Back to Journals » Patient Preference and Adherence » Volume 19
Context Factors Associated with Medication Adherence Among Thai Adolescents with Major Depressive Disorder
Authors Inwanna S, Matthews AK, Handrup CT ![]() , Steffen AD, Thongpan M
, Steffen AD, Thongpan M ![]() , Abboud S
, Abboud S ![]()
Received 22 June 2025
Accepted for publication 23 October 2025
Published 27 November 2025 Volume 2025:19 Pages 3769—3784
DOI https://doi.org/10.2147/PPA.S540183
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Qizhi (Cathy) Yao
Suchanart Inwanna,1 Alicia K Matthews,2 Cynthia Taylor Handrup,3 Alana D Steffen,3 Masatha Thongpan,4 Sarah Abboud5
1Ramathibodi School of Nursing, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand; 2School of Nursing, Columbia University, New York, NY, USA; 3Department of Population Health Nursing Science, College of Nursing, University of Illinois Chicago, Chicago, IL, USA; 4Department of Psychiatry, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand; 5Department of Human Development Nursing Science, College of Nursing, University of Illinois Chicago, Chicago, IL, USA
Correspondence: Suchanart Inwanna, Ramathibodi School of Nursing, Faculty of Medicine Ramathibodi Hospital, Mahidol University, 270 Rama VI Road, Phayathai, Ratchathewi, Bangkok, 10400, Thailand, Email [email protected]
Purpose: Major depressive disorder (MDD) is a significant mental health issue among adolescents globally. In Thailand, medication adherence among adolescents with MDD is low. While international studies highlight factors such as family support and beliefs about medication, these may not apply to the Thai context, where cultural norms, stigma, and access to care differ. Guided by the Individual and Family Self-management Theory (IFSMT), this study explored context-specific factors influencing medication adherence among Thai adolescents with MDD.
Methods: A cross-sectional quantitative study was conducted with 146 adolescent-legal guardian dyads recruited via purposive sampling from two psychiatric outpatient clinics in Thailand. Guided by the IFSMT, the study assessed context factors across three domains: condition-specific, physical and social environment, and individual and family factors. To examine associations between IFSMT context factors and medication adherence, multiple linear regression analysis was performed. Written informed assent and consent were obtained.
Results: The adolescents (mean age = 16.16 years, 71.92% female) and legal guardians (mean age = 48.62 years, 77.40% female, 90.41% parents) completed the survey. Approximately 80% of adolescents reported low adherence to the guidelines. Three context factors were significantly associated with adherence: antidepressant side effects, adolescent preference for medication-only treatment, and legal guardian preference for medication-only treatment (p < 0.05). Other variables were not significant.
Conclusion: Medication adherence among Thai adolescents with MDD was associated with side effects and treatment preferences of both adolescents and their legal guardians. These findings highlight the importance of addressing individual and family preferences during treatment planning. Culturally informed interventions that consider these contextual influences may improve adherence outcomes. Future research should explore these factors further using longitudinal designs.
Keywords: context factors, adolescents, legal guardians, family, medication adherence, major depressive disorder
Introduction
Major depressive disorder (MDD) affects 8% of adolescents globally and is thus a significant public health concern.1 In Thailand, the prevalence of depression in adolescents is approximately 2.4%.2 MDD in this population is associated with increased risk of suicide—the leading cause of death among adolescents—and with other psychiatric conditions such as anxiety and substance use disorders.3,4 Notably, around 30% of children with MDD experience suicidality, and over 10% attempt suicide.5 Early detection of MDD and prompt selection of appropriate treatment for the condition are key to alleviating depressive symptoms, reducing the risk of suicide, and decreasing the risk of comorbidities, as well as helping adolescents succeed in school and maintain healthy relationships.6
In Thailand, a variety of antidepressant medications are used to treat adolescents with MDD, including sertraline and fluoxetine.7 Additionally, Thai clinical practice guidelines recommend treatment of depression with a combination of medication and cognitive behavioral therapy [CBT].7 Despite the availability of practical treatment approaches, the rate of depression relapse in adolescents is 38.6%, highlighting the significant challenges of managing MDD in Thailand.7
The rate of medication nonadherence in the world’s adolescent population with mental illness is worrisome, ranging from 8% to as high as 69%.8 Previous studies have identified various factors related to medication nonadherence that can be categorized into several groups,9 including patient, medication, clinician, structural, and environmental factors. Patient factors encompass patient characteristics and socioeconomic factors that influence the regular intake of medication. For example, patient-level barriers to adherence include negative treatment attitudes, misconceptions about antidepressants,9 and developmental stages and challenges.10 Medication factors include side effects and taking multiple medicines daily, referred to as pill burden,11 while clinician-related factors include inadequate communication of medication instructions, lack of shared decision-making, lack of follow-up treatment,9 and unsatisfactory clinician-patient relationships.12 Additionally, structural factors include social stigma, limited access to medication information, and high medication costs.9,11 Finally, environmental factors include the presence or absence of sufficient social support from family members.13 Although medication adherence studies have been conducted in multiple countries, none have examined factors related to medication adherence in the target population.
Moreover, during the adolescent developmental stage, individuals continue to develop physically, cognitively, psychosocially, and emotionally. At this stage of their development, adolescents may be limited in their ability to perceive and judge risk,8,14 which in turn may affect their understanding of the importance of administering their prescribed medication correctly or their ability to adhere to it.8,14,15 Therefore, adolescents’ medication adherence behaviors may depend at least partially on others, especially their parents and other family members, to ensure that the adolescents are taking their medications regularly.14,16 Several studies have investigated caregiver factors related to adolescents’ medication behaviors and found that caregivers’ attitudes toward medications, knowledge, and beliefs, as well as family function, were associated with their children’s adherence.16,17 In addition, a systematic review revealed several parental factors related to adolescents’ medication adherence, including socioeconomic status, education, family living status, roles of family functioning, and parents’ psychological health and attitudes toward psychotropic medication.8 Given these previous findings, meaningful examination of adolescents’ medication adherence must also consider the influences of family members. Based on the literature review, no studies have examined these influences among this population.
Therefore, the purpose of this study was to examine factors associated with medication adherence among Thai adolescents with MDD. This study employed the Individual and Family Self-Management Theory (IFSMT) as a theoretical framework to identify factors associated with adherence behaviors. Ryan and Sawin18 developed the IFSMT to improve individuals’ health outcomes, change health behaviors, increase quality of life, and decrease the cost of healthcare services. The IFSMT posits that both context factors (condition-specific, physical, and social environment, as well as individual and family factors) and process factors (knowledge and beliefs, self-regulation skills and abilities, and social facilitation) influence individuals’ health outcomes (see Figure 1). In this light, interventions developed based on the IFSMT have been found to increase individual and family self-management responsibility and to improve outcomes among patients with chronic conditions, such as knee osteoarthritis and chronic kidney disease, in Thailand and other countries.19–21 The IFSMT was chosen because it addresses both individual and family perspectives. Given the central role of family in Thai culture, IFSMT was most appropriate for examining adolescents’ and guardians’ perspectives on medication adherence. Moreover, no IFSMT-based studies have investigated the influence of context factors on medication adherence in this study population.
 |
Figure 1 Individual and family self-management theory.22 |
This study focused on context factors, as they can form the foundation for self-management behaviors. Medication adherence in adolescents is shaped by systemic and interpersonal influences—such as family dynamics, environmental support, and illness-related factors—that align with IFSMT’s context domains. Focusing solely on these factors allows for a more precise examination of their specific impact on medication adherence. Therefore, this study aimed to examine the direct association between context factors and medication adherence among Thai adolescents with MDD.
