Back to Journals » Psychology Research and Behavior Management » Volume 19
Impact of Adverse Childhood Experiences and Rumination on Metacognition in Chinese Urban Adolescents with Major Depressive Disorder
Authors Li J, Zhu J, Zhou B, Sun J, Zhou S ![]() , Qi M, Chen J
, Qi M, Chen J ![]()
Received 20 July 2025
Accepted for publication 23 January 2026
Published 11 March 2026 Volume 2026:19 555078
DOI https://doi.org/10.2147/PRBM.S555078
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Jiuju Li,1,* JiaQi Zhu,2,* Bingjie Zhou,3 Jiaqi Sun,3 Shuangjiang Zhou,1 Meng Qi,1 Jingxu Chen1
1Sleep Medicine Center, Beijing Huilongguan Hospital, Capital Medical University, Beijing, 100096, People’s Republic of China; 2Department of Psychiatry and Psychology, Beijing Children’s Hospital, Capital Medical University, Beijing, 100045, People’s Republic of China; 3Department of Psychology, Chengde Medical University, Chengde, 067000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jingxu Chen, Sleep Medicine Center, Beijing Huilongguan Hospital, No. 7, Nandian Road, Changping District, Beijing, 100096, People’s Republic of China, Email [email protected]
Background: Major depressive disorder (MDD) in adolescents represents a significant global public health challenge. Moreover, metacognitive dysfunction plays a critical role in its onset, progression, and prognosis, but research on the metacognitive characteristics of Chinese adolescents with MDD remains highly limited.
Methods: The study was conducted from January 2024 to January 2025 and employed a cross-sectional design with convenience sampling. The participants included 202 adolescents who were diagnosed with MDD, with a mean age of 15 years. All the subjects completed a self-administered general information questionnaire to collect demographic information. The Patient Health Questionnaire (PHQ-9), Generalized Anxiety Disorder Scale (GAD-7), Adverse Childhood Experience Questionnaire-Revised (ACE), Rumination Response Scale Chinese Version (RRS), and Metacognitive Questionnaire-30 (MCQ) were utilized to evaluate the psychological well-being of adolescents diagnosed with MDD.
Results: Multiple linear regression analyses demonstrated the potential of the RRS total score, reflective pondering and household dysfunction as predictors of metacognitive deficits in adolescents diagnosed with MDD, with statistical significance at p < 0.05. Furthermore, the total ACE scores of adolescents diagnosed with MDD were significantly positively correlated with the MCQ (β = 0.189, p < 0.001) and RRS (β = 0.380, p < 0.001) scores. Additionally, the total RRS score was positively correlated with the MCQ score (β = 0.675, p < 0.001). Mediation analyses demonstrated that rumination mediated the association between adverse childhood experiences and metacognitive deficits, with a mediating effect value of 1.136 and a 95% confidence interval of [0.639, 1.635], explaining 57.32% of the total effect.
Conclusion: Rumination mediates the relationship between adverse childhood experiences and metacognitive deficits in adolescents with MDD. Rumination, reflective pondering and household dysfunction in adolescents with MDD can predict metacognitive dysfunction to varying degrees. Our study highlights that interventions targeting rumination may be particularly effective in mitigating the negative impact of ACEs on metacognitive functioning in adolescents with MDD.
Keywords: adolescents, major depressive disorder, metacognition, rumination, adverse childhood experiences, mediation
Introduction
Adolescents diagnosed with major depressive disorder (MDD) frequently present with symptoms including but not limited to, significantly low mood, marked anhedonia, cognitive deficits, and behavioral changes.1 The prevalence of MDD among adolescents is increasing annually, making it a pressing concern within the domain of mental health, both domestically and internationally.2 The pathogenesis of MDD in adolescents is characterized by multidimensional interactions, yet the associations among adverse childhood experiences (ACEs), rumination, and metacognitive dysfunction remain unclear.
ACEs are strongly associated with a wide range of adverse psychological and physiological outcomes in adulthood and are strong predictors of the severity of MDD and metacognitive deficits.3 In line with Wells’ S-REF model, cross-sectional studies conducted on nonclinical samples have demonstrated that individuals exposed to multiple ACEs are more prone to developing dysfunctional metacognitive beliefs.4,5 Individuals with ACEs, such as abuse and neglect, are not only more likely to engage in repetitive negative thinking (eg, worry and rumination) but also exhibit a strong association between such rumination and poorer clinical outcomes, including more severe psychopathology and major depressive disorder.6 Research suggests that during exposure to ACEs, maladaptive metacognitive beliefs are formed, shaping an individual’s negative perceptions of their own thoughts. These beliefs may then contribute to the development of PTSD by transforming the experience into a traumatic one, and ultimately serve as a maintaining factor of the disorder.7
Metacognition, defined as the awareness and regulation of one’s own cognitive processes, plays a pivotal role in the development and maintenance of MDD, particularly in adolescent patients.8 Meta-analyses have indicated a robust correlation between deficits in metacognitive functioning and the prevalence of depression and anxiety in adolescent populations.9 The development of metamemory and meta-attention commences during the preschool years, with the utilization of metacognitive strategies being contingent upon adult modeling. These abilities gradually stabilize and mature during late childhood and adolescence.10 Neuroimaging evidence establishes the default mode network (DMN), particularly its dorsomedial prefrontal cortex (dmPFC) subsystem involved in metacognition, as the core neural substrate of rumination—a network which is similarly hyperactive in MDD.11 As Eze et al argue, emotional fluctuations have the potential to disrupt this stability. Damage to the connectivity of these brain regions has been demonstrated to exacerbate maladaptive coping strategies, such as rumination.12 Adolescents diagnosed with MDD may become entrapped within a negative thought cycle characterized by metacognitive beliefs that are negative in nature (eg, “Why do I always fail?”). This cycle has been shown to perpetuate depressive episodes.13
Rumination, a repetitive and passive focus on negative experiences, is a core cognitive feature in adolescent with MDD, strongly associated with family upbringing, and it is a core cognitive feature that is closely related to the onset and maintenance of MDD.14 The internalization of the parental belief that “without academic success, there is no future” compounded by long-term academic rumination, cultivates a unique form of cognitive vulnerability in Chinese adolescents.15 In adolescents diagnosed with MDD, rumination has been shown to exacerbate depressive symptoms by maintaining a negative attentional focus and impeding effective problem solving. Furthermore, it has been demonstrated to disrupt cognitive processes, including metacognition.16 When individuals diagnosed with MDD faced with a new stressor like exam pressure, they automatically revert to their old pattern of negative, repetitive thinking, rapidly spiraling back into a major depressive state, prolong the duration of the illness.17
There is a strong interaction between adverse childhood experiences, rumination and metacognition in adolescents with major depressive disorder. In this study, we aimed to explore the factors influencing metacognition in adolescents with major depressive disorder and provide a theoretical basis for its prevention and intervention. Therefore, the following hypotheses are proposed:
H1: Adverse childhood experiences and ruminative thinking are predictors of metacognition in adolescents with MDD. H2: Rumination will mediate the effect of adverse childhood experiences on metacognition in adolescents with MDD.
