")
Back to Journals » Patient Related Outcome Measures » Volume 14
Impact of Safinamide on Patient-Reported Outcomes in Parkinson’s Disease
Authors Espinoza-Vinces C , Villino-Rodríguez R, Atorrasagasti-Villar A, Martí-Andrés G, Luquin MR
Received 31 July 2023
Accepted for publication 7 October 2023
Published 10 October 2023 Volume 2023:14 Pages 285—295
DOI https://doi.org/10.2147/PROM.S369590
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Robert Howland
Christian Espinoza-Vinces,1 Rafael Villino-Rodríguez,1 Ainhoa Atorrasagasti-Villar,1 Gloria Martí-Andrés,2 María-Rosario Luquin1
1Department of Neurology, Clínica Universidad de Navarra, Pamplona, Spain; 2Department of Neurology, Hospital Universitario de Navarra, Pamplona, Spain
Correspondence: María-Rosario Luquin, Clínica Universidad de Navarra, Avenida de Pio XII 36, Pamplona, 31008, Spain, Email [email protected]
Introduction: Parkinson’s disease (PD) is a chronic and progressive neurodegenerative condition due to the degeneration of nigral dopaminergic cells. Both motor and non-motor symptoms (NMS) of PD produce a marked impairment in PD patients’ quality of life (QoL), but contrary to motor features, NMS do not improve with dopamine replacement. Novel therapeutic interventions for PD have successfully controlled most motor manifestations of PD, but the management of NMS is still challenging. Since NMS have a negative impact on the QoL of PD patients, researchers are currently looking for drugs that can modulate the activity of neurotransmitter systems other than dopamine in the hope that can alleviate NMS in PD. Among the recently approved drugs for patients experiencing fluctuations in motor symptoms, safinamide stands out as an effective add-on therapy to levodopa. Safinamide is a monoamine oxidase type-B inhibitor (MAOB-I), with proven efficacy in reducing motor fluctuations. Its distinctive mechanism of action impacts dopaminergic pathways via MAOB inhibition and glutamatergic pathways by blocking sodium and calcium channels. Findings from Phase III clinical trials, meta-analysis, post-hoc analysis, and real-life experiences indicate that safinamide benefits motor symptoms such as tremor, bradykinesia, rigidity, and gait. Additionally, it shows promise for improving NMS like fatigue, pain, mood, and sleep disturbances in patients with PD.
Areas Covered: In this article, the authors explore the impact of safinamide on patient-reported outcomes in PD. A thorough search was conducted on PubMed focusing on studies published between 2018 and 2023 in English. The inclusion criteria encompassed clinical trials, randomized controlled trials, systematic reviews, meta-analyses, and reviews. The search strategy revolved around the implementation of MeSH terms related to safinamide and its impact on the quality of life in PD.
Conclusion: Our data strongly support the improving effect on QoL, reducing the disabling NMS reported in patients with PD.
Keywords: safinamide, Parkinson’s disease, non-motor symptoms, monoamine oxidase inhibitors
Introduction
Parkinson’s disease (PD) is the second-most frequent neurodegenerative disorder after Alzheimer’s disease. It is characterized by the progressive loss of the pigmented dopamine-producing neurons of the midbrain, leading to a marked decrease in the striatal dopamine content. The main cardinal features of PD include resting tremor, rigidity, and bradykinesia while balance and postural impairment usually appear later in the course of the disease. Protein deposits of aggregated forms of α-synuclein in neuronal cytoplasm (Lewy bodies) and neuronal process (Lewy neurites) are the hallmarks of the disease. Interestingly, it has been suggested that misfolded α -synuclein protein might spread either from peripheral structures (for instance, form the gastrointestinal tract) to the medulla and neocortex (body first phenotype) or from the amygdala to peripheral structures (brain first phenotype).1 In both circumstances α -synuclein deposits reach substantia nigra neurons, resulting in dopamine cell death, decreased striatal dopamine content, and ultimately the appearance of the PD symptoms.
NMS are very common in PD patients. Although they frequently develop prior to the occurrence of the motor manifestations of the disease, they are much more common in the advanced stages, particularly when motor fluctuations appear.2 NMS in PD include neuropsychiatric features like anxiety, apathy, and depression, pain, fatigue, olfactory impairment, autonomic dysfunction, and sleep and cognitive disturbances.3 Increasing evidence is showing that in addition to the degeneration of nigrostriatal dopaminergic neurons, dysfunction of other neurotransmitter systems seems to be implicated in the pathophysiology of the disease, and they appear to massively contribute to the appearance of NMS. For instance, depression, anxiety, fatigue, sleep, and cognitive impairment have been ascribed to serotonin and cholinergic dysfunction.4 This fact might account for the lack of response of NMS to dopamine replacement and targeting non-dopaminergic systems might be a good strategy to control NMS in PD. Thus, it is plausible that drugs acting on dopamine and non-dopamine systems might alleviate NMS. On the other hand, it is unknown the relevance of α -synuclein protein deposits in structures outside the substantia nigra (both in the central and peripheral nervous system) in the development of the NMS, and it would be interesting to know if the use monoclonal anti-a-synuclein antibodies can be of value in the control of the NMS.
