Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Kinesiophobia in Patients with Chronic Obstructive Pulmonary Disease: A Concept Analysis
Authors Yin H ![]() , Li R
, Li R ![]() , Hu Y
, Hu Y ![]() , Huang L
, Huang L
Received 12 November 2025
Accepted for publication 29 January 2026
Published 10 February 2026 Volume 2026:21 580903
DOI https://doi.org/10.2147/COPD.S580903
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Huifang Yin, Rongrong Li, Yidan Hu, Lihua Huang
Nursing Department, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China
Correspondence: Lihua Huang, Nursing Department, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China, Tel +86 13867129329, Email [email protected]
Background: Kinesiophobia (fear of movement) is a significant barrier to pulmonary rehabilitation and functional recovery in patients with Chronic Obstructive Pulmonary Disease (COPD). Despite its considerable impact on clinical outcomes, this concept currently lacks a unified definition and comprehensive theoretical framework.
Objective: To clarify the concept of kinesiophobia in COPD by identifying its defining attributes, antecedents, and consequences, and to integrate these elements into a cohesive conceptual framework.
Methods: A comprehensive literature search was performed in CNKI, Wanfang, VIP, Web of Science, PubMed, CINAHL, and Cochrane Library databases from inception to April 1, 2025. Following Rodgers’ evolutionary methodology, two researchers independently screened studies and conducted a systematic thematic synthesis.
Results: Twenty-nine studies met inclusion criteria. Kinesiophobia in COPD is characterized by four defining attributes: symptom hypervigilance, maladaptive cognition, complex emotional responses, and behavioral avoidance. These are influenced by sociodemographic, disease-related, and psychological antecedents, and lead to functional decline and reduced quality of life.
Conclusion: This analysis synthesizes a unified conceptual framework that integrates dyspnea-related and pain-related kinesiophobia, addressing a critical gap in the literature. This framework provides the foundation for developing precise assessment tools and mechanism-based interventions tailored to specific fear subtypes, ultimately aiming to disrupt the debilitating cycle of fear and avoidance in COPD.
Plain Language Summary: What was known:
Fear of movement (kinesiophobia) makes exercise and recovery very difficult for patients with chronic obstructive pulmonary disease (COPD). However, research on this problem has been split, looking separately at fear of breathlessness or fear of pain.
What this study adds:
Our research brings these ideas together into one clear framework. This framework helps to explain the key parts, causes, and results of movement fear in COPD.
What this means:
This new understanding is a critical step toward helping healthcare professionals better identify movement fear and create personalized strategies to break the cycle of fear and inactivity, improving patients’ lives.
Keywords: kinesiophobia, chronic obstructive pulmonary disease, concept analysis, fear of movement, symptom catastrophizing, activity avoidance, pulmonary rehabilitation
Introduction
Chronic obstructive pulmonary disease (COPD) represents a major global health challenge, characterized by persistent respiratory symptoms and airflow limitation.1 As the third leading cause of mortality worldwide, COPD imposes a substantial disease burden on healthcare systems.1 Pulmonary rehabilitation, with exercise training as its cornerstone, is universally recommended for COPD management.2,3 However, the effectiveness of this intervention is consistently compromised by low participation and adherence rates.4,5
A critical barrier is kinesiophobia, an excessive, irrational fear of movement that is distinct from related constructs such as general anxiety or isolated dyspnea fear, as it is specifically tied to the anticipation of movement-induced adverse sensations.6 In COPD, this fear initiates a debilitating cycle: activity avoidance leads to physical deconditioning, which worsens respiratory symptoms and further reinforces fear-driven behaviors.7–9 Substantial evidence confirms that kinesiophobia is highly prevalent and a stronger predictor of functional limitation than traditional biomedical indicators.10,11
Despite a growing number of empirical studies, a critical conceptual ambiguity persists. This ambiguity is not merely academic; it has direct, negative practical consequences. It leads to the proliferation of assessment tools with inconsistent psychometric properties and unclear applicability across conditions,12 and the conflation of kinesiophobia with related constructs (eg, exertional dyspnea fear, dyspnea beliefs, activity anxiety) results in definitional overlap and operational blurring.12–14 This lack of clarity impedes the development of precise assessment tools—where instruments designed for pain-related fear may be misapplied to dyspnea-related fear—and leads to intervention mismatch, ultimately hindering the development of effective, targeted management strategies.15
To address this gap, Rodgers’ evolutionary concept analysis (ECA) methodology was selected for this study.16,17 Unlike more static methodological approaches (eg, Walker & Avant), Rodgers’ ECA is specifically designed to analyze dynamic, context-dependent concepts. This is particularly suitable for kinesiophobia in COPD, a chronic and evolving condition influenced by cultural perceptions of disease and physical activity. The ECA approach will allow us to trace the concept’s evolution and synthesize its core attributes within the specific context of COPD.
Consequently, this study aims to systematically clarify the concept of kinesiophobia in COPD by delineating its conceptual boundaries, identifying its core attributes, antecedents, and consequences, and establishing a solid theoretical foundation to advance research and clinical practice.
Methods
Study Design: Rodgers’ Evolutionary Concept Analysis
This study employed Rodgers’ evolutionary concept analysis (ECA) to clarify the concept of kinesiophobia within the context of Chronic Obstructive Pulmonary Disease (COPD).16 The ECA approach was selected because it emphasizes the dynamic, context-dependent nature of concepts that evolve over time through social usage, making it particularly suitable for investigating a complex construct like kinesiophobia, which may be subject to evolving interpretations across disciplines.17
Analytical Procedure and Data Synthesis
The analysis was conducted following the six sequential steps of Rodgers’ evolutionary concept analysis framework,16,18 with the data synthesis being an iterative process involving two researchers working independently and then achieving consensus.
The analytical steps were as follows:
Identifying the Concept and Surrogate Terms: The concept of interest was defined as “kinesiophobia in COPD”, and related expressions (eg, “fear of movement”, “dyspnea-related fear”) were identified.
Selecting the Data Field and Collecting Data: A systematic literature search was conducted across multiple disciplines. Two researchers then independently performed initial coding of the full-text articles to identify all text segments relevant to kinesiophobia.
Identifying Attributes, Antecedents, and Consequences: The initial codes were discussed and grouped into preliminary categories through a process of category refinement. These categories were continuously compared and refined through iterative discussions.
Analyzing Data: The refined categories were synthesized into overarching themes (thematic synthesis), which formed the basis for defining the core elements of kinesiophobia. Regular consensus meetings were held throughout the process to compare interpretations and resolve discrepancies. A third reviewer was consulted to arbitrate any unresolved disagreements.
Identifying a Model Case and Related Concepts: A model case was developed to ground the abstract concept in clinical practice.
