Back to Journals » Journal of Pain Research » Volume 18
Impact of Tobacco Exposure on Low Back Pain-Related Disability-Adjusted Life Years in China: Trends From 1990–2021 and Projections for the Next 15 years Using ARIMA Modeling
Authors Song S, Feng S, Lu H, Li B
Received 5 June 2025
Accepted for publication 29 September 2025
Published 8 October 2025 Volume 2025:18 Pages 5303—5320
DOI https://doi.org/10.2147/JPR.S544871
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Alaa Abd-Elsayed
Shilei Song,* Shengyi Feng,* Haiming Lu, Bo Li
Joint Surgery Department, Yueyang Hospital of Integrated Traditional Chinese and Western Medicine, Shanghai University of Traditional Chinese Medicine, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Bo Li, Email [email protected]
Background: Low back pain (LBP) is a leading cause of disability - adjusted life years (DALYs) globally. Tobacco exposure has been linked to LBP, but critical research gaps remain in quantifying its impact on LBP-related DALYs in China.
Objective: This study aims to analyze the disease burden of tobacco - related LBP among the Chinese population across all age groups from 1990 to 2021 using the latest Global Burden of Disease (GBD) 2021 data and project trends for the next 15 years.
Methods: We utilized data from the GBD 2021 study, applying joinpoint regression and age - period - cohort analysis to assess the disease burden of tobacco - related LBP among the Chinese population across all age groups. The autoregressive integrated moving average (ARIMA) model was employed to forecast future trends.
Results: From 1990 to 2021, the total DALYs attributed to tobacco - related LBP in China showed an increasing trend, while the age - standardized rate (ASR) significantly declined. Specifically, the ASR for females decreased more sharply than that for males. The joinpoint regression analysis revealed a significant overall downward trend in the disease burden. The age - period - cohort analysis indicated that age significantly impacts the ASR, which is high in middle - to - old age groups. The ARIMA model forecast predicts a continued decline in the ASR of DALYs over the next 15 years.
Conclusion: The findings highlight the positive impact of tobacco - control measures in reducing the disease burden of tobacco - related LBP in China. However, the persistent high burden among males and older age groups remains a challenge. Continued and targeted tobacco - control efforts are essential to further reduce the disease burden. The findings of this study provide critical evidence for formulating targeted tobacco control policies, supporting the enhancement of tobacco intervention measures for high-risk populations (eg, males and older adults) and the implementation of tobacco control strategies to reduce the LBP-related disease burden and improve population health outcomes.
Keywords: ARIMA models, China, disability-adjusted life years, global burden of disease, low back pain, prediction, tobacco exposure
Introduction
Low back pain (LBP) is a common musculoskeletal symptom, with presentations ranging from non - specific discomfort and stiffness to severe pain. Typically, the pain is localized between the lower edge of the ribs and the top of the buttocks, and may be accompanied by sciatica.1,2 LBP is highly prevalent globally, affecting people across all age groups and socioeconomic backgrounds in both developed and developing countries.3,4 As a leading cause of disability - adjusted life years (DALYs), it impacted 746.313 per 100,000 individuals worldwide in 2021.5 It is projected that by 2050, this number will surpass 800 million,6 with total DALYs reaching 70,156,962.5 Though LBP is not life - threatening, its significant contribution to DALYs makes it a major public health issue.7,8 LBP is frequently accompanied by functional disability, psychological distress (eg, depression and anxiety), and maladaptive pain cognitions (eg, catastrophizing and fear-avoidance beliefs), all of which further amplify disability severity.9–11 Current therapeutic modalities for LBP primarily comprise pharmacotherapy, exercise-based interventions, and surgical procedures.12–14 LBP limits patients’ mobility, work ability and quality of life, imposing a heavy economic and healthcare burden on individuals, families and nations.15,16
Tobacco, a major global public health concern, is well - known for its harmful effects on health. It’s closely linked to various chronic diseases, including cardiovascular diseases, respiratory diseases, and different cancers.17 Recently, more studies have pointed out that smoking might also negatively impact the musculoskeletal system, particularly causing LBP.18 The harmful substances in tobacco can raise the risk of LBP and worsen its symptoms. This is because these substances may reduce the nutrition supply to the intervertebral discs, promote inflammatory responses, and decrease bone density.19–22 Furthermore, smoking may potentially delay the recovery of LBP. In contrast, aerobic exercises (eg, cycling) and neuromuscular rehabilitation training (eg, Mckenzie therapy) may counteract nicotine-induced muscle atrophy and microcirculatory dysfunction. Furthermore, patient education plays a pivotal role in both the prevention and treatment of LBP.14,23
China, with the world’s largest and most rapidly growing aging population, is experiencing an increasing burden of LBP, which is highly prevalent among the elderly.24 Data from the China Health Statistics Yearbook 2023 indicate that among inpatients discharged from public hospitals in China in 2022, the number of admissions attributed to intervertebral disc diseases reached 995,714, with the average medical expenditure per admission amounting to as high as 11,923.19 yuan. Notably, LBP often serves as a common manifestation of intervertebral disc diseases. While the China Health Statistics Yearbook and other Chinese databases do not publicly release direct data on LBP, the aforementioned findings indirectly demonstrate that LBP imposes a substantial disease burden on China.25 Given that smoking is a significant risk factor for LBP and China has a high smoking rate (27.7% in males),26 the public has long overlooked the burden of LBP caused by tobacco exposure. Consequently, analyzing the long-term impact of tobacco exposure on the disease burden of LBP in China is critical. Previous studies using the 2021 GBD data have analyzed disease burden for LBP in China,15 yet the specific effects of risk factors (particularly tobacco) on the disease burden remain unclear. In the GBD 2021 database, three level 2 risk factors—namely Tobacco, Occupational risks, and High body-mass index—collectively contribute to the DALYs burden of LBP, with Tobacco accounting for a non-negligible proportion thereof (https://vizhub.healthdata.org/gbd-compare/). Furthermore, although Wang et al27 quantified the global burden of LBP attributable to smoking across 204 countries—a study that identified a substantial burden of smoking-related LBP on a global scale—a China-specific estimate was not provided. More importantly, smoking represents only one component of tobacco exposure, which also encompasses second-hand smoke and chewing tobacco. Notably, within the China-focused risk-factor analyses of the Global Burden of Disease Study 2021, only high body-mass index28,29 has been evaluated to date; the contribution of overall tobacco exposure to LBP remains unexamined. Consequently, the impact of tobacco exposure on LBP burden among the Chinese population remains entirely unquantified. This study leverages the latest GBD 2021 data and employs joinpoint regression and age-period-cohort analysis to investigate how tobacco has shaped the LBP burden in China from 1990 to 2021. The findings offer valuable insights into the evolving patterns of LBP burden over the past 32 years. The analysis and prediction of these specific trends hold significant value for policy formulation, resource allocation, and the targeted positioning of intervention measures.
Materials and Methods
Research Population and Data Compilation
The GBD 2021 study, with updated epidemiological data and enhanced standardization, quantified health loss from 371 diseases across 204 regions, using the death, DALYs and etc. metric.6 The GBD study evaluates the extent to which various risk factors contribute to disease burden by comparing observed levels to a theoretical minimum risk exposure level.30 The definition of tobacco exposure can be found in Li et al’s research.31 The GBD 2021 database classifies disease according to the International Classification of Diseases, 10th Revision (ICD-10).15 In the ICD-10, LBP is categorized under the codes M54.3 and M54.4.4 In GBD, the disease burden from tobacco - related LBP is measured by DALYs and years of life lost (YLLs). Since LBP is not fatal, the deaths and years lived with disability (YLDs) metrics do not apply, and DALYs equal YLLs here. Our analysis focuses on “China”. To facilitate comparison with other risk factors for LBP, we also extracted data on all level 2 risk factors for LBP and included them in the subsequent analysis.
