Back to Journals » Journal of Inflammation Research » Volume 16
Increased Systemic Immune-Inflammation Index Was Associated with Type 2 Diabetic Peripheral Neuropathy: A Cross-Sectional Study in the Chinese Population
Authors Li J, Zhang X, Zhang Y, Dan X ![]() , Wu X, Yang Y, Chen X, Li S, Xu Y, Wan Q
, Wu X, Yang Y, Chen X, Li S, Xu Y, Wan Q ![]() , Yan P
, Yan P ![]()
Received 4 August 2023
Accepted for publication 8 November 2023
Published 11 December 2023 Volume 2023:16 Pages 6039—6053
DOI https://doi.org/10.2147/JIR.S433843
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Adam Bachstetter
Jia Li,1– 5,* Xing Zhang,1– 5,* Yi Zhang,1– 5,* Xiaofang Dan,1– 5 Xian Wu,1– 5 Yuxia Yang,1– 5 Xiping Chen,6 Shengxi Li,7 Yong Xu,1– 5 Qin Wan,1– 5 Pijun Yan1– 5
1Department of Endocrinology and Metabolism, the Affiliated Hospital of Southwest Medical University, Luzhou, People’s Republic of China; 2Metabolic Vascular Disease Key Laboratory of Sichuan Province, Luzhou, People’s Republic of China; 3Sichuan Clinical Research Center for Nephropathy, Luzhou, People’s Republic of China; 4Cardiovascular and Metabolic Diseases Key Laboratory of Luzhou, Luzhou, People’s Republic of China; 5Sichuan Clinical Research Center for Diabetes and Metabolism, Luzhou, China, Luzhou, People’s Republic of China; 6Clinical medical college, Southwest Medical University, Luzhou, People’s Republic of China; 7Basic Medical College, Southwest Medical University, Luzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Pijun Yan, Department of Endocrinology, The Affiliated Hospital of Southwest Medical University, Luzhou, Sichuan, 646000, People’s Republic of China, Tel/Fax +86-830-3165361, Email [email protected]
Background: Systemic immune-inflammation index (SII), a novel inflammatory marker, has been demonstrated to be associated with type 2 diabetes mellitus (T2DM) and its vascular complications, however, the relation between SII and diabetic peripheral neuropathy (DPN) has been never reported. We aimed to explore whether SII is associated with DPN in Chinese population.
Methods: A cross-sectional study was conducted among 1460 hospitalized patients with T2DM. SII was calculated as the platelet count × neutrophil count/lymphocyte count, and its possible association with DPN was investigated by correlation and multivariate logistic regression analysis, and subgroup analyses.
Results: Patients with higher SII quartiles had higher vibration perception threshold and prevalence of DPN (all P< 0.01), and SII was independently positively associated with the prevalence of DPN (P< 0.01). Multivariate logistic regression analysis showed that the risk of prevalence of DPN increased progressively across SII quartiles (P for trend < 0.01), and participants in the highest quartile of SII was at a significantly increased risk of prevalent DPN compared to those in the lowest quartile after adjustment for potential confounding factors (odds rate: 1.211, 95% confidence intervals 1.045– 1.404, P< 0.05). Stratified analysis revealed positive associations of SII quartiles with risk of prevalent DPN only in men, people less than 65 years old, with body mass index < 24 kg/m2, duration of diabetes > 5 years, hypertension, dyslipidaemia, poor glycaemic control, and estimated glomerular filtration rate < 90 mL/min/1.73 m2 (P for trend < 0.01 or P for trend < 0.05). The receiver operating characteristic curve analysis revealed that the optimal cut-off point of SII for predicting DPN was 617.67 in patients with T2DM, with a sensitivity of 45.3% and a specificity of 73%.
Conclusion: The present study showed that higher SII is independently associated with increased risk of DPN, and SII might serve as a new risk biomarker for DPN in Chinese population.
Keywords: systemic immune-inflammation index, diabetic peripheral neuropathy, vibration perception threshold, type 2 diabetes mellitus, Chinese population
Introduction
Diabetic peripheral neuropathy (DPN) is one of the most common long-term complications of diabetes that frequently presents with peripheral nerve dysfunction accompanied with typical characteristics of pain and numbness, which not only results in an increase in the risk of foot ulceration and subsequent amputation, but also leads to a considerable disability and cardiovascular mortality.1–3 Therefore, DPN has posted a great challenge for both medical professionals and the entire society. Despite a high lifetime prevalence of approximately 50%,4 the symptoms are insidious in onset,1 and there is no approved therapy to prevent or cure DPN apart from good glycemic therapy.3 Therefore, emphasis should be laid on effective surveillance, early detection and diagnosis of DPN.
Although the pathogenesis is complex and not well established, chronic inflammation has been suggested to be involved in the occurrence and development of DPN.5,6 Recently, close interaction of inflammation and immune system-related cells such as neutrophils, lymphocytes, and platelets, and their combinations such as neutrophil-to-lymphocyte (NLR) and platelet-to-lymphocyte (PLR) with the pathogenesis of DPN has attracted great attention.7–9 However, these indicators that include just one or two kinds of immune-inflammatory cells may not adequately reflect the state of inflammation. The systemic immune-inflammation index (SII), an integrated and novel inflammatory biomarker integrating three different cells, could better and more objectively reflect the state of inflammation and immune balance in the body compared with neutrophil and lymphocyte counts as well as the NLR and PLR,10–12 and has been developed to predict and evaluate the prognosis and clinical outcomes of various malignant tumors types, autoimmune disorders, atherosclerotic cardio-cerebrovascular diseases, and other diseases.10,11,13–16 Moreover, emerging data have also shown that elevated levels of SII were found to be associated with diabetes mellitus, diabetic retinopathy (DR), diabetic kidney disease (DKD), and diabetic foot infections,17–21 all of which are associated with high burden of inflammation.22–24 Considering the role of chronic inflammation in the pathogenesis of DPN, and that DPN, DR, DKD, and diabetic foot infections share multiple common pathogenetic pathways and risk factors, such as inflammation, thus elevated levels of SII may be associated with the development of DPN. As far as we are aware, the relationship of the SII with DPN, however, has never been investigated.
Therefore, the objective of the present study was to investigate the relationship between SII and risk of presence of DPN in Chinese adults with type 2 diabetes mellitus (T2DM), which may help clinicians early recognize patients at high risk for DPN and initiate the prompt, appropriate treatment for prevention.
Materials and Methods
Study Population
This is a cross-sectional study, where T2DM inpatients aged 18–89 years were recruited from August 2012 to September 2015 in the department of Endocrinology and Metabolism at the Affiliated Hospital of Southwest Medical University. T2DM was defined according to the 1999 World Health Organization (WHO) diagnostic criteria.25 Subjects with diabetic foot ulcers and amputation were excluded from the study. Diabetic subjects with stroke were not an exclusion criterion. The details of the other inclusion and exclusion criteria are described elsewhere.26 Ultimately, 1460 eligible participants (716 men and 744 women) were included in the analysis.
The study was approved by the Ethics Committee of the Affiliated Hospital of Southwest Medical University in China, and informed consent was obtained from all patients before data collection. Study procedures were performed in accordance with the Declaration of Helsinki ethical principles for medical research involving human subjects.
General Clinical and Biochemical Measurements
A face-to-face interview was carried out by trained interviewers to collect data, including demographic data, lifestyle (smoking and drinking status, etc.), personal medical history, duration of diabetes, and family history of diabetes. Body weight in light clothes and without shoes was measured with a digital scale to the nearest 0.1 kg, and height was measured without shoes to the nearest 0.1 cm. Body mass index (BMI) was calculated as weight in kilograms divided by the square of height in meters. The patients’ systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured three times using a mercury sphygmomanometer while the subject in a sitting position, and the mean value was recorded.26
After all subjects had fasted for at least 8 h, venous blood samples were collected. Fasting blood glucose (FBG), 2 hour postprandial blood glucose (PBG), total cholesterol (TC), triglyceride (TG), high density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), and serum creatinine (Cr) were measured using a 7060 full-automatic biochemical analyzer (Hitachi) at the registered central laboratory located at the Affiliated Hospital of Southwestern Medical University. Glycated hemoglobin A1C (HbA1c) was measured by the anion exchange high performance liquid chromatography (Arkray Eluent 80A). Neutrophil count, lymphocyte count, and platelet (PLT) count were determined using an automated blood cell counter (Mindray BC-6800). The NLR was calculated by dividing the neutrophil count by lymphocyte count. The SII was calculated as platelet × neutrophil/lymphocyte counts.6 The glycemic exposure (GE) index was calculated using the following equation: GE index = (HbA1c)1/2x (duration of DM in years)1/8.27 The estimated glomerular filtration rate (eGFR) was estimated using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation that includes age, sex, and race.26,28
According to the manufacturer’s instructions, urinary albumin and creatinine were measured from three fresh morning spot urine sample on three separate occasions within 6 months, and the urinary albumin-to-creatinine ratio (ACR) was computed and was reported in milligrams per gram (mg/g).29
Assessment and Diagnostic Criteria of DPN
All T2DM patients were asked whether they had neuropathic symptoms, including numbness, pain (prickling or stabbing, shooting, electric shocks, burning or aching pain), and paresthesia (abnormal cold or heat sensation, allodynia and hyperalgesia) in the toes, feet, legs or upper-limb. Vibration perception threshold (VPT) was assessed at the metatarsophalangeal joint dig I using a neurothesiometer (Bio-Thesiometer; Bio-Medical Instrument Co., Newbury, OH, USA) according to previously published methods.29 A VPT ≥ 15 V was defined as impaired vibration perception.30–32 DPN was diagnosed clinically based on the presence of one or more neuropathic symptoms and impaired vibration perception in the feet,30,31 and then participants were divided into DPN group and no DPN group.