Identifying Implications for Future Development: Implications for research and practice were proposed.
Determination of Conceptual Saturation: Conceptual saturation was defined a priori as the point at which no new attributes were identified in three consecutively reviewed articles. An attribute was defined as “new” if it represented a distinct characteristic of kinesiophobia not yet captured by the existing thematic structure. The decision on whether an identified characteristic constituted a “new” attribute was made jointly by the two primary researchers during consensus meetings.
Search Strategy
A comprehensive literature search was conducted across seven electronic databases: PubMed, Cochrane Library, CINAHL, Web of Science, CNKI (China National Knowledge Infrastructure), VIP Database, and Wanfang Database from inception to April 2025. The search terms used were a combination of MeSH terms and free-text words. Boolean logic operators “AND, OR, NOT” were used for comprehensive retrieval. Additional articles were manually retrieved from reference lists. We searched for (“pulmonary disease, chronic obstructive”[MeSH] OR “COPD” OR “COAD” OR “chronic obstructive pulmonary disease” OR “chronic obstructive lung disease” OR “chronic obstructive airway disease” OR “chronic airflow obstruction*”) AND (“kinesiophobia” OR “fear of movement” OR “fear of activity” OR “fear avoidance”).
Inclusion and Exclusion Criteria
The study selection followed predefined criteria:
Inclusion Criteria: (1) Population: Adults (≥18 years) with a clinical diagnosis of COPD; (2) Focus: Studies explicitly addressing the constructs of kinesiophobia (eg, attributes, antecedents, consequences, conceptualization); (3) Language: Publications in English or Chinese.
Exclusion Criteria: (1) Full text unavailable; (2) Duplicate publications; (3) Conference abstracts or proceedings.
Literature Screening Process
The literature screening process was performed independently by two reviewers, with disagreements resolved through discussion or by a third reviewer. The process followed the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. Briefly, of the 637 records identified through database searching, 153 underwent title and abstract screening after deduplication. Subsequently, 76 full-text articles were assessed for eligibility, resulting in the final inclusion of 29 studies. A detailed flow diagram of the selection process is provided in Figure 1.
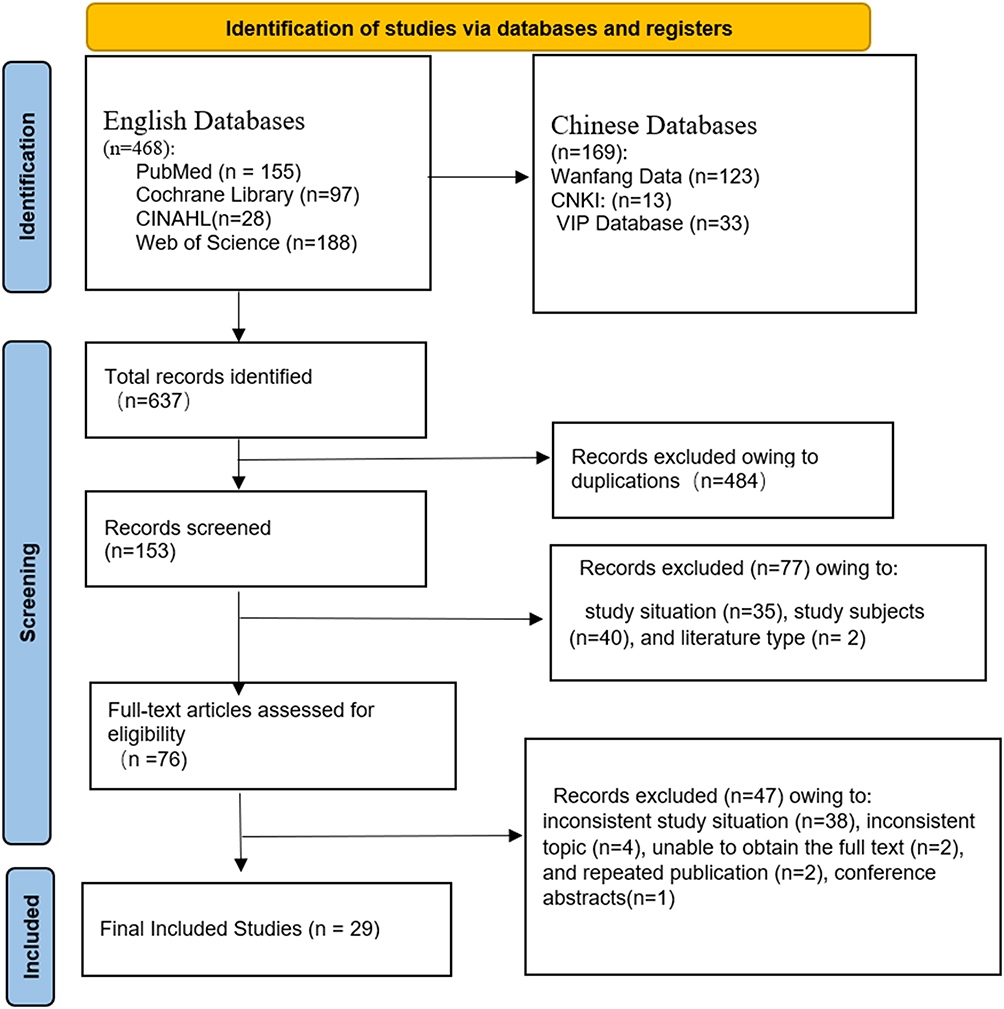 |
Figure 1 PRISMA 2020 flow diagram of the study selection process of the concept analysis. |
Results
In this section, we present the findings of the concept analysis, structured into key components: Study characteristics, Evolution of the concept’s definition and usage, Alternative terms and related concepts, Defining attributes, Antecedents, Consequences, Model cases, Operational definition of kinesiophobia in COPD patients. Additionally, we discuss measurement tools used to assess this concept.
Study Characteristics
Based on the inclusion and exclusion criteria, 29 papers were finally included for conceptual analysis, with contributions from 9 countries. The distribution of studies was as follows: China (n=17), Türkiye (n=4), Belgium (n=2), United States (n=1), Canada (n=1), Germany (n=1), Cyprus (n=1), India (n=1), and Japan (n=1). Most used cross-sectional and quantitative research designs. Study details are provided in Table 1.