Materials and Methods
Participants
This study was a cross-sectional survey of Chinese adolescents with MDD conducted via convenience sampling. The study was conducted from January to December 2024 in the outpatient and inpatient wards of a tertiary care psychiatric hospital in Beijing, China, and adolescents with major depressive disorder were recruited. Potential participants were initially screened by assessors to determine their eligibility on the basis of inclusion and exclusion criteria. After informed consent was obtained from the participants and their guardians, the subjects were formally enrolled in the study. All participants completed the paper-based questionnaires independently under the direct supervision of the study investigator or a psychiatrist. To prevent any external influence, guardians or family members were not permitted to be present or intervene during the entire completion process. The principal investigator provided detailed instructions on how to complete the questionnaire and precautions, and guidance statements were added to each scale to ensure that the participants understood all the items accurately.
The patient inclusion criteria were (1) meeting the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) diagnostic criteria for MDD; (2) between the ages of 12 and 18, regardless of sex; and (3) no reading or writing disabilities or ability to cooperate with the assessment. The exclusion criteria were as follows: (1) significant physical illness, brain injury, or other organic damage; (2) history of substance abuse or drug dependence; (3) comorbidities with other mental illnesses diagnosed by the DSM-5; and (4) withdrawal of informed consent by the participant or his/her guardian.
A total of 239 adolescents with MDD were recruited for this study. After excluding 37 cases due to withdrawal during the study or invalid questionnaires, 202 cases were ultimately included, resulting in a survey response rate of 84.77%. This study was approved by the Ethics Committee of Beijing HuiLongGuan Hospital, with approval number 2024-10-Science and Technology, in accordance with the Declaration of Helsinki. This trial was prospectively registered at the Chinese Clinical Trial Registry (http://www.chictr.org.cn/) under identifier ChiCTR2400090543. All participants and their guardians signed an informed consent form.
Questionnaire Survey
General Information
General information was assessed via a self-constructed questionnaire, which included general demographic information, such as sex, age, and educational level, as well as history of psychiatric disorders.
Clinical Evaluation
The Patient Health Questionnaire-9 (PHQ-9),18 developed by Kroenke et al in 2001, is a self-assessment tool for depressive symptoms and is widely used for rapid screening in clinical and community settings. On the basis of the diagnostic criteria for MDD, the PHQ-9 comprises nine items scored on a scale from 0--3, with total scores ranging from 0 to 27. Higher scores are indicative of more severe depression. In this study, the Cronbach’s α coefficient was 0.830.
The Generalized Anxiety Disorder-7 (GAD-7),19 created by Spitzer et al in 2006, is designed for the rapid screening of anxiety symptoms. It consists of seven items scored on a scale from 0 to 3, with a total score ranging from 0 to 21. Higher GAD-7 scores reflect more severe anxiety symptoms. The Cronbach’s α coefficient in this study was 0.887.
Adverse Childhood Experience
The Adverse Childhood Experience Questionnaire-Revised (ACE)20,21 is utilized to investigate adverse childhood experiences before the age of 18 years within the context of Chinese culture. It includes 14 questions answered in a yes/no format. The questionnaire covers three dimensions: household dysfunction, neglect, and abuse. Household Dysfunction refers to severe disruptions in the family system during childhood, such as parental separation/divorce, household mental illness, substance abuse, exposure to intimate partner violence, or incarceration of a household member. Neglect encompasses the failure of caregivers to meet a child’s basic emotional or physical needs. Abuse involves intentional harm inflicted on a child, including physical, emotional, and sexual abuse. Higher scores on this scale are associated with a greater degree of exposure to adverse childhood experiences. The Cronbach’s α coefficient in this study was 0.799.
Rumination
The Ruminative Responses Scale-Chinese Version (RRS),22,23 originally compiled by Nolen-Hoeksema in 1987 and revised by Han and Yang in 2009 for this study. It is a self-assessment scale comprising 22 items scored on a four-point Likert scale (1–4). The scale includes three dimensions, namely, symptom rumination, reflective pondering, and brooding, with items from each dimension intermixed throughout the questionnaire. Higher scores indicate a stronger tendency toward rumination. It should be highlighted that this scale has undergone cross - cultural testing and has demonstrated good reliability and validity. The Cronbach’s α coefficient in this study was 0.943.
Metacognition
Metacognition Questionnaire-30 (MCQ),24 developed by Wells et al, consists of 30 items scored on a four-point Likert scale (1–4), with 1 indicating strong disagreement and 4 indicating strong agreement. It has good reliability and validity among Chinese adolescents. The questionnaire assesses five dimensions of metacognition: cognitive confidence (CC), positive beliefs about worry (POS), cognitive self-consciousness (CSC), negative beliefs about uncontrollability and danger of worry (NEG), and the need to control thoughts (NC). Each dimension’s items are intermixed within the scale. Higher scores on each subscale indicate a more pronounced degree of metacognitive impairment. The Cronbach’s α coefficient in this study was 0.910.