Based on the IFSMT, the conceptual model for this study consists of two major concepts: context factors and proximal outcomes. The context dimension encompasses condition-specific factors (receiving psychosocial intervention, medication regimens, depressive symptoms, and medication side effects), as well as physical and social environment factors (transportation barriers, stigma toward mental illness, and patient-doctor relationships), and individual and family factors (treatment preferences and family functioning). The proximal outcome is medication adherence. The researchers hypothesized that adolescent and family context factors are directly associated with the medication adherence behaviors of Thai adolescents (see Figure 2).
 |
Figure 2 Conceptual model of context factors for adolescents with MDD. Adapted from the IFSMT framework. |
Materials and Methods
Study Design and Sample
The study employed a quantitative, correlational, cross-sectional design to examine the relationships of key IFSMT context factors to proximal medication adherence behaviors. Based on the IFSMT, the researchers investigated the relationships between selected context factors, including condition-specific, physical, and social-environmental factors, individual and family factors, and the proximal outcome of medication adherence among adolescents with MDD. A purposive sampling approach was used to recruit participants. For each adolescent participant, the sample also included one legal guardian, such as a grandparent, uncle, aunt, or sibling, who was responsible for the adolescent’s primary care.
To support the study’s multiple regression analysis, a priori sample size estimation was conducted using a standard formula. Based on the study’s conceptual model, 10 context factors were specified as predictors in Set A, and four self-management process factors were included as predictors in Set B. Assuming a statistical power of 0.80, an alpha level of 0.01, and an anticipated effect size (f2) of 0.15, the minimum required sample size was 128 adolescent-legal guardian dyads. The final sample of 146 dyads exceeded this threshold, ensuring sufficient statistical power for the planned analysis.
Inclusion Criteria
Adolescent participants had to meet the following criteria: (1) aged 12 to 18 years, (2) diagnosed with MDD by a psychiatrist, (3) prescribed antidepressants and potentially other psychotropic medicines in at least three clinic visits while receiving treatment at the OPD, (4) visiting the clinic with their legal guardian, and (5) able to understand the Thai language well enough to complete the study survey. Adolescents with MDD and comorbid psychiatric conditions such as anxiety or attention-deficit/hyperactivity disorder were eligible to participate.
In addition, a participating legal guardian had to (1) be older than 18 years old, (2) serve as the primary caregiver for the adolescent with MDD, and (3) understand the Thai language well enough to complete the study survey.
Exclusion Criteria
We excluded adolescents whose medical records showed cognitive impairment or psychotic symptoms severe enough to prevent them from completing the study survey. Additionally, if either an adolescent or a legal guardian was excluded or unwilling to participate in the study, both members of the dyad were excluded from the study.
Procedures
Study approval was obtained from the Institutional Review Board (IRB) of the University of Illinois Chicago (UIC) and the Faculty of Medicine, Ramathobodi Hospital, Mahidol University, Bangkok, Thailand. Study activities were conducted in the outpatient department (OPD) settings at two university hospitals in Bangkok and Samut Prakarn provinces, Thailand. Potentially eligible participants were identified in advance through a review of hospital medical records, and they, along with their legal guardians, were approached in the waiting area. After being fully informed about the study, both the adolescent and the legal guardian signed written consent forms. We then offered two options to each adolescent and legal guardian: they could complete the study survey using paper-and-pencil questionnaires or online through UIC Research Electronic Data Capture (REDCap). All study procedures complied with the ethical principles outlined in the Declaration of Helsinki.
Two surveys were administered: the adolescent survey and the legal guardian survey. The adolescent survey consisted of 128 items, and the legal guardian survey contained 61 items, each measuring contextual factors. The surveys included separate researcher-developed socioeconomic questionnaires for adolescents and legal guardians. All but one of the standardized survey questionnaires had previously been translated into Thai. The Antidepressant Side-Effect Checklist was translated into Thai by the research team. For this questionnaire, we followed the translation and adaptation process recommended by the World Health Organization guidelines. Specifically, the process included forward and back translation; pre-testing of content validity by a panel of five Thai experts using a content validity index (CVI), with a resulting value of 1.0; and final confirmation of the translation by two bilingual Thai experts.
Measurements
The survey questionnaires were categorized into three groups: (1) sociodemographic data, (2) context factors (including condition-specific factors, the physical and social environment, and individual and family factors), and (3) proximal outcome (medication adherence). A summary of the measures employed in this study is provided in Table 1.
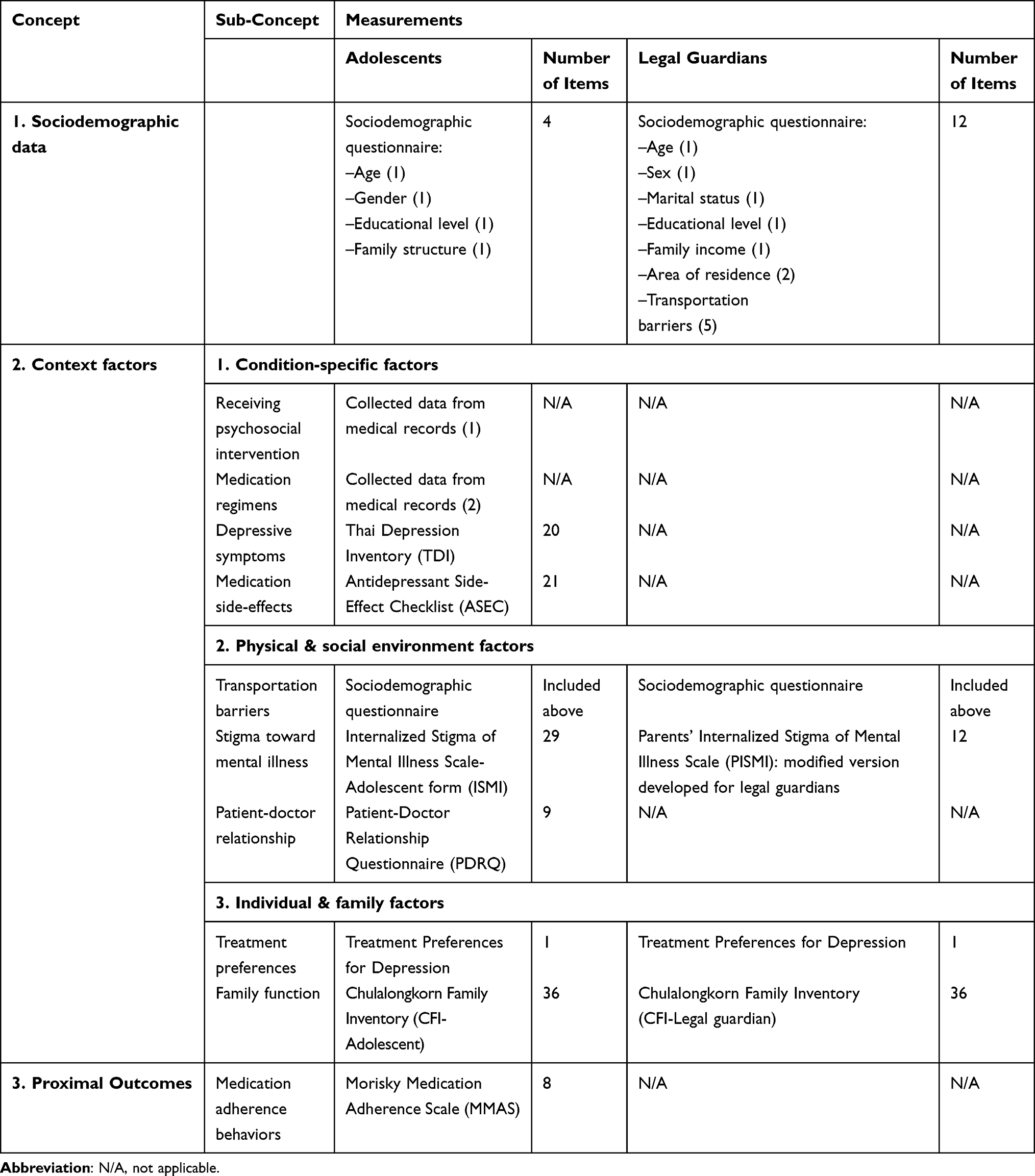 |
Table 1 Summary of Quantitative Variables and Measures |
Sociodemographic Data
The researchers used a single sociodemographic questionnaire for adolescents and a separate one for their legal guardians. For adolescents, standard questions were used to measure their age, gender, educational level, and family structure (ie, living with parents, living with one parent, or other arrangements). For legal guardians, standard questions were used to measure their age, gender, marital status, educational level, and family income.