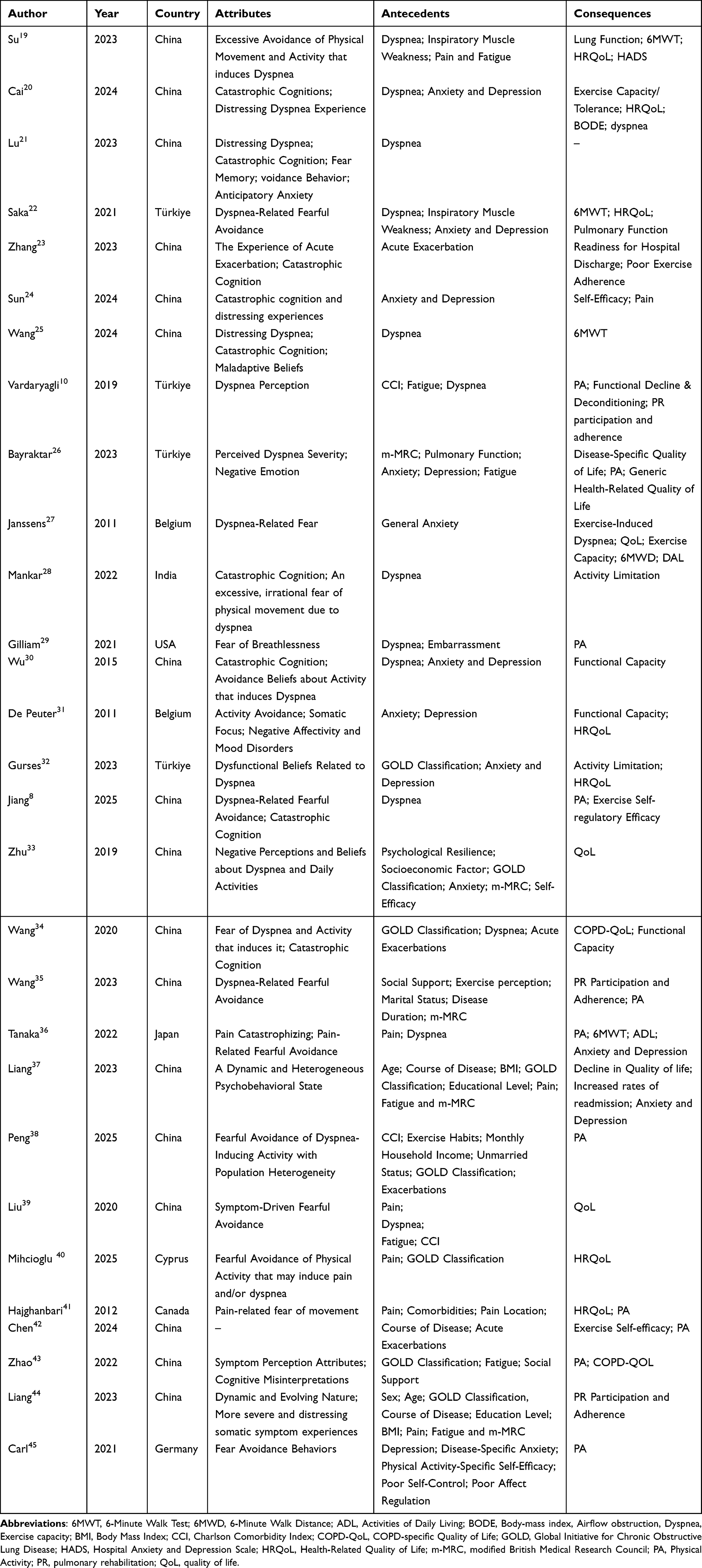 |
Table 1 The General Information of the Included Studies (n=29) |
Evolving Definition and Use of the Concept
The concept of kinesiophobia in COPD has evolved from foundational psychological models, primarily the fear-avoidance model, which established that threat perception—rather than symptom intensity alone—drives disability.46 The term was later coined to describe the “excessive, irrational fear of movement” in chronic pain populations,47 a definition empirically validated as a stronger predictor of disability than pain itself.11
Its translation to respiratory medicine introduced a critical COPD-specific pathway: dyspnea attack → catastrophic interpretation → activity-specific fear → functional decline, thereby identifying catastrophizing as a key mediator.27,31 A significant conceptual expansion was the identification of pain as an independent source of kinesiophobia in COPD, distinct from dyspnea-related fear.41 This evolution underscores a critical conceptual distinction for COPD: kinesiophobia manifests primarily through two subtypes—dyspnea-related (fear of breathlessness/suffocation) and pain-related (fear of musculoskeletal injury). A precise, syndrome-specific definition must acknowledge these distinct threat appraisals and mechanistic pathways to guide targeted interventions.6
Alternative Terms and Related Concepts
Alternative terms refer to lexical variants that describe the same conceptual entity.16 In the context of COPD, the terms “kinesiophobia”, “fear of movement”, and “activity avoidance phobia” are often used interchangeably to describe the phobic avoidance of activities due to fear of inducing dyspnea or other symptoms.10,26,48 Related concepts, while sharing certain attributes, lack full conceptual equivalence. As a critical step in concept analysis, we delineate kinesiophobia from its related concept, activity anxiety. Conceptually, activity anxiety represents a manifestation of general anxiety within the specific context of anticipating physical exertion.49 Distinct from the catastrophic avoidance pattern that is the hallmark of kinesiophobia, activity anxiety manifests primarily as a state of pathological hypervigilance and worry about dyspnea and other symptoms during or in anticipation of physical exertion.27 This critical distinction is supported by prior research. For instance, dyspnea-related fear (a core component of kinesiophobia) has been shown to mediate the relationship between general anxiety (a trait closely linked to activity anxiety) and exercise-induced dyspnea.27 Furthermore, the neurocognitive responses underpinning the anticipatory fear of symptoms (activity anxiety) and the phobic avoidance of activities (kinesiophobia) are understood to involve overlapping yet distinct pathways.50,51
Defining Attributes
Symptom Perception Attributes
Kinesiophobia in COPD is profoundly influenced by the symptomatic interplay of dyspnea and pain. A high prevalence of pain correlates strongly with elevated kinesiophobia,41 and this symptomatic synergy amplifies the fear response. A key attribute is the catastrophic misinterpretation of symptoms: patients frequently mislabel normal exertional dyspnea as a sign of clinical deterioration, reinforcing avoidance behavior.8,27 This is compounded by a shared neurocognitive basis for dyspnea and pain perception, which lowers the threshold for fear activation and facilitates generalized avoidance to both symptom triggers.50,51
Complex Emotional Responses
The emotional dimension of kinesiophobia in COPD is characterized by a pattern of anticipatory anxiety and maladaptive emotional reactivity rooted in the recall of prior dyspnea episodes. This manifests not as a single emotion but as a constellation of negative affective states, including feelings of worthlessness, social isolation, depression, and disease-related stigmatization.31,46,52 A core attribute is the amplification of somatic sensations, whereby this dysregulated emotionality lowers the threshold for detecting and catastrophically interpreting physical sensations such as dyspnea and pain during activity.31,46
This emotional profile fuels a distinct cognitive-affective process: contextual conditioning. Through this process, neutral activity-associated cues become triggers for anticipatory fear, leading to preemptive avoidance behaviors independent of immediate physiological need.50–53 The core of this emotional response can be distilled into two primary driving fears: Activity Aversion: A resentment toward exertion-induced symptom exacerbation. Suffocation Fear: A terror of dyspnea-evoked asphyxiation sensations.52,54
These specific affective drivers are fundamental to the kinesiophobia construct, directly linking emotional experience to avoidance behavior and thereby reinforcing the cyclical nature of the condition.
