Back to Journals » Patient Preference and Adherence » Volume 20
Intention to Engage in Exercise Rehabilitation Among Patients with Cardiovascular Disease: A Scoping Review
Authors Song Y, Peng L, Wu L, Liu X, Wang Y
Received 31 October 2025
Accepted for publication 13 January 2026
Published 29 January 2026 Volume 2026:20 578094
DOI https://doi.org/10.2147/PPA.S578094
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Yanyan Song, Lishu Peng, Lin Wu, Xue Liu, Yan Wang
School of Nursing, Hebei University, Baoding, Hebei, 071000, People’ s Republic of China
Correspondence: Yan Wang, School of Nursing, Hebei University, No. 342 of Yuhua East Road, Lianchi District, Baoding City, Hebei Province, 071000, People’s Republic of China, Tel +86 13833258628, Email [email protected]
Purpose: This paper compiles the scope of research on exercise rehabilitation intention among patients with cardiovascular diseases and identifies the current landscape, influencing factors, assessment instruments, and intervention strategies related to exercise rehabilitation intention, aiming to inform clinical efforts aimed at encouraging active patient engagement in rehabilitation.
Methods: Eleven Chinese and English databases were systematically searched between the database’s creation and August 28, 2024, under the scoping review methodology. Two researchers independently performed literature screening and data extraction.
Results: A total of 25 studies were included (21 in English, 4 in Chinese), 16 specifically assessed exercise rehabilitation intentions in cardiovascular disease patients, approximately half (8/16) of the cardiovascular disease patients exhibited suboptimal exercise rehabilitation intention. The assessment tools for exercise rehabilitation intentions are diverse, with dimensions primarily focused on willingness and planning. Determinants included psychosocial, disease-related, and sociodemographic factors. Identified intervention strategies included group health education, individual psychological support, and motivational interviewing.
Conclusion: Among cardiovascular disease patients exercise rehabilitation intentions remain inconsistent, as approximately half of the studies indicating medium-to-low average levels, which are influenced by several factors. Therefore, to accurately assess patients’ levels of exercise rehabilitation intention, further research may focus on enhancing the dimensions, reliability, and validity of assessment tools. Exploring multifaceted and varied intervention strategies could potentially improve patients’ exercise rehabilitation intention and compliance.
Keywords: cardiovascular disease, behavioral intention, exercise rehabilitation intention, prevention, scope review
Introduction
Cardiovascular disease(CVD)has emerged as a major public health problem that threatens human life and health.1 In China, CVD morbidity and mortality rates remain persistently high, and it is the primary cause of death for urban and rural residents.2 Research demonstrates that exercise rehabilitation, a core component of cardiac rehabilitation (CR), significantly enhances exercise capacity, endurance in CVD patients, and effectively delays the progression of CVD, improving their long-term prognosis.3–7 All CVD patients without contraindications to exercise rehabilitation should receive exercise-focused CR during the stabilization period.8,9 However, the percentage of patients participating in and adhering to exercise rehabilitation is low, ranging from 19% to 34%.10,11
Exercise rehabilitation intention reflects an individual’s subjective assessment of their willingness or likelihood to engage in future exercise rehabilitation and the degree of effort they plan to exert.12 While physical activity intention emphasizes general willingness to exercise, it primarily targets health-oriented motivations for initiating or maintaining exercise, thereby constituting a different measurement form of the same concept. Moreover, existing literature often utilizes related concepts, such as behavioral change stages and exercise readiness, as surrogate indicators for exercise rehabilitation intention; these concepts are also integrated into the operational definition of this review. According to the Theory of Planned Behavior, behavioral intention reflects a subjective decision-making process before action and constitutes a fundamental component of numerous participation models. Studies confirm the level of exercise rehabilitation intention significantly affects the participation rate and adherence to exercise of patients, which is a key factor in exercise adherence.13–15 This predictive relationship is particularly crucial amid the global shift toward home-based, community-based, and remote rehabilitation models, as the success of these decentralized models heavily depends on patient engagement and adherence. Given that exercise rehabilitation intention is a robust predictor of post-discharge rehabilitation participation, assessing and intervening in patients’ intention before discharge is critical to optimizing their subsequent active engagement in exercise rehabilitation programs.
Despite the significant influence of exercise rehabilitation intention on participation in exercise rehabilitation behaviors and outcomes, current research on exercise rehabilitation intention among CVD patients is fragmented. Although exercise rehabilitation intention strongly predicts patients’ future exercise rehabilitation behavior, current research on its influencing factors still insufficient, limiting the development of effective intervention measures. This is reflected in the limited number of interventional studies and the proliferation of assessment tools that generally lack multidimensionality and rigorous validation. These tools only assess whether patients are willing or intend to engage in exercise rehabilitation, failing to comprehensively reflect the level of their exercise rehabilitation intention. They also do not adequately address assessment needs within specific cultural contexts or resource-constrained settings. Furthermore, the lack of rigorous validation mechanisms further restricts the selection and application of these tools by clinical practitioners during evaluations. Existing intervention studies predominantly focus on specific aspects or dimensions of exercise rehabilitation intention, lacking in-depth interventions targeting individual patient beliefs. This limitation partially undermines the effectiveness and applicability of intervention measures.
A scoping review methodology enables a rapid description of research progress within a specific field, synthesizes existing knowledge, and identifies gaps in the literature. Therefore, this study employed a scoping review methodology16 to map the existing literature on exercise rehabilitation intention among CVD patients, including assessment tools or methods, influencing factors, and intervention approaches. The overall objective is to guide research in the field of exercise intentions among cardiovascular patients by reviewing existing studies, identifying research gaps, and proposing a series of actionable research recommendations. Guided by the Participants-Concept-Context (PCC) framework,17 the primary objectives of this review are to explore the following issues: 1) What levels of exercise rehabilitation intention exist among CVD patients? 2) Which assessment tools or methods currently measure exercise rehabilitation intention in this population? 3) What factors influence exercise rehabilitation intention in CVD patients? 4) What intervention studies have targeted exercise rehabilitation intention in this population?
Materials and Methods
This study is based on the scoping review framework by Arksey and O’Malley, which includes the following sequential steps: defining the research question, identifying relevant studies, selecting studies, extracting data graphs, organizing summaries, and reporting results.16 The study also adheres to the scoping review reporting checklist (PRISMA extension for scoping reviews, PRISMA-ScR).18 Although a protocol was developed by the study authors, this was not published. Given the heterogeneous methods used in available studies from qualitative interviews to quantitative surveys, and lack of a harmonized approach in the field, no formal quality assessment was conducted, which is consistent with the purpose of a scoping review, but caution is needed when interpreting results.
Operational Definitions
We defined exercise rehabilitation intention as an individual’s subjective assessment of their willingness or likelihood to engage in future exercise rehabilitation and the degree of effort they plan to exert. Physical activity intention represents a different measurement form of the same concept. Moreover, behavioral change stages and exercise readiness are frequently used as surrogate indicators for exercise rehabilitation intention.