Context Factors
Data addressing condition-specific factors, physical and social environment, and individual and family factors were collected using medical record reviews and self-report questionnaires.
1 Condition-specific Factors
As condition-specific factors, we collected data from adolescents on psychosocial interventions received, medication regimens, depressive symptoms, and medication side effects, as described below.
1.1 Psychosocial intervention received referred to adolescents receiving psychosocial interventions during MDD treatment to improve depressive symptoms. These included psychoeducation, cognitive-behavioral therapy, family-focused therapy, and interpersonal and social rhythms therapy. We reviewed each adolescent participant’s medical records to gather intervention data. If the participant was receiving an intervention, we recorded the type of intervention being administered.
1.2 Medication regimens referred to adolescents’ antidepressant prescriptions with respect to the number of medications prescribed (polypharmacy) and daily doses. We reviewed each adolescent participant’s medical record to gather these data. Specifically, we determined whether the adolescent was receiving prescribed medications and, if so, identified the specific medications and their frequency per day (as 1, 2, 3, or ≥ 4).
1.3 Depressive symptoms referred to adolescents’ current level of depressive symptom severity. The Thai Depression Inventory (TDI), a 20-item tool, was used to measure this variable. The TDI was developed by Thai psychiatrists.23 Each item is rated on a 4-point Likert scale ranging from 0 to 3 based on symptom severity during the previous week. The total TDI score can range from 0 to 60. Raw scores of less than 21 indicate no depression, 21 to 25 indicate mild depression, 26 to 34 indicate moderate depression, 35 to 40 indicate severe depression, and more than 40 indicate very severe depression. The TDI showed good internal consistency with a Cronbach’s alpha value of .86.23 In addition, the TDI showed good concurrent validity with the Hamilton Rating Scale for Depression for depressed patients (r = 0.72).23 In this study, the Cronbach’s alpha for the TDI was .88.
1.4 Medication side-effects referred to adolescents’ experience of side-effects of antidepressants prescribed by their psychiatrist. The Antidepressant Side-Effect Checklist (ASEC) was applied to measure 21 potential side effects in adolescents.24 For each item, the participants rated the severity of a symptom on a 4-point scale (0 = Absent, 1 = Mild, 2 = Moderate, 3 = Severe), and whether each symptom (if present) was a side-effect of antidepressants (by responding yes or no). In addition, three open-ended questions allowed participants to comment on the impact of adverse reactions to antidepressants; examples are “Have you had any treatment for a side-effect?” and “Has any side-effect led to you discontinuing the antidepressant medication?” Total ASEC scores can range from 0 to 63, with higher scores indicating a more severe effect profile.24 The ASEC previously demonstrated moderate internal consistency with a Cronbach’s alpha value of .78.24 In this study, the Cronbach’s alpha for the ASEC was .88.
2 Physical and Social Environment Factors
To assess physical and social environment factors, data were collected from both adolescents and their legal guardians. Adolescents provided self-reports on the quality of the patient-doctor relationship, and legal guardians reported on transportation barriers. Both adolescents and their legal guardians assessed perceived stigma toward mental illness.
2.1 Transportation barriers referred to travel barriers experienced by legal guardians between their area of residence and the two OPDs. We used four questions in the sociodemographic questionnaire to measure this factor.
2.2 Stigma toward mental illness referred to adolescents’ perspectives on social stigma toward MDD. To measure this variable, we used the Internalized Stigma of Mental Illness (ISMI) scale,25 which was available in the Thai language.26 This 29-item scale employs a 4-point Likert scale (1 = strongly disagree, 2 = disagree, 3 = agree, 4 = strongly agree). The total score ranges from 29 to 116. A higher score indicates that perceived internalized stigma is more severe and negative. The ISMI scale was found to have good internal consistency reliability with Cronbach’s alpha values ranging from .88 to .92.25,27 Moreover, the ISMI was reported to have excellent concurrent validity and divergent validity.25 In addition, the ISMI has been used among adolescents with mental illnesses such as attention deficit and hyperactivity disorder.28 In this study, the Cronbach’s alpha for the ISMI was .94.
To measure legal guardians’ perspectives on perceived stigma toward mental illness, the researchers used the modified Parents’ ISMI (PISMI).29 The modified PISMI consists of 12 items, and the total score ranges from 12 to 60, with higher scores indicating that legal guardians’ perceived internalized stigma was more severe and negative. The PISMI was reported to have moderate internal consistency, with a Cronbach’s alpha value of .76.29 In this study, the Cronbach’s alpha for the PISMI was .87.
2.3 Patient-doctor relationship referred to how much adolescents perceived their psychiatric healthcare providers as being effective and helpful in managing their disorder. Adolescent participants completed the Patient-Doctor Relationship Questionnaire (PDRQ-9),30 which had been previously translated into Thai.31 The PDRQ-9 has nine items, each requiring a response on a 5-point Likert scale (1 = not at all appropriate, 2 = somewhat appropriate, 3 = appropriate, 4 = mostly appropriate, 5 = totally appropriate). The total score ranges from 9 to 45, with higher scores indicating a more favorable relationship.32 Previous studies have shown that the PDRQ-9 has excellent internal consistency, with Cronbach’s alpha values ranging from .94 to .97.30,32 In this study, the Cronbach’s alpha for the PDRQ-9 was .93.
3. Individual and Family Factors
Adolescents’ and legal guardians’ treatment preferences and perspectives toward family function were measured.
3.1 Treatment preferences referred to the preference of adolescents and their legal guardians regarding treatment of MDD. To measure the treatment preferences of both adolescents and legal guardians, we used one item developed based on a previous systematic review study.33
3.2 Family function was measured from the perspectives of both adolescents and legal guardians using the Chulalongkorn Family Inventory (CFI), a self-report instrument developed in the Thai language by Trangkasombat.34 The 36 instrument items are rated on the following 4-point scale: 1 = Strongly disagree, 2 = Disagree, 3 = Agree, and 4 = Strongly agree. Total instrument scores range from 36 to 144, with higher scores indicating healthier family functioning. The CFI has demonstrated good internal consistency with Cronbach’s alpha values ranging from .88 to .92.34,35 In this study, the Cronbach’s alpha for the CFI in the adolescents’ dataset was .94 and in the legal guardians’ dataset was .92.