Cognitive Misinterpretations
The cognitive dimension of kinesiophobia is defined by a constellation of maladaptive illness and symptom appraisals. A fundamental attribute is impaired discriminative ability, wherein patients are unable to differentiate between physiological exertional dyspnea and pathological breathlessness signaling an exacerbation.9,27,31 This perceptual deficit directly fosters a catastrophic misinterpretation of symptoms, characterized by the appraisal of breathlessness as a sign of impending suffocation or life-threatening distress.9,27,31
This cognitive profile is compounded by pain catastrophizing (in patients with comorbid pain) and fundamental misconceptions about disease progression, notably the erroneous belief that “exercise worsens COPD”.36,54,55 These distortions synergistically amplify fear and drive avoidance behaviors.28,35 Conversely, deficits in understanding the therapeutic role of physical activity significantly increase kinesiophobia risk, while awareness of exercise benefits serves as a key protective factor.8,35
The behavioral manifestation of these core cognitive distortions is a pervasive global activity avoidance, which accelerates functional decline through multiple pathways and reinforces a catastrophic illness perception.2,7,35,52 Therefore, correcting these specific cognitive appraisals through targeted education is critical for mitigating kinesiophobia.15,20,25
Subjective Avoidance Behavior
The subjective avoidance behavior inherent to kinesiophobia manifests as a pervasive pattern of activity restriction driven by anticipatory fear and maladaptive cognitions. This behavior is characterized by two primary dimensions: social and behavioral withdrawal, evidenced by the avoidance of essential and social activities,52,53 and the systematic restriction of activity levels, exemplified by the adoption of a sedentary “minimal movement principle” even when physical capacity permits.37,56
A core mechanism sustaining this behavior is negative reinforcement through symptom avoidance, wherein the immediate relief from feared symptoms following activity cessation reinforces the maladaptive belief that inactivity ensures safety.53 This reinforcement establishes a self-perpetuating cycle of avoidance, deconditioning, and symptom exacerbation.2,7,57
Furthermore, the social environment can inadvertently reinforce avoidance through compensatory dependency behaviors, where well-intentioned family support that encourages rest and activity substitution reinforces patient dependency and avoidance patterns.53,56 Addressing these behavioral and environmental reinforcing factors is therefore critical for breaking the cycle of disability.
Antecedents
Antecedents are predisposing factors that create vulnerability to or increase the risk of developing kinesiophobia. The analysis identified three interconnected antecedent domains: Sociodemographic, Physiological & Disease-Related, and Psychological.
Sociodemographic Factors
Key sociodemographic antecedents create vulnerability through limited access to resources and support. Lower educational attainment and socioeconomic status constrain health literacy and access to care, fostering catastrophic illness beliefs.33,37,38 Advanced age compounds physiological decline and reinforces fear conditioning through prolonged disease experience.37,43 Conversely, social support systems, indicated by marital status, serve as a protective factor by providing encouragement and practical assistance for maintaining activity.35,38
Physiological & Disease-Related Factors
This domain encompasses disease-specific burdens that directly fuel fear of movement. The core antecedents are symptom severity—including dyspnea, fatigue, and pain—which provides the aversive experiences that condition fear.10,35,37,41 This is compounded by markers of disease progression, such as longer duration, advanced GOLD stage, frequent exacerbations, and comorbidities, which signal worsening health and reinforce the perceived threat of physical exertion.10,35,37–39,43 Nutritional status abnormalities further reflect and contribute to overall disease burden and deconditioning.37
Psychological Factors
Psychological factors are pivotal antecedents that function as both risk amplifiers and protective resources for kinesiophobia. Negative affective states, particularly anxiety and depression, serve as primary risk factors by lowering the perceptual threshold for symptoms and fostering catastrophic interpretations, which directly amplifies fear.26,33,48 These states initiate a vicious cycle wherein kinesiophobia-driven avoidance worsens physical deconditioning, which in turn heightens affective distress.7,9 Consequently, a dose-dependent relationship exists between the severity of affective symptoms and movement-related fear.48
Conversely, positive psychological resources mitigate kinesiophobia. Exercise self-regulatory efficacy—one’s confidence in managing exercise challenges—shows a significant negative correlation with kinesiophobia severity.33,42,58 Similarly, knowledge of exercise benefits serves as a protective factor, buffering against fear-driven avoidance.35,38
Consequences
Kinesiophobia in COPD initiates a cascade of adverse outcomes that collectively accelerate disease progression and functional decline. The consequences manifest across four interrelated domains, forming a self-perpetuating cycle:
The primary consequence is behavioral avoidance of physical activity, which directly stems from fear-driven movement restriction.8,35 This avoidance triggers progressive physical deconditioning, characterized by functional deterioration and reduced exercise capacity.7,9 Concurrently, significant impairment in health-related quality of life occurs, reflecting the broad psychosocial impact of fear-avoidance behaviors.26,27,31,34 Furthermore, kinesiophobia exacerbates psychological distress, intensifying pre-existing anxiety and depression through a bidirectional feedback loop.7,9,48
These consequences interact dynamically, forming a vicious cycle: kinesiophobia reinforces avoidance, which worsens deconditioning and symptom burden, thereby validating and strengthening the original fear. This cycle encapsulates the core pathogenic mechanism through which kinesiophobia perpetuates disability in COPD.
Measurement Tools
The measurement of kinesiophobia in COPD reflects its conceptual complexity and evolution. The application of generic tools like the Tampa Scale for Kinesiophobia (TSK), particularly its 13-item version (TSK-13), highlights the transdiagnostic nature of fear of movement, adapting a pain-centric tool to COPD.41
In contrast, the disease-specific Breathlessness Beliefs Questionnaire (BBQ) was developed to capture the core COPD-specific attributes of dyspnea-related catastrophic beliefs and activity avoidance.27 The coexistence of these tools operationalizes the conceptual duality of kinesiophobia in COPD—encompassing both general activity-related fear (assessed by TSK) and respiratory-specific threat appraisal (assessed by BBQ). The variation in clinical cut-off scores between studies further underscores the ongoing challenge in establishing a unified diagnostic standard for this concept.12,32
Model Case
The following case describes a fictional COPD patient with kinesiophobia, created to better illustrate the clinical identification and application of the concept.
