")
Back to Journals » Psychology Research and Behavior Management » Volume 17
Insomnia and Alexithymia in Chinese Adolescents with Major Depressive Disorder: A Cross-Sectional Study of Sex Differences and Associations
Authors Yang X , Liu L, Tian Y, Yang C, Ling C, Liu H
Received 26 October 2023
Accepted for publication 29 January 2024
Published 20 February 2024 Volume 2024:17 Pages 615—625
DOI https://doi.org/10.2147/PRBM.S446788
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Professor Mei-Chun Cheung
Xiaoxue Yang,1– 3 Lewei Liu,1– 3 Yinghan Tian,1– 3 Cheng Yang,1– 3 Chen Ling,1– 3 Huanzhong Liu2,3
1Department of Psychiatry, School of Mental Health and Psychological Sciences, Anhui Medical University, Hefei, Anhui Province, People’s Republic of China; 2Department of Psychiatry, Chaohu Hospital of Anhui Medical University, Hefei, Anhui Province, People’s Republic of China; 3Anhui Psychiatric Center, Anhui Medical University, Hefei, Anhui Province, People’s Republic of China
Correspondence: Huanzhong Liu, Department of Psychiatry, Chaohu Hospital of Anhui Medical University, Hefei, Anhui Province, People’s Republic of China, Tel +86-551-82324616, Fax +86-551-82324252, Email [email protected]
Purpose: Insomnia is related to alexithymia in adults, but the relationship between insomnia and alexithymia in adolescents with major depressive disorder remains unclear. This study aimed to investigate the sex differences and the association between insomnia and alexithymia in adolescents with major depressive disorder.
Patients and Methods: From October 2020 to April 2022, adolescent patients with major depressive disorder were recruited from psychiatric departments of seven hospitals in Anhui Province, China. Their general demographic and clinical information were collected. The 20-item Toronto Alexithymia Scale, the Center for Epidemiologic Studies of Depression Scale, and the Insomnia Severity Index Scale were used to assess their alexithymia, depression, and insomnia symptoms, respectively. The analysis of variance (ANOVA), Student’s t-test and Mann–Whitney U-test were used for continuous variables and chi-square tests for categorical variables. Pearson’s correlation analysis and Spearman correlation analysis were used to examine the correlation between ISI and demographic and clinical variables. Multiple binary logistic regression analyses with the “Enter” method were carried out to explore the correlations of insomnia.
Results: The prevalence of insomnia in female adolescent patients was similar to that of male patients (χ2=1.84, p = 0.175). Compared with those without insomnia, patients with insomnia had worse family relationships (F = 7.71, p = 0.021), perceived heavier academic stress (F = 6.32, p = 0.012), more likely to take sedative-hypnotics (F = 5.51, p = 0.019), had higher levels of depression (F = 81.57, p < 0.001) and alexithymia (F = 28.57, p < 0.001). Correlation analysis showed that alexithymia was significantly associated with insomnia in adolescent patients (r = 0.360, p < 0.01). Binary logistic regression analyses showed that, alexithymia was significantly associated with insomnia in female patients (OR = 1.050, p < 0.05) but not male patients.
Conclusion: In female adolescent patients, alexithymia is a risk factor of insomnia, which is of great importance in the understanding of the psychopathological mechanisms, treatments and psychological interventions of insomnia in adolescents with major depressive disorder.
Keywords: adolescents, major depressive disorder, insomnia, alexithymia
Introduction
Major depressive disorder (MDD) is a significant mental disease and one of the leading causes of years lived with disability (YLDs).1 The global point prevalence of MDD in adults (aged 18–99 years) is around 4.7%.2 Adolescents is vulnerable to mental disorders due to the physiological and psychological changes. Across adolescents aged 10–19 years, the global point prevalence and the lifetime prevalence rate of MDD are 8% and 19%, respectively.3 Sleep disturbances often occur in patients with MDD and are the most prominent symptom in many circumstances. It is reported that the insomnia rate in patients with a major depressive episode (MDE) is 85.2%.4 At least two thirds of adolescents with MDD experienced insomnia.5 Evidence shows that insomnia and depression have a closely two-way relationship.6 According to a meta-analysis, children and adolescents with sleep disorders are more likely to develop depression.7 A cohort study showed that compared to healthy controls, the risk of insomnia increased by 2–3 times in adolescents with depression.8 In patients with MDD, more severe insomnia symptoms indicate worse health-related outcomes.9 Thus, it is vital to reveal the risk factors of insomnia in MDD patients.
