Back to Journals » International Journal of Women's Health » Volume 17
Insulin Resistance in GDM A1 vs Healthy Pregnancy: A Comparative Study Using METS-IR and TyG Index
Authors Jiang H, Shang M, Gao S ![]()
Received 3 August 2025
Accepted for publication 14 October 2025
Published 23 October 2025 Volume 2025:17 Pages 3789—3797
DOI https://doi.org/10.2147/IJWH.S557974
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Hao Jiang,1 Min Shang,1 Songkun Gao2
1Department of Gynecology and Obstetrics, Beijing Friendship Hospital, Capital Medical University, Beijing, People’s Republic of China; 2Department of Gynecologic Oncology, Beijing Obstetrics and Gynecology Hospital, Capital Medical University, Beijing Maternal and Child Health Care Hospital, Beijing, People’s Republic of China
Correspondence: Songkun Gao, Department of Gynecologic Oncology, Beijing Obstetrics and Gynecology Hospital, Capital Medical University, Beijing Maternal and Child Health Care Hospital, Dongcheng District, Beijing, People’s Republic of China, Email [email protected]
Purpose: To compare the whole-pregnancy insulin resistance level between women with gestational diabetes mellitus A1 (GDM A1) and healthy pregnant women by means of the METS-IR and the TyG index, and to assess the impact of such resistance on pregnancy outcomes.
Methods: 344 parturients were classified as GDM A1 (n=118) or normal by 75-g oral glucose tolerance test (OGTT) conducted at 24– 28 weeks of gestation. Body mass index (BMI), fasting plasma glucose, triglycerides, and high-density lipoprotein cholesterol were measured in early, mid-, and late pregnancy to calculate METS-IR and TyG index values for each period. Longitudinal changes and early-pregnancy values of METS-IR and TyG were compared between groups and related to obstetric outcomes. Furthermore, mediation analysis was conducted to assess the mediating effect of BMI gain on the relationship between TyG index and METS-IR during pregnancy.
Results: METS-IR indicated that insulin resistance in mid- and late pregnancy was significantly higher in the GDM A1 group than in the control group, while the TyG index showed a similar trend beginning in early pregnancy. However, the magnitude of increase in insulin resistance from early to mid-pregnancy did not differ significantly between the two groups. From mid- to late pregnancy, METS-IR increased more rapidly in the control group than in the GDM A1 group, whereas no significant difference was observed in TyG index changes. Early-pregnancy METS-IR and TyG values were not significantly associated with mode of delivery, neonatal birth weight, or placental weight. Mediation analysis revealed that BMI gain had a significantly greater mediating effect on METS-IR elevation than on TyG increase.
Conclusion: Women with GDM A1 exhibited higher insulin resistance throughout pregnancy compared to healthy controls. Early-pregnancy METS-IR and TyG indices were associated with GDM A1 diagnosis but not with delivery characteristics or fetal parameters. Due to the influence of BMI changes during pregnancy, METS-IR may not be a reliable surrogate marker of insulin resistance in this population.
Keywords: GDM A1, insulin resistance, METS-IR, TyG
Introduction
Gestational diabetes mellitus (GDM) occurs in approximately one in seven pregnancies, and an increasing number of women are affected,1 especially in developing countries such as China.2–4 It is associated with adverse outcomes for both mother and infant during pregnancy, delivery, and throughout life.5–7 Recent data further indicate that GDM significantly elevates the risks of neonatal hypoglycaemia, hyperbilirubinaemia and acute respiratory distress syndrome.8
During normal pregnancy, the mother adapts her glucose metabolism to ensure continuous glucose transfer to the fetus. A series of metabolic changes take place: fat accretion is promoted in early pregnancy, whereas late pregnancy is characterized by insulin resistance and lipolysis.9,10 These alterations may be related to ineffective insulin-receptor phosphorylation and decreased IRS-1 expression. Concurrently, rising human placental lactogen and prolactin enhance pancreatic β-cell mass and glucose-stimulated insulin secretion, thereby preserving maternal glucose homeostasis despite increasing insulin resistance.11 Compared with women with uncomplicated pregnancies, patients with GDM exhibit more pronounced subclinical inflammation, reduced secretion of placental hormones and adiponectin, and excessive lipolysis, which collectively lead to more severe insulin resistance.9 The degree of insulin resistance in GDM has been linked to adverse pregnancy outcomes, including hypertensive disorders of pregnancy, higher cesarean-section rates, and fetal complications.11,12
GDM can be further subclassified as diet-controlled (GDM A1) or medication-controlled (GDM A2).13 Studies have shown that maternal and neonatal outcomes in women with GDM A1 are comparable to those in women without a GDM diagnosis but with abnormal oral glucose tolerance test results, and are significantly better than outcomes in women with GDM A2.14 This difference is likely attributable to poorer glycaemic control in the GDM A2 group. However, whether the degree of insulin resistance in women with GDM A1 is similar to that in healthy pregnant women remains unclear.
