Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Epidemiological Trends and Projections of PM2.5-Attributable COPD Burden in China Over 1990–2035
Authors Li M, Wang L, Amhare AF, Song Y, Wan P, Shi S, Qiao L, Guo Y
Received 3 September 2025
Accepted for publication 3 March 2026
Published 16 March 2026 Volume 2026:21 565060
DOI https://doi.org/10.2147/COPD.S565060
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jill Ohar
Miaoqian Li,1– 3,* Liangjia Wang,2,3,* Abebe Feyissa Amhare,3,4 Yufei Song,2,3 Ping Wan,2,3 Shaoteng Shi,2,3 Lichun Qiao,2,3 Yijie Guo1
1Department of Psychiatry, The First Affiliated Hospital of Xi’an Jiaotong University, Xi’an, People’s Republic of China; 2School of Public Health, Xi’an Jiaotong University Health Science Center, Xi’an, People’s Republic of China; 3Health Science Center, Xi’an Jiaotong University, Xi’an, People’s Republic of China; 4The Second Affiliated Hospital, Xi’an Jiaotong University Health Science Center, Xi’an, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yijie Guo, First Affiliated Hospital of Xi’an Jiaotong University, Xi’an, People’s Republic of China, Email [email protected]
Objective: This study investigated long-term trends in the burden of chronic obstructive pulmonary disease (COPD) attributable to PM2.5 in China from 1990 to 2021 and projected future patterns through 2035.
Methods: Data were obtained from the Global Burden of Disease Study 2021. Key indicators included disability-adjusted life years (DALYs), deaths, age-standardized disability-adjusted life years rates (ASDR), and age-standardized mortality rates (ASMR), which together characterize both individual-level and population-level disease burden. Analyses were stratified by sex and age group. Future trends were projected using a Bayesian age–period–cohort (BAPC) model.
Results: From 1990 to 2021, the COPD burden in China showed a sustained downward trend. The overall ASDR decreased from 2692.65 to 473.09 per 100,000 population (approximately an 82.4% reduction), while the ASMR declined from 162.33 to 28.22 per 100,000 population (approximately an 82.6% reduction). More pronounced declines were observed during the mid-1990s to early 2000s. A modest increase in PM2.5-attributable COPD burden was noted in 2020, which may be associated with disruptions related to the COVID-19 pandemic. In 2021, COPD attributable to PM2.5 accounted for an estimated 9.16 million DALYs and 497,000 deaths, with a consistently higher burden observed among males. Projections indicate a continued overall decline in COPD burden by 2035, although a slight upward trend in ASMR is projected among males.
Conclusion: COPD attributable to PM2.5 continues to impose a substantial public health burden in China. Despite long-term declines in age-standardized rates, the observed fluctuation in 2020 suggests ongoing vulnerability among individuals with chronic respiratory diseases. Continued efforts targeting air quality improvement and smoking reduction may contribute to further mitigation of COPD burden, particularly among high-risk populations.
Keywords: chronic obstructive pulmonary disease, air pollution, disease burden, epidemiology, global burden of disease, disability-adjusted life years, smoking
Introduction
Chronic obstructive pulmonary disease (COPD) is a progressive lung condition characterized by persistent airflow limitation, which impairs respiratory function.1 The onset of COPD is typically slow, with early symptoms being subtle, so many patients are not diagnosed until the disease reaches advanced stages.2 COPD is primarily exacerbated by a variety of environmental and behavioral risk factors, with smoking and environmental pollution, particularly long-term exposure to fine particulate matter (PM2.5), being the most significant contributors.3 While smoking has long been recognized as the primary risk factor for COPD,4,5 the contribution of environmental pollutants—particularly long-term exposure to PM2.5—has gained increasing attention in recent years, especially in developing countries like China. PM2.5 particles can penetrate deep into the lungs, triggering oxidative stress and inflammatory responses that contribute to airway remodeling and airflow limitation, thereby exacerbating respiratory conditions such as COPD.6–9
The impact of COPD extends beyond respiratory dysfunction, leading to a range of severe health issues, including pulmonary failure,10 cor pulmonale, and premature death.2 As the disease progresses, the quality of life for COPD patients significantly declines, often requiring frequent hospitalizations and long-term medical interventions.11 Furthermore, COPD patients often suffer from comorbidities such as cardiovascular diseases12 and diabetes,13 which further exacerbate the burden of the disease.
Globally, COPD is one of the leading causes of death, responsible for approximately 3.28 million deaths annually, representing a significant proportion of global mortality.14 In China, the burden of COPD is particularly severe, with the country accounting for about a quarter of the world’s COPD patients.15 The prevalence and incidence of COPD in China have been steadily increasing due to changes in lifestyle, urbanization, and rising industrial pollution.16,17 Particularly, the high concentration of fine particulate matter has become a key factor in exacerbating this trend.18 PM2.5 particles, with a diameter of 2.5 micrometers or less, are not chemically uniform pollutants but rather a complex mixture of components—including elemental carbon (soot), transition metals, sulfates, nitrates, and secondary organic aerosols (SOAs)—that can penetrate deep into the lungs, triggering oxidative stress and inflammatory responses that contribute to chronic airway remodeling and airflow limitation.7,19,20 Moreover, PM2.5 not only directly damages lung tissue but can also affect other organs, including the heart, through the bloodstream. It may also cause abnormal immune responses, making the airways more susceptible to infection and inflammation, thereby accelerating the progression of COPD.21 In 1990, China experienced relatively high levels of smoking prevalence and ambient PM2.5 exposure, whereas by 2021, smoking prevalence had declined and air quality had improved overall, alongside changes in the burden of COPD.22,23
In parallel with these epidemiological changes, China has implemented a series of national-level public health and environmental interventions over the past three decades. Tobacco control efforts have gradually expanded since the 1990s, including restrictions on smoking in public places24 and the adoption of the WHO Framework Convention on Tobacco Control in the mid-2000s.25 Meanwhile, environmental policies targeting air pollution have evolved through progressively stricter emission standards and revisions of the Ambient Air Quality Standards, particularly after 2013.26 Although the effects of these interventions may vary across populations and time periods, their staggered implementation provides an important policy context for examining long-term temporal trends in COPD burden attributable to PM2.5 exposure.
This study aims to analyze the long-term trends in the COPD burden attributable to PM2.5 exposure in China from 1990 to 2021. Using data from the Global Burden of Disease Study 2021 (GBD 2021), we will focus on exploring changes in mortality, disability-adjusted life years (DALYs), and age-standardized rates (ASR). These indicators will not only provide insights into the epidemiology of COPD but also reveal the contribution of PM2.5 exposure to the disease burden, especially across different regions and populations. Therefore, this study aimed to examine long-term trends in PM2.5-attributable COPD burden in China from 1990 to 2021, as measured by mortality, disability-adjusted life years, and age-standardized rates, and to project future trends for 2022–2035.