Data Analysis
Overview
We initiated our data analysis by assessing the dataset structure to estimate the number and age - standardized rate (ASR) of DALYs from tobacco - induced LBP in China. Then, we analyzed measurement changes from 1990 to 2021. This analysis was conducted for the DALYs per 100,000 years and the ASR.7 To calculate the estimated annual percentage change (EAPC), we used the formula: EAPC = 100×(exp(β) - 1). The 95% confidence interval (CI) for EAPC came from a linear model.8,9 An increasing trend in age - standardized metrics was indicated when both the EAPC value and the lower bound of the 95% CI exceeded zero. A decreasing trend was observed if both the EAPC value and the upper bound of the 95% CI were below zero. A consistent trend was suggested when the 95% CI of EAPC included zero.9,10 To determine relative changes (RC), we applied the formula: RC (%) = [(value in 2021 - value in 1990)/value in 1990]×100%. This was also based on cases per 100,000 people and ASR.11
Joinpoint Regression Analysis
The joinpoint regression model comprises multiple linear statistical models employed to assess temporal fluctuations in disease burdens associated with tobacco - induced LBP. This model employs a statistical methodology that quantifies fluctuations in disease incidence via the least squares technique, circumventing the subjectivity inherent in conventional trend assessments reliant on linear trends.32 The computation of the squared sum of the residual error between the estimated and actual values determines the inflection point of the trend’s variation. The model was developed using Joinpoint (version 5.1.0.0; National Cancer Institute, Rockville, MD, USA). This software analyzes temporal data patterns and subsequently applies a fundamental model by linking multiple line segments on a logarithmic scale. The annual percentage change (APC) was computed to evaluate trends.21 The optimal number of joinpoints was identified through a synthesis of statistical benchmarks and model fit evaluations. The model selection workflow initiated with the minimum number of joinpoints (ie, zero) and gradually augmented this number; the increment process ceased when the addition of further joinpoints no longer yielded a significant improvement in model fit. Notably, the built-in algorithm of Joinpoint software was employed for this purpose, as it leverages a permutation test to assess the statistical significance of each potential joinpoint. This software computes the residual sum of squares difference between the model incorporating the additional joinpoint and the one excluding it.33
Age-Period-Cohort Analysis
In epidemiology, age - period - cohort models are commonly utilized to distinguish the impacts of age, time period, and birth cohort on disease burden.34 These models, built on Poisson distributions, enable the analysis of DALYs trends over time across various age groups, periods, and birth cohorts.35 To mitigate multicollinearity among age, period, and cohort effects, the Intrinsic Estimator (IE) method was adopted. Through the imposition of constraints on model parameters, the IE method stabilizes parameter estimates and reduces biases arising from multicollinearity, thereby allowing for an accurate representation of the true effect of each factor.36 A log-linear regression model (expressed as log(Yi) = μ + α*agei + β*periodi + γ*cohorti + ε) was utilized, where Yi denotes the disease burden metrics of interest. In our study, following the GBD classification, individuals were grouped into different age brackets at five-year intervals.37 We analyzed data from 1990 to 2021 in five - year cycles, calculating total DALYs for each age group. APC model fitting was done via R version 4.3.3.
Predictive Analysis
To forecast future trends in the DALYs burden of tobacco - induced LBP, we employed the autoregressive integrated moving average (ARIMA) model. This model was chosen for predictive purposes based on its proficiency in characterizing long-term trends of non-stationary time series. It addresses non-stationarity through differencing (d) and captures linear interdependencies via autoregressive (p) and moving average (q) terms. Parameterization adhered to a data-driven framework: subsequent to verifying stationarity using the Augmented Dickey-Fuller (ADF) test, the auto.arima algorithm fine-tuned the (p, d, q) parameters with the Akaike Information Criterion (AIC) and Bayesian Information Criterion (BIC), thereby avoiding subjective bias.38,39 This model leverages the autocorrelation of time-series data to predict future values based on historical observations. The core principle of ARIMA is that data series are time-dependent random variables, characterized by their autocorrelation structure. For the model to be effective, the time series must be stationary and stochastic, with a mean of zero.38,39 To ensure the reliability of the prediction results, we also employed the Bayesian Age-Period-Cohort (BAPC) model as a supplementary approach for prediction.40 R version 4.3.3 and JD_GBDR (V2.22, Jingding Medical Technology Co., Ltd.) was used for the drawing of the figures in the predictive analysis.
Results
Overview of the Global Burden
Results of the Trend Analysis for DALYs Burden of Tobacco - Induced LBP in China
In the GBD 2021 database, the level 2 risk factors associated with LBP comprise three distinct categories: Occupational risks, Tobacco, and High body-mass index. The burden that these three factors contribute to LBP-related DALYs is illustrated in Figure 1. Notably, tobacco exposure imposes a non-negligible burden on LBP-related DALYs.
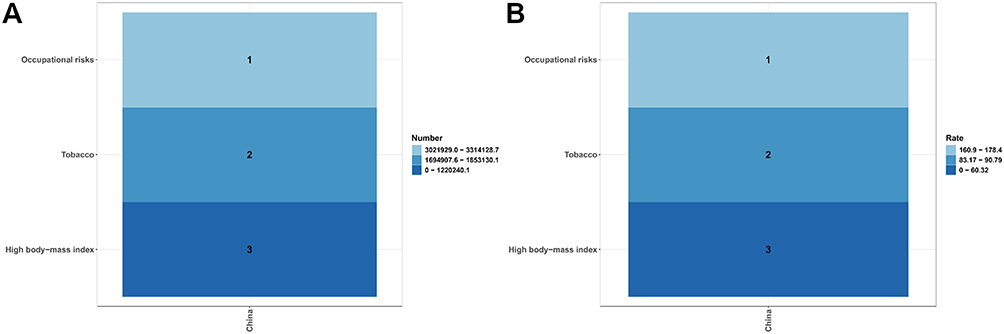 |
Figure 1 Heatmap of Contributions of Different Level 2 Risk Factors to LBP-Related DALYs in China. (A) Absolute numbers of DALYs; (B) ASR of DALYs. |
In 1990, the total DALYs attributed to LBP caused by tobacco exposure in China was 1,296,252.183 (95% UI: 792,675.648–1,906,635.951), with an ASR of 130.990 (95% UI: 79.755–191.821). Specifically, males accounted for 1,071,076.120 (95% UI: 662,748.772–1,560,749.618) in total DALYs, corresponding to an ASR of 209.046 (95% UI: 129.466–301.633); females had a total of 225,176.064 (95% UI: 123,887.756–361,890.708) DALYs, with an ASR of 49.505 (95% UI: 27.310–79.032).
By 2021, compared with 1990, the total DALYs for LBP due to tobacco exposure in China had increased to 1,853,130.073 (95% UI: 1,084,580.575–2,703,582.504), representing a 42.96% rise, while the ASR decreased by 30.69% to 90.789 (95% UI: 53.256–131.008). Among males, total DALYs rose by 45.52% to 1,558,580.115 (95% UI: 931,831.256–2,265,680.096), with a 26.11% decline in ASR to 154.468 (95% UI: 92.951–224.169); among females, total DALYs increased by 30.81% to 294,549.958 (95% UI: 158,883.597–472,835.863), accompanied by a 45.43% drop in ASR to 27.017 (95% UI: 14.458–43.125).
Findings from the EAPC revealed a downward trend in the overall ASR from 1990 to 2021 (−1.02 [95% CI: −1.12, −0.93]), with females showing a more pronounced decline (−1.75 [95% CI: −1.87, −1.63]) compared to males (−0.81 [95% CI: −0.90, −0.72]) (Table 1, Figure 2).
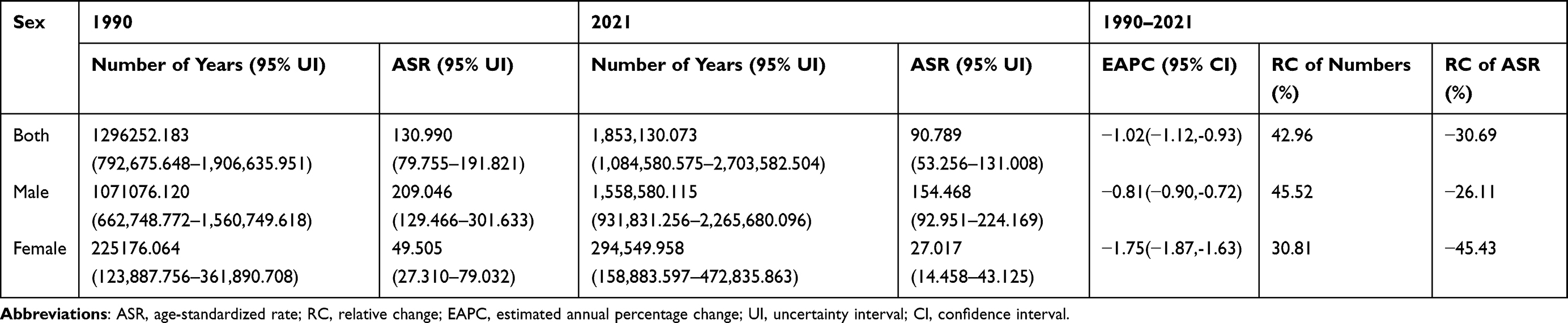 |
Table 1 DALYs Burden of Tobacco-Induced Low Back Pain in China by Sex, 1990–2021 |
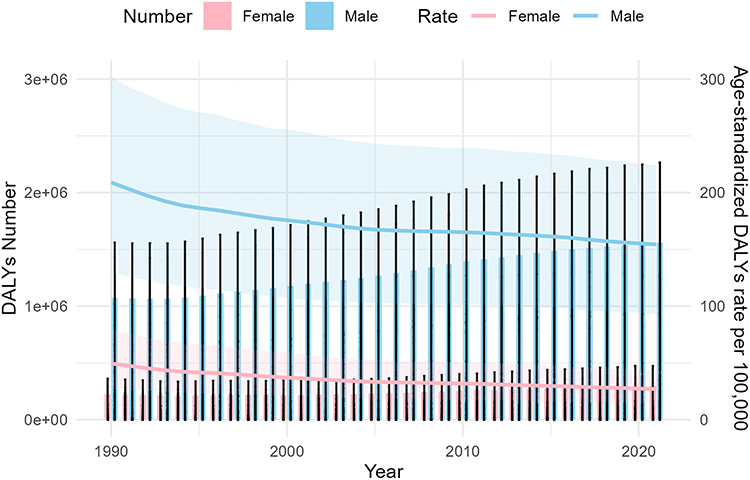 |
Figure 2 Age-standardized DALYs (per 100000) and number of DALYs of females and males in China from 1990 to 2021. |
Results of the Trends by Year, Sex and Age for DALYs Burden of Tobacco - Induced LBP in China
Figure 3 shows the disease burden of DALYs caused by tobacco - induced LBP across different age and sex groups in China in 2021. It can be seen that from the age of 30–34, tobacco - related LBP begins to impact the Chinese population, with the disease burden increasing with age, peaking at 50–54 years old, then declining but still affecting those aged 95 and above. ASR also shows similar trends. It should be noted that in terms of both total number and ASR, males are significantly higher than females.