The metabolic score for insulin resistance (METS-IR) and the triglyceride–glucose index (TyG) are laboratory-based surrogate markers of insulin resistance. They are widely used when the gold-standard hyperinsulinaemic–euglycaemic clamp (HEC) method is not feasible, yet assessment of insulin resistance is still required.15 Because the required laboratory parameters are routinely available and easy to obtain, these surrogates are particularly suitable for retrospective and cohort studies.16,17 To date, longitudinal data on insulin resistance in pregnant women with GDM A1 remain scarce, largely because repeated application of the HEC markedly increases antenatal costs and reduces maternal compliance. In the present study, these surrogate markers allowed us to evaluate longitudinal changes in insulin resistance across pregnancy without adding any tests beyond routine antenatal care.
By collecting routine antenatal examination results from women with GDM A1 and healthy controls, we calculated insulin-resistance surrogates in early, mid-, and late pregnancy. Our aim was to delineate the trajectory of insulin resistance throughout gestation and to explore its relationship with pregnancy outcomes. This will facilitate a more comprehensive understanding of GDM A1 from the perspective of insulin resistance and provide clinical evidence for the application of similar pharmacological strategies.
Methods
Patients
Clinical data were collected from women who delivered at the Department of Obstetrics and Gynecology, Beijing Friendship Hospital, Capital Medical University, between January and June 2025. GDM was diagnosed by a 75-g oral glucose tolerance test (OGTT) performed at 24–28 weeks’ gestation. Women whose glycaemic targets (fasting ≤ 5.3 mmol/L, postprandial ≤ 6.7 mmol/L) were achieved with diet and exercise alone, without pharmacological therapy, were classified as GDM (A1).
Inclusion criteria: 1. GDM diagnosed by OGTT; 2. Complete serological data available for early (7 weeks), mid- (24–28 weeks), and late pregnancy (36–37 weeks); 3. Delivery by vaginal birth or caesarean section with a live neonate.
Exclusion criteria: 1. Pre-pregnancy diabetes or impaired fasting glucose; 2. Use of insulin or oral hypoglycaemic agents at any time during pregnancy; 3. Re-diagnosis of GDM by repeat OGTT in the second or third trimester for any reason.
Healthy controls were recruited from women who delivered at the same hospital between April and June 2025 and who had neither pre-existing diabetes nor GDM diagnosed at any time during pregnancy.
OGTT Procedure
At 24–28 weeks’ gestation, after an overnight fast of 8–14 h, participants ingested 300 mL of solution containing 75 g glucose. Venous blood samples were obtained at 0, 1, and 2 h. GDM was diagnosed when any single value met or exceeded the following thresholds: fasting ≥ 5.1 mmol/L, 1 h ≥ 10.0 mmol/L, or 2 h ≥ 8.5 mmol/L.18
Data Collection
Maternal age, gravidity, parity, and serological parameters at 7, 24–28, and 36–37 weeks were extracted. Parameters included fasting plasma glucose (FPG), triglycerides (TG), total cholesterol, high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), uric acid, and glycated haemoglobin. All blood samples were drawn in the morning after ≥ 8 h fasting. FPG, TG, total cholesterol, HDL-C, and LDL-C were converted to mg/dL for calculation.
Surrogate indices of insulin resistance were computed as follows:
TyG = ln [TG (mg/dL) × FPG (mg/dL) / 2]
METS-IR = ln [2 × FPG (mg/dL) + TG (mg/dL)] × BMI (kg/m²) / ln [HDL-C (mg/dL)]
Statistics
All analyses were performed with SPSS 26.0, SigmaStat 3.5, and Excel. Ordinal data were analysed using ANOVA. Normally distributed continuous variables were compared between groups by one-way ANOVA; non-normally distributed variables were analysed with the Mann–Whitney U or Kruskal–Wallis test.
Since the calculation of METS-IR incorporates maternal BMI in addition to serological parameters, we sought to determine whether longitudinal changes in METS-IR reflect variations in insulin resistance rather than mere fluctuations in BMI. To this end, we evaluated the mediating role of the TyG index between BMI and METS-IR. All analyses were performed with the “mediation” package in R, using 5000 non-parametric bootstrap iterations to estimate the 95% confidence intervals for the natural direct and indirect effects.