Materials and Methods
Study Data Source
This study utilizes data from the GBD 2021, which provides comprehensive epidemiological information for 204 countries and regions, covering 21 geographical areas from 1990 to 2021. The GBD 2021 data were retrieved from the Global Health Data Exchange (GHDx) platform (http://ghdx.healthdata.org/gbd-results-tool). The analysis focuses on COPD in China, evaluating metrics such as DALYs, mortality, and age-standardized disability-adjusted life years rate (ASDR) and age-standardized mortality rate (ASMR). These metrics were stratified by sex and age, with age groups divided into 5-year categories from 25–29 years to ≥75 years. All estimates were reported with 95% uncertainty intervals (95% UI). The study was conducted in accordance with the Guidelines for Accurate and Transparent Health Estimates Reporting (GATHER).
Statistical Analysis
COPD data from China between 1990 and 2021 were grouped by 5-year age intervals to assess mortality and DALY trends across different age groups. Age-standardized rates were calculated for both the ASDR and the ASMR to facilitate comparison of temporal changes in the overall COPD burden. In addition, the relationship between the Socio-demographic Index (SDI) a composite indicator incorporating income per capita, educational attainment, and fertility rate, and COPD burden was examined to explore how levels of socio-economic development may be associated with variations in COPD burden across regions and over time.
To better understand the association between PM2.5 exposure and respiratory outcomes, we also examined the burden of major diseases attributable to PM2.5 as defined in the Global Burden of Disease (GBD) 2021 study. In addition, we assessed the contributions of major environmental and behavioral risk factors to the COPD burden. These risk factors included ambient ozone pollution, high and low temperature, occupational exposure to particulate matter, gases, and fumes, particulate matter pollution, secondhand smoke, and smoking.
Attributable COPD-related DALYs and deaths for each risk factor were directly extracted from the GBD Results Tool, which applies a standardized comparative risk assessment (CRA) framework. This method uses population-attributable fractions (PAFs) derived from exposure distributions and theoretical minimum risk levels to quantify the portion of disease burden attributable to each risk factor. In this study, both total COPD burden and PM2.5-attributable COPD burden were analyzed separately to clearly distinguish overall trends from those specifically linked to environmental exposures.
Sex-specific and temporal trends in both total and risk-attributable COPD burden were assessed from 1990 to 2021. To quantify these temporal patterns, the estimated annual percentage change (EAPC) was calculated for ASRs. An EAPC with a 95% uncertainty interval (UI) that did not cross zero was considered statistically significant, with positive values indicating increasing trends and negative values indicating decreasing trends. Projections of COPD burden from 2021 to 2035 were generated using a Bayesian age-period-cohort (BAPC) model. A two-sided P-value of less than 0.05 was considered indicative of statistical significance. It is important to note that the GBD 2021 estimates used in this study assess the health burden attributable to PM2.5 based on total mass concentration, without distinguishing among specific chemical components or emission sources.
Sensitivity and Robustness Analyses
To assess the robustness of our findings, all estimates of mortality, DALYs, and age-standardized rates were reported with corresponding 95% uncertainty intervals (UIs) provided by the GBD 2021 study. Temporal trends were considered robust when conclusions remained consistent within these uncertainty ranges. In addition, sensitivity analyses were conducted by comparing age-standardized rates with crude rates, and by examining trends stratified by sex and age groups.
Results
Disease Burden and Trends
From 1990 to 2021, the burden of COPD in China showed a steady decline, with significant reductions observed at two key inflection points: in 1994 for the ASDR, and in 2003 for the ASMR, where the rates of decline accelerated markedly (Figure 1A and B). However, in 2020, there was an uptick in both the number of DALYs and deaths, along with an increase in ASDR and ASMR (Figure 1C and D). By 2021, the total COPD burden in China was estimated at approximately 9.16 million DALYs and 497,000 deaths. Of these, a significant proportion was attributable to PM2.5 exposure, based on GBD 2021 estimates. Temporal patterns revealed a steady decline in both total and PM2.5-attributable COPD burden between 1990 and 2021. In terms of gender differences, females exhibited lower ASDR and ASMR compared to males, with corresponding EAPC of −6.42% (−6.76% to −6.08%) and −6.74% (−7.14% to −6.34%), respectively (Table 1). Although females generally showed lower rates of DALYs and mortality across all age groups, in 1990, the DALYs and mortality rates for females aged 75 years and older exceeded those of males (Figure 2), indicating a higher burden of COPD among elderly females in this age group.