Numerous studies have reported the contribution of NMS to the deterioration of health-related-quality of life (HRQoL) which the World Health Organization defines as “the individual perception and evaluation by patients themselves of the impact caused on their lives by the disease and its consequences”.5 In the last two decades, NMS have proven to be an essential part of the PD phenomenology and have been established as the major determinant of worse HRQoL. Contrary to initial reports that indicated that HRQoL and health care in PD were associated with motor symptoms severity and motor fluctuations, more recent evidence suggests a close relationship between NMS frequency and severity and HRQoL as a whole. The PRIAMO study (Barone et al, 2009) is the largest study (826 PD patients were enrolled) that investigated the relationship between NMS and HRQoL and found that apathy was associated with worse HRQoL, followed by cardiovascular symptoms, fatigue, attention/memory, and respiratory symptoms.5 Subsequent studies identified the neuropsychiatric symptoms (apathy, depression) as the most important independent factor of HRQoL. In addition, longitudinal studies have demonstrated that the non-motor burden significantly progresses over time and considerably affects QoL.
More recently, Bock et al performed a cross-sectional analysis enrolling 23,058 PD patients and conducted a univariate and stepwise multivariate linear regression analysis of HRQoL. They found that patients with more moderate and severe depression, more severe motor symptoms, and higher burden of medical comorbidities had the most substantially decreased HRQoL.6 Another study that included 689 PD patients from the cohort of Patients with Parkinson Disease in Spain (COPADIS) described that the NMS are closely associated with mobility, emotional well-being, and cognition. In addition, the most influential NMS were found to be fatigue, feeling sad, hyperhidrosis, impaired concentration, and daytime sleepiness. All these data clearly indicate that NMS have a negative impact on the HRQoL of PD patients and could lead to major functional impairment than motor symptoms by themselves.7 Thus, improvement of NMS should be considered a major outcome variable in clinical trials. Most clinical trials in PD have been designed to assess the effect of a specific drug on controlling motor symptoms of the disease. However, numerous studies do not reflect the relevance of the motor improvement in HRQoL which is the most determinant feature for PD patients and caregivers’ well-being. In addition, despite the large number of studies indicating that NMS are crucial determinants of PD HRQoL, NMS management remains challenging, and few randomized clinical trials have been focused on this issue. Thus, there is an urgent need for developing new drugs or strategies that can improve the NMS of PD since their presence is the major determinant of HRQoL in PD.
Here we review the impact of safinamide, a reversible MAO-B inhibitor, on patient-reported outcomes. Since modification in NMS seems to be the best determinant of patient-outcome we have focused on reviewing the effect of safinamide on HRQoL and NMS.
Safinamide: General Characteristics
Safinamide is an orally administered α-aminoamide derivative that combines potent, selective, and reversible inhibition of monoamine oxidase (MAO)-B with blockade of voltage-dependent Na+ (VSCCs) and Ca2+ (VSCCs) channels and inhibition of glutamate release, thus targeting both dopaminergic and glutaminergic systems. Consequently, safinamide is the prototype of new generation MAO-B inhibitors approved as an add-on to levodopa in PD patients experiencing motor fluctuations. Two doses of safinamide are available, 50 and 100 mg, which display a similar inhibitory effect on MAO-B activity. However, safinamide at doses of 100 mg also blocks VSSCs and VSCCs thus inhibiting glutamate transmission at overactive synapsis and reducing the excitatory overdrive in the basal ganglia motor circuits. Based on these properties, safinamide was initially developed as an antiepileptic drug. More recently, its anti-glutamatergic action has been associated with the reduction of the dyskinesia rating scale reported in a subgroup of PD patients with moderate-severe dyskinesia. These findings indicate that the anti-glutamatergic activity created by high doses of safinamide might be used for the management of levodopa-induced dyskinesia. In fact, safinamide might reduce the excessive glutamate release, created by dopamine depletion in the direct strio-pallidal pathway, which seems to underlie levodopa-induced dyskinesia. Interestingly, excessive glutamate transmission also negatively influences on several NMS of the disease, particularly cognitive, neuropsychiatric, and sensory features, and in these circumstances; in addition to motor improvement safinamide might exert a beneficial effect on these symptoms.8
The reversibility of safinamide represents an important advantage since the unspecific inhibition of MAO-B leads to un-metabolized dietary amines entering the bloodstream, where they produce noradrenaline release from peripheral adrenergic neurons, leading to a potentially fatal hypertensive response. Therefore, to avoid such effects, MAO-B selective inhibitors, such as safinamide, are essential for the treatment of PD.9 Furthermore, MAO-B inhibition is also fully reversible, as it does not form irreversible covalent bonds with MAO-B, unlike rasagiline and selegiline.9
Safinamide is a small, water-soluble molecule that is rapidly absorbed with a half-life of approximately 21–24 hours, which allows for once-daily administration. Safinamide it is not metabolized by CYP450, thus avoiding significant drug interactions. The drug is metabolized by MAOA and amine hydrolases into pharmacologically inert acidic and N-dealkylated products.8
Studies in animal PD models have demonstrated that brain levels of safinamide are higher than the corresponding plasma concentrations, indicating that there is a significant biotransformation of the drug. This is further supported by the very low concentrations of unchanged safinamide found in feces and urine. The drug exhibits a plasma protein binding of 92%, and only a small proportion is excreted unchanged.10
Safinamide has the potential for drug interactions and requires certain precautions. Concurrent use of specific opioids and antidepressants may increase the risk of developing serotonin syndrome. Safinamide should not be given to patients with uveitis and retinopathy due to the reported retinal degeneration in animal studies.11
The efficacy and safety profile of safinamide have been confirmed in a recent multicentric cohort study (SYNAPSES trial) and in elderly people.12 Safinamide has demonstrated good tolerability in various randomized, controlled, and observational trials. Most adverse events are related to its dopaminergic activity and are common with other dopaminergic drugs.