Figures were generated in R 4.4.1 using the “tidyverse” and “ggsignif” packages. Statistical significance was set at P < 0.05.
Results
A total of 344 women were enrolled: 161 in the GDM A1 group and 183 in the control group. Maternal characteristics and serological findings across early, mid-, and late pregnancy are presented in Table 1. Women with GDM A1 were older and had higher gravidity and parity than controls (P < 0.05). Throughout pregnancy, fasting plasma glucose and triglyceride levels were consistently higher in the GDM (A1) group (P < 0.001). In mid-pregnancy, HDL-C was significantly higher (P = 0.004) and LDL-C significantly lower (P = 0.006) in the GDM A1 group; these differences were no longer evident in late pregnancy.
 |
Table 1 General Characteristics and Serological Results in Early, Mid-, and Late Pregnancy of the GDM (A1) and Control Groups |
We calculated the METS-IR and TyG indices as markers of insulin resistance in different periods of pregnancy using the aforementioned formulas. The complete gestational trajectories of both METS-IR and TyG indices are presented in Table 2. METS-IR showed no significant differences in insulin resistance between the GDM and control groups in early and mid-pregnancy, but significant differences emerged from mid- to late pregnancy. TyG indicated a significant increase in insulin resistance from early to mid- and late pregnancy (P < 0.001). Between-group comparisons revealed that insulin resistance was consistently higher in the GDM group than in the control group throughout pregnancy (P < 0.001, Figure 1).
 |
Table 2 METS-IR and TyG Results During Pregnancy in GDM (A1) and Control Groups |
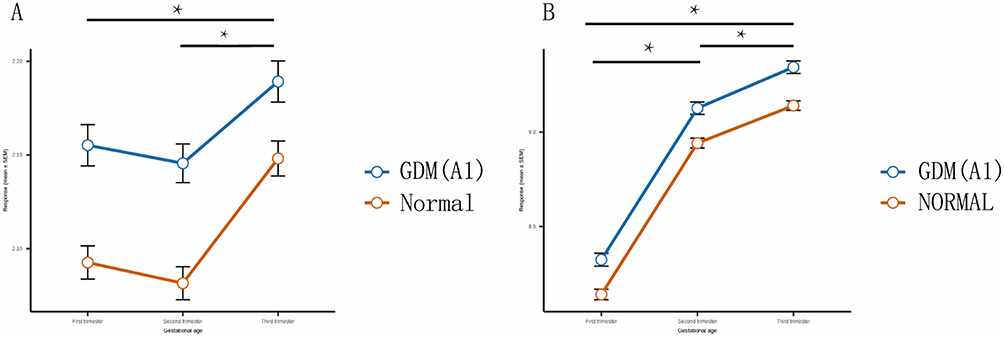 |
Figure 1 Changes in Insulin Resistance Throughout Pregnancy in the Two Groups. (A) Changes in METS-IR During Pregnancy in the Two Groups. (B) Changes in TyG During Pregnancy in the Two Groups. *indicates P < 0.05 between the two groups. |
We compared the rates of change in insulin resistance between the two groups. Within-group comparisons showed that the increase in insulin resistance from mid- to late pregnancy was significantly higher than that from early to mid-pregnancy in both groups (P < 0.001). Between-group comparisons indicated no significant difference in the increase in insulin resistance from early to mid-pregnancy (P = 0.674). However, METS-IR showed that the increase in insulin resistance from mid- to late pregnancy was faster in the control group than in the GDM A1 group (control group: GDM A1 group=1.023 (1.003, 1.04) vs 1.03 (1.015, 1.045), P = 0.006), while TyG showed no such difference (P = 0.939). We also analyzed the delivery outcomes of the two groups. There were no significant differences in mode of delivery (P = 0.367), neonatal birth weight (P = 0.228), or placental weight (P = 0.879) between the groups. However, the gestational age at delivery was significantly lower in the GDM A1 group than in the control group (38.81 vs 39.11 weeks, P = 0.024).
We divided all participants into quartiles (Q1, Q2, Q3, Q4) based on early-pregnancy METS-IR and TyG values (Table 3). Analysis showed that higher early-pregnancy METS-IR was associated with an increased likelihood of GDM A1 diagnosis (P = 0.001), but not with gestational age at delivery, mode of delivery, neonatal birth weight, or placental weight (P > 0.05). Early-pregnancy TyG was associated with maternal age, parity, and gravidity (P < 0.05). Higher early-pregnancy TyG was also linked to an increased likelihood of GDM A1 diagnosis (P < 0.001), consistent with METS-IR, but not with delivery or neonatal outcomes (P > 0.05).