Statistical Methods
Statistical analyses were conducted via SPSS 26.0. The Kolmogorov‒Smirnov test (p < 0.05) revealed that none of the continuous data in this study conformed to a normal distribution. Continuous data are expressed as the median (interquartile range) (M(QR)). For the demographic data, the categorical variables are expressed as frequencies and percentages (%) and were analyzed via the chi-square test. The Mann‒Whitney U-test was employed to analyze the test of variance, and Spearman correlation analysis was utilized to examine the relationships between the scales. Multiple linear regression models were constructed on the basis of the dimensions of the existing scales to explore their interrelationships. The mediation effect path analysis was conducted via Model 4 in Process 4.1, and the significance of the mediation effect was tested via the bias-corrected bootstrap method. A total of 5000 self-help samples were collected for the purpose of estimating 95% confidence intervals for the mediation effect. The significance level was set at p < 0.05 to indicate a statistically significant difference.
Results
Common Method Bias
Harman’s single-factor test was employed to assess common method bias in the data. The results indicated that there were 12 factors with eigenvalues greater than 1. The first unrotated factor accounted for 28.11% of the cumulative variance, which is below the critical threshold of 40%. This suggests that there is no significant common method bias in the data.
General Information Associated with Depression, Anxiety, Childhood Adverse Experiences, Rumination and Metacognition
This cross-sectional survey was conducted from January 2024-January 2025 at the outpatient and inpatient wards of Beijing HuiLongGuan Hospital. A total of 239 adolescents with depression were initially recruited. After excluding 37 cases due to withdrawal during the study or invalid questionnaires, 202 cases were ultimately included, resulting in a survey response rate of 84.77%. The adolescents with depression in this survey had a median age of 15.00 (3.00) years. Fifty-four patients (26.7%) were recruited from inpatient wards, whereas 148 patients (73.3%) were recruited from outpatient clinics. There were 44 males (21.8%) and 158 females (78.2%). Table 1 presents the illness duration information of adolescents with depression. Table 2 presents the differences in demographic variables, MCQ results, and