Back to Journals » Journal of Hepatocellular Carcinoma » Volume 13
Integrating Combination Therapy and Smart Embolic Materials to Overcome the Therapeutic Ceiling of Transarterial Chemoembolization in Hepatocellular Carcinoma
Authors Fu Y ![]() , Bai C, Ling Y, Liu Y, Li W, Li G
, Bai C, Ling Y, Liu Y, Li W, Li G ![]()
Received 29 April 2026
Accepted for publication 12 June 2026
Published 19 June 2026 Volume 2026:13 620956
DOI https://doi.org/10.2147/JHC.S620956
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr David Gerber
Yantao Fu, Chenglin Bai, Yunzhi Ling, Yijun Liu, Weijun Li, Guoming Li
Department of General Surgery, Chaoyang City Center Hospital of China Medical University, Chaoyang, Liaoning, People’s Republic of China
Correspondence: Guoming Li, Department of General Surgery, Chaoyang City Center Hospital of China Medical University, Chaoyang, Liaoning, People’s Republic of China, Email [email protected]
Abstract: Transarterial chemoembolization (TACE) remains standard for intermediate-stage hepatocellular carcinoma (HCC), but its long-term efficacy is limited by post-embolic hypoxia-driven angiogenesis and high recurrence rates. Combining TACE with targeted therapy, immunotherapy, or ablation improves outcomes. Concurrently, smart embolic agents are transforming TACE from passive embolization into active modulation of the tumor microenvironment. This review systematically evaluates clinical evidence for TACE-based combinations and principles guiding individualized selection. We delineate synergistic mechanisms of TACE with systemic and locoregional therapies, and highlight functional design of novel embolic materials. Although some triplet regimens have shown progression-free survival benefits, overall survival superiority remains unproven, as exemplified by the negative OS outcome in the LEAP-012 trial. However, the available network meta-analyses are constrained by substantial heterogeneity in study design, TACE protocols, and outcome definitions, warranting cautious interpretation. Finally, we propose a multidisciplinary paradigm integrating interventional radiology, diagnostic imaging, and biomaterials science. The convergence of material innovation and combination optimization holds promise for overcoming TACE’s therapeutic ceiling.
Plain Language Summary: Hepatocellular carcinoma is the most common primary liver cancer. For intermediate-stage disease, TACE is standard, but its long-term effectiveness is limited because the oxygen-deprived environment it creates can stimulate tumor regrowth. Two strategies have been developed to overcome this: combining TACE with other treatments (targeted drugs, immunotherapy, ablation) and designing new smart embolic materials (hydrogels that respond to tumor conditions). This review integrates these two research directions, synthesizes evidence from clinical trials and network meta-analyses, and proposes a multidisciplinary paradigm to help clinicians and researchers develop more effective, personalized strategies. An infographic schematic titled Precision-Guided Intervention in HCC. Three labeled circles form the core: Intervention at the top, Images at the lower left and Materials at the lower right. Curved arrows connect Intervention with Images and with Materials and a curved arrow connects Images with Materials. Example items feed into the circles with arrows: TACE (liver diagram labeled liver, tumor, catheter, hepatic artery and tumor area) points to Intervention. Ablation (a probe) points to Images. Radiation therapy (cell with a target symbol) points to Images; the label Radiation therapy appears twice. On the Materials side, three sample illustrations point to Materials and the bottom label reads New Embolization Materials. A downward arrow from the central circles points to a liver illustration above the title Precision-Guided Intervention in HCC. The bottom right includes the text Created in link.Infographic of HCC precision-guided intervention linking images, materials and TACE.
Keywords: hepatocellular carcinoma, transarterial chemoembolization, combination therapy, smart embolic materials, stimuli-responsive hydrogels, tumor microenvironment
Introduction
HCC represents a growing global health burden, with most patients presenting with disease precluding curative resection at diagnosis.1–3 TACE exploits the dual hepatic blood supply to induce selective ischemia and deliver localized chemotherapy, establishing it as the standard intervention for intermediate-stage HCC.4 Nonetheless, TACE monotherapy has reached a therapeutic plateau: post-embolic hypoxia drives the upregulation of vascular endothelial growth factor (VEGF), promotes epithelial–mesenchymal transition of residual tumor cells, and contributes to high recurrence rates.5,6 Notably, the etiological composition of HCC (viral hepatitis versus non-alcoholic steatohepatitis) is associated with profound differences in the tumor immune microenvironment and treatment response patterns, which may explain heterogeneity across clinical trials.7
Two parallel research directions have emerged. First, combining TACE with systemic therapies (targeted agents, immune checkpoint inhibitors) or locoregional modalities (ablation, radiotherapy) yields synergistic antitumor effects.8 Pivotal trials EMERALD-1 and LEAP-012 have shown that TACE plus targeted immunotherapy significantly prolongs progression-free survival,9,10 and meta-analyses corroborate superior outcomes for TACE plus ablation or radiotherapy.11,12 Second, innovations in embolic materials are reshaping TACE. Conventional agents (Lipiodol, gelatin sponge, drug-eluting beads) are constrained by poor radiopacity, suboptimal drug-loading capacity, and unfavorable intratumoral distribution.13 Smart hydrogels with tunable properties, microenvironmental responsiveness, and enhanced imaging capabilities are now emerging.13
These two directions are not independent. Optimizing combination regimens requires understanding how embolic materials influence drug release and microenvironment modulation, while novel material design must address clinical demands of combination therapy.14,15 The current literature largely consists of unidimensional reviews, lacking systematic integration. This review aims to fill this gap, synthesizing clinical evidence and decision logic for TACE-based combinations, critically examining heterogeneity, tracing smart embolic materials from design to functional integration, and proposing a multidisciplinary precision treatment paradigm.
Literature Search Strategy
Given the narrative synthesis nature of this review, we performed a systematic literature search of PubMed, Web of Science, and the Cochrane Library from database inception to October 2025. The search strategy combined MeSH terms and keywords related to “hepatocellular carcinoma”, “transarterial chemoembolization”, “combination therapy”, “immunotherapy”, “tyrosine kinase inhibitor”, “radiotherapy”, “ablation”, “smart hydrogel”, and “embolic agent”. Inclusion criteria comprised original research or systematic reviews or meta-analyses evaluating TACE-based combination regimens or novel embolic materials, studies reporting clinical outcomes (survival, response rate, safety) or preclinical performance of embolic agents, and articles published in English. Exclusion criteria were case reports with fewer than five patients, editorials or commentaries without original data, and in vitro studies without in vivo validation for embolic materials. Relevant articles were selected after title or abstract screening and full-text review. Due to significant heterogeneity in study design, patient populations, and treatment protocols, a formal quantitative meta-analysis was not feasible. We conducted a narrative synthesis with qualitative comparisons. We acknowledge that the predominance of studies from Chinese research groups reflects regional publication patterns and availability of certain domestic agents, which may introduce geographic bias (further addressed in Discussion).
Evidence Quality Assessment
In evaluating the included network meta-analyses, we paid particular attention to study design (prospective vs retrospective), heterogeneity in patient selection (Child-Pugh class, tumor burden, portal vein invasion), TACE protocol variability (conventional vs drug eluting bead TACE (DEB-TACE); fixed vs on-demand schedules), and outcome definitions (progression free survival (PFS) vs time to progression (TTP); Response Evaluation Criteria in Solid Tumors (RECIST) vs modified RECIST (mRECIST)). As noted by Ades et al,16 minimizing heterogeneity is critical to network meta-analysis reliability Using the newly developed Risk of Bias in Network Meta Analysis (RoB NMA) tool, recent studies have identified suboptimal adherence in transitivity assessment and meta-regression.17 In TACE trials, heterogeneity in technique and timing fundamentally weakens conclusions, especially without strict protocol enforcement.18 Additionally, outcome criteria (RECIST vs mRECIST) significantly affect response rate estimates and prognostic conclusions.19 Where available, we report I2 statistics and sensitivity analyses. Readers are cautioned that most primary studies informing these network meta-analyses are retrospective, limiting the strength of comparative inferences.