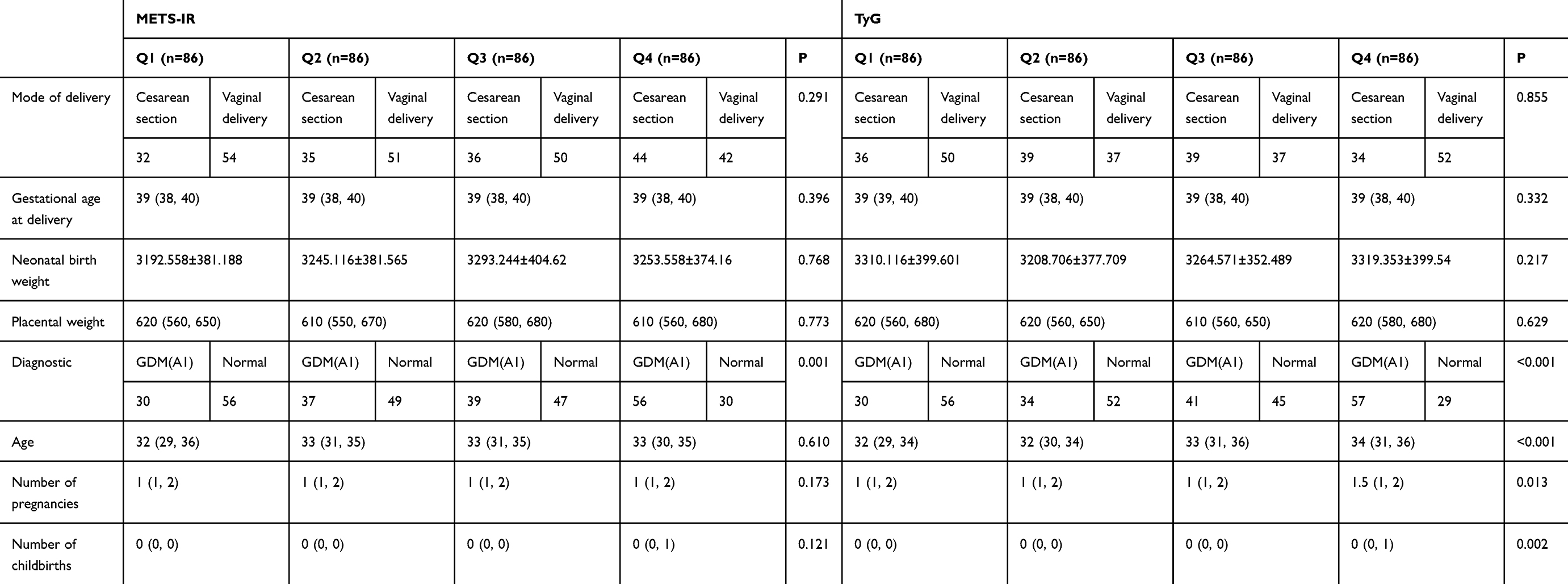 |
Table 3 Pre-Pregnancy and Delivery Outcomes After Classifying Participants According to Quartiles of Early-Pregnancy METS-IR and TyG |
Finally, we quantified the mediating effect of BMI on the relationship between the TyG index and METS-IR. In both healthy controls and women with GDM A1, BMI exerted a direct positive effect on METS-IR. Among GDM A1 participants, 32% of the change in METS-IR was attributable to TyG, whereas only 16% of the total effect was mediated by TyG in the control group; the majority of the effect was driven by BMI variation (Table 4). Across early, mid- and late pregnancy, the TyG index consistently displayed a stronger mediating role between BMI and METS-IR in the GDM (A1) group than in the control group (Table 5).