related psychological mechanism scales among adolescents with depression. Significant gender differences were observed in the scores of CSC in the MCQ and neglect in the ACE scale, with males scoring higher than females (Z=−2.445, p=0.014; Z=1.976, p=0.048). For the ACE scale, the neglect scores of junior high school students were significantly higher than those of senior high school students (Z=−2.428, p=0.015). Compared with those without a family history of depression, adolescents with a family history of depression had higher scores in the ACE and abuse dimensions (Z=2.815, p=0.005; Z=5.525, p<0.001).
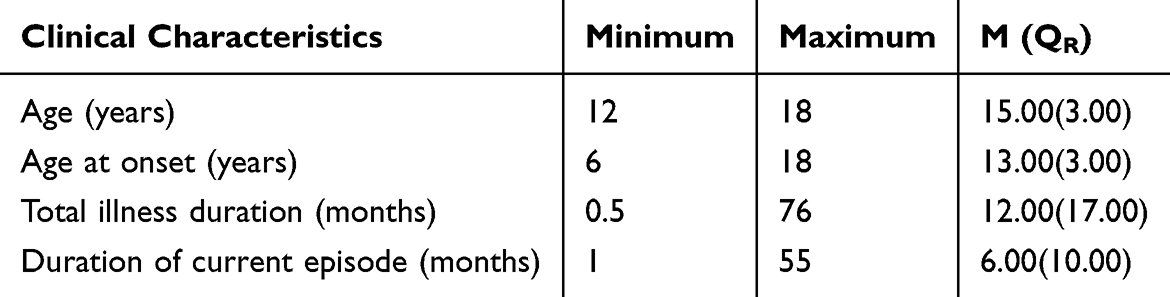 |
Table 1 General Clinical Characteristics of Adolescents with MDD (Median (QR)) |
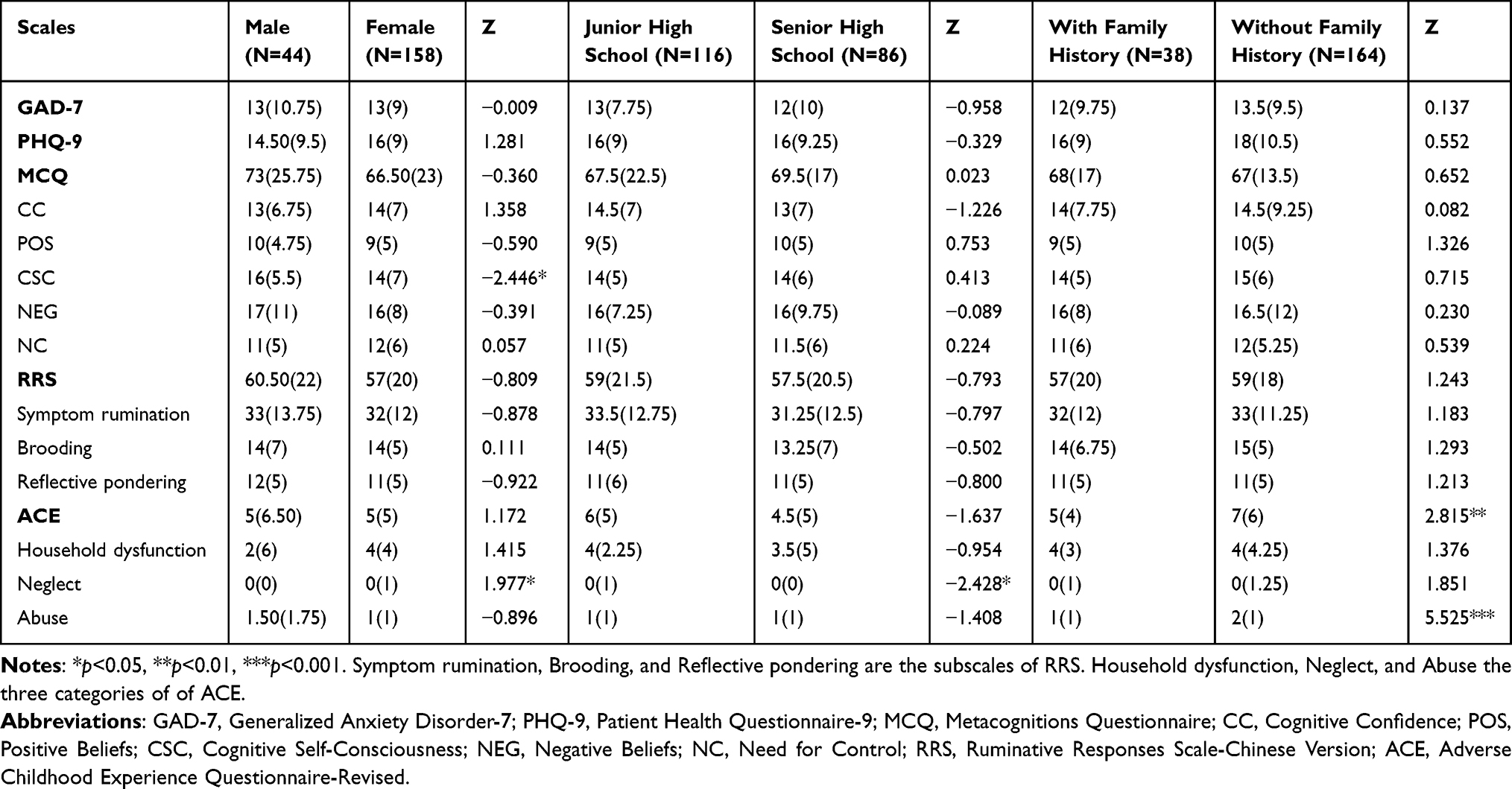 |
Table 2 Differences in Scale Scores Among Adolescents with MDD by General Information (Median (QR)) |
Relationships Among Depression, Anxiety, Childhood Adverse Experiences, Rumination and Metacognition in Chinese Adolescents with MDD
As shown in Table 3, the scores of the GAD-7, PHQ-9, MCQ, RRS, and ACE were positively correlated with each other, with correlation coefficients ranging from 0.236 to 0.756, all of which were statistically significant (p<0.05).
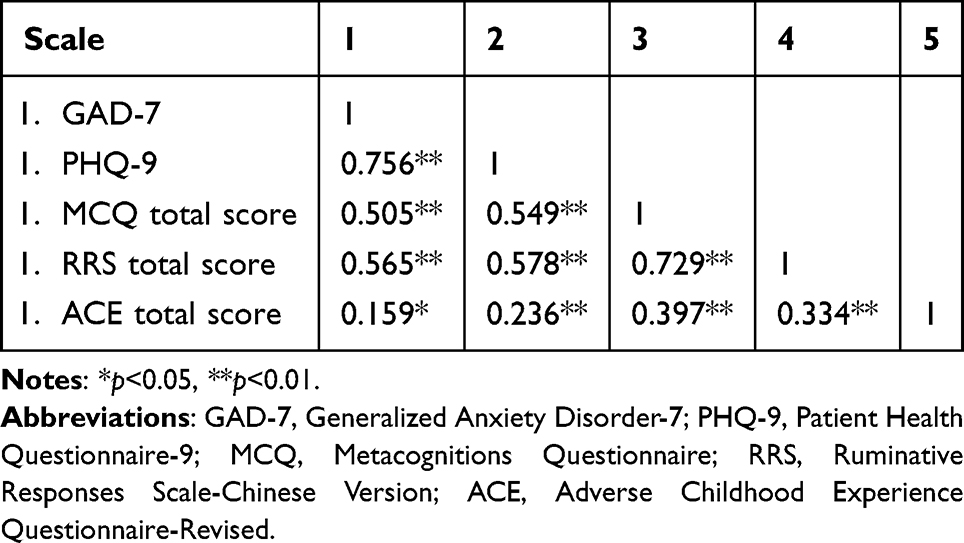 |
Table 3 Correlation Analysis of Depression, Anxiety, Metacognition, Adverse Childhood Experience, Rumination (N=202) |
Multivariate Regression Analysis of Metacognitive Deficits in Adolescents with MDD
SPSS 26.0 was used for linear regression analysis, and the MCQ total score was set as the dependent variable, while the general demographic variables GAD-7, PHQ-9, RRS, ACE, and subscales of these questionnaires were set as independent variables. The stepwise method was employed to select independent variables and construct the optimal predictive model. The final results (Table 4) revealed that the Durbin‒Watson statistic was 1.921, indicating that the model data met the independence requirement. The tolerance range was 0.302–0.910, and the variance inflation factor (VIF) was 1.099–3.314, suggesting that there was no significant multicollinearity in the model. ANOVA revealed that R=0.776, R2 = 0.602, F=4.657, and p = 0.032, indicating an acceptable model fit. The total RRS score, reflective pondering score, and household dysfunction score in adolescents with MDD were found to have varying degrees of predictive effects on metacognitive deficits (p<0.05).
