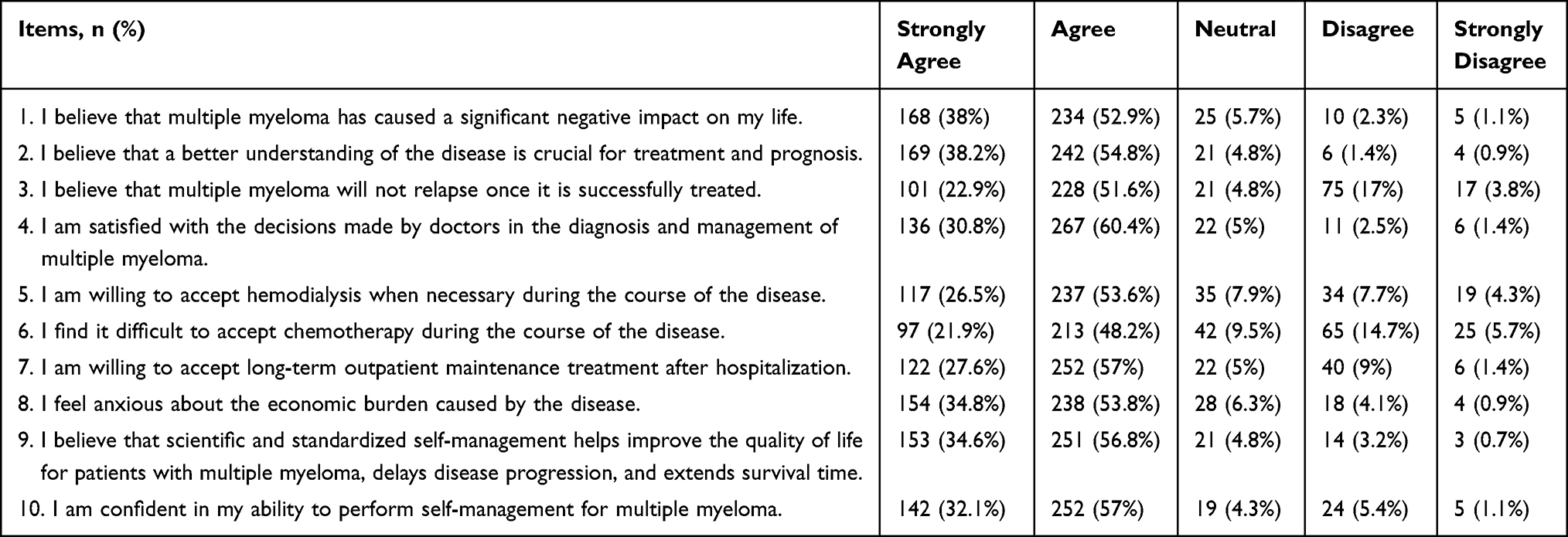 |
Table 3 Distribution of Attitude Dimension Responses |
Responses to the practice dimension showed that 16.1% occasionally and 5.9% never participate in courses on managing MM (P9), 13.3% occasionally and 3.2% never monitor symptoms related to venous thrombosis daily (P3), and 9% occasionally and 2.9% never engage in appropriate physical exercise as guided by a professional (P7) (Table 4).
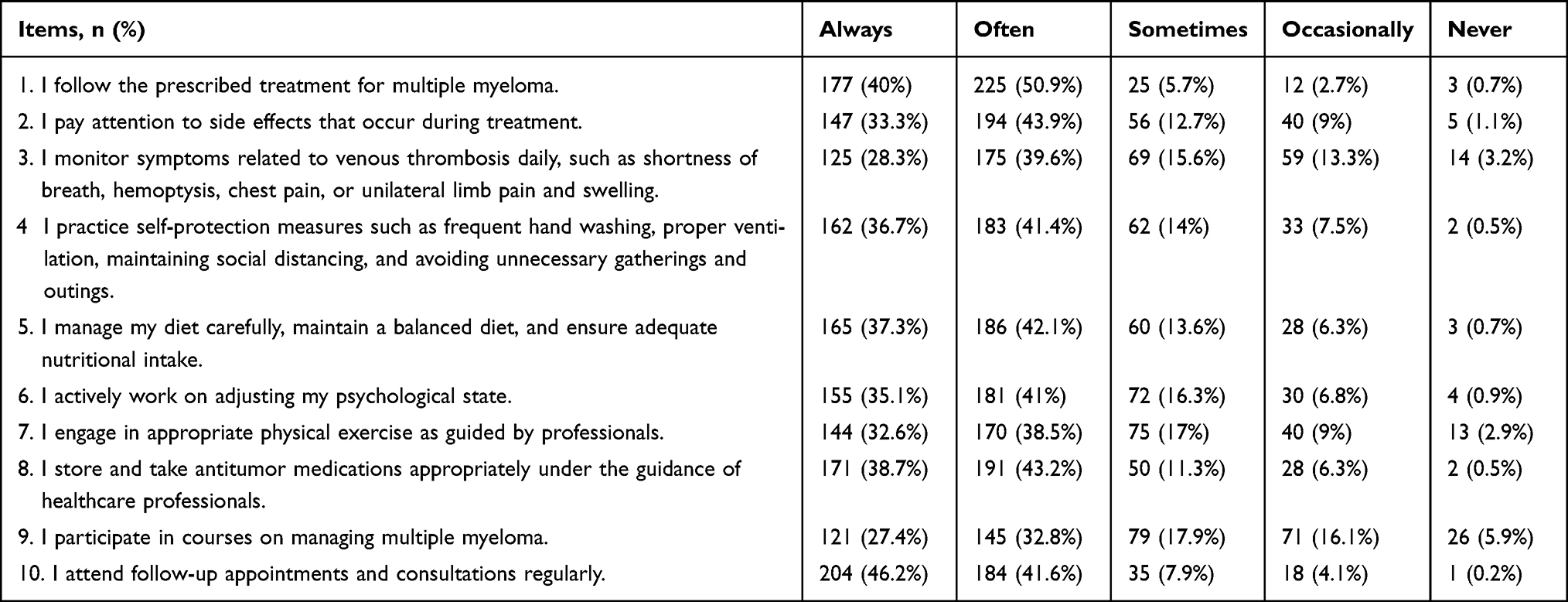 |
Table 4 Distribution of Practice Dimension Responses |
Consistently higher KAP scores were observed in participants who first visited the hematology department vs. non-hematology departments. There was also a significant difference in the attitude-practice correlation between the two subgroups (Table S1).