 |
Table 4 Mediating Effect of the TyG Index Between BMI and METS-IR in the GDM A1 Group and the Normal Group |
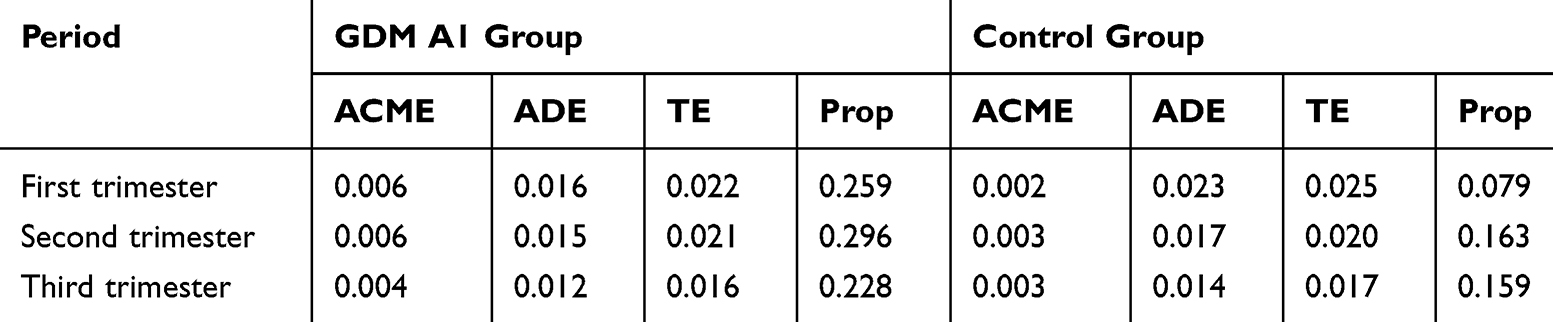 |
Table 5 Mediation Analysis Results by Trimester for GDM and Normal Groups |
Discussion
Gestational diabetes mellitus (GDM) is a state of glucose intolerance first detected during pregnancy, characterized by relatively reduced insulin secretion and pregnancy-associated insulin resistance.19 However, women diagnosed with GDM may have already had insulin resistance before conception, even if their blood glucose levels did not fluctuate significantly.20 In this study, our results showed that in early pregnancy, women with GDM A1 had higher insulin resistance than those in the control group, suggesting that it is possible to identify potential GDM patients earlier using insulin resistance tests or surrogate markers before the OGTT (at 24 weeks). Insulin resistance is thought to be strongly associated with pregnancy weight gain,21 but in this study, there was no significant difference in the increase in insulin resistance from early to mid-pregnancy between the two groups. From mid- to late pregnancy, the increase in insulin resistance was even faster in the control group than in the GDM A1 group, indicating that the increase in insulin resistance due to pregnancy was not significantly different between the two groups. The higher insulin resistance in women with GDM A1 was mainly due to their higher pre-pregnancy insulin resistance levels and was not significantly related to pregnancy.
TyG and METS-IR have been proven to be surrogate markers of insulin resistance,22,23 and early-pregnancy results are associated with the risk of GDM.24,25 However, METS-IR is rarely used in pregnancy studies, possibly because BMI is required for calculation, and the weight of pregnant women includes the weight of the fetus and its appendages. Due to hormonal changes during pregnancy, insulin resistance changes with increasing gestational age. In longitudinal studies, Thaweethai et al26 showed in their longitudinal observational study that insulin sensitivity was slightly reduced in early pregnancy and significantly decreased in mid- and late pregnancy.
In this study, we used both METS-IR and TyG to assess the same pregnant women. In mid-pregnancy, METS-IR values showed no significant decrease, but TyG values increased significantly. In late pregnancy, both METS-IR and TyG results increased significantly, indicating enhanced insulin resistance in pregnant women, similar to other longitudinal studies. In the quartile analysis, both surrogate markers showed that the likelihood of GDM diagnosis at the time of OGTT increased with higher values, suggesting that METS-IR may be as effective as TyG in measuring insulin resistance in pregnant women with GDM. However, subsequent mediation analyses revealed that BMI exerted a substantially greater influence on METS-IR than did TyG, a metric that is independent of adiposity. Given that gestational weight encompasses the fetus and its appendages, the validity of METS-IR for quantifying insulin resistance in pregnant women remains to be confirmed by comparison with reference indices such as the homeostasis model assessment of insulin resistance (HOMA-IR) or the quantitative insulin sensitivity check index (QUICKI).
We also analyzed the relationship between TyG and METS-IR values and mode of delivery, neonatal birth weight, and placental weight in this study. Previous studies have suggested that insulin resistance during pregnancy is closely related to neonatal birth outcomes. Ikenoue et al27 showed that maternal insulin resistance in mid- and late pregnancy was significantly associated with fetal fat mass but not with fetal weight. In another study, Yamashita et al28 found that maternal insulin resistance in mid-pregnancy was associated with neonatal birth weight. In other studies using surrogate markers of insulin resistance, early-pregnancy TyG was not associated with macrosomia, small for gestational age, preterm birth, or cesarean section.29 In our study, TyG and METS-IR values were not associated with neonatal birth weight, placental weight, or mode of delivery, consistent with previous studies, indicating that a single surrogate marker cannot predict neonatal obstetric outcomes.