TACE Combined with Locoregional Therapies
TACE alone yields a 5-year survival rate of only 26% in a large cohort of 8510 patients.20 Combining TACE with locoregional ablative therapies or radiotherapy improves prognosis. Commonly used modalities include radiofrequency ablation (RFA), microwave ablation (MWA), high-intensity focused ultrasound (HIFU), percutaneous ethanol injection (PEI), and radiotherapy (RT).21–24 Each combination yields superior 1- and 2-year OS rates relative to TACE alone.25
TACE Combined with RFA
The heat sink effect limits RFA; blood flow dissipates thermal energy, causing residual lesions. TACE preemptively embolizes tumor-feeding arteries, reducing local blood flow and allowing RFA-generated heat to accumulate efficiently, expanding coagulative necrosis by 30–50% versus RFA alone.21 RFA achieves a safe ablative margin of 0.5–1.0 cm beyond the tumor border, eradicating residual viable cells at the tumor periphery after TACE. Sublethal hyperthermia (42–45°C) increases cell membrane permeability, enhancing chemotherapy penetration.26,27 TACE suppresses heat shock protein overexpression induced by RFA alone, attenuating thermal damage repair. A pooled analysis focusing on 3–5 cm HCC lesions showed significantly superior 3-year survival for TACE+RFA versus RFA alone.25
TACE Combined with MWA
MWA uses high-frequency electromagnetic fields >900 MHz (typically 2450 MHz) to generate instantaneous high temperatures (>100°C) via polar water molecule friction, inducing coagulative necrosis.28 MWA has direct heating, faster temperature rise, larger ablation zone, and reduced heat sink susceptibility, making it suitable for tumors >3 cm or adjacent to major vessels.28 TACE reduces perfusion, mitigating the heat sink effect and providing imaging targets via Lipiodol deposition.29 A retrospective study of 258 patients with large/multi-nodular HCC showed TACE+MWA achieved median OS 26.6 vs 17.1 months (P<0.001), with 1-/2-/3-year OS rates 85.9%/59.8%/32.6% vs 59.0%/40.4%/11.4% for TACE alone. Time to progression was also prolonged (12.5 vs 6.7 months, P<0.001). A pooled analysis of 10 studies (1799 patients) confirmed OS HR 0.50 (95% CI 0.40–0.62) and PFS HR 0.47 (0.37–0.61) for TACE+RFA/MWA versus TACE alone, without significant increase in serious complications (OR 1.26, 0.74–2.16).29 Regarding optimization, the timing of sequential MWA is critical. In current practice, MWA is typically performed 2 to 4 weeks after TACE, when Lipiodol deposition is stable, blood flow blockade persists, and post-embolization syndrome has subsided.28 However, MWA has limitations: the ablation antenna (≈5 mm) may increase puncture tract bleeding and needle-track seeding, and improper multi-antenna spacing can cause insufficient ablation zone overlap.28 In summary, TACE combined with MWA is an important option for unresectable HCC, offering high ablation efficiency, reduced heat-sink susceptibility, and superior large-tumor coverage. It is particularly suited for tumors >5 cm, multinodular disease, and lesions adjacent to vessels.28
TACE Combined with HIFU
For residual lesions adjacent to major vessels, bile ducts, or diaphragm, HIFU offers noninvasive conformal ablation.30 HIFU depends on instantaneous high temperatures (>65°C) and cavitation effects, less affected by blood flow. TACE-induced flow reduction further enhances HIFU heating efficiency. HIFU can stimulate cavitation of microbubbles on drug-eluting beads, generating microjets and shock waves that increase chemotherapeutic agent diffusion distance.30 Emerging evidence shows that embolic microspheres loaded with sonosensitizers, upon HIFU irradiation, produce reactive oxygen species (ROS) that eradicate viable tumor cells in the post-embolization hypoxic zone, compensating for the insensitivity of hypoxic cells to embolization alone.30 A pooled analysis showed TACE+HIFU significantly improved 1-year survival (OR 3.13), 2-year survival (OR 3.38), and overall response (OR 3.61) without additional liver impairment.31
TACE Combined with PEI
PEI injects absolute ethanol to destroy tumor cells, but dense fibrous septa impede ethanol diffusion, causing incomplete necrosis.32 TACE induces ischemic necrosis, disrupting fibrous septa and creating diffusion channels. By occluding tumor-feeding arteries, TACE reduces intratumoral blood flow, prolonging ethanol retention and enhancing effect.33 Moreover, Lipiodol deposited during TACE provides a clear landmark for PEI puncture guidance. The foremost advantage of PEI over RFA or MWA is its superior safety profile, specifically the absence of thermal injury risk.33 A multicenter study of HCC lesions in high-risk areas (diaphragm, gallbladder, or gastrointestinal tract) showed that TACE combined with a single PEI session achieved a complete ablation rate of 80.6%, with no gastrointestinal perforation or biliary fistula, confirming the unique safety and efficacy of this regimen for high-risk lesions.33 A pooled analysis of 12 RCTs (825 patients) showed TACE+PEI significantly improved 1-year (risk ratio 1.37), 2-year (1.61), and 3-year (2.66) survival versus TACE alone.33
TACE Combined with RT
For locally advanced disease with major vascular invasion, TACE+RT significantly prolongs survival.11 RT precisely targets extrahepatic collateral territories and hypovascular tumor thrombi missed by TACE.15 TACE induces cell-cycle synchronization (G2/M arrest), the most radiosensitive phase. Lipiodol provides a high-density marker for target delineation. RT disrupts vascular endothelium, increasing permeability and enhancing chemotherapy uptake.15
High-dose RT induces immunogenic cell death (ICD), synergizing with TACE-induced ICD to transform locoregional therapy into an in situ vaccine. For portal vein tumor thrombus (PVTT), RT can recanalize portal flow and alleviate portal hypertension, restoring hepatic function.11,15
Collectively, TACE combined with locoregional modalities consistently demonstrates superior outcomes versus TACE alone. Table 1 summarizes core synergistic mechanisms, advantages, limitations, and efficacy outcomes. Table 2 presents preferred regimens by clinical scenario based on SUCRA rankings from a network meta-analysis of 40 RCTs. With the caveat of substantial heterogeneity across the included RCTs, the efficacy data presented in Table 1 and the exploratory rankings outlined in Table 2 are derived from a network meta-analysis published in BMC Gastroenterology in 2025, which employed Bayesian methodology to rank seven interventional strategies for unresectable HCC across 40 RCTs.25 These rankings should be considered hypothesis-generating rather than definitive.
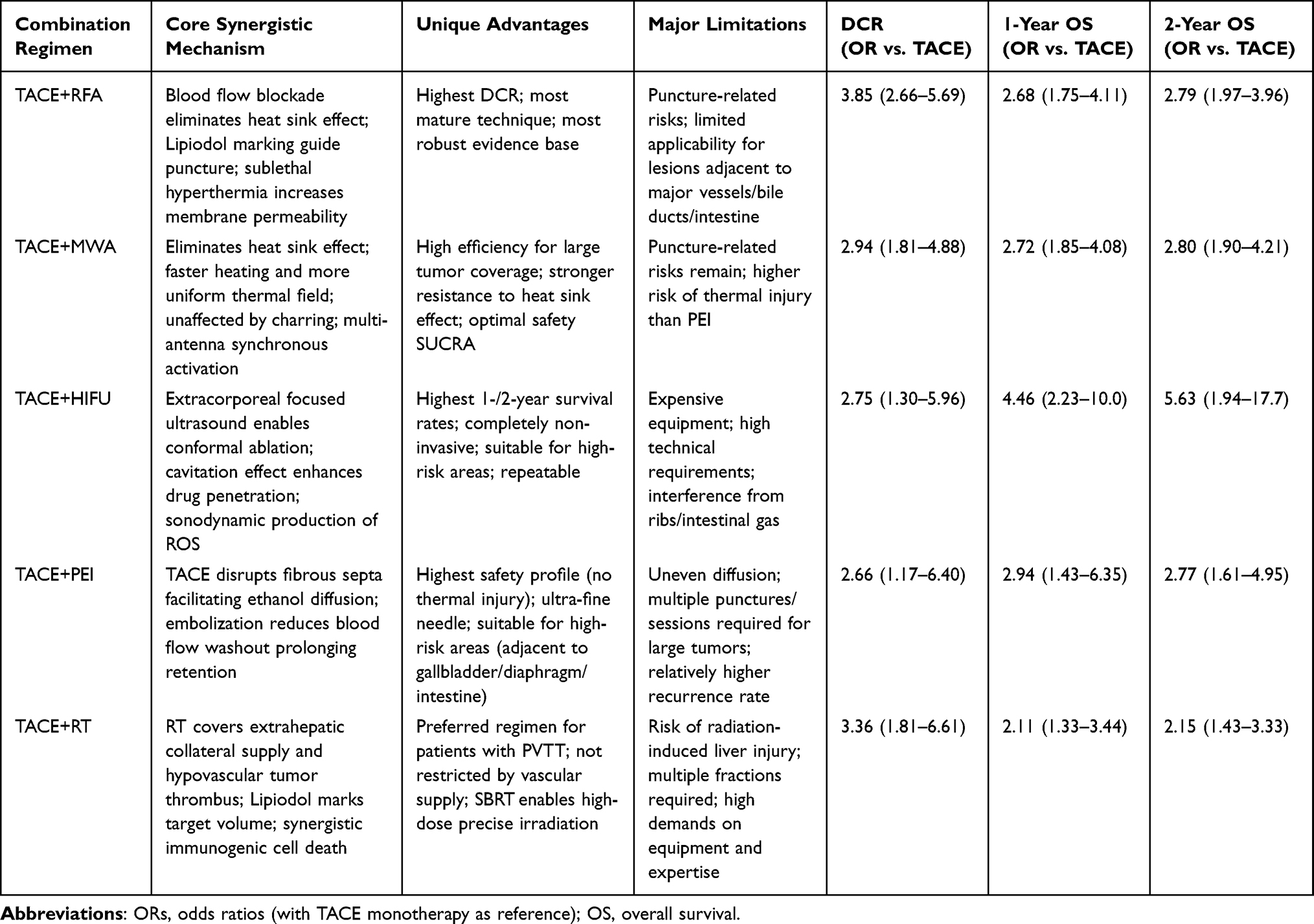 |
Table 1 Comparative Summary of TACE Combined with Five Locoregional Therapeutic Modalities for Hepatocellular Carcinoma |
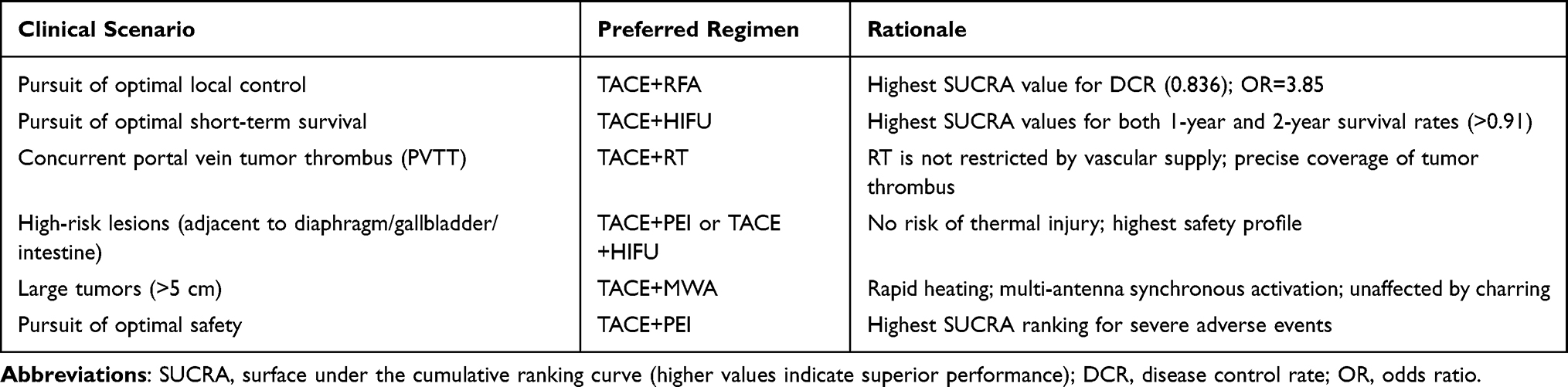 |
Table 2 Recommended TACE-Based Combination Regimens Stratified by Clinical Scenario |
TACE Combined with Systemic Therapies
TACE Combined with Targeted Agents
Post-TACE VEGF elevation drives tumor recurrence and metastasis.34 The post-TACE VEGF elevation justifies combining TACE with TKIs. TKIs inhibit VEGFR, PDGFR, and FGFR, suppressing collateral circulation and revascularization, thereby achieving spatiotemporal synergy between embolization-induced starvation and anti-angiogenic blockade.34 The TACTICS trial first showed TACE+sorafenib significantly prolonged PFS (22.8 vs 13.5 months; HR 0.661; P=0.02).35 Lenvatinib, with FGFR4 inhibition and high ORR (24.1% in REFLECT), is frequently used.36 LAUNCH trial showed TACE+lenvatinib as first-line for advanced HCC achieved median OS 17.8 vs 11.5 months (HR 0.45).37 Donafenib demonstrated OS superiority over sorafenib in ZGDH3 (12.1 vs 10.3 months; HR 0.83; P=0.0245) with better safety.38 For progression on first-line TKIs, regorafenib (HR 0.63 in RESORCE) and cabozantinib (HR 0.76 in CELESTIAL) provide second-line options.39,40 Table 3 summarizes TKI characteristics.