Proximal Outcome
Medication adherence refers to the behaviors surrounding medication-taking among adolescents, as prescribed by a psychiatrist, in terms of frequency and dosage. To measure this outcome, we utilized the eight-item Morisky Medication Adherence Scale (MMAS-8), a self-report instrument designed to assess medication-taking behavior.36 The MMAS-8 was translated into Thai by Sakthong, Chabunthom and Charoenvisuthiwongs.37 Items 1 through 7 use a dichotomous response scale (Yes = 1, No = 0), except for item 5, which is coded as Yes = 0 and No = 1. Item 8 was evaluated using a 5-point rating scale ranging from 1 to 0 (Never/Rarely = 1, Once in a while = 0.75, Sometimes = 0.50, Usually = 0.25, and All the time = 0). The possible total score ranges from 0 to 8, with higher scores indicating greater medication adherence.38 In addition, the MMAS-8 score was categorized into three groups: (1) 8 or higher indicated high medication adherence, (2) 6 to 8 indicated medium adherence, and (3) 5 or lower indicated low adherence.36 Morisky, Ang, Krousel-Wood and Ward36 reported that the MMAS-8 was reliable (Cronbach’s alpha = .83) and had good concurrent and predictive validity. In this study, the Cronbach’s alpha for the MMAS-8 was .70. (The license for this measure was purchased before its use in this study).
Statistical Analyses
The dataset in UIC REDCap was imported into STATA version 16.1 (StataCorp., College Station, TX, USA) for all study analyses. Descriptive and inferential statistics were used for analysis purposes. Univariate analysis was employed to examine participants’ characteristics and other study variables, yielding statistics including frequency distributions, percentages, means, and standard deviations (SD).
Testing for normal data distribution was conducted before the statistical analyses. For bivariate analyses, non-parametric tests were performed. Associations between medication adherence scores and independent variables were examined; Spearman’s rank correlation analysis was conducted for continuous independent variables, and the Mann–Whitney U-test was performed for categorical independent variables. Multiple linear regression assumptions were tested. To address the study objectives, we conducted stepwise regressions to identify the most significant context variables associated with medication adherence behaviors. During the stepwise process, independent variables with p-values greater than 0.2 were excluded from the model, while those with p-values less than 0.2 were retained.
Results
Adolescent Participant Characteristics
Among the 146 adolescent participants, the mean age was 16.16 years (SD = 1.58). Most participants (71.92%) were female and enrolled in high school (62.33%). About two-thirds (64.38%) of the adolescent participants lived with both biological parents, and approximately one-quarter (25.34%) lived with one biological parent. The majority of the participants had been diagnosed with MDD (86.99%), followed by persistent depressive disorder (PDD; 7.53%) or dysthymia (5.48%). While 65.75% of these participants reported no comorbidity, for the remaining participants, ADHD was the most commonly reported comorbidity (18.49%). All the participants had been prescribed antidepressants, which most participants combined with benzodiazepines (41.78%), antipsychotics (36.30%), or central nervous system (CNS) stimulants (19.18%). Table 2 summarizes the characteristics of the adolescent participants.
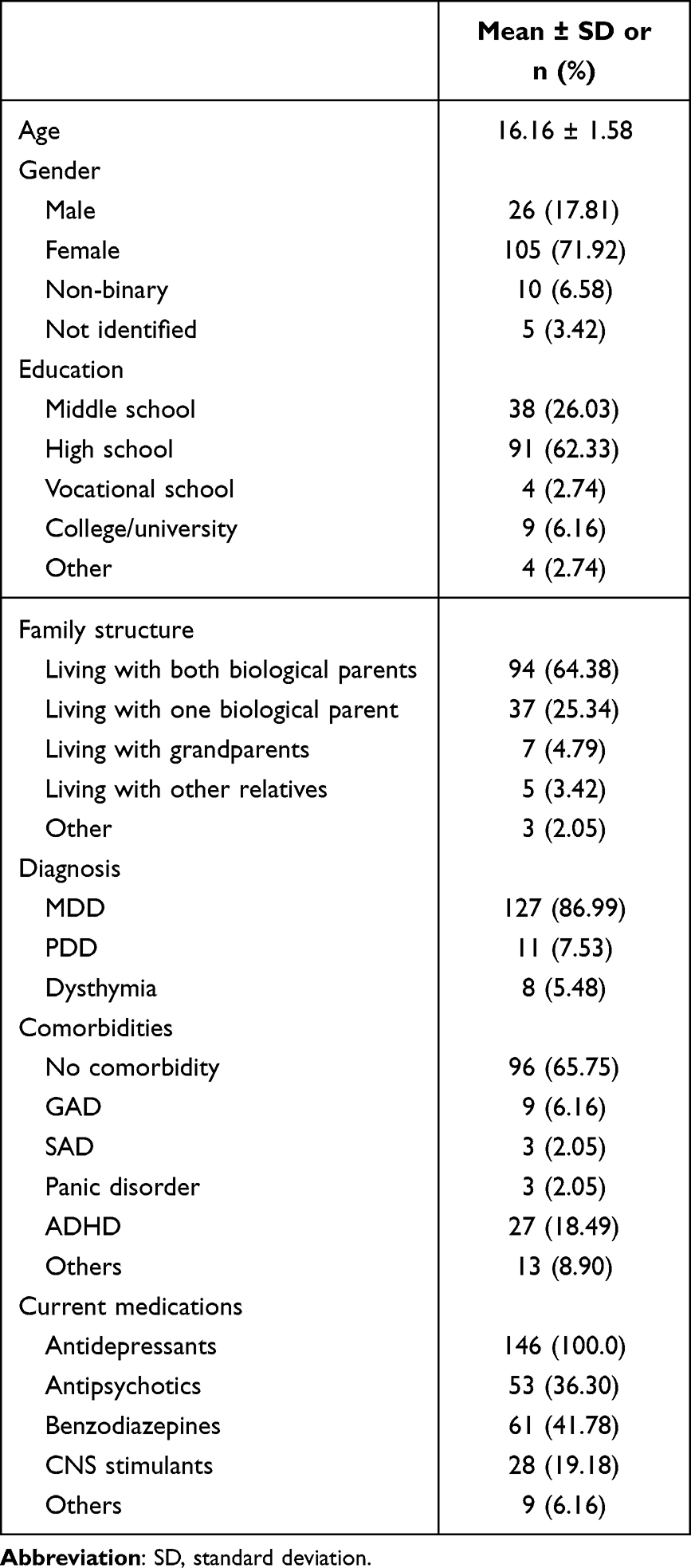 |
Table 2 Characteristics of Adolescent Participants (n = 146) |
Legal Guardian Participant Characteristics
The total number of legal guardian participants was 146, with a mean age of 48.62 years (SD = 6.73). Most of these participants were female (77.40%) and were parents of adolescent participants (90.41%). Among the legal guardian participants, about half had a bachelor’s degree (50.68%), and more than half were married (65.07%). Approximately 50% had a household income exceeding 50,001 Baht per month, which is a higher-than-average household income in Thailand, equivalent to approximately 1,348 USD. Most of these participants (89.04%) resided in Bangkok and its metropolitan areas. Additionally, the overall mean distance from their area of residence to the hospital they visited was 39.85 kilometers (SD = 81.77). Regarding access to transportation to the hospital, 54.11% of legal guardian participants used private vehicles, while 45.89% relied on public transportation. The median transportation cost was 300 Thai Baht, with 85.62% of participants reporting expenses of less than 500 Thai Baht. Given the transportation cost, most of these participants could afford to take their children to the hospital (97.95%). Table 3 summarizes the characteristics of the legal guardian participants.