Methods
To gather relevant information, a thorough search was conducted on PubMed, focusing on studies published between 2018 and 2023 in English.
The search strategy revolved around the implementation of MeSH terms related to safinamide and its impact on the quality of life (QoL) in PD. For further insights, see Table 1, which provides a comprehensive overview of the search strategy employed.
 |
Table 1 Details of the Search Strategies |
The inclusion criteria encompassed clinical trials, randomized controlled trials, systematic reviews, meta-analyses, and reviews. Detailed information about the studies is shown in Table 2.
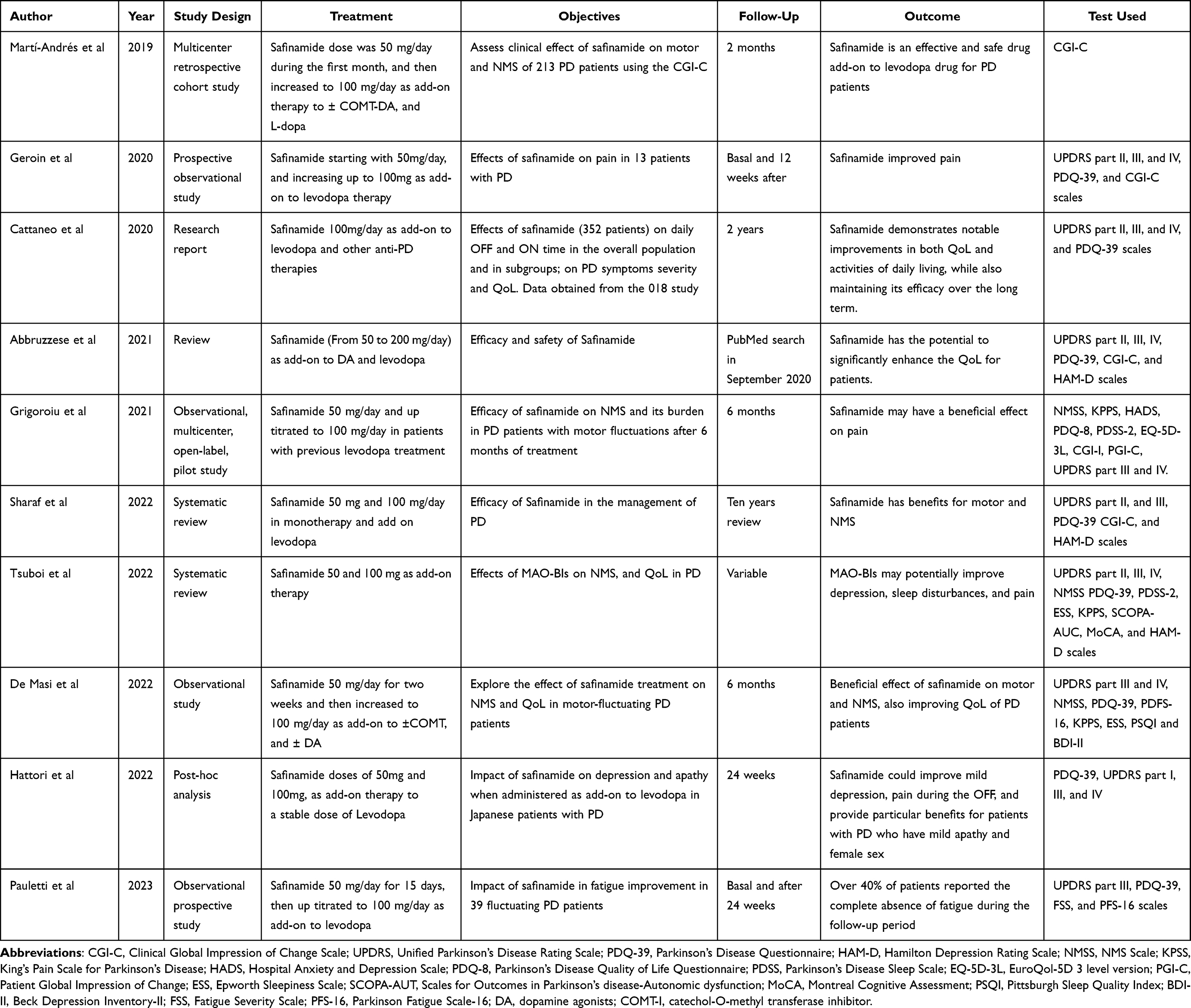 |
Table 2 Characteristics and Results of the Studies Included in This Review |
Safinamide and Motor Fluctuations
Most randomized controlled studies have consistently demonstrated that safinamide as an add-on therapy provides a substantial and maintained increase in the daily on time without troublesome dyskinesia in PD patients with motor fluctuations. In addition, in a retrospective analysis, Martí et al described an improvement in motor (80.4%) and NMS (32.5%) assessed by the CGI-C scale in PD patients after switching from rasagiline to safinamide, indicating that safinamide could elicit an additional motor benefit in PD patients treated with rasagiline and suboptimal motor control.13
A recent meta-analysis reported that safinamide as an add-on therapy to levodopa improved motor fluctuations in PD, with favorable tolerability and good adherence to treatment. The analysis assessed the impact of safinamide using three quantifiable measures: daily “on-time without troublesome dyskinesia”, daily “off-time”, and modifications in the UPDRS part III score. Notably, at 100 mg per day, safinamide elicited a significant improvement in all three parameters.14 These findings provide additional evidence to support the effectiveness of safinamide in managing motor fluctuations in PD.15 Considering the significant impact of motor fluctuations on patients’ QoL evaluation, safinamide seems to be a good strategy for treating PD patients in the early and advanced stages of the disease.