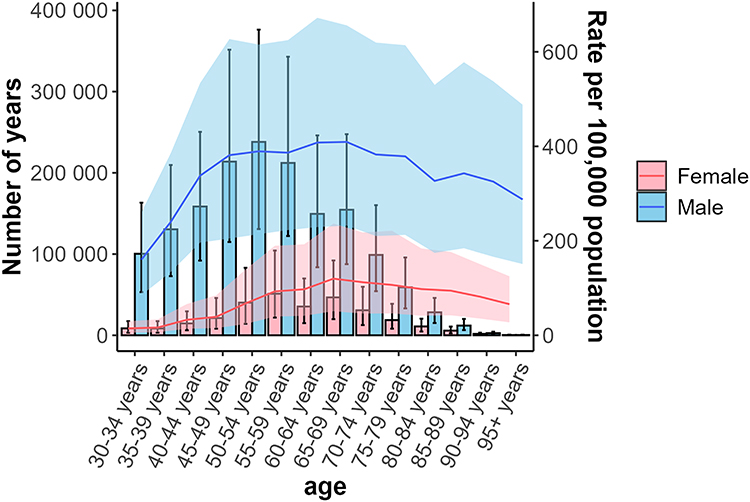 |
Figure 3 Trends in DALYs number and age-standardized rate of tobacco-induced low back pain by gender and age group in China, 2021. |
Table 2 presents a detailed analysis of the DALYs burden caused by tobacco - induced LBP in China for the years 1990 and 2021. In 1990, the highest DALYs burden was observed in the 35–39 years age group, while the lowest was in those aged 95+. The highest ASR was in the 65–69 years age group, and the lowest in the 30–34 years group. By 2021, the highest DALYs burden shifted to the 50–54 years age group, with the lowest remaining in the 95+ years group. The highest ASR in 2021 was in the 30–34 years age group. In terms of relative changes, the 95+ years group showed the most significant increase in total DALYs (884.77%), while the 35–39 years group experienced the most noticeable decrease (−22.75%). For ASR, all age groups saw a decline, with the 45–49 years group having the smallest decrease (−23.65%) and the 70–74 years group the largest (−38.75%). The EAPC results indicated that between 1990 and 2021, the DALYs burden grew the most in the 95+ years age group, while the 30–34 years age group saw a reduction in DALYs.
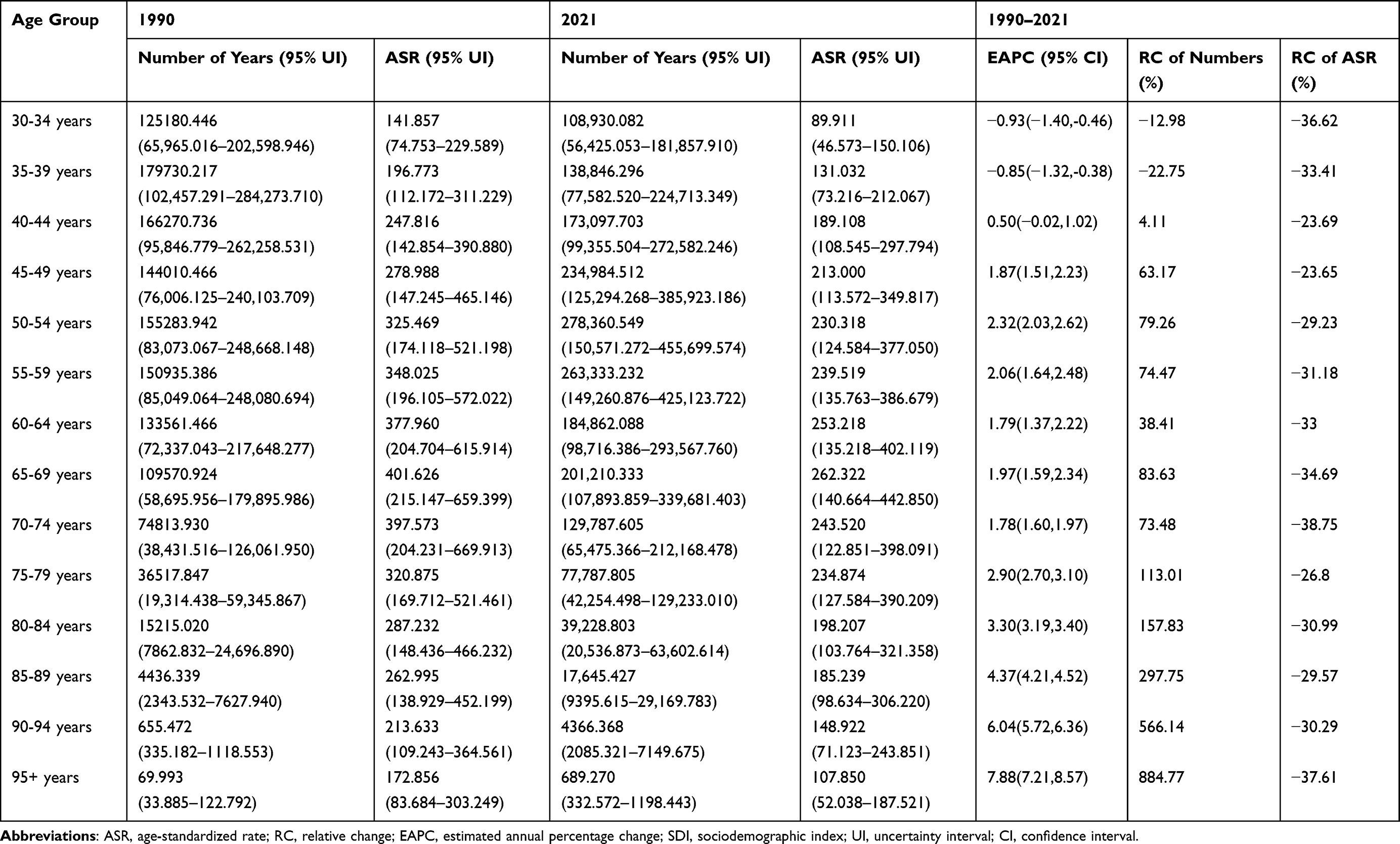 |
Table 2 DALYs Burden of Tobacco-Induced Low Back Pain in China by Different Age Groups, 1990–2021 |
Results of the Joinpoint Analysis
Joinpoint analysis revealed an overall AAPC of −1.18 (−1.21 to −1.15) from 1990 to 2021, indicating a statistically significant downward trend in the burden of tobacco - induced LBP. This trend was segmented into five distinct phases: 1990–1993 (APC: −3.05 [95% CI: −3.23 to −2.87]), 1993–1999 (APC: −1.51 [95% CI: −1.59 to −1.43]), 1999–2005 (APC: −1.27 [95% CI: −1.36 to −1.19]), 2005–2012 (APC: −0.44 [95% CI: −0.50 to −0.38]), and 2012–2021 (APC: −0.84 [95% CI: −0.87 to −0.81]), with all periods demonstrating significant trends (P < 0.05). The temporal patterns for males and females were broadly consistent with the overall trend (Table 3, Figure 4).