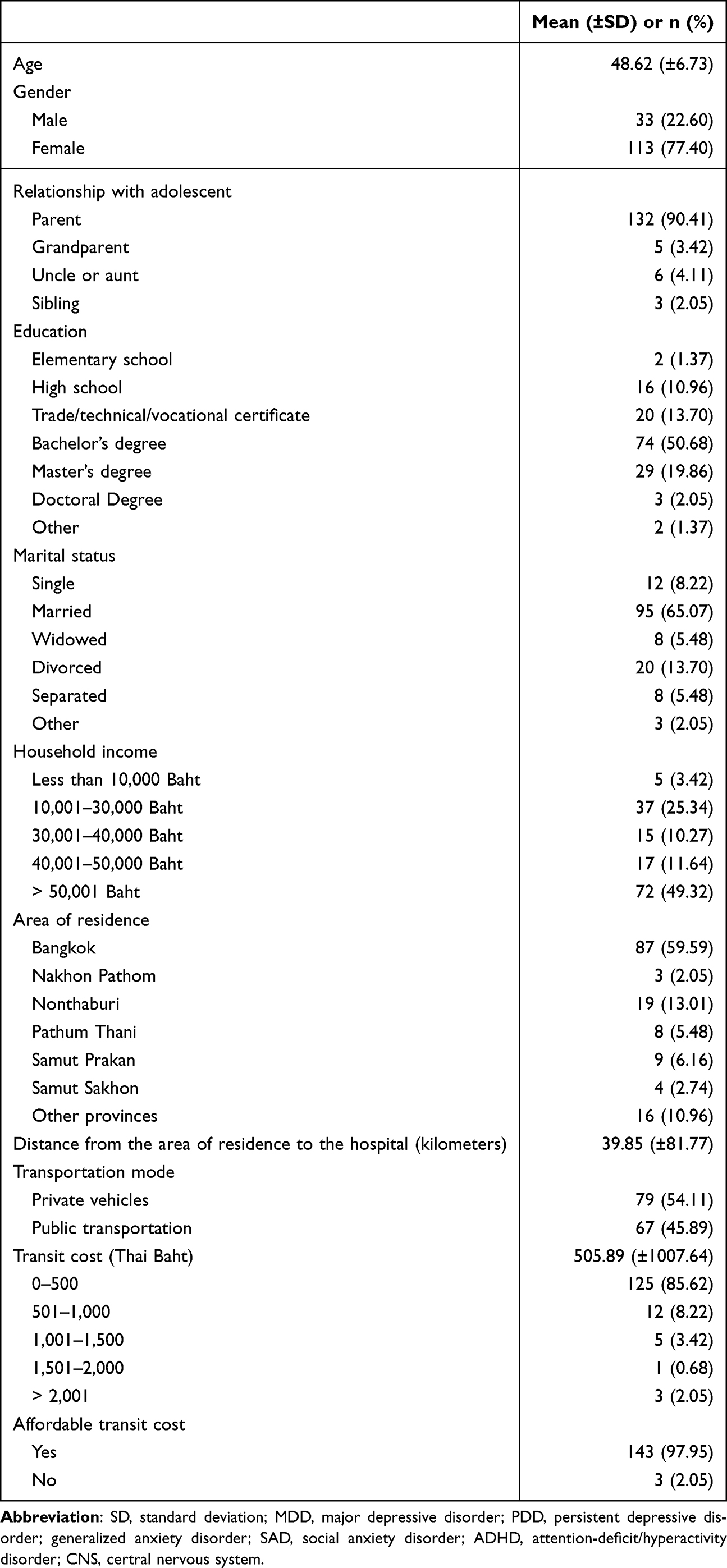 |
Table 3 Characteristics of Legal Guardian Participants (n = 146) |
Univariate Analysis: Context Factors and Medication Adherence
Condition-Specific Factors
Four condition-specific factors, including received psychosocial intervention, medication regimens, depressive symptoms, and medication side effects were analyzed. Received psychosocial intervention, medication regimens, and depressive symptoms were further described in Supplement Table 1.
Most participants (86.30%) did not receive psychosocial interventions. The most common frequency of prescribed medication was reported as two times per day by 45.89% of participants. Based on TDI results, varying proportions of the adolescent participants exhibited moderate depression (34.25%), severe depression (21.23%), and very severe depression (18.49%); the mean TDI score was 32.30 (SD = 10.21).
The mean ASEC score for experiencing antidepressant side effects was 22.06 (SD = 12.17), indicating a relatively low incidence of side effects (Supplement Table 2). Drowsiness, yawning, and insomnia were rated as the side effects of greatest severity by adolescent participants, with means of 1.92 (SD = 1.06), 1.89 (SD = 1.12), and 1.53 (SD = 1.16), respectively. Approximately 52.74% of participants reported that drowsiness was likely a side effect of antidepressant medication, while the prevalence of the other side effects was less than 50%. More than half of the participants expressed uncertainty about whether the listed side effects were related to antidepressants, with four participants specifically commenting on their uncertainty. One participant noted, “I don’t know the side effects.”
Physical and Social Environment Factors
Three physical and environmental factors were examined, including transportation barriers, stigma toward mental illness, and patient-doctor relationships.
Among the legal guardian participants, the most common transportation times were approximately 30 minutes to 1 hour (48.63%) and 1 to 2 hours (34.93%), with 22.6% reporting transportation issues. For stigma regarding mental illness, the mean ISMI-29 score among adolescent participants was 69.18 (SD = 14.24), indicating a somewhat severe and negative internalized stigma. The mean PISMI-12 score for legal guardians was 19.78 (SD = 12.90), indicating less severe and less negative internalized stigma. For the patient-doctor relationship, the mean PDRQ-9 score among adolescent participants was 36.53 (SD = 6.85), reflecting a relatively favorable relationship.
Individual and Family Factors
Two individual and family factors were measured: treatment preferences and family functioning. Adolescents primarily favored treatment with medication (72.60%), followed by psychotherapy (56.85%) and a combination of medication and psychotherapy (43.84%). Similarly, their legal guardians’ preferences for their treatment included medication (85.62%), psychotherapy (85.62%), and a combination of medication and psychotherapy (72.60%) (Supplement Table 3).
The mean CFI score for family functioning among adolescents was 97.27 (SD = 12.90), indicating relatively healthy family function. Similarly, among legal guardians, this score was 105.59 (SD = 9.74), also indicating relatively healthy family function.
Medication Adherence of Adolescent Participants
The mean MMAS-8 score for medication adherence behaviors was 3.95 (SD = 1.96), indicating low adherence. Based on MMAS-8 scores, adolescent participants were categorized into three groups: (1) low adherence, n = 118 (80.82%); (2) medium adherence, n = 26 (17.81%); and (3) high adherence, n = 2 (1.37%).
Among the MMAS-8 results, the most common adherence issue was forgetting to take medication, which was reported by 92.47% of participants. Approximately 73% (72.60%) reported taking all their medication the day prior to the survey, and 69.86% acknowledged occasionally forgetting to bring their medication when traveling. About 64.38% had missed taking medication for reasons other than forgetfulness. Over half (56.85%) reported feeling that taking medication daily was a burden. Regarding discontinuation behaviors, 39.04% had reduced or stopped their medication without informing their doctor, and 36.99% had stopped taking medication when they felt their condition was under control. In terms of remembering to take medication, 51.37% reported rarely or never having difficulty remembering, while 31.51% experienced difficulty “once in a while”, 12.33% “sometimes”, 3.42% “usually”, and 1.37% “all the time.”
Bivariate Analysis: Relationship of Context Factors to Medication Adherence
The bivariate analysis for continuous variables revealed a significant negative correlation between the experience of antidepressant side effects and medication adherence (rs = −0.20, p <0.05). In contrast, other variables did not show significant correlations (p >0.05) (Supplement Table 4).
Two variables, adolescents’ receipt of psychosocial intervention and legal guardians’ transportation issues, were analyzed using the Mann–Whitney U-test (Supplement Table 5). Adolescents without transportation issues showed significantly greater medication adherence than those who had experienced transportation issues (z = 2.121, p = 0.034). However, adolescents receiving psychosocial interventions showed no significant difference in medication adherence scores from those who received no such intervention (z = 0.302, p = 0.762).