Effect of Safinamide on Non-Motor Symptoms
NMS encompass a variety of conditions such as depression, psychosis, apathy, pain, sleep disorders, and urinary dysfunction.15 These symptoms are considered inherent to the disease, but in some cases, can be exacerbated by dopaminergic treatment. They are not easily recognized in the clinical practice, particularly by general neurologist practitioners and their treatment is challenging.16 Due to the NMS’s impact on the QoL of patients, most clinical trials include changes the NMS scale as a major primary clinical outcome.
One of the most commonly used scales for NMS in PD is the NMSS. It evaluates a wide range of NMS categorized into nine domains: cardiovascular (2 items), sleep/fatigue (4 items), mood/cognition (6 items), perceptual problems/hallucinations (3 items), attention/memory (3 items), gastrointestinal tract (3 items), urinary (3 items), sexual function (2 items), and miscellaneous (4 items).17
The observational VALE-SAFI study reported that safinamide produced a marked and sustained decrease in the NMS global score among PD patients, along with a significant decrease in the PDQ-39 global score, indicating an enhancement in PD patients’ overall QoL.18 Furthermore, it was observed that safinamide, even at the dose of 50 mg/day and reinforced at 100 mg/day, exhibited improvements in specific NMS such as pain, sleep disorders, and mood, whether associated with or independent of motor fluctuations.19
Effect of Safinamide on Quality of Life
Extensive investigation has assessed the effectiveness of safinamide in improving various aspects of QoL in patients with PD. The assessment of HRQoL in PD can be accomplished using the UPDRS part II scale and the PDQ-39 summary index score.20 The PDQ-39 is a patient-reported outcome measure that specifically targets the disease and comprises 39 questions covering eight health dimensions: mobility, activities of daily living, emotional well-being, stigma, social support, cognition, communication, and bodily pain.21 It is widely recognized as the most extensively utilized questionnaires for evaluating HRQoL in PD and provides valuable insights into the severity of NMS, which is known to have a negative impact on HRQoL. Additionally, PDQ39 questionnaries’ can be used to monitor the patient’s response to specific treatment and disease progression.20
In a meta-analysis, Abdelalem et al found that safinamide was superior to placebo in enhancing the QoL of PD patients. This improvement was demonstrated using different tools, including the UPDRS II scale, the PDQ-39 questionnaire, HAM-D, and the Mini-Mental State Examination (MMSE).14
Similarly, Giossi et al reported an increased PDQ-39 score in PD patients receiving 100 mg of safinamide.22 Furthermore, Borgohain et al documented highlighting improvements in the PDQ-39 score and other QoL measures such as emotional well-being, communication, and physical comfort after adding 100 mg per day of safinamide compared to placebo.23 In the study performed by Cattaneo et al involving 352 patients, the effect of safinamide added to levodopa on daily OFF and ON times was assessed. In this study, patients treated with safinamide showed a significant improvement in the PDQ39 summary index score with a −4.07 point score reduction, while the reduction in the placebo group was −1.03 points.20 Finally, Martí-Andrés et al enrolled 213 patients diagnosed with PD and observed a significant improvement (76.4%) in the CGI-C score when evaluating the impact of safinamide on both motor symptoms and NMS as a whole. Regarding NMS, there were no statistically significant differences in CGI-C scores among the final doses of safinamide (determined through Fisher exact test, p = 0.139); however, it is important to note that this study was conducted retrospectively. The authors concluded that safinamide is an effective and safe addition to levodopa therapy in PD, supporting patients’ optimal adherence to treatment in real-world scenarios.13
Effect of Safinamide on Neuropsychiatric Symptoms
Among neuropsychiatric manifestations, depression, anxiety, and cognitive decline are the more frequent and disabling NMS of the disease. They occur at every stage of the disease, but are more prevalent in advanced stages. Depression affects more than 80% of the patient population and, as reflected by numerous studies, has a highly negative impact on patients’ QoL. Results from numerous clinical trials indicate that dopamine replacement elicits a marginal improvement in depression scores in PD patients. In addition, molecular neuroimaging techniques with Positron Emission Tomography (PET) have revealed that depression in PD is characterized by an upregulation of serotonergic receptors (SER) in specific structures of the brainstem and limbic system; which reflects a lower availability of serotonin in the synaptic cleft that may have some influence in the pathophysiology of this symptom in PD patients.24 The MAO-B inhibitor rasagiline failed to improve depressive symptoms in PD patients without cognitive dysfunction, thus further supporting the notion that in PD, dopamine is not involved in depression and warranting the use of drugs acting on other neurotransmitter system to control depression in these patients.25
Interestingly, in addition to enhancing the striatal dopamine content, safinamide has the potential to modulate glutamate release from the cortico-striatal pathway, and hypothetically might contribute to alleviating depressive symptoms.26 Furthermore, anxiety, another commonly observed NMS in PD with a significant impact on QoL, might share a similar pathophysiological mechanism as depression.