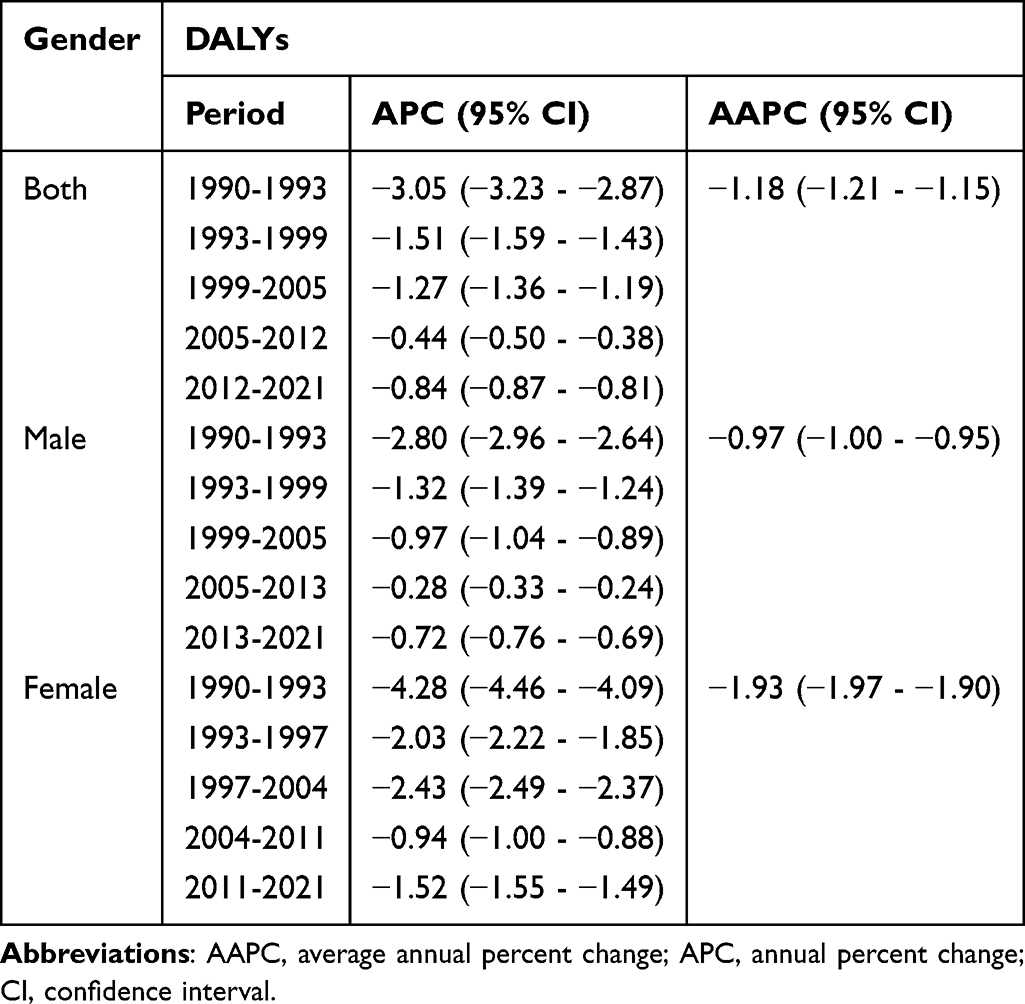 |
Table 3 Joinpoint Regression Analysis: Trends in Age-Standardized DALYs Rates (per 100,000 Years) Among Both Sexes, Males, and Females in China, 1990–2021 |
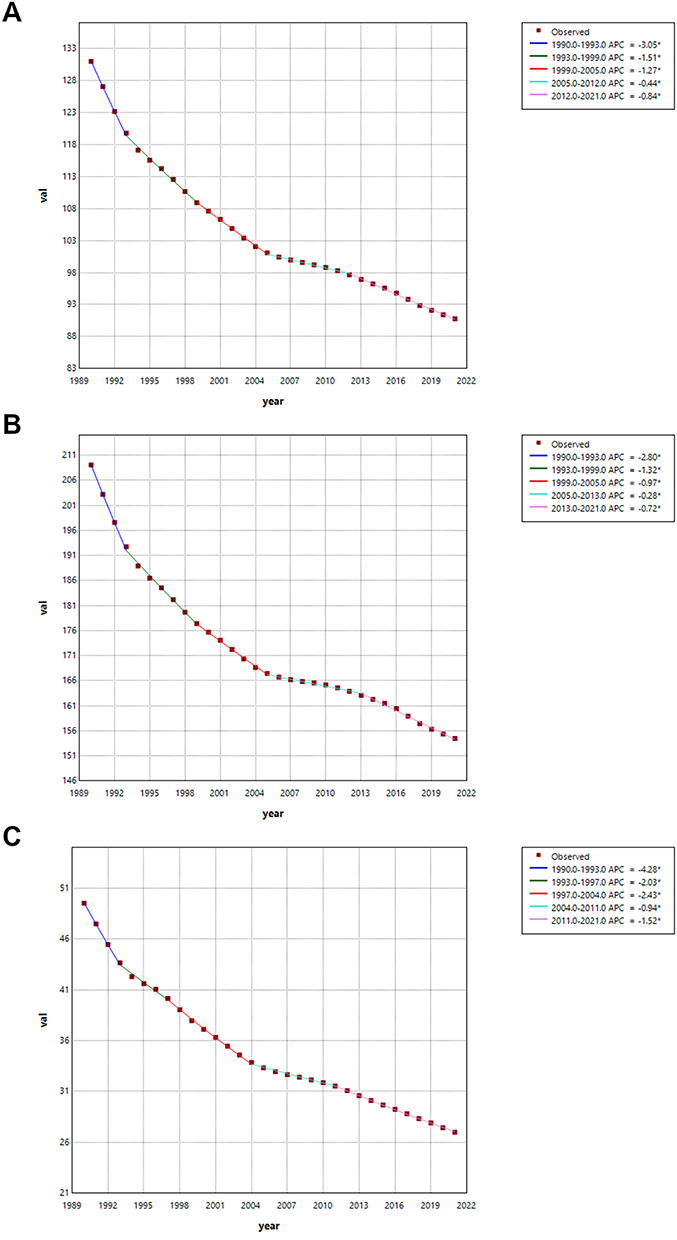 |
Figure 4 Joinpoint regression analysis of sex-specific age-standardized DALYs rates for tobacco-induced low back pain in China: a study spanning 1990 to 2021 (A) both sexes, (B) males, (C) females. |
Results of the Age-Period-Cohort Analysis
Figure 4 presents the age-period-cohort analysis of the age - standardized DALYs rate (ASDR) for tobacco - induced LBP in China. Age significantly impacts the ASDR, which is high in middle - to - old age (around 40–75 years). Both the longitudinal (Figure 5A) and cross - sectional (Figure 5B) analyses confirm this. Age deviations (Figure 5C) reveal that the actual risk in this age range is higher than expected. The long - term and cross - sectional rate ratio (Figure 5D) shows a downward trend, indicating that the age - related increase in DALYs has become less pronounced in recent periods.
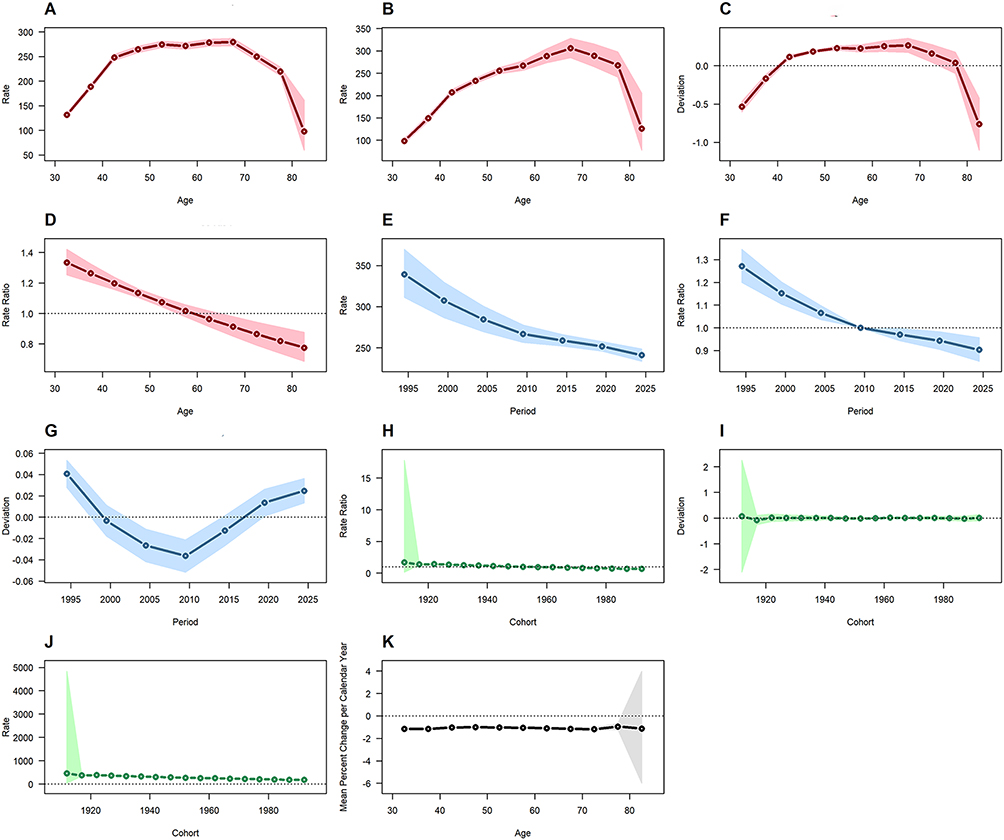 |
Figure 5 Results of Age - Period - Cohort Analysis: Trends and Deviations in Rates across Age, Period, and Cohort Dimensions. (A) Longitudinal Age Curve, (B) Cross - Sectional Age Curve, (C) Age Deviations, (D) Long vs Cross RR, (E) Fitted Temporal Trends, (F) Period RR, (G) Period Deviations, (H) Cohort RR, (I) Cohort Deviations, (J) Fitted Cohort Pattern, (K) Local Drifts. |
Over the entire period, the ASDR has decreased (Figure 5E). The period rate ratio (Figure 5F) indicates a lower - than - before risk in later periods. However, period deviations (Figure 5G) show that recent ASDR is higher than expected.
Different birth cohorts show slight, nonsignificant differences in ASDRs from tobacco - related LBP. Newer cohorts have somewhat lower rates than older ones (Figure 5H). Cohort deviations (Figure 5I) reveal minimal variation around expected values, with minor fluctuations in early cohorts (around 1920). The fitted cohort pattern (Figure 5J) also shows higher ASDRs in older cohorts and lower ones in newer cohorts.
Finally, the local drifts (Figure 5K) remain below zero throughout the study period, indicating a downward trend in ASDRs.