Identifying Relevant Studies
To ensure comprehensive coverage of relevant literature, systematic searches were conducted across 11 databases from their inception to August 28, 2024. These included international platforms (PubMed, Web of Science, Cochrane Library, Embase, EBSCO, Scopus, OpenGrey) to capture global research, and Chinese databases (China National Knowledge Infrastructure, Chinese Biomedical Literature Service System, Wanfang, VIP) to incorporate region-specific studies.The search strategy integrated controlled vocabulary (Medical Subject Headings, Emtree terms) with free-text keywords, co-designed by a professor with long-standing expertise in cardiac rehabilitation research and clinical practice to align with field-specific terminology. A representative string example: (cardiovascular diseases OR cardiac diseases OR coronary heart disease OR circulatory system diseases) AND (exercise rehabilitation willingness OR exercise rehabilitation intention OR exercise willingness OR exercise intention OR cardiac rehabilitation willingness). Full platform-specific strategies are detailed in Appendix 1.
Study Selection
Inclusion criteria: (1) The study population was patients with CVD; (2) Age≥18 years; (3) the literature included studies related to exercise rehabilitation intention, including those on general physical activity intention; (4) The study context focused on the level of exercise rehabilitation intention, assessment tools/methods, influencing factors, and intervention trials; (5) Inpatient, post-discharge, and community populations; (6) The language was either Chinese or English; (7) The study was an original investigation. Exclusion criteria: (1) Studies involving patients with concurrent major non-cardiovascular diseases, such as malignant tumors and severe mental illness; (2) Conference abstracts and letters to the editor; (3) literature that has been repeatedly published or for which the full text is unavailable.
Study Screening and Data Extraction and Analysis
After importing the retrieved literature into Note Express software for duplicate removal, two researchers trained in evidence-based nursing independently screened the titles and abstracts according to the inclusion and exclusion criteria. They then conducted a secondary screening by reading the full text of the eligible literature. In case of any dispute, the full text was reviewed and discussed with a third researcher who also had experience with evidence-based nursing course training to determine the final included literature.
Data extraction was independently performed by two researchers using pre-designed Microsoft Excel spreadsheet. To ensure reliability of the process, Cohen’s kappa coefficient for inter-rater agreement was computed after dual independent extraction of five records, resulting in κ = 0.88, where a Kappa of greater than 0.8 is considered to represent a high level of agreement between the researchers. Discrepancies were resolved via researcher deliberation; unresolved issues were adjudicated by a third independent researcher. After consensus was reached, the extraction template was finalised and included: first author, publication year, country, study type, research subjects, sample size, level of exercise rehabilitation intention, assessment tools/methods, influencing factors, results, intervention measures (including intervention content, control measures, and effect evaluation), and other relevant findings. The extraction results were compared. If discrepancies arose, both researchers re-examined the literature and discussed the issues to reach a consensus. If the issue remained unresolved, a third researcher was consulted. Further details are presented in Figure 1.
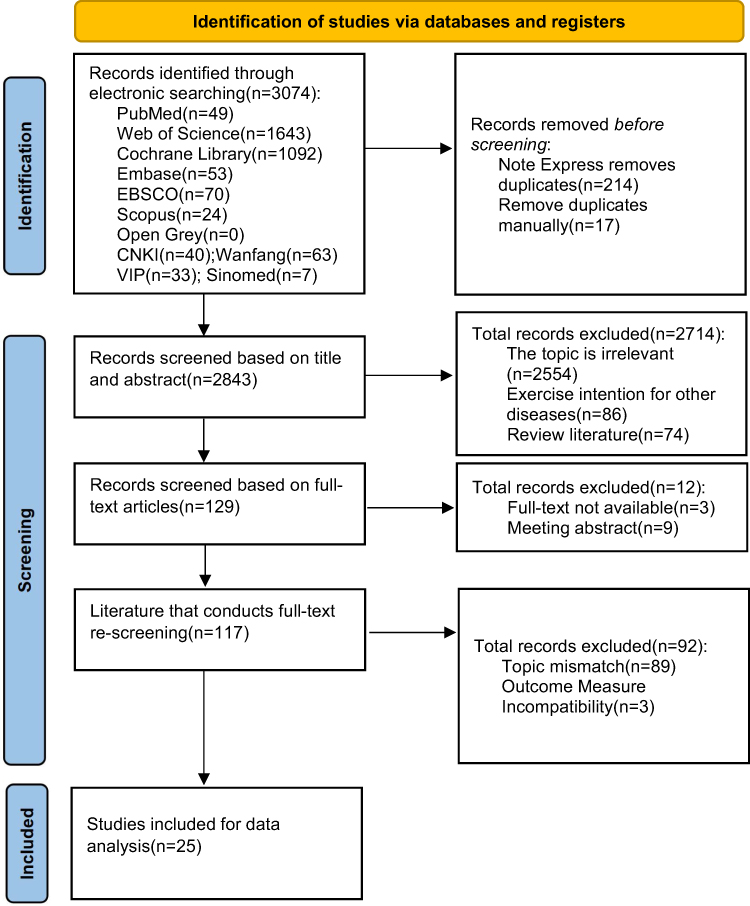 |
Figure 1 Flowchart of the study retrieval process. |
Collate, Summarize and Report Results
Focusing on organizing key elements including exercise intention levels, assessment tools/modalities, influencing factors, and intervention studies among cardiovascular disease patients, we employed a qualitative content analysis approach (Levac, Colquhoun, and O’Brien, 2010). The analytical findings are as follows: (1) Most patients exhibited moderate to low levels of exercise rehabilitation intention; (2) A total of 15 assessment tools or modalities were identified, varying in quality; (3) Influencing factors were categorized into socio-demographic, disease-related, and psycho-social factors; (4) Intervention methods included motivational interviewing, brief psychological interventions, and group health education.
Ethical Consideration
Since this study used secondary data from the literature, there were no ethical issues.
Results
Descriptive Statistics Summary
A total of 3074 documents were retrieved and 25 were finally included after de-weighting and screening, with a total sample size of 13,210 cases.
Basic Information of the Included Literature
The 25 included articles comprised 21 in English13–15,19–36 and 4 articles in Chinese.37–40 The publication period spanned from 1991 to 2024. These studies included 1115,19,24,25,27,29,35–37,39,40 cross-sectional studies, 520,21,23,26,30 qualitative studies, 513,22,32–34 prospective studies, 214,38 parallel randomized controlled trials, and 228,31 experimental studies. In terms of regions, 7 studies13,23,30,37–40 were from China, 6 studies were from Canada,14,31–34,36 3 studies were from the United States,15,22,25 2 studies were from Sweden,21,26 Germany,19 France,20 Jordan,24 European multicenter countries,27 Austria,28 Thailand,29 and Australia.35 1 article each. The basic characteristics of the included studies are shown in Table 1.