Correlation Analysis of KAP
Further correlation analysis revealed positive correlations between knowledge scores and attitude scores (r = 0.339, P < 0.001), as well as between knowledge scores and practice scores (r = 0.493, P < 0.001). Additionally, attitude scores were positively correlated with practice scores (r = 0.463, P < 0.001) (Table 5). However, although the bivariate Spearman correlation suggested a positive association between knowledge and attitude, the SEM path analysis showed that knowledge exerted a negative direct effect on attitude after adjustment for other variables.
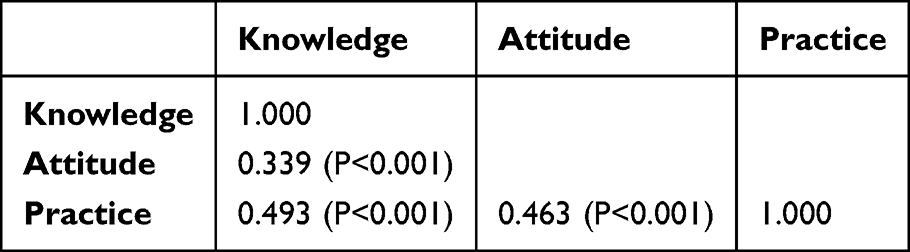 |
Table 5 Spearman Correlation Analysis |
Interactions Between KAP and Other Factors
The fitting indices of the initial SEM model (RMSEA = 0.074; SRMR = 0.065; TLI = 0.806; CFI = 0.820) met the respective threshold values, but were borderline (Table S2). After removing non‑significant paths and re‑estimating the model, the final SEM demonstrated acceptable but borderline fit to the data (RMSEA = 0.071; SRMR = 0.068; TLI = 0.814; CFI = 0.828) (Table S3). The SEM results of the original model are shown in Table S4 and Figure S1. In the final model, SEM analysis showed that the duration of diseases (β = 0.097, P = 0.047) and first-visit department (β = −0.198, P < 0.001) were directly associated with knowledge. Knowledge (β = −0.554, P < 0.001) was directly associated with attitude. Knowledge (β = 0.512, P < 0.001), attitude (β = −0.628, P < 0.001), and education (β = 0.091, P = 0.016) were directly associated with practice. Meanwhile, the first-visit department (β = 0.110, P < 0.001) was indirectly associated with attitude. Knowledge (β = 0.348, P < 0.001), duration of diseases (β = 0.050, P = 0.050), and first-visit department (β = −0.102, P < 0.001) were indirectly associated with practice (Table S5 and Figure 1). The knowledge-attitude path persisted across models in which potentially influential covariates were removed, suggesting that the association is not solely driven by model complexity; however, the attenuation of the effect in some specifications indicates that it should be interpreted with caution (Tables S6, S7 and Figure S2).