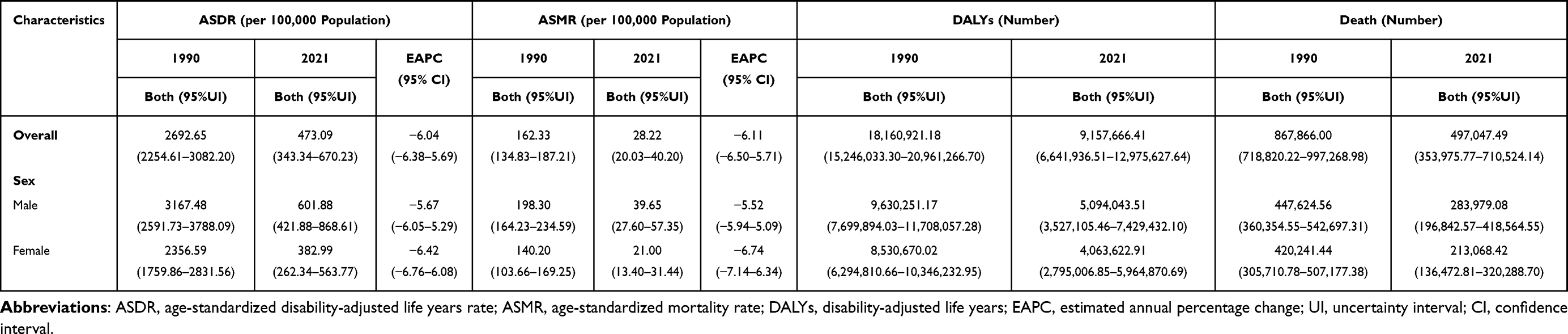 |
Table 1 Changes in the DALYs Number, Deaths Number, ASDR, and ASMR from 1990 to 2021 |
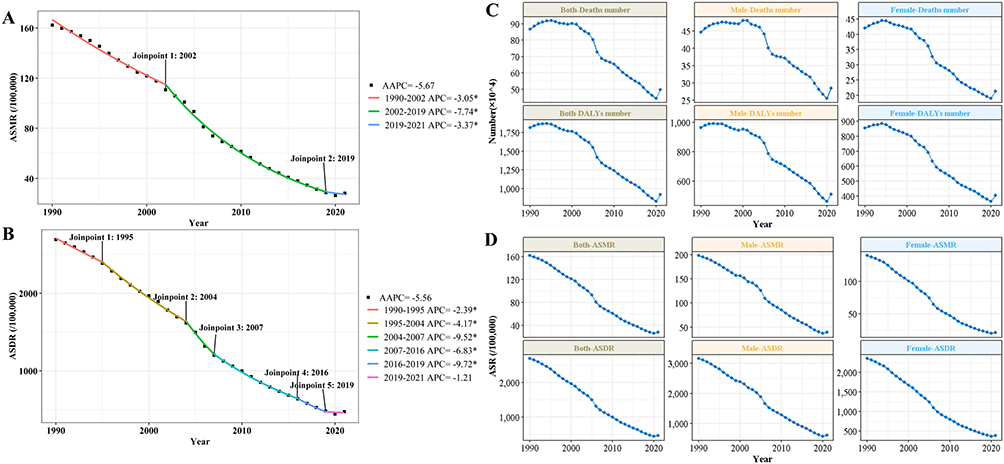 |
Figure 1 Time Series Analysis of the Impact of PM2.5 on COPD in China. (A and B) The AAPC in ASDR and ASMR from 1990 to 2021. (C and D) Temporal trends in the number of DALYs and the number of deaths, as well as ASDR and ASMR, by sex from 1990 to 2021. * P < 0.05. Abbreviations: COPD, chronic obstructive pulmonary disease; AAPC, average annual percent change; ASDR, age-standardized disability-adjusted life years rate; ASMR, age-standardized mortality rate; DALYs, disability-adjusted life years. |
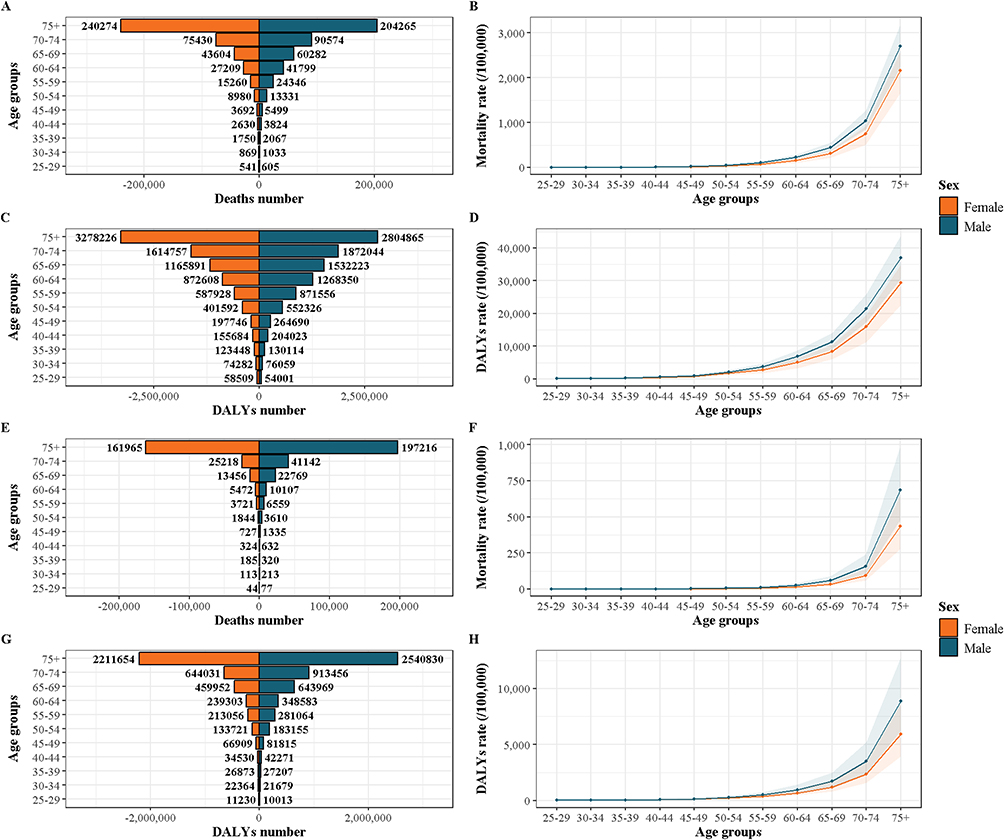 |
Figure 2 Analysis of the Impact of PM2.5 on COPD by Sex in China. (A–D) The number and rate of deaths and DALYs by sex for 1990. (E–H) The number and rate of deaths and DALYs by sex for 2021. Abbreviations: COPD, chronic obstructive pulmonary disease; DALYs, disability-adjusted life years. |
The Changing Trends of Major Risk Factors
From 1990 to 2021, the seven leading risk factors contributing to the COPD burden included ambient ozone pollution, high temperature, low temperature, occupational exposure to particulate matter, gases, and fumes, particulate matter pollution, secondhand smoke, and smoking. Among these factors, particulate matter pollution had a particularly significant impact, especially on females, where it consistently contributed to high DALY and mortality rates. Although the influence of particulate matter pollution on COPD among females has gradually decreased over the past 30 years, its proportion remains substantially higher than other risk factors.
In contrast, smoking has remained the dominant risk factor among males, accounting for over 60% of the DALYs and deaths associated with COPD. Over time, smoking has surpassed particulate matter pollution in approximately 2003 to become the leading risk factor for COPD among males. Overall, particulate matter pollution and smoking are the two primary risk factors for the COPD burden. Despite a gradual decline in the proportion of DALYs and deaths attributable to particulate matter pollution, a turning point was observed in 2020, indicating a resurgence, which underscores the continued significance of this risk factor (Figure 3).