In a systematic review and meta-analysis, Abdelalem et al showed that safinamide was superior to placebo in improving the HAM-D scale, a score widely used for assessing depressive symptoms in most settings.14 These results were, subsequently confirmed by Borgohain in a similar study, with safinamide superior to placebo in increasing HAM-D scores over a 24-week period.23
The 016 and 018 (extension study) studies showed the superiority of safinamide in comparison to placebo regarding the HAM-D scores and the emotional well-being subscore of the PDQ-39.27 However, Borgohain et al reported that these benefits were evident with 100 mg of safinamide but not with lower doses.23 Furthermore, a post hoc analysis of the 016 and 018 studies confirmed a clear effect of 100 mg of safinamide on depression.27
Hattori et al did a post-hoc analysis of data from II and III-phase clinical trials, and reported that safinamide exhibited significant improvement in patients with PD experiencing wearing-off symptoms, regardless of whether they received the 50 mg or 100 mg dose.28 The initial study focused on evaluating changes in the UPDRS Part I item 3 score (depression) and item 4 (apathy), as well as the PDQ-39” emotional well-being.29 Notably, reductions in depression were associated with changes in daily ON-time of at least 1 hour, the presence of pain during the OFF-time at baseline, and female sex.28
Several studies have described that cognitive dysfunction in PD is due to cholinergic neurotransmitter impairment.30 This fact might account for the lack of cognitive improvement after imitating levodopa therapy and explain the cognitive benefit provided by cholinesterase inhibitors like rivastigmine. On the other hand, there is some evidence that has described improvement of frontal executive functions in PD patients with mild cognitive impairment under rasagiline therapy, but the rest of the cognitive domains remained unchanged. These results were explained by the increased frontal dopamine content created by rasagiline.
De Micco et al assessed the effect of 50 mg of safinamide on cognitive and behavioral symptoms over a 6-month period of treatment. Safinamide induced benefit was assessed by changes in the MoCA score range (0–30 points) and the PD Cognitive Rating Scale (PD-CRS) score range (0–134 points) that evaluate global cognitive functioning. However, the results of neuropsychological evaluations did not indicate any significant changes in global cognitive functioning or the five cognitive subdomains when comparing the follow-up period to the baseline assessment.16
Additionally, the results from the VALE-SAFI study in PD patients indicated that safinamide improves the irritability component accompanying the depressive episodes.18
Effect of Safinamide on Pain
Pain is a frequent complaint among individuals with PD.26 It is very frequently observed in fluctuating PD patients during OFF periods, and in these circumstances, it improves with strategies that provide more continuous dopamine stimulation (studio recover with rotigotine).31 However, other central dopamine-independent mechanisms can be involved in the appearance of pain. Safinamide has been recognized for its analgesic properties, which are attributed to its dual modulation of dopaminergic and glutaminergic pathways.32
A comprehensive systematic review and meta-analysis have evaluated the analgesic benefit of several PD therapies, including safinamide, cannabinoids, COMT inhibitors, dopaminergic agonists, and others, and concluded that safinamide was superior to other treatments for relieving pain in PD.33
In a study conducted by Geroin et al involving 13 patients, safinamide significantly reduced pain as assessed by various measures, including the KPPS, Brief Pain Inventory (BPI) intensity and interference, and Numeric Rating Scale (NRS). A notable proportion of patients (7 out of 13) exhibited a responder status with an NRS improvement of more than 50%.34
Similar results were observed in the study by Grigoriou et al where a wide range of NMS, including pain, were assessed, and it was found that safinamide significantly reduced the KPPS score.35 Pain improvement was also described in the post-hoc analysis of several clinical trials.20
In a large double-blind, placebo-controlled randomized controlled trial (RCT), advanced PD patients receiving safinamide 100 mg demonstrated significant amelioration of pain compared to placebo based on the PDQ-39 bodily discomfort subscore.23 Additional open-label studies also reported positive outcomes based on the KPPS, indicating that safinamide 100 mg improves fluctuation-related pain.36 All these data indicate that safinamide improve pain in PD patients, probably due to a central mechanism linked to the modulation of calcium channel activity induced by safinamide.
Effect of Safinamide on Fatigue
Fatigue is characterized by a profound lack of energy and increased effort for performing common daily activities, it is one of the most common and disabling NMS of PD, and it is independent of others like apathy and sleep disorders.37 Up to 37% of de novo PD patients and 50% of treated PD subjects suffer from fatigue. The severity of the disease, but not the degree of decreased striatal tracer uptake in the DAT-scan imaging, are associated with fatigue scores. Functional neuroimaging PET studies using the serotonin tracer 11C-DASB have reported decreased tracer binding in the striatum and limbic structures in PD patients with fatigue as compared with controls and no fatigue PD patients. However, both groups of PD patients exhibit similar decreased striatal uptake in the F-dopa PET, and dopamine replacement does not improve fatigue in PD patients.38 All these data do not support the role of dopamine in the genesis of fatigue. However, a sub-analysis of the ADAGIO study that enrolled 1105 early PD patients demonstrated that the MAOB inhibitor rasagiline (1 and 2 mg) produced a lower deterioration of PFS scores than placebo. As motor scores and motor fluctuations also improved in the rasagiline treated arm, the effect on fatigue has been attributed to the better motor outcome of the rasagiline-treated patients.39
Pauletti et al assessed the benefit of safinamide as an add-on therapy for fatigue. They included 39 PD patients experiencing fatigue and motor fluctuations. The study found a significant improvement in fatigue scores after 24 weeks of safinamide treatment. Both FSS (pre: 5.1 ± 1.4, post: 4.2 ± 1.6; p < 0.001) and PFS-16 (pre: 3.5±0.9, post: 3.2±0.9; p=0.02) were significantly reduced.40 Furthermore, this study reported that the beneficial effect on fatigue was maintained for at least 6 months. Remarkably, over 40% of patients experienced a complete absence of fatigue at follow-up, suggesting that drugs like safinamide, which interact with multiple neurotransmission systems, have the potential to reduce this symptom and improve QoL. The multifactorial nature of PD-related fatigue suggests that dysfunction in the glutamatergic system may be a contributing factor to its development.40
Similar results found by De Micco et al who described a significant alleviation of fatigue when safinamide was added. The study demonstrated a large effect size, indicating the positive impact of safinamide on fatigue levels in PD patients.16
Additionally, the outcomes of the SAFINONMOTOR study supported the effectiveness of safinamide in improving fatigue scores in PD patients.41 Consequently, safinamide holds promise as a potential treatment option for managing fatigue in individuals with PD.