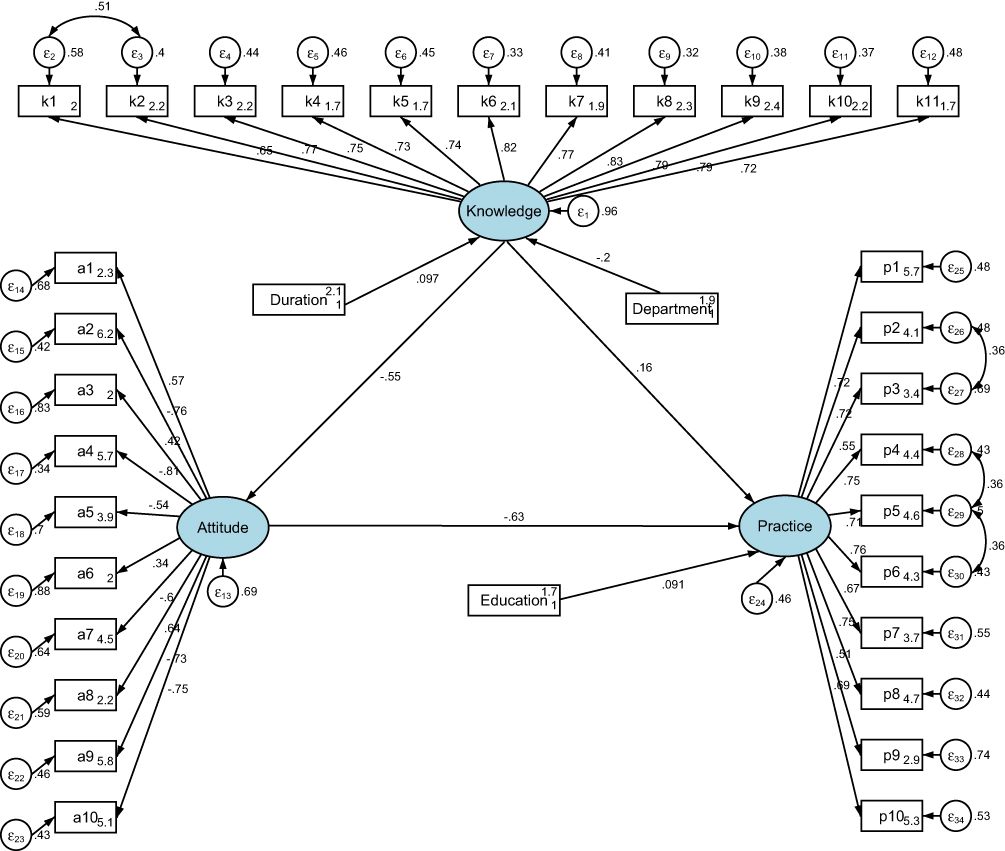 |
Figure 1 Structural equation modeling of the final model. Oval shapes represent latent variables. The measured variables are drawn in rectangular shapes. The circles with the caption starting with “e” indicate measurement errors in each observed variable. Solid straight lines refer to direct effects, while curved solid lines represent indirect effects. Each number on the arrows indicates an individual standardized regression coefficient of each dependency. |
Discussion
Patients with MM exhibited insufficient knowledge and slightly negative attitudes. Although mean practice scores were relatively high, important gaps persisted in key behaviors. This study suggests priority areas and target groups for educational initiatives, but it does not directly assess the impact of specific educational methods. Educational strategies should therefore be considered as hypotheses for future interventional research. This study extends the limited literature on patient‑level KAP in MM by integrating knowledge, attitudes, and practices within a multivariable structural framework. While KAP surveys are well established in public health and chronic disease research, their application to a biologically complex, relapsing hematologic malignancy remains rare, and few prior studies have formally modeled interrelationships among KAP domains in this context. Our findings should therefore be viewed as hypothesis‑generating rather than definitive, providing an initial empirical exploration of how informational, attitudinal, and behavioral dimensions may interact in patients with MM.
Previous research has consistently shown that patients with chronic and complex diseases often lack an adequate understanding of their condition, which can hinder effective disease management and adherence to treatment plans.28,29 In this study, many patients also demonstrated limited awareness of MM-specific complications and treatments. For instance, a considerable proportion of patients lacked knowledge about venous thromboembolism as a major complication and were unfamiliar with common treatments such as autologous hematopoietic stem cell transplantation. Similar gaps in disease knowledge have been reported in studies on other hematological malignancies, where patients’ limited understanding directly affected their ability to recognize symptoms and adhere to prescribed treatments.30,31 These findings underscore the urgent need for more effective patient education strategies tailored to the complexities of MM. Additionally, patients diagnosed in specialized hematology departments demonstrated higher knowledge levels compared to those diagnosed in other departments, such as orthopedics or nephrology. This discrepancy highlights inconsistencies in patient education across medical specialties, a challenge similarly noted in studies examining disparities in cancer care education across healthcare systems.32,33 These disparities suggest that standardized patient education protocols across departments are necessary to ensure that all patients receive comprehensive and consistent information regardless of their point of diagnosis. Nevertheless, the pattern of knowledge gaps observed in this study is consistent with clinical experience and prior reports indicating that venous thromboembolism and autologous hematopoietic stem cell transplantation are often under‑recognized aspects of MM care among patients. Despite the well‑documented increased risk of blood clots in patients with hematologic malignancies, including multiple myeloma, a substantial proportion of our participants reported limited understanding of thrombosis risk and preventive strategies, underscoring the need to strengthen education on these topics.
At a biological level, multiple myeloma is sustained by a complex bone marrow microenvironment in which malignant plasma cells depend on and reshape their niche. Bone marrow stromal cells, osteoclasts, endothelial cells, and immunosuppressive cell populations provide growth and survival signals (eg., interleukin‑6, insulin‑like growth factors) and foster immune escape, allowing myeloma cells to persist and adapt under therapeutic pressure. Mechanisms such as cell‑adhesion-mediated drug resistance, immune checkpoint upregulation, and T‑cell dysfunction contribute to a form of ecological resilience in which drug resistance is effectively seeded during precursor stages, including MGUS and smoldering myeloma, and becomes clinically evident as the disease evolves and successive therapies are exhausted.4–6 By contrast, patient awareness seldom mirrors this biological complexity. Patients typically encounter myeloma as a sequence of clinical events (diagnosis, response, relapse, treatment change) without direct access to the microenvironmental dynamics that silently anticipate therapeutic failure. This discrepancy between the biological ecosystem sustaining disease persistence and the partial, sometimes fragmented understanding available to patients may help explain why increased knowledge can coexist with, or even amplify, anxiety and ambivalence about treatment, particularly when therapeutic targets are perceived in isolation rather than within the broader context of disease evolution.
