Back to Journals » International Journal of General Medicine » Volume 19
Inflammatory Burden Index is Associated with Increased Long-Term Risk of Major Advers Cardiovascular Events in Myocardial Infarction with Non-Obstructive Coronary Arteries
Authors Tao Y, Liu W, Yin J, Chen Z, Shen Q, Chen L
Received 14 October 2025
Accepted for publication 22 January 2026
Published 31 January 2026 Volume 2026:19 572612
DOI https://doi.org/10.2147/IJGM.S572612
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Redoy Ranjan
Yifei Tao,1,* Wei Liu,1,* Jiayu Yin,2,* Zhixian Chen,1 Qian Shen,1 Le Chen1
1Department of Cardiology, the Affiliated Changshu Hospital of Nantong University, Changshu, Jiangsu, 215500, People’s Republic of China; 2Department of Cardiology, the Second Affiliated Hospital of Soochow University, Suzhou, Jiangsu, 215004, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Le Chen, Department of Cardiology, the Affiliated Changshu Hospital of Nantong University, Changshu, Jiangsu, 215500, People’s Republic of China, Email [email protected] Qian Shen, Department of Cardiology, the Affiliated Changshu Hospital of Nantong University, Changshu, Jiangsu, 215500, People’s Republic of China, Email [email protected]
Background: Myocardial infarction with non-obstructive coronary arteries (MINOCA) refers to patients who meet the universal definition of acute myocardial infarction but show no significant stenosis on coronary angiography, and it is associated with a non-benign prognosis. The prognostic relevance of inflammatory burden index (IBI), a useful inflammatory biomarker, in patients with MINOCA remains to be elucidated. We evaluated the association between the IBI and long-term major adverse cardiovascular events (MACE) in MINOCA.
Methods: In this single-center retrospective cohort, we included 267 consecutive patients with clinically diagnosed MINOCA. Cox proportional hazards models assessed associations between baseline IBI and MACE. Discrimination was evaluated using receiver operating characteristic (ROC) analysis with area under the curve (AUC) comparisons by the DeLong test.
Results: Over a median follow-up of 42 (15, 56) months, 53 MACE occurred (19.9%). In multivariable models adjusting for clinical covariates and key biomarkers, IBI remained independently associated with MACE (HR 1.342, 95% CI 1.168– 1.542; P < 0.001), as did NT-proBNP (HR 1.711, 95% CI 1.446– 2.023; P < 0.001) and the ST-segment elevation (HR 1.780, 95% CI 1.031– 3.075; P = 0.039). For predicting MACE, IBI achieved an AUC of 0.737 (95% CI 0.673– 0.801), outperforming hs-CRP (AUC 0.698, 95% CI 0.630– 0.766) and NLR (AUC 0.650, 95% CI 0.564– 0.736). Patients with high IBI had a significantly higher cumulative incidence of MACE on Kaplan–Meier analysis (log-rank P < 0.001).
Conclusion: Elevated IBI is an independent risk factor of long-term MACE in MINOCA. As an inexpensive, routinely available composite biomarker, IBI may aid risk stratification and follow-up planning in MINOCA. Despite these findings, the external generalizability of this study is limited by its design.
Keywords: acute myocardial infarction, MINOCA, inflammatory burden index, PROGNOSIS, risk stratification
Introduction
Myocardial infarction with non-obstructive coronary arteries (MINOCA) refers to patients who meet the universal definition of acute myocardial infarction (AMI) but show no significant stenosis on coronary angiography.1 Prior evidence indicates that MINOCA is not a “benign” condition; the risk of major adverse cardiovascular events (MACE) is comparable to that of obstructive myocardial infarction.1,2 Clinically, the pronounced etiological heterogeneity of MINOCA poses challenges for treatment and management.3 Achieving effective risk stratification and individualized management within this heterogeneous population remains a shared challenge for clinical practice and research.