Current studies have confirmed several insomnia-related factors, such as age, sex, heredity, characteristics, life events, stress, unhealthy sleep behaviors and emotions. A body of researches have investigated the relationship between alexithymia and sleep problems and suggested that alexithymia is also a possible factor that related to sleep disturbances.10 Alexithymia is a psychological trait including two aspects: difficulty identifying and describing emotions and externally oriented thinking.11 It is correlated to a series of physical and psychiatric disorders and may be a susceptible factor for a range of symptoms in various diseases.12 An early survey of a group of Japanese working men showed that sleep characteristics including insomnia are related to high scores of alexithymia.13 Another study that conducted in a representative Finnish adult population reported independent correlation between alexithymia and sleep disorder symptoms.14 In a sample of young adults, alexithymia participants scored more on sleep symptoms including insomnia than the non-alexithymia ones.15 In another sample of college students, alexithymia is positively correlated with insomnia.16 A research confirmed that in two online-recruited healthy adult groups, alexithymia is associated with poor sleep quality, and the association is dependent from the co-occurring depression or anxiety.17 There are also studies reaching the same conclusions in the depression participants.18 While few studies applied objective measurements of sleep, Bazydlo et al have reported association between alexithymia with more light sleep and less deep sleep.19
Although, among all the legible studies, few researches have been conducted on the underage population. In fact, there is growing evidence that alexithymia may have the same adverse effects on their health as adults.20 Moreover, patients with MDD may find it challenging to identify and describe emotions subjectively since they usually use emotional inhibition strategies to protect themselves from distress, consequently, patients with MDD experience more severe alexithymia than those with other psychiatric disorders.21 Therefore, it is necessary to explore the relationship of insomnia and alexithymia in adolescent MDD patients.
It is worth noticing that in adolescent populations, there is sex differences not only in the prevalence rate of MDD but also in the clinical symptoms of MDD. For example, male adolescents are less likely to experience insomnia, and female adolescents display more affective and atypical symptoms.22 There are also sex differences in alexithymia as well as in insomnia. On the one hand, the risk of alexithymia in men is higher than that of women.23 Previous study found that alexithymia is related to an imbalance in the noradrenergic and basal activity of the hypothalamic–pituitary–adrenal axis in male MDD patients.24 Moreover, alexithymia is correlated with deficiencies in right hemisphere function and interhemispheric transfer in men, not women.25 On the other hand, objective sleep measurements showed different polysomnography (PSG) sleep parameters in early-onset MDD male and female patients.26 Therefore, in this study, while investigating the association between insomnia and alexithymia in adolescent patients with MDD, we also paid attention to the sex differences in the association.
Taken together, the focus of this study was to (1) investigate the sleep disturbances of adolescents with MDD; (2) explore the association between insomnia and alexithymia in adolescents with MDD. We hypothesized that (1) the prevalence rate of insomnia is high in adolescent MDD patients; (2) insomnia is associated with alexithymia in adolescents with MDD; (3) female MDD adolescents with alexithymia is more likely to experience insomnia symptoms.
Materials and Methods
Participants
This study used a cross-sectional design. It was carried out in seven hospitals of seven cities in Anhui Province, from October 2020 to April 2022. Patients were consecutively recruited from the psychiatric outpatients and inpatients of these hospitals. Inclusion criteria: (1) meeting the diagnostic criteria for MDD mentioned in the fifth edition of the diagnostic and statistical manual (DSM-5), two trained psychiatrists made the diagnosis; (2) aged 12–18 years; (3) with an ability of comprehension. Exclusion criteria: (1) meeting the DSM-5 diagnostic criteria of other psychiatric disorders or intellectual disabilities; (2) with severe physical diseases; (3) unable to collaborate.