The correlation analysis indicated positive associations between knowledge, attitude, and practice, suggesting that enhanced knowledge could support improved health behaviors. However, SEM revealed a more complex pattern, with higher knowledge associated with a more negative attitude despite the positive bivariate correlation. This finding should be interpreted cautiously, given the cross‑sectional design and borderline model fit. Two main mechanisms may explain this discrepancy. First, a statistical explanation: in multivariable modeling, suppressor effects can lead to differences between bivariate and adjusted associations, such that the direction of a relationship changes after accounting for other variables.34 Second, a substantive explanation: greater knowledge may increase awareness of disease severity, relapse risk, treatment burden, and financial toxicity, thereby fostering anxiety or ambivalence despite improved understanding. This is supported by the high proportion of patients reporting anxiety about economic burden (73.6%) and difficulty accepting chemotherapy (70.1%), consistent with the concept of the “burden of knowing” in oncology.35,36 Together, these findings suggest that the negative association between knowledge and attitude reflects the complex psychological impact of disease awareness rather than a simple causal effect, highlighting the need for cautious interpretation and for integrating psychological support into patient education strategies.
Despite these knowledge and attitude challenges, mean practice scores were relatively high, including adherence to prescribed treatments and regular follow-up visits. However, participation in educational programs on disease management was notably low, indicating a disconnect between patients’ knowledge levels and their engagement in comprehensive self-management strategies. This pattern mirrors findings in other chronic disease populations, where patients often comply with basic treatment recommendations but fail to fully engage in preventive or educational activities due to limited awareness or motivational barriers.36,37 Moreover, the negative influence of attitude on health practice, as demonstrated by the SEM analysis, suggests that emotional distress may act as a barrier to consistent self-management behaviors. This observation is consistent with existing research highlighting the role of emotional resilience and psychological support in promoting sustained health behaviors among patients with chronic conditions.38
The observed patterns in KAP should also be interpreted in light of the broader psycho‑oncological context. Prior work has shown that patients with MM frequently experience substantial psychological distress and unmet supportive‑care needs.39 At the same time, low or limited health literacy is common in oncology and has been associated with poorer understanding of cancer information and less favorable outcomes. In our cohort, higher knowledge may coexist with heightened awareness of treatment toxicity, risk of relapse, and financial burden, potentially contributing to more ambivalent or negative attitudes despite better informational scores.11,22 This multidimensional context offers a plausible explanation for the counterintuitive negative association between knowledge and attitude observed in the structural model and underscores the importance of integrating emotional, cognitive, and financial factors when interpreting KAP relationships in MM. Our findings align with patient‑reported outcomes research in MM, which has highlighted the cumulative burden of symptoms, treatment‑related side effects, and financial strain on patients’ quality of life and satisfaction with care.10,11 Positioning KAP constructs alongside these domains may help identify patient subgroups who are both informationally vulnerable and psychosocially burdened, and who might benefit most from tailored supportive and educational interventions.
Disease duration emerged as a significant factor in our analysis, showing direct effects on knowledge and indirect effects on both attitudes and practices. Patients with a longer disease duration demonstrated better disease knowledge, likely due to accumulated experience with symptoms, treatments, and healthcare interactions.40,41 However, this increased knowledge and extended experience with the disease indirectly led to more complex attitudes and practices, suggesting that long-term patients may develop different support needs as they progress through their disease journey.42,43 This finding highlights the importance of providing tailored educational interventions that account for patients’ disease duration and evolving needs throughout their MM journey. For newly diagnosed patients, educational efforts may need to prioritize basic understanding of the disease, treatment intent, and initial regimen, whereas patients with longer disease duration may require more nuanced support focused on managing cumulative toxicity, navigating successive lines of therapy, and addressing fatigue and financial burden. Designing phase‑specific educational and supportive care programs that explicitly account for disease duration could therefore improve alignment between content and patients’ stage‑specific concerns.
Patients whose first visit for myeloma‑related symptoms occurred in orthopedics or nephrology had significantly lower knowledge scores than those initially seen in hematology, highlighting gaps in disease‑specific education at these entry points. This finding suggests a need for standardized referral pathways and educational hand‑offs whereby clinicians in non‑hematology departments (eg., orthopedics managing pathological fractures, nephrology treating myeloma‑related renal impairment) provide clear information about the suspicion of multiple myeloma and promptly refer patients to specialized hematology care, in line with optimal care pathway recommendations. Embedding basic myeloma education and referral checklists into these services, potentially supported by patient navigation programs, may help reduce informational disparities associated with the first‑visit department.
To effectively address these challenges, healthcare providers should implement comprehensive educational interventions that not only deliver accurate medical information but also address the emotional and psychological needs of patients. Educational content should be designed to be accessible and understandable, utilizing diverse delivery methods such as interactive workshops, visual aids, and digital platforms. Importantly, integrating psychological counseling into educational programs could help mitigate the anxiety that may arise from increased disease awareness, fostering a more positive attitude, and improving adherence to self-care behaviors. Similar integrated interventions combining education and psychological support have been successful in other patient populations, leading to better mental health outcomes and improved disease management.44,45 Furthermore, establishing standardized patient education protocols across all departments is essential to eliminate discrepancies in information delivery. Such standardization has proven effective in multidisciplinary cancer care models, where consistent educational practice has led to improved patient engagement and health outcomes.46,47 Educational content should specifically target weak areas identified in this study, including knowledge of venous thromboembolism, autologous stem cell transplantation, and participation in MM management courses.