This study still has certain limitations. First, as a retrospective study, we were unable to collect data on insulin secretion, which prevented us from using more widely accepted surrogate markers of insulin resistance, such as HOMA-IR. Although we utilized currently recognized surrogate indices of insulin resistance, accurate insulin-related measurements are still required to verify whether the results obtained from these surrogates are reliable. Because METS-IR involves body weight, it is not possible to measure the weight of pregnant women separately in mid- and late pregnancy to exclude the weight of the fetus and its appendages. The accuracy of METS-IR in mid- and late pregnancy is questionable and needs to be verified against the gold standard to determine whether it can reflect the insulin resistance levels of pregnant women in these periods. Second, this study only focused on GDM A1 patients. Since GDM A2 patients use long-acting or intermediate-acting insulin at night, which affects the next day’s fasting insulin measurement, further research is needed to determine whether surrogate markers can be used to evaluate insulin resistance in patients with GDM A2. On the other hand. This study is a single-center retrospective investigation; given the substantial heterogeneity in maternal characteristics and insulin resistance across different regions, multicenter or regional studies are warranted to confirm our findings.
Conclusion
In this study, our results showed that women with GDM A1 had higher insulin resistance than the control group in early pregnancy. There was no significant difference in the rate of increase in insulin resistance from early to mid-pregnancy between women with GDM A1 and normal pregnant women. The increase in insulin resistance from mid- to late pregnancy was even higher in normal pregnant women than in those with GDM A1. There were no significant differences in delivery outcomes or fetal and placental conditions between the GDM A1 group and normal parturients. Both early-pregnancy METS-IR and TyG were associated with GDM A1 diagnosis but not with delivery outcomes or fetal conditions. The observed rise in METS-IR may largely reflect gestational BMI gain rather than a genuine increase in insulin resistance. Our data confirm that insulin resistance intensifies with advancing gestation, and both TyG and METS-IR measured in early pregnancy may serve as early predictors of GDM. Nevertheless, BMI accretion during the second and third trimesters could weaken the concordance between METS-IR and actual insulin resistance; additional clinical studies are therefore required to clarify whether METS-IR reliably mirrors insulin resistance throughout pregnancy. Although the present analysis found no association between surrogate-estimated insulin resistance and pregnancy outcomes, heightened vigilance and management of GDM remain essential in clinical practice to prevent adverse events.
Ethical Approval
The study was carried out in accordance with the ethical standards laid down in the Declaration of Helsinki, and was approved by the ethics committees of Beijing friendship hospital, Capital Medical University (YYXSSC-2022-209). The ethics committee felt that this study could exempt patients from informed consent. Potential participants’eligibility was established by reviewing their medical records. As this was a retrospective study and all patient treatments and outcomes had already been determined, the ethics committee waived the requirement for informed consent. All patients’ privacy is ensured by assigning anonymous codes instead of personal identifiers.
Acknowledgments
This manuscript was edited for language and style by Kimi, an AI language model developed by Moonshot AI. Kimi assisted in refining the text to ensure clarity, coherence, and adherence to scientific writing standards. The authors are responsible for the content and any errors that remain.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
All authors have no conflicts of interest to declare in this work.
References
1. Hivert MF, White F, Allard C, et al. Placental IGFBP1 levels during early pregnancy and the risk of insulin resistance and gestational diabetes. Nat Med. 2024;30(6):1689–1695. PMID: 38627562; PMCID: PMC11186792. doi:10.1038/s41591-024-02936-5