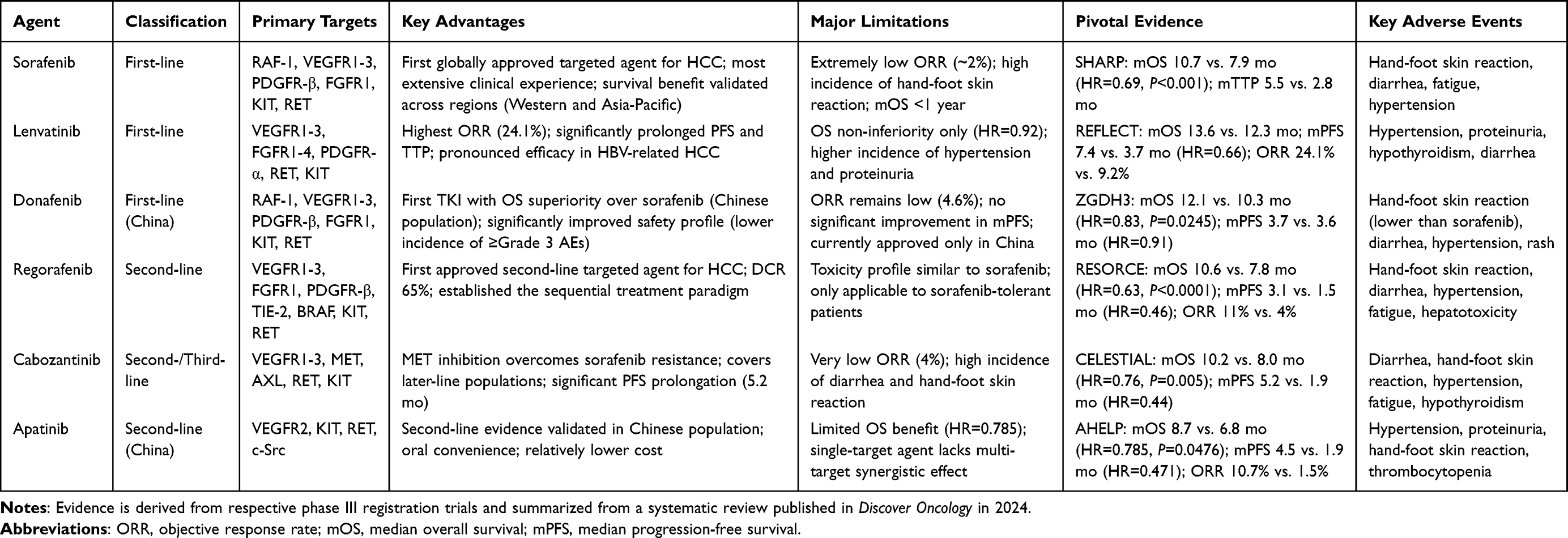 |
Table 3 Comprehensive Comparison of Tyrosine Kinase Inhibitors (TKIs) Approved for the Systemic Treatment of Advanced Hepatocellular Carcinoma |
TACE Combined with Immunotherapy: Synergistic Mechanisms and Clinical Translation
The combination of TACE with immune checkpoint inhibitors (ICIs) has become a pivotal strategy for intermediate- to advanced-stage HCC, based on TACE’s ability to remodel the tumor immune microenvironment.41 Specifically, TACE triggers immunogenic cell death (ICD) via ischemic necrosis and concentrated chemotherapy, releasing tumor-associated antigens (TAAs) and damage-associated molecular patterns (DAMPs) that are captured by dendritic cells (DCs) and cross-presented to T cells, thereby priming tumor-specific immunity and establishing the foundation for subsequent ICIs.42 Concurrently, TACE-induced hypoxia upregulates PD-L1 on residual tumor cells and PD-1 on infiltrating T cells via the HIF-1α pathway. This dual effect both facilitates tumor immune evasion and provides accessible targets for ICIs, rendering the post-TACE period an ideal therapeutic window for PD-1/PD-L1 inhibition.43 The synergy of TACE with immunotherapy involves immunogenic cell death, antigen release, dendritic cell activation, and immune microenvironment remodeling (Figure 1). At the microenvironmental level, TACE increases intratumoral CD8+ T and NK cells while reducing Tregs and MDSCs, shifting cold tumors to hot tumors.44 T-cell receptor (TCR) repertoire analyses show that TACE plus immunotherapy expands TCR clonal diversity, helping overcome antigen escape under monotherapy.45 By blocking PD-1/PD-L1, ICIs reverse T-cell exhaustion and promote memory T-cell formation, generating systemic and durable antitumor immunity beyond local TACE effects.45
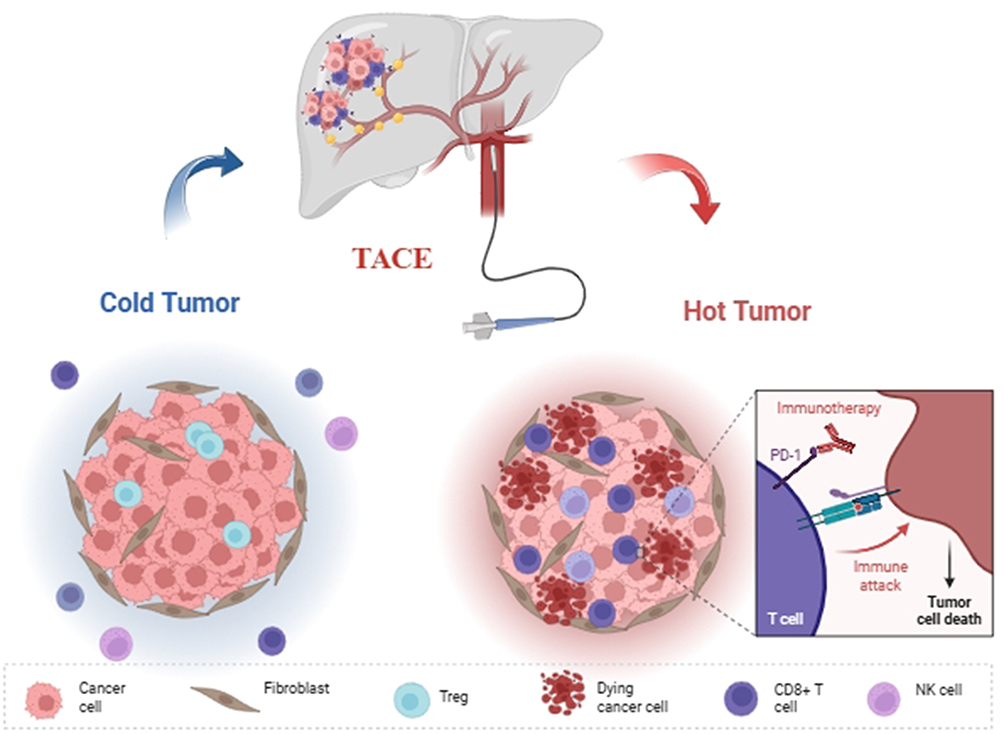 |
Figure 1 Mechanisms of TACE-ICI synergy. TACE triggers immunogenic cell death, releasing tumor antigens that prime dendritic cells and T cells. It also upregulates PD-L1 on residual tumor cells via HIF-1α, creating a therapeutic window for immune checkpoint inhibitors. The combination converts an immunosuppressive “cold” microenvironment into a “hot” immune-active state. Abbreviations: TACE, transarterial chemoembolization; ICI, immune checkpoint inhibitor; NK, natural killer cell; Treg, regulatory T cell; PD-1, programmed death-1; PD-L1, programmed death-ligand 1. |
These mechanisms are supported by Phase III trials. EMERALD-1 showed that TACE plus durvalumab and bevacizumab prolonged PFS versus TACE alone (15.0 vs 8.2 months; HR 0.77),46 and LEAP-012 confirmed that adding lenvatinib and pembrolizumab to TACE improved median PFS (14.6 vs 10.0 months; HR 0.66; P=0.0002).47 Notably, in the PETAL trial, TACE followed by pembrolizumab yielded an ORR of 53% and a median OS of 33.5 months, without a significant increase in synergistic toxicity.48,49 Collectively, these data establish the important role of TACE plus immunotherapy in HCC management. Future efforts using liquid biopsy to dynamically monitor post-TACE antigen release and PD-L1 expression may enable individualized timing of combination therapy. Table 4 summarizes approved ICI-based regimens to guide regimen selection. The underlying synergy involves ICD, antigen release, DC activation, and TME remodeling (Figure 1). The TME, which comprises tumor, stromal, and immune cells, drives HCC progression and resistance, and TACE-based combinations exert multi-nodal regulatory effects within this network (Figure 2).