In addition, treatment preferences showed no significant effect on medication adherence among adolescents, whether they preferred receiving medication only or psychotherapy (p >0.05). On the other hand, legal guardians who preferred medication-only treatment for their children showed a significant difference in their children’s medication adherence scores from legal guardians who did not prefer medication-only treatment (z = −2.14, p = 0.03). However, legal guardians’ preference for psychotherapy showed no significant effect on adolescents’ medication adherence (p =0.50). The associations between treatment preferences and medication adherence among adolescents and their legal guardians were provided in the Supplement Table 6.
One-way ANOVA was performed to compare the association of travel time on medication adherence scores, considering the travel time from participants’ areas of residence to the hospitals (<30 minutes, 30 minutes to 1 hour, 1 to 2 hours, and >2 hours). There was no significant association between travel time and medication adherence scores at the 0.05 level across the four conditions (F(3, 142) = 0.16, p = 0.933) (Supplement Table 7).
Regression Analysis: Effects of Context Factors on Medication Adherence
All context factors were entered in the stepwise regression model, and five variables together accounted for 14.07% of the variance in the medication adherence score (R2 =0.1407, F(5, 140) = 4.59, p <0.001). Of these, three variables showed significant associations with medication adherence scores: antidepressant side effects (Beta = −0.027, p = 0.035), adolescent’s preferred medication-only treatment (Beta =0.786, p = 0.034), and legal guardian’s preferred medication-only treatment for their child (Beta = 1.025, p = 0.022). The two remaining predictor variables—legal guardians’ experience of transportation issues and adolescents’ preferred psychotherapy treatment— were not significantly associated with medication adherence scores (Beta = −0.725, p = 0.052 and Beta = −0.545, p = 0.104, respectively) (see Table 4).
 |
Table 4 Regression Analysis of Contextual Factors Associated with Medication Adherence |
Discussion
This study examined the relationship between IFSMT context factors and medication adherence among Thai adolescents with MDD. To our knowledge, it is among the first studies to explore these factors in Thailand among both adolescents and their legal guardians. Approximately 80% of adolescent participants reported low medication adherence—higher than the 58% to 73% doing so in a systematic review of adolescents with chronic illness.39 Among the context variables, three factors were significantly associated with medication adherence: antidepressant side effects, adolescent preference for medication-only treatment, and legal guardian preference for medication-only treatment.
Adverse antidepressant side effects—particularly drowsiness and yawning—may interfere with adolescents’ school performance and daily functioning, contributing to nonadherence. Limited knowledge about these side effects was observed among the study’s adolescent participants. As prior research suggests a positive link between health literacy and adherence,40 efforts to improve mental health literacy among adolescents and their families are essential.
Treatment preferences also showed significant associations with medication adherence. Both adolescents and their legal guardians showed a preference for medication-only treatment, which was associated with higher adherence. These results contrast with findings of some earlier research in which counseling was favored41 and may reflect the participants’ strong trust in medication efficacy and healthcare provider recommendations. Given these results, incorporating shared decision-making and psychoeducation into care may support long-term adherence.42
Several context factors were not significantly associated with adherence. Transportation barriers, for example, did not significantly influence medication adherence—likely due to consistent family support, as all adolescents attending appointments were accompanied by legal guardians who covered the transportation costs. Some families also accessed telehealth, further reducing logistical challenges.
Adjunct psychosocial interventions were also not significantly related to medication adherence, possibly due to low utilization of such interventions (13.7%) and lack of intervention content on adherence. Similarly, medication regimen complexity (eg, dosing frequency) was not associated with medication adherence, possibly because most adolescents received family assistance with their daily medication routines.
In addition, depressive symptom severity, perceived stigma, patient-provider relationships, and family functioning were not significantly associated with medication adherence. By way of explanation, the lack of association with depression severity may stem from limited variability in adolescents’ symptom levels, and social media exposure and evolving adolescent autonomy may have influenced perceptions of stigma and healthcare relationships.43,44 Furthermore, the non-significance of family functioning could indicate that some adolescents adapted to poor family environments by developing independent medication management strategies.8
While this study focused on adolescent and family context factors, it is important to recognize that other influences—such as peer relationships and the broader school environment—may also contribute to adherence behaviors. Alternative theoretical perspectives, such as the social-ecological model and family systems theory, also highlight that adolescent medication adherence is shaped by multiple, interacting layers of influence beyond the individual and family. These considerations, along with related limitations, are discussed further in the Limitations section.
In summary, this study highlights that among various context factors, antidepressant side effects and both adolescent and guardian treatment preferences were significantly associated with medication adherence. These findings support the IFSMT framework, underscoring the direct influence of context on self-management outcomes. Future research should further explore these relationships to inform culturally tailored interventions for improving medication adherence among adolescents with MDD.
Strengths and Limitations
This study addresses a significant public health concern by investigating factors associated with medication adherence among Thai adolescents with MDD. The study offers a deeper understanding of the influence of context factors on adherence, and the application of the IFSMT enhances its conceptual rigor. An additional strength is its innovative approach, incorporating perspectives from both adolescents and their legal guardians to identify key factors influencing adherence behaviors. The findings provide a strong foundation for developing targeted interventions to promote medication adherence and reduce non-adherence in a vulnerable adolescent population.
Several limitations should also be acknowledged. First, the adolescent-legal guardian dyads were recruited using relatively narrow inclusion and exclusion criteria, and data were primarily collected from urban and suburban areas, as well as a predominantly female adolescent sample. These factors may limit the generalizability of the findings to the broader population of Thai adolescents with MDD and their families. Additionally, approximately 13% of the adolescent participants had been diagnosed with persistent depressive disorder or dysthymia rather than MDD. While these conditions are generally less severe than MDD, they are chronic depressive disorders that also require long-term antidepressant treatment,45 justifying their inclusion in this study. The use of purposive sampling may not have captured the full diversity of experiences and characteristics within the adolescent MDD population.
Second, the study’s cross-sectional design limits the ability to capture dynamic adherence patterns and draw causal inferences about the relationships between context factors and medication adherence. Additionally, unmeasured factors such as peer influence and school environment may also play a role in adolescents’ adherence behaviors. Additionally, the relatively small sample size may have limited the study’s statistical power to detect certain associations.
Third, the analytic approach has limitations. The bivariate analyses were presented to provide transparency by reporting exact p-values and effect sizes; however, such unadjusted associations may not fully account for potential confounding factors and should be interpreted as exploratory rather than causal. Although we consistently applied a two-sided α = 0.05 for all analyses, the α = 0.01 reported in the sample size calculation section reflected only a conservative planning assumption. We did not apply formal adjustments for multiple comparisons, so the possibility of an inflated Type I error cannot be excluded; accordingly, readers are encouraged to place greater emphasis on effect sizes and overall association patterns rather than relying solely on p-values. Furthermore, in our analysis, adolescent–guardian dyads were treated as the unit of analysis, with one observation per dyad in the dataset. This approach preserved the paired nature of the data but may not have fully addressed potential within-dyad correlation. Therefore, future studies employing dyadic or mixed-model approaches may provide additional insights.
Finally, reliance on self-report instruments may have introduced bias in assessing participants’ behaviors.
Implications for Clinical Practice and Future Research
This study identified key context factors—particularly antidepressant side effects and treatment preferences of both adolescents and their legal guardians—that showed significant associations with medication adherence among Thai adolescents with MDD. These findings can guide psychiatric nurses and mental health professionals in developing targeted interventions to promote adherence and improve clinical outcomes.