Common mechanisms of MINOCA include coronary vasospasm, microvascular dysfunction, plaque disruption, and myocardial-related factors such as myocarditis.4 Among these pathways, inflammation has been shown to play a key role, providing a shared and cross-mechanistic pathophysiological basis.5–7 While inflammatory biomarkers such as high-sensitivity C-reactive protein (hs-CRP), neutrophils, and lymphocytes have been widely applied in cardiovascular disease, single inflammatory indices are often affected by short-term fluctuations and sampling timing, limiting their predictive performance.8 Composite inflammatory indices can, to some extent, integrate multidimensional inflammatory information and improve stability and discrimination. The inflammatory burden index (IBI) is a simple and reproducible composite inflammatory marker, calculated as the product of the neutrophil-to-lymphocyte ratio and CRP, and it provides a more comprehensive assessment of systemic inflammatory load and immune imbalance than single markers.9 In recent years, IBI has been shown to play an important role across multiple cohorts, including acute coronary syndrome, arrhythmias, heart failure, and stroke, and has demonstrated incremental predictive value over single inflammatory biomarkers in some studies.10–12 However, evidence specific to MINOCA remains limited. In this study, we aimed to systematically evaluate the association between baseline IBI and long-term adverse outcomes in a clinically diagnosed MINOCA cohort and to assess its robustness and incremental value as an independent predictor.
Methods
Study Design and Population
This single-center, retrospective cohort study consecutively enrolled hospitalized patients meeting diagnostic criteria for MINOCA at The Second Affiliated Hospital of Soochow University from January 2020 to December 2024. MINOCA was defined according to the universal definition of AMI, with coronary angiography showing no stenosis of any major coronary artery of 50% or greater, and with exclusion of other causes of non-ischemic myocardial injury and definite type 2 MI (exclusion of prior AMI or obstructive coronary artery disease, as well as thrombolytic therapy before or during the index hospitalization).13 AMI was defined by an elevation of high-sensitivity troponin T (hs-TnT) above the 99th percentile in conjunction with supportive clinical features consistent with the Fourth Universal Definition of Myocardial Infarction.14 Inclusion criteria were: age ≥18 years; fulfillment of the clinical diagnosis of MINOCA; and availability of complete clinical data. Exclusion criteria were: severe hepatic or renal insufficiency; malignancy or hematologic disorders; inflammatory diseases or autoimmune diseases; and inability to complete follow-up. In total, 267 patients with MINOCA were included in the study cohort (Figure 1). The study was approved by the Institutional Review Board (IRB) of The Second Affiliated Hospital of Soochow University, informed consent was waived by the IRB due to minimal risk to patients.
 |
Figure 1 Study flowchart. MINOCA, myocardial infarction with non-obstructive coronary arteries; MACE, major adverse cardiovascular events. |
Clinical Data
Demographic characteristics (age, sex, height, weight) and risk factors (hypertension, diabetes mellitus, smoking status) were obtained from electronic medical records. Laboratory parameters collected included hs-CRP, neutrophil and lymphocyte counts, N-terminal pro-brain natriuretic peptide (NT-proBNP), hs-TnT, total cholesterol, triglycerides, fasting plasma glucose, and estimated glomerular filtration rate (eGFR). All complete blood count tests were obtained from patients’ first laboratory examination at the hospital after symptom onset. The neutrophil-to-lymphocyte ratio (NLR) was calculated, and IBI was defined as hs-CRP multiplied by NLR. Due to skewed distributions, IBI, NT-proBNP, and hs-TnT were natural log–transformed for modeling. In addition, we recorded medication use and left ventricular ejection fraction (LVEF) during hospitalization.
Follow-Up and Endpoint Definitions
The end of follow-up was January 2025, and follow-up data were obtained through outpatient clinic visits and review of medical records. The primary endpoint was the time to first MACE during follow-up, comprising all-cause death, recurrent MI, heart failure, stroke, and angina. Only the first event was counted. Recurrent MI and heart failure were adjudicated according to contemporary European Society of Cardiology (ESC) guidelines.14,15 Stroke was defined as a new neurological deficit with imaging-confirmed ischemic or hemorrhagic cerebrovascular injury.16 Follow-up was performed through outpatient visits and/or telephone contact, supplemented by medical record review.