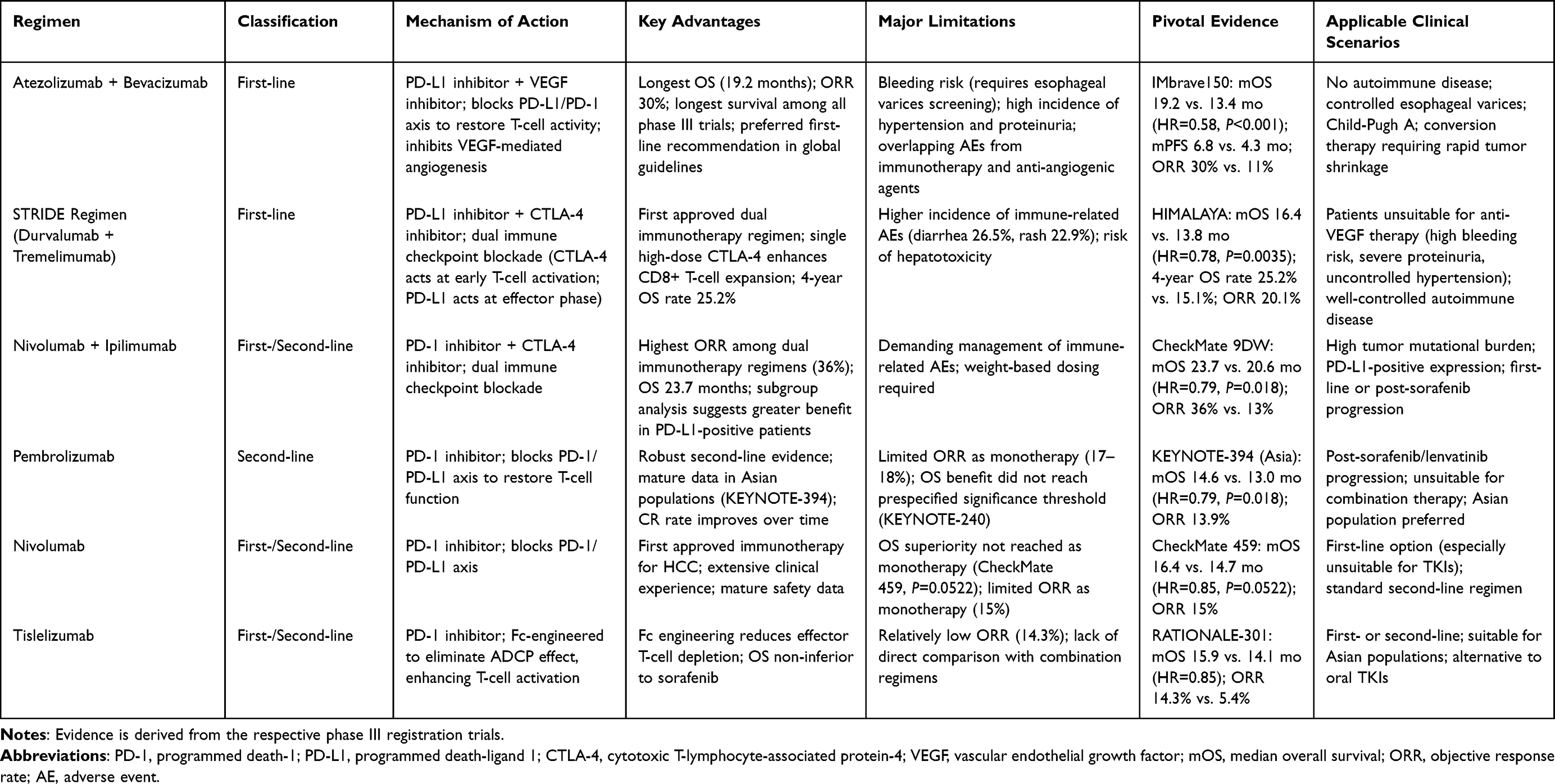 |
Table 4 Comprehensive Comparison of Immune Checkpoint Inhibitor-Based Regimens Approved for the Systemic Treatment of Advanced Hepatocellular Carcinoma |
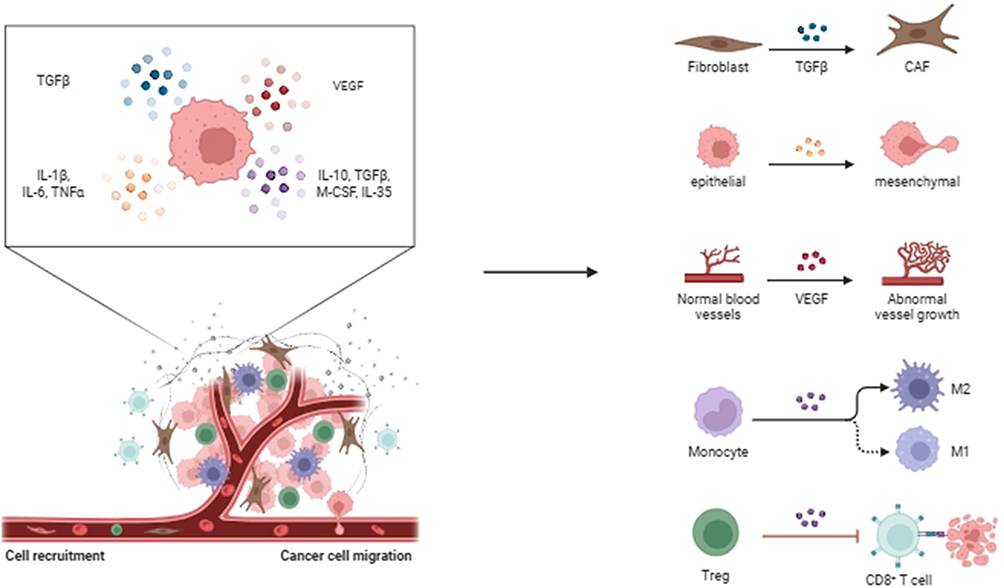 |
Figure 2 Tumor microenvironment (TME) modulation by TACE-based combination therapy. The TME contains tumor cells, cancer-associated fibroblasts (CAFs), and immune cells. TACE-induced hypoxia upregulates VEGF and immunosuppressive cytokines (e.g, TGF-β, IL-10), which promote CAF activation, epithelial-mesenchymal transition (EMT), abnormal angiogenesis, and polarization of macrophages toward an M2-like phenotype, along with recruitment of regulatory T cells (Tregs). Tyrosine kinase inhibitors block VEGFR signaling, reducing angiogenesis and immune suppression. Immune checkpoint inhibitors reactivate exhausted CD8⁺ T cells. The combination strategy aims to reprogram the TME into an anti-tumor state. Abbreviations: TGF-β, transforming growth factor-β; IL, interleukin; VEGF, vascular endothelial growth factor; EMT, epithelial-mesenchymal transition; Treg, regulatory T cell; CAF, cancer-associated fibroblast. |
TACE Combined with Targeted Therapy and Immunotherapy: Advances in Triplet Regimens
The triplet regimen (TACE+TKI+ICI) is among the most actively investigated strategies for intermediate to advanced HCC, leveraging complementary synergy: TACE induces ICD and antigen release, TKIs suppress post-TACE VEGF-driven angiogenesis, and ICIs reverse T-cell exhaustion to amplify systemic immunity.50,51 The phase III LEAP-012 trial first evaluated lenvatinib plus pembrolizumab with TACE in unresectable, non-metastatic HCC, meeting its primary PFS endpoint (14.6 vs 10.0 months; HR 0.66; P=0.0002) and receiving regulatory approval in China in 2025. However, OS did not reach statistical significance, leading to trial termination and suggesting that triplet therapy’s PFS benefit may be confounded by competing risks such as liver disease progression.47
In contrast, the CHANCE2202 study (941 patients) showed that TACE plus ICIs and anti-angiogenic agents significantly prolonged OS (32.9 vs 23.0 months; HR 0.57) and PFS (18.0 vs 12.9 months; HR 0.70) versus TACE alone, with acceptable grade ≥3 adverse events (20.8% vs 6.8%). A network meta-analysis (45 studies, mostly retrospective, 4738 patients) suggested that TACE+TKI+ICI may be superior to TACE+TKI doublet in PFS and ORR, but findings require prospective validation. In the same analysis, tislelizumab-containing triplet was associated with median PFS 11.7 months, ORR 72%, and safety SUCRA 0.426, while toripalimab-containing triplet showed the most favorable OS performance (SUCRA 0.981).50 These SUCRA rankings are exploratory and not equivalent to direct comparative evidence.
For conversion therapy, a study of 57 BCLC B/C uHCC patients reported a conversion resection rate of 14.0% and disease control rate of 66.7% with triplet therapy, with resected patients achieving superior OS. A pooled analysis of 560 conversion cases further supported triplet’s advantage over TACE alone, TKI alone, or TKI+ICI doublet.50 In a propensity score-matched study of 278 patients with high-tumor-burden uHCC, triplet therapy (TACE/HAIC+lenvatinib+PD-1 inhibitor) significantly prolonged OS (22.4 vs 17.6 months; HR 0.55) and PFS (13.5 vs 8.5 months; HR 0.53) versus doublet (TACE/HAIC+lenvatinib), without increasing early liver function deterioration, suggesting high-tumor-burden patients may benefit preferentially.52
It is noteworthy that the efficacy of different ICI agents within triplet regimens varies. The SUCRA rankings from the network meta-analysis, despite the limitations discussed in Evidence Quality Assessment., suggest that tislelizumab and toripalimab demonstrate superior performance in terms of PFS and ORR, and OS, respectively. These observations are hypothesis-generating and require prospective head-to-head comparisons. Given the predominantly retrospective nature of available studies, the optimal drug combination remains unclear, and future trials should address TACE timing (concurrent vs sequential), TKI dosing, and ICI duration.50
In summary, TACE+TKI+ICI triplet therapy represents a paradigm shift toward deeper integration of locoregional and systemic therapy. Although LEAP-012’s OS results temper enthusiasm, data from CHANCE2202 and meta-analyses support its PFS, ORR, and conversion therapy benefits. Future directions include biomarker-driven patient selection, optimal sequencing and timing, and novel ICI agents. Individualized decision-making based on tumor burden, liver function, vascular invasion, and tolerance is key (Figure 3).
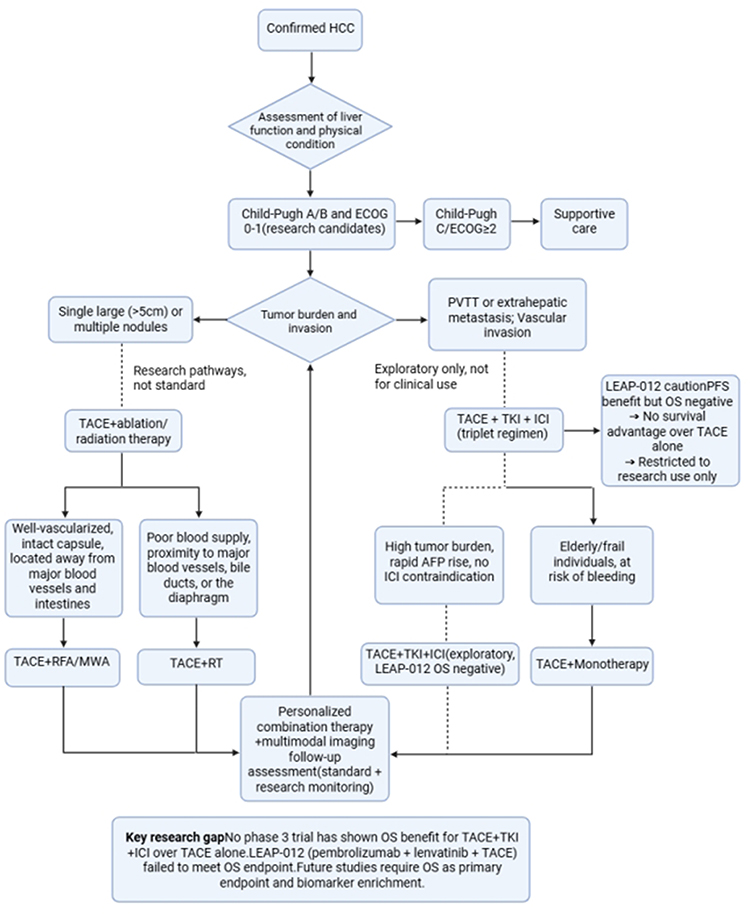 |
Figure 3 Hypothetical research framework to guide future investigation of triplet therapy (TACE + TKI + ICI) in hepatocellular carcinoma. This framework is not intended for clinical decision-making. It incorporates the negative overall survival result of the phase 3 LEAP-012 trial (pembrolizumab + lenvatinib + TACE) as a cautionary constraint. Solid arrows represent established treatment options supported by prospective data. Dashed arrows indicate exploratory, unvalidated relationships. The triplet pathway is hypothesis-generating only and should be restricted to prospective randomized controlled trials with overall survival as the primary endpoint, ideally with biomarker stratification. All patient selection criteria depicted are illustrative and require prospective validation. Abbreviations: ECOG, Eastern Cooperative Oncology Group; PVTT, portal vein tumor thrombus; RFA, radiofrequency ablation; MWA, microwave ablation; RT, radiotherapy; PEI, percutaneous ethanol injection; TKI, tyrosine kinase inhibitor; AFP, alpha-fetoprotein. |
Advances in Novel Smart Embolic Materials for TACE