A key clinical implication is the integration of psychoeducation into routine outpatient care. Providing adolescents and their caregivers with information about the expected side effects of psychotropic medications, their duration, and management strategies may enhance understanding, reduce anxiety, and support adherence. Encouraging adolescents to communicate openly about their experiences with side effects can also help providers tailor treatment plans and select medications with more tolerable profiles.
To further support medication adherence, healthcare providers should prioritize enhancing mental health literacy—particularly regarding pharmacologic treatments—through psychopharmacology-informed interventions. Empowering adolescents and their legal guardians with this knowledge can promote shared decision-making and strengthen engagement in treatment.
For future research, studies with larger and more diverse samples are needed to fully examine the influence of depressive symptom severity and other context variables. Longitudinal designs should incorporate context variables, such as peer networks and school environments, to better understand adherence trajectories. Also, alternative theoretical frameworks may enrich understanding when examined alongside IFSMT. Additionally, research in rural populations and among underrepresented genders is necessary to ensure findings are generalizable. Finally, incorporating objective measures—such as electronic medication monitoring, pill counts, or biomarkers—can improve the accuracy of adherence assessment beyond self-reported measurements.
Conclusion
Medication adherence is critical for adolescents with MDD to reduce symptoms and support both short- and long-term quality of life. This study is the first in Thailand to examine how context factors influence medication adherence in this population. The findings suggest that adolescents’ experience of antidepressant side effects, as well as treatment preferences of both adolescents and their legal guardians, are important context factors associated with medication adherence behaviors. Clinicians can use these insights to assess adherence and identify potential barriers in practice more effectively. Additionally, the results provide foundational insight for researchers designing interventions aimed at improving low medication adherence rates and promoting sustained adherence.
Acknowledgments
The authors wish to acknowledge the editorial contribution of Mr. Jon Mann, University of Illinois at Chicago, during the development of this manuscript.
This manuscript is derived from the first author’s doctoral thesis, Medication Adherence among Thai Adolescents with Major Depressive Disorder, which is publicly available in the University of Illinois Chicago institutional repository (Indigo): https://indigo.uic.edu/articles/thesis/Medication_Adherence_among_Thai_Adolescents_with_Major_Depressive_Disorder/27152184.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Shorey S, Ng ED, Wong CHJ. Global prevalence of depression and elevated depressive symptoms among adolescents: a systematic review and meta-analysis. Brit J Clin PsychoL. 2022;61(2):287–305. doi:10.1111/bjc.12333
2. Department of Mental Health. The prevalence of major depressive disorder in Thai population aged 15 and over; 2022. Available from http://healthkpi.moph.go.th/kpi/kpi-list/view/?id=780.
3. Thanoi W, Phancharoenworakul K, Thompson EA, Panitrat R, Nityasuddhi D. Thai adolescent suicide risk behaviors: testing a model of negative life events, rumination, emotional distress, resilience and social support. Pac Rim Int J Nurs Res. 2013;14(3):187–202 Available from https://he02.tci-thaijo.org/index.php/PRIJNR/article/view/6274.
4. United Nations International Children’s Emergency Fund. A situation analysis of adolescents in Thailand 2015–2016; 2021. Available from https://www.unicef.org/thailand/sites/unicef.org.thailand/files/2018-08/adolescent-situation-analysis-thailand-en.pdf.
5. Walter HJ, Abright AR, Bukstein OG, et al. Clinical practice guideline for the assessment and treatment of children and adolescents with major and persistent depressive disorders. Am Acad Child Adolesc Psychiatry. 2023;62(5):479–502. doi:10.1016/j.jaac.2022.10.001
6. Beirão D, Monte H, Amaral M, Longras A, Matos C, Villas-Boas F. Depression in adolescence: a review. Middle East Curr Psychiatry. 2020;27(1):50. doi:10.1186/s43045-020-00050-z
7. Prukkanone B, Vos T, Bertram M, Lim S. Cost-effectiveness analysis for antidepressants and cognitive behavioral therapy for major depression in Thailand. Value Health. 2012;15(1 Suppl):S3–8. doi:10.1016/j.jval.2011.11.009
8. Kalaman CR, Ibrahim N, Shaker V, et al. Parental factors associated with child or adolescent medication adherence: a systematic review. Healthcare. 2023;11(4):501. doi:10.3390/healthcare11040501
9. Dell’Osso B, Albert U, Carrà G, et al. How to improve adherence to antidepressant treatments in patients with major depression: a psychoeducational consensus checklist. Ann Gen Psychiatry. 2020;19(1):61. doi:10.1186/s12991-020-00306-2
10. Taddeo D, Egedy M, Frappier JY. Adherence to treatment in adolescents. Paediatr Child Health. 2008;13(1):19–24. doi:10.1093/pch/13.1.19
11. Marasine NR, Sankhi S. Factors associated with antidepressant medication non-adherence. Turk J Pharm Sci. 2021;18(2):242–249. doi:10.4274/tjps.galenos.2020.49799
12. Staton D. Achieving adolescent adherence to treatment of major depression. Dolesc Health Med Ther. 2010;1:73–85. doi:10.2147/ahmt.S8791
13. Sloand E, Butz A, Rhee H, et al. Influence of social support on asthma self-management in adolescents. J Asthma. 2021;58(3):386–394. doi:10.1080/02770903.2019.1698601
14. Sanders RA. Adolescent psychosocial, social, and cognitive development. Pediatr Rev. 2013;34(8):354–359. doi:10.1542/pir.34-8-354
15. El-Rachidi S, LaRochelle JM, Morgan JA. Pharmacists and pediatric medication adherence: bridging the gap. Hosp Pharm. 2017;52(2):124–131. doi:10.1310/hpj5202-124
16. Ge P, Liu ST, Xu SX, et al. The influence of parents on medication adherence of their children in China: a cross-sectional online investigation based on health belief model. Front Public Health. 2022;10:845032. doi:10.3389/fpubh.2022.845032
17. Psihogios AM, Fellmeth H, Schwartz LA, Barakat LP. Family functioning and medical adherence across children and adolescents with chronic health conditions: a meta-analysis. Pediatr Psychol. 2019;44(1):84–97. doi:10.1093/jpepsy/jsy044
18. Ryan P, Sawin KJ. The individual and family self-management theory: background and perspectives on context, process, and outcomes. Nur Outlook. 2009;57(4):217–225.e6. doi:10.1016/j.outlook.2008.10.004
19. Bunsanong T, Chaimongkol N. A self-management support intervention on knee functional status and health-related quality of life among middle-age women: a randomized controlled trial. J Adv Nurs. 2021;77(1):376–386. doi:10.1111/jan.14600
20. Lucas R, Zhang Y, Walsh SJ, Evans H, Young E, Starkweather A. Efficacy of a breastfeeding pain self-management intervention: a pilot randomized controlled trial. Nurs Res. 2019;68(2):E1–e10. doi:10.1097/nnr.0000000000000336
21. Sezer TA, Çavuşoğlu H, Düzova A. Self-management program for adolescents with chronic kidney disease: a randomized controlled trial. J Ren Care. 2021;47(3):146–159. doi:10.1111/jorc.12357
22. Ryan P, Sawin KJ. Individual and family self-management theory (IFSMT). Available from https://uwm.edu/nursing/centers-institutes/self-management-science-center/theory/.
23. Lotrakul M, Sukanich P. Development of the Thai depression inventory. J Med Assoc Thai. 1999;82(12):1200–1207 Available from https://pubmed.ncbi.nlm.nih.gov/10659561/.