All patients and their guardians signed consent forms after being informed of the method and purpose of this study. These patients were told that they could terminate the study at any time. Those who are not qualified or comorbid with other disorders were excluded. Finally, 349 patients were initially enrolled, 20 of which were excluded because they did not complete the questionnaire, and 329 patients were finally included. This study was approved by the Ethics Committee of Chaohu Hospital, Anhui Medical University (202009-kyxm-04).
Design and Measurements
Participants who met the criteria were given a face-to-face questionnaire by uniformly trained and qualified investigators. Demographic and clinical data were collected using a predesigned questionnaire, supplemented by interviews with their relatives and reviews of their medical records.
Demographic and clinical variables included age, sex, BMI, only child, academic stress, family relationships, exercise, age of onset (years), duration of illness (months), and the use of sedative-hypnotics.
Clinical psychiatric evaluations included the Insomnia Severity Index Scale (ISI), the 20-item Toronto Alexithymia Scale (TAS-20) and the Center for Epidemiologic Studies of Depression Scale (CES-D).
The ISI is a 7 items self-report questionnaire, rated on a Likert-5 point scale. Each item score ranges from 0 to 4. A higher score meant more severe insomnia symptoms. The total score of ISI ≥ 8 is defined as insomnia.27 The Cronbach’s α coefficient for ISI in Chinese adolescents was 0.83, and the 2-week test–retest reliability was 0.79.28 The item loads of the Chinese version of ISI (0.617–0.797) were rated Good and Excellent in Comrey’s Item Load Grading Criteria, supporting good construct validity.29 It has been verified in adolescents aged 12–19 years in Hong Kong, China and showed good psychometric properties.28
The TAS-20 consists of 20 items with a 5-level score (1: completely disagree, 5: agree entirely). It comprises three subfactors: difficulty in identifying feelings (DIF), difficulty in describing feelings (DDF), and externally oriented thinking (EOT).30 With a total score of 20–100, the higher the score, the more severe the alexithymia. The Cronbach’s α coefficient for TAS-20 in Chinese adolescents is 0.87.31 The test–retest reliability is 0.87.32 The Chinese version TAS-20 has good structural validity among teenagers with the values of GFI, NFI, CFI and TLI were all above 0.9.32 The TAS-20 has shown good validity in Chinese adolescents.33
The CES-D was used to evaluate depression symptoms. The CES-D contains 20 items, among which 16 items assess negative emotions and 4 measure positive affections.34 The total score ranges from 0 to 60, reflecting the existence and severity of depression. The Cronbach’s α coefficient for CES-D in Chinese adolescents is 0.88.35 The test–retest reliability is 0.87.36 The sensitivity and specificity of CES-D is 95% and 93%, respectively.36 It has been widely used in Chinese research. Studies have shown that CES-D could effectively evaluate depression symptoms in Chinese adolescents with MDD.37
Statistical Analysis
The SPSS26.0 statistical software was used for statistical analysis. Continuous and categorical variables are presented as mean (SD), Median (interquartile range), and numbers (percentage), respectively. We compared the demographic and clinical variables between male and female patients. The analysis of variance (ANOVA), Student’s t-test and Mann–Whitney U-test were used for continuous variables and chi-square tests for categorical variables. Pearson’s correlation analysis was used to examine the correlation among ISI, CES-D, TAS-20 and its subfactors. Pearson’s correlation analysis and Spearman correlation analysis was used to examine the correlation between ISI and demographic and clinical variables. Multiple binary logistic regression analyses with the “Enter” method were carried out to explore the correlations of MDD with insomnia in the whole sample and separately by sex. P <0.05 (two-tailed) was considered statistically significant.