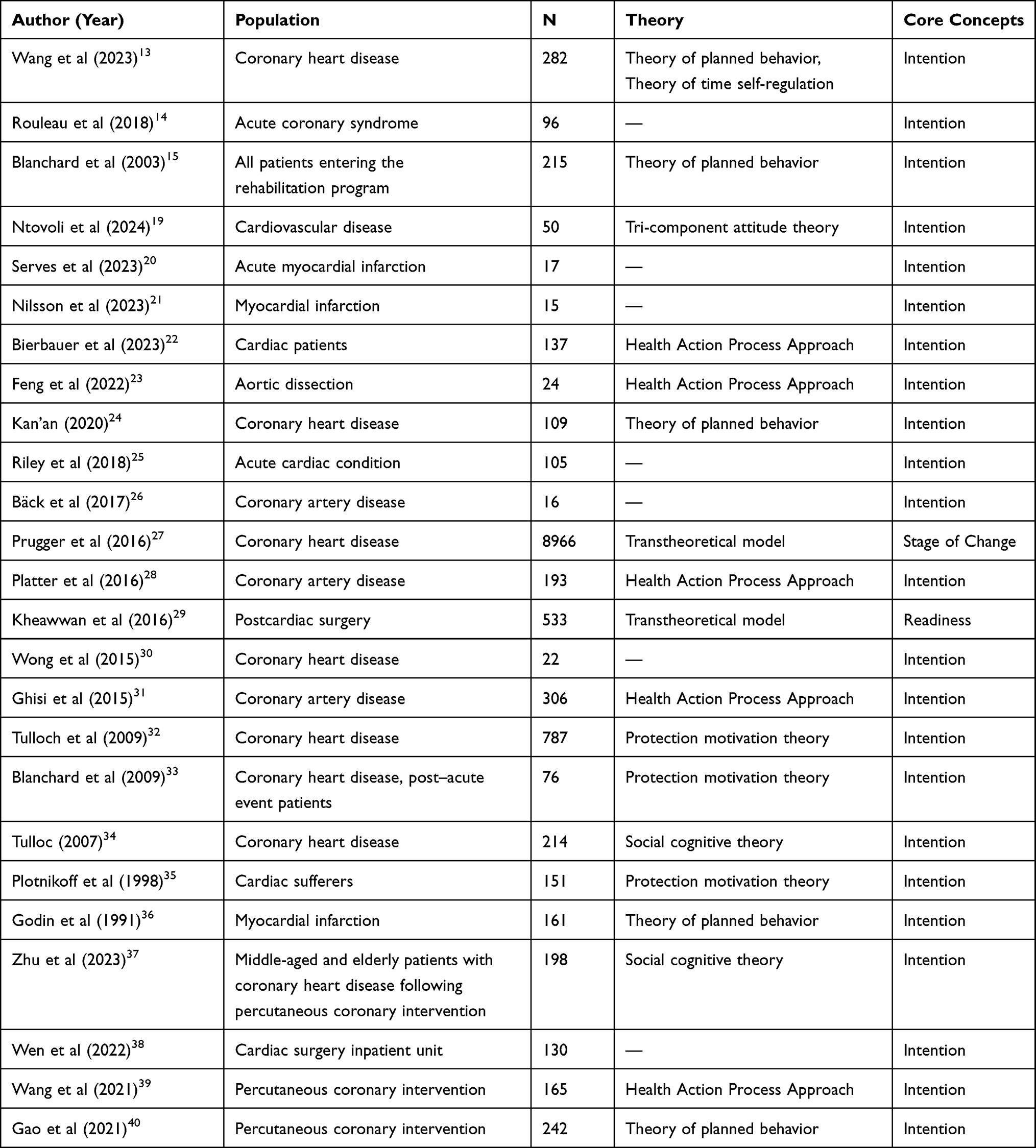 |
Table 1 Basic Characteristics of Included Studies (n=25) |
Research on the Intention Level and Assessment Tools of Exercise Rehabilitation in Patients with CVD
A total of 16 out of 25 included studies reported levels of CVD patients’ exercise rehabilitation intention.13–15,19,22–24,27,28,32–34,36,37,39,40 Of these 16 studies, 10 reported intention levels as mean and standard deviation values, while 2 adopted a level grading system (High/Medium/Low), and 4 reported the proportion of participants expressing intent to engage in active exercise rehabilitation. Within this subset of 16 studies, 813–15,32–34,36,40 reported high exercise rehabilitation intention levels and a relatively high proportion of patients with positive exercise rehabilitation intention, while the remaining 819,22–24,27,28,37,39 reported moderate-to-low intention levels.
Patients with high exercise rehabilitation intention scores were predominantly those diagnosed with acute coronary syndrome (ACS) and post-acute coronary artery disease (CAD) events, whereas low scores were observed primarily in patients with stable coronary artery disease, aortic dissection, and middle-aged and elderly patients who had undergone percutaneous coronary intervention (PCI). Postoperative recovery periods may induce physical discomfort and psychological distress, which hinders patients’ adoption of positive behavioral changes. In addition, middle-aged and elderly patients often experience heightened physiological limitations and comorbidities related to aging, which compromises their exercise rehabilitation intention. Furthermore, across the 16 included studies, a total of 15 assessment tools or methods were identified. These tools primarily focused on the dimensions of intention and planning but exhibited substantial variability: most were non-standardized, and different scales varied in their sensitivity to measuring patients’ intentions, resulting in inconsistencies in result interpretation. Only two evaluation tools were developed by Chinese scholars, with specific details presented in Table 2.
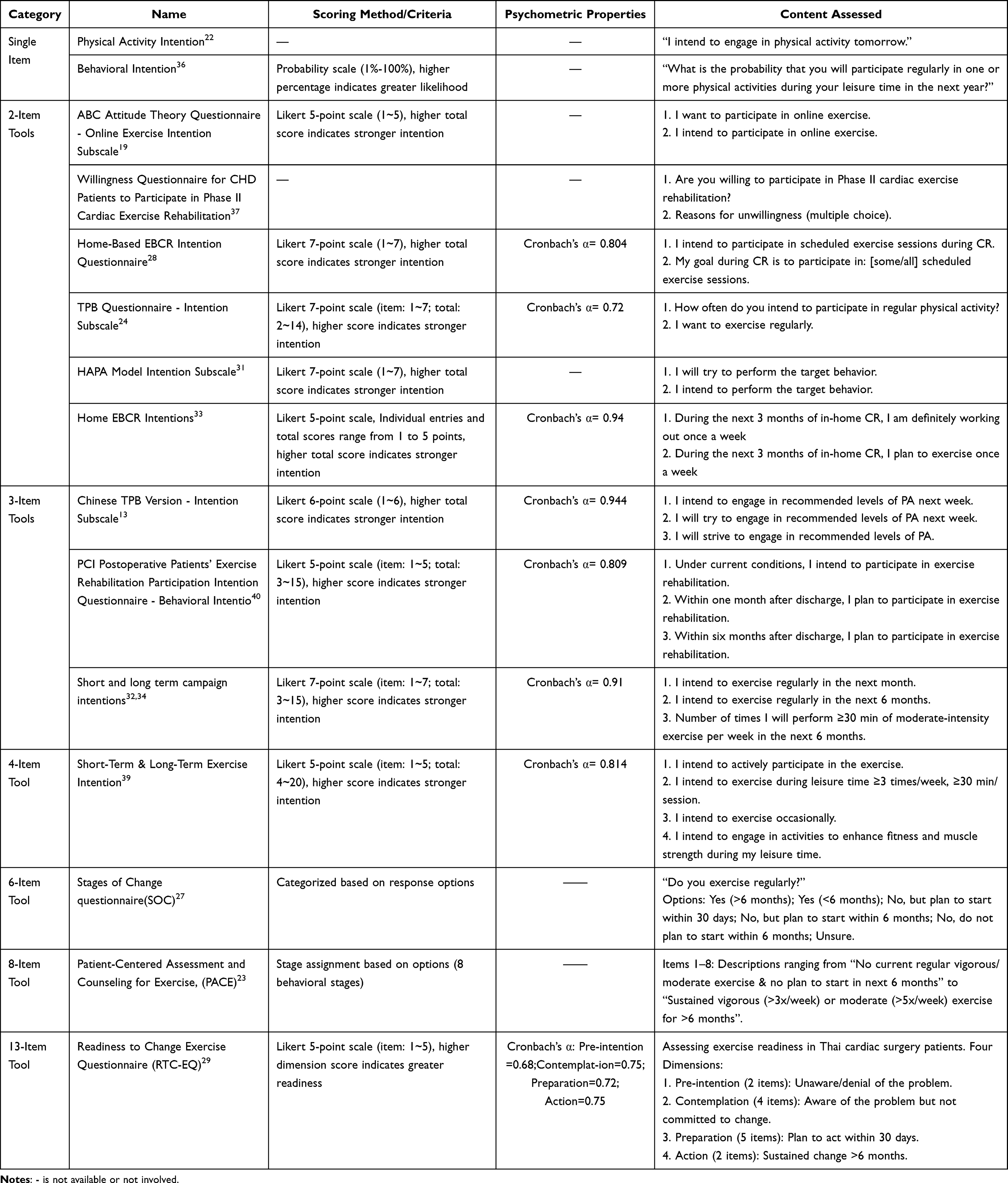 |
Table 2 An Assessment Tool for Exercise Rehabilitation Intentions (n=15) |
Research on the Influencing Factors of Exercise Rehabilitation Intention in Patients with CVD
Among the 25 included studies, 20 investigated factors influencing exercise rehabilitation intentions in CVD patients, including 15 quantitative studies and five qualitative studies. The theoretical frameworks, core concepts, and specific influencing factors underlying each study were systematically organized and summarized in Table 3.