Mr. Zhang (pseudonym), a 68- year- old, with a 10-year history of COPD, GOLD Stage 3, with 2 exacerbations requiring hospitalization in the past year, was admitted 5 day ago for an acute exacerbation. After initial treatment, his condition is now stable and in the recovery phase. Medical orders have been transitioned from “strict bed rest” to permitting gradual resumption of activity. During hospitalization, he constantly monitored his pulse oximetry (SpO2), remaining intensely anxious even with normal readings (>94%), interpreting any minor respiratory variation as a premonitory sign of severe dyspnea. He equated the normal, mild exertional breathlessness (physiological dyspnea) of the recovery period with the suffocating, life-threatening sensation experienced during the acute exacerbation (Symptom Perception). He existed in a state of persistent high anxiety, particularly pronounced at night, where his excessive focus on breathing severely disrupted his sleep. He developed an intense phobic fear of “dyspnea”, specifically linked to the traumatic memory of the recent exacerbation and its associated “feeling of impending death”. This overwhelming fear became the primary driver dominating his behavior (Emotional Response - Complex Emotions Centered on Anxiety and Fear). He held firm catastrophic beliefs: “Getting out of bed will make me breathless”, “Exercise will worsen my shortness of breath and lead to another hospitalization”. He overgeneralized from his past distressing experience (post-exertion exacerbation) to conclude that “any activity is dangerous”. He lacked knowledge about the benefits of exercise and distrusted assurances that scientifically guided, gradual rehabilitation under medical supervision was safe and beneficial. His wife’s perspective (“exercise will worsen his condition”) further reinforced this misconception (Cognition - Entrenched Catastrophic Beliefs and Misguided Illness Perception). His core behavior was “refusal”: refusal to leave the bed, refusal to attempt any activity, refusal to accept rehabilitation guidance from medical staff. He opted for absolute bed rest, an extreme behavior perceived as “safe”, aimed at avoiding at all costs a recurrence of the feared dyspnea. This behavior directly promoted disuse muscle atrophy and functional decline, setting the stage for increased susceptibility to dyspnea upon future activity, thereby creating a vicious cycle (Behavior - Safety-Seeking and Complete Avoidance).
This case exemplifies the core antecedent (acute exacerbation), the key attributes (catastrophic misinterpretation of dyspnea, complex anxiety, safety-seeking avoidance behavior), and the ensuing consequence (functional deconditioning cycle) of kinesiophobia as defined in this analysis. It serves as a practical illustration of the conceptual framework.
Conceptual Definition
Kinesiophobia in chronic obstructive pulmonary disease (COPD) is conceptually defined as a maladaptive, psychophysiological fear of movement. It is characterized by the dynamic interplay of four core attributes (Figure 2): (1) heightened Symptom Perception, (2) catastrophic Cognitive Misinterpretations, (3) dysregulated Emotional Responses, and (4) pervasive Subjective Avoidance Behavior.
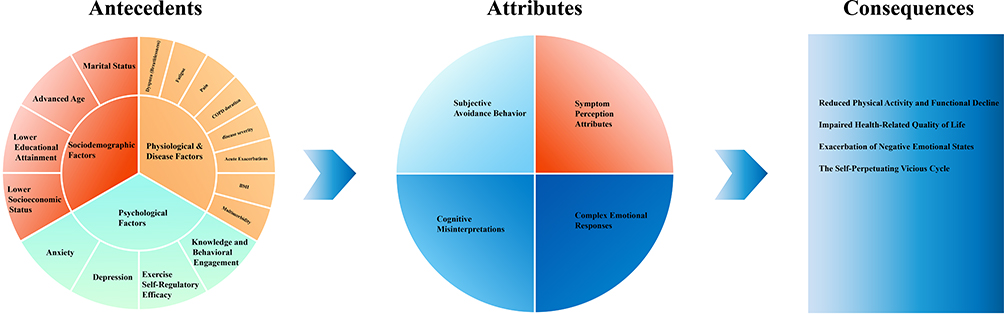 |
Figure 2 The antecedents, attributes and consequences of the concept. |
This fear arises from and is reinforced by a multilevel network of antecedents encompassing sociodemographic, physiological, and psychological factors. Its primary consequences include functional decline, reduced quality of life, and exacerbated psychological distress, which collectively form a self-perpetuating, debilitating cycle that reinforces the initial fear.
Discussion
The primary objective of managing chronic obstructive pulmonary disease (COPD) is to enhance functional capacity and improve overall quality of life.3 A pivotal, yet frequently overlooked barrier to achieving this goal is kinesiophobia (fear of movement). The unique contribution of this concept analysis is the development of a unified conceptual framework that integrates the distinct manifestations of dyspnea-related and pain-related kinesiophobia in COPD. This synthesis addresses a critical gap in the literature, where these subtypes have often been siloed, hindering a comprehensive understanding. By elucidating their shared and unique pathways within a single model, our analysis provides a more nuanced and clinically relevant conceptualization essential for addressing the complex needs of the COPD population.
To achieve this conceptual integration, and guided by Rodgers’ evolutionary method, this analysis delineates four core, interrelated attributes of kinesiophobia in COPD: Symptom Perception, Complex Emotional Responses, Cognitive Misinterpretations, and Subjective Avoidance Behavior. A key advancement offered by this unified framework is its ability to accommodate both dyspnea-driven and pain-driven fear presentations. These attributes are not static but dynamically interact and intensify through lived experience, perpetuating a debilitating fear-avoidance cycle. Shaped by sociodemographic, disease-related, and psychological antecedents, this cycle leads to a cascade of adverse outcomes, including reduced rehabilitation participation, functional decline, and diminished quality of life.2,7,43
The current reliance on assessment tools adapted from other fields, such as the pain-centric Tampa Scale for Kinesiophobia (TSK-13)59 and the dyspnea-specific Breathlessness Beliefs Questionnaire (BBQ),31 operationally reflects the historical conceptual separation of kinesiophobia subtypes. The TSK-13’s limited application in COPD41 and the conceptual non-congruence of the BBQ with the broader construct of kinesiophobia12 highlight a fundamental challenge: the lack of a unified conceptual standard. Our proposed framework directly addresses this limitation by providing the theoretical foundation necessary for developing a comprehensive, disease-specific assessment tool that can reliably evaluate the integrated attributes of kinesiophobia and differentiate between its primary subtypes.