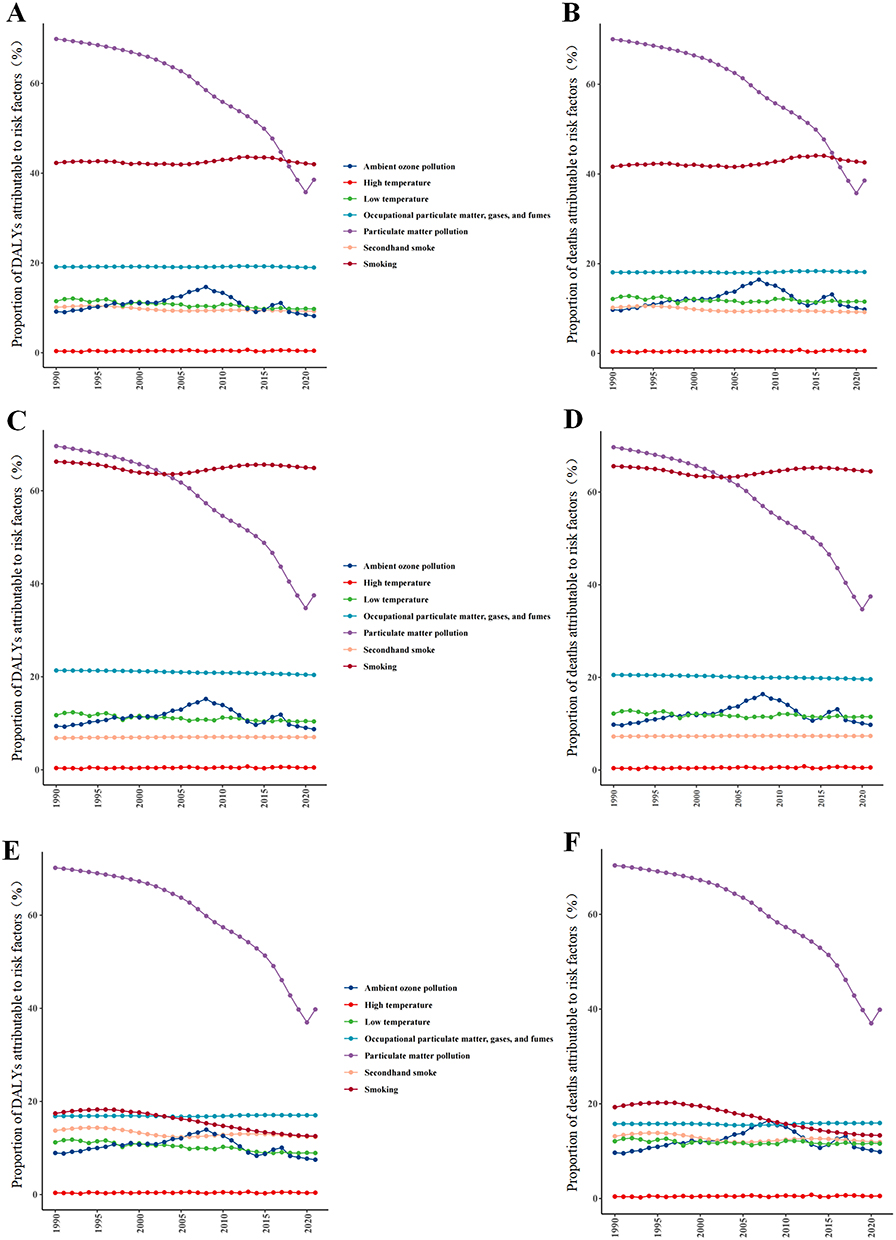 |
Figure 3 The Progression of COPD Risk Factors over the Period from 1990 to 2021. (A–F) The proportion of COPD’s DALYs and death attributable to risk factors. (A) Results for overall DALYs; (B) Results for overall death; (C) Results for male DALYs; (D) Results for male death; (E) Results for female DALYs; (F) Results for female death. Abbreviations: COPD, chronic obstructive pulmonary disease; DALYs, disability-adjusted life years. |
Status of COPD and Its Correlation with the SDI
Among diseases attributable to PM2.5 exposure, COPD ranked first in terms of ASDR and ASMR in 1990 and remained among the top three contributors in 2021 (Figure 4).
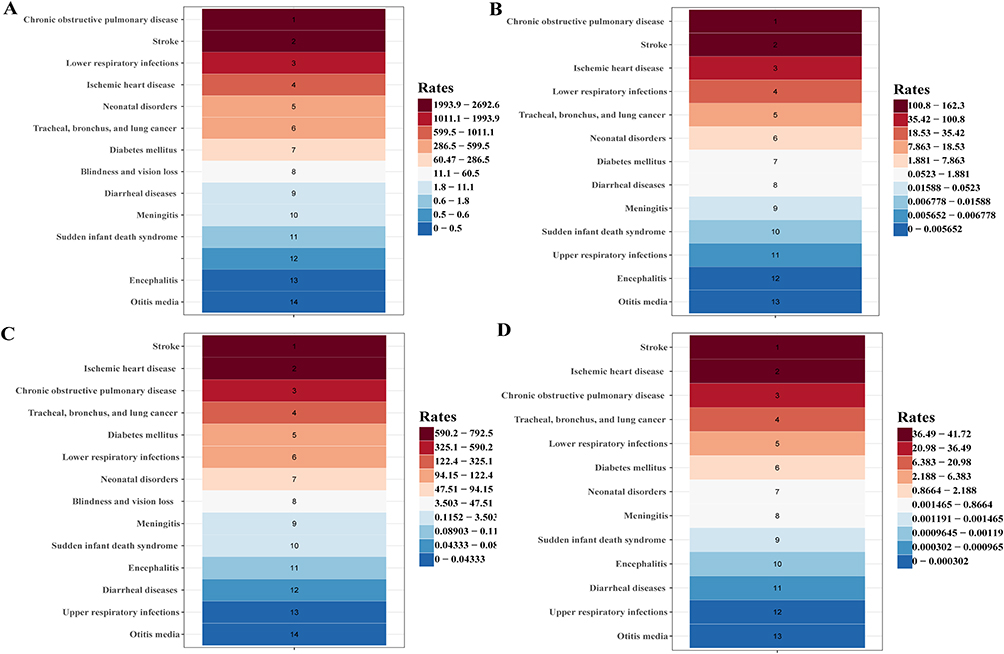 |
Figure 4 The Ranking of PM2.5-related Diseases from 1990 to 2021. (A) ASDR of PM2.5-related diseases for 1990; (B) ASMR of PM2.5-related diseases for 2021; (C) ASDR of PM2.5-related diseases for 1990; (D) ASMR of PM2.5-related diseases for 2021. Abbreviations: ASDR, age-standardized disability-adjusted life years rate; ASMR, age-standardized mortality rate. |
There is a negative correlation between SDI and both ASDR and ASMR for COPD, with Pearson correlation coefficients of −0.8579 and −0.8564, respectively. As the SDI increases, a clear downward trend is observed in COPD’s ASDR and ASMR. China’s SDI, ranging from approximately 0.6 to 0.7, reflects relatively low ASDR and ASMR for COPD. However, when compared with countries of similar SDI levels, such as Argentina, Brazil, and Chile, China shows a slightly higher COPD disease burden. Compared with countries of similar SDI levels, such as Argentina, Brazil, and Chile, China showed relatively higher ASDR and ASMR values for COPD, suggesting a persistent burden despite comparable socioeconomic conditions (Figure 5).