Statistical Analysis
Data distributions were assessed using the Kolmogorov–Smirnov test. Normally distributed continuous variables are presented as mean ± standard deviation and were compared using the t test; non-normally distributed variables are presented as median (interquartile range) and were compared using the Mann–Whitney U-test. Categorical variables are presented as counts (percentages) and were compared using the chi-square or Fisher’s exact test. Cox proportional hazards regression was used for univariable and multivariable analyses. Variables with P < 0.05 in univariable Cox regression analysis were included in the multivariable model using a stepwise approach. To avoid collinearity, the components of IBI were excluded from the multivariable model. Hazard ratios (HRs) and 95% confidence intervals (CIs) were reported. The proportional hazards assumption was assessed using Schoenfeld residuals. Receiver operating characteristic (ROC) curves were constructed and the area under the curve (AUC) was calculated to compare the discriminative performance of IBI, hs-CRP, and NLR for MACE; AUCs were compared using the DeLong test. The optimal cut-off, sensitivity, and specificity were reported. Patients were stratified by the ROC–Youden threshold and Kaplan–Meier curves were plotted; event rates between high and low IBI groups were compared using the Log rank test. All analyses were conducted with SPSS version 27.0 (IBM) and R. Two-sided (P<0.05) was considered statistically significant.
Results
Baseline Characteristics
A total of 267 patients with MINOCA were included. Over a median follow-up of 42 (15, 56) months, 53 MACE occurred (Table 1). Compared with the non-MACE group (n = 214), patients with MACE were older (70.13 ± 10.18 vs 65.86 ± 14.03 years, P = 0.013) and had a higher proportion of ST-segment elevation (41.51% vs 24.30%, P = 0.012). Regarding inflammatory indices, the MACE group had significantly higher IBI [60.79 (20.78, 223.39) vs 13.34 (3.66, 66.19), P < 0.001], higher NLR [7.80 (3.93, 14.84) vs 5.29 (2.77, 8.41), P < 0.001], and higher hs-CRP [7.70 (4.10, 29.30) vs 2.75 (0.70, 10.43) mg/L, P < 0.001], with lower absolute lymphocyte counts (1.24 ± 0.89 vs 1.79 ± 1.14 × 10^9/L, P = 0.001) and higher absolute neutrophil counts (9.76 ± 3.91 vs 8.27 ± 5.11 × 10^9/L, P = 0.048). In addition, NT-proBNP levels were higher in the MACE group [1317.00 (288.00, 13,098.00) vs 424.75 (248.10, 822.40) pg/mL, P < 0.001] (Table 2).
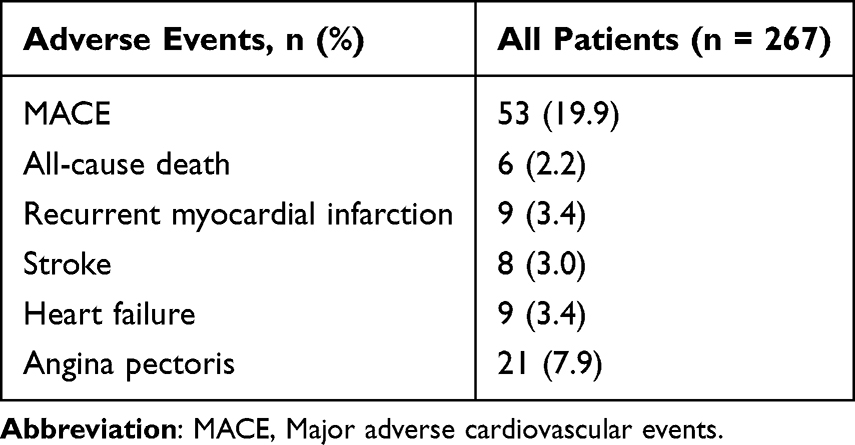 |
Table 1 Adverse Events During Follow-Up |
 |
Table 2 Baseline Characteristics |
Cox Regression Analysis
In univariable Cox regression analysis, IBI was significantly associated with MACE (HR 1.415, 95% CI 1.235–1.621, P < 0.001). In addition, age, STEMI, WBC, NLR, hs-CRP, lymphocyte count, eGFR, and NT-proBNP were associated with MACE risk (all P < 0.05). After adjustment for variables with P < 0.05 in univariable Cox regression analysis, IBI (HR 1.342, 95% CI 1.168–1.542, P < 0.001), NT-proBNP (HR 1.711, 95% CI 1.446–2.023, P < 0.001), and the ST-segment elevation (HR 1.780, 95% CI 1.031–3.075, P = 0.039) remained independent predictors of MACE (Table 3).