Other Classifications and Definitions
According to the Chinese Guidelines on Prevention and Treatment of obesity in Adults, participants with a BMI of 24–27.9 kg/m2 were defined as overweight, and obesity was defined as BMI of ≥28 kg/m2.33 Hypertension was defined as SBP ≥ 140 mmHg, DBP ≥ 90 mmHg, or use of antihypertensive medication.26,32,34 Dyslipidaemia was defined as either incident abnormal lipid laboratory results (comprised of TC > 200 mg/dL, TG > 150 mg/dL, LDL-C >130 mg/dL, or HDL-C <40 mg/dL) or incident lipid-lowering medications prescriptions (consisting of prescription of statins, bile acid resins, and fibrates).35 Glycaemic control was assessed in terms of the HbA1c level and poor glycaemic control was defined as HbA1c ≥7% and a level <7% reflects good glycaemic control, according to the American Diabetes Association.36 Coronary heart disease (CHD) was defined as a positive history of myocardial infarction, bypass operation, a diagnostic finding in angiography or positive exercise test.26,34 Stroke was considered present if diagnosed according to previous medical records or if a pathological finding by CT and MRI of the brain.34 Peripheral arterial disease (PAD) was considered present in all subjects with an ankle-brachial index (ABI) < 0.9 in one leg, and/or a history of prior treatment for PAD.26,29,34 DR was determined by using fundus photography (Canon Inc., Kanagawa, Japan), which was performed by an ophthalmologist.26,29,34 A participant with an eGFR < 90 mL/min/1.73 m2 was considered to have impaired renal function, and mild and moderate impaired renal function were defined as 60 ≤eGFR < 90 mL/min/1.73 m2 and 30 ≤eGFR < 60 mL/min/1.73 m2 respectively.37,38 Albuminuria was defined as urinary ACR ≥ 30 mg/g.29 Albuminuria was then divided into microalbuminuria (30 mg/g ≤ urinary ACR < 300 mg/g) and macroalbuminuria (urinary ACR ≥ 300 mg/g).39,40 DKD was diagnosed with eGFR < 60 mL/min/1.73 m2, albuminuria, or both in T2DM patients.26,29,34
Statistical Analysis
Statistical analyses were conducted using the Statistical Package for Social Sciences (SPSS) (version 20.0; IBM, Chicago, IL). For continuous variables, results were presented as mean ± standard deviation (SD). Continuous variables were compared by Student’s t test and one-way analysis of variance (ANOVA), whereas skewed distribution variables were compared by Mann-Whitney U and Kruskal–Wallis tests. For categorical variables, results were presented as n (%), and intergroup comparisons were analyzed using a χ2 test. Correlations between variables were examined using Spearman correlation analysis and partial correlation analysis. The univariate and multivariable logistic regression analyses were conducted to investigate the association of SII and other variables with the risk of presence of DPN. We then categorized patients into four quartile groups by SII levels: quartile (Q)1 group, 71.16–328.44; Q2 group, 328.49–478.92; Q3 group, 479.89–735.59; and Q4 group, 741.09–7173.95. Binary logistic regression analyses were conducted to investigate the association between SII quartiles and DPN. The Q1 served as the reference group. The odds ratios (ORs) and 95% confidence intervals (CI) were reported. Possible dose-response relationships between SII levels and DPN were examined by the trend test. We also conducted stratified analyses by sex (men and women), age (≥65 and <65 years), BMI (≥24 and <24 kg/m2), duration of diabetes (>5 and ≤5 years), hypertension (Yes and No), dyslipidaemia (Yes and No), poor glycaemic control (Yes and No), and eGFR (≥90 and <90 mL/min/1.73 m2) to further validate the consistency of the above-mentioned findings. Last, the predictive validity of SII for the presence of DPN was determined using receiver operating characteristic (ROC) curves and area under the curve (AUC) in all subjects, male subjects, and female subjects. All tests were two-tailed, and P-value of <0.05 was considered statistically significant.
Results
Clinical and Laboratory Characteristics
Clinical and laboratory characteristics of participants are given in Table 1. Among the 1460 participants included in this study, 590 participants (40.41%) had DPN. The prevalence of DPN according to SII quartiles were 31.23%, 32.88%, 41.64% and 55.89% respectively. The subjects with higher SII were more likely to be older (P < 0.05). Moving from the lowest to the highest SII quartile, we observed increased levels of FBG, PBG, HbA1c, GE index, neutrophil count, NLR, PLT count, serum Cr, urinary ACR, VPT, as well as increased percentages of participants with HbA1c ≥9% and VPT≥25V, prevalence of overweight, hypertension, microalbuminuria, macroalbuminuria, albuminuria, moderate impaired renal function, DKD, and PAD, and decreased levels of weight, BMI, TG, lymphocyte count, and eGFR (P<0.01 or P<0.05). No significant difference was seen between SII quartiles for sex distribution, height, duration of diabetes, smoking, drinking, SBP, DBP, TC, HDL-C, LDL-C, ABI, percentages of participants with HbA1c 7–9% and VPT 15–25V, prevalence of obesity, dyslipidaemia, DR, mild impaired renal function, CHD, and Stroke (P>0.05). Supplementary Table 1 reported characteristics of all T2DM patients by DPN. In type 2 diabetic patients, participants with DPN showed significantly older age, longer duration of diabetes, less drinking, higher levels of SBP, GE index, HbA1c, neutrophil count, NLR, SII, serum Cr, urinary ACR, VPT, prevalence of hypertension, microalbuminuria, macroalbuminuria, albuminuria, DKD, DR, CHD, stroke, and PAD, and lower TC, TG, DBP, lymphocyte count, eGFR, ABI, and prevalence of overweight and dyslipidaemia (P<0.01 or P<0.05). Supplementary Table 2 reported characteristics of all T2DM patients by sex. Compared with men, the women had significantly older age, longer duration of diabetes, less smoking and drinking, higher levels of lymphocyte count, PLT count, percentages of participants with HbA1c <7%, prevalence of hypertension, DR, and PAD, and lower FBG, PBG, HbA1c, NLR, ABI, percentages of participants with HbA1c ≥9%, and prevalence of overweight, dyslipidaemia, macroalbuminuria, albuminuria, DKD, and PAD (P<0.01 or P<0.05).
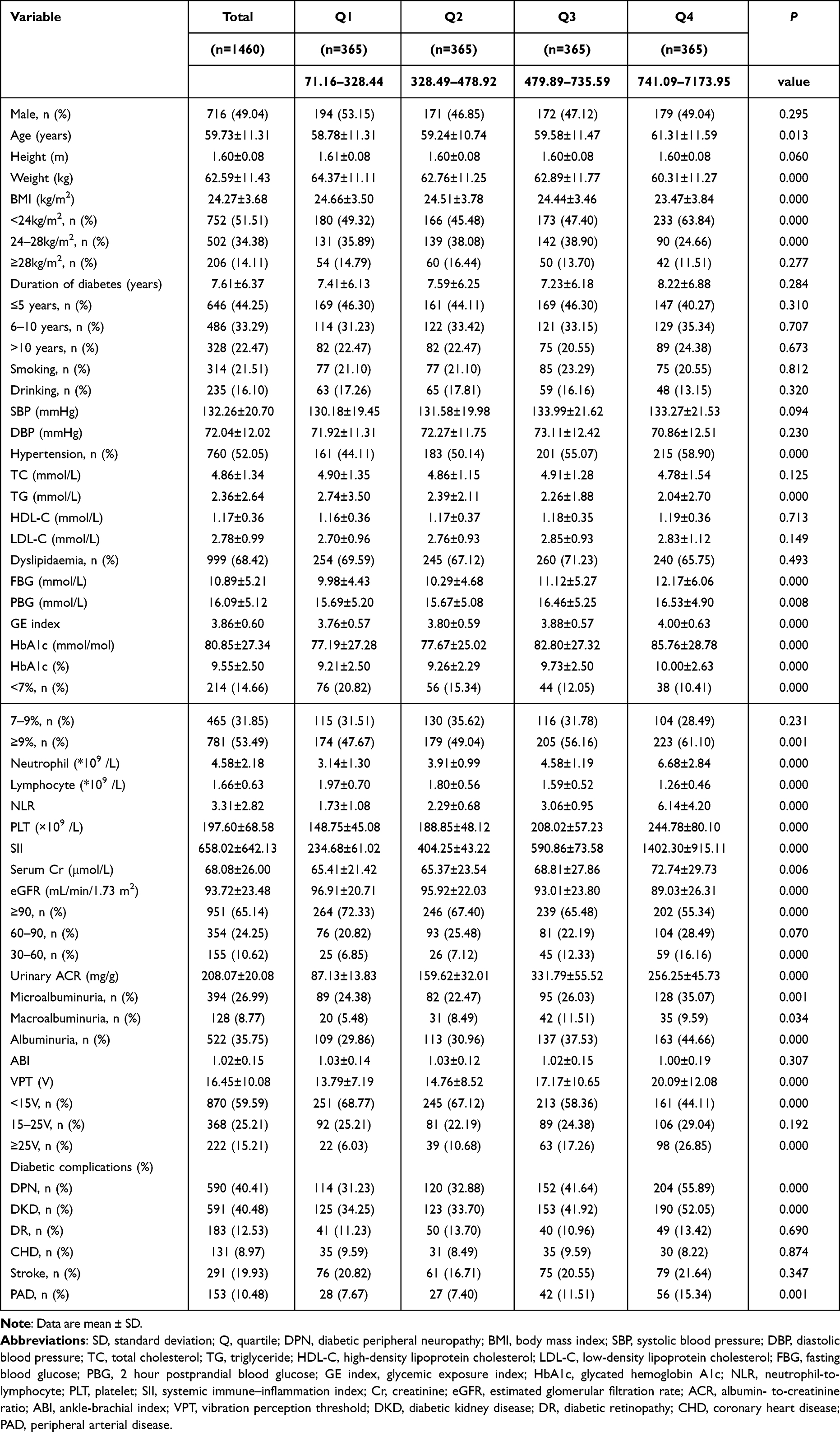 |
Table 1 Characteristics of Study Participants According to SII Quartiles |
The Relationships Between SII and DPN- Related Risk Factors
Spearman correlation analysis showed that SII was positively associated with age, SBP, FBG, PBG, GE index, HbA1c, neutrophil count, NLR, PLT count, serum Cr, urinary ACR and VPT and the prevalence of hypertension, microalbuminuria, macroalbuminuria, albuminuria, moderate impaired renal function, DKD, DPN, and PAD, and negatively with BMI, drinking, TC, TG, lymphocyte count, and eGFR (P<0.01 or P<0.05; Table 2). Partial correlation analysis controlling for sex, age, BMI, and duration of diabetes demonstrated that SII was positively associated with FBG, PBG, GE index, HbA1c, neutrophil count, PLT count, serum Cr, VPT, prevalence of obesity, hypertension, microalbuminuria, albuminuria, moderate impaired renal function, DKD, DPN, PAD, and inversely correlated with TC, lymphocyte count, eGFR, and ABI (P<0.01 or P<0.05; Table 2).