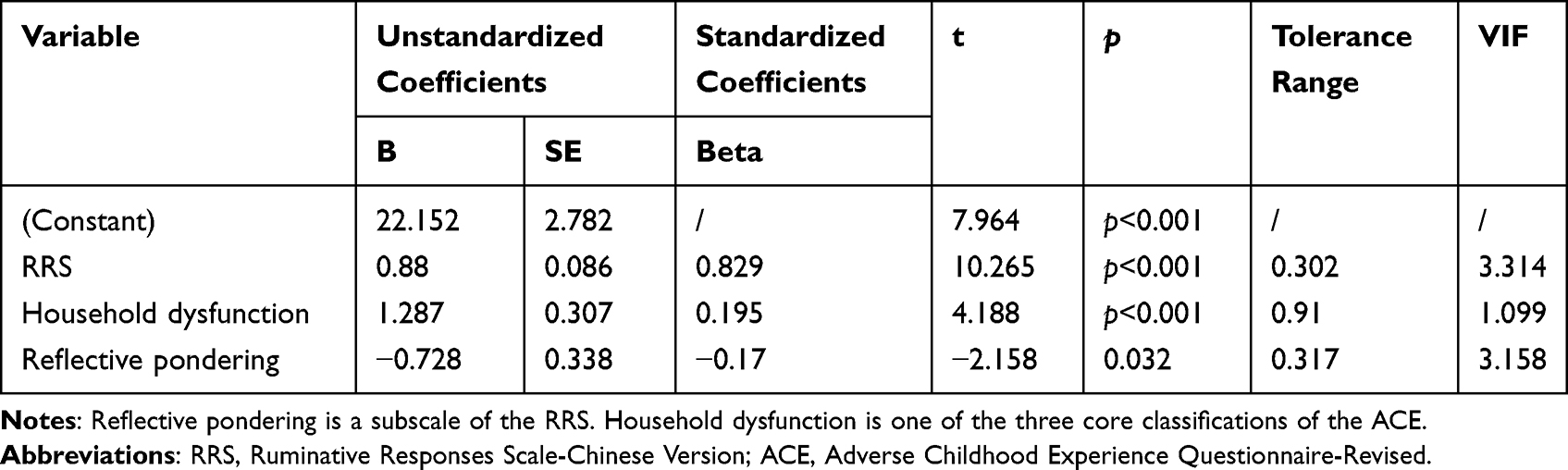 |
Table 4 Multifactorial Regression Analysis of Metacognition in Adolescents with MDD |
Impact of Childhood Adverse Experiences on Metacognition in Adolescents with MDD: The Mediating Role of Rumination
Correlation analysis revealed that among adolescents with MDD, the total ACE, MCQ, and RRS scores were positively correlated with each other, and the correlation coefficients were statistically significant (p<0.05). Therefore, a mediation effect test could be further conducted. This study utilized the Process 4.1 macro in SPSS 26.0 software and applied Model 4 to explore the underlying mechanism of rumination in the impact of adverse childhood experiences on metacognition among adolescents with MDD. Specifically, the total ACE score was set as the independent variable, the total MCQ score was set as the dependent variable, and the total RRS score was set as the mediator variable. Additionally, age, education level, sex, family history, age of onset, total disease duration, and duration of the current episode were included as covariates. The study model is shown in Figure 1, and the path coefficients and effect sizes are detailed in Tables 5 and 6.
 |
Table 5 Regression Analysis of Childhood Adverse Experiences, Rumination, and Metacognition in Adolescents with MDD |
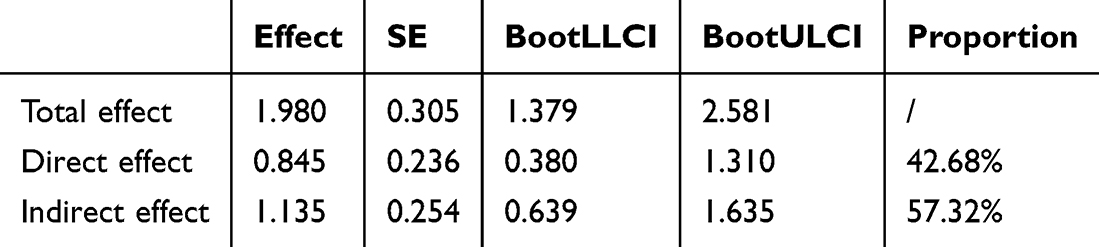 |
Table 6 Bootstrap Test of the Mediating Effect of Rumination on the Impact of Childhood Adverse Experiences on Metacognition |
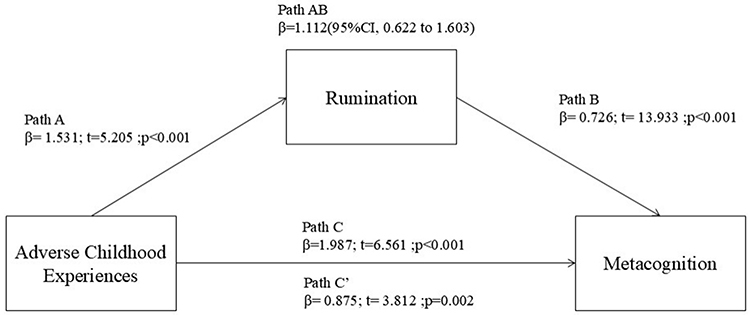 |
Figure 1 Shows Model 4 Path diagram of the mediation model (X = ACE total score; Y = MCQ total score; M= RRS total score). Path C’ and Path C represent the direct and total effect between ACE total score and MCQ total scare. Path AB represents the mediation effect and is significant at p<0.05 in the models. |
The path analysis results of this study revealed that the total ACE score of adolescents with MDD can significantly positively predict the total MCQ score (B=0.844, β=0.189, p<0.001) and the total RRS score (B=1.587, β=0.380, p<0.001). Moreover, the total RRS score positively predicted the total MCQ score (B=0.723, β=0.675, p<0.001). The model fit indices are R=0.444, R2=0.198, F=4.259, p<0.05, indicating an acceptable fit.
Discussion
The subjects of this survey were adolescents with MDD in the outpatient clinic and inpatient ward of a tertiary A psychiatric specialist in Beijing, with a predominance of female patients accounting for 78.2%, a proportion similar to that reported in previous studies.25 In this study, significant correlations were found between depression, anxiety, metacognition, rumination, and adverse childhood experiences among adolescents with MDD. Early exposure to negative events is a crucial factor in the development of future depression. The use of maladaptive coping strategies increases the likelihood of depression, while higher levels of neuroticism and perceived stress can also indirectly influence depression.26 Furthermore, the study revealed that adolescents with a family history of MDD scored higher on both the total score and the abuse subscale of ACE. This phenomenon may be attributed to the interplay between genetic predispositions and environmental factors. ACEs have been demonstrated to be robust predictors of future MDD, particularly experiences of abuse and neglect, which may render adolescents more susceptible to mental health issues when confronted with familial stress.27 Adolescents with MDD in junior high school reported higher levels of neglect in adverse childhood experiences than did those in senior high school. This may be related to the rapid economic development in China, changes in social structure and family structure, and the increasing busyness of parents, as well as shifts in living and economic conditions following the pandemic.25 Chinese filial piety may exacerbate psychological stress among adolescents from dysfunctional families, thereby amplifying the detrimental effects of ACEs.28 This heightened stress can subsequently shape a maladaptive ruminative thinking style, characterized by guilt over perceived failures to meet parental expectations. Such persistent, guilt-laden rumination may, in turn, disrupt the healthy development of metacognitive functioning.