2. American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2013;36 Suppl 1(Suppl 1):S67–74. doi:10.2337/dc13-S067
3. Leng J, Shao P, Zhang C, et al. Prevalence of gestational diabetes mellitus and its risk factors in Chinese pregnant women: a prospective population-based study in Tianjin, China. PLoS One. 2015;10(3):e0121029. PMID: 25799433; PMCID: PMC4370728. doi:10.1371/journal.pone.0121029
4. Hunsberger M, Rosenberg KD, Donatelle RJ. Racial/ethnic disparities in gestational diabetes mellitus: findings from a population-based survey. Womens Health Issues. 2010;20(5):323–328. PMID: 20800768. doi:10.1016/j.whi.2010.06.003
5. HAPO Study Cooperative Research Group; Metzger BE, Lowe LP, Dyer AR, et al. Hyperglycemia and adverse pregnancy outcomes. N Engl J Med. 2008;358(19):1991–2002. PMID: 18463375. doi:10.1056/NEJMoa0707943
6. Ye W, Luo C, Huang J, Li C, Liu Z, Liu F. Gestational diabetes mellitus and adverse pregnancy outcomes: systematic review and meta-analysis. BMJ. 2022;377:e067946. PMID: 35613728; PMCID: PMC9131781. doi:10.1136/bmj-2021-067946
7. Fox NS, Gerber RS, Saltzman DH, et al. Glycemic control in twin pregnancies with gestational diabetes: are we improving or worsening outcomes? J Matern Fetal Neonatal Med. 2016;29(7):1041–1045. PMID: 25938874. doi:10.3109/14767058.2015.1038517
8. Liu Y, Wang M, Zhou J. Impact of gestational diabetes mellitus on neonatal birth outcomes. Br J Hosp Med. 2024;85(11):1–12. PMID: 39618206. doi:10.12968/hmed.2024.0410
9. Barbour LA, McCurdy CE, Hernandez TL, Kirwan JP, Catalano PM, Friedman JE. Cellular mechanisms for insulin resistance in normal pregnancy and gestational diabetes. Diabetes Care. 2007;30 Suppl 2(Supplement_2):S112–9. PMID: 17596458. doi:10.2337/dc07-s202
10. Catalano PM, Huston L, Amini SB, Kalhan SC. Longitudinal changes in glucose metabolism during pregnancy in obese women with normal glucose tolerance and gestational diabetes mellitus. Am J Obstet Gynecol. 1999;180(4):903–916. PMID: 10203659. doi:10.1016/s0002-9378(99)70662-9
11. Ellerbrock J, Spaanderman B, Drongelen JV, et al. Role of beta cell function and insulin resistance in the development of gestational diabetes mellitus. Nutrients. 2022;14(12):2444. PMID: 35745174; PMCID: PMC9231208. doi:10.3390/nu14122444
12. Sun YY, Juan J, Xu QQ, Su RN, Hirst JE, Yang HX. Increasing insulin resistance predicts adverse pregnancy outcomes in women with gestational diabetes mellitus. J Diabetes. 2020;12(6):438–446. PMID: 31808991. doi:10.1111/1753-0407.13013
13. Barrozo ER, Racusin DA, Jochum MD, et al. Discrete placental gene expression signatures accompany diabetic disease classifications during pregnancy. Am J Obstet Gynecol. 2025;232(3):326.e1–326.e15. PMID: 38763341. doi:10.1016/j.ajog.2024.05.014
14. Nataly F, Hadas GH, Ohad G, Letizia S, Michal K. Is there a difference in placental pathology in pregnancies complicated with gestational diabetes A2 versus gestational diabetes A1, versus one abnormal value, on 100 gr glucose tolerance test? Placenta. 2022;120:60–64. PMID: 35217317. doi:10.1016/j.placenta.2022.02.009
15. Gao S, Wang J, Wang T, Wang J. Is insulin resistance a high-risk factor for postmenopausal endometrial cancer: insights from the triglyceride glucose (TyG) index and the metabolic score for insulin resistance (METS-IR). Int J Womens Health. 2024;16:2355–2363. PMID: 39742345; PMCID: PMC11687295. doi:10.2147/IJWH.S500936
16. Duan M, Zhao X, Li S, et al. Metabolic score for insulin resistance (METS-IR) predicts all-cause and cardiovascular mortality in the general population: evidence from NHANES 2001-2018. Cardiovasc Diabetol. 2024;23(1):243. PMID: 38987779; PMCID: PMC11238348. doi:10.1186/s12933-024-02334-8
17. Jiang L, Zhu T, Song W, et al. Assessment of six insulin resistance surrogate indexes for predicting stroke incidence in Chinese middle-aged and elderly populations with abnormal glucose metabolism: a nationwide prospective cohort study. Cardiovasc Diabetol. 2025;24(1):56. PMID: 39915878; PMCID: PMC11804005. doi:10.1186/s12933-025-02618-7
18. Obstetrics Subgroup, Chinese Society of Obstetrics and Gynecology, Chinese Medical Association; Chinese Society of Perinatal Medicine, Chinese Medical Association; Committee of Pregnancy with Diabetes Mellitus, China Maternal and Child Health Association. [Guideline of diagnosis and treatment of hyperglycemia in pregnancy (2022) [Part two]]. Zhonghua Fu Chan Ke Za Zhi. 2022;57(2):81–90. Tonga, Chinese. PMID: 35184468. doi:10.3760/cma.j.cn112141-20210917-00529