Addressing socioeconomic disparities is equally critical in enhancing patient knowledge and practice. This study found that patients with lower educational attainment and unstable employment exhibited poorer knowledge and less effective health practices, reflecting broader social determinants of health. Socioeconomic challenges often limit patients’ access to educational resources and healthcare services, ultimately affecting their capacity for effective disease management.48,49 Healthcare systems should prioritize targeted interventions for socioeconomically disadvantaged groups, such as providing free or low-cost educational workshops, developing community outreach programs, and offering financial counseling services. Community-based interventions tailored to underserved populations have been shown to significantly improve disease knowledge and management behaviors in various health contexts.50,51 Consistent with intuitive expectations and prior KAP‑based research in oncology and chronic disease populations, higher knowledge and higher educational attainment were associated with more active self‑management practices in our cohort. These results largely reinforce existing evidence that informational and socioeconomic resources facilitate engagement in recommended behaviors, rather than representing fundamentally new relationships.
Moreover, healthcare providers should explore innovative methods for patient engagement, such as integrating mobile health applications and telemedicine services to deliver personalized educational content and support. These digital tools can help bridge gaps in health literacy and provide ongoing guidance, especially for patients who face logistical challenges in accessing in-person services. Evidence from chronic disease management programs suggests that digital health interventions can improve patient knowledge, self-efficacy, and adherence to treatment regimens.52,53 Additionally, involving family members in educational initiatives may provide patients with essential social support, further encouraging positive health behaviors. Based on these findings, it is recommended to implement phase-specific patient education, integrate psychological counseling into routine care, and promote multidisciplinary collaboration. Digital tools and community-based programs should also be developed to enhance disease understanding and self-management, particularly among disadvantaged populations.
This study has several limitations. First, this study was conducted at a single center, which may limit the generalizability of the findings to other regions, healthcare settings, or populations with different sociodemographic or cultural characteristics. The results should therefore be interpreted as most applicable to populations similar to our study site, and caution is warranted when extrapolating to other contexts. Second, its cross-sectional design prevents the establishment of causal relationships between knowledge, attitude, and practice. In addition, the SEM was estimated using cross‑sectional data, which precludes causal inference and may be subject to residual confounding. Because this was an observational, cross‑sectional study, we were unable to evaluate the effectiveness of any specific educational interventions; any suggestions regarding educational approaches are therefore speculative and intended to guide future research and program development rather than to prescribe particular methods. Third, model fit indices were borderline, suggesting that the specified relationships do not fully capture the underlying structure of the data. Consequently, the negative association between knowledge and attitude should be regarded as tentative and requires confirmation in longitudinal or experimental studies with alternative model specifications. Fourth, another important limitation is the reliance on self‑reported questionnaire data, which is inherently subject to recall bias and social desirability bias. Participants may have over‑reported socially acceptable responses or under‑reported behaviors perceived as undesirable, potentially leading to misclassification of knowledge, attitudes, and practices and biasing the observed associations. In addition, the questionnaire was newly developed for this study, and although it was based on national guidelines and best‑evidence summaries and demonstrated high internal consistency in pilot and main samples, we did not perform formal exploratory or confirmatory factor analysis to establish its latent structure. As a result, the construct validity and dimensional stability of the KAP domains remain incompletely characterized, and the use of structural equation modeling with these latent variables should be interpreted as exploratory. Future research should include more comprehensive psychometric evaluation, including content validity indices, factor analysis, and item‑level discrimination, to strengthen the measurement foundation for latent variable modeling. Although our model incorporates several clinical/contextual variables, including disease duration and first‑visit department, it does not capture key biological and treatment‑related determinants that shape the course and management of MM. Fifth, the study was conducted at a single hospital, which may restrict the generalizability of the findings due to potential differences in patient demographics, healthcare access, or treatment practices across different regions or countries. Sixth, although efforts were made to accommodate patients with low literacy, the use of an online questionnaire may have excluded less digitally literate individuals, potentially introducing selection bias. In addition, our quality‑control procedure excluded 51 questionnaires that contained logical inconsistencies or incorrect responses to the embedded trap question (“20 + 20 = 50”). Although this step was intended to improve data quality, it may have disproportionately excluded older patients or those with lower educational attainment, who may be more likely to misinterpret the trap item or to make inadvertent errors when completing the questionnaire independently. Such differential exclusion could have led to an overestimation of the average knowledge level and may have altered the observed relationships among KAP domains. Future studies should carefully weigh the benefits of quality‑control exclusions against the risk of introducing selection bias, and consider whether alternative approaches (eg., sensitivity analyses including and excluding trap‑question failures) can help evaluate the robustness of the findings. Although we used consecutive recruitment of eligible patients and standardized procedures for mixed‑mode questionnaire administration, we cannot exclude selection bias or residual interviewer influence, particularly for attitude and practice items completed with assistance. These factors may affect the generalizability and internal validity of the findings. Finally, although the KAP items were originally collected on ordinal scales, our SEM treated the domain scores as continuous variables and used maximum likelihood estimation, which does not fully account for the ordinal nature of the underlying data. This choice may affect the accuracy of standard errors and fit indices, and the SEM findings should therefore be interpreted with caution. Future studies should consider SEM approaches tailored to ordinal data, such as robust ML or WLSMV applied to polychoric correlation matrices, particularly when modeling item‑level responses. Future research should aim to externally validate these findings in independent samples and across multiple centers with more diverse patient populations. Multicenter studies using the same measurement instruments and analytic framework would allow assessment of the stability of the factor structure, path coefficients, and overall model fit across settings, thereby strengthening the external validity of the conclusions.