TACE efficacy depends on embolic agent properties. Conventional agents (Lipiodol, gelatin sponge, PVA, drug-eluting beads) have inherent limitations: Lipiodol is readily washed out, gelatin sponge degrades uncontrollably within days, drug-eluting beads lack precise release kinetics, and most lack intrinsic imaging capability for real-endpoint assessment.52 Conventional materials provide only passive embolization without actively modulating post-TACE TME remodeling, a limitation magnified in the combination therapy era. Compensatory responses (hypoxia-driven angiogenesis, immunosuppressive cell infiltration, cancer stem cell enrichment) compromise embolic efficacy and may reduce sensitivity to subsequent systemic therapies.53 Thus, material innovation has shifted from better embolization to smarter microenvironment modulation, heralding smart hydrogels as next-generation embolic agents. These hydrogels reshape TACE through tunable properties, stimulus responsiveness, and enhanced imaging.54 Adjusting crosslinking density and polymer composition enables precise control over swelling, mechanical strength, and degradation rate to match vessels of varying calibers. Unlike preformed microspheres, hydrogels can undergo in situ gelation, achieving deep embolization from terminal arterioles to capillaries while reducing collateral circulation risk. TME features such as temperature, pH, and ROS have been exploited to design responsive hydrogel systems.55 These materials exploit TME features such as low pH, high reducing capacity, or aberrant enzyme expression, remaining in sol state systemically and undergoing sol-gel transition upon tumor-specific stimuli for on-demand embolization. The thermosensitive nanogel Embogel is a landmark example: flowable at room temperature (≈230 nm), it undergoes hydrophilic-to-hydrophobic phase transition at body temperature (37 °C), reducing particle size to 80 nm and forming a 3D gel network that occludes 20–800 μm vessels for conformal embolization.53 In a preliminary study of 10 patients with intermediate- to advanced-stage HCC, Embogel-TACE achieved a 1-month DCR of 90% and ORR of 40%, with mild procedural pain and fewer adverse reactions than conventional TACE.53 For imaging, novel hydrogels incorporating contrast agents (tantalum nanoparticles or iodinated compounds via covalent or physical doping) enable multimodal imaging (CT, MRI, DSA), facilitating real-time intraprocedural navigation and postprocedural assessment.54 Recent multifunctional hydrogels have shifted from single-function embolization to embolization-chemotherapy-immunomodulation synergy. The raltitrexed-kaempferol-tantalum (RKT@gel) system self-assembles from raltitrexed fibers; kaempferol enhances mechanical properties and suppresses angiogenesis, while tantalum nanoparticles provide X-ray visibility and radiosensitization.56 RKT@gel goes beyond embolization by inducing ICD, promoting dendritic cell activation and antigen presentation; its immunostimulatory effect amplifies with radiotherapy, converting local embolization into systemic immune activation. Another example is Pt-P@PND thermosensitive nanogel, which undergoes sol-gel transition at body temperature to occlude vessels while releasing polyphosphate to activate coagulation, forming a gel-clot composite network that prolongs embolization and downregulates HIF-1α and VEGF.57 Hyaluronic acid-based degradable adhesive microspheres use CD44-mediated targeting to bind tumor endothelium; their elastic deformability enables tight packing (void fraction 28%), increasing embolization density versus commercial Embosphere. Separately, oxygen-carrying magnetocaloric drug-eluting beads directly supply oxygen and enhance its penetration via magnetocaloric effect, reversing post-TACE hypoxia-mediated chemoresistance.58
Unlike Lipiodol (washed out within 48 hours) and PVA particles (100–300 μm, cannot reach small arterioles), smart hydrogels resolve the flowability-embolization paradox via in situ sol-gel transition: low viscosity at room temperature ensures delivery, and body-temperature gelation provides durable conformal embolization.52 However, challenges remain, including batch-to-batch consistency, long-term safety, workflow compatibility, and regulatory pathways.53
Smart embolic materials will reshape HCC treatment. Embogel’s X-ray visibility enables real-time monitoring to avoid ectopic embolization.54 Multifunctional integration allows a single TACE procedure to achieve vessel occlusion, sustained chemotherapy, microenvironment modulation, and immune activation, potentially elevating TACE from palliative to curative. Degradable materials (eg, 3Asphere, >90% degradation within 8 weeks) restore vessel patency for repeated procedures. Future directions include nanocomposite systems for programmed TME responses, theranostic platforms integrating imaging and therapy, immunomodulatory materials leveraging post-TACE immune dynamics, and individualized material selection via radiomics and liquid biopsy.53 In summary, ongoing innovation in smart embolic materials and optimization of combination strategies will bidirectionally empower each other: novel materials enhance drug delivery and microenvironment modulation, while clinical needs guide material design. Their convergence will advance HCC management toward precision-guided intervention (Table 5).
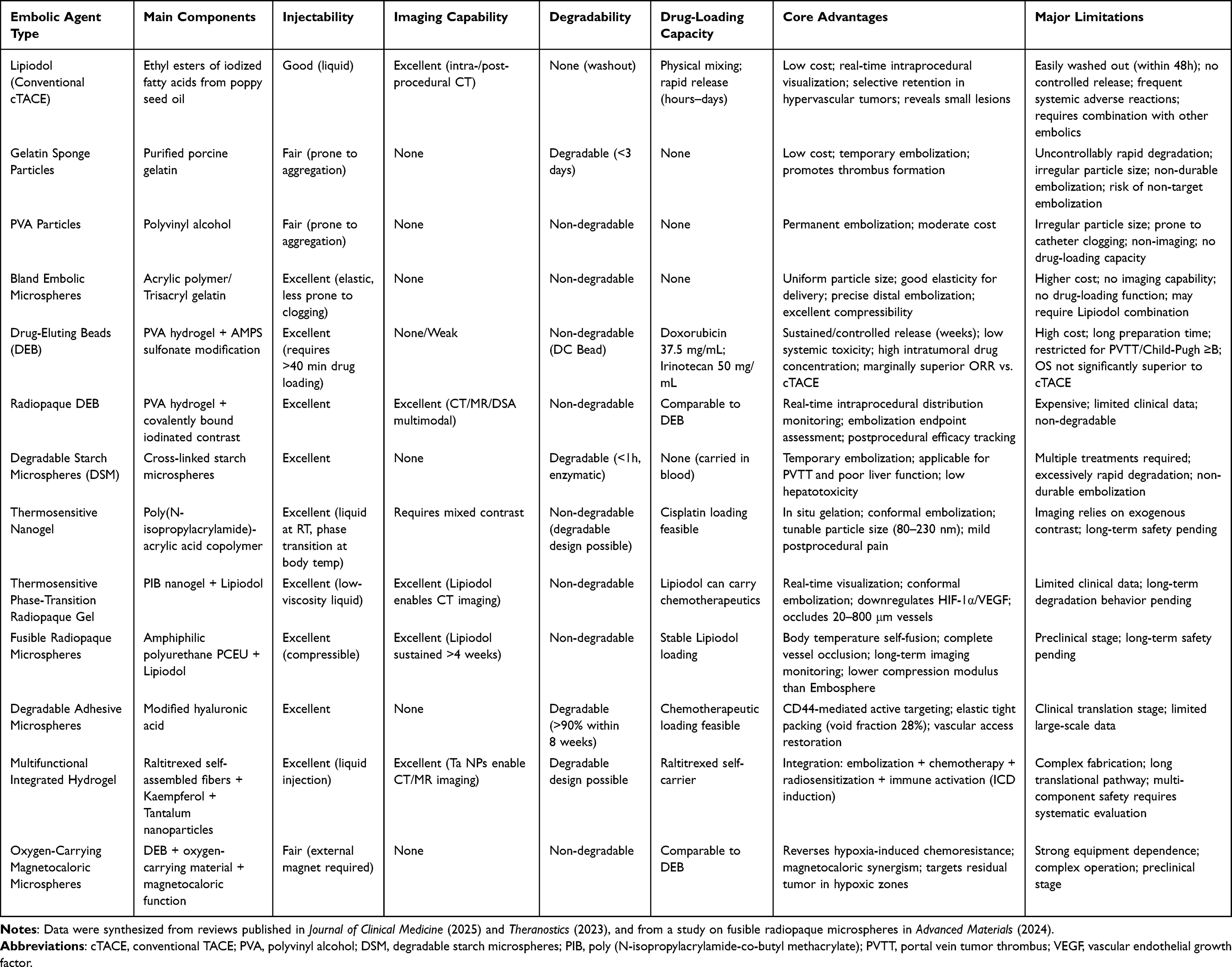 |
Table 5 Comprehensive Comparison of Conventional and Novel Embolic Agents Employed in Transarterial Chemoembolization for Hepatocellular Carcinoma |
Translational Challenges and Unmet Needs
Despite the promise of smart embolic materials, several barriers hinder clinical adoption. First, long-term safety data are sparse; most studies report only short-term outcomes, leaving chronic tissue responses, degradation product toxicity, and delayed foreign-body reactions uncharacterized. For in situ gelling materials, systemic biodistribution and cumulative organ effects warrant particular scrutiny.59–61 Second, manufacturing consistency is a hurdle. Many stimuli-responsive hydrogels require complex, multi-step synthesis that is difficult to standardize across batches, and quality control frameworks remain underdeveloped.62 Third, economic viability has received little attention. Next-generation agents may substantially increase procedural costs, yet formal health-economic analyses (cost-effectiveness, budget impact) are lacking.63–67 A comparative assessment of these translational parameters across different embolic platforms is provided in Table 6. Until these evidence gaps are addressed, enthusiasm for smart embolic materials must be tempered.
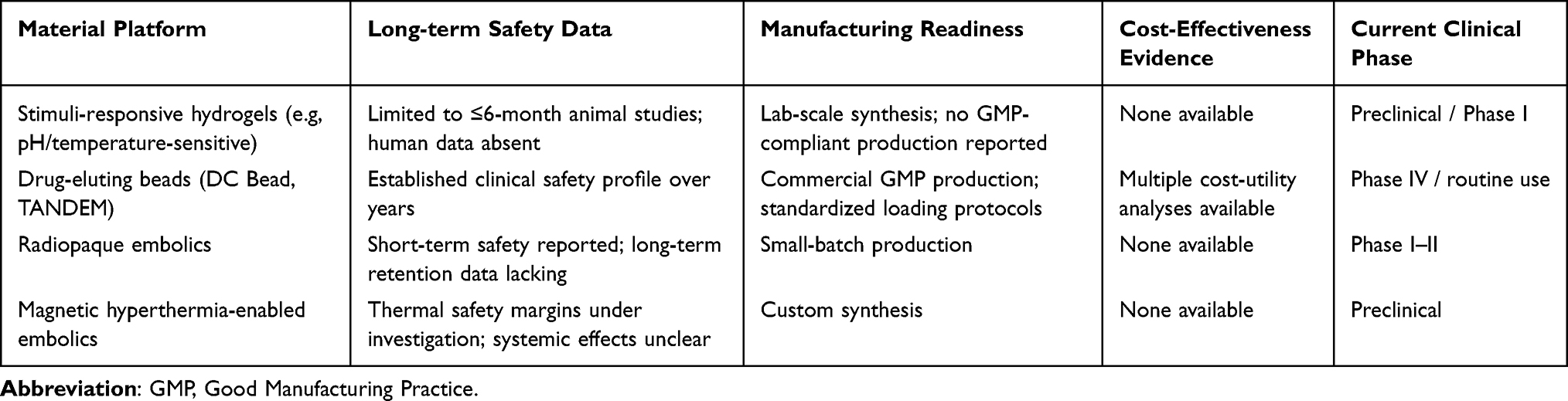 |
Table 6 Comparative Assessment of Translational Readiness Across Embolic Material Platforms for HCC |
Discussion
This review has systematically examined two parallel and evolving research trajectories, namely TACE-based combination therapy and smart embolic materials, and has sought to integrate them within the unifying framework of moving from combination to integration. The current therapeutic landscape of intermediate- to advanced-stage HCC is undergoing profound transformation. On the one hand, strategies combining TACE with locoregional ablation, RT, targeted therapy, and immunotherapy have progressed from single-center experiential accumulation to multicenter phase III evidence-based validation.11 On the other hand, the inherent limitations of conventional embolic agents have catalyzed a wave of innovation in novel embolic materials, exemplified by smart hydrogels. Nevertheless, the cross-fertilization between these two domains remains in its infancy, and several critical issues warrant in-depth discussion.