This survey revealed that adolescents with MDD exhibited metacognitive deficits. These findings are consistent with previous neurocognitive studies.29 Adaptive metacognitive beliefs about worry as a problem-solving strategy may have a protective effect, and positive self-perception is independently associated with the improvement of depressive symptoms.30 In terms of gender differences, male adolescents with MDD had higher scores for cognitive self-consciousness than females did, indicating weaker cognitive confidence. Female adolescents with MDD showed greater accuracy in facial emotion recognition tasks, which may be related to more refined metacognitive monitoring and is positively correlated with NSSI behavior and female emotion orientation.31 This suggests that excessive self-focus may have negative effects. With respect to social role expectations and gender stereotypes, males are often expected to be more independent and achieve higher academic success, whereas females are required to express more emotions and engage in more social interactions. Therefore, when facing depressive emotions, male adolescents tend to internalize problems, such as self-doubt and excessive rumination.32
Rumination, reflective pondering and household dysfunction functioning in adolescents with MDD can predict metacognitive dysfunction to varying degrees. In the context of Chinese culture, strict parenting styles and family conflicts, which are indicative of impaired family functioning, can easily lead adolescents to form negative self-cognitive patterns. This, in turn, increases the occurrence of rumination and metacognitive impairments by repeatedly thinking about negative experiences.33 Prior research has suggested that the confluence of intense academic pressure, traditional parenting styles emphasizing behavioral control,34 and Confucian values that encourage self-scrutiny35 may cultivate a cognitive vulnerability to maladaptive rumination. This ruminative style, often focused on academic failure and familial expectations, can lead to intense self-criticism and a diminished ability to adopt a detached, metacognitive perspective on one’s difficulties. A longitudinal study of 192 children and adolescents showed that female participants with higher levels of depression and who more frequently employed expressive suppression and rumination had higher levels of suicidal ideation and risk.36 Catastrophizing, passive acceptance, and ruminative brooding are common negative cognitive characteristics among adolescents with MDD. These traits may lead to an overestimation of their own incompetence, triggering anxiety and depression. Over time, this reinforces the behavior pattern and results in a vicious cycle.37 Adolescents with high levels of rumination and brooding may become overly immersed in emotion regulation, making it difficult to break free from negative thinking.38 This weakens cognitive flexibility and affects metacognitive function.
In this study, the ACE scores of adolescents with MDD significantly and positively predicted the level of metacognitive impairment. Rumination played a mediating role in the impact of ACEs on metacognitive impairment in adolescents with MDD, accounting for 57.32% of the total effect, compared with previous studies, the proportion of cases in which this cognitive mechanism plays a role is higher.39 The presence of ACEs, particularly those related to emotional abuse and family conflict, poses a significant risk for long-term psychological and cognitive impairments in adolescents and is an important risk factor for the development of MDD. This finding corroborates the core tenets of psychoanalytic theory. According to this theory, unresolved psychological conflicts caused by childhood trauma become embedded in an individual’s subconscious and manifest themselves in adolescence in the form of self-punishing behaviours, such as rumination or NSSI, or self-destructive behaviours, such as suicide attempts, serving as functional adaptive mechanisms to alleviate feelings of guilt and psychological distress.40 During their development, adolescents with MDD are more likely to lack support from a healthy family environment, experience adverse childhood events, and fail to develop adaptive cognitive and emotional regulation strategies (such as rumination and worry), making it more difficult for them to develop metacognitive abilities.
The limitations of this study are attributable to its cross-sectional design, which captures data at a single time point. This restricts the observation of changes in metacognitive function over time and the elucidation of the long-term trajectory of metacognitive impairments and their dynamic interplay with depressive symptoms. Furthermore, the exclusive utilization of questionnaire scales restricts the study to psychological assessments, excluding neurobiological evidence. The sample reflects adolescents with MDD in the Beijing area, with geographical and sampling biases limiting the generalizability of the findings. It is recommended that future research be designed as a nationwide longitudinal survey with random sampling to dynamically track changes in metacognitive functions. In circumstances where this is possible, objective measures such as fMRI and ERP should be utilized to assess psychological ability.
Despite these limitations, the present study provides insights into the clinical characteristics and psychological abilities, including metacognition, of adolescents with MDD through a cross-sectional survey. Our study provides a comprehensive theoretical foundation for the prevention and treatment of emotional disorders in adolescents and serves as a valuable reference source for psychological interventions. Future research, which incorporates refined designs and diverse measurement methods, has the potential to further enhance our understanding of and ability to intervene in cases of adolescent depression.
Conclusion
Among adolescents with MDD, rumination, reflective pondering, and household dysfunction emerge as significant predictors of metacognitive impairments, albeit to varying extents. Furthermore, in adolescents with MDD, ACEs are positively correlated with both metacognitive deficits and rumination. Notably, rumination serves as a mediator between ACEs and metacognitive deficits. Our study highlights the pivotal role of rumination-focused interventions in potentially alleviating the negative effects of ACEs on metacognition among adolescents with MDD.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of Beijing HuiLongGuan Hospital, with approval number 2024-10-Science and Technology, in accordance with the Declaration of Helsinki. This trial was prospectively registered at the Chinese Clinical Trial Registry (http://www.chictr.org.cn/) under identifier ChiCTR2400090543. All protocol modifications were documented in the registry. All participants and their guardians signed an informed consent form.
Acknowledgments
The authors thank all the staff and graduate students who contributed to this study. Their diligent efforts and support were essential to the completion of this work.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The work was supported by the following two projects:1. Beijing Municipal Hospitals’ Scientific Research Cultivation Program [Project PX2025068]2. Beijing High-Level Innovation and Entrepreneurship Talent Support Program leading talent projects [Project G202511067]
Disclosure
The authors report no conflicts of interest in this work.