In conclusion, this single-center, cross-sectional study identified insufficient disease-related knowledge and generally less favorable attitudes among patients with multiple myeloma, alongside practice patterns that were relatively favorable for some core behaviors but clearly suboptimal in others (eg., structured education, symptom monitoring, and physical activity). The observed associations among knowledge, attitudes, practices, and clinical/contextual factors (such as first-visit department and disease duration) suggest that both patient-level and system-level determinants may shape self-management in this population, but these relationships are exploratory and cannot be interpreted as causal. Taken together, the findings indicate that tailored, phase-specific educational and supportive strategies may be warranted, ideally integrated into multidisciplinary care pathways that address informational gaps as well as emotional and practical concerns; however, longitudinal and interventional studies in larger, more diverse cohorts are needed to confirm these patterns and to determine which specific approaches are most effective in improving patient experience and outcomes.
Abbreviations
ANOVA, analysis of variance; CFI, Comparative Fit Index; KAP, knowledge, attitudes, and practices; KMO, Kaiser-Meyer-Olkin; MM, multiple myeloma; MRD, measurable residual disease; RMSEA, Root Mean Square Error of Approximation; SD, standard deviation; SEM, Structural Equation Modeling; SRMR, Standardized Root Mean Square Residual; TLI, Tucker-Lewis Index.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethics Approval and Consent to Participate
This work has been carried out in accordance with the Declaration of Helsinki (2000) of the World Medical Association. I confirm that all methods were performed in accordance with the relevant guidelines. The study was granted by the Medical Ethics Committee of Ruian People’s Hospital (Approval Number: YJ2024127), and informed consent was obtained from all participants prior to data collection.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare they have no conflicts of interest in this work.
References
1. Cowan AJ, Green DJ, Kwok M, et al. Diagnosis and management of multiple myeloma: a review. JAMA. 2022;327(5):464–16. doi:10.1001/jama.2022.0003
2. Kyle RA, Gertz MA, Witzig TE, et al. Review of 1027 patients with newly diagnosed multiple myeloma. Mayo Clin Proc. 2003;78(1):21–33. doi:10.4065/78.1.21
3. Liu J, Liu W, Mi L, et al. Burden of multiple myeloma in China: an analysis of the Global Burden of Disease, Injuries, and Risk Factors Study 2019. Chin Med J. 2023;136(23):2834–2838. doi:10.1097/CM9.0000000000002600
4. Dimopoulos MA, Terpos E, Boccadoro M, et al. EHA–EMN Evidence-based guidelines for diagnosis, treatment and follow-up of patients with multiple myeloma. Nat Rev Clin Oncol. 2025;22(9):680–700. doi:10.1038/s41571-025-01041-x
5. Wu Y, Shi X, Yao X, Du X. Biological research on the occurrence and development of multiple myeloma and its treatment. Immun Inflammat Dis. 2023;11(5):e850. doi:10.1002/iid3.850
6. Fairfield H, Falank C, Avery L, Reagan MR. Multiple myeloma in the marrow: pathogenesis and treatments. Ann N Y Acad Sci. 2016;1364(1):32–51. doi:10.1111/nyas.13038
7. Lonial S, Anderson KC. Association of response endpoints with survival outcomes in multiple myeloma. Leukemia. 2014;28(2):258–268. doi:10.1038/leu.2013.220
8. Rajkumar SV. Multiple myeloma: 2020 update on diagnosis, risk-stratification and management. Am J Hematol. 2020;95(5):548–567. doi:10.1002/ajh.25791
9. Riebler A, Held L. Projecting the future burden of cancer: bayesian age-period-cohort analysis with integrated nested Laplace approximations. Biom J. 2017;59(3):531–549. doi:10.1002/bimj.201500263
10. Rowland S, Forbes R, Howell D, et al. Psychosocial and supportive care needs of individuals with advanced myeloma. Can Oncol Nurs J. 2023;33(2):215–222. doi:10.5737/23688076332215
11. Lamers J, Hartmann M, Goldschmidt H, Brechtel A, Hillengass J, Herzog W. Psychosocial support in patients with multiple myeloma at time of diagnosis: who wants what? Psycho-Oncology. 2013;22(10):2313–2320. doi:10.1002/pon.3284
12. Holden CE, Wheelwright S, Harle A, Wagland R. The role of health literacy in cancer care: a mixed studies systematic review. PLoS One. 2021;16(11):e0259815. doi:10.1371/journal.pone.0259815
13. Ryman C, Warnicke C, Hugosson S, Zakrisson AB, Dahlberg K. Health literacy in cancer care: a systematic review. Eur J Oncol Nurs. 2024;70:102582. doi:10.1016/j.ejon.2024.102582
14. Koni A, Taha S, Daifallah A, et al. A cross-sectional evaluation of knowledge, attitudes, practices, and perceived challenges among Palestinian pharmacists regarding COVID-19. SAGE Open Med. 2022;10:20503121211069278. doi:10.1177/20503121211069278