Results of the Predictive Analysis
Our forecast projects the future 15 - year disease burden of tobacco - induced LBP in terms of DALYs. As shown in Table 4, the model validation results of the ARIMA model indicate that the predictive models for females and the overall population are superior to that for males, yet all of them exhibit a high level of credibility. Looking ahead to the next 15 years, the ASR of DALYs is anticipated to continue its decline, regardless of gender or for the overall population (Figure 6). The temporal trends of the prediction results from the BAPC model and the ARIMA model are almost identical, which reinforces the reliability of the ARIMA model’s prediction results (Figure 7).
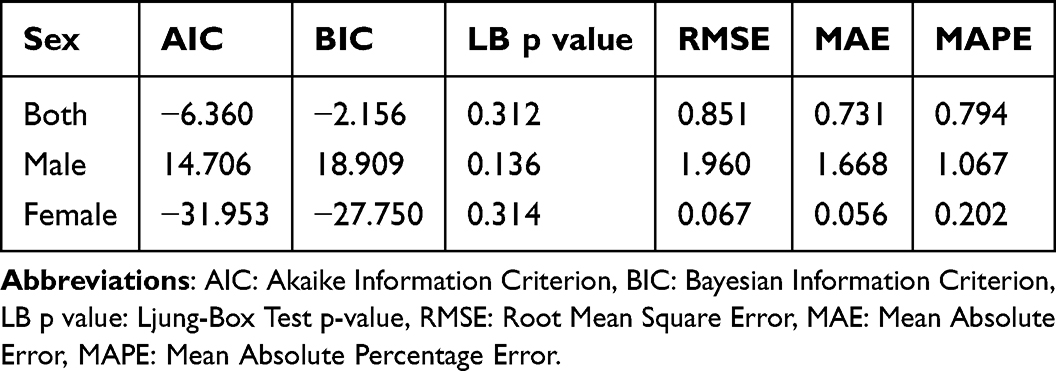 |
Table 4 Validation of ARIMA’s Suitability for Long-Term Predictions |
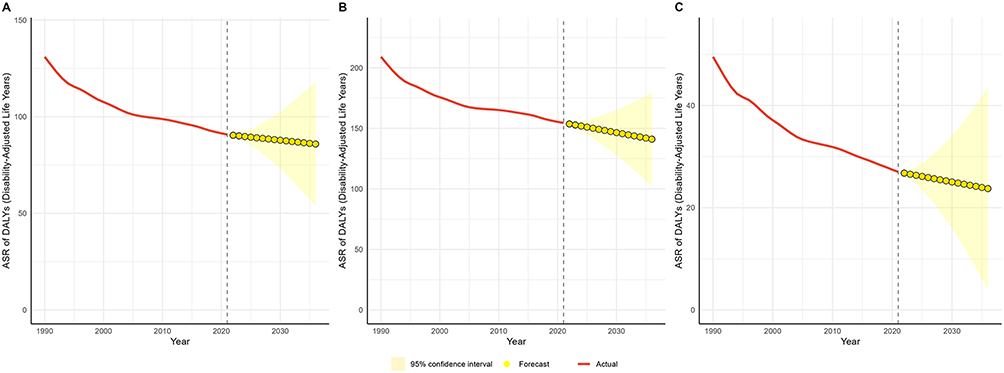 |
Figure 6 Predicted trends of tobacco-induced low back pain over the next 15 years (2022–2036) using the ARIMA model (A) ASR of DALYs of both sex; (B) ASR of DALYs of male; (C) ASR of DALYs of female). Red lines represent the true trend during 1990–2021; yellow dot lines and shaded regions represent the predicted trend and its 95% CI. |
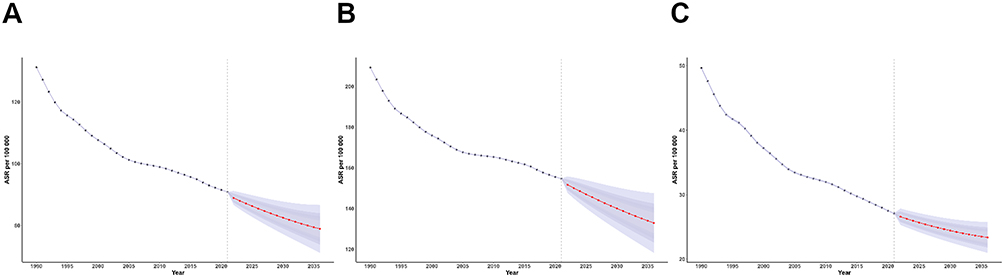 |
Figure 7 Predicted trends of tobacco-induced low back pain over the next 15 years (2022–2036) using the BAPC model (A) ASR of DALYs of both sex; (B) ASR of DALYs of male; (C) ASR of DALYs of female). Grey blue lines represent the true trend during 1990–2021; red lines and shaded regions represent the predicted trend and its 95% CI. |
Discussion
Discussion on Chinese Trend Analysis Results
Our analysis reveals a rising trend in the total DALYs attributed to tobacco - induced LBP in China from 1990 to 2021, yet the ASR exhibits a significant decline. This pattern reflects the positive impact of China’s tobacco - control efforts in curbing the risk and burden of LBP.
When examining gender - specific differences, the pronounced decline in ASR among females indicates that tobacco - control measures and health promotion strategies have been more effective in this group. In contrast, the substantial increase in total DALYs among males may stem from their historically higher smoking rates,26 which contribute to a persistent rise in LBP incidence due to the long - term cumulative effects of smoking. Another potential explanation for such disparities lies in findings from a national survey in China, which reported a smoking prevalence of 27.7% among males, whereas the corresponding rate among females was only 2.0%.26 Furthermore, females demonstrated significantly higher willingness to quit smoking and higher success rates in smoking cessation compared to males.41
The EAPC analysis further confirms the downward trend in overall ASR, with distinct gender differences. This suggests that tobacco - control policies and preventive strategies for LBP should be tailored to different genders. Additionally, it is essential to explore other potential factors underlying the changes in disease burden, such as improved healthcare and enhanced health awareness, to provide a comprehensive basis for further reducing the burden of tobacco - related LBP.
Synthesis of Gender and Age Trends
The analysis of DALYs burden trends by year, sex, and age for tobacco - induced LBP in China reveals several important patterns.
The increasing disease burden with age, peaking at 50–54 years old, and the higher burden in males than females may be due to the accumulation of smoking - related health damage over time, and the higher smoking rates among males. The shift in the highest DALYs burden from the 35–39 years age group in 1990 to the 50–54 years age group in 2021 could reflect changes in smoking patterns and the delayed impact of smoking on health.42 Meanwhile, the significant increase in total DALYs in the 95+ years group might be associated with the aging population and increased survival of individuals with smoking - related health problems. Studies have demonstrated that the proportion of the elderly population in China has exhibited the fastest growth rate, giving rise to a unique phenomenon of “second-stage aging.”43 When combined with the relatively high prevalence of LBP in this elderly group—whose LBP burden is partially attributable to decades of tobacco exposure—such an excessive disease burden becomes the fundamental driver of the increase in LBP-related DALYs. The overall decline in ASR across all age groups indicates the positive effect of tobacco - control measures and improved healthcare, especially since China signed the WHO Framework Convention on Tobacco Control in November 2003 and it came into effect in January 2006,44,45 but the differences in changes among age groups suggest that the effectiveness of these measures may vary across different generations.
The EAPC results further highlight the complex dynamics of the DALYs burden over time. The growth in the 95+ years group and the reduction in the 30–34 years group may imply that younger generations are less affected by tobacco - induced LBP, possibly due to more effective prevention and control efforts targeting younger populations in recent years. However, the growing high burden in older age groups remains a challenge.
In summary, these findings emphasize the importance of continued and targeted tobacco - control efforts across different age groups and genders to further reduce the disease burden of tobacco - induced LBP in China.
Interpreting the Positive Impact of Tobacco - Control Measures Through Joinpoint Regression Analysis
The Joinpoint regression analysis of the disease burden of tobacco - related LBP in China from 1990 to 2021 reveals a significant overall downward trend, as evidenced by the AAPC of −1.18. This finding is highly consistent with the positive outcomes of tobacco - control initiatives and healthcare improvements implemented over the years, especially since the WHO FCTC came into force in China in January 2006, China has achieved remarkable results in tobacco control in the following aspects: Monitor Tobacco Use and Prevention Policies, Protect People from Tobacco Smoke, Offer Help to Quit Tobacco Use, Warn about the Dangers of Tobacco, Anti - tobacco Mass Media Campaigns, Health Warning Labels, Enforce Bans on Tobacco Advertising, Promotion and Sponsorship, and Raise Taxes on Tobacco.44 The downward trend in disease burden indicates that these measures have had a tangible impact on reducing the health risks associated with tobacco exposure.