To disrupt the kinesiophobia cycle, interventions must be strategically aligned with the specific attributes they target. Cognitive-Behavioral Therapy (CBT)20 and narrative nursing23 effectively address catastrophic Cognitive Misinterpretations. Mindfulness24 and other adjunctive approaches modulate maladaptive Emotional Responses. Physiotherapeutic techniques like Inspiratory Muscle Training (IMT)19,22 and the Active Cycle of Breathing Techniques (ACBT)60 aim to modify the underlying Symptom Perception. This attribute-targeted approach, organized by our framework, moves beyond a generic intervention model and supports the development of personalized, mechanism-driven treatment strategies. Emerging technologies like Virtual Reality (VR) hold promise for creating immersive environments that simultaneously target multiple attributes.21,25
These insights lead to distinct implications. Clinically, there is an urgent need for routine screening using validated tools and the implementation of caregiver training to prevent the reinforcement of avoidance behaviors.61 For future research, the highest priority is to build upon the unified framework presented here. This includes: (1) developing and validating a new assessment instrument grounded in the integrated attributes; (2) conducting intervention trials that specifically test the efficacy of targeting different attribute combinations, especially for distinct kinesiophobia subtypes; and (3) elucidating the shared and distinct neurocognitive pathways underlying dyspnea-related and pain-related fear.14,50 Ultimately, by providing this consolidated and actionable conceptual framework, which integrates dyspnea- and pain-related fear, this analysis enables a paradigm shift that paves the way for precise and effective interventions to break the cycle of fear and avoidance in COPD.
Limitations
This study has several limitations. First, the literature search was limited to Chinese and English publications, which may have excluded relevant studies in other languages and introduced potential selection bias. The main limitation, however, arises from the considerable methodological heterogeneity among the included studies. Despite strict inclusion and exclusion criteria, the studies varied in design, sample size, measurement tools, and analytical methods. For example, different cut-off values were used to define kinesiophobia, and various instruments were employed to assess related constructs (eg, anxiety, self-efficacy). This variability complicates direct comparison of results and synthesis of the evidence, potentially affecting the strength and consistency of the conclusions. Furthermore, kinesiophobia is still an evolving concept in COPD research, lacking a standardized definition and consensus on its core attributes. Thus, the conceptual analysis presented here is based on the current understanding and may require refinement as the field advances.
Conclusion
In conclusion, this study establishes a unified conceptual framework for kinesiophobia in COPD by integrating the distinct pathways of dyspnea-related and pain-related fear. This synthesis of core attributes, antecedents, and consequences addresses a critical gap in the literature and provides a foundational theory for the field. The framework paves the way for developing precise assessment tools and mechanism-based interventions, ultimately aiming to disrupt the debilitating cycle of fear and avoidance in patients with COPD. As with any conceptual analysis, this model is evolutionary and will be refined by future empirical and clinical research.
Data Sharing Statement
This study is a conceptual analysis and does not involve a primary dataset. The “data” generated and analyzed during this study consist entirely of the conceptual elements derived from the literature review (such as defining attributes, antecedents, consequences, and model cases). All these data are comprehensively presented within the main body of the manuscript and its included tables/figures. No separate supplementary data files are associated with this work.
Acknowledgments
We extend our gratitude to the authors of all the studies included in this review, and the organization that funded our research (the “Double First-Class” Construction Project of Nursing Advantageous and Characteristic Discipline at Zhejiang University, HL2024019). We also thank our colleague, Yunyun Sheng, from the Intensive Care Unit of the First Affiliated Hospital, Zhejiang University School of Medicine, for his valuable assistance in creating the figures for this manuscript.
Funding
The study was supported by the “Double First-Class” Construction Project of Nursing Advantageous and Characteristic Discipline at Zhejiang University (HL2024019).
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Soriano JB, Kendrick PJ, Paulson KR. Prevalence and attributable health burden of chronic respiratory diseases, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Respir Med. 2020;8(6):585–14. doi:10.1016/S2213-2600(20)30105-3
2. Gloeckl R, Schneeberger T, Jarosch I, et al. Pulmonary rehabilitation and exercise training in chronic obstructive pulmonary disease. Dtsch Arztebl Int. 2018;115(8):117–123. doi:10.3238/arztebl.2018.0117
3. Singh D, Agusti A, Anzueto A, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease: the GOLD science committee report 2019. Eur Respir J. 2019;53(5):1900164. doi:10.1183/13993003.00164-2019
4. Xie L, Liu Z, Hao S, et al. Assessment of knowledge, attitude, and practice towards pulmonary rehabilitation among COPD patients: a multicenter and cross-sectional survey in China. Respir Med. 2020;174:106198. doi:10.1016/j.rmed.2020.106198
5. Wang T. Research and practice progress of pulmonary rehabilitation in China and America. Chin Nurs Res. 2020;34(6):1046–1051. doi:10.12102/j.issn.1009-6493.2020.06.028