References
1. Dong W, Liu Y, Bai R, Zhang L, Zhou M. Corrigendum to “the prevalence and associated disability burden of mental disorders in children and adolescents in China: a systematic analysis of data from the global burden of disease study” [the lancet regional health-western pacific]. Lancet Reg Health West Pac. 2025;(58):101556. doi:10.1016/j.lanwpc.2025.101556
2. Psychogiou L, Navarro MC, Orri M, Côté SM, Ahun MN. Childhood and adolescent depression symptoms and young adult mental health and psychosocial outcomes. JAMA Network Open. 2024;7(8):e2425987. doi:10.1001/jamanetworkopen.2024.25987
3. Frodl T, Janowitz D, Schmaal L, et al. Childhood adversity impacts on brain subcortical structures relevant to depression. J Psychiatr Res. 2017;86:58–11. doi:10.1016/j.jpsychires.2016.11.010
4. Horváth D, Kovács-Tóth B, Oláh B, Fekete Z. Trends in the dose-response relationship between adverse childhood experiences and maladaptive metacognitive beliefs: a cross-sectional study. Compr Psychiatry. 2024;132:152489. doi:10.1016/j.comppsych.2024.152489
5. Wells A, Matthews G. Modelling cognition in emotional disorder: the S-REF model. Behav Res Ther. 1996;34(11–12):881–888. doi:10.1016/S0005-7967(96)00050-2
6. Mansueto G, Cavallo C, Palmieri S, Ruggiero GM, Sassaroli S, Caselli G. Adverse childhood experiences and repetitive negative thinking in adulthood: a systematic review. Clin Psychol Psychother. 2021;28(3):557–568. doi:10.1002/cpp.2590
7. Hosseini Ramaghani NA, Rezaei F, Sepahvandi MA, Gholamrezaei S, Mirderikvand F. The mediating role of the metacognition, time perspectives and experiential avoidance on the relationship between childhood trauma and post-traumatic stress disorder symptoms. Eur J Psychotraumatol. 2019;10(1):1648173. doi:10.1080/20008198.2019.1648173
8. Fleming SM. Metacognition and confidence: a review and synthesis. Annu Rev Psychol. 2024;75:241–268. doi:10.1146/annurev-psych-022423-032425
9. Thingbak A, Capobianco L, Wells A, O’Toole MS. Relationships between metacognitive beliefs and anxiety and depression in children and adolescents: a meta-analysis. J Affect Disord. 2024;361:36–50. doi:10.1016/j.jad.2024.05.123
10. Schneider W, Tibken C, Richter T. The development of metacognitive knowledge from childhood to young adulthood: major trends and educational implications. Adv Child Dev Behav. 2022;63:273–307. doi:10.1016/bs.acdb.2022.04.006
11. Zhou HX, Chen X, Shen YQ, et al. Rumination and the default mode network: meta-analysis of brain imaging studies and implications for depression. NeuroImage. 2020;206:116287. doi:10.1016/j.neuroimage.2019.116287
12. Eze UC, Bhaduri A, Haeussler M, Nowakowski TJ, Kriegstein AR. Single-cell atlas of early human brain development highlights heterogeneity of human neuroepithelial cells and early radial glia. Nat Neurosci. 2021;24(4):584–594. doi:10.1038/s41593-020-00794-1
13. Akbari M, Mohammadaliha N, Mohammadkhani S, Seydavi M, Griffiths MD. Cognitive, metacognitive, motivational, and emotional predictors of the intensity of internet gaming disorder among adolescents. Psychiatr Q. 2024;95(3):385–414. doi:10.1007/s11126-024-10075-w
14. Dunning EE, Birk S, Olino TM, Alloy LB. Intergenerational transmission of rumination via parenting behaviors and family characteristics: the impact on adolescent internalizing symptoms. Child Psychiatry Hum Dev. 2022;53(1):27–38. doi:10.1007/s10578-020-01104-3
15. Leung JTY, Shek DTL. The influence of parental expectations and parental control on adolescent well-being in poor Chinese families. Appl Res Quality Life. 2019;14(4):847–865. doi:10.1007/s11482-017-9540-9
16. Özbek MM, Çıray RO. Analysis of the relationship between emotion regulation difficulties and impulsivity and cognitive/metacognitive skills in adolescents diagnosed with major depressive disorder. Psychiatry Clin Psychopharmacol. 2024;34(2):144–152. doi:10.5152/pcp.2024.23762
17. Koster EHW, De Lissnyder E, Derakshan N, De Raedt R. Understanding depressive rumination from a cognitive science perspective: the impaired disengagement hypothesis. Clin Psychol Rev. 2011;31(1):138–145. doi:10.1016/j.cpr.2010.08.005
18. Leung DYP, Mak YW, Leung SF, Chiang VCL, Loke AY. Measurement invariances of the PHQ-9 across gender and age groups in Chinese adolescents. Asia Pac Psychiatry. 2020;12(3):e12381. doi:10.1111/appy.12381
19. Sun J, Liang K, Chi X, Chen S. Psychometric properties of the generalized anxiety disorder scale-7 item (GAD-7) in a large sample of Chinese adolescents. Healthcare. 2021;9(12):1709. doi:10.3390/healthcare9121709
20. Li W, Zhang X, Chu M, Li G. The impact of adverse childhood experiences on mobile phone addiction in Chinese college students: a serial multiple mediator model. Front Psychol. 2020;11:834. doi:10.3389/fpsyg.2020.00834
21. Wang Y, Lin P, Cao F. Validity and reliability of the Chinese version of the Revised Adverse Childhood Experience Questionnaire. Chin Mental Health J. 2014;28(6):460–465. doi:10.3969/j.issn.1000-6729.2018.09.010
22. Liu D, Liu S, Deng H, et al. Depression and suicide attempts in Chinese adolescents with mood disorders: the mediating role of rumination. Eur Arch Psychiatry Clin Neurosci. 2023;273(4):931–940. doi:10.1007/s00406-022-01444-2
23. Han X, Yang H. Chinese version of Nolen-Hoeksema Ruminative Responses Scale (RRS) used in 912 college students: reliability and validity. Chin J Clin Psychol. 2009;17(05):550–551+549. doi:10.16128/j.cnki.1005-3611.2009.05.028