 |
Figure 5 The Relationship Between the Burden of COPD and SDI in 2021. (A) The relationship between the ASDR and SDI in 2021. (B) The relationship between the ASMR and SDI in 2021. Abbreviations: COPD, chronic obstructive pulmonary disease; SDI, Socio-Demographic Index; ASDR, age-standardized disability-adjusted life years rate; ASMR, age-standardized mortality rate. Note, different colors of text correspond to different countries or regions. |
Projection from 2021 to 2035
The analysis of DALY rates across all age groups shows a significant overall decline during the study period, with a brief increase observed in 2020. In the 25–29 years group, the DALY rate is projected to decrease from 1.06 to 0.06 per 100,000 population, with an estimated APC of –6.25%. Similarly, the 45–49 years group is expected to decline from 17.87 to 0.70 per 100,000, corresponding to an APC of –6.94% (Figure 6).
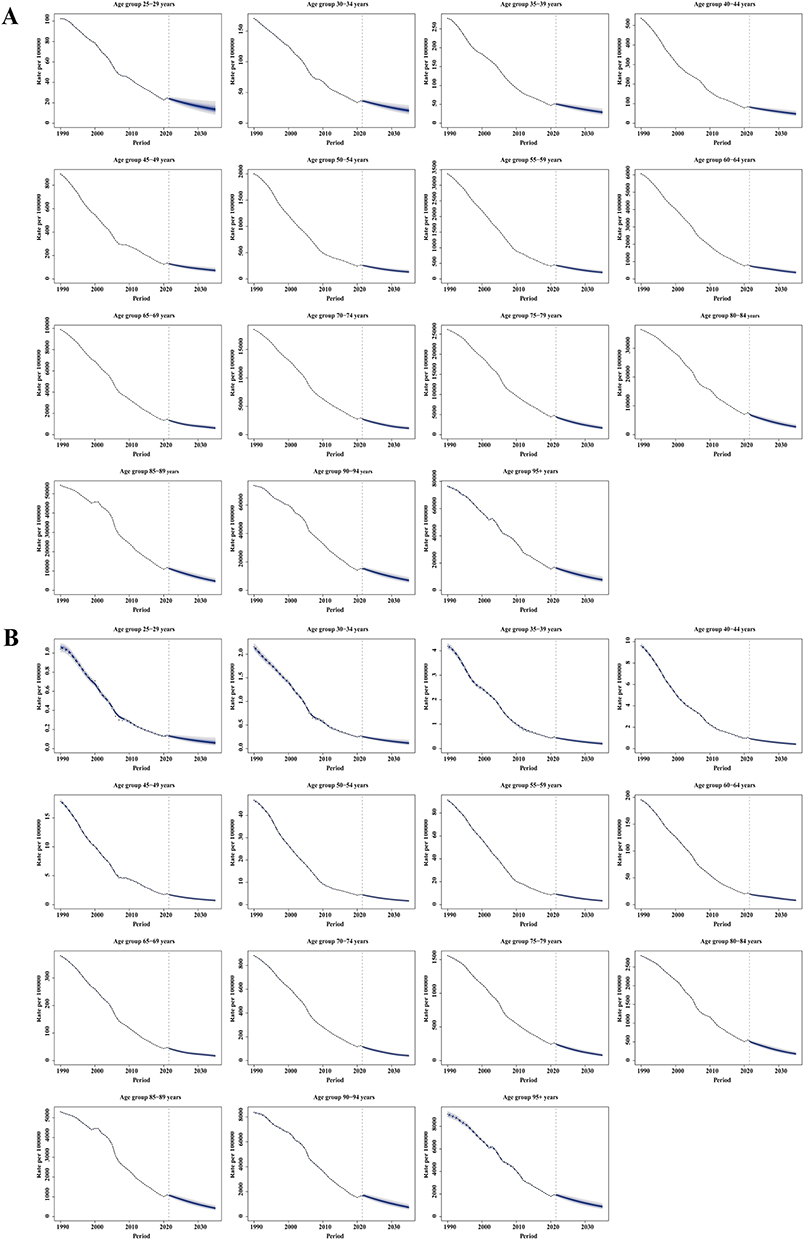 |
Figure 6 The Projected Results for DALYs Rate And Death Rate of COPD Across Different Age Groups Up to 2035. (A) Predicted results of DALYs rate for different age groups. (B) Predicted results of death rate for different age groups. Abbreviations: DALYs, disability-adjusted life years; COPD, chronic obstructive pulmonary disease. |
The most pronounced reductions were observed among middle-aged populations. Specifically, the 35–39 years group showed a decline from 4.19 to 0.20 per 100,000, corresponding to an APC of –6.54%, and the 40–44 years group decreased from 9.64 to 0.41 per 100,000, with an APC of –6.80%. These trends indicate a sustained and substantial decrease in COPD burden across working-age and older adults (Figure 6).
When analyzing the overall and gender-specific trends in ASDR and ASMR, the projections indicate divergent trajectories between males and females. The ASDR for males is projected to decline from 165.04 per 100,000 in 1990 to 10.58 in 2035. For females, the ASDR is expected to drop from 142.49 to 32.46 over the same period. The decline is more pronounced in males, leading to a narrowing gender gap in COPD mortality. In contrast, the age-standardized mortality rate (ASMR) is projected to increase slightly among males by 2035, while it is expected to decrease slightly among females. Both projections are accompanied by wide uncertainty intervals, indicating greater variability in long-term trends. These results reflect persistent gender disparities in COPD burden and highlight the influence of risk exposure differences and healthcare accessibility between males and females (Figure 7).