6. Li S, Zhou QS, He W. Research progress of kinesophobia in patients with chronic obstructive pulmonary disease. Geriatrics Res. 2024;5(5):59–63. doi:10.3969/j.issn.2096-9058.2024.05.012
7. Ramon MA, Ter Riet G, Carsin A, et al. The dyspnoea-inactivity vicious circle in COPD: development and external validation of a conceptual model. Eur Respir J. 2018;52(3):1800079. doi:10.1183/13993003.00079-2018
8. Jiang Z, Li H, Yu L, et al. The relationship between dyspnea-related kinesiophobia and physical activity in people with COPD: a moderated mediation model. Sci Rep. 2025;15(1):9190. doi:10.1038/s41598-025-94108-9
9. Hanania NA, O’Donnell DE. Activity-related dyspnea in chronic obstructive pulmonary disease: physical and psychological consequences, unmet needs, and future directions. Int J Chron Obstruct Pulmon Dis. 2019;14:1127–1138. doi:10.2147/COPD.S188141
10. Vardar-Yagli N, Calik-Kutukcu E, Saglam M, et al. The relationship between fear of movement, pain and fatigue severity, dyspnea level and comorbidities in patients with chronic obstructive pulmonary disease. Disabil Rehabil. 2019;41(18):2159–2163. doi:10.1080/09638288.2018.1459886
11. Crombez G, Vlaeyen JW, Heuts PH, et al. Pain-related fear is more disabling than pain itself: evidence on the role of pain-related fear in chronic back pain disability. Pain. 1999;80(1–2):329–339. doi:10.1016/S0304-3959(98)00229-2
12. Li Z, Feng L, Yang J, et al. A scoping review of assessment tools for fear of movement. J Nurs Sci. 2024;39(20):124–128. doi:10.3870/j.issn.1001-4152.2024.20.124
13. Wu Q, Guo A. Concept and measurement of breathlessness beliefs in patients with COPD. Chin J Nurs. 2015;50(4):454–459. doi:10.3761/j.issn.0254-1769.2015.04.017
14. Cai S, Zhang M, Xiang X, et al. Research progress of dyspnea belief intervention in patients with chronic obstructive pulmonary disease. Chin J Pract Nurs. 2024;40(5):397–401. doi:10.3760/cma.j.cn211501-20230807-00212
15. Wu S, Yan M, Yuan M, et al. Development and validation of the exercise avoidance scale for patients with chronic obstructive pulmonary disease. J Nurs Sci. 2025;40(13):12–15. doi:10.3870/j.issn.1001-4152.2025.13.012
16. Rodgers BL. Concepts, analysis and the development of nursing knowledge: the evolutionary cycle. J Adv Nurs. 1989;14(4):330–335. doi:10.1111/j.1365-2648.1989.tb03420.x
17. Tofthagen R, Fagerstrom LM. Rodgers’ evolutionary concept analysis--a valid method for developing knowledge in nursing science. Scand J Caring Sci. 2010;24 Suppl 1:21–31. doi:10.1111/j.1471-6712.2010.00845.x
18. Rodgers BL, Jacelon CS, Knafl KA. Concept analysis and the advance of nursing knowledge: state of the science. J Nurs Scholarsh. 2018;50(4):451–459. doi:10.1111/jnu.12386
19. Su G, Wang J, Liu Y, et al. Effect of inspiratory muscle training on COPD exercise phobia. Chin J Lung Dis. 2023;16(3):421–423. doi:10.3877/cma.j.issn.1674-6902.2023.03.034
20. Cai S, Yao J, Han M, et al. The effect of cognition in combination with an ACBT on dyspnea-related kinesiophobia in patients with moderate to severe COPD: quasirandomized controlled trial study. Geriatr Nurs. 2024;56:138–147. doi:10.1016/j.gerinurse.2024.01.002
21. Lu X, Niu M, Han Y, et al. Development of a virtual reality-based fear of dyspnea adaptation program for patients with chronic obstructive pulmonary disease. Military Nurs. 2023;40(9):52–55,91. doi:10.3969/j.issn.2097-1826.2023.09.013
22. Saka S, Gurses HN, Bayram M. Effect of inspiratory muscle training on dyspnea-related kinesiophobia in chronic obstructive pulmonary disease: a randomized controlled trial. Complement Ther Clin Pract. 2021;44:101418. doi:10.1016/j.ctcp.2021.101418
23. Zhang D, Qi H, An X, et al. Intervention of narrative nursing on breathlessness beliefs in chronic obstructive pulmonary disease patients. J Clin Med Pract. 2023;27(1):115–119. doi:10.7619/jcmp.20222657
24. Sun Z, Wang Y. Effect of mindfulness based stress reduction training on reducing kinetophobia of COPD patients. Smart Healthcare. 2024;10(25):76–79. doi:10.19335/j.cnki.2096-1219.2024.25.023
25. Wang M, Wan H, Wang Y. Effect of VR technology-assisted cognitive behavioral nursing on dyspnea-related fear in COPD patients. Guizhou Med J. 2024;48(10):1679–1680. doi:10.3969/j.issn.1000-744X.2024.10.061
26. Bayraktar D, Felekoglu E, Ozgen Alpaydin A, et al. Breathlessness beliefs and related factors in male patients with chronic obstructive pulmonary disease. Thorac Res Pract. 2023;24(3):137–142. doi:10.5152/ThoracResPract.2023.22184
27. Janssens T, De Peuter S, Stans L, et al. Dyspnea perception in COPD: association between anxiety, dyspnea-related fear, and dyspnea in a pulmonary rehabilitation program. Chest. 2011;140(3):618–625. doi:10.1378/chest.10-3257
28. Mankar S, Rayas R, Ashok K, et al. Correlation between dyspnea-related kinesiophobia and activity limitation in patients with chronic respiratory diseases. Ind J Resp Care. 2022;11(1):20–23. doi:10.4103/ijrc.ijrc_77_21
29. Gilliam EA, Kilgore KL, Liu Y, et al. Managing the experience of breathlessness with Tai Chi: a qualitative analysis from a randomized controlled trial in COPD. Respir Med. 2021;184:106463. doi:10.1016/j.rmed.2021.106463
30. Wu Q. Dyspnea Beliefs and Their Impact on Functional Status in Patients with Chronic Obstructive Pulmonary Disease. Peking Union Medical College; 2015. doi:10.7666/d.Y2818597
31. De Peuter S, Janssens T, Van Diest I, et al. Dyspnea-related anxiety: the Dutch version of the breathlessness beliefs questionnaire. Chron Respir Dis. 2011;8(1):11–19. doi:10.1177/1479972310383592
32. Gurses HN, Saka S, Zeren M, et al. Validity and reliability of the Turkish version of breathlessness beliefs questionnaire. Physiotherapy Theory and Practice. 2023;39(4):834–839. doi:10.1080/09593985.2022.2027586