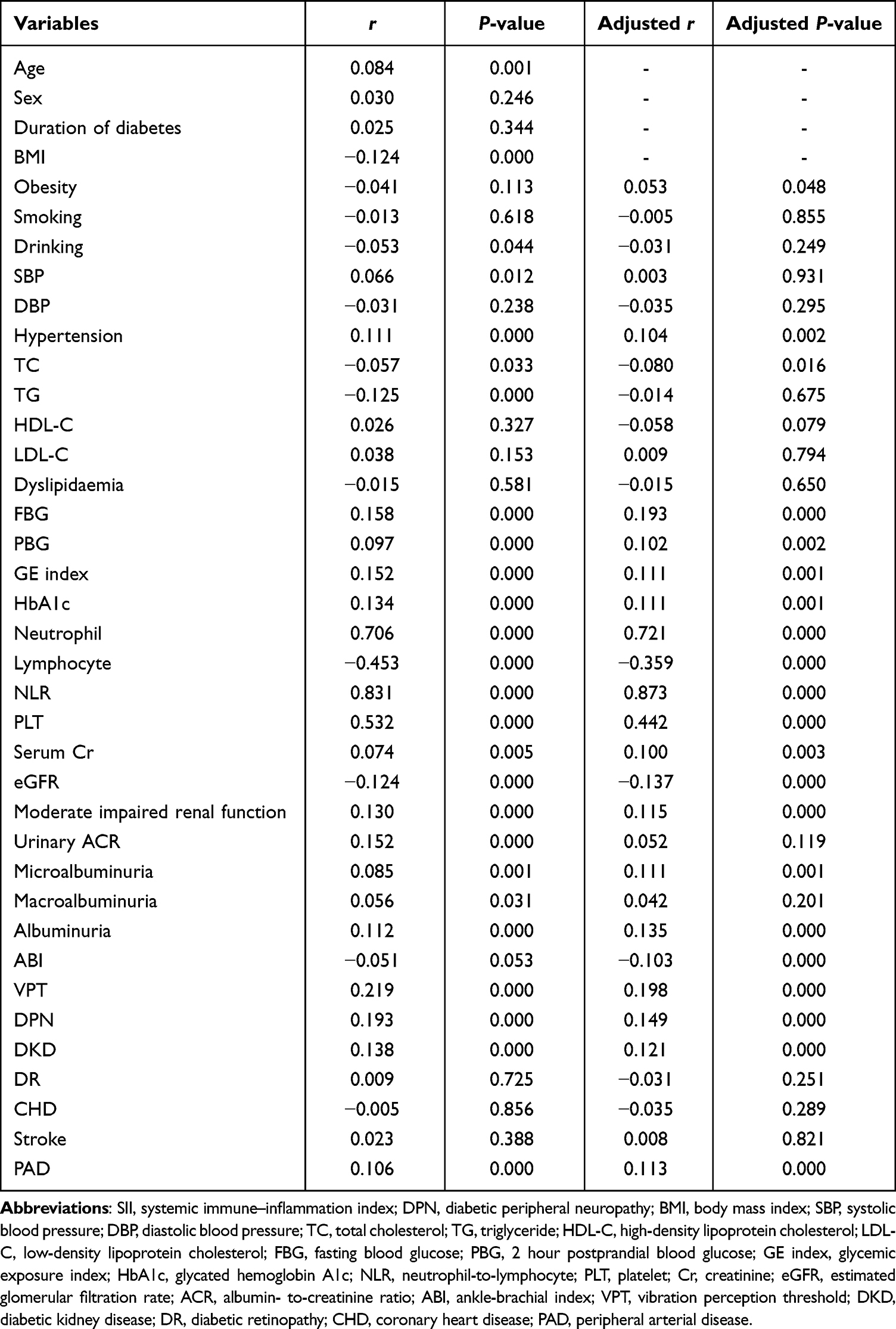 |
Table 2 The Relationships between SII and DPN-Related Risk Factors |
Univariate and Multivariate Logistic Analysis of Factors Associated with DPN
Table 3 shows univariable and multivariable analyses of factors associated with DPN. On univariable analysis, age, duration of diabetes, GE index, HbA1c, NLR, SII, hypertension, dyslipidaemia, DKD, DR, CHD, stroke, and PAD were significantly associated with DPN (P<0.01 or P<0.05). SII remained independently significantly associated with an increased risk of DPN on multivariable analysis (OR = 1.001, 95% CI 1.000–1.001; P<0.05).
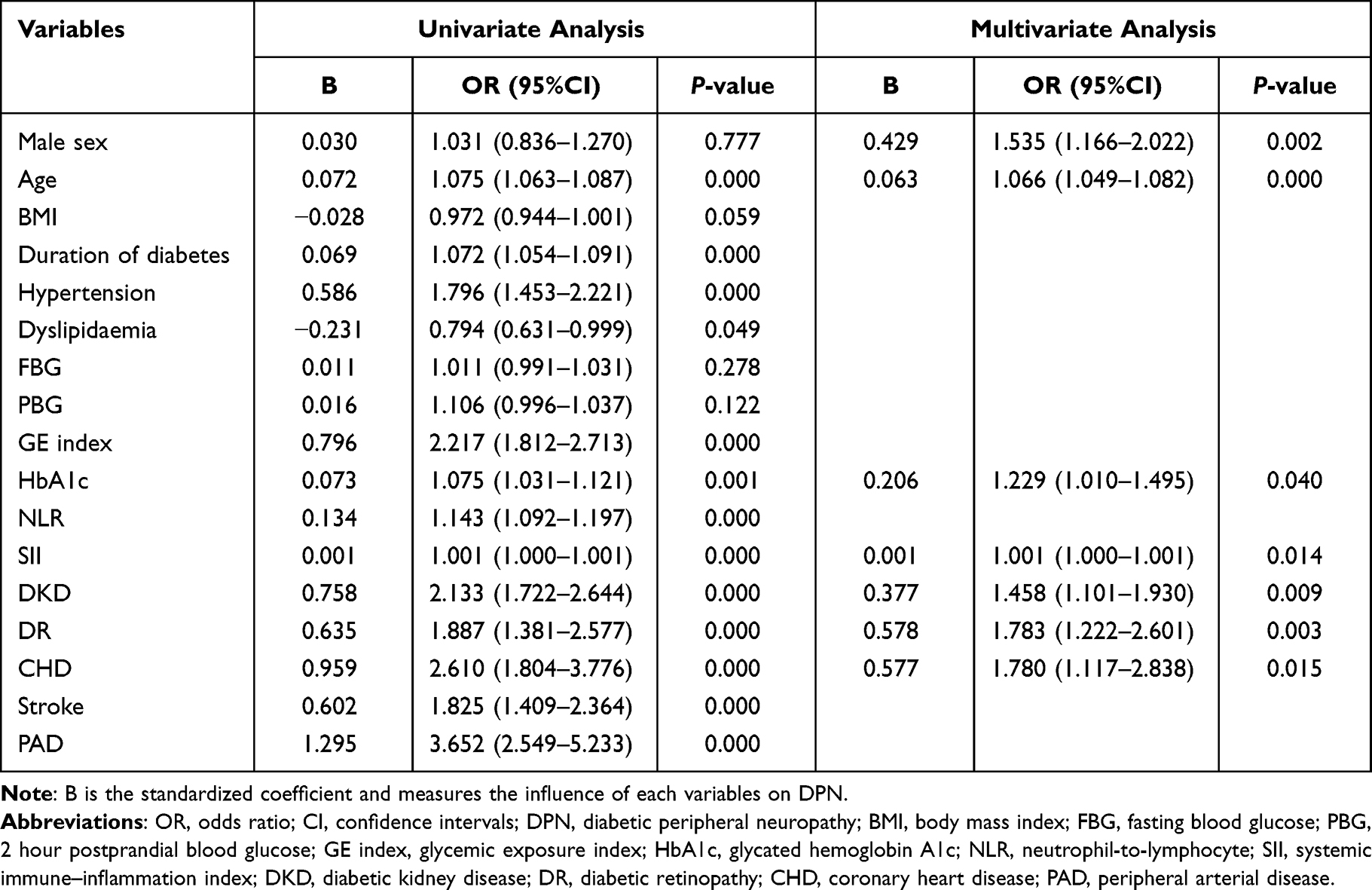 |
Table 3 Univariate and Multivariate Logistic Analysis of Factors Associated with DPN |
Adjusted ORs and 95% CIs for DPN According to SII Quartiles
As presented in Table 4, there was a 35.7% increase in DPN risk per SD increase in SII (OR = 1.357, 95% CI 1.041–1.769) after adjusting for sex, age, BMI, duration of diabetes, smoking, drinking, hypertension, dyslipidaemia, HbA1c, NLR, DKD, DR, CHD, stroke, and PAD. A graded association with DPN and increase in SII quartiles was observed (P for trend <0.01). Participants in the highest quartile of SII had a significantly higher risk of DPN compared with those in Q1 (OR = 1.211, 95% CI 1.045–1.404). Moreover, there was a significant association of DPN in participants with the highest SII compared with those with lower SII levels (OR for Q4 versus Q1, 2, 3 = 1.517, 95% CI 1.069–2.154) after multivariate adjustment.