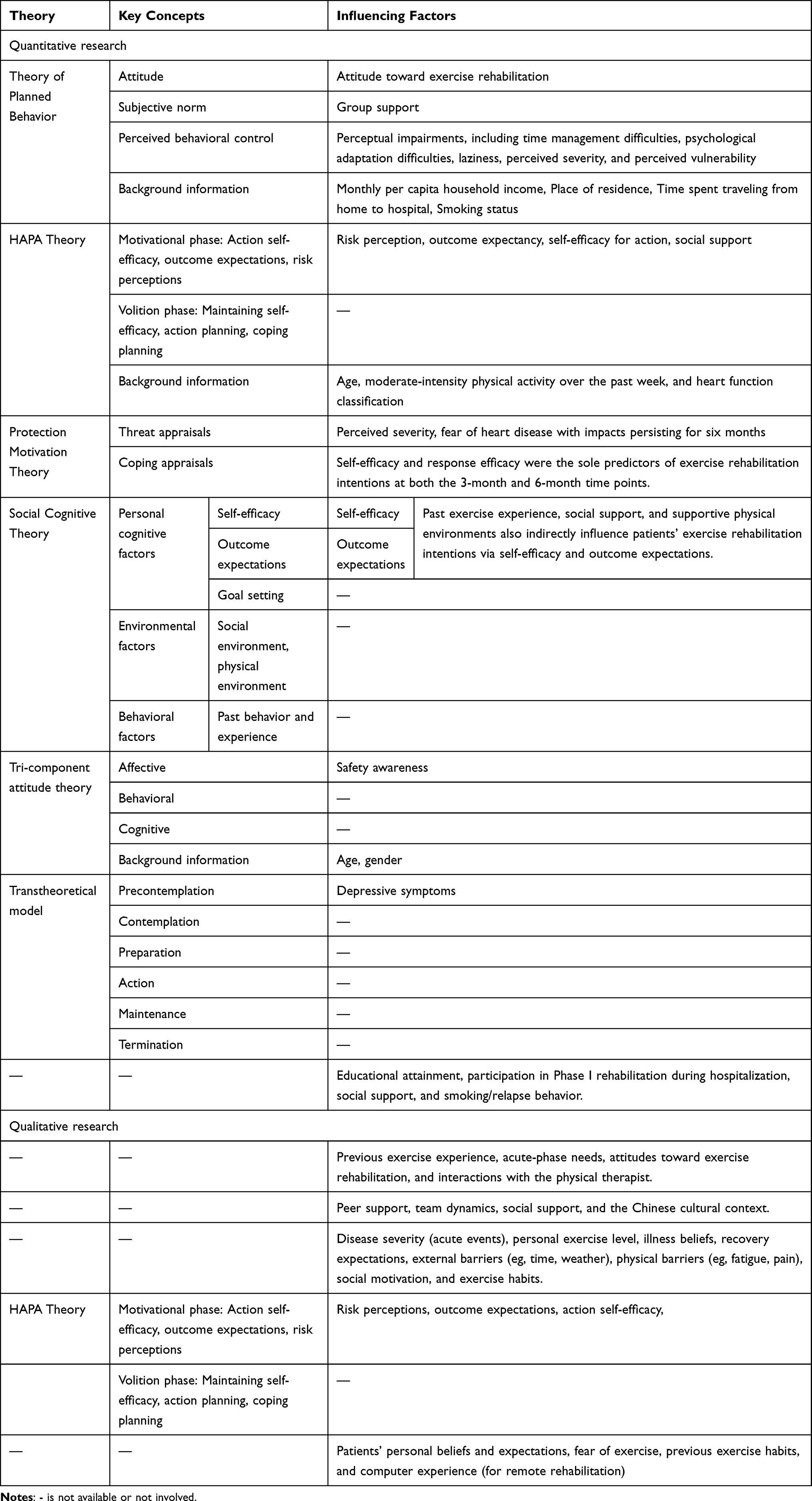 |
Table 3 Factors Influencing Exercise Rehabilitation Intentions Among Patients with CVD (n=20) |
Five studies,13,15,24,36,40 grounded in the Theory of Planned Behavior (TPB),41 collectively illustrate that behavioral intention is jointly driven by behavioral attitude, which reflects individuals’ positive or negative evaluations of exercise rehabilitation; subjective norm, which encompasses perceived social pressure, such as support and expectations from family and healthcare teams; and perceived behavioral control, which includes individuals’ perceived ability to perform exercise rehabilitation and perceived barriers, such as time, energy, and physical condition.15,24,36,40 Additionally, one study13 integrated the TPB with the Theory of Time Self-Regulation,42 thereby highlighting the role of long-term consequence perception in decision-making trade-offs. Two studies,22,39 grounded in Health Action Process Approach (HAPA) theory,43 provided evidence from a dynamic stage perspective,22 validating the foundational role of core motivational stage variables, such as risk perception, outcome expectancy, and behavioral self-efficacy, in intention formation and examining the influence of multiple contextual factors on exercise rehabilitation intention.39 Furthermore, three studies,32,33,35 grounded in protective motivation theory (PMT),44 conducted in-depth analyses of the mechanisms underlying threat and response assessments. Consistent findings indicate that in response evaluation, self-efficacy and response efficacy are the strongest predictors of intention.32 Conversely, in threat evaluation, perceptions of disease severity and the resulting fear do not directly drive action but may exert complex influences on the long-term maintenance of intention.33,35 Other studies grounded in Social Cognitive Theory (SCT),34,45 tri-component (ABC) theory of attitudes,19,46 and Trans theoretical Model (TTM)27,47 have likewise demonstrated the significant influence of self-efficacy, outcome expectancy, affective attitudes such as perceived safety, and psychological states such as depression on exercise rehabilitation intentions. Two studies25,37 identified influencing factors such as literacy, participation in Phase I cardiac exercise rehabilitation during hospitalization, social support, smoking, and resumption or continuation of smoking after discharge using questionnaires and regression analysis with different variables.