24. Li F, Yuan D, Gao C, Xiong K, Geng F, Zhang L. Validity and reliability of the metacognitions questionnaire-30 (MCQ-30) among Chinese adolescents. Child Psychiatry Hum Dev. 2025;56(4):1031–1040. doi:10.1007/s10578-023-01625-7
25. Du X, Wu H, Yalikun S, et al. Trajectories of Chinese adolescent depression before and after COVID-19: a cross-temporal meta-analysis with segmented regression. J Affect Disord. 2025;373:333–344. doi:10.1016/j.jad.2024.12.094
26. Qin Q, Jiang Y, Mei X, et al. The effect of childhood trauma on depression in college students: a moderated mediation model. J Affect Disord. 2024;352:490–497. doi:10.1016/j.jad.2024.02.067
27. Racine N, Bellis MA, Madigan S. An introduction to twenty-five years of adverse childhood experiences: a special issue. Child Abuse Negl. 2025;168(Pt 1):107224. doi:10.1016/j.chiabu.2024.107224
28. Han X, Cheung MC. The relationship between dual filial piety and mental disorders and symptoms among adolescents: a systematic review of quantitative and qualitative studies. Adolescent Res Rev. 2025;10(1):31–45. doi:10.1007/s40894-024-00234-2
29. Bienek O, Allott K, Antonucci L, et al. Neurocognitive dysfunction in adolescents with recent onset major depressive disorder: a cross-sectional comparative study. Eur Child Adolesc Psychiatry. 2025;34(6):1873–1882. doi:10.1007/s00787-024-02599-0
30. Dean RL, Lester KJ, Grant E, Field AP, Orchard F, Pile V. The impact of interventions for depression on self-perceptions in young people: a systematic review & meta-analysis. Clin Psychol Rev. 2025;115:102521. doi:10.1016/j.cpr.2024.102521
31. He K, Ji S, Sun L, et al. Gender differences in facial emotion recognition among adolescents depression with non-suicidal self-injury. Psychol Res Behav Manag. 2023;16:3531–3539. doi:10.2147/PRBM.S418966
32. Gadassi Polack R, Sened H, Aubé S, Zhang A, Joormann J, Kober H. Connections during crisis: adolescents’ social dynamics and mental health during COVID-19. Dev Psychol. 2021;57(10):1633–1647. doi:10.1037/dev0001211
33. Li M, Wang J, Ma P, Sun W, Gong H, Gao Y. The relationship between harsh parenting and adolescent depression. Sci Rep. 2023;13(1):20647. doi:10.1038/s41598-023-48138-w
34. Liu J, Chan C, Leung PWL. Youth psychopathology: universal or culture-specific? Testing the syndrome models of youth self-report in Chinese population. J Child Adolesc Psychiatr Nurs. 2022;35(2):126–141. doi:10.1111/jcap.12353
35. Lin RM, Hong YJ, Xiao HW, Lian R. Honesty-humility and dispositional awe in confucian culture: the mediating role of zhong-yong thinking style. Pers Individ Dif. 2020;167:110228. doi:10.1016/j.paid.2020.110228
36. Thompson RJ, Whalen DJ, Gilbert K, et al. Preadolescent suicidal thoughts and behaviors: an intensive longitudinal study of risk factors. J Am Acad Child Adolesc Psychiatry. 2025;64(3):375–385. doi:10.1016/j.jaac.2024.03.018
37. Guo X, Tang G, Lin F, Fang H, Chen J, Zou T. Biological links between psychological factors and adolescent depression: childhood trauma, rumination, and resilience. BMC Psychiatry. 2024;24(1):907. doi:10.1186/s12888-024-06369-9
38. Fang X, Wu Z, Wen L, et al. Rumination mediates the relationship between childhood trauma and depressive symptoms in schizophrenia patients. Eur Arch Psychiatry Clin Neurosci. 2023;273(5):1085–1094. doi:10.1007/s00406-022-01525-2
39. Wang H, Wen S, Wang Y, Zhou Y, Niu B. Rumination, loneliness, and non-suicidal self-injury among adolescents with major depressive disorder: the moderating role of resilience. Soc Sci Med. 2025;364:117512. doi:10.1016/j.socscimed.2024.117512
40. Li W, Han Y, Hu Z, Zhang Y. Childhood trauma and non-suicidal self-injury among Chinese adolescents: the chain mediating effects of alexithymia and experiential avoidance. Acta Psychol. 2024;251:104634. doi:10.1016/j.actpsy.2024.104634
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Insomnia and Alexithymia in Chinese Adolescents with Major Depressive Disorder: A Cross-Sectional Study of Sex Differences and Associations
Yang X, Liu L, Tian Y, Yang C, Ling C, Liu H
Psychology Research and Behavior Management 2024, 17:615-625
Published Date: 20 February 2024
The Relationship Between Childhood Trauma and Non-Suicidal Self-Injury Behavior in Adolescents with Depression: The Mediating Role of Rumination
Fu W, Li X, Ji S, Yang T, Chen L, Guo Y, He K
Psychology Research and Behavior Management 2024, 17:1477-1485
Published Date: 6 April 2024
Association Between the Time Spent on and Sources of the News of Russo-Ukrainian War and Psychological Distress Among Individuals in Poland and Ukraine: The Mediating Effect of Rumination
Li DJ, Chudzicka-Czupała A, Paliga M, Hapon N, Karamushka L, Żywiołek-Szeja M, McIntyre RS, Chiang SK, Chen YL, Yen CF, Man RHC
Psychology Research and Behavior Management 2024, 17:1855-1866
Published Date: 3 May 2024
Context Factors Associated with Medication Adherence Among Thai Adolescents with Major Depressive Disorder
Inwanna S, Matthews AK, Handrup CT, Steffen AD, Thongpan M, Abboud S
Patient Preference and Adherence 2025, 19:3769-3784
Published Date: 27 November 2025
Psychosocial and Biological Factors Associated with Non-Suicidal Self-Injury in Chinese Child and Adolescent Inpatients with Major Depressive Disorder
Liu C, Zhu XY, Shi YN, Wang PJ, Jiang WH, Zhou J, Qiu JC, Chen PF, Ding JC, Yan Q, Ding YQ
Neuropsychiatric Disease and Treatment 2026, 22:570371
Published Date: 24 January 2026