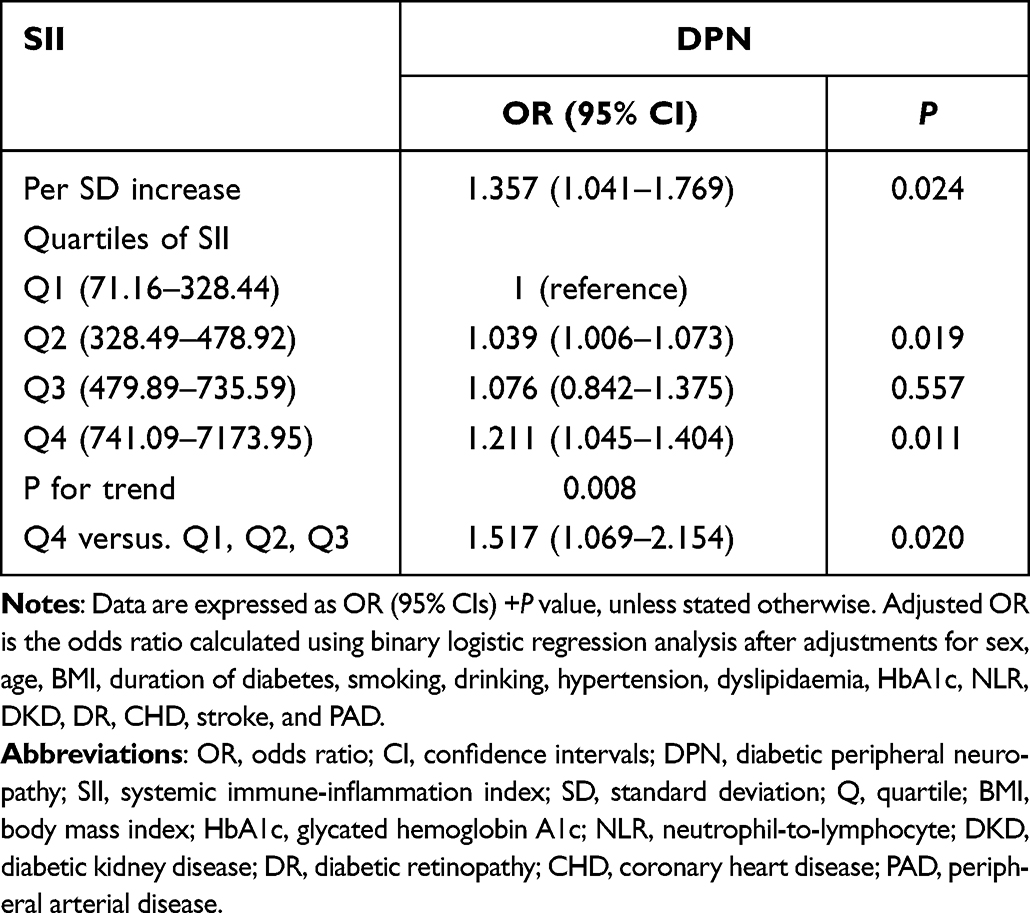 |
Table 4 Adjusted ORs and 95% CIs for DPN According to SII Quartiles |
Association of SII Quartiles with Increased Risk of DPN in Stratified Analysis
Stratified analyses were adopted in the different subgroups to further validate the above-mentioned results, shown in Table 5. After comprehensive adjustment of sex, age, BMI, duration of diabetes, smoking, drinking, hypertension, dyslipidaemia, HbA1c, NLR, DKD, DR, CHD, stroke, and PAD, except the strata variable, higher SII quartiles showed significant correlations with elevated risk of DPN prevalence only in men, people less than 65 years old, with BMI < 24 kg/m2, duration of diabetes >5 years, hypertension, dyslipidaemia, poor glycaemic control, and eGFR <90 mL/min/1.73 m2 (P for trend <0.01 or P for trend <0.05). Interactions of age, duration of diabetes, hypertension, dyslipidaemia, hypertension, dyslipidaemia and poor glycaemic control, and eGFR stratification with SII quartiles were significant (P for interaction <0.01 or P for interaction< 0.05).
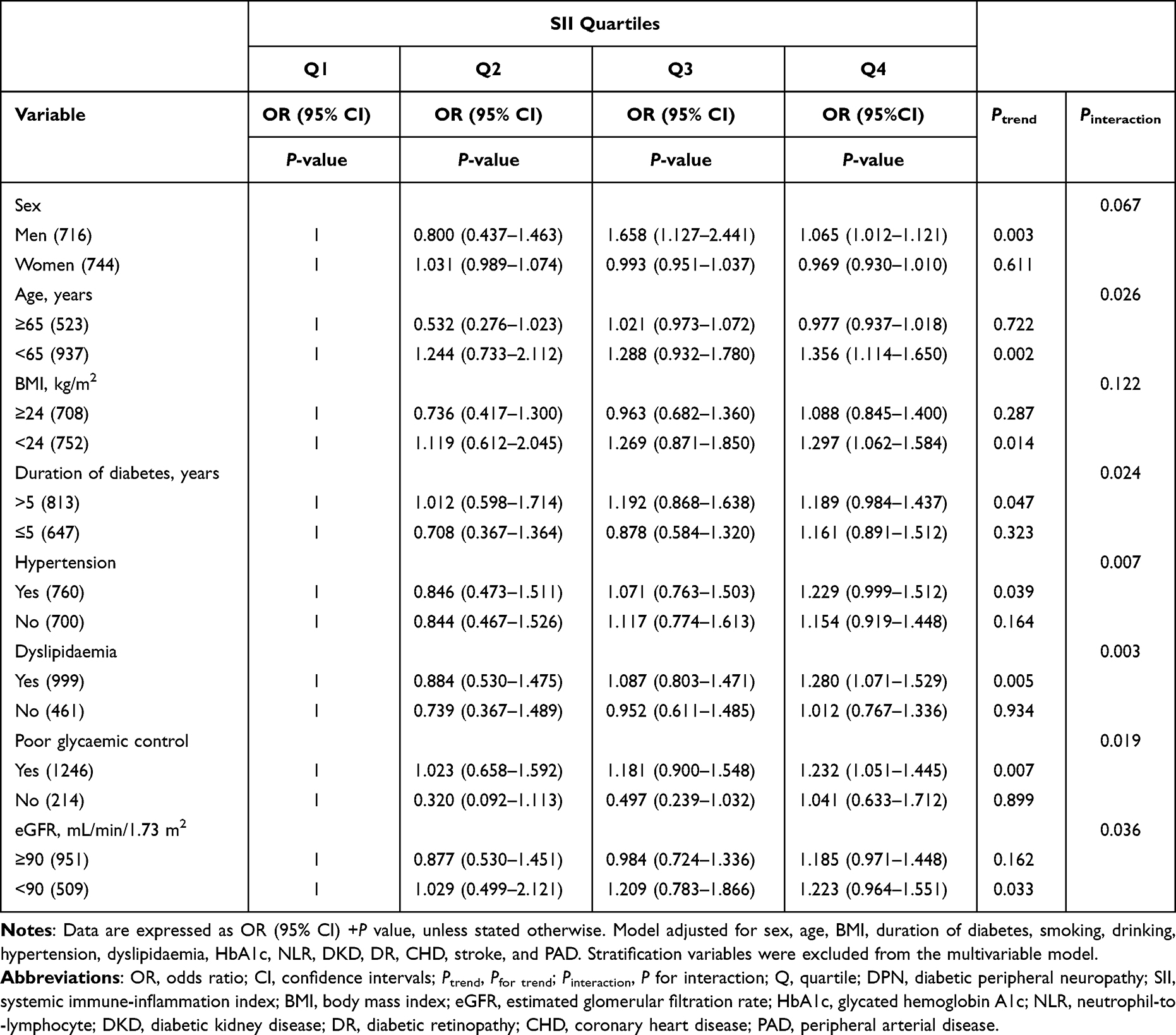 |
Table 5 Stratified Analyses of SII and Risk of Prevalence of DPN by Sex, Age, BMI, Duration of Diabetes, Hypertension, Dyslipidaemia, Poor Glycaemic Control, and eGFR |
Predictive Value of SII in Screening for the Presence of DPN in T2DM Patients
To further explore the predictive value of SII for DPN, the ROC curve analysis was performed. As shown in Figure 1, the best cut-off value for SII to predict the presence of DPN was 617.67 (sensitivity: 45.3%; specificity: 73%; and AUC: 0.614; Figure 1A), 557.25 (sensitivity: 55.8%; specificity: 72.4%; and AUC: 0.662; Figure 1B), and 617.67 (sensitivity: 41.6%; specificity: 69.5%; and AUC: 0.564; Figure 1C) in all diabetic subjects, male diabetic subjects, and female diabetic subjects, respectively.