Results
Sex Differences in Demographic and Clinical Characters in Adolescents with MDD
The demographic and clinical data of male and female patients are presented in Table 1. In the 329 adolescent patients with MDD, 89 were male and 240 were female. The prevalence of clinically significant levels of insomnia was 78.1% (n = 257) in the whole sample, 80.0% and 73.0% in female and male patients, respectively (χ2=1.84, p = 0.175). Compared with male patients, female patients were less likely to exercise (χ2 = 5.94, p = 0.015), had lower rate of being only child (χ2= 9.47, p = 0.002) and experienced more severe depression (t = 3.12, p = 0.002) and alexithymia (t = 3.20, p = 0.002). There were no significant sex differences in age of onset, duration of illness, BMI, academic stress, family relationships, the use of sedative-hypnotics and ISI scores.
 |
Table 1 Demographic and Clinical Characteristics and Sex Differences in Adolescents with MDD |
As shown in Table 2, two-way ANOVAs were carried out to explore the interaction between insomnia and sex. Compared with patients without insomnia, those with insomnia had worse family relationships (F = 7.71, p = 0.021), perceived heavier academic stress (F = 6.32, p = 0.012), more likely to take sedative-hypnotics (F = 5.51, p = 0.019), had higher levels of depression (F = 81.57, p < 0.001) and alexithymia (F = 28.57, p < 0.001). These analyses also showed that there were significant sex differences in only-child, exercise and CES-D scores. There was significant insomnia × sex effect in BMI (F = 5.06, p = 0.025).
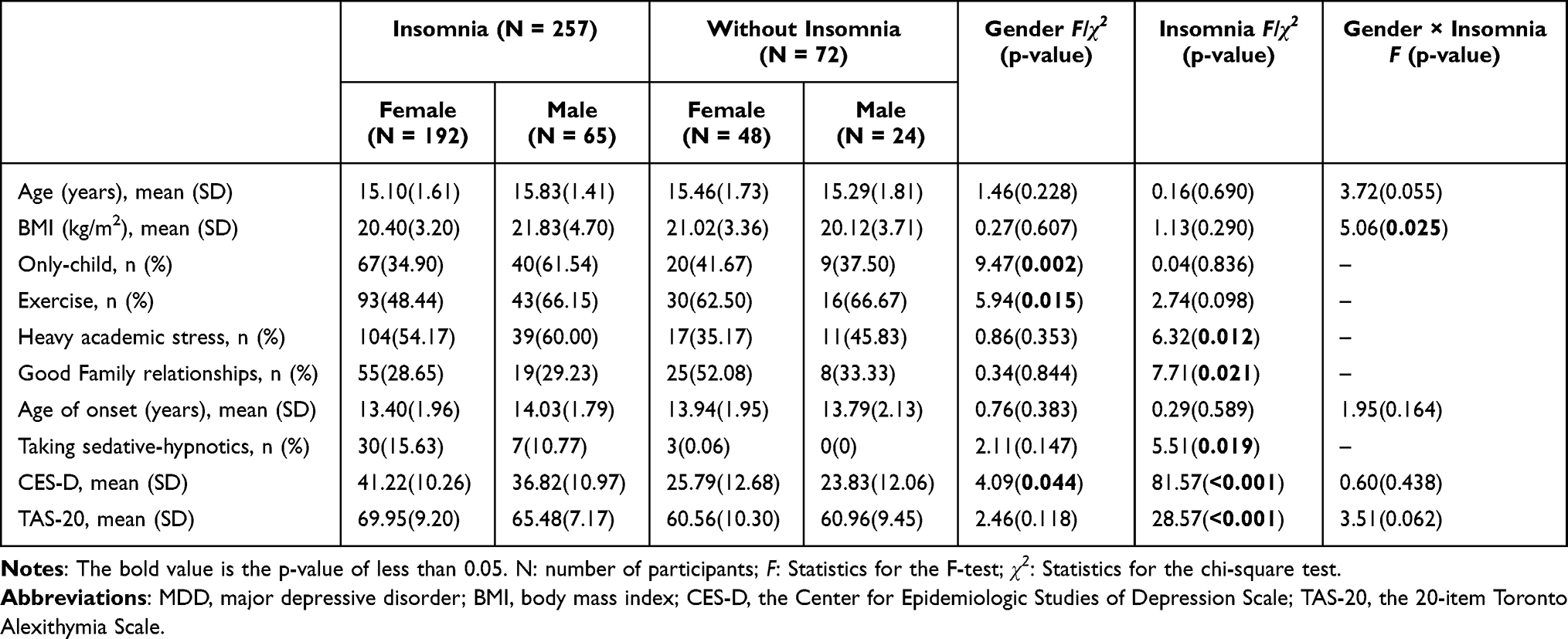 |
Table 2 Comparisons of Male and Female Adolescents with MDD with and without Insomnia |
The Correlation Between CES-D, TAS-20 and Its Subfactors in Adolescents with MDD
The correlation analysis of CES-D with TAS-20 and its subfactors was illustrated in Table 3. Irrelevant, weak, moderate and strong correlation(r) were defined as r between 0–0.09, 0.10–0.30, 0.30–0.50 and 0.50–1.00, respectively.38 The correlations between TAS, DIF, DDF, and CES-D were moderate to strong (r = 0.434 to 0.547, all p < 0.01). The correlation between EOT and CES-D was weak (r = 0.191, p < 0.01).
 |
Table 3 Correlations Among CES-D, TAS-20 and Its Subfactors in the Whole Sample |