24. Uher R, Farmer A, Henigsberg N, et al. Adverse reactions to antidepressants. Br J Psychiatry. 2009;195(3):202–210. doi:10.1192/bjp.bp.108.061960
25. Ritsher JB, Otilingam PG, Grajales M. Internalized stigma of mental illness: psychometric properties of a new measure. Psychiatry Res. 2003;121(1):31–49. doi:10.1016/j.psychres.2003.08.008
26. Wong-Anuchit C, Mills AC, Schneider JK, Rujkorakarn D, Kerdpongbunchote C, Panyayong B. Internalized stigma of mental illness scale - Thai version: translation and assessment of psychometric properties among psychiatric outpatients in central Thailand. Arch Psychiatr Nurs. 2016;30(4):450–456. doi:10.1016/j.apnu.2016.01.012
27. Dikeç G, Bilaç Ö, Uzunoğlu G, Ozan E. Validity and reliability of the internalized stigma of mental illness scale–adolescent form. J Child Adolesc Psychiatr Nurs. 2021;34(2):96–104. doi:10.1111/jcap.12300
28. Dikeç G, Bilaç Ö, Kardelen C, Sapmaz, ŞY. Do we learn to internalize stigma from our parents? Comparison of internalized stigmatization in adolescents diagnosed with ADHD and their parents. Adolescents. 2022;2(4):439–447. doi:10.3390/adolescents2040034
29. Zisman-Ilani Y, Levy-Frank I, Hasson-Ohayon I, Kravetz S, Mashiach-Eizenberg M, Roe D. Measuring the internalized stigma of parents of persons with a serious mental illness: the factor structure of the parents’ internalized stigma of mental illness scale. J Nerv Ment Dis. 2013;201(3):183–187. doi:10.1097/NMD.0b013e3182845d00
30. Van der Feltz-Cornelis CM, Van Oppen P, Van Marwijk HWJ, De Beurs E, Van Dyck R. A patient-doctor relationship questionnaire (PDRQ-9) in primary care: development and psychometric evaluation. Gen Hosp Psychiatry. 2004;26(2):115–120. doi:10.1016/j.genhosppsych.2003.08.010
31. Pitanupong J, Sammathit J. Knowledge and attitudes on medication adherence and residual symptoms in individuals with depression: a survey at a University Hospital. BMC Psychiatry. 2023;23(1):210. doi:10.1186/s12888-023-04706-y
32. Calderón C, Lorenzo-Seva U, Ferrando PJ, et al. Psychometric properties of the PDRQ-9 in cancer patients: patient-doctor relationship questionnaire. Psicothema. 2021;33(2):304–311. doi:10.7334/psicothema2020.393
33. Gelhorn HL, Sexton CC, Classi PM. Patient preferences for treatment of major depressive disorder and the impact on health outcomes: a systematic review. Prim Care Companion CNS Disord. 2011;13(5):
34. Trangkasombat U. Family functioning in the families of psychiatric patients: a comparison with nonclinical families. J Med Assoc Thai. 2006;89(11):1946–1953 Available from https://pubmed.ncbi.nlm.nih.gov/17205879/.
35. Puasiri S, Sitthimongkol Y, Tilokskulchai F, Sangon S, Nityasuddhi D. Adaptation of Thai families with mentally ill young people. Pac Rim Int J Nurs Res. 2013;15(2):137–151 Available from https://he02.tci-thaijo.org/index.php/PRIJNR/article/view/6521.
36. Morisky DE, Ang A, Krousel-Wood M, Ward HJ. Predictive validity of a medication adherence measure in an outpatient setting. J Clin Hypertens. 2008;10(5):348–354. doi:10.1111/j.1751-7176.2008.07572.x
37. Sakthong P, Chabunthom R, Charoenvisuthiwongs R. Psychometric properties of the Thai version of the 8-item Morisky medication adherence scale in patients with type 2 diabetes. Ann Pharmacother. 2009;43(5):950–957. doi:10.1345/aph.1L453
38. Silavanich V, Nathisuwan S, Phrommintikul A, Permsuwan U. Relationship of medication adherence and quality of life among heart failure patients. Heart Lung. 2019;48(2):105–110. doi:10.1016/j.hrtlng.2018.09.009
39. Yang C, Hao Z, Yu D, Xu Q, Zhang L. The prevalence rates of medication adherence and factors influencing adherence to antiepileptic drugs in children with epilepsy: a systematic review and meta analysis. Epilepsy Res. 2018;142:88–99. doi:10.1016/j.eplepsyres.2018.03.018
40. Miller TA. Health literacy and adherence to medical treatment in chronic and acute illness: a meta-analysis. Patient Educ Couns. 2016;99(7):1079–1086. doi:10.1016/j.pec.2016.01.020
41. Jaycox LH, Asarnow JR, Sherbourne CD, Rea MM, LaBorde AP, Wells KB. Adolescent primary care patients’ preferences for depression treatment. Adm Policy Ment Health. 2006;33(2):198–207. doi:10.1007/s10488-006-0033-7
42. Krist AH, Tong ST, Aycock RA, Longo DR. Engaging patients in decision-making and behavior change to promote prevention. Stud Health Technol Inform. 2017;240:284–302. doi:10.3233/ISU-170826
43. Christie D, Viner R. Adolescent development. BMJ. 2005;330(7486):301–304. doi:10.1136/bmj.330.7486.301
44. Harris M. How social media is changing the way we think about mental illness; 2021. Available from https://www.nami.org/media-and-pop-culture/how-social-media-is-changing-the-way-we-think-about-mental-illness/.
45. MacQueen G, Santaguida P, Keshavarz H, et al. Systematic review of clinical practice guidelines for failed antidepressant treatment response in major depressive disorder, dysthymia, and subthreshold depression in adults. Can J Psychiatry. 2017;62(1):11–23. doi:10.1177/0706743716664885
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Insomnia and Alexithymia in Chinese Adolescents with Major Depressive Disorder: A Cross-Sectional Study of Sex Differences and Associations
Yang X, Liu L, Tian Y, Yang C, Ling C, Liu H
Psychology Research and Behavior Management 2024, 17:615-625
Published Date: 20 February 2024
The Association Between Medication Adherence, Internalized Stigma and Social Support Among Outpatients with Major Depressive Disorder in a Malaysian Hospital: A Cross-Sectional Study
Halim R, Kaur M, Syed Mokhtar SS, Chemi N, Sajatovic M, Tan YK, Siau CS, Ng CG
Psychology Research and Behavior Management 2025, 18:209-223
Published Date: 4 February 2025
Psychosocial and Biological Factors Associated with Non-Suicidal Self-Injury in Chinese Child and Adolescent Inpatients with Major Depressive Disorder
Liu C, Zhu XY, Shi YN, Wang PJ, Jiang WH, Zhou J, Qiu JC, Chen PF, Ding JC, Yan Q, Ding YQ
Neuropsychiatric Disease and Treatment 2026, 22:570371
Published Date: 24 January 2026
Impact of Adverse Childhood Experiences and Rumination on Metacognition in Chinese Urban Adolescents with Major Depressive Disorder
Li J, Zhu J, Zhou B, Sun J, Zhou S, Qi M, Chen J
Psychology Research and Behavior Management 2026, 19:555078
Published Date: 11 March 2026
Efficacy and Safety of Escitalopram for Major Depressive Disorder in Children and Adolescents: A Systematic Review and Meta-Analysis with Age-Specific Findings
Maneeton B, Maneeton N, Pojanapotha P, Putthisri S, Oon-arom A, Karawekpanyawong N, Kawilapat S, Maneeton P, Srichan K
Neuropsychiatric Disease and Treatment 2026, 22:595606
Published Date: 5 May 2026