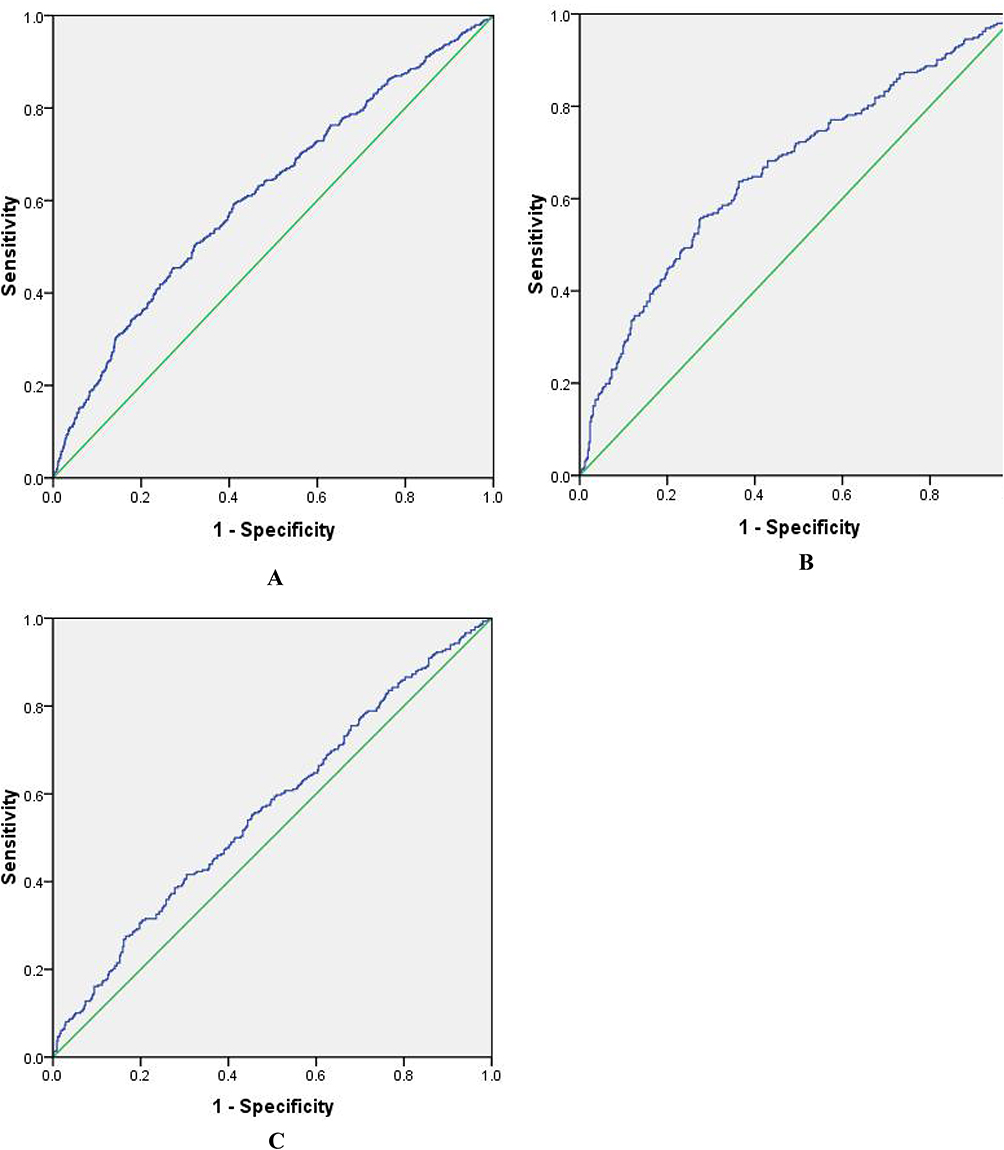 |
Figure 1 (A) ROC analysis of SII to indicate DPN for all subjects. AUC = 0.614; 95% CI: 0.584–0.641; P <0.05; identified SII cutoff value = 617.67; Youden index = 0.183; sensitivity: 45.3%; specificity: 73%. (B) ROC analysis of SII to indicate DPN for male subjects. AUC = 0.662; 95% CI: 0.621–0.703; P <0.05; identified SII cutoff value = 557.25; Youden index = 0.282; sensitivity: 55.8%; specificity: 72.4%. (C) ROC analysis of SII to indicate DPN for female subjects. AUC = 0.564; 95% CI: 0.522–0.606; P <0.05; identified SII cutoff value = 617.67; Youden index = 0.111; sensitivity: 41.6%; specificity: 69.5%. Abbreviations: ROC, receiver operating characteristic; SII, systemic immune-inflammation index; DPN, diabetic peripheral neuropathy; AUC, area under the curve. |
Discussion
To our knowledge, this is the first study to explore the potential association of SII with DPN in Chinese patients with T2DM. We revealed that T2DM patients with DPN had significantly elevated SII levels, and the risk of DPN progressively increased across SII quartiles. Additionally, stratified analysis showed that subjects with higher SII quartiles had an increased risk of DPN than those with lower quartiles, especially in men, people less than 65 years old, with BMI<24 kg/m2, duration of diabetes >5 years, hypertension, dyslipidaemia, poor glycaemic control, and eGFR <90 mL/min/1.73 m2. Last, the ROC curve analysis revealed that the optimal cut-off point of SII for predicting DPN was 617.67 in patients with T2DM, with a sensitivity of 45.3% and a specificity of 73%. These findings suggest that high SII may be associated with the presence of DPN in Chinese patients with T2DM, and may be used as an additional indicator of risk of DPN.
There is substantial evidence showing that low-grade inflammation are also contributing factors in the development and progression of T2DM and its microvascular complications, such as DPN.5,6,18,21,26 SII is a relatively novel inflammation biomarker based on peripheral lymphocyte, neutrophil, and platelet counts, which largely reflects three pathways of inflammatory response, thrombus formation and adaptive immune response in the host.41–43 Studies have demonstrated that SII can predict the prognosis and clinical outcomes of certain inflammatory diseases, various atherosclerotic cardio-cerebrovascular diseases (eg myocardial infarction, heart failure, stroke, peripheral arterial disease), and other diseases,16,42–45 and may be associated with s metabolic disorder and its components, such as diabetes mellitus, metabolic syndrome, dyslipidemia, central obesity, DR, DKD, diabetic foot infections16–18,37 that are closely associated with low-grade inflammation,22–24 suggesting that SII may be associated with the presence of DPN, and high SII may be an early signal for being at risk for DPN. In the present study, we found that patients in the highest quartile of SII levels had significantly higher prevalence of DPN, percentages of participants with VPT ≥ 25V, and levels of VPT, a widely recommended indicator of the presence and severity of confirmed clinical neuropathy,26 than those in the lowest quartile. Likewise, increased levels of SII were observed in patients with DPN. Moreover, SII was found to be positively associated with VPT levels and prevalence of DPN, even after adjusting for sex, age, BMI, and duration of diabetes. These results together demonstrated that elevated SII seem to be closely associated with DPN. In addition, we observed that SII was independently associated with an increased risk of DPN even after multivariable adjustment, and the risk of DPN was progressively increased across SII quartiles. Of note, participants in the highest quartile of SII had a 51.7% increased risk of developing DPN compared to those in the lower quartiles. These results indicate that there may be a potential mechanistic association between elevated levels of SII and the prevalence of DPN. More importantly, SII could predict the presence of DPN, especially in the male patients, suggesting that elevated SII may be an early signal for being at risk for DPN, and SII could be considered to be a sensitive parameter in predicting the DPN. SII can be considered as a modified powerful combination of NLR and PLR, and has been proposed to be more valuable than either NLR or PLR alone in predicting inflammatory status and prognosis in various clinical settings.12,46,47 Our findings are consistent with previous literature showing that inflammatory biomarkers, such as NLR and PLR were independently associated with DPN,7–9,48,49 further suggesting that SII, another marker of inflammation, could be linked to an increased risk of the presence and severity of DPN, and SII might be a novel and reliable predictive marker of DPN in Chinese patients with T2DM.