When examining the different phases identified by the Joinpoint analysis, it is evident that the rate of decline has fluctuated over time. The most substantial reduction in disease burden occurred during the earlier periods (1990–1993 and 1993–1999), with APCs of −3.05 and −1.51, respectively. This suggests that the initial tobacco - control measures may have had a more pronounced effect during these years.46 However, the APC gradually slowed down in the following periods (1999–2005, 2005–2012, and 2012–2021), indicating that while the disease burden continued to decrease, the pace of reduction has become less pronounced over time. This could be due to a variety of factors, such as the increasing complexity of tobacco - induced health issues, the emergence of new risk factors, or potential limitations in the reach and effectiveness of current tobacco - control strategies.46 One of the more prominent contributing factors is electronic cigarettes, which have rapidly emerged as a globally prevalent tobacco alternative since their invention in China in 2003. As the world’s largest producer of e-cigarettes, China’s e-cigarette market has expanded rapidly against a backdrop of inadequate strict regulation, particularly exhibiting a marked increase in appeal among adolescents and young adults.47,48 Reported data indicate that in 2021, the experimental use rate of e-cigarettes among middle school students reached 13.07%, while the current use rate stood at 3.74%.49
It is also worth noting that the temporal patterns for males and females were broadly consistent with the overall trend. This implies that both genders have benefited from the tobacco - control measures and healthcare improvements, although the specific impact and effectiveness may still vary between males and females. For example, males may have experienced a more significant reduction in disease burden due to their historically higher smoking rates and the subsequent greater potential for improvement. On the other hand, females may have benefited from targeted interventions and prevention programs aimed at reducing tobacco exposure and exposure in this population.
In summary, the Joinpoint analysis provides valuable insights into the long - term trends and patterns of the disease burden of tobacco - related LBP in China. While the overall downward trend is encouraging, the varying rates of decline across different periods highlight the need for continued and refined tobacco - control efforts. Future research and policy development should focus on addressing the evolving challenges in tobacco control and identifying more effective strategies to further reduce the disease burden, particularly in light of emerging health trends.
Age-Period-Cohort Analysis of ASDR for Tobacco - Induced LBP in China: Trends and Insights
The age-period-cohort analysis of the ASDR for tobacco - induced LBP in China reveals several noteworthy trends and patterns.
Age significantly impacts the ASDR, with middle-to-old age groups (around 40–75 years) experiencing higher rates. This is likely due to the cumulative effects of smoking over time, as well as the increased vulnerability to tobacco-related health issues with advancing age. Smoking has a harmful effect on bone health, linked to osteoporosis. It can lead to reduced vertebral bone density and cause tiny bone fractures. Over time, this damages bone tissue, triggers chronic inflammation, and increases the likelihood and severity of further spinal harm.20 Both the longitudinal and cross-sectional analyses confirm the heightened ASDR in this age range, and age deviations indicate that the actual risk is higher than expected. However, the long-term and cross-sectional rate ratio shows a downward trend, suggesting that the age-related increase in DALYs has become less pronounced in recent periods. This could be attributed to improved healthcare, increased awareness of smoking risks, or more effective tobacco-control measures targeting older populations in recent years.
Over the entire period, the ASDR has decreased, which is a positive indication of the overall effectiveness of tobacco-control efforts. The period rate ratio indicates a lower-than-before risk in later periods, reflecting the positive impact of comprehensive tobacco-control strategies implemented over time. However, period deviations reveal that the recent ASDR is higher than expected. This might be due to factors such as the introduction of new tobacco products, changes in smoking patterns, or challenges in the enforcement of tobacco-control policies in recent years.50,51
When examining different birth cohorts, there are slight, nonsignificant differences in ASDRs. Newer cohorts tend to have somewhat lower rates than older ones, which may be associated with generational shifts in smoking behavior, greater awareness of health risks, or the influence of tobacco-control policies over time. For instance, China has been strengthening its regulation on smoking among minors.44 Cohort deviations show minimal variation around expected values, with minor fluctuations in early cohorts (around 1920). The fitted cohort pattern also indicates higher ASDRs in older cohorts and lower ones in newer cohorts, further supporting the idea that younger generations are less affected by tobacco-related LBP. Furthermore, demographic changes constitute another factor affecting tobacco exposure. For instance, after becoming fathers, males in China tend to reduce smoking or quit altogether due to concerns about their children’s health.52 Additionally, demographic disparities between urban and rural areas may contribute to differences in smoking patterns: the smoking prevalence among residents in rural areas is 40% higher than that in urban areas.53,54 Furthermore, the middle-aged and elderly populations also exhibit relatively high smoking prevalence.55
Finally, the local drifts show a downward trend in ASDRs, which reinforces the notion that tobacco-control measures and public health initiatives have been effective in reducing the disease burden of tobacco-induced LBP in China.
In summary, the age-period-cohort analysis provides valuable insights into the complex interplay of age, period, and cohort effects on the ASDR of tobacco-induced LPB. While age remains a significant factor, the overall decreasing trend in ASDR and the lower rates in newer cohorts are encouraging signs of the positive impact of tobacco-control efforts. However, the recent higher-than-expected ASDR highlights the need for continued vigilance and the refinement of tobacco-control strategies to address emerging challenges.44
Predictive Analysis of Tobacco-Induced LBP and Discussion on Prevention and Control Strategies
The forecasted decline in the ASR of DALYs for tobacco-related LBP over the next 15 years is a promising indicator of the potential reduction in disease burden. This positive outlook can be attributed to the ongoing efforts in tobacco control and the improvement of public health awareness and healthcare services. The superior predictive models for females and the overall population, as indicated by the ARIMA model validation, suggest that the implemented tobacco control measures may have been more effective in these groups. However, the relatively less accurate model for males highlights the need for more targeted interventions, especially considering the historically higher smoking rates among males. Despite the anticipated decline, the persistence of tobacco - induced LBP remains a public health challenge. It is crucial to continue strengthening tobacco control policies, promoting smoking cessation programs, and raising awareness about the harmful effects of smoking on musculoskeletal health. Additionally, further research should be conducted to better understand the gender-specific factors influencing the disease burden and to develop more effective strategies to address the disparities in tobacco - induced health outcomes.
Public Health Policy Recommendations Based on Research Findings
Based on the study’s findings, several public health policy recommendations are proposed. First, strengthening tobacco - control policies is crucial. This includes stricter enforcement of smoking bans in public places, higher taxes on tobacco products, and more prominent health warning labels.56 Tailored public education campaigns should be implemented to raise awareness of the link between smoking and LBP, and to highlight the long - term musculoskeletal benefits of smoking cessation. Given the higher burden of tobacco - related LBP among males and the elderly, targeted interventions for these groups are essential. Workplace and community programs designed for men, along with senior - friendly smoking cessation services, can help address these disparities.57 Additionally, it is recommended to integrate multidisciplinary resources to establish “tobacco - control and musculoskeletal health” clinics within primary care services. This integration, combined with the development of domestic prospective cohorts for improved data monitoring, can support early detection and management of LBP and inform policy adjustments. Training healthcare providers on the role of tobacco in LBP can enhance preventive care. Furthermore, given that the DALYs burden of tobacco - related LBP begins in individuals aged 30–34 years, and considering the cumulative effects of tobacco exposure from a younger age, it is imperative to strengthen tobacco - control policies targeting adolescents in China.26 Finally, continued monitoring and research into the health impacts of tobacco are necessary to inform effective policy adjustments.
Limitations
This study has several limitations. First, it relies on GBD 2021 model-derived estimates rather than direct observational data, which may introduce uncertainties, especially in regions with sparse primary data. Second, evolving diagnostic criteria for LBP across the study period (1990–2021) could affect longitudinal comparability. Third, the analysis does not account for confounding factors like physical activity or obesity, potentially limiting causal inference.
Furthermore, risk factor attribution in GBD studies relies on model algorithms and may be subject to certain uncertainties. Nevertheless, GBD studies place particular emphasis on verifying the reliability of model outcomes. All calculations are accompanied by 95% UI, with uncertainty aggregation achieved via drawing 1000 samples from the posterior distribution—while accounting for both modeling and sampling uncertainties. This comprehensive uncertainty handling approach can mitigate the impact of confounding factors to a certain extent.58 Therefore, the inherent assumptions of the model should be interpreted with caution. Additionally, the study lacks granular regional data within China, using broad GBD classifications that obscure provincial or rural-urban disparities. Predictive models assume stable historical trends, which may not hold with emerging factors like e-cigarettes or demographic shifts.59 Finally, the focus on population-level metrics excludes qualitative patient outcomes and economic costs, limiting insights into holistic health impacts.
For future studies, it is recommended to consider the dose-response curves of tobacco exposure and LBP. Point-to-point quantitative results would facilitate a more accurate assessment of the burden imposed by tobacco exposure. Therefore, it would be more scientifically sound to compare the attributable burden of tobacco exposure among different populations in various regions (especially research focusing on urban and rural areas requires further integration of relevant data within the GBD database, followed by the public release of such integrated data, to enable in-depth investigations), taking into account the spatiotemporal variations in tobacco exposure patterns (eg, smoking prevalence, types of tobacco products) and the susceptibility profiles of specific populations (eg, age, gender, genetic factors). The results of this study provide valuable epidemiological evidence to inform targeted interventions for countries worldwide, aiming to mitigate tobacco-related LBP burden and its associated DALYs.
Conclusion
This study analyzed the impact of tobacco exposure on LBP-related DALYs in China from 1990 to 2021 and projected trends for the next 15 years. The results showed an increasing trend in total DALYs, but the ASR exhibited a significant decline. This reflects the positive impact of China’s tobacco-control efforts. The ASR for females decreased more pronouncedly than that for males, indicating that tobacco-control measures and health promotion strategies have been more effective in females. However, the substantial increase in total DALYs among males may be due to their higher smoking rates and the long-term cumulative effects of smoking. Our forecast projects a continued decline in the ASR of DALYs over the next 15 years. In conclusion, this study not only provides empirical evidence for evaluating the effectiveness of tobacco control policies but also offers targeted recommendations for specific target populations (ie, the elderly and males), and emphasizes the importance of continuing and strengthening tobacco-control efforts across different age groups and genders to further reduce the disease burden of tobacco-induced LBP in China.