Although network meta-analyses have provided quantitative evidence for ranking the efficacy of different combination regimens, substantial heterogeneity among the included studies must be acknowledged. Differences in patient selection (tumor stage, liver function, etiology), TACE technique (conventional vs. DEB-TACE, number of sessions), and outcome definitions (PFS vs. TTP, ORR criteria) preclude definitive quantitative synthesis across all comparisons. Most network meta-analyses cited herein are based on aggregate rather than individual patient data, limiting the ability to explore effect modifiers. A recent pooled analysis (which included both prospective and retrospective studies) encompassing 20 studies with 5485 patients suggested that TACE combined with systemic therapy may be associated with improved OS (HR, 0.75) and PFS (HR, 0.57). Given the heterogeneity in patient selection and treatment protocols, these estimates should be interpreted with caution and are not directly comparable across different regimens. However, the enrolled populations exhibited marked heterogeneity in tumor stage, hepatic functional reserve, and prior treatment history.57 Several observations offer directional guidance for clinical decision-making. TACE plus RFA yields the highest disease control rate (SUCRA, 0.836), TACE plus HIFU achieves the highest 1-year and 2-year survival rates (SUCRA exceeding 0.91), and TACE plus RT demonstrates pronounced superiority in patients with concurrent portal vein tumor thrombus.25 Nevertheless, these findings do not yet provide a definitive answer to the question of which patient should receive which combination regimen at which time point. Future research efforts should be directed toward constructing therapeutic response prediction models that integrate radiomics, liquid biopsy, and immune microenvironment profiling. This approach would upgrade recommendations based on population-averaged effects to decisions grounded in individual biological characteristics.
The preponderance of Chinese trials and domestically developed agents (donafenib, tislelizumab, toripalimab) in the cited literature warrants comment. While these studies provide high-volume real-world data from HBV-endemic regions, the relative underrepresentation of Western pivotal trials reflects both the rapid pace of HCC research in Asia and regional availability of certain agents. This geographic distribution may influence the generalizability of our synthesis to populations with different etiologies (NASH-related HCC) or healthcare systems. Ongoing global phase III trials and collaborative international registries are needed to validate the applicability of these findings across diverse settings.
The triplet regimen represents the highest-intensity combination strategy in the comprehensive management of HCC, yet its clinical value remains a subject of ongoing debate.50 The LEAP-012 trial demonstrated a significant PFS benefit (14.6 months versus 10.0 months; HR, 0.66) but did not meet its prespecified OS endpoint, a finding that tempers enthusiasm for universal adoption of triplet therapy. Without OS superiority in some phase III trials, triplet therapy should be considered investigational or reserved for highly selected patients with preserved liver function and high tumor burden. This finding contrasts sharply with the CHANCE2202 study, which reported significantly prolonged OS (32.9 months versus 23.0 months; HR, 0.57).47 A recent pooled analysis pooling three phase III trials, namely EMERALD-1, LEAP-012, and TALENTACE, demonstrated consistent PFS benefit for triplet therapy over TACE alone (HR, 0.69).48 However, OS data remain immature, and the risk of grade 3 or higher adverse events was increased by 88%, underscoring the imperative to carefully manage toxicity while pursuing maximal therapeutic efficacy. This discrepancy may be attributable to several factors. First, differences exist between prospective RCTs and real-world studies in the severity of underlying liver disease, accessibility of subsequent therapies, and duration of follow-up. Second, heterogeneity in the efficacy of different ICI agents within triplet regimens precludes definitive identification of the optimal drug combination. SUCRA rankings from network meta-analyses suggest that tislelizumab and toripalimab demonstrate superior performance in terms of PFS and ORR, and OS, respectively.44 However, the predominance of retrospective data and the absence of head-to-head comparisons limit the strength of these observations. Third, the impact of TACE timing relative to systemic therapy, whether concurrent or sequential, on synergistic effects remains to be fully elucidated. Furthermore, the additive toxicity of triplet therapy necessitates careful assessment of patient tolerance while pursuing maximal therapeutic efficacy. Reported rates of grade 3 or higher adverse events reach 20.8%. For the favorable subgroup characterized by high tumor burden, rapidly rising alpha-fetoprotein (AFP), and well-preserved hepatic functional reserve, the benefit-risk ratio of triplet therapy may be optimal. Conversely, for elderly patients or those with marginal liver function, de-escalation strategies may be more appropriate. These strategies include TACE plus TKI doublet therapy or sequential TACE followed by ICI.50
As noted by Liu et al in a recent comprehensive review, hydrogel-based embolic agents have demonstrated impressive performance in preclinical studies. However, their clinical translation continues to face multifaceted challenges. Key translational barriers include ensuring batch-to-batch consistency under GMP conditions, verifying the long-term safety of degradation products in large animal models, achieving seamless compatibility with existing TACE workflows, and demonstrating cost-effectiveness relative to conventional agents. Without rigorous health-economic validation, the incremental clinical benefit of multifunctional smart hydrogels may not justify their higher upfront costs.53 First, batch-to-batch consistency in large-scale production constitutes a critical threshold for regulatory approval. Specifically, the quality congruence between laboratory-scale synthesis and GMP-grade manufacturing must be rigorously ensured. Second, long-term safety requires systematic evaluation in large animal models and long-term follow-up studies. Key considerations include the metabolic fate of degradation products from degradable materials and the long-term impact of retained non-degradable materials on the vessel wall and surrounding tissues. Third, compatibility with conventional TACE procedural workflows will determine the ease of clinical adoption. The degree to which the injection parameters of novel materials, such as flow rate, pressure, and temperature control, align with existing catheter systems is particularly important.53 Fourth, cost-effectiveness remains a critical consideration. Multifunctional integration inevitably escalates material costs, and real-world studies are needed to verify whether the incremental clinical benefit over conventional embolic agents justifies the price premium.
The multidisciplinary integration paradigm proposed herein centers on dismantling disciplinary silos to achieve knowledge translation and workflow reconfiguration. At the pre-procedural planning level, radiomics can extract features related to tumor vascularity, necrotic propensity, and immune microenvironment phenotype, thereby providing quantitative parameters to guide embolic agent selection and combination regimen decision-making. At the intra-procedural execution level, the imaging visibility characteristics of novel embolic materials enable real-time navigation and precise determination of the embolization endpoint. At the post-procedural assessment level, liquid biopsy dynamically monitors minimal residual disease and immune response status, thereby informing the timing and intensity adjustments of subsequent systemic therapy. Achieving this closed-loop system necessitates the establishment of a regularized collaborative mechanism involving interventional radiology, diagnostic imaging, medical oncology, biomaterials science, and basic research teams. Such a mechanism entails not merely an additive aggregation of consultations but rather deep integration across case discussion, regimen formulation, and therapeutic efficacy evaluation.
Limitations
This review has several limitations that merit explicit discussion. First, although we have systematically synthesized the clinical evidence for TACE-based combination therapies, the source studies aggregated in the cited network meta-analyses are predominantly retrospective and single-arm in design. These studies exhibit substantial heterogeneity in patient selection criteria, TACE protocols, and endpoint definitions, which may introduce confounding that cannot be fully resolved by meta-analytical techniques. Consequently, the pooled effect estimates should be interpreted as hypothesis-generating rather than definitive, and their conclusions require validation in prospective randomized trials.
Second, the network meta-analyses cited herein rely on aggregate data rather than individual patient data. This precludes the exploration of key effect modifiers, including tumor burden, hepatic functional reserve, and the etiology of underlying liver disease, all of which may fundamentally influence both the efficacy and safety of combination strategies. Given the increasing recognition that viral versus non-viral HCC etiologies are associated with distinct tumor immune microenvironments, this represents a critical gap in the current evidence.
Third, many of the novel smart embolic materials discussed, particularly stimuli-responsive hydrogels, remain in preclinical or early-phase clinical development. Critical translational parameters, including long-term in vivo safety, batch-to-batch manufacturing consistency, sterilization compatibility, and formal cost-effectiveness analyses, have not been systematically evaluated across material platforms. These gaps represent substantial barriers to regulatory approval and clinical adoption that are frequently underappreciated in the biomaterial literature. Without rigorous head-to-head comparisons of these parameters, claims regarding the clinical superiority of one material over another remain premature.
Fourth, the rapid evolution of systemic therapy options for HCC, with new immune checkpoint inhibitors, bispecific antibodies, and combination regimens continuously emerging, means that the optimal combination partners and sequencing strategies for TACE will likely continue to shift. The evidence synthesized herein therefore represents a snapshot of a rapidly moving field.
Fifth, the multidisciplinary integration paradigm proposed in this review, while conceptually grounded in the converging trajectories of interventional oncology, diagnostic imaging, and biomaterials science, remains untested in real-world clinical workflows. Its feasibility, cost-effectiveness, and incremental benefit over standard multidisciplinary team approaches await empirical validation, as exemplified by the negative overall survival outcome in the LEAP-012 trial, which underscores the caution required when translating promising concepts into practice.
In summary, future research should address these limitations through prospective, biomarker-enriched randomized trials that evaluate both oncologic outcomes and patient-centered endpoints. Rigorous health-economic analyses that systematically assess the value proposition of novel embolic technologies and combination strategies, including comparative assessments of long-term safety, manufacturing consistency, and cost-effectiveness, are equally essential to bridge the gap between technical innovation and clinical implementation.
Conclusion
The ongoing development of TACE-based combination therapy and smart embolic materials may reshape the diagnostic and therapeutic landscape, but definitive conclusions are constrained by the heterogeneity and retrospective nature of most available evidence. The most distinctive contribution of this review is the articulation of a multidisciplinary integration paradigm that converges interventional radiology, diagnostic imaging, and biomaterials science. Under this paradigm, the synergistic development of TACE-based combination therapy and smart embolic materials reconfigures the management of intermediate to advanced HCC.
In the domain of combination therapy, TACE plus locoregional ablation or radiotherapy offers spatial complementarity, while TACE plus targeted agents or immunotherapy remodels the tumor microenvironment. The triplet regimen has shown a progression-free survival benefit in exploratory analyses, but its overall survival advantage remains unproven, as highlighted by the negative OS outcome of the LEAP-012 trial.47 In the domain of embolic materials, smart hydrogels enable active microenvironmental modulation, with preliminary clinical data supporting their feasibility.