19. Vejrazkova D, Vcelak J, Vankova M, et al. Steroids and insulin resistance in pregnancy. J Steroid Biochem Mol Biol. 2014;139:122–129. PMID: 23202146. doi:10.1016/j.jsbmb.2012.11.007
20. McIntyre HD, Catalano P, Zhang C, Desoye G, Mathiesen ER, Damm P. Gestational diabetes mellitus. Nat Rev Dis Primers. 2019;5(1):47. PMID: 31296866. doi:10.1038/s41572-019-0098-8
21. Stuebe AM, McElrath TF, Thadhani R, Ecker JL. Second trimester insulin resistance, early pregnancy body mass index and gestational weight gain. Matern Child Health J. 2010;14(2):254–260. PMID: 19194791. doi:10.1007/s10995-009-0449-2
22. Brito ADM, Hermsdorff HHM, Filgueiras MS, et al. Predictive capacity of triglyceride-glucose (TyG) index for insulin resistance and cardiometabolic risk in children and adolescents: a systematic review. Crit Rev Food Sci Nutr. 2021;61(16):2783–2792. PMID: 32744083. doi:10.1080/10408398.2020.1788501
23. Bello-Chavolla OY, Almeda-Valdes P, Gomez-Velasco D, et al. METS-IR, a novel score to evaluate insulin sensitivity, is predictive of visceral adiposity and incident type 2 diabetes. Eur J Endocrinol. 2018;178(5):533–544. PMID: 29535168. doi:10.1530/EJE-17-0883
24. Guo Y, Lu J, Bahani M, et al. Triglyceride-glucose index in early pregnancy predicts the risk of gestational diabetes: a prospective cohort study. Lipids Health Dis. 2024;23(1):87. doi:10.1186/s12944-024-02076-2
25. Cui J, Jiang H, Huang F, et al. First-trimester triglyceride-glucose index and birth weight: a retrospective cohort mediation analysis of preterm birth and gestational complications. BMC Pregnancy Childbirth. 2025;25(1):765. PMID: 40670958; PMCID: PMC12265213. doi:10.1186/s12884-025-07885-6
26. Thaweethai T, Soetan Z, James K, Florez JC, Powe CE. Distinct insulin physiology trajectories in euglycemic pregnancy and gestational diabetes mellitus. Diabetes Care. 2023;46(12):2137–2146. PMID: 37126832; PMCID: PMC10698215. doi:10.2337/dc22-2226
27. Ikenoue S, Waffarn F, Sumiyoshi K, et al. Maternal insulin resistance in pregnancy is associated with fetal fat deposition: findings from a longitudinal study. Am J Obstet Gynecol. 2023;228(4):455.e1–455.e8. PMID: 36283481. doi:10.1016/j.ajog.2022.10.015
28. Yamashita H, Yasuhi I, Fukuda M, et al. The association between maternal insulin resistance in mid-pregnancy and neonatal birthweight in uncomplicated pregnancies. Endocr J. 2014;61(10):1019–1024. PMID: 25109752. doi:10.1507/endocrj.ej14-0163
29. Gurza G, Martínez-Cruz N, Lizano-Jubert I, et al. Association of the triglyceride-glucose index during the first trimester of pregnancy with adverse perinatal outcomes. Diagnostics. 2025;15(9):1129. PMID: 40361947; PMCID: PMC12072019. doi:10.3390/diagnostics15091129
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Relationship Between Four Non-Insulin-Based Indexes of Insulin Resistance and Serum Uric Acid in Patients with Type 2 Diabetes: A Cross-Sectional Study
Han R, Zhang Y, Jiang X
Diabetes, Metabolic Syndrome and Obesity 2022, 15:1461-1471
Published Date: 9 May 2022
Association Between Triglyceride-Glucose Index and Serum Uric Acid Levels: A Biochemical Study on Anthropometry in Non-Obese Type 2 Diabetes Mellitus Patients
Luo Y, Hao J, He X, Wang C, Zhao H, Zhang Z, Yang L, Ren L
Diabetes, Metabolic Syndrome and Obesity 2022, 15:3447-3458
Published Date: 3 November 2022
A Novel Metabolic Score for Insulin Resistance and Symptomatic Intracranial Hemorrhage in Ischemic Stroke Patients After Endovascular Thrombectomy
Chen S, E Y, Zhang X, Wei B, Wang S, Xu Z, Gong P, Xie Y, Qin C, Zhang Y
Neuropsychiatric Disease and Treatment 2023, 19:321-328
Published Date: 5 February 2023
First-Trimester Triglyceride-Glucose Index and Triglyceride/High-Density Lipoprotein Cholesterol are Predictors of Gestational Diabetes Mellitus Among the Four Surrogate Biomarkers of Insulin Resistance
Ma N, Bai L, Lu Q
Diabetes, Metabolic Syndrome and Obesity 2024, 17:1575-1583
Published Date: 8 April 2024
Is Insulin Resistance a High-Risk Factor for Postmenopausal Endometrial Cancer: Insights from the Triglyceride Glucose (TyG) Index and the Metabolic Score for Insulin Resistance (METS-IR)
Gao S, Wang J, Wang T, Wang J
International Journal of Women's Health 2024, 16:2355-2363
Published Date: 27 December 2024