A particularly novel finding in this study is the sex disparities in the relationship between SII and DPN, namely, higher SII quartiles were significantly associated with the risk of prevalence of DPN in men but not in women in stratified analyses, which further was supported by the results of the multivariable logistic regression analysis showing that male sex was independently significantly associated with the risk of prevalence of DPN. Such a sex discrepancy might be attributed to several factors. First, compared with female diabetic patients, male diabetic patients had significantly poorer glycaemic control (higher levels of FBG, PBG, and HbA1c), greater prevalence of overweight, dyslipidaemia and macroalbuminuria, and higher levels of inflammation (higher NLR and lower lymphocyte), all of which have been reported to be related to DPN.26,50,51 Second, men’s lifestyle may be more hazardous than women’s is. Specifically, compared with women, men might have more smokers and drinkers, more stressful jobs, less seeking of health consultation and services, and lower compliance with treatment,51,52 which were risk factors for DPN.53–55 Third, testosterone deficiency may be another plausible explanation for the sex disparity observed in the association of SII with DPN. Studies have demonstrated that 7% of men would develop testosterone deficiency after 50 years old,56 and testosterone deficiency is more common in men with diabetes than those without,57 while male diabetic patients in our study had a mean age of over 58, resulting in an increased risk of testosterone deficiency. Moreover, epidemiological surveys have shown that circulating total testosterone level is inversely related to obesity, and the prevalence of testosterone deficiency is up to 79% in obese individuals,56 while our study population had an overweight/obesity prevalence of 51.54%. Therefore, many male diabetic patients in the present study are at risk for testosterone deficiency. It is reported that testosterone deficiency may lead to a more pronounced deficit of neurosteroids and further result in loss of function of neurosteroids’s protection and regeneration of peripheral nerves affected by different forms of pathologic alterations, ultimately leading to the development and development of DPN.52,57 Studies found that abnormal sex hormone levels may cause alterations in inflammatory state and immune response,16 and increased risk of testosterone deficiency is associated with the SII in men.16,56 These results together demonstrated that there might be a positive correlation between SII and testosterone deficiency and DPN, and testosterone deficiency might at least partially mediate the potential relationship between SII and DPN. Nevertheless, the current research cannot fully explain this phenomenon, more evidence is needed to illuminate the actual mechanisms of gender difference in the association of SII with DPN risk.
Compelling data indicate that advanced age and overweight/obesity play important roles in the development and progression of DPN.7,34 The present study also revealed that T2DM patients with DPN had significantly older age than those without, and age was independently significantly associated with the risk of prevalence of DPN, further supporting the role of advanced age in DPN. However, the stratified analysis demonstrated a significant correlation of higher SII quartiles with an increased risk for DPN prevalence in subjects aged < 65 years old but not those aged ≥ 65 years old, which be due to several factors. First, a significant difference in sample size of two subgroups might lead to imprecise estimations. Second, there is an interaction of age with SII on DPN in T2DM patients, SII might impact the effect of the prevalence of DPN greater than the effect of age. Another surprising finding in our study is that a significantly association between SII and the risk of prevalence of DPN was only observed in non-overweight/obesity subjects in stratified analyses, which was consistent with previous literature from Yan et al and Tayama et al showing that visceral fat area and preperitoneal fat levels were positively correlated with nerve conduction velocity and amplitude potential,34,58 suggesting that there might be a complex mechanism correlation between overweight/obesity or visceral fat and DPN. In the present study, insignificant decrease in BMI was observed in T2DM patients with DPN, and SII was negatively associated with BMI, which were inconsistent with previous studies showing that higher baseline levels of BMI was associated with DPN59 and SII had a significant positive linear correlation with increased BMI.60 These seemingly contradictory results might by interpreted as unintentional weight loss in individuals with longstanding inadequate diabetes control as well as multiple systemic insults or comorbidities.61 In addition, although diabetic subjects with overweight/obesity are often accompanied by dyslipidemia, multiple macrovascular complications, such as CHD, hypertension, macrovascular arteriosclerosis, and microvascular complications than those without, they may become more concerned about their condition and adopt various measures, such as controlling blood glucose, blood pressure, and blood lipids, and making dietary and lifestyle changes that are beneficial for weight loss and improved neurological function,34 which may be one of the causes for the difference in the relationship between SII and DPN in diabetic subjects with and without overweight/obesity, but further studies need to be designed for confirmation.
Emerging studies have suggested that longer diabetes duration, poor glycaemic control, hypertension, dyslipidaemia, and impaired renal function are important risk factors for DPN.55,62 The present study also showed that T2DM subjects with DPN had significantly longer diabetes duration, higher GE index, HbA1c, proportions of poor glycaemic control, SBP, TG, urinary ACR, prevalence of hypertension, dyslipidaemia, impaired renal function, microalbuminuria, macroalbuminuria, albuminuria, and lower eGFR compared with those without. Moreover, the logistic regression analysis demonstrated that diabetes duration, GE index, hypertension, dyslipidaemia, especially HbA1c and DKD were significantly associated with the risk of prevalence of DPN. These results further suggested that longer diabetes duration, poor glycaemic control, hypertension, dyslipidaemia, and DKD might be correlated with the prevalence of DPN. In addition, the stratified analysis demonstrated significant correlations of higher SII quartiles with an increased risk for DPN only in subjects with diabetes duration >5 years, hypertension, dyslipidaemia, poor glycaemic control, and eGFR <90 mL/min/1.73 m2. Besides, we observed interactions of diabetes duration, poor glycaemic control, hypertension, dyslipidaemia, and eGFR with SII on DPN in T2DM subjects. Moreover, the subjects in the higher SII quartiles exhibited higher FBG, PBG, GE index, HbA1c, proportions of HbA1c ≥ 9%, urinary ACR, microalbuminuria, macroalbuminuria, albuminuria, and prevalence of hypertension, moderate impaired renal function, and DKD, and lower eGFR, and partial correlation analysis controlling for sex, age, BMI, and duration of diabetes demonstrated that SII was positively associated with FBG, PBG, GE index, HbA1c, prevalence of hypertension, microalbuminuria, albuminuria, moderate impaired renal function, DKD, and inversely correlated with eGFR. These results together suggested that interplays between elevated SII and longer diabetes duration, poor glycaemic control, hypertension, dyslipidaemia, and DKD synergistically contribute to the development and progression of DPN. Thus, it is of great importance to monitor SII for early screening for DPN among specific populations in the inflammatory states to further prevent and delay the development and progression of DPN by incorporating changes in lifestyle and necessary medical treatments. We believe that considering SII as part of the management strategy is beneficial for DPN care.
There are some potential limitations to interpreting our results that need to be addressed. First, the retrospective cross-sectional nature of this study rendered our observations susceptible to inherent bias and causality could not be established, allowing for only an interpretation of an association between SII and DPN. Therefore, prospective studies with larger sample size are still required to clarify the causality. Second, the present regression models did not contain the jobs, compliance with treatment, dietary habits, lifestyle, consumption of various medicines, such as hypoglycemic agents, antihyperlipidemic drugs, anti-hypertension drugs, antiplatelet drugs, and dietary habits and lifestyle, and we did not consider the effects of above mentioned factors on inflammation, coagulation parameters, and metabolism levels. Third, participants in our study were mainly middle-age or elderly, and were inpatients who generally had poorer metabolic control and a more serious illness than those in outpatient, which may limit the generalization of our findings to other populations. Fourth, validated but not routinely used inflammatory markers, such as C-reactive protein, tumor necrosis factor-α, interleukin-6, and circulating testosterone were not used to reflect the inflammatory status and sex hormones levels because these markers are not routinely determined for all T2DM patients in our hospital. Despite these limitations, our analyses also have some noteworthy strengths. A key finding was that our study was the first study to reveal the association of SII with DPN in Chinese patients with T2DM and its different subgroups. Second, the study followed a relatively large sample of middle-aged and elderly people, a standardized method of data collection and measurement and evaluation of various cardiovascular metabolic diseases at a single center, and was controlled for most potential confounders, which can raise the reliability of our findings.
Conclusion
SII levels were significantly higher in T2DM patients with DPN than in the subjects with non-DPN, and elevated levels of SII were independently associated with an increased risk of DPN in Chinese patients with T2DM, especially in men, people less than 65 years old, with BMI < 24 kg/m2, duration of diabetes >5 years, hypertension, dyslipidaemia, poor glycaemic control, and eGFR < 90 mL/min/1.73 m2. Moreover, SII could predict the presence of DPN. These data suggest that SII, potentially reflecting the balance of the inflammatory, immune, and thrombotic pathways, might be a novel and useful biomarker of DPN, and could further help identify T2DM patients at high-risk of developing DPN. We believe that by targeting these high-risk patients and implementing early intensive multiple metabolic and vascular risk factors control, we may help reduce their future risk of DPN and its associated adverse clinical outcomes, further providing an important guiding significance for early screening and management of DPN in Chinese patients with T2DM.