 |
Table 3 Cox Regression Analysis |
Discrimination and ROC Comparison
ROC analysis showed that IBI yielded an AUC of 0.737 (95% CI 0.673–0.801) for MACE, with an optimal cut-off of 17.23, corresponding to a sensitivity of 0.925 and a specificity of 0.547. The AUCs for hs-CRP and NLR were 0.698 (95% CI 0.630–0.766) and 0.650 (95% CI 0.564–0.736), respectively. The DeLong test indicated that the AUC for IBI was significantly higher than that for NLR (z = 2.022, P = 0.043) and hs-CRP (z = 2.014, P = 0.044) (Figure 2, Table 4).
 |
Table 4 ROC Curve of Inflammatory Biomarkers |
 |
Figure 2 Receiver operating characteristic analysis (ROC) of predictors for MACE. Abbreviations: IBI, inflammatory burden index; CRP, C-reactive protein; NLR, neutrophil-to-lymphocyte ratio; MACE, major adverse cardiovascular events. |
Follow-up and Survival Curves
Based on the ROC–Youden threshold, patients were classified into a high-IBI group (IBI > 17.23) and a low-IBI group (IBI ≤ 17.23). Kaplan–Meier curves showed that the cumulative incidence of MACE was significantly higher in the high-IBI group than in the low-IBI group (log-rank P < 0.001) (Figure 3).
 |
Figure 3 Kaplan-Meier curve for MINOCA patients based on the cut-off values of IBI. Abbreviations: IBI, inflammatory burden index; MINOCA, myocardial infarction with non-obstructive coronary arteries; MACE, major adverse cardiovascular events. |
Discussion
To our knowledge, this is the first study to explore the relationship between baseline IBI and long-term MACE risk in a MINOCA cohort. The principal finding is that elevated IBI is significantly and independently associated with an increased long-term risk of MACE in patients with MINOCA. In terms of discriminative ability, the AUC for IBI was significantly superior to those for hs-CRP and NLR considered individually.
In recent years, IBI has been validated as a useful inflammatory marker associated with adverse prognosis in multiple diseases.9–12 In a previous multicenter prospective study, higher admission IBI was significantly associated with 1-year MACE in patients with large-artery atherosclerosis ischemic stroke and outperformed NLR and CRP.10 In another study enrolling patients with chest pain and no obstructive coronary artery disease, IBI levels were significantly higher in those with the coronary slow flow phenomenon compared with controls, and IBI improved CSFP risk identification and predictive value better than single indicators.17 Consistent with these studies, our work innovatively demonstrates that elevated IBI is an independent risk factor for long-term MACE in patients with MINOCA. Clinically, MINOCA is a heterogeneous syndrome encompassing multiple etiologies. Major mechanisms include plaque rupture with distal microembolization, coronary vasospasm, coronary microvascular dysfunction, and coronary embolism. Across this heterogeneous mechanistic spectrum, inflammation and immune dysregulation permeate key links.18–20 hs-CRP reflects an IL-6–centered acute-phase response and the intensity of systemic inflammation, with biological effects that include endothelial dysfunction and activation of coagulation.21 NLR reflects a phenotype of neutrophil activation with relative lymphocyte suppression—indicative of thromboinflammatory activation and reduced anti-inflammatory/immune regulatory capacity.22,23 Thus, higher IBI signifies