What this paradigm means in practice. Implementation would reconfigure HCC workflows across three stages. Preprocedural planning should integrate radiomics and liquid biopsy for patient selection. Intraprocedural execution should use imaging-visible embolic materials for real-time navigation. Postprocedural assessment should employ dynamic immune profiling to guide subsequent therapy. Empirical evidence supports such integration: a meta-analysis of 13 studies demonstrated that multidisciplinary team care reduces mortality in patients with liver cancer.68
Priority unanswered questions. Despite the progress summarized in this review, several critical knowledge gaps remain to be addressed. First, whether biomarker-enriched patient selection can improve overall survival in triplet therapy warrants prospective investigation, particularly given the negative LEAP-012 result. Second, the incremental clinical benefit of smart embolic materials relative to their added complexity and cost requires formal health-economic evaluation. Third, the optimal timing of TACE within multidisciplinary workflows should be defined to maximize synergy and minimize toxicity. Fourth, etiology-based stratification (viral versus NASH-associated HCC) holds promise for improving combination therapy selection, but its utility requires prospective validation.7 Fifth, the balance between treatment intensity and patient tolerance, especially in elderly or frail individuals, needs to be carefully characterized. Sixth, regulatory frameworks that facilitate the clinical translation of smart embolic materials while ensuring patient access and cost-effectiveness remain to be established. Prospective, standardized trials with OS as the primary endpoint are urgently needed. Until such evidence emerges, current comparative estimates should be considered hypothesis generating rather than practice changing.
Data Sharing Statement
No new data were generated or analyzed in this study. Data sharing is not applicable to this article.
Ethics Approval
Ethical approval was not required for this review as it does not involve original human or animal data.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Reig M, Forner A, Rimola J, et al. BCLC strategy for prognosis prediction and treatment recommendation: the 2022 update. J Hepatol. 2022;76(3):681–19. doi:10.1016/j.jhep.2021.11.018
2. Bruix J, Reig M, Sherman M. Evidence-based diagnosis, staging, and treatment of patients with hepatocellular carcinoma. Gastroenterology. 2016;150(4):835–853. doi:10.1053/j.gastro.2015.12.041
3. Kudo M, Kawamura Y, Hasegawa K, et al. Management of hepatocellular carcinoma in Japan: JSH consensus statements and recommendations 2021 update. Liver Cancer. 2021;10(3):181–223. doi:10.1159/000514174
4. Forner A, Gilabert M, Bruix J, Raoul J. Treatment of intermediate-stage hepatocellular carcinoma. Nat Rev Clin Oncol. 2014;11(9):525–535. doi:10.1038/nrclinonc.2014.122
5. Kudo M, Ueshima K, Ikeda M, et al. Randomised, multicentre prospective trial of transarterial chemoembolisation (TACE) plus sorafenib as compared with TACE alone in patients with hepatocellular carcinoma: TACTICS trial. Gut. 2020;69(8):1492–1501. doi:10.1136/gutjnl-2019-318934
6. Duan R, Gong F, Wang Y, et al. Transarterial chemoembolization (TACE) plus tyrosine kinase inhibitors versus TACE in patients with hepatocellular carcinoma: a systematic review and meta-analysis. World J Surg Oncol. 2023;21(1):120. doi:10.1186/s12957-023-02961-7
7. Pfister D, Nunez NG, Pinyol R, et al. NASH limits anti-tumour surveillance in immunotherapy-treated HCC. Nature. 2021;592(7854):450–456. doi:10.1038/s41586-021-03362-0
8. Dolphin J, Zubillaga J, Jamal QM, et al. Optimizing transarterial chemoembolization in hepatocellular carcinoma: current strategies, innovations, and future directions. Cureus. 2025;17(10):e95128. doi:10.7759/cureus.95128
9. Su J, Su Y, Mai R, et al. Comparative efficacy of combination regimens based on interventional therapy and immune checkpoint inhibitors (ICIs) in patients with intermediate- and advanced-stage hepatocellular carcinoma: a systematic review, meta-analysis, and network meta-analysis. Cancer Immunol Immunother. 2026;75(3):67. doi:10.1007/s00262-025-04251-5
10. Wang L, Luo B, Zhao M, Shen J. Transarterial chemoembolization combined with immunotherapy and targeted therapy as first-line treatment for unresectable and non-metastatic hepatocellular carcinoma: a meta-analysis of phase III trials. Ther Adv Gastroenterol. 2025;18:1128579400. doi:10.1177/17562848251396424
11. Patel KR, Menon H, Patel RR, Huang EP, Verma V, Escorcia FE. Locoregional therapies for hepatocellular carcinoma: a systematic review and meta-analysis. JAMA Netw Open. 2024;7(11):e2447995. doi:10.1001/jamanetworkopen.2024.47995
12. Kim YR, Kim E, Kim HI, Han S, An J, Shim JH. Updated network meta-analysis of first-line systemic treatments for advanced HCC: consistent role of TACE. Liver Cancer. 2026;15(1):117–134. doi:10.1159/000546697
13. Wu H, Lv S, Zhang R, et al. Next-generation flexible embolic systems: targeted transarterial chemoembolization strategies for hepatocellular carcinoma. Adv Mater. 2025;37(24):e2503971. doi:10.1002/adma.202503971
14. Yuan G, Liu Z, Wang W, et al. Multifunctional nanoplatforms application in the transcatheter chemoembolization against hepatocellular carcinoma. J Nanobiotechnol. 2023;21(1):68. doi:10.1186/s12951-023-01820-7
15. Peng Y, Liu H, Liang X, et al. Self-assembling chemodrug fiber-hydrogel for transarterial chemoembolization and radiotherapy-enhanced antitumor immunity. J Control Release. 2025;380:1–16. doi:10.1016/j.jconrel.2025.01.088
16. Ades AE, Welton NJ, Dias S, Phillippo DM, Caldwell DM. Twenty years of network meta-analysis: continuing controversies and recent developments. Res Synth Meth. 2024;15(5):702–727. doi:10.1002/jrsm.1700
17. Lunny C, Veroniki A, Higgins JPT, et al. Methodological review of NMA bias concepts provides groundwork for the development of a list of concepts for potential inclusion in a new risk of bias tool for network meta-analysis (RoB NMA Tool). Syst Rev. 2024;13(1):25. doi:10.1186/s13643-023-02388-x
18. Hassan IN. Critical commentary on camrelizumab-based triple therapy for unresectable hepatocellular carcinoma. Ann Hepatol. 2025;30(2):101940. doi:10.1016/j.aohep.2025.101940
19. Yu H, Bai Y, Xie X, Feng Y, Yang Y, Zhu Q. RECIST 1.1 versus mRECIST for assessment of tumour response to molecular targeted therapies and disease outcomes in patients with hepatocellular carcinoma: a systematic review and meta-analysis. BMJ Open. 2022;12(6):e52294. doi:10.1136/bmjopen-2021-052294
20. Takayasu K, Arii S, Ikai I, et al. Prospective cohort study of transarterial chemoembolization for unresectable hepatocellular carcinoma in 8510 patients. Gastroenterology. 2006;131(2):461–469. doi:10.1053/j.gastro.2006.05.021
21. Liu Z, Gao F, Yang G, et al. Combination of radiofrequency ablation with transarterial chemoembolization for hepatocellular carcinoma: an up-to-date meta-analysis. Tumour Biol. 2014;35(8):7407–7413. doi:10.1007/s13277-014-1976-z
22. Kim HI, An J, Han S, Shim JH. Loco-regional therapies competing with radiofrequency ablation in potential indications for hepatocellular carcinoma: a network meta-analysis. Clin Mol Hepatol. 2023;29(4):1013–1028. doi:10.3350/cmh.2023.0131
23. Wang Y, Ma R, Wang Z, et al. Transcatheter arterial chemoembolization in combination with high-intensity focused ultrasound for intermediate and advanced hepatocellular carcinoma: a meta-analysis. Front Oncol. 2022;12:797349. doi:10.3389/fonc.2022.797349
24. Huo YR, Eslick GD. Transcatheter arterial chemoembolization plus radiotherapy compared with chemoembolization alone for hepatocellular carcinoma: a systematic review and meta-analysis. JAMA Oncol. 2015;1(6):756–765. doi:10.1001/jamaoncol.2015.2189
25. Le X, Feng J, Yu X, et al. A network meta-analysis of different interventional treatment strategies for unresectable hepatocellular carcinoma. BMC Gastroenterol. 2025;25(1):360. doi:10.1186/s12876-025-03980-2
26. Chen L, Wang L, Wang H. Comparison of stereotactic body radiotherapy following transcatheter arterial chemoembolization vs transcatheter arterial chemoembolization alone in hepatocellular carcinoma. World J Gastrointest Surg. 2025;17(10):105360. doi:10.4240/wjgs.v17.i10.105360
27. Li L, Zhang H, Zhao H, et al. Radiofrequency-thermal effect of cisplatin-crosslinked nanogels for triple therapies of ablation-chemo-embolization. Chem Eng J. 2022;450:138421. doi:10.1016/j.cej.2022.138421
28. Xu Z, Xie H, Zhou L, Chen X, Zheng S. The Combination Strategy of Transarterial Chemoembolization and Radiofrequency Ablation or Microwave Ablation against Hepatocellular Carcinoma. Anal Cell Pathol. 2019;2019:8619096. doi:10.1155/2019/8619096
29. Yang Y, Yu H, Qi L, et al. Combined radiofrequency ablation or microwave ablation with transarterial chemoembolization can increase efficiency in intermediate-stage hepatocellular carcinoma without more complication: a systematic review and meta-analysis. Int J Hyperthermia. 2022;39(1):455–465. doi:10.1080/02656736.2022.2048095
30. Sofuni A, Takeuchi H, Sugimoto K, Itoi T, Miyazawa H. High-intensity focused ultrasound treatment for hepatocellular carcinoma. J Med Ultrason. 2024. doi:10.1007/s10396-024-01469-1
31. Hu J, Mao H, He Y. Systematic review and meta-analysis of the efficacy and safety of high-intensity focused ultrasound combined with transarterial chemoembolization and transarterial chemoembolization alone in the treatment of liver cancer. Transl Cancer Res. 2022;11(6):1678–1688. doi:10.21037/tcr-22-1094
32. Wang S, Zhuang L, Meng Z. Hepatocellular carcinoma more than 3 cm in diameter: a systematic review of transcatheter arterial chemoembolization plus percutaneous ethanol injection versus transcatheter arterial chemoembolization alone. ISRN Gastroenterol. 2013;2013:526024. doi:10.1155/2013/526024
33. Feng W, Guo Y, Lu S, Yin Y, Xue T, Li Z. Transarterial chemoembolization combined with percutaneous ethanol injection for the treatment of hepatocellular carcinoma at high-risk areas. J Cancer Res Ther. 2025;21(2):395–400. doi:10.4103/jcrt.jcrt_2226_24
34. Chen Q, Chen S, Zhao M. The synergistic mechanisms and prospects of transarterial chemoembolization combined with immunotherapy for hepatocellular carcinoma. J Hepatocell Carcinoma. 2025;12:841–854. doi:10.2147/JHC.S514881
35. Kudo M, Ueshima K, Ikeda M, et al. Final results of TACTICS: a randomized, prospective trial comparing transarterial chemoembolization plus sorafenib to transarterial chemoembolization alone in patients with unresectable hepatocellular carcinoma. Liver Cancer. 2022;11(4):354–367. doi:10.1159/000522547
36. Kudo M, Finn RS, Qin S, et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: a randomised Phase 3 non-inferiority trial. Lancet. 2018;391(10126):1163–1173. doi:10.1016/S0140-6736(18)30207-1
37. Peng Z, Fan W, Zhu B, et al. Lenvatinib combined with transarterial chemoembolization as first-line treatment for advanced hepatocellular carcinoma: a Phase III, randomized clinical trial (LAUNCH). J Clin Oncol. 2023;41(1):117–127. doi:10.1200/JCO.22.00392
38. Qin S, Bi F, Gu S, et al. Donafenib versus sorafenib in first-line treatment of unresectable or metastatic hepatocellular carcinoma: a randomized, open-label, parallel-controlled Phase II-III trial. J Clin Oncol. 2021;39(27):3002–3011. doi:10.1200/JCO.21.00163
39. Abou-Alfa GK, Meyer T, Cheng A, et al. Cabozantinib in patients with advanced and progressing hepatocellular carcinoma. N Engl J Med. 2018;379(1):54–63. doi:10.1056/NEJMoa1717002
40. Bruix J, Qin S, Merle P, et al. Regorafenib for patients with hepatocellular carcinoma who progressed on sorafenib treatment (RESORCE): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2017;389(10064):56–66. doi:10.1016/S0140-6736(16)32453-9
41. Yang F, Xu G, Huang J, et al. Transarterial chemoembolization combined with immune checkpoint inhibitors and tyrosine kinase inhibitors for unresectable hepatocellular carcinoma: efficacy and systemic immune response. Front Immunol. 2022;13:847601. doi:10.3389/fimmu.2022.847601
42. Pinato DJ, Murray SM, Forner A, et al. Trans-arterial chemoembolization as a loco-regional inducer of immunogenic cell death in hepatocellular carcinoma: implications for immunotherapy. J Immunother Cancer. 2021;9(9). doi:10.1136/jitc-2021-003311.