Five qualitative studies further enriched the understanding of influencing factors. Findings revealed that factors such as the quality of interactions with healthcare professionals,26 culturally specific social dynamics,30 personalized beliefs and emotions about illness, such as fear,20 and specific physical and situational barriers,23 such as fatigue, weather, and computer experience, may be simplified in quantitative models but hold significant weight in patients’ decision-making experiences. One study,21 conducted through interviews within the HAPA theoretical framework, yielded results consistent with quantitative research and highlighted the central role of risk perception, outcome expectancy, and self-efficacy.
In synthesizing the current evidence, research on factors influencing exercise rehabilitation intentions among CVD patients centers on three primary domains: sociodemographic characteristics, disease-related variables, and psychosocial determinants.
Interventional Study on Exercise Rehabilitation Intention in CVD Patients
Among the 25 studies, four focused on intervention research regarding exercise rehabilitation intentions in cardiovascular disease patients. The theoretical frameworks, intervention measures, duration/frequency of interventions, and outcome measures of each study were systematically reviewed and summarized in Table 4.
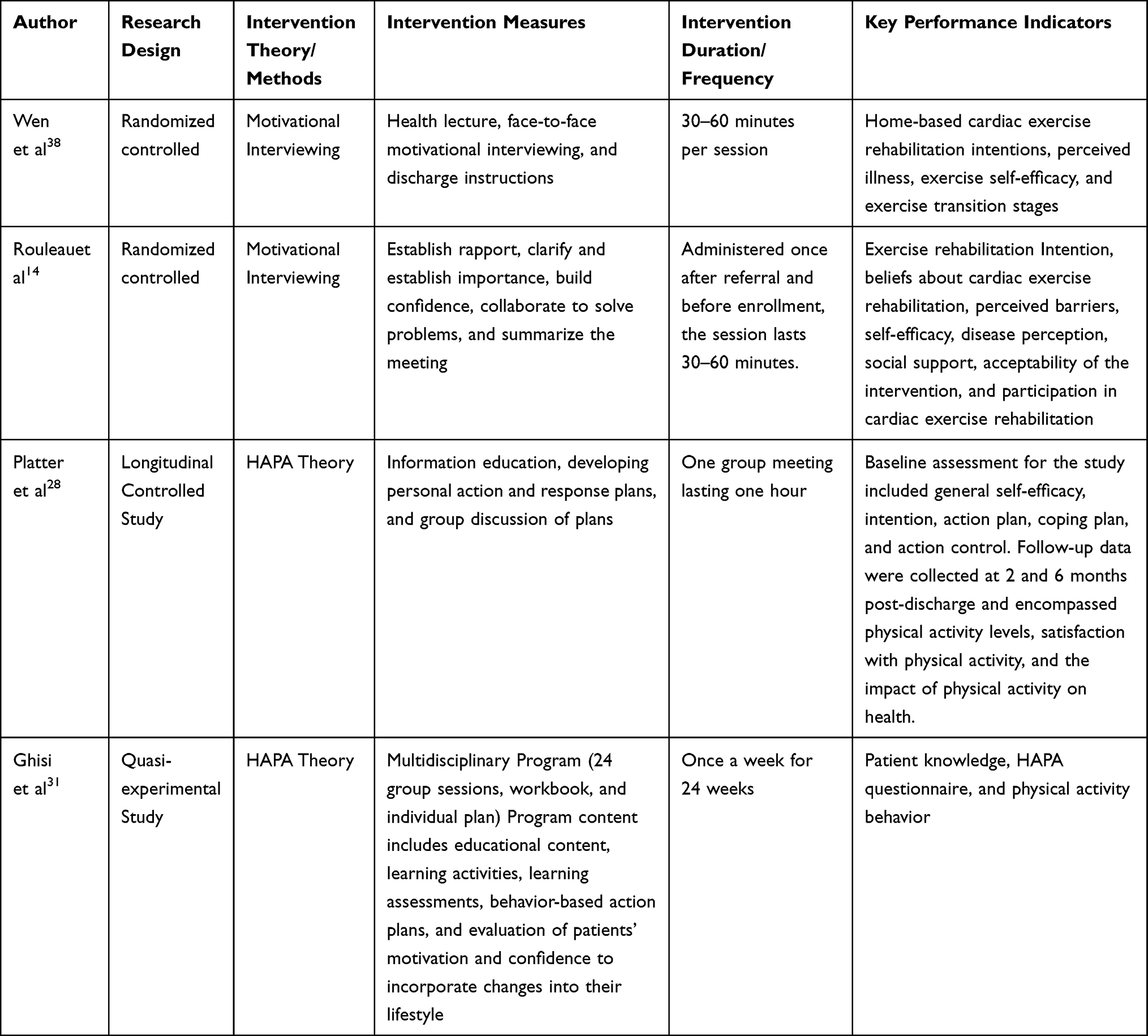 |
Table 4 Basic Characteristics of Intervention Studies on Exercise Rehabilitation Intentions Among Patients with CVD (n=4) |
Existing intervention pathways predominantly rely on two major theoretical frameworks. The first pathway involves interpersonal psychological strategies, exemplified by Motivational Interviewing (MI),14,38 which resolves patients’ internal psychological conflicts through empathetic dialogue to enhance intrinsic motivation, targeting the intention formation stage. The second pathway comprises structured education programs based on HAPA theory,28,31 guiding patients in developing concrete action plans and coping strategies to elevate intention and translate it into actionable behavioral plans, targeting the execution stage. Collectively, these two pathways address critical weak links in the behavioral change chain. In terms of intervention content, measures generally extend beyond single-faceted health education to integrate information provision, skills training, and psychological support. Intervention contact points, duration, and frequency varied widely, ranging from single 30- to 60-minute motivational interviews,14 one-time group education sessions, to 24-week structured courses,31 reflecting different studies’ explorations of intervention dosage. In summary, the intervention studies included in this review demonstrate the feasibility of enhancing patients’ exercise rehabilitation intentions through structured psychological interventions and educational programs, providing a foundational reference for subsequent research and practice.
Discussion
Research on Exercise Rehabilitation Intention in CVD Patients Warrants Significant Strengthening
Exercise rehabilitation intention serves as a primary determinant of active engagement and sustained adherence to post-discharge rehabilitation protocols among CVD patients. However, research in this area is hampered by theoretical and methodological inconsistencies. Although many studies cite frameworks like the TPB or the HAPA, some studies integrate concepts such as behavioral stages from TTM without clearly distinguishing constructs. These issues may contribute to inconsistent conclusions regarding the same influencing factors. The absence of standardized and normative assessment tools restricts the ability of existing methods to effectively assess patients’ exercise rehabilitation intentions at discharge. Moreover, these methods fail to comprehensively capture the intrinsic causes influencing such intentions, thereby limiting healthcare professionals’ capacity to implement targeted interventions tailored to individual patient differences. Studies examining influencing factors often lack comprehensiveness and systematization, and inadequately address multidimensional influences, such as cultural background, economic status, and personal preferences. As a result, they do not fully address the influences on patients’ exercise rehabilitation intentions, and the findings regarding some factors are inconsistent. Additionally, frailty, cognitive function, and depressive symptoms are common in the elderly population and are important factors affecting intention and behavior, yet current research often overlooks them, making them worthy of future focus.48 Existing research on intention has generally paid less attention to the stages of behavioral change and the maintenance of long-term behavior. Future research may benefit from exploring the dynamics of intention and the mechanisms underlying its long-term maintenance.49 Dietary adjustments can indirectly influence exercise rehabilitation intentions through various pathways. Future research could potentially explore the synergistic effects between dietary modifications and exercise rehabilitation intentions on rehabilitation outcomes.50,51 The number of intervention studies is relatively limited, and existing programs typically address only a single dimension, with significant variations in the approach and content of the intervention and evaluation indicators. Current evidence suggests that future research could consider delving deeper into these areas to enhance the comprehensiveness and scientific validity of the studies.