a more prominent systemic proinflammatory–prothrombotic–prospastic milieu, thereby driving MACE risk. Moreover, CRP, neutrophils, and lymphocytes also play important roles in long-term myocardial remodeling and progression to heart failure;24–26 patients with elevated IBI may be more prone to an “inflammation–fibrosis–heart failure” trajectory, promoting MACE occurrence. Currently, studies investigating the association of NLR or CRP with MINOCA prognosis remain limited. In a previous study, ROC analysis showed that NLR predicted acute coronary syndrome in MINOCA patients with an AUC of 0.670.27 This is consistent with our findings, suggesting that the prognostic discriminatory ability of individual inflammatory markers in MINOCA patients appears to be limited. In our study, ROC and DeLong analyses suggest that IBI has substantially better predictive performance for MACE than hs-CRP or NLR alone, supporting its use as a preferred metric to quantify inflammatory risk. Similarly, as a composite index, IBI reduces measurement error and short-term fluctuations inherent to single biomarkers, thereby improving stability and discrimination; its multiplicative form amplifies the high-risk phenotype characterized by simultaneous elevation of both CRP and NLR, which may explain its larger effect size and higher AUC. However, although the ROC analysis of IBI showed relatively high sensitivity, the specificity at the selected cut-off was low, which may limit its clinical utility and increase the risk of overclassifying patients as high risk. Therefore, caution should be exercised when applying this threshold in clinical practice. Stronger evidence may require further studies with multicenter designs and larger sample sizes.
IBI is derived entirely from routine laboratory tests, making it low-cost, reproducible, and feasible at the bedside; it is suitable for risk stratification early during hospitalization or before discharge. For the heterogeneous MINOCA population, IBI has the potential to serve as a simple tool for quantifying the “inflammatory phenotype”, helping to identify high-risk patients and optimize secondary prevention and follow-up strategies, such as intensified statin therapy, spasm management, cardiac rehabilitation, and lifestyle interventions.
Limitations
First, as a single-center study, external generalizability is limited, and the ROC-derived optimal threshold was cohort-driven, which may entail optimism bias. Second, inflammatory markers were modeled using a single baseline measurement, which does not capture dynamic changes; differences in acute-phase sampling timing may have affected absolute values. Third, we lacked etiological imaging modalities such as cardiac magnetic resonance and OCT, and residual confounding cannot be fully excluded. Fourth, the specific mechanistic role of IBI warrants further elucidation through related basic and translational research.
Conclusion
Elevated IBI is an independent risk factor of long-term MACE in patients with MINOCA. As a simple and useful inflammatory biomarker derived from routine testing, IBI shows promising clinical translational potential in the MINOCA population.
Data Sharing Statement
The datasets used and/or analysed during the current study available from the two corresponding authors on reasonable request (Le Chen, [email protected]; Qian Shen, [email protected]).