Data Sharing Statement
The dataset used and/or analyzed during the present study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
Study procedures were performed in accordance with the Declaration of Helsinki ethical principles for medical research involving human subjects. The study was approved by the Ethics Committee of the Affiliated Hospital of Southwest Medical University in China, and informed consent was obtained from all patients before data collection.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study is supported by the grants from the key Research and Development Program of Science and Technology Department of Sichuan Province (2022YFS0612).
Disclosure
Jia Li, Xing Zhang and Yi Zhang are co-first authors for this study. All authors declare no conflicts of interest in this work.
References
1. Selvarajah D, Kar D, Khunti K, et al. Diabetic peripheral neuropathy: advances in diagnosis and strategies for screening and early intervention. Lancet Diabetes Endocrinol. 2019;7(12):938–948. doi:10.1016/S2213-8587(19)30081-6
2. Elafros MA, Andersen H, Bennett DL, et al. Towards prevention of diabetic peripheral neuropathy: clinical presentation, pathogenesis, and new treatments. Lancet Neurol. 2022;21(10):922–936. doi:10.1016/S1474-4422(22)00188-0
3. Pek SLT, Sum CF, Yeoh LY, et al. Association of apolipoprotein-CIII (apoC-III), endothelium-dependent vasodilation and peripheral neuropathy in a multi-ethnic population with type 2 diabetes. Metabolism. 2017;72:75–82. doi:10.1016/j.metabol.2017.03.016
4. Argoff CE, Cole BE, Fishbain DA, Irving GA. Diabetic peripheral neuropathic pain: clinical and quality-of-life issues. Mayo Clin Proc. 2006;81(4 Suppl):S3–S11. doi:10.1016/s0025-6196(11)61474-2
5. Sloan G, Selvarajah D, Tesfaye S. Pathogenesis, diagnosis and clinical management of diabetic sensorimotor peripheral neuropathy. Nat Rev Endocrinol. 2021;17(7):400–420. doi:10.1038/s41574-021-00496-z
6. Yang K, Wang Y, Li YW, et al. Progress in the treatment of diabetic peripheral neuropathy. Biomed Pharmacother. 2022;148:112717. doi:10.1016/j.biopha.2022.112717
7. Liu S, Zheng H, Zhu X, et al. Neutrophil-to-lymphocyte ratio is associated with diabetic peripheral neuropathy in type 2 diabetes patients. Diabetes Res Clin Pract. 2017;130:90–97. doi:10.1016/j.diabres.2017.05.008
8. Allwright M, Karrasch JF, O’Brien JA, Guennewig B, Austin PJ. Machine learning analysis of the UK Biobank reveals prognostic and diagnostic immune biomarkers for polyneuropathy and neuropathic pain in diabetes. Diabetes Res Clin Pract. 2023;201:110725. doi:10.1016/j.diabres.2023.110725
9. Chen M, Zhu Y, Wang J, Wang G, Wu Y. The predictive value of neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio levels of diabetic peripheral neuropathy. J Pain Res. 2021;14:2049–2058. doi:10.2147/JPR.S304595
10. Xie R, Xiao M, Li L, et al. Association between SII and hepatic steatosis and liver fibrosis: a population-based study. Front Immunol. 2022;13:925690. doi:10.3389/fimmu.2022.925690
11. Zhu Q, Wu Y, Mai J, et al. Comprehensive metabolic profiling of inflammation indicated key roles of glycerophospholipid and arginine metabolism in coronary artery disease. Front Immunol. 2022;13:829425. doi:10.3389/fimmu.2022.829425
12. Yaşar E, Bayramoğlu A. Systemic immune-inflammation index as a predictor of microvascular dysfunction in patients with cardiac syndrome X. Angiology. 2022;73(7):615–621. doi:10.1177/00033197221087777
13. Liu B, Wang J, Li YY, Li KP, Zhang Q. The association between systemic immune-inflammation index and rheumatoid arthritis: evidence from NHANES 1999–2018. Arthritis Res Ther. 2023;25(1):34. doi:10.1186/s13075-023-03018-6
14. Ren B, Chen X, Lei P, et al. The relationship between preoperative systemic immune inflammation index and prognostic nutritional index and the prognosis of patients with alveolar hydatid disease. Front Immunol. 2021;12:691364. doi:10.3389/fimmu.2021.691364
15. Cao Y, Li P, Zhang Y, et al. Association of systemic immune inflammatory index with all-cause and cause-specific mortality in hypertensive individuals: results from NHANES. Front Immunol. 2023;14:1087345. doi:10.3389/fimmu.2023.1087345
16. Wei C, Zhang W, Chen J, et al. Systematic analysis between inflammation-related index and sex hormones in American adults: cross-sectional research based NHANES 2013–2016. Front Immunol. 2023;14:1175764. doi:10.3389/fimmu.2023.1175764
17. Özata Gündoğdu K, Doğan E, Çelik E, Alagöz G. Serum inflammatory marker levels in serous macular detachment secondary to diabetic macular edema. Eur J Ophthalmol. 2022;32(6):3637–3643. doi:10.1177/11206721221083465
18. Guo W, Song Y, Sun Y, et al. Systemic immune-inflammation index is associated with diabetic kidney disease in Type 2 diabetes mellitus patients: evidence from NHANES 2011–2018. Front Endocrinol (Lausanne). 2022;13:1071465. doi:10.3389/fendo.2022.1071465
19. Ozer Balin S, Ozcan EC, Uğur K. A new inflammatory marker of clinical and diagnostic importance in diabetic foot infection: systemic immune-inflammation index. Int J Low Extrem Wounds. 2022;15347346221130817. doi:10.1177/15347346221130817
20. Qin Z, Li H, Wang L, et al. Systemic immune-inflammation index is associated with increased urinary albumin excretion: a population-based study. Front Immunol. 2022;13:863640. doi:10.3389/fimmu.2022.863640
21. Taslamacioglu Duman T, Ozkul FN, Balci B. Could systemic inflammatory index predict diabetic kidney injury in type 2 diabetes mellitus?. Diagnostics. 2023;13(12):2063. doi:10.3390/diagnostics13122063
22. Kocak MZ, Aktas G, Erkus E, et al. Neuregulin-4 is associated with plasma glucose and increased risk of type 2 diabetes mellitus. Swiss Med Wkly. 2019;149:w20139. doi:10.4414/smw.2019.20139
23. Aktas G, Yilmaz S, Kantarci DB, et al. Is serum uric acid-to-HDL cholesterol ratio elevation associated with diabetic kidney injury?. Postgrad Med. 2023;135(5):519–523. doi:10.1080/00325481.2023.2214058
24. Aktas G. Serum C-reactive protein to albumin ratio as a reliable marker of diabetic neuropathy in Type 2 diabetes mellitus. Preprints. 2023;2023060202. doi:10.20944/preprints202306.0202.v1
25. Mostafa SA, Davies MJ, Webb D, et al. The potential impact of using glycated haemoglobin as the preferred diagnostic tool for detecting Type 2 diabetes mellitus. Diabet Med. 2010;27(7):762–769. doi:10.1111/j.1464-5491.2010.03015.x
26. Yan P, Wu Y, Dan X, et al. Aspartate aminotransferase/alanine aminotransferase ratio was associated with type 2 diabetic peripheral neuropathy in a Chinese population: a cross-sectional study. Front Endocrinol (Lausanne). 2023;14:1064125. doi:10.3389/fendo.2023.1064125
27. Lee KO, Nam JS, Ahn CW, et al. Insulin resistance is independently associated with peripheral and autonomic neuropathy in Korean type 2 diabetic patients. Acta Diabetol. 2012;49(2):97–103. doi:10.1007/s00592-010-0176-6
28. Levey AS, Stevens LA, Schmid CH, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150(9):604–612. doi:10.7326/0003-4819-150-9-200905050-00006
29. Yan P, Zhang Z, Wan Q, et al. Association of serum uric acid with bone mineral density and clinical fractures in Chinese type 2 diabetes mellitus patients: a cross-sectional study. Clin Chim Acta. 2018;486:76–85. doi:10.1016/j.cca.2018.07.033
30. Ponirakis G, Elhadd T, Chinnaiyan S, et al. Prevalence and management of diabetic neuropathy in secondary care in Qatar. Diabetes Metab Res Rev. 2020;36(4):e3286. doi:10.1002/dmrr.3286
31. Liu M, Gao Y, Chen DW, et al. Quantitative vibration perception threshold in assessing diabetic polyneuropathy: should the cut-off value be adjusted for Chinese individuals with type 2 diabetes?. J Diabetes Investig. 2021;12(9):1663–1670. doi:10.1111/jdi.13515
32. Jiang TN, Li YF, Huo LL, et al. Association between serum uric acid and large-nerve fiber dysfunction in type 2 diabetes: a cross-sectional study. Chin Med J (Engl). 2019;132(9):1015–1022. doi:10.1097/CM9.0000000000000223
33. Li X, Xu J, Yao H, Guo Y, Chen M, Lu W. Obesity and overweight prevalence and its association with undiagnosed hypertension in Shanghai population, China: a cross-sectional population-based survey. Front Med. 2012;6(3):322–328. doi:10.1007/s11684-012-0204-8
34. Wu Y, Wan Q, Xu Y, et al. Lower visceral fat area in patients with Type 2 diabetic peripheral neuropathy. Diabetes Metab Syndr Obes. 2022;15:3639–3654. doi:10.2147/DMSO.S388330
35. Xu E, Xie Y, Al-Aly Z. Risks and burdens of incident dyslipidaemia in long COVID: a cohort study. Lancet Diabetes Endocrinol. 2023;11(2):120–128. doi:10.1016/S2213-8587(22)00355-2
36. Kim SH, Baek CO, Lee KA, Park TS, Baek HS, Jin HY. Clinical implication of elevated CA 19-9 level and the relationship with glucose control state in patients with type 2 diabetes. Endocrine. 2014;46(2):249–255. doi:10.1007/s12020-013-0058-0
37. Reid A, Stöhr W, Walker AS, et al. Severe renal dysfunction and risk factors associated with renal impairment in HIV-infected adults in Africa initiating antiretroviral therapy. Clin Infect Dis. 2008;46(8):1271–1281. doi:10.1086/533468