15. Rajkumar SV. Multiple myeloma: 2024 update on diagnosis, risk-stratification, and management. Am J Hematol. 2024;99(9):1802–1824. doi:10.1002/ajh.27422
16. Callander NS, Baljevic M, Adekola K, et al. NCCN Guidelines® insights: multiple myeloma, version 3.2022. J Natl Compr Canc Netw. 2022;20(1):8–19. doi:10.6004/jnccn.2022.0002
17. Nicol JL, Hill MM, Burton NW, Skinner TL. Promoting exercise for patients with multiple myeloma: attitudes and practices of clinical haematologists. J Cancer Survivorship. 2022;16(1):1–8. doi:10.1007/s11764-021-01137-0
18. Pooe AM, Dlova AN, Ntuli ST. Medical practitioners’ knowledge and awareness of multiple myeloma at public hospitals, Gauteng, South Africa. S Afr Family Pract. 2023;65(3). doi:10.4102/safp.v65i1.5644
19. Zou L, Li J, Xiang H, Tan J, Zeng Y. Knowledge, attitude and practice towards multiple myeloma among medical staff in Enshi Region. Sci Rep. 2025;15(1):3406. doi:10.1038/s41598-025-88079-0
20. Derman BA, Jasielec JK, Jakubowiak AJ. Clinician attitudes and practices toward measurable residual disease in multiple myeloma. Br J Haematol. 2020;190(3):470–472. doi:10.1111/bjh.16805
21. Delforge M, Ludwig H. How I manage the toxicities of myeloma drugs. Blood. 2017;129(17):2359–2367. doi:10.1182/blood-2017-01-725705
22. Fiala MA, Lepisto E, Amadi-Mgbenka C, Schulman J, Mulligan G, Cho HJ. Financial toxicity and satisfaction with cancer treatment among patients with multiple myeloma: an analysis of the MMRF’s curecloud initiative. Clin Lymphoma Myeloma Leukemia. 2026;26(2):e254–e260. doi:10.1016/j.clml.2025.10.007
23. Chinese Hematology Association CSoH. Guidelines for the diagnosis and management of multiple myeloma in China (2022 revision). Chinese J Int Med. 2022;61(05):480–487. doi:10.3760/cma.j.cn112138-20220309-00165
24. Han S, Chu H, Ying X, Wang L. Summary of the best evidence for home self-management in patients with multiple myeloma. Chinese Modern Nursing Journal. 2023;29(31):4246–4253.
25. Lee F, Suryohusodo AA. Knowledge, attitude, and practice assessment toward COVID-19 among communities in East Nusa Tenggara, Indonesia: a cross-sectional study. Front Public Health. 2022;10:957630. doi:10.3389/fpubh.2022.957630
26. Tam W, Lo K, Woo B. Reporting sample size calculations for randomized controlled trials published in nursing journals: a cross-sectional study. Int J Nurs Stud. 2020;102:103450. doi:10.1016/j.ijnurstu.2019.103450
27. Wolf EJ, Harrington KM, Clark SL, Miller MW. Sample size requirements for structural equation models: an evaluation of power, bias, and solution propriety. Educ Psychol Meas. 2013;76(6):913–934. doi:10.1177/0013164413495237
28. Padala SA, Barsouk A, Barsouk A, et al. Epidemiology, staging, and management of multiple myeloma. Med Sci. 2021;9(1).
29. Rajkumar SV. Multiple myeloma: 2022 update on diagnosis, risk stratification, and management. Am J Hematol. 2022;97(8):1086–1107. doi:10.1002/ajh.26590
30. Abramson M, Mehdi A. Hematological malignancies and the kidney. Adv Chronic Kidney Dis. 2022;29(2):127–140.e121. doi:10.1053/j.ackd.2022.02.003
31. Li W, Wang F, Guo R, Bian Z, Song Y. Targeting macrophages in hematological malignancies: recent advances and future directions. J Hematol Oncol. 2022;15(1):110. doi:10.1186/s13045-022-01328-x
32. Goodall RJ, Ellauzi J, Tan MKH, Onida S, Davies AH, Shalhoub J. A systematic review of the impact of foot care education on self efficacy and self care in patients with diabetes. Eur J Vasc Endovasc Surg. 2020;60(2):282–292. doi:10.1016/j.ejvs.2020.03.053
33. Condurache CI, Chiu S, Chotiyarnwong P, et al. Screening for high hip fracture risk does not impact on falls risk: a post hoc analysis from the SCOOP study. Osteoporos Int. 2020;31(3):457–464. doi:10.1007/s00198-019-05270-6
34. Chung V, Sun V, Ruel N, Smith TJ, Ferrell BR. Improving palliative care and quality of life in pancreatic cancer patients. J Palliat Med. 2022;25(5):720–727. doi:10.1089/jpm.2021.0187
35. Fortin J, Leblanc M, Elgbeili G, Cordova MJ, Marin MF, Brunet A. The mental health impacts of receiving a breast cancer diagnosis: a meta-analysis. Br J Cancer. 2021;125(11):1582–1592. doi:10.1038/s41416-021-01542-3
36. Arad M, Goli R, Parizad N, Vahabzadeh D, Baghaei R. Do the patient education program and nurse-led telephone follow-up improve treatment adherence in hemodialysis patients? A randomized controlled trial. BMC Nephrol. 2021;22(1):119. doi:10.1186/s12882-021-02319-9
37. Gordon M, Sinopoulou V, Ibrahim U, Abdulshafea M, Bracewell K, Akobeng AK. Patient education interventions for the management of inflammatory bowel disease. Cochrane Database Syst Rev. 2023;5(5):Cd013854.