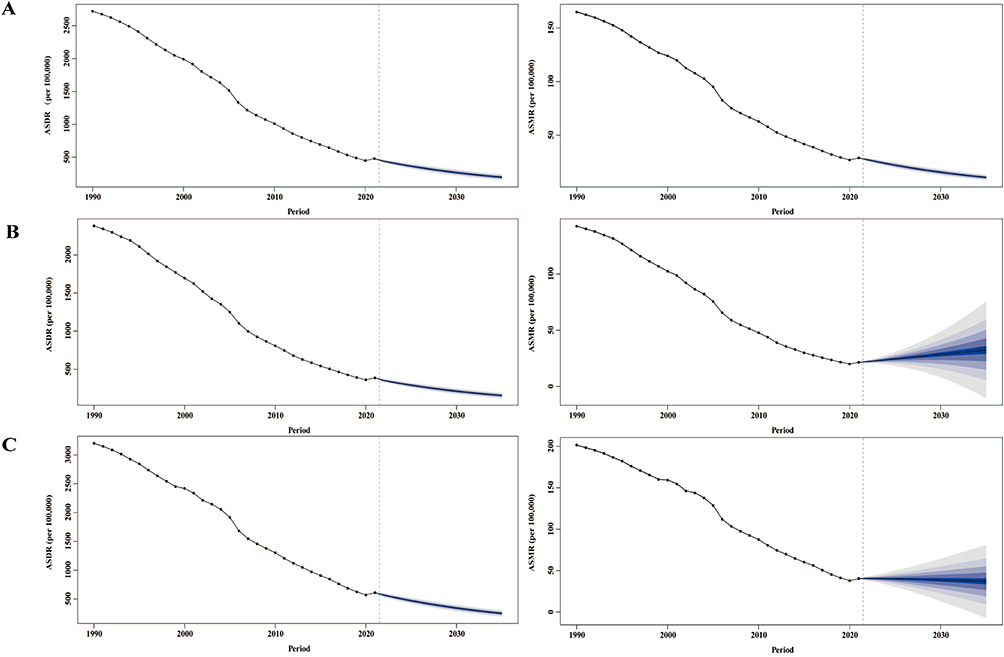 |
Figure 7 Forecasts for the Overall and Sex-specific ASDR and ASMR for COPD. (A) Predicted results for overall of ASDR and ASMR. (B) Predicted results for male of ASDR and ASMR. (C) Predicted results for female of ASDR and ASMR. Abbreviations: ASDR, age-standardized disability-adjusted life years rate; ASMR, age-standardized mortality rate; COPD, chronic obstructive pulmonary disease. |
Discussions
The overall burden of COPD in China has decreased from 1990 to 2021, with notable declines in both DALYs and mortality rates. However, a slight resurgence occurred in 2020 across both male and female populations, which coincided with the COVID-19 pandemic. Previous studies have shown that individuals with pre-existing chronic respiratory diseases, including COPD, tend to experience poorer clinical outcomes following SARS-CoV-2 infection.27 This increased vulnerability may be related to altered pulmonary physiology and immune responses in COPD patients.28–30 In addition, the pandemic placed substantial strain on healthcare systems in 2020, which may have disrupted routine management and follow-up care for chronic diseases. Together, these factors may partially explain the short-term fluctuation observed in COPD burden during this period, although causal attribution cannot be definitively established.
In terms of DALYs and mortality rates, both the absolute numbers and proportions of COPD burden increase with age, with the highest burden observed in individuals aged 75 and above. This indicates that older adults face the most significant health and life expectancy losses due to COPD. As a progressive respiratory disease, COPD is characterized by cumulative functional decline over the life course, and age-related physiological changes may further exacerbate disease severity.31 These age-related vulnerabilities likely contribute to higher disability and mortality risks in older populations.32–35
In terms of gender differences, with males consistently exhibiting higher overall DALYs and mortality rates, a pattern that aligns with historically higher smoking prevalence among men in China.36 Notably, in 1990, females aged 75 years and older exhibited higher COPD-related DALYs and mortality rates than their male counterparts. This finding may be associated with long-term exposure to indoor air pollution from biomass fuel use, which has been more prevalent among women in earlier decades, as well as potential disparities in healthcare access and disease recognition.37 Over the next 15 years, although the overall burden of COPD is expected to decline, the ASMR for men may experience a slight increase. This trend could be attributed to the continued prevalence of smoking among males. However, as China’s “Healthy China 2030” initiative, which aims to reduce the smoking rate from 27.7% in 2015 to 20% by 2030, is progressively implemented, the progressive implementation of tobacco control measures, including non-price interventions and increased tobacco taxes, may contribute to a gradual reduction in smoking prevalence at the population level.38 Consequently, although the ASMR may continue to rise, the rate of increase may decelerate over time, potentially reflecting the long-term population-level benefits of declining smoking prevalence rather than effects directly demonstrated by the study data. Based on this forecast, it is crucial to emphasize the importance of adopting healthy lifestyles, including a balanced diet and regular sleep patterns. From a public health perspective, early diagnosis and regular screening for individuals with impaired lung function are widely recognized as important strategies for reducing disability and mortality associated with advanced COPD.
While many studies have documented the biological effects of PM2.5 and smoking on COPD risk, few have quantitatively assessed how public health interventions have influenced long-term COPD trends at the population level.9,39,40 Our study addresses this gap by revealing two major inflection points in COPD burden—around 1994 and 2003—that may coincide with the implementation of national policies such as early smoking bans,41 emission control programs,42 and stricter air quality standards.43 Although causality cannot be definitively established, the temporal alignment of these policy shifts with observed declines suggests a potentially meaningful impact. These results highlight the importance of sustained, large-scale interventions in reducing COPD burden.
This study has several limitations that should be acknowledged. First, the analysis relies on data from the GBD study, which may be subject to quality limitations, particularly in low- and middle-income regions where underreporting or misclassification of COPD cases could affect the accuracy of burden estimates. In addition, the spatial resolution of the available data is relatively coarse, as estimates are primarily reported at the national level, which limits the ability to examine subnational or regional heterogeneity in PM2.5 exposure and COPD burden. Moreover, the GBD framework estimates PM2.5-attributable burden based on total mass concentration without differentiating between chemical components or emission sources. Given that PM2.5 is a heterogeneous mixture—including elemental carbon, sulfates, metals, and secondary organic aerosols—with varying toxicological profiles, this limitation restricts more detailed interpretation of component-specific toxicity and limits the ability to distinguish potential differences in health effects associated with varying PM2.5 sources across regions. Additionally, while our projections provide useful insights, they are based on historical trends and may not account for future interventions or unexpected environmental changes. This study also did not apply time-series models such as Joinpoint regression or ARIMA, which could better characterize non-linear trends and account for autocorrelation. Furthermore, due to data availability constraints, external or out-of-sample validation of the BAPC projections was not conducted. Future research may benefit from incorporating higher-resolution spatial data and component-specific exposure information, as well as applying backtesting strategies, to improve causal inference and forecasting accuracy.
Conclusion
In conclusion, COPD continues to pose a substantial public health challenge in China, particularly among older adults. Over the past three decades, a general decline in COPD burden has been observed, as reflected by reductions in DALYs and mortality rates. It may reflect disruptions in healthcare access and data collection during the COVID-19 pandemic rather than underlying long-term trends.
Smoking and particulate matter pollution remain important contributors to the development and progression of COPD. Consistent with previous evidence, smoking appears to play a more prominent role among males, while exposure to particulate matter pollution remains a relevant concern for females, potentially reflecting differences in exposure patterns. Projections suggest that although the overall COPD burden is expected to continue declining by 2035, older adults will remain disproportionately affected, and a modest increase in ASMR among males cannot be excluded.