The Related Factors of Insomnia in MDDAdolescents
In total sample, correlations between ISI scores and heavy academic stress (r = 0.185, p < 0.01), family relationships(r = 0.111, p < 0.05), CES-D scores (r = 0.602, p < 0.01) and TAS-20 scores (r = 0.360, p < 0.01) were significant (Table 4). Further binary logistic regression showed that only CES-D scores were correlated with insomnia (OR = 1.102, 95% CI: 1.066–1.139, p < 0.001), R2=0.355 (Table 5).
 |
Table 4 Correlations Between the ISI Scores and Demographic and Clinical Variable in Adolescents with MDD |
 |
Table 5 Multiple Binary Logistic Regression Analyses for Associations with Insomnia in the Whole Sample and Separately by Sex |
In male patients, correlation between ISI scores and CES-D scores (r = 0.524, p < 0.01) was significant (Table 4). Further binary logistic regression indicated that insomnia was significantly associated with depression symptom’s severity (OR = 1.098, 95% CI: 1.047–1.150, p < 0.001), R2 = 0.286 (Table 5).
In female patients, correlations between ISI scores and heavy academic stress (r = 0.229, p < 0.01), CES-D scores(r = 0.629, p < 0.01) and TAS-20 scores (r = 0.402, p < 0.01) were significant (Table 4). Further binary logistic regression indicated that two factors were significantly associated with insomnia: depression (OR = 1.094, 95% CI: 1.054–1.135), alexithymia (OR = 1.050, 95% CI: 1.003–1.099), R2=0.371 (Table 5).
Discussion
As far as we know, this is the first study to explore the sex differences in alexithymia severity between adolescent MDD patients with and without insomnia. This study found no significant differences in age, age of onset, BMI, academic stress, family relationships, rate of taking sedative-hypnotics, alexithymia and insomnia between male and female adolescent patients with MDD. Compared with patients without insomnia, those with insomnia experienced more severe alexithymia. Binary logistic regression analyses showed that insomnia was independently correlated with higher level of alexithymia in female patients but not in male patients. This indicated that there might be sex differences in the relationship between insomnia and alexithymia in adolescent MDD patients.