38. O’Donnell EK, Shapiro YN, Yee AJ, et al. Quality of life, psychological distress, and prognostic perceptions in patients with multiple myeloma. Cancer. 2022;128(10):1996–2004. doi:10.1002/cncr.34134
39. Tuckey N, Iasiello M, Ali K, et al. The unmet psychological needs of people living with multiple myeloma and smouldering myeloma: a review of current approaches and future directions. Clin Lymphoma Myeloma Leukemia. 2025;25(12):e1145–e1159. doi:10.1016/j.clml.2025.09.016
40. Guzdar A, Costello C. Supportive care in multiple myeloma. Curr Hematol Malig Rep. 2020;15(2):56–61. doi:10.1007/s11899-020-00570-9
41. Minnie SA, Hill GR. Immunotherapy of multiple myeloma. J Clin Invest. 2020;130(4):1565–1575. doi:10.1172/JCI129205
42. Bansal R, Rakshit S, Kumar S. Extramedullary disease in multiple myeloma. Blood Cancer J. 2021;11(9):161. doi:10.1038/s41408-021-00527-y
43. Bladé J, Beksac M, Caers J, et al. Extramedullary disease in multiple myeloma: a systematic literature review. Blood Cancer J. 2022;12(3):45. doi:10.1038/s41408-022-00643-3
44. Chan MK, Sharkey JD, Nylund-Gibson K, Dowdy E, Furlong MJ. Social support profiles associations with adolescents’ psychological and academic functioning. J Sch Psychol. 2022;91:160–177. doi:10.1016/j.jsp.2022.01.006
45. Labrague LJ. Psychological resilience, coping behaviours and social support among health care workers during the COVID-19 pandemic: a systematic review of quantitative studies. J Nurs Manag. 2021;29(7):1893–1905. doi:10.1111/jonm.13336
46. Zheng C, Zhong J, Wang Y, et al. Deep learning radiomic analysis of MRI combined with clinical characteristics diagnoses placenta accreta spectrum and its subtypes. J Magn Reson Imaging. 2024;60(6):2705–2715. doi:10.1002/jmri.29317
47. Keller DS, Berho M, Perez RO, Wexner SD, Chand M. The multidisciplinary management of rectal cancer. Nat Rev Gastroenterol Hepatol. 2020;17(7):414–429. doi:10.1038/s41575-020-0275-y
48. Ernstmeyer KE, Christman EI. Adopting open educational resources as an equity strategy. Nurs Educ Perspect. 2023;44(5):306–307. doi:10.1097/01.NEP.0000000000001170
49. Friday VE, Hunt C. Open educational resources: equitable and affordable nursing education. Nurs Educ Perspect. 2023;44(5):303–305. doi:10.1097/01.NEP.0000000000001180
50. Mazzeo G, Bendixen R. Community-Based interventions for childhood trauma: a scoping review. OTJR. 2023;43(1):14–23. doi:10.1177/15394492221091718
51. Seven M, Marie Moraitis A. Community-based interventions designed to optimize health behaviors among cancer survivors: an integrative systematic review. Support Care Cancer. 2022;30(10):8405–8415. doi:10.1007/s00520-022-07097-0
52. Brands MR, Gouw SC, Beestrum M, Cronin RM, Fijnvandraat K, Badawy SM. Patient-Centered digital health records and their effects on health outcomes: systematic review. J Med Internet Res. 2022;24(12):e43086. doi:10.2196/43086
53. Zangger G, Bricca A, Liaghat B, et al. Benefits and harms of digital health interventions promoting physical activity in people with chronic conditions: systematic review and meta-analysis. J Med Internet Res. 2023;25:e46439.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Knowledge, Attitudes and Practices Towards Psoriasis Among Patients and Their Family Members
Zhang X, Du H, Liu X, Liu L, Zhang T
Clinical, Cosmetic and Investigational Dermatology 2024, 17:769-782
Published Date: 3 April 2024
Knowledge, Attitudes and Practices Toward Physical Literacy Among the College Students During COVID-19 School Closure
Ma C, Yue M, Zhu X
Journal of Multidisciplinary Healthcare 2024, 17:1629-1640
Published Date: 15 April 2024
Knowledge, Attitude and Practice of Radiologists Regarding Artificial Intelligence in Medical Imaging
Huang W, Li Y, Bao Z, Ye J, Xia W, Lv Y, Lu J, Wang C, Zhu X
Journal of Multidisciplinary Healthcare 2024, 17:3109-3119
Published Date: 4 July 2024
Knowledge, Attitude, and Practice Toward Varicocele in Patients with Varicoceles: A Cross-Sectional Study in Chinese Patients
Gong P, Shen J, Yang Y, Xue D, Lu H, Zhuang Q, Wang X, Tian Z, Chen Y, Chen C, Cao Y
International Journal of General Medicine 2024, 17:3423-3432
Published Date: 7 August 2024
Knowledge, Attitude, and Practice Towards Rehabilitation in Patients with Breast Cancer: A Cross-Sectional Study
Zhou Y, Lu Q, Yu X
Journal of Multidisciplinary Healthcare 2025, 18:1483-1492
Published Date: 12 March 2025