Data Sharing Statement
The datasets utilized in this investigation are accessible in open repositories. The repository names and accession numbers are provided below: All data may be accessed via the IHME website (https://vizhub.healthdata.org/gbd-results/).
Ethics Approval and Consent to Participate
This study is exempt from ethical review for the following reasons: According to the “Measures for the Ethical Review of Human-Involved Life Science and Medical Research” (Guo Wei Ke Jiao Fa [2023] No. 4), issued on February 18, 2023 (https://www.nhc.gov.cn/qjjys/c100016/202302/6b6e447b3edc4338856c9a652a85f44b.shtml [accessed on 10, October, 2025]), the provisions of Items (1) and (2) of Article 32 are as follows: Article 32 For human-involved life science and medical research conducted using human information, data, or biological samples that falls into the following circumstances—causing no harm to the human body and not involving sensitive personal information or commercial interests—ethical review may be exempted. This is intended to reduce unnecessary burdens on researchers and facilitate the advancement of human-involved life science and medical research. (1) Research utilizing legally obtained public data, or data generated through observation that does not interfere with public behaviors; (2) Research using anonymized information and data. The aforementioned provisions define two specific categories of research scenarios eligible for exemption from ethical review. Their core objective lies in limiting data sources (in terms of public availability and non-interference) and data processing methods (anonymization), which not only reduces the costs associated with ethical review for scientific research but also safeguards the rights and interests of research participants against infringement. This study conducts analyses based on the public Global Burden of Disease (GBD) database and is in compliance with the aforementioned provisions.
Acknowledgments
We sincerely acknowledge Dr. Yujun He for his valuable guidance on the statistical analysis, topic selection, and the writing and revision of this manuscript. We express our gratitude to the Institute for Health Metrics and Evaluation (IHME) for facilitating open access. We especially thank the team for providing authorization and technical support for the JD_GBDR software.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study is supported by National Natural Science Foundation of China (Youth Science Fund Project) (No. 82405422).
Disclosure
Shilei Song, Shengyi Feng, and Haiming Lu, share first authorship. The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Knezevic NN, Candido KD, Vlaeyen JWS, Van Zundert J, Cohen SP. Low back pain. Lancet. 2021;398(10294):78–92. doi:10.1016/S0140-6736(21)00733-9
2. Urits I, Burshtein A, Sharma M, et al. Low back pain, a comprehensive review: pathophysiology, diagnosis, and treatment. Curr Pain Headache Rep. 2019;23(3):23. doi:10.1007/s11916-019-0757-1
3. Vlaeyen JWS, Maher CG, Wiech K, et al. Low back pain. Nat Rev Dis Primers. 2018;4(1):52. doi:10.1038/s41572-018-0052-1
4. Chen S, Chen M, Wu X, et al. Global, regional and national burden of low back pain 1990-2019: a systematic analysis of the global burden of disease study 2019. J Orthop Translat. 2022;32:49–58. doi:10.1016/j.jot.2021.07.005
5. Yang N, Di J, Wang W, Feng H. Global burden of low back pain from 1990 to 2021: a comprehensive analysis of risk factors and trends using the global burden of disease study 2021. BMC Public Health. 2025;25(1):1886. doi:10.1186/s12889-025-23178-1
6. Ferreira ML, de Luca K, Haile LM. Global, regional, and national burden of low back pain, 1990–2020, its attributable risk factors, and projections to 2050: a systematic analysis of the global burden of disease Study 2021. Lancet Rheumatol. 2023;5(6):e316–29. doi:10.1016/S2665-9913(23)00098-X
7. Hartvigsen J, Hancock MJ, Kongsted A, et al. What low back pain is and why we need to pay attention. Lancet. 2018;391(10137):2356–2367. doi:10.1016/S0140-6736(18)30480-X
8. Özüdoğru A, Canlı M, Ceylan İ, Kuzu Ş, Alkan H, Karaçay BÇ. Five times sit-to-stand test in people with non-specific chronic low back pain-a cross-sectional test-retest reliability study. Ir J Med Sci. 2023;192(4):1903–1908. doi:10.1007/s11845-022-03223-3
9. Doménech-Fernández J, Ezzeddine Angulo A, Peñalver-Barrios L, et al. Catastrophizing and fear avoidance beliefs in chronic low back pain: a cross-sectional study. Eur J Phys Rehabil Med. 2025;61(2):305–312. doi:10.23736/S1973-9087.25.08419-9
10. Millere A, Kalnberza-Ribule Z, Mezals M, Nulle A, Millere I, Deklava L. Disability, pain catastrophizing and stress coping of patients with low back pain in rehabilitation practice in Latvia. J Back Musculoskelet Rehabil. 2020;33(2):323–328. doi:10.3233/BMR-170945
11. Bean DJ, Johnson MH, Kydd RR. Relationships between psychological factors, pain, and disability in complex regional pain syndrome and low back pain. Clin J Pain. 2014;30(8):647–653. doi:10.1097/AJP.0000000000000007
12. Dimitrijević V, Rašković B, Jevtić N, Nikolić S, Viduka D, Obradović B. Pain and disability therapy with stabilization exercises in patients with chronic low back pain: a meta-analysis. Healthcare. 2025;13(9):960. doi:10.3390/healthcare13090960
13. Ketenci A. Pharmacological and non-pharmacological treatment approaches to chronic lumbar back pain. Turk J Phys Med Rehabil. 2021;67(1):1–10. doi:10.5606/tftrd.2021.8216
14. Baroncini A, Maffulli N, Schäfer L, et al. Physiotherapeutic and non-conventional approaches in patients with chronic low-back pain: a level I Bayesian network meta-analysis. Sci Rep. 2024;14(1):11546. doi:10.1038/s41598-024-62276-9
15. Liang B, Wei Y, Pei H, Liang X, Chen G, Pei L. Temporal trends of low back pain burden and joinpoint and age-period-cohort analysis in China from 1990 to 2021. BMC Public Health. 2025;25(1):1598. doi:10.1186/s12889-025-22774-5
16. Yetiş M, Yildiz NT, Canli M, et al. Determination of predictors associated with pain in non‑surgically treated adults with idiopathic scoliosis. J Orthop Surg Res. 2024;19(1):406. doi:10.1186/s13018-024-04912-8
17. West R. Tobacco smoking: health impact, prevalence, correlates and interventions. Psychol Health. 2017;32(8):1018–1036. doi:10.1080/08870446.2017.1325890
18. Xu HR, Zhang YH, Ngo TL, Yang QH, Du SH, Wang XQ. Association between smoking and incident back pain: a prospective cohort study with 438 510 participants. J Glob Health. 2023;13:04152. doi:10.7189/jogh.13.04152
19. Jing D, Wu W, Deng X, et al. FoxO1a mediated cadmium-induced annulus fibrosus cells apoptosis contributes to intervertebral disc degeneration in smoking. J Cell Physiol. 2021;236(1):677–687. doi:10.1002/jcp.29895
20. Cusano NE. Skeletal Effects of Smoking. Curr Osteoporos Rep. 2015;13(5):302–309. doi:10.1007/s11914-015-0278-8
21. Elmasry S, Asfour S, de Rivero Vaccari JP, Travascio F. Effects of tobacco smoking on the degeneration of the intervertebral disc: a finite element study. PLoS One. 2015;10(8):e0136137. doi:10.1371/journal.pone.0136137
22. Xu HR, Zhang YH, Zheng YL. The effect and mechanism of motor control exercise on low back pain: a narrative review. EFORT Open Rev. 2023;8(7):581–591. doi:10.1530/EOR-23-0057
23. Migliorini F, Maffulli N, Schäfer L, et al. Impact of education in patients undergoing physiotherapy for lower back pain: a level I systematic review and meta-analysis. Eur J Trauma Emerg Surg. 2025;51(1):113. doi:10.1007/s00068-025-02788-9
24. Zhang J, Tian Y, Li Y, et al. Time trends in the burden of low back pain and its associated risk factors in China from 1990 to 2019. J Orthop Translat. 2024;45:256–265. doi:10.1016/j.jot.2024.02.006
25. National Health Commission of the People’s Republic of China. China Health Statistics Yearbook 2023. Vol. 409. Beijing: Peking Union Medical College Press; 2024:150.