33. Zhu X. Current Status and Influencing Factors of Dyspnea Beliefs in COPD Patients. Yangtze University; 2019.
34. Wang Y, Zhang L, Zhu Y, et al. Breathlessness beliefs status and its relation to quality of life in patients with chronic obstructive pulmonary disease. Pract J Cardiac Cerebral Pneumal Vasc Dis. 2020;28(1):70–74. doi:10.3969/j.issn.1008-5971.2020.01.010
35. Wang J, Bai C, Zhang Z, et al. The relationship between dyspnea-related kinesiophobia and physical activity in people with COPD: cross-sectional survey and mediated moderation analysis. Heart Lung. 2023;59:95–101. doi:10.1016/j.hrtlng.2023.02.007
36. Tanaka T, Okita M, Jenkins S, et al. Clinical and psychological impact of chronic pain in people with chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2022;17:893–903. doi:10.2147/COPD.S359223
37. Liang F, Liu M, Yin Y, et al. Investigation on the development trajectories of exercise fear in patients with chronic obstructive pulmonary disease. Chin J Nurs. 2023;58(6):721–726. doi:10.3761/j.issn.0254-1769.2023.06.012
38. Peng L, Xu M, Wang Y, et al. Latent profile analysis of dyspnea-related kinesiophobia in older adults with chronic obstructive pulmonary disease. Heart Lung. 2025;69:241–247. doi:10.1016/j.hrtlng.2024.10.016
39. Liu C, Zhong C, Luo C, et al. Study on the occurrence and related factors of motion phobia in patients with chronic obstructive pulmonary disease. J Xinjiang Med Univ. 2020;43(10):1328–1331. doi:10.3969/j.issn.1009-5551.2020.10.013
40. Mihcioglu S, Malkoc M. The effect of muscle energy technique on pain, kinesiophobia, and quality of life in patients with COPD with chronic pain. Sci Rep. 2025;15(1):3884. doi:10.1038/s41598-025-88304-w
41. Hajghanbari B, Holsti L, Road JD, et al. Pain in people with chronic obstructive pulmonary disease (COPD). Respir Med. 2012;106(7):998–1005. doi:10.1016/j.rmed.2012.03.004
42. Chen H, Cheng X, Chen L, et al. Mediating effect of exercise self-efficacy between kinesiophobia and physical activity in elderly patients with chronic obstructive pulmonary disease. Military Nurs. 2024;41(11):53–56. doi:10.3969/j.issn.2097-1826.2024.11.013
43. Zhao M, Xi F, Yang J, et al. Status quo and influencing factors of breathlessness beliefs in patients with chronic obstructive pulmonary disease. Chin J Mod Nurs. 2022;28(18):2412–2416. doi:10.3760/cma.j.cn115682-20211010-04564
44. Liang F, Liu M, Han H, et al. Identifying patterns of kinesiophobia trajectories among COPD patients: a longitudinal study. Nurs Open. 2023;10(6):3925–3935. doi:10.1002/nop2.1650
45. Carl J, Schultz K, Janssens T, et al. The “can do, do do” concept in individuals with chronic obstructive pulmonary disease: an exploration of psychological mechanisms. Respir Res. 2021;22(1):260. doi:10.1186/s12931-021-01854-1
46. Lethem J, Slade PD, Troup JD, et al. Outline of a fear-avoidance model of exaggerated pain perception—I. Behav Res Ther. 1983;21(4):401–408. doi:10.1016/0005-7967(83)90009-8
47. Kori SH, Miller RP, Todd DD. Kinesiophobia: a new view of chronic pain behaviour. Pain Manag. 1990;1(3):35–43.
48. Farris SG, Abrantes AM, Bond DS, et al. Anxiety and fear of exercise in cardiopulmonary rehabilitation: patient and practitioner perspectives. J Cardiopulm Rehabil Prev. 2019;39(2):E9–E13. doi:10.1097/HCR.0000000000000401
49. Vlaeyen JWS, Crombez G. Behavioral conceptualization and treatment of chronic pain. Annual Rev Clin Psychol. 2020;16:187–212. doi:10.1146/annurev-clinpsy-050718-095744
50. von Leupoldt A, Sommer T, Kegat S, et al. Dyspnea and pain share emotion-related brain network. Neuroimage. 2009;48(1):200–206. doi:10.1016/j.neuroimage.2009.06.015
51. Stoeckel MC, Esser RW, Gamer M, et al. Brain responses during the anticipation of dyspnea. Neural Plast. 2016;2016:6434987. doi:10.1155/2016/6434987
52. Luo YR, Chen MX, Wu S, et al. Daily physical activity in patients living with COPD: A qualitative study. Chin Gen Pract. 2020;23(21):2635–2641. doi:10.12114/j.issn.1007-9572.2020.00.007
53. Kosteli M, Heneghan NR, Roskell C, et al. Barriers and enablers of physical activity engagement for patients with COPD in primary care. Int J Chron Obstruct Pulmon Dis. 2017;12:1019–1031. doi:10.2147/COPD.S119806
54. Wang J, Bai C, Zhang Z, et al. The current status of exercise perception and its influencing factors in elderly patients with chronic obstructive pulmonary disease. Chin J Nurs. 2022;57(1):36–42. doi:10.3761/j.issn.0254-1769.2022.01.005
55. Miao X, Niu M, Han Y, et al. Influencing factors and the pathway analysis of dyspnea-related fear in patients with chronic obstructive pulmonary disease. J Nurs Sci. 2024;39(18):37–41,47. doi:10.3870/j.issn.1001-4152.2024.18.037
56. Zhou D, Niu M, Han Y, et al. Barriers to changing sedentary behavior in patients with chronic obstructive pulmonary disease: a qualitative study. J Nurses Train. 2021;36(22):2085–2089. doi:10.16821/j.cnki.hsjx.2021.22.014
57. Troosters T, Janssens W, Demeyer H, et al. Pulmonary rehabilitation and physical interventions. Eur Respir Rev. 2023;32(168):220222. doi:10.1183/16000617.0222-2022
58. Davis AHT, Figueredo AJ, Fahy BF, et al. Reliability and validity of the Exercise Self-Regulatory Efficacy Scale for individuals with chronic obstructive pulmonary disease. Heart Lung. 2007;36(3):205–216. doi:10.1016/j.hrtlng.2006.08.007
59. Goubert L, Crombez G, Van Damme S, et al. Confirmatory factor analysis of the Tampa Scale for Kinesiophobia: invariant two-factor model across low back pain patients and fibromyalgia patients. Clin J Pain. 2004;20(2):103–110. doi:10.1097/00002508-200403000-00007
60. Bott J, Blumenthal S, Buxton M, et al. Guidelines for the physiotherapy management of the adult, medical, spontaneously breathing patient. Thorax. 2009;64 Suppl 1:i1–i51. doi:10.1136/thx.2008.110726
61. Kakkera K, Padala KP, Kodali M, et al. Association of chronic obstructive pulmonary disease with mild cognitive impairment and dementia. Curr Opin Pulm Med. 2018;24(2):173–178. doi:10.1097/MCP.0000000000000458
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development and Validation of a Multivariable Exercise Adherence Prediction Model for Patients with COPD: A Prospective Cohort Study

Ricke E, Bakker EW
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:385-398
Published Date: 22 March 2023
Effects of Early Pulmonary Rehabilitation on Hospitalized Patients with Acute Exacerbation of Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis
Lu HY, Chen CF, Lee DL, Tsai YJ, Lin PC
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:881-893
Published Date: 15 May 2023
Development of a Pulmonary Rehabilitation Patient Decision Aid for Patients with Chronic Obstructive Pulmonary Disease: Mixed Methods Study
Jiang Y, Guo J, Chen M, Zou X, Sun P, Gao J, Nuerdawulieti B, Wang S
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:1377-1389
Published Date: 12 July 2023
Effects of Pedometer-Based Step-Feedback on Physical Activity of Severe COPD Patients
Tsujimura Y, Akiyama A, Hiramatsu T, Mikawa K, Tabira K
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2277-2287
Published Date: 17 October 2023
Exercise Prescription Training in Chronic Obstructive Pulmonary Disease: Benefits and Mechanisms
Liu S, Yang A, Yu Y, Xu B, Yu G, Wang H
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:1071-1082
Published Date: 15 April 2025