Effect of Safinamide on Sleep
Sleep disturbances are a prevalent and troubling NMS experienced by individuals with PD. These disturbances can manifest at any stage of the disease, but typically worsen as the disease progresses and exert an undesirable impact on the QoL of individuals with moderate and advanced stages of the disease.42
In the VALE SAFI study, De Masi et al examined sleep quality using the PSQI, a questionnaire consisting of 19 self-assessment questions that collectively form 7 component scores. These components include subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleeping medication, and daytime dysfunction. The study revealed a significant decrease in the global score of the PSQI from baseline to follow-up, indicating an improvement in sleep quality.18
SAFINONMOTOR was a groundbreaking prospective study designed to evaluate the impact of safinamide on sleep quality and daytime sleepiness, as well as on NMS. The study proved that after one month of safinamide treatment at a dosage of 50 mg/day, significantly improved both sleep and daytime sleepiness. However, no additional improvement was observed with a higher dosage (100 mg/day).43
Finally, Liguori et al, studied the effects of safinamide on patients’ sleep quality and daytime sleepiness using the PDSS2, PSQI, and ESS. They showed a significant reduction in PDSS2 and ESS scores in patients treated by safinamide.44
Effect of Safinamide on Autonomic Dysfunction
Autonomic dysfunction is manifested by excessive sweating, orthostatic hypotension, and urinary or sexual symptoms. It is particularly prevalent and more pronounced in advanced stages of the disease, although some authors consider that these symptoms could be the first manifestation of the disease, and can precede the motor manifestations of the disease.45 The prevalence of these symptoms varies along the course of the disease, with a higher frequency in advanced stages (ranging from 24% to 96%).46 Among these symptoms, nocturia is the most commonly reported in individuals with PD, and has a marked impact on sleep quality and daily functioning.45
In 2021, a small retrospective study examined the impact of safinamide on urological symptoms in PD patients and found that safinamide as an add-on therapy led to improvements in urological symptoms.47
In a small single-center, open-label, prospective study conducted on advanced PD patients, safinamide 50 mg demonstrated improvements in overall autonomic symptoms based on the SCOPA-AUT after 6 months.16
Similarly, a large single-center, open-label, retrospective study revealed that safinamide 100 mg reduced the urinary problems subscore of the SCOPA-AUT scale after 3 months.47
Furthermore, in a multicenter, open-label, prospective study focusing on PD patients with a high non-motor burden, safinamide 100 mg showed positive effects on autonomic symptoms as assessed by the subscore of the NMSS.36
Conclusion
Data from the literature strongly indicate that, in addition to the improvement of motor fluctuations, safinamide markedly reduces the intensity of NMS particularly depression, apathy, and fatigue and to a lesser extent, sleep quality, which negatively influence the QoL in PD patients. The central dopaminergic and glutamatergic effects produced by safinamide might account for the alleviation of NMS in PD subjects. However, although some of the clinical benefits observed in PD patients taking safinamide have been attributed to its glutamatergic effect, more clinical research is required to confirm the usefulness of safinamide in the control of NMS and the mechanism underlying this effect. In summary, based on the data published in the literature safinamide might be the best option for PD with motor fluctuations and NMS. It remains unclear whether safinamide can be given to de novo PD patients with a high NMS burden.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Horsager J, Andersen KB, Knudsen K, et al. Brain-first versus body-first Parkinson’s disease: a multimodal imaging case-control study. Brain. 2020;143(10):3077–3088. doi:10.1093/brain/awaa238
2. Poewe W, Seppi K, Tanner CM, et al. Parkinson disease. Nat Rev Dis Prim. 2017;3(1):17013. doi:10.1038/nrdp.2017.13
3. LeWitt PA, Chaudhuri KR. Unmet needs in Parkinson disease: motor and non-motor. Parkinsonism Relat Disord. 2020;80(Suppl 1):S7–S12. doi:10.1016/j.parkreldis.2020.09.024
4. Titova N, Simon CP, Ray JGLK, Chaudhuri KR. Parkinson’s: a syndrome rather than a disease? J Neural Transm. 2017;124(8):907–914. doi:10.1007/s00702-016-1667-6