This study found that the insomnia rate in adolescents with MDD was 78.1%, which is slightly higher than that in another study of Chinese adolescents with depression (70.71%).39 An early survey conducted in 187 adolescents with MDD in the New York State Psychiatric Institute showed that the prevalence of insomnia was 74%.40 Another study involving 553 children with MDD from Hungary reported a prevalence of 53.5%.5 It is worth noting that among these children, 55% of them were male. In fact, the prevalence of insomnia reported in different studies varies due to the different age and sex ratio of the patient samples and various diagnostic and assessment methods. We already know that insomnia rates are higher in older or female adolescents.6 Moreover, the present study was conducted at the time of the outbreak and epidemic of COVID-19. During the COVID-19 epidemic in China, the prevalence of psychological and sleep problems was higher than usual,41 and children and adolescents were more affected.42 The insomnia rates between male and female patients did not show notable difference, which is inconsistent with earlier studies. Previous study showed that insomnia was more common in male adolescent MDD patients.22 Although the study was carried out in Hungary, more researches need to be performed on adolescent MDD patients in different countries.
In female patients, insomnia is associated with alexithymia after controlling for depressive symptoms, which consisted with earlier studies. The reason for this correlation might be biological, such as hyper arousal. It is demonstrated that higher levels of arousal play a crucial part in the pathophysiology of insomnia. Researchers suggested that internalizing psychic conflicts and being unable to verbalize them may lead to increased neurological arousal and subsequent sleep disturbances.43 Alexithymia also causes hyperarousal,44 which indicates that alexithymia may increase the risk of insomnia through hyper arousal.
In this study, the relationship between insomnia and alexithymia existed only in female adolescents. However, a study conducted in university students, mainly female students, showed that after eliminating the contribution of depression, the association between alexithymia and insomnia disappeared.45 In another study, after adjusting the contribution of depression, the association between alexithymia and insomnia existed only in male patients.46 The studies of interoception in recent years might provide new insights into this discrepancy. Recently, it has been pointed out that alexithymia is closely related to interoceptive impairment. The multiple psychiatric symptoms that co-occur with alexithymia indicate the impaired interoception among clinical patients.47 Interoception is the ability of perceiving the body’s internal state, which is related to a variety of basic functions, and it may be the reason behind some cross-disorder symptoms, such as sleep disorders.48 For example, a study measured the interoceptive sensitivity using MAIA (Multidimensional Assessment of Interoceptive Awareness) and found that sleep quality was associated with alexithymia in people with low interoceptive sensitivity, while in people with moderate and high interoceptive sensitivity, sleep quality was associated with negative emotions.49 Thus, alexithymia may induce varying consequences to the sleep quality of people with different levels of interoception sensitivity. We speculate that the sex differences in the interoceptive sensitivity of adolescents are sophisticated, which explains the discrepancy in the sex differences of the relationship between insomnia and alexithymia. It might be interesting to conduct more studies in this area.
Researchers also used PSG to assess objective sleep quality of alexithymia patients and reported that alexithymia was associated with increased light sleep and decreased deep sleep.19 However, PSG findings showed that compared with patients’ self-report, the objective total sleep time is usually longer.50 The subjective-objective sleep discrepancy is common and should be considered in sleep studies. It has been suggested that in the study of adolescent MDD, in addition to objective sleep/wake behavior, it may be more critical to evaluate their feelings about sleep.51
This study showed that the severity of insomnia in adolescents with MDD is associated with depression. Previous evidence indicated that insomnia is not related to immunologic, neurotrophic and neuroendocrine biomarkers that resemble the pathophysiology of MDD.52 Studies also showed that the improvements in insomnia symptoms were independent of depression remission.53 These findings support that insomnia may be a separate disorder rather than a common symptom of mental illness, and it has been suggested that insomnia needs to be conceiving as a comorbidity.54 Thus, insomnia requires effective interventions during the treatment of depression, as a separate focus of therapy, including behavioral, cognitive, and pharmacologic interventions.55 However, there is inadequate evidence on pharmacological interventions’ effectiveness and long-term outcome for adolescent insomnia. Although some drugs are used clinically to treat adolescent insomnia, the American Academy of Sleep Medicine recommends that further studies be conducted to clarify the appropriate dosage, safety, and efficacy of these drugs in adolescents.56 Therefore, insomnia in adolescent MDD patients needs other treatments, relevant researches has proven cognitive behavioral therapies (CBTs) effective in treating teenage insomnia.57 Recent studies suggested that short-term psychoanalytic psychotherapy (STPP) might help reducing sleep disturbances in early-onset MDD.58
In this study, insomnia was related to higher BMI in male patients but lower BMI in female patients. But the relationship between insomnia and BMI remains to be controversial. A study showed that obesity assessed by BMI was associated with chronic insomnia only in women, and this revealed sex-specific associations of BMI with different types of insomnia.59 Another study indicated that lower weight was related to the most severe type of insomnia, which is insomnia associated with physiological hyperarousal.60 Although limited study investigated the relationship between adolescents’ sleep and their eating behaviors, insufficient sleep has been associated with worse health status and irregular eating habits in adolescents.61 To sum up, the association between insomnia and BMI is affected by multiple factors and more intensive research is needed.