43. Li J, Zhang Y, Hu L, et al. T-cell receptor repertoire analysis in the context of transarterial chemoembolization synergy with systemic therapy for hepatocellular carcinoma. J Clin Transl Hepatol. 2025;13(1):69–83. doi:10.14218/JCTH.2024.00238
44. Greten TF, Mauda-Havakuk M, Heinrich B, Korangy F, Wood BJ. Combined locoregional-immunotherapy for liver cancer. J Hepatol. 2019;70(5):999–1007. doi:10.1016/j.jhep.2019.01.027
45. Lei Y, Bai Y, Bai X, et al. TACE empowers immune checkpoint inhibitors and tyrosine kinase inhibitors in unresectable HCC: a multicenter retrospective study. J Cancer. 2025;16(8):2750–2761. doi:10.7150/jca.112706
46. Sangro B, Kudo M, Erinjeri JP, et al. Durvalumab with or without bevacizumab with transarterial chemoembolisation in hepatocellular carcinoma (EMERALD-1): a multiregional, randomised, double-blind, placebo-controlled, phase 3 study. Lancet. 2025;405(10474):216–232. doi:10.1016/S0140-6736(24)02551-0
47. Kudo M, Ren Z, Guo Y, et al. Transarterial chemoembolisation combined with lenvatinib plus pembrolizumab versus dual placebo for unresectable, non-metastatic hepatocellular carcinoma (LEAP-012): a multicentre, randomised, double-blind, phase 3 study. Lancet. 2025;405(10474):203–215. doi:10.1016/S0140-6736(24)02575-3
48. Llovet JM, Vogel A, Madoff DC, et al. Randomized Phase 3 LEAP-012 study: transarterial chemoembolization with or without lenvatinib plus pembrolizumab for intermediate-stage hepatocellular carcinoma not amenable to curative treatment. Cardiovasc Intervent Radiol. 2022;45(4):405–412. doi:10.1007/s00270-021-03031-9
49. Pinato DJ, D’Alessio A, Fulgenzi CAM, et al. Safety and preliminary efficacy of pembrolizumab following transarterial chemoembolization for hepatocellular carcinoma: the PETAL Phase Ib study. Clin Cancer Res. 2024;30(11):2433–2443. doi:10.1158/1078-0432.CCR-24-0177
50. Wang Z, Zhang C, Yin J, Li N. Conversion therapy with TACE, TKIs, and ICIs for unresectable BCLC stage B and C hepatocellular carcinoma. Front Immunol. 2025;16:1451965. doi:10.3389/fimmu.2025.1451965
51. Lu W, Li Z, Pan C, et al. Optimal sequencing of locoregional and systemic therapies for intermediate and advanced hepatocellular carcinoma: a network meta-analysis. J Cancer Res Clin Oncol. 2025;151(6):196. doi:10.1007/s00432-025-06233-7
52. Wang Z, Yan G, Ning Y, et al. Multifunctional luteolin-Fe@PVA microspheres for combined hepatocellular carcinoma treatment: embolization/sonodynamic/chemodynamic therapy. Appl Mater Today. 2025;46:102880. doi:10.1016/j.apmt.2025.102880
53. Liu Y, Liu J, Zheng C, Ma Z. Recent advances in embolic agents for transarterial chemoembolization of hepatocellular carcinoma. Adv Healthc Mater. 2026;15(10):e2566.
54. Owen J, Negussie AH, Burks SR, et al. Microbubbles bound to drug-eluting beads enable ultrasound imaging and enhanced delivery of therapeutics. Sci Rep. 2024;14(1):20929. doi:10.1038/s41598-024-71831-3
55. Shi D, Ren Y, Liu Y, et al. Temperature-sensitive nanogels combined with polyphosphate and cisplatin for the enhancement of tumor artery embolization by coagulation activation. Acta Biomater. 2024;185:240–253. doi:10.1016/j.actbio.2024.07.022
56. Guo J, Huang J, Huang Z, et al. Tumor vessel-adaptable adhesive and absorbable microspheres for sustainable transarterial chemoembolization therapy. Nat Commun. 2025;16(1):6239. doi:10.1038/s41467-025-61621-4
57. Liu Z, Zhong B, Wei G, Cheng J, Peng Z. Transarterial intervention therapy plus systemic therapy for unresectable hepatocellular carcinoma: a systematic review and meta-analysis. EngMedicine. 2025;2(3):100091. doi:10.1016/j.engmed.2025.100091
58. Huang J, Zhang W, Wu Y, et al. A study on overcoming Post-TACE drug resistance in HCC based on controllable oxygen release-magnetic hyperthermia therapy. Adv Healthc Mater. 2024;13(32):e2402253. doi:10.1002/adhm.202402253
59. Sharma KV, Bascal Z, Kilpatrick H, et al. Long-term biocompatibility, imaging appearance and tissue effects associated with delivery of a novel radiopaque embolization bead for image-guided therapy. Biomaterials. 2016;103:293–304. doi:10.1016/j.biomaterials.2016.06.064
60. Li X, Ullah MW, Li B, Chen H. Recent progress in advanced hydrogel-based embolic agents: from rational design strategies to improved endovascular embolization. Adv Healthc Mater. 2023;12(17):e2202787. doi:10.1002/adhm.202202787
61. Yang J, Choi Y, Ahn S, et al. Vascular embolic nanobiomaterials for efficient tumor treatment. Tissue Cell. 2025;96:102954. doi:10.1016/j.tice.2025.102954
62. Luxenhofer R. Polymers and nanomedicine: considerations on variability and reproducibility when combining complex systems. Nanomedicine. 2015;10(20):3109–3119. doi:10.2217/nnm.15.139
63. Akpinar I, Unsal A, Paulden M, Round J. A systematic review of health economic evaluation quality assessment instruments for medical devices. Int J Technol Assess Health Care. 2025;41(1):e40. doi:10.1017/S0266462325000212
64. Gajjar AA, Chen JY, Moore ME, Tzorfas D, Paul AR. Cost comparison of liquid versus particulate embolic agents for middle meningeal artery embolization in chronic subdural hematoma. Interv Neuroradiol. 2025;2025:290528992.
65. Rognoni C, Bhoori S, Crocetti L, et al. Cost-benefit analysis of trans-arterial radio-embolization with Y-90 glass microspheres versus drug-eluting bead trans-arterial chemo-embolization in patients with hepatocellular carcinoma in Italy. Cardiovasc Intervent Radiol. 2025;48(11):1614–1624. doi:10.1007/s00270-025-04214-4
66. Andreozzi G, Lorenzoni V, Bargellini I, Cioni R, Turchetti G. Drug-eluting microspheres compared to conventional transarterial chemoembolization as first line treatment for unresectable hepatocellular carcinoma: a single-center retrospective cost-utility analysis. Cardiovasc Intervent Radiol. 2023;46(3):319–326. doi:10.1007/s00270-022-03335-4
67. Gunn KJ, Sleasman E, Akkipeddi SMK, et al. Supply cost and outcome comparison of nBCA, Onyx, and coils for middle meningeal artery embolizations: a single-center retrospective analysis. J Neurointerv Surg. 2025. doi:10.1136/jnis-2025-024003
68. Peng Q, Li L, Yang J, et al. Assessing the impact of multidisciplinary team (MDT) care on patients with liver cancer/cirrhosis: a systematic review and meta-analysis. Iran J Public Health. 2025;54(2):240–251.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Transarterial Chemoembolization Combined with Immune Checkpoint Inhibitors Plus Tyrosine Kinase Inhibitors versus Immune Checkpoint Inhibitors Plus Tyrosine Kinase Inhibitors for Advanced Hepatocellular Carcinoma
Huang JT, Zhong BY, Jiang N, Li WC, Zhang S, Yin Y, Yang J, Shen J, Wang WS, Zhu XL
Journal of Hepatocellular Carcinoma 2022, 9:1217-1228
Published Date: 30 November 2022
Tyrosine Kinase Inhibitors Plus Anti-PD-1 Antibodies with Hepatic Arterial Infusion Chemotherapy or Transarterial Chemoembolization for Unresectable Hepatocellular Carcinoma
Yu B, Zhang N, Feng Y, Zhang Y, Zhang T, Wang L
Journal of Hepatocellular Carcinoma 2023, 10:1735-1748
Published Date: 6 October 2023
Comparable Clinical Outcomes Between Transarterial Chemoembolization or Hepatic Arterial Infusion Chemotherapy Combined with Tyrosine Kinase Inhibitors and PD-1 Inhibitors in Unresectable Hepatocellular Carcinoma
Long T, Yang Z, Zeng H, Wu W, Hu Z, Yang Z, Hu D, Zhou Z, Chen M, Zhang Y
Journal of Hepatocellular Carcinoma 2023, 10:1849-1859
Published Date: 20 October 2023
The Influence of Drug-Eluting Beads Transarterial Chemoembolization on Serum Levels of Soluble Programmed Cell Death Protein-1 in Advanced Hepatocellular Carcinoma Patients
Ma X, Sun X, Xie F, Jian W, Wang Q, Xie Y, Li C, Zhang K
Journal of Hepatocellular Carcinoma 2024, 11:619-628
Published Date: 25 March 2024
Combination Therapy of Transarterial Chemoembolization, Lenvatinib, and PD-1 Inhibitors Achieves Significant Tumor Response in Hepatocellular Carcinoma with Bile Duct Tumor Thrombus: A Case Report
Fu Y, Wu J, Wu J, Li Y, Zeng Z, Liu D, Li H, Ou X, Lin Z, Wei S, Song H, Yan M
Cancer Management and Research 2025, 17:793-799
Published Date: 13 April 2025