5. Barone P, Antonini A, Colosimo C, et al. The PRIAMO study: a multicenter assessment of nonmotor symptoms and their impact on quality of life in Parkinson’s disease. Mov Disord. 2009;24(11):1641–1649. doi:10.1002/mds.22643
6. Bock MA, Brown EG, Zhang L, Tanner C. Association of motor and nonmotor symptoms with health-related quality of life in a large online cohort of people with Parkinson disease. Neurology. 2022;98(22):E2194–E2203. doi:10.1212/WNL.0000000000200113
7. Santos-García D, Mir P, Cubo E, et al. COPPADIS-2015 (COhort of Patients with Parkinson’s disease in Spain, 2015), a global -clinical evaluations, serum biomarkers, genetic studies and neuroimaging- prospective, multicenter, non-interventional, long-term study on Parkinson’s disease progression. BMC Neurol. 2016;16(1):1–14. doi:10.1186/s12883-016-0548-9
8. Alborghetti M, Bianchini E, Carolis L, De Galli S, Pontieri FE, Rinaldi D. Type-B monoamine oxidase inhibitors in neurological diseases: clinical applications based on preclinical findings. Neural Regen Res. 2024;19(1):16–21. doi:10.4103/1673-5374.375299
9. Teixeira FG, Gago MF, Marques P, et al. Safinamide: a new hope for Parkinson’s disease? Drug Discov Today. 2018;23(3):736–744. doi:10.1016/j.drudis.2018.01.033
10. Stocchi F, Torti M. Adjuvant therapies for Parkinson’s disease: critical evaluation of safinamide. Drug Des Devel Ther. 2016;10:609–618. doi:10.2147/DDDT.S77749
11. Jamshidi N, Dawson A. The hot patient: acute drug-induced hyperthermia. Aust Prescr. 2019;42(1):24–28. doi:10.18773/austprescr.2019.006
12. Abbruzzese G, Kulisevsky J, Bergmans B, Gomez-esteban JC. A European observational study to evaluate the safety and the effectiveness of safinamide in routine clinical practice: the SYNAPSES trial 1. J Parkinsons Dis. 2021;11(1):187–198. doi:10.3233/JPD-202224
13. Martí-Andrés G, Jiménez-Bolaños R, Arbelo-González JM, et al. Safinamide in clinical practice: a Spanish multicenter cohort study. Brain Sci. 2019;9(10):1–11. doi:10.3390/brainsci9100272
14. Abdelalem Aziz Ahmed M. A systematic review and meta-analysis of safety and efficacy of safinamide for motor fluctuations in patients with Parkinson’s disease. F1000Research. 2019;8:2078. doi:10.12688/f1000research.21372.1
15. Schapira AHV, Fox SH, Hauser RA, et al. Assessment of safety and efficacy of safinamide as a levodopa adjunct in patients with Parkinson disease and motor fluctuations a randomized clinical trial. JAMA Neurol. 2017;74(2):216–224. doi:10.1001/jamaneurol.2016.4467
16. De Micco R, Satolli S, Siciliano M, et al. Effects of safinamide on non-motor, cognitive, and behavioral symptoms in fluctuating Parkinson’s disease patients: a prospective longitudinal study. Neurol Sci. 2022;43(1):357–364. doi:10.1007/s10072-021-05324-w
17. Cova I, Di Battista ME, Vanacore N, et al. Validation of the Italian version of the non motor symptoms scale for Parkinson’s disease. Park Relat Disord. 2017;34:38–42. doi:10.1016/j.parkreldis.2016.10.020
18. De Masi C, Liguori C, Spanetta M, et al. Non-motor symptoms burden in motor-fluctuating patients with Parkinson’s disease may be alleviated by safinamide: the VALE-SAFI study. J Neural Transm. 2022;129(11):1331–1338. doi:10.1007/s00702-022-02538-w
19. Abbruzzese G, Barone P, Lopiano L, Stocchi F. The current evidence for the use of safinamide for the treatment of Parkinson’s disease. Drug Des Devel Ther. 2021;15:2507–2517. doi:10.2147/DDDT.S302673
20. Cattaneo C, Jost WH, Bonizzoni E. Long-term efficacy of safinamide on symptoms severity and quality of life in fluctuating Parkinson’s disease patients. J Parkinsons Dis. 2020;10(1):89–97. doi:10.3233/JPD-191765
21. Hagell P, Nilsson MH. The 39-item Parkinson’s Disease Questionnaire (PDQ-39): is it a unidimensional construct ? Ther Adv Neurol Disord. 2009;2(4):205–214. doi:10.1177/1756285609103726
22. Giossi R, Carrara F, Mazzari M, et al. Overall efficacy and safety of safinamide in Parkinson’s disease: a systematic review and a meta-analysis. Clin Drug Investig. 2021;41(4):321–339. doi:10.1007/s40261-021-01011-y
23. Borgohain R, Szasz J, Stanzione P, et al. Randomized trial of safinamide add-on to levodopa in Parkinson’s disease with motor fluctuations. Mov Disord. 2014;29(2):229–237. doi:10.1002/mds.25751
24. Maillet A, Krack P, Pelissier P, et al. The prominent role of serotonergic degeneration in apathy, anxiety and depression in de novo Parkinson’s disease. Brain. 2016;139(9):2486–2502. doi:10.1093/aww190
25. Weintraub D, Hauser RA, Elm JJ, et al. Rasagiline for mild cognitive impairment in Parkinson’s disease: a placebo-controlled trial. Mov Disorders. 2016;31(5):709–714. doi:10.1002/mds.26617