38. National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am J Kidney Dis. 2002;39(2 Suppl 1):S1–S266.
39. Looker HC, Krakoff J, Funahashi T, et al. Adiponectin concentrations are influenced by renal function and diabetes duration in Pima Indians with type 2 diabetes. J Clin Endocrinol Metab. 2004;89(8):4010–4017. doi:10.1210/jc.2003-031916
40. Alonso A, Lopez FL, Matsushita K, et al. Chronic kidney disease is associated with the incidence of atrial fibrillation: the Atherosclerosis Risk in Communities (ARIC) study. Circulation. 2011;123(25):2946–2953. doi:10.1161/CIRCULATIONAHA.111.020982
41. Xu JP, Zeng RX, Zhang YZ, et al. Systemic inflammation markers and the prevalence of hypertension: a NHANES cross-sectional study. Hypertens Res. 2023;46(4):1009–1019. doi:10.1038/s41440-023-01195-0
42. Xia Y, Xia C, Wu L, Li Z, Li H, Zhang J. Systemic Immune Inflammation Index (SII), System Inflammation Response Index (SIRI) and risk of all-cause mortality and cardiovascular mortality: a 20-year follow-up cohort study of 42,875 US adults. J Clin Med. 2023;12(3):1128. doi:10.3390/jcm12031128
43. Xu M, Chen R, Liu L, et al. Systemic immune-inflammation index and incident cardiovascular diseases among middle-aged and elderly Chinese adults: the Dongfeng-Tongji cohort study. Atherosclerosis. 2021;323:20–29. doi:10.1016/j.atherosclerosis.2021.02.012
44. Yildiz C, Yuksel Y, Rakici IT, Katkat F, Ayça B, Turhan Çağlar FN. Assessment of systemic immune-inflammation index and systemic inflammation-response index in different coronary artery plaque types. Angiology. 2023;74(6):536–544. doi:10.1177/00033197231158937
45. Lin H, Bai Z, Wu Q, et al. Inflammatory indexes for assessing the severity and disease progression of ulcerative colitis: a single-center retrospective study. Front Public Health. 2022;10:851295. doi:10.3389/fpubh.2022.851295
46. Yi HJ, Sung JH, Lee DH. Systemic inflammation response index and systemic immune-inflammation Index are associated with clinical outcomes in patients treated with mechanical thrombectomy for large artery occlusion. World Neurosurg. 2021;153:e282–e289. doi:10.1016/j.wneu.2021.06.113
47. Chen J, Huang W, Xu X, et al. Prognostic implications of systemic immune-inflammation index in patients with bone metastases from hepatocellular carcinoma treated with radiotherapy. Front Oncol. 2023;13:1076428. doi:10.3389/fonc.2023.1076428
48. Xu T, Weng Z, Pei C, et al. The relationship between neutrophil-to-lymphocyte ratio and diabetic peripheral neuropathy in Type 2 diabetes mellitus. Medicine (Baltimore). 2017;96(45):e8289. doi:10.1097/MD.0000000000008289
49. Onalan E, Gozel N, Donder E. Can hematological parameters in type 2 diabetes predict microvascular complication development?. Pak J Med Sci. 2019;35(6):1511–1515. doi:10.12669/pjms.35.6.1150
50. D’Onofrio L, Ferdousi M, Kalteniece A, et al. Corneal confocal microscopy identifies small nerve fibre damage in patients with hypertriglyceridemia. J Clin Lipidol. 2022;16(4):463–471. doi:10.1016/j.jacl.2022.04.006
51. Geng T, Zhu K, Lu Q, et al. Healthy lifestyle behaviors, mediating biomarkers, and risk of microvascular complications among individuals with type 2 diabetes: a cohort study. PLoS Med. 2023;20(1):e1004135. doi:10.1371/journal.pmed.1004135
52. Kamenov ZA, Parapunova RA, Georgieva RT. Earlier development of diabetic neuropathy in men than in women with type 2 diabetes mellitus. Gend Med. 2010;7(6):600–615. doi:10.1016/j.genm.2010.11.001
53. Pouwer F, Kupper N, Adriaanse MC. Does emotional stress cause type 2 diabetes mellitus? A review from the European Depression in Diabetes (EDID) Research Consortium. Discov Med. 2010;9(45):112–118.
54. Marinho FS, Moram CBM, Rodrigues PC, Leite NC, Salles GF, Cardoso CRL. Treatment adherence and its associated factors in patients with Type 2 diabetes: results from the Rio de Janeiro Type 2 diabetes cohort study. J Diabetes Res. 2018;2018:8970196. doi:10.1155/2018/8970196
55. Li Z, Lei X, Xu B, Wang S, Gao T, Lv H. Analysis of risk factors of diabetes peripheral neuropathy in type 2 diabetes mellitus and nursing intervention. Exp Ther Med. 2020;20(6):127. doi:10.3892/etm.2020.9257
56. Li Y, Liu M, Cui Y, et al. Increased risk of testosterone deficiency is associated with the systemic immune-inflammation index: a population-based cohort study. Front Endocrinol (Lausanne). 2022;13:974773. doi:10.3389/fendo.2022.974773
57. Al Hayek AA, Khader YS, Jafal S, Khawaja N, Robert AA, Ajlouni K. Prevalence of low testosterone levels in men with type 2 diabetes mellitus: a cross-sectional study. J Family Community Med. 2013;20(3):179–186. doi:10.4103/2230-8229.122006
58. Tayama K, Inukai T, Shimomura Y. Preperitoneal fat deposition estimated by ultrasonography in patients with non-insulin-dependent diabetes mellitus. Diabetes Res Clin Pract. 1999;43(1):49–58. doi:10.1016/s0168-8227(98)00118-1
59. Andersen ST, Witte DR, Andersen H, et al. Risk-Factor trajectories preceding diabetic polyneuropathy: ADDITION-Denmark. Diabetes Care. 2018;41(9):1955–1962. doi:10.2337/dc18-0392
60. Furuncuoğlu Y, Tulgar S, Dogan AN, Cakar S, Tulgar YK, Cakiroglu B. How obesity affects the neutrophil/lymphocyte and platelet/lymphocyte ratio, systemic immune-inflammatory index and platelet indices: a retrospective study. Eur Rev Med Pharmacol Sci. 2016;20(7):1300–1306.
61. Man RE, Sabanayagam C, Chiang PP, et al. Differential association of generalized and abdominal obesity with diabetic retinopathy in Asian patients with type 2 diabetes. JAMA Ophthalmol. 2016;134(3):251–257. doi:10.1001/jamaophthalmol.2015.5103
62. Cameron NE, Eaton SE, Cotter MA, Tesfaye S. Vascular factors and metabolic interactions in the pathogenesis of diabetic neuropathy. Diabetologia. 2001;44(11):1973–1988. doi:10.1007/s001250100001
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Association of HbA1c Variability with Vibrating Perception Threshold in Middle-Aged and Elderly Patients with Type 2 Diabetes Mellitus: A Retrospective Cohort Study
Ding J, Shi Q, Dong L, Su H, Du Y, Pan T, Zhong X
Diabetes, Metabolic Syndrome and Obesity 2024, 17:193-202
Published Date: 10 January 2024
Lower Free Triiodothyronine is a Risk Factor of Diabetic Peripheral Neuropathy in Patients with Type 2 Diabetes Mellitus
Chen Y, Sun L, Chen M, Zhang H, Song B, Wang H, Jiang A, Zhang L, Li S, Wang J, Wang W, Zhang H
Diabetes, Metabolic Syndrome and Obesity 2024, 17:4407-4415
Published Date: 25 November 2024
Blood Cell Count-Based Inflammatory Markers Exhibit Superior Association with Diabetic Peripheral Neuropathy Compared to Protein-Based Markers
Ko FS, Wu TH, Su GY, Lin YH, Juan CC, Hwu CM
Journal of Inflammation Research 2025, 18:10609-10617
Published Date: 7 August 2025
Causal Central Network Remodeling in Diabetic Neuropathy: An Integrated MR-fMRI Study
Li X, Gao L
Diabetes, Metabolic Syndrome and Obesity 2025, 18:2753-2765
Published Date: 9 August 2025
J-Shaped Relationship Between Visceral Fat Area and Large-Nerve Fiber Dysfunction Estimated by Vibration Perception Threshold in Type 2 Diabetes: A Cross-Sectional Study
Tang D, Gu X, Xuan Y, Liu Q, Lu L
Diabetes, Metabolic Syndrome and Obesity 2025, 18:2935-2943
Published Date: 20 August 2025