From a public health perspective, these findings highlight the potential value of closer integration between environmental air quality monitoring and clinical COPD surveillance systems to better capture population-level risks. In addition, prevention strategies may benefit from adopting a gender-sensitive approach, including increased attention to indoor PM2.5 exposure among women. Continued efforts in tobacco control, air quality improvement, and access to early diagnosis and management—within the broader framework of initiatives such as “Healthy China 2030”—may contribute to further reductions in COPD burden in the future.
Data Sharing Statement
The data used for the analyses are publicly available from http://ghdx.healthdata.org/gbd-results-tool.
Ethical Approval
No applicable. This study used data derived from the publicly accessible GBD 2021 database. The University of Washington Institutional Review Board granted a waiver of informed consent for GBD studies, as the study relied solely on publicly available data, with no involvement of confidential or personally identifiable information. Therefore, ethical approval was not required.
Acknowledgments
We extend our gratitude to the staff at the Institute for Health Metrics and Evaluation and their collaborators for their contributions.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Supported by the National Natural Science Foundation of China, No. 82571711 and the Natural Science Basis Research Plan in Shaanxi Province of China, No. 2025JC-YBMS-850.
Disclosure
The authors declare that they have no known financial conflicts of interest or personal relationships that could have influenced the work presented in this study.
References
1. Christenson SA. COPD Phenotyping. Resp Care. 2023;68(7):871–14. doi:10.4187/respcare.11035
2. Ritchie AI, Definition WJA. Causes, pathogenesis, and consequences of chronic obstructive pulmonary disease exacerbations. Clin Chest Med. 2020;41(3):421–438. doi:10.1016/j.ccm.2020.06.007
3. Agusti A, Celli BR, Criner GJ, et al. Global initiative for chronic obstructive lung disease 2023 report: GOLD executive summary. Eur Respir J. 2023;61(4):2300239. doi:10.1183/13993003.00239-2023
4. Upadhyay P, Wu CW, Pham A, et al. Animal models and mechanisms of tobacco smoke-induced chronic obstructive pulmonary disease (COPD). J Toxicol Env Heal B. 2023;26(5):275–305. doi:10.1080/10937404.2023.2208886
5. Chen L, Xiong H, Wen Q, et al. The role of active and passive smoking in chronic obstructive pulmonary disease and systemic inflammation: a 12-year prospective study in China. J Epidemiol Glob Hea. 2024;14(3):1332–1340. doi:10.1007/s44197-024-00290-w
6. Sang S, Chu C, Zhang T, Chen H, Yang X. The global burden of disease attributable to ambient fine particulate matter in 204 countries and territories, 1990–2019: a systematic analysis of the Global Burden of Disease Study 2019. Ecotox Environ Safe. 2022;238:113588. doi:10.1016/j.ecoenv.2022.113588
7. Wang Q, Liu S. The effects and pathogenesis of PM2.5 and its components on chronic obstructive pulmonary disease. Int J Chronic Obstr. 2023;18:493–506. doi:10.2147/COPD.S402122
8. Ma Q, Huang D, Zhang H, Wang S, Chen X. Exposure to particulate matter 2.5 (PM2.5) induced macrophage-dependent inflammation, characterized by increased Th1/Th17 cytokine secretion and cytotoxicity. Int Immunopharmacol. 2017;50:139–145. doi:10.1016/j.intimp.2017.06.019
9. Fan X, Dong T, Yan K, Ci X, Peng L. PM2.5 increases susceptibility to acute exacerbation of COPD via NOX4/Nrf2 redox imbalance-mediated mitophagy. Redox Biol. 2023;59:102587. doi:10.1016/j.redox.2022.102587
10. MacIntyre NR. Acute hypercapnic respiratory failure in COPD. Resp Care. 2023;68(7):973–982. doi:10.4187/respcare.10560
11. Suissa S, Dell’Aniello S, Ernst P. Long-term natural history of chronic obstructive pulmonary disease: severe exacerbations and mortality. Thorax. 2012;67(11):957–963. doi:10.1136/thoraxjnl-2011-201518
12. Andre S, Conde B, Fragoso E, Boleo-Tome JP, Areias V, Cardoso J. COPD and Cardiovascular Disease. Pulmonology. 2019;25(3):168–176. doi:10.1016/j.pulmoe.2018.09.006
13. Park SS, Perez PJ, Perez GB, et al. Mechanisms linking COPD to type 1 and 2 diabetes mellitus: is there a relationship between diabetes and COPD? Medicina-Lithuania. 2022;58(8). doi:10.3390/medicina58081030
14. Li M, Hanxiang C, Na Z, et al. Burden of COPD in China and the global from 1990 to 2019: a systematic analysis for the Global Burden of Disease Study 2019. BMJ Open Respir Res. 2023;10(1). doi:10.1136/bmjresp-2023-001698
15. Yin P, Wu J, Wang L, et al. The burden of COPD in China and its provinces: findings from the global burden of disease study 2019. Front Public Health. 2022;10:859499. doi:10.3389/fpubh.2022.859499
16. Wang H, Meng R, Wang X, et al. A nested case-control study of the effects of dust exposure, smoking on COPD in coal workers. Bmc Public Health. 2023;23(1):2056. doi:10.1186/s12889-023-16944-6
17. Fang L, Gao P, Bao H, et al. Chronic obstructive pulmonary disease in China: a nationwide prevalence study. Lancet Resp Med. 2018;6(6):421–430. doi:10.1016/S2213-2600(18)30103-6
18. Adeloye D, Chua S, Lee C, et al. Global and regional estimates of COPD prevalence: systematic review and meta-analysis. J Glob Health. 2015;5(2):020415. doi:10.7189/jogh.05.020415
19. Varshney P, Saini R, Taneja A. Trace element concentration in fine particulate matter (PM2.5) and their bioavailability in different microenvironments in Agra, India: a case study. Environ Geochem Hlth. 2016;38(2):593–605. doi:10.1007/s10653-015-9745-5
20. Offer S, Hartner E, Di Bucchianico S, et al. Effect of atmospheric aging on soot particle toxicity in lung cell models at the air-liquid interface: differential toxicological impacts of biogenic and anthropogenic Secondary Organic Aerosols (SOAs). Environ Health Perspect. 2022;130(2):27003. doi:10.1289/EHP9413