26. Sharaf J, Williams KAD, Tariq M, et al. The efficacy of safinamide in the management of Parkinson’s disease: a systematic review. Cureus. 2022;14(9). doi:10.7759/cureus.29118
27. Cattaneo C, Müller T, Bonizzoni E, Lazzeri G, Kottakis I, Keywood C. Long-term effects of safinamide on mood fluctuations in Parkinson’s disease. J Parkinsons Dis. 2017;7(4):629–634. doi:10.3233/JPD-171143
28. Hattori N, Kogo Y, Koebis M, et al. The effects of safinamide adjunct therapy on depression and apathy in patients with Parkinson’s Disease: post-hoc Analysis of a Japanese Phase 2/3 Study. Front Neurol. 2022;12. doi:10.3389/fneur.2021.752632
29. Hattori N, Tsuboi Y, Yamamoto A, Sasagawa Y, Nomoto M. Efficacy and safety of safinamide as an add-on therapy to L-DOPA for patients with Parkinson’s disease: a randomized, double-blind, placebo-controlled, phase II/III study. Park Relat Disord. 2020;75:17–23. doi:10.1016/j.parkreldis.2020.04.012
30. Shimada H, Hirano S, Shinotoh H, et al. Mapping of brain acetylcholinesterase alterations in Lewy body disease by PET. Neurology. 2009;73(4):273 LP- 278. doi:10.1212/WNL.0b013e3181ab2b58
31. Ray Chaudhuri K, Martinez-Martin P, Antonini A, et al. Rotigotine and specific non-motor symptoms of Parkinson’s disease: post hoc analysis of RECOVER. Parkinsonism Relat Disord. 2013;19(7):660–665. doi:10.1016/j.parkreldis.2013.02.018
32. Blair HA, Dhillon S. Safinamide: a review in Parkinson’s disease. CNS Drugs. 2017;31(2):169–176. doi:10.1007/s40263-017-0408-1
33. Stocchi F, Antonini A, Berg D, et al. Safinamide in the treatment pathway of Parkinson’s disease: a European Delphi Consensus. Npj Park Dis. 2022;8(1). doi:10.1038/s41531-022-00277-z
34. Geroin C, Di Vico IA, Squintani G, Segatti A, Bovi T, Tinazzi M. Effects of safinamide on pain in Parkinson’s disease with motor fluctuations: an exploratory study. J Neural Transm. 2020;127(8):1143–1152. doi:10.1007/s00702-020-02218-7
35. Grigoriou S, Martínez-Martín P, Ray Chaudhuri K, et al. Effects of safinamide on pain in patients with fluctuating Parkinson’s disease. Brain Behav. 2021;11(10):1–9. doi:10.1002/brb3.2336
36. García DS, Guerra CL, Baña RY, et al. Safinamide improves non‐motor symptoms burden in Parkinson’s disease: an open‐label prospective study. Brain Sci. 2021;11(3):1–15. doi:10.3390/brainsci11030316
37. Siciliano M, Kluger B, De Micco R, et al. Validation of new diagnostic criteria for fatigue in patients with Parkinson disease. Eur J Neurol. 2022;29(9):2631–2638. doi:10.1111/ene.15411
38. Pavese N, Metta V, Bose SK, Chaudhuri KR, Brooks DJ. Fatigue in Parkinson’s disease is linked to striatal and limbic serotonergic dysfunction. Brain. 2010;133(11):3434–3443. doi:10.1093/brain/awq268
39. Rascol O, Fitzer-Attas CJ, Hauser R, et al. A double-blind, delayed-start trial of rasagiline in Parkinson’s disease (the ADAGIO study): prespecified and post-hoc analyses of the need for additional therapies, changes in UPDRS scores, and non-motor outcomes. Lancet Neurol. 2011;10(5):415–423. doi:10.1016/S1474-4422(11)70073-4
40. Pauletti C, Locuratolo N, Mannarelli D, et al. Fatigue in fluctuating Parkinson’s disease patients: possible impact of safinamide. J Neural Transm. 2023;130(7):915–923. doi:10.1007/s00702-023-02654-1
41. Qureshi AR, Rana AQ, Malik SH, et al. Comprehensive examination of therapies for pain in Parkinson’s disease: a systematic review and meta-analysis. Neuroendocrinology. 2018;51(3–4):190–206. doi:10.1159/000492221
42. Neikrug AB, Maglione JE, Liu L, et al. Effects of sleep disorders on the non-motor symptoms of Parkinson disease. J Clin Sleep Med. 2013;9(11):1119–1129. doi:10.5664/jcsm.3148
43. Santos García D, Cabo López I, Labandeira Guerra C, et al. Safinamide improves sleep and daytime sleepiness in Parkinson’s disease: results from the SAFINONMOTOR study. Neurol Sci. 2022;43(4):2537–2544. doi:10.1007/s10072-021-05607-2
44. Liguori C, Stefani A, Ruffini R, Mercuri NB, Pierantozzi M. Safinamide effect on sleep disturbances and daytime sleepiness in motor fluctuating Parkinson’s disease patients: a validated questionnaires-controlled study. Park Relat Disord. 2018;57:80–81. doi:10.1016/j.parkreldis.2018.06.033
45. Batla A, Phé V, De Min L, Panicker JN. Nocturia in Parkinson’s disease: why does it occur and how to manage? Mov Disord Clin Pract. 2016;3(5):443–451. doi:10.1002/mdc3.12374
46. Jost WH. Urological problems in Parkinson’s disease: clinical aspects. J Neural Transm. 2013;120(4):587–591. doi:10.1007/s00702-012-0914-8
47. Gómez-López A, Sánchez-Sánchez A, Natera-Villalba E, et al. Surinpark: safinamide for urinary symptoms in Parkinson’s disease. Brain Sci. 2021;11(1):1–8. doi:10.3390/brainsci11010057
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.