26. Deng S, Li H, Zuo W, Liu Z, Wu Y. Smoking prevalence among adults in China Mainland and their age of smoking initiation during adolescence: a national cross-sectional study. BMJ Open. 2024;14(9):e082717. doi:10.1136/bmjopen-2023-082717
27. Wang B, Zhang J, Du P, Ke H, Zang L, Yuan S. Global burden of low back pain attributable to smoking in 204 countries and territories in 1990-2021. Front Public Health. 2025;13:1584659. doi:10.3389/fpubh.2025.1584659
28. Xu J, Li J, Huang H, et al. High-BMI-related low back pain in China: a GBD-based observational study on sex-age trends and projections (1990-2021). Eur J Med Res. 2025;30(1):496. doi:10.1186/s40001-025-02765-3
29. Ye J, Chen J, Ding H, Xia Z, Wang J, Jia Y. The global burden of low back pain attributable high body mass index over the period 1990-2021 and projections up to 2035. Front Nutr. 2025;12:1568015. doi:10.3389/fnut.2025.1568015
30. He Y, Tang W, Chen J, et al. Global burden of chronic kidney disease due to hypertension (1990–2021): a systematic analysis of epidemiological trends, risk factors, and projections to 2036 from the GBD 2021 study. BMC Nephrol. 2025;26(1):448. doi:10.1186/s12882-025-04386-8
31. Li Y, Li H, Tang L, Chen C, Huang C. Global burden and cross-national inequalities of tobacco-attributable cancers in adults aged 40 and above, 1990–2021: a population-based study. Front Oncol. 2025;15:1631356. doi:10.3389/fonc.2025.1631356
32. Kim H-J, Fay MP, Feuer EJ, Midthune DN. Permutation tests for joinpoint regression with applications to cancer rates. Stat Med. 2000;19(3):335–351. doi:10.1002/(SICI)1097-0258(20000215)19:3<335::AID-SIM336>3.0.CO;2-Z
33. Joinpoint Help System [Internet]. Selecting the Final Model. Available from: https://surveillance.cancer.gov/help/joinpoint/tech-help/frequently-asked-questions/selecting-the-final-model. Accessed 2025 May 20.
34. Lv JC, Zhang LX. Prevalence and disease burden of chronic kidney disease. Adv Exp Med Biol. 2019;1165:3–15.
35. Yang Y, Schulhofer‐Wohl S, Fu WJ, Land KC. The intrinsic estimator for age‐period‐cohort analysis: what it is and how to use it. Am J Sociol. 2008;113(6):1697–1736. doi:10.1086/587154
36. Luo L. Assessing validity and application scope of the intrinsic estimator approach to the age-period-cohort problem. Demography. 2013;50(6):1945–1967. doi:10.1007/s13524-013-0243-z
37. Yang Y. Social inequalities in happiness in the United States, 1972 to 2004: an age-period-cohort analysis. Am Sociological Rev. 2008;73(2):204–226. doi:10.1177/000312240807300202
38. Nguyen HV, Naeem MA, Wichitaksorn N, Pears R. A smart system for short-term price prediction using time series models. Comput Electr Eng. 2019;76:339–352. doi:10.1016/j.compeleceng.2019.04.013
39. Li Y, Ning Y, Shen B, et al. Temporal trends in prevalence and mortality for chronic kidney disease in China from 1990 to 2019: an analysis of the global burden of disease study 2019. Clin Kidney J. 2022;16(2):312–321. doi:10.1093/ckj/sfac218
40. Riebler A, Held L. Projecting the future burden of cancer: bayesian age–period–cohort analysis with integrated nested Laplace approximations. Biometrical J. 2017;59(3):531–549. doi:10.1002/bimj.201500263
41. Lin B, Xie L, Xie X, Yan Y, Zhang L, Xiao L. Predictors for quitting smoking in smoking cessation clinics among female smokers in China. Tob Induc Dis. 2023;21:26. doi:10.18332/tid/159132
42. Kranjac D, Kranjac AW. Age–period–cohort effects of adult cigarette smoking in the United States, 1971–2020. Sci Rep. 2025;15(1):14341. doi:10.1038/s41598-025-98843-x
43. Liu T. Super-aging and social security for the most elderly in China. Z Gerontol Geriatr. 2018;51(1):105–112. doi:10.1007/s00391-016-1062-9
44. Sun D, Pang Y, Lyu J, Li L. Department of epidemiology & biostatistics, school of public health, Peking university, Beijing, China, Peking university center for public health and epidemic preparedness & response, Beijing, China. current progress and challenges to tobacco control in China. China CDC Weekly. 2022;4(6):101–105.
45. Shiwei L, Lin X. Tobacco monitoring in China development and challenges of tobacco epidemic surveillance in China. Chin J Epidemiol. 2022;43(06):804–810.
46. Min K, Jing S. Age⁃period⁃cohort analysis and prediction of asthma burden attributed to tobacco in China from 1990 to 2019. J Internal Med Concepts Pract. 2024;1–6.
47. Yao T, Jiang N, Grana R, Ling PM, Glantz SA. A content analysis of electronic cigarette manufacturer websites in China. Tob Control. 2016;25(2):188–194. doi:10.1136/tobaccocontrol-2014-051840
48. Wang W, He Z, Feng N, Cai Y. Electronic cigarette use in China: awareness, prevalence and regulation. Tob Induc Dis. 2019;17(April):30. doi:10.18332/tid/105393
49. Fan J, Mao T, Zhen S, Xu Y, Qu C. Comparative analysis of e-cigarette prevalence and influencing factors among adolescents in Jiangsu Province, China. Front Public Health. 2023;11:1221334. doi:10.3389/fpubh.2023.1221334
50. Ling PM, Kim M, Egbe CO, Patanavanich R, Pinho M, Hendlin Y. Moving targets: how the rapidly changing tobacco and nicotine landscape creates advertising and promotion policy challenges. Tob Control. 2022;31(2):222–228. doi:10.1136/tobaccocontrol-2021-056552
51. Flor LS, Reitsma MB, Gupta V, Ng M, Gakidou E. The effects of tobacco control policies on global smoking prevalence. Nat Med. 2021;27(2):239–243. doi:10.1038/s41591-020-01210-8
52. Mao A, Bottorff JL, Oliffe JL, Sarbit G, Kelly MT. A qualitative study of Chinese Canadian fathers’ smoking behaviors: intersecting cultures and masculinities. BMC Public Health. 2015;15(1):286. doi:10.1186/s12889-015-1646-0
53. Mao A, Yang T, Bottorff JL, Sarbit G. Personal and social determinants sustaining smoking practices in rural China: a qualitative study. Int J Equity Health. 2014;13(1):12. doi:10.1186/1475-9276-13-12
54. Hu SS. Writing committee of the report on cardiovascular health and diseases in china. influencing factors on cardiovascular health in China. J Geriatr Cardiol. 2024;21(1):4–33. doi:10.26599/1671-5411.2024.01.009
55. Ding L, Liang Y, Tan ECK, et al. Smoking, heavy drinking, physical inactivity, and obesity among middle-aged and older adults in China: cross-sectional findings from the baseline survey of CHARLS 2011-2012. BMC Public Health. 2020;20(1):1062. doi:10.1186/s12889-020-08625-5
56. National Health Commission. Healthy China initiative (2019-2030) [Internet]. Available from: https://www.gov.cn/xinwen/2019-07/15/content_5409694.htm. Accessed October 2, 2025.
57. Li X. China adult tobacco survey report 2018 [Internet]. Beijing: People’s Medical Publishing House; 2020. Available from: https://cn.bing.com/search?q=China+adult+tobacco+survey+report+2018&cvid=e92e27ef8c4944bc9fe7703bfdea6371&gs_lcrp=EgRlZGdlKgYIABBFGDkyBggAEEUYOTIGCAEQABhA0gEHNDQ5ajBqNKgCCLACAQ&FORM=ANAB01&PC=U531.
58. Liu C, Wang Y, Liu M, et al. Global, regional, and national burden and trends of tension-type headache among adolescents and young adults (15–39 years) from 1990 to 2021: findings from the global burden of disease study 2021. Sci Rep. 2025;15(1):18254. doi:10.1038/s41598-025-02818-x
59. Lee PN, Farsalinos K. Comparing smoking-related disease rates from e-cigarette use with those from tobacco cigarette use: a reanalysis of a recently-published study. Harm Reduct J. 2025;22(1):78. doi:10.1186/s12954-025-01230-y
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Global, Regional and National Burden of Low Back Pain in Adolescents Aged 10–19 years, 1990–2021: A Systematic Analysis of the Global Burden of Disease Study 2021
Wang S, Zhang S, Li M, Chen S, Chen Y, Song Y, Zhang X
Journal of Pain Research 2025, 18:3171-3183
Published Date: 26 June 2025
Edentulism Trends in Chinese Women vs US and Global Women: GBD 2021 Outlook
Chen H, Jing Y, Song Y, Jia Z, He X, Zhang S, Wu M
International Journal of Women's Health 2025, 17:4661-4670
Published Date: 20 November 2025
Global, Regional, and National Burden of Alopecia Areata in Children and Adolescents Aged 0-19 years from 1990 to 2021 and Projection to 2040
Lu H, Li J, Ma K, Li L, Wang S, Wang T, Zhang B
Clinical, Cosmetic and Investigational Dermatology 2026, 19:582775
Published Date: 6 February 2026
Global, Regional, and National Burden of Adolescent Polycystic Ovary Syndrome from 1990 to 2021, with Projections of Disease Burden to 2041: A Systematic Analysis Based on the Global Burden of Disease Study 2021
Cao X, Yu Z, Wu S
International Journal of Women's Health 2026, 18:587430
Published Date: 13 March 2026
Epidemiological Trends and Projections of PM2.5-Attributable COPD Burden in China Over 1990–2035
Li M, Wang L, Amhare AF, Song Y, Wan P, Shi S, Qiao L, Guo Y
International Journal of Chronic Obstructive Pulmonary Disease 2026, 21:565060
Published Date: 16 March 2026