21. Yang J, Kim EK, Park HJ, McDowell A, Kim YK. The impact of bacteria-derived ultrafine dust particles on pulmonary diseases. Exp Mol Med. 2020;52(3):338–347. doi:10.1038/s12276-019-0367-3
22. Parascandola M, Xiao L. Tobacco and the lung cancer epidemic in China. Transl Lung Cancer R. 2019;8(Suppl 1):S21–S30. doi:10.21037/tlcr.2019.03.12
23. Su X, Li H, Li F, et al. Trends in the burden of COPD attributable to ambient PM(2.5) exposure in China 1990–2019: an age-period-cohort analysis. Risk Manag Healthc P. 2023;16:69–77. doi:10.2147/RMHP.S395278
24. Lin H, Chang C, Liu Z, Zheng Y. Subnational smoke-free laws in China. Tob Induc Dis. 2019;17:78. doi:10.18332/tid/112665
25. Hu T, Lee AH, Mao Z. WHO framework convention on tobacco control in China: barriers, challenges and recommendations. Glob Health Promot. 2013;20(4):13–22. doi:10.1177/1757975913501910
26. Expert CTF, Shi X, Duan G. Recommendations of controlling and preventing acute health risks of fine particulate matter pollution - China, 2021. China Cdc Weekly. 2022;4(16):329–341. doi:10.46234/ccdcw2022.078
27. Ejaz H, Alsrhani A, Zafar A, et al. COVID-19 and comorbidities: deleterious impact on infected patients. J Infect Public Heal. 2020;13(12):1833–1839. doi:10.1016/j.jiph.2020.07.014
28. Higham A, Singh D. Increased ACE2 expression in bronchial epithelium of COPD patients who are overweight. Obesity. 2020;28(9):1586–1589. doi:10.1002/oby.22907
29. Halpin D, Criner GJ, Papi A, et al. Global initiative for the diagnosis, management, and prevention of chronic obstructive lung disease. The 2020 GOLD Science Committee Report on COVID-19 and Chronic Obstructive Pulmonary Disease. Am J Resp Crit Care. 2021;203(1):24–36. doi:10.1164/rccm.202009-3533SO
30. Higham A, Mathioudakis A, Vestbo J, Singh D. COVID-19 and COPD: a narrative review of the basic science and clinical outcomes. Eur Respir Rev. 2020;29(158):200199. doi:10.1183/16000617.0199-2020
31. Bagdonas E, Raudoniute J, Bruzauskaite I, Aldonyte R. Novel aspects of pathogenesis and regeneration mechanisms in COPD. Int J Chronic Obstr. 2015;10:995–1013. doi:10.2147/COPD.S82518
32. Jarad N. Chronic obstructive pulmonary disease (COPD) and old age? Chron Resp Dis. 2011;8(2):143–151. doi:10.1177/1479972311407218
33. Hillas G, Perlikos F, Tsiligianni I, Tzanakis N. Managing comorbidities in COPD. Int J Chronic Obstr. 2015;10:95–109. doi:10.2147/COPD.S54473
34. Koskela J, Kilpelainen M, Kupiainen H, et al. Co-morbidities are the key nominators of the health related quality of life in mild and moderate COPD. Bmc Pulm Med. 2014;14:102. doi:10.1186/1471-2466-14-102
35. Barnes PJ, Celli BR. Systemic manifestations and comorbidities of COPD. Eur Respir J. 2009;33(5):1165–1185. doi:10.1183/09031936.00128008
36. Chang JT, Meza R, Levy DT, Arenberg D, Jeon J. Prediction of COPD risk accounting for time-varying smoking exposures. PLoS One. 2021;16(3):e0248535. doi:10.1371/journal.pone.0248535
37. Prasad R, Singh A, Garg R, Giridhar GB. Biomass fuel exposure and respiratory diseases in India. Biosci Trends. 2012;6(5):219–228. doi:10.5582/bst.2012.v6.5.219
38. Goodchild M, Zheng R. Tobacco control and Healthy China 2030. Tob Control. 2019;28(4):409–413. doi:10.1136/tobaccocontrol-2018-054372
39. Guo X, Yang S, Zhu H, et al. Involvement of M2 macrophages polarization in PM2.5-induced COPD by upregulating MMP12 via IL4/STAT6 pathway. Ecotox Environ Safe. 2024;283:116793. doi:10.1016/j.ecoenv.2024.116793
40. Yu H, Lin Y, Zhong Y, et al. Impaired AT2 to AT1 cell transition in PM2.5-induced mouse model of chronic obstructive pulmonary disease. Resp Res. 2022;23(1):70. doi:10.1186/s12931-022-01996-w
41. Chan KH, Xiao D, Zhou M, Peto R, Chen Z. Tobacco control in China. Lancet Public Health. 2023;8(12):e1006–e1015. doi:10.1016/S2468-2667(23)00242-6
42. Schmid R, Xiong X. China’s environmental solutions. Appl Microbiol Biot. 2023;107(4):987–1002. doi:10.1007/s00253-022-12340-z
43. Wang Z, Tan Y, Guo M, et al. Prospect of China’s ambient air quality standards. J Environ Sci. 2023;123:255–269. doi:10.1016/j.jes.2022.03.036
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Health Inequality in the Global Burden of Chronic Obstructive Pulmonary Disease: Findings from the Global Burden of Disease Study 2019
Li H, Liang H, Wei L, Shi D, Su X, Li F, Zhang J, Wang Z
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:1695-1702
Published Date: 28 July 2022
Patients with Chronic Obstructive Pulmonary Disease and Evidence of Eosinophilic Inflammation Experience Exacerbations Despite Receiving Maximal Inhaled Maintenance Therapy
Chen S, Miravitlles M, Rhee CK, Pavord ID, Jones R, Carter V, Emmanuel B, Alacqua M, Price DB
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2187-2200
Published Date: 9 September 2022
Von Willebrand Disease Epidemiology, Burden of Illness and Management: A Systematic Review
Du P, Bergamasco A, Moride Y, Truong Berthoz F, Özen G, Tzivelekis S
Journal of Blood Medicine 2023, 14:189-208
Published Date: 2 March 2023
Global, Regional, and National Burden of COPD Attributable to Occupational Particulate Matter, Gases, and Fumes, 1990–2019: Findings from the Global Burden of Disease Study 2019
Su X, Gu H, Li F, Shi D, Wang Z
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2971-2983
Published Date: 12 December 2023
Frequency of Exacerbations of Chronic Obstructive Pulmonary Disease Associated with the Long-Term Exposure to Air Pollution in the AIREPOC Cohort

Herrera Lopez AB, Torres-Duque CA, Casas Herrera A, Arbeláez MP, Riojas-Rodríguez H, Texcalac-Sangrador JL, Rojas NY, Rodriguez-Villamizar LA
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:425-435
Published Date: 22 February 2025