Ethics Statement
The study protocol was approved by the Ethics Committee of the Second Affiliated Hospital of Soochow University and complied with the Declaration of Helsinki (JD-HG-2025-105). Given the absence of additional interventions, the requirement for written informed consent was waived.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Sucato V, Comparato F, Ortello A, Galassi AR. Myocardical infarction with non-obstructive coronary arteries (MINOCA): pathogenesis, diagnosis and treatment. Curr Probl Cardiol. 2024;49(7):102583. doi:10.1016/j.cpcardiol.2024.102583
2. Alves da Silva P, Bucciarelli-Ducci C, Sousa A. Myocardial infarction with non-obstructive coronary arteries: etiology, diagnosis, treatment and prognosis. Revista Portuguesa de Cardiologia. 2023;42(7):655–10. doi:10.1016/j.repc.2022.10.007
3. Lindahl B, Baron T, Albertucci M, Prati F. Myocardial infarction with non-obstructive coronary artery disease. EuroIntervention. 2021;17(11):e875–e887. doi:10.4244/EIJ-D-21-00426
4. Singh T, Chapman AR, Dweck MR, Mills NL, Newby DE. MINOCA: a heterogenous group of conditions associated with myocardial damage. Heart. 2021;107(18):1458–1464. doi:10.1136/heartjnl-2020-318269
5. Chan K, Wahome E, Tsiachristas A, et al. Inflammatory risk and cardiovascular events in patients without obstructive coronary artery disease: the ORFAN multicentre, longitudinal cohort study. Lancet. 2024;403(10444):2606–2618. doi:10.1016/S0140-6736(24)00596-8
6. Sagris M, Theofilis P, Antonopoulos AS, et al. Inflammation in coronary microvascular dysfunction. Int J Mol Sci. 2021;22(24):13471. doi:10.3390/ijms222413471
7. Ciliberti G, Bergamaschi L, Armillotta M, Angeli F, Pizzi C. MINOCA and inflammation: another piece of the puzzle. Int J Cardiol. 2025;419:132724. doi:10.1016/j.ijcard.2024.132724
8. Zhang E, Gao M, Gao J, et al. Inflammatory and hematological indices as simple, practical severity predictors of microdysfunction following coronary intervention: a systematic review and meta-analysis. Angiology. 2020;71(4):349–359. doi:10.1177/0003319719896472
9. Xie H, Ruan G, Ge Y, et al. Inflammatory burden as a prognostic biomarker for cancer. Clin Nutr. 2022;41(6):1236–1243. doi:10.1016/j.clnu.2022.04.019
10. Mo J, Liu X, Zhang H, et al. Inflammatory burden index and one-year clinical outcomes in large artery atherosclerosis ischemic stroke: a multicenter prospective study. Eur J Neurol. 2025;32(6):e70242. doi:10.1111/ene.70242
11. Peng S, Li F, Jin M, Zhang Y, Li H, Yin J. Inflammatory burden index associated with recurrence of atrial fibrillation after radiofrequency catheter ablation. Ther Clin Risk Manag. 2025;21:681–689. doi:10.2147/TCRM.S518620
12. Lu W, Liao X, Jiang Y, Luo B, Chen L, Lin Y. Association between inflammatory burden index and prognosis in patients with coronary heart disease: a retrospective study. PLoS One. 2025;20(7):e0325287. doi:10.1371/journal.pone.0325287
13. Byrne RA, Rossello X, Coughlan JJ, et al. ESC guidelines for the management of acute coronary syndromes. Eur Heart J. 2023;44(38):3720–3826. doi:10.1093/eurheartj/ehad191
14. Thygesen K, Alpert JS, Jaffe AS, et al. Fourth universal definition of myocardial infarction. J Am Coll Cardiol. 2018;72(18):2231–2264. doi:10.1016/j.jacc.2018.08.1038
15. McDonagh TA, Metra M, Adamo M, et al. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure [published correction appears in. Eur Heart J. 2021 Dec;42(48):4901]. Eur Heart J. 2021;42(36):3599–3726. doi:10.1093/eurheartj/ehab368
16. Hicks KA, Mahaffey KW, Mehran R, et al. Cardiovascular and stroke endpoint definitions for clinical trials. J Am Coll Cardiol. 2018;71(9):1021–1034. doi:10.1016/j.jacc.2017.12.048