Validated Instruments for Assessing Exercise Rehabilitation Intention in CVD Patients Await Development
Exercise rehabilitation intention is a multidimensional concept that falls under behavioral intention. According to the theory of planned behavior, it refers to an individual’s willingness to perform a specific behavior, their planning, and the degree of effort they invest in achieving it. This intention is influenced by attitudes, subjective norms, and perceived behavioral control. Among the 15 assessment tools included in this study, PACE questionnaires have been applied across different countries and populations, demonstrating high reliability and validity. Home EBCR Intentions also demonstrate high reliability. These tools offer standardized and reliable measurement methods for assessing patients’ exercise rehabilitation intention. However, despite these contributions, there are still limitations in the current assessment tools. Willingness and planning were the most frequently assessed dimensions. The tools that reflect this content in the two entries are suitable for rapid clinical screening. Some tools evaluated only patients’ willingness or intention to engage in exercise rehabilitation.19,22,31,33,36,39,40 Others focused on self-efficacy or perceived barriers.13,14,24,34,38 In contrast, attitudes, subjective norms, and other aspects have received limited attention, being included in only a few instruments or assessed by separate scales. Additionally, some instruments reflected the stages of patients’ exercise rehabilitation,23,27,29 but none comprehensively captured all dimensions of exercise rehabilitation intention. Moreover, most existing exercise rehabilitation intention assessment tools focusing solely on the patient perspective, which is inherently subjective and uncertain. This limits the assessment of patients’ exercise rehabilitation intention at discharge and precludes effective determination of the intrinsic factors influencing patients’ intentions. Consequently, it is challenging to guide healthcare professionals in implementing targeted interventions. This is a limitation in assessing patients’ exercise rehabilitation intention at discharge. Accurate assessment of patients’ pre-discharge intention to participate in exercise rehabilitation is critical for effectively guiding patients to actively participate in exercise rehabilitation after discharge and ensuring their adherence to future rehabilitation programs. Given the current limitations, future research may explore a more scientifically rigorous assessment tool that integrates theories and comprehensively covers the multidimensional aspects of exercise rehabilitation intention. This includes patients’ willingness to participate, plans, effort, practical barriers, attitudes, and social support. This will enhance the accuracy of assessing patients’ intention to participate in exercise rehabilitation and provide healthcare professionals with a basis for targeted interventions, thereby improving patients’ participation and adherence to exercise rehabilitation.
The Need for Further Enrichment in Intervention Studies on Exercise Rehabilitation Intention Among CVD Patients
Among the 25 included studies, four interventional studies each utilized the strategies of motivational interviewing, psychosocial health interventions, and educational interventions. Two of the motivational interviews, one study enhanced patients’ awareness and self-efficacy for exercise rehabilitation through rapport-building, emphasis on home-based rehabilitation importance, and barrier resolution, resulting in some improvement in both willingness for home-based exercise and exercise self-efficacy. Another study14 enhanced participation willingness through trust-building, importance clarification, confidence development, and collaborative problem-solving, indirectly improving rehabilitation adherence. Platter et al28 conducted a study using a brief health psychology intervention in the form of a group education session to encourage patients to develop individual physical activity actions and coping plans, which were discussed within the group. In the short term, this study reported positive effects on the patients’ exercise rehabilitation intention and physical activity levels. A comparative educational study31 developed a new educational program based on the HAPA establishment, but it did not significantly differ from traditional education as expected. However, its role in promoting action planning must not be overlooked. Action planning within the HAPA model acts as a crucial link between intention and behavior, enabling patients to translate their intentions into concrete actions. Additionally, constructs like task self-efficacy and outcome expectancy may bolster patients’ exercise intentions and planning, thus increasing the likelihood of behavioral change. Thus, despite current research not showing significant benefits of HAPA-based programs, their potential to facilitate behavioral change merits further investigation in future studies. Given the limited quantity of evidence and high heterogeneity among these studies, currently, it can only preliminarily suggest that motivational interviewing, group psychological interventions, and educational interventions have potential in improving intention, but this still needs to be confirmed by more high-quality randomized controlled trials.
In addition, these interventions primarily focused on isolated dimensions of exercise rehabilitation intention. While the first two studies addressed attitudes and subjective norms, the latter two emphasized perceived behavioral control. Exercise rehabilitation intention is inherently multidimensional rather than unidimensional. Although individualized interventions accommodate varying rehabilitation needs, they often neglect multidimensional intention differences. In line with patient needs and the principle of patient-centered care, single-dimensional programs struggle to address patients’ complex demands and support individualized decision-making. For instance, individuals with low self-efficacy stemming from past sports injuries may struggle to adhere to such programs due to psychological barriers even when their intention to engage is strong, highlighting a clear disconnect between interventions and real-world clinical contexts. In terms of evidentiary support, a study by Ghisi et al31 suggested that multidimensional integrated interventions may enhance patient adherence, with outcomes that appear to be more favorable than those of single-dimensional approaches. Current evidence indicates the potential constraints that current limitations impose on rehabilitation effectiveness. Therefore, future research could consider transcend the single-dimensional framework. Notably, the TPB provides a comprehensive framework for exercise rehabilitation intention interventions. Beyond attitudes and perceived behavioral control, factors like social support significantly influence behavioral intention. Therefore, healthcare professionals should target broader dimensions, including enhancing social support and reducing barriers, during intervention design. Practical approaches encompass developing social support networks, establishing peer groups, and implementing educational communications. Internet technology52 further enables deeper integration of social resources,53 facilitating multidimensional,54 diversified, and structured55 patient education. Importantly, enhancing CR participation depends not only on individual intentions but also on systemic factors like standardized programs, insurance coverage, and accessibility. Policy and institutional improvements are essential to address these broader challenges. Collectively, these integrated approaches may comprehensively enhance exercise rehabilitation intention, thereby improving participation and adherence.
Limitations
This scoping review adhered to Arksey and O’Malley’s methodological framework while acknowledging several constraints. Primarily, the linguistic scope remained restricted exclusively to Chinese and English publications, potentially introducing cultural and geographic bias. Furthermore, supplementary citation tracking was omitted from the screening protocol, creating possible gaps in source identification. The exclusion criteria systematically eliminated non-traditional publication formats including but not limited to conference abstracts, letters, and commentaries, which may contain emergent findings. Additionally, gray literature interrogation was limited to partial database coverage rather than comprehensive retrieval, potentially overlooking unpublished datasets and institutional reports. Notably, no pre-registration of the review protocol was conducted, which may increase the risk of selective reporting bias. Finally, consistent with scoping review methodology, no critical appraisal of included studies was performed, precluding assessment of evidence strength and necessitating cautious interpretation of findings.
Conclusions
This study synthesizes relevant research on exercise rehabilitation intention in the cardiovascular field, highlighting key areas for future research and clinical action. Our review uniquely consolidates findings on intention levels, influencing factors, assessment tools, and intervention methodologies, underscoring the importance of intention-based guidance. Future research may benefit from further exploring the multidimensional influencing factors of exercise rehabilitation intention. Additionally, efforts should focus on selecting, developing, or revising assessment tools to achieve a more scientific and comprehensive evaluation of exercise rehabilitation intention in CVD patients. In clinical practice, strengthening inter-professional teamwork and multidimensional joint interventions could improve patients’ levels of exercise rehabilitation intention, enhance their participation in exercise rehabilitation, and ultimately promote better health outcomes. Concurrently, the standardized intervention model and management plan can be constructed based on the theoretical framework of planned behavior, taking into account the current situation of CR and the individual needs of CVD patients. This approach not only enhances exercise adherence but also promotes overall health, making it a valuable contribution to the field of cardiovascular rehabilitation.
Funding
Science and Technology Program of Hebei Province (S&T Program of Hebei) (no. 18277735D).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Timmis A, Kazakiewicz D, Torbica A. et al. Cardiovascular disease care and outcomes in West and South European countries. Lancet Regional Health. 2023;33(100781):100718. doi:10.1016/j.lanepe.2023.100718
2. Mingbo L, Xinye H, Xiaohong Y, et al. Interpretation of report on cardiovascular health and diseases in China 2023. Chin J Intervent Cardiol. 2024;32(10):541–16.
3. Pelliccia A, Sharma S, Gati S, et al. 2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease: the Task Force on sports cardiology and exercise in patients with cardiovascular disease of the European Society of Cardiology (ESC). Eur Heart J. 2021;42(1):17–96. doi:10.1093/eurheartj/ehaa605
4. Kim C, Sung J, Lee JH, et al. Clinical practice guideline for cardiac rehabilitation in Korea. Ann Rehabil Med. 2019;43(3):355. doi:10.5535/arm.2019.43.3.355
5. Aacvpr. Guidelines for cardiac rehabilitation and secondary prevention programs[M]. Human Kinetics. 2013;2013:1.
6. Balady GJ, Ades PA, Bittner VA, et al. Referral, enrollment, and delivery of cardiac rehabilitation/secondary prevention programs at clinical centers and beyond: a presidential advisory from the American Heart Association. Circulation. 2011;124(25):2951–2960. doi:10.1161/CIR.0b013e31823b21e2
7. Kokkinos P, Faselis C, Samuel IBH, et al. Changes in Cardiorespiratory Fitness and Survival in Patients With or Without Cardiovascular Disease. J Am College of Cardiol. 2023;81(12):1137–1147. doi:10.1016/j.jacc.2023.01.027
8. Smith Jr SC, Benjamin EJ, Bonow RO, et al. AHA/ACCF secondary prevention and risk reduction therapy for patients with coronary and other atherosclerotic vascular disease: 2011 update: a guideline from the American Heart Association and American College of Cardiology Foundation. Circulation. 2011;124(22):2458–2473. doi:10.1161/CIR.0b013e318235eb4d
9. Anderson L, Thompson DR, Oldridge N, et al. Exercise‐based cardiac rehabilitation for coronary heart disease. Cochrane Database Syst Rev. 2016;2016(1):2.
10. Do Simon M, Do Korn K, Cho L, et al. Cardiac rehabilitation: a class 1 recommendation. Cleveland Clin J Med. 2018;85(7):551. doi:10.3949/ccjm.85a.17037
11. Karmali KN, Davies P, Taylor F, et al. Promoting patient uptake and adherence in cardiac rehabilitation. Cochrane Database Syst Rev. 2014;6:CD007131.
12. Xiangquan W, Xiaofeng W, Guoqiang L. Autonomous health promotion of urban residents based on the theory of behavior transformation. Shandong Sports Sci Technol. 2017;39(4):1–6.
13. Wang W, Wu M, Hua Y, et al. Using an integrated model of the theory of planned behavior and the temporal self-regulation theory to explain physical activity in patients with coronary heart disease. Front Psychol. 2023;14:1049358. doi:10.3389/fpsyg.2023.1049358
14. Rouleau CR, King-Shier KM, Tomfohr-Madsen LM, et al. The evaluation of a brief motivational intervention to promote intention to participate in cardiac rehabilitation: a randomized controlled trial. Patient Educ Couns. 2018;101(11):1914–1923. doi:10.1016/j.pec.2018.06.015
15. Blanchard CM, Courneya KS, Rodgers WM, et al. Is the Theory of Planned Behavior a Useful Framework for Understanding Exercise Adherence During Phase II Cardiac Rehabilitation? J Cardiopulm Rehabil. 2003;23(1):29–39. doi:10.1097/00008483-200301000-00007
16. Arksey H, O’malley L. Scoping studies: framework, Towards a methodological. International Journal of Social Research Methodology. 2005;8(1):19–32. doi:10.1080/1364557032000119616
17. Peters MD, Marnie C, Tricco AC, et al. Updated methodological guidance for the conduct of scoping reviews. JBI Evidence Synth. 2020;18(10):2119–2126. doi:10.11124/JBIES-20-00167
18. C TA, Lillie E, Zarin W, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): checklist and Expla nation. Ann Internal Med. 2018;169(7):467–473. doi:10.7326/M18-0850
19. Ntovoli A, Anifanti M, Koukouvou G, et al. The Attitudes of Patients with Cardiovascular Diseases towards Online Exercise with the Mobile Monitoring of Their Health-Related Vital Signs. Sports. 2024;12(2):47. doi:10.3390/sports12020047
20. Serves N, Pazart L, Gabriel D, et al. Adherence to rehabilitation and home exercise after myocardial infarction: a qualitative study of expectations, barriers and drivers. BMC Sports Sci Med Rehabil. 2023;15(1):98. doi:10.1186/s13102-023-00714-3
21. Nilsson U, Öberg B, Bäck M. Patients’ Perceptions of Exercise-Based Cardiac Telerehabilitation after a Myocardial Infarction—A Qualitative Study. Int J Environ Res Public Health. 2023;20(7):5420. doi:10.3390/ijerph20075420
22. Bierbauer W, Bermudez T, Bernardo A, et al. Predicting physical activity following cardiac rehabilitation: a longitudinal observational study. Rehabilitation Psychology. 2023;68(3):338–349. doi:10.1037/rep0000490
23. Feng D, Huang S, Lang X. Attitudes and behavioral intentions of aortic dissection survivors towards exercise: an application of the health action process approach framework. Rev cardiovasc med. 2022;23(2):64. doi:10.31083/j.rcm2302064
24. Kan’an SM. Predicting Intentions to Physical Activity in Jordanian Patients with Coronary Artery Disease: impact of Attitudes, Subjective Norms, and Perceived Behavioral Control [doctoral thesis]. Kent, OH, USA: Kent State University; 2020.