17. Wen ZG, Long JJ, Wang Y. Association between inflammatory burden index and coronary slow flow phenomenon in patients with chest pain and no obstructive coronary arteries. BMC Cardiovasc Disord. 2024;24(1):595. doi:10.1186/s12872-024-04281-4
18. Hung M-J, Cherng W-J, Cheng C-W, Li L-F. Comparison of serum levels of inflammatory markers in patients with coronary vasospasm without significant fixed coronary artery disease versus patients with stable angina pectoris and acute coronary syndromes with significant fixed coronary artery disease. Am J Cardiol. 2006;97(10):1429–1434. doi:10.1016/j.amjcard.2005.12.035
19. Faccini A, Kaski JC, Camici PG. Coronary microvascular dysfunction in chronic inflammatory rheumatoid diseases. Eur Heart J. 2016;37(23):1799–1806. doi:10.1093/eurheartj/ehw018
20. Semerdzhieva NE, Dimitrov S, Tsakova A, Gospodinova M, Atanasov P, Lozanova V. Markers in acute coronary syndrome: distal coronary embolism at percutaneous coronary intervention. J Cardiovasc Develop Dis. 2025;12(8):315. doi:10.3390/jcdd12080315
21. Fichtlscherer S, Zeiher AM. Endothelial dysfunction in acute coronary syndromes: association with elevated C-reactive protein levels. Ann Med. 2000;32(8):515–518. doi:10.3109/07853890008998830
22. Zahorec R. Neutrophil-to-lymphocyte ratio, past, present and future perspectives. Bratisl Lek Listy. 2021;122(7):474–488. doi:10.4149/BLL_2021_078
23. Afari ME, Bhat T. Neutrophil to lymphocyte ratio (NLR) and cardiovascular diseases: an update. Expert Rev Cardiovasc Ther. 2016;14(5):573–577. doi:10.1586/14779072.2016.1154788
24. Zhang R, Pan Y, Ren YK, et al. Mediating effect of the NLR on the relationship between HbA1c and left atrial stiffness in overweight patients with hypertension. Am J Hypertens. 2024;37(8):597–603. doi:10.1093/ajh/hpae043
25. Bai B, Cheng M, Jiang L, Xu J, Chen H, Xu Y. High neutrophil to lymphocyte ratio and its gene signatures correlate with diastolic dysfunction in heart failure with preserved ejection fraction. Front Cardiovasc Med. 2021;8:614757. doi:10.3389/fcvm.2021.614757
26. Anzai T. Inflammatory mechanisms of cardiovascular remodeling. Circ J. 2018;82(3):629–635. doi:10.1253/circj.CJ-18-0063
27. Gürdal A, Keskin K, Siğirci S, Yildiz SS, Kiliçkesmez KO. Prognostic value of the neutrophil-to-lymphocyte ratio in patients with myocardial infarction with non-obstructive coronary arteries. Angiology. 2020;71(9):812–816. doi:10.1177/0003319720938621
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Thrombo-Inflammatory Prognostic Scores Improve BISAP-Based Risk Stratification in Acute Pancreatitis Patients: A Retrospective Cohort Study
Han T, Cheng T, Liao Y, Lai Q, Tang S, Liu B, He Y, Lei C, Cao Y, Cao Y
Journal of Inflammation Research 2022, 15:3323-3335
Published Date: 4 June 2022
A Novel Biomarker Scoring System Alone or in Combination with the GRACE Score for the Prognostic Assessment in Non-ST-Elevation Myocardial Infarction
Yao Y, Shao C, Li X, Wang Z, Zuo C, Yan Y, Lv Q
Clinical Epidemiology 2022, 14:911-923
Published Date: 2 August 2022
Prognostic Value of Inflammation-Immunity-Nutrition Score and Inflammatory Burden Index for Hepatocellular Carcinoma Patients After Hepatectomy
Song R, Ni H, Huang J, Yang C, Qin S, Wei H, Luo J, Huang Y, Xiang B
Journal of Inflammation Research 2022, 15:6463-6479
Published Date: 28 November 2022
A New Scoring System for Predicting Ventricular Arrhythmia Risk in Patients with Acute Myocardial Infarction
Sun L, Han B, Wang Y, Zhu W, Jiang J, Zou A, Chi B, Mao L, Ji Y, Wang Q, Tang L
Clinical Interventions in Aging 2023, 18:283-292
Published Date: 21 February 2023
Clinical Analysis and Prognostic Prediction Model for Patients with Uterine Leiomyosarcoma at FIGO Stage I
Chen S, Deng Y, Zhai Y, Zhan Y, Li X, Wang J, Bai H
International Journal of Women's Health 2023, 15:545-557
Published Date: 11 April 2023