25. Riley H, Headley S, Winter C, et al. The Effect of Smoking Status on Exercise Perception and Intentions for Cardiac Rehabilitation Enrollment among Patients Hospitalized with an Acute Cardiac Condition. J Cardiopulmonary Rehabil Prevent. 2018;38(5):286–290. doi:10.1097/HCR.0000000000000288
26. Bäck M, Öberg B, Krevers B. Important aspects in relation to patients’ attendance at exercise-based cardiac rehabilitation – facilitators, barriers and physiotherapist’s role: a qualitative study. BMC Cardiovascular Disorders. 2017;17(1):77. doi:10.1186/s12872-017-0512-7
27. Prugger C, Wellmann J, Heidrich J, et al. Regular exercise behaviour and intention and symptoms of anxiety and depression in coronary heart disease patients across Europe: results from the EUROASPIRE III survey. Eur J Preventive Cardiol. 2016;24(1):84–91. doi:10.1177/2047487316667781
28. Platter M, Hofer M, Hölzl C, et al. Supporting cardiac patient physical activity: a brief health psychological intervention. Wiener klinische Wochenschrift. 2016;128(5–6):175–181. doi:10.1007/s00508-016-0968-y
29. Kheawwan P, Chaiyawat W, Aungsuroch Y, et al. Patient Readiness to Exercise After Cardiac Surgery. J Cardiovasc Nurs. 2016;31(2):186–193. doi:10.1097/JCN.0000000000000221
30. Wong EML, Zhong XB, Sit JWH, et al. Attitude toward the out-patient cardiac rehabilitation program and facilitators for maintenance of exercise behavior. Psychol Health Med. 2015;21(6):724–734. doi:10.1080/13548506.2015.1115107
31. Ghisi GLDM, Grace SL, Thomas S, et al. Behavior determinants among cardiac rehabilitation patients receiving educational interventions: an application of the health action process approach. Patient Educ Couns. 2015;98(5):612–621. doi:10.1016/j.pec.2015.01.006
32. Tulloch H, Reida R, D’angeloa MS, et al. Predicting short and long-term exercise intentions and behaviour in patients with coronary artery disease: a test of protection motivation theory. Psychol Health. 2009;24(3):255–269. doi:10.1080/08870440701805390
33. Blanchard CM, Reid RD, Morrin LI, et al. Does protection motivation theory explain exercise intentions and behavior during home-based cardiac rehabilitation? J Cardiopulmonary Rehabi Prevention. 2009;3(3):188–192. doi:10.1097/HCR.0b013e3181a333a3
34. Tulloc H. Social Cognitive Determinants of Exercise Intentions and Behaviour in Patients with Coronary Artery Disease [doctoral thesis]. Ottawa, Canada: University of Ottawa Hospital, School of Psychology: 2007.
35. Plotnikoff RC, Higginbotham N. Protection motivation theory and the prediction of exercise and low-fat diet behaviours among Australian cardiac patients. Psychol Health. 1998;13(3):411–429. doi:10.1080/08870449808407300
36. Godin G, Valois P, Jobin J, et al. Prediction of intention to exercise of individuals who have suffered from coronary heart disease. Journal of Clinical Psychology. 1991;47(6):762–772. doi:10.1002/1097-4679(199111)47:6<762::AID-JCLP2270470606>3.0.CO;2-T
37. Zhu C, Li H, Pan Q, et al. Determinants of Phase II Cardiac Rehabilitation Participation Intention in Older Adults with Coronary Heart Disease Post-Percutaneous Coronary Intervention. Internal Med. 2023;18(03):289–294.
38. Wen S, Yao F, Cheng Y, et al. Effect of motivational interviewing intervention on the willingness and exercise transition stage of home and exercise based cardiac rehabilitation in patients undergoing cardiac surgery. J Jining Medical Univ. 2022;45(02):106–110.
39. Wang F, Li Y, Zhou J, et al. Current status and influencing factors of exercise intention among patients after percutaneous coronary artery stent implantation. Chin J Modern Nursing. 2021;16(3):326–329.
40. Gao Y. Analysis of Influencing Factors for Exercise Rehabilitation Participation Intention in Post-PCI Patients Based on the Theory of Planned Behavior[D]. Henan University; 2021.
41. Ajzen I. The theory of planned behavior. Organizational Beha Human Decis Processes. 1991;50(2):179–211. doi:10.1016/0749-5978(91)90020-T
42. Hall PA, Fong GT. Temporal self-regulation theory: a model for individual health behavior. Health Psychology Rev. 2007;1(1):6–52. doi:10.1080/17437190701492437
43. Schwarzer R, Lippke S, Luszczynska A. Mechanisms of health behavior change in persons with chronic illness or disability: the Health Action Process Approach (HAPA). Rehabil Psychol. 2011;56(3):161–170. doi:10.1037/a0024509
44. Ronald W, Rogers T. A Protection Motivation Theory of Fear Appeals and Attitude Change1. J Psychol. 1975;91(1):93–114. doi:10.1080/00223980.1975.9915803
45. Bandura A. Social cognitive theory: an agentic perspective. Annu Rev Psychol. 2001;52(1):1–26. doi:10.1146/annurev.psych.52.1.1
46. M JR. Cognitive,Affective,and Behavioral Components of Attitudes. Attitude Organization Change. 1960;1960:1–14.
47. Prochaska JO, Velicer WF. The transtheoretical model of health behavior change. Am J Health Promot. 1997;12(1):38–48. doi:10.4278/0890-1171-12.1.38
48. Yuan Y, Peng C, Burr JA, et al. Frailty, cognitive impairment, and depressive symptoms in Chinese older adults: an eight-year multi-trajectory analysis. BMC Geriatr. 2023;23(1):843. doi:10.1186/s12877-023-04554-1
49. Koenders N, Van Oorsouw R, Conijn D, et al. Patient Needs Regarding Cardiac Rehabilitation: a Systematic Review and Meta‐Ethnographic Synthesis. Journal of the American Heart Association. 2025;14(18):e040588. doi:10.1161/JAHA.124.040588
50. He Y, Wu Q, Liu D, et al. Effect of dietary habits on multiple cardiovascular diseases: a comprehensive Mendelian randomization study. Medicine. 2025;104(36):e44352. doi:10.1097/MD.0000000000044352
51. He Y, Liu D, Wu Q, et al. Is skimmed milk really heart-healthy?: a mediation Mendelian randomization analysis of coronary risk via serum metabolites. Medicine. 2025;104(34):e42653. doi:10.1097/MD.0000000000042653
52. Mizna S, Arora S, Saluja P, et al. An analytic research and review of the literature on practice of artificial intelligence in healthcare. Eur J Med Res. 2025;30(1):382–392. doi:10.1186/s40001-025-02603-6
53. Zhang Z, Pack Q, Squires RW, et al. Availability and characteristics of cardiac rehabilitation programmes in China. Heart Asia. 2016;8(2):9–12. doi:10.1136/heartasia-2016-010758
54. Yousefiazar A, Ghahramanian A, Rahmani A, et al. Designing and validating a patient education model for cardiovascular patients: protocol for a multilevel mixed-method study. BMJ Open. 2025;15(4):e092234. doi:10.1136/bmjopen-2024-092234
55. Shi W, Ghisi GL, Zhang L, et al. Systematic review, meta‐analysis and meta‐regression to determine the effects of patient education on health behaviour change in adults diagnosed with coronary heart disease. J Clin Nurs. 2023;32(15–16):5300–5327. doi:10.1111/jocn.16519
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Woman’s Heart: Improving Uptake and Awareness of Cardiovascular Screening for Middle-Aged Populations
Kazzi B, Shankar B, Elder-Odame P, Tokgözoğlu LS, Sierra-Galan LM, Michos ED
International Journal of Women's Health 2023, 15:1171-1183
Published Date: 24 July 2023
Managing Cardiovascular Risk in Systemic Lupus Erythematosus: Considerations for the Clinician
Semalulu T, Tago A, Zhao K, Tselios K
ImmunoTargets and Therapy 2023, 12:175-186
Published Date: 8 December 2023