Consistent with previous studies, we found that alexithymia and its subcomponents DIF and DDF were moderately correlated with depressive symptoms, whereas EOT was only weakly correlated with depressive symptoms.62 EOT is a pragmatic thinking style that does not value emotions and the inner world.63 Studies showed that high EOT tendency can protect us from traumatic stressful experiences and cause harmful psychosomatic consequences by depriving positive or soothing experiences.64 Besides, people with high EOT tendency are prone to regulate stress through externalizing behaviors such as substance use.65
This study investigated the prevalence of insomnia and the correlation between insomnia and alexithymia in adolescents with MDD. It provided new insight into psychopathological mechanisms, treatments and psychological interventions in adolescents with MDD. However, there are several limitations in this study. First, the current design was cross-sectional, and the causality relationships between insomnia and alexithymia could not be adequately obtained. Second, since this study was conducted in a convenience sample, the sample size was small, and the sex ratio was imbalanced; therefore, the selection bias and sampling bias were inevitable All patients were recruited from seven hospitals in Anhui Province, China. Thus, the findings might not be generalized to other adolescents with MDD from different regions and cultures. Third, there was no matched healthy control group in this study, so we could not compare the clinical features between MDD and community adolescents. Fourth, the assessment tools used in this study are self-rating scales, which may lead to a certain recall bias. Finally, other relevant factors that may cause insomnia, such as anxiety, somatic diseases and poor sleep hygiene behaviors, were not controlled.
Conclusion
To sum up, the prevalence of insomnia was high in adolescent MDD patients. There was no sex difference in the insomnia rate in adolescents with MDD. Patients with insomnia experienced more severe alexithymia than those without insomnia. The relationship between insomnia and alexithymia existed only in female patients, but not in male patients. In female adolescent MDD patients, alexithymia is a risk factor for insomnia. Future treatments of insomnia in MDD adolescents need to design programs to improve the ability of emotional regulation.
Abbreviations
MDD, major depressive disorder; YLDs, years lived with disability; MDE, major depressive episode; PSG, polysomnography; DSM-5, the diagnostic and statistical manual; BMI, body mass index; CES-D, the Center for Epidemiologic Studies of Depression Scale; TAS-20, the 20-item Toronto Alexithymia Scale; DIF, difficulty in identifying emotions; DDF, difficulty in describing emotions; EOT, externally oriented thinking; PSQI, the Pittsburgh Sleep Quality Index; SD, standard deviations; ANOVA, the analysis of variance; CI, confidence interval; OR, odds ratio; MAIA, multidimensional assessment of interoceptive awareness; COVID-19, Corona Virus Disease 2019; CBT, cognitive behavioral therapies; STPP, short-term psychoanalytic psychotherapy.
Data Sharing Statement
As this study is still ongoing, the raw datasets for the current study will not be available until the end of this research project. Please contact the first author (Xiaoxue Yang, [email protected]) for raw data requests.
Ethical Statement and Consent to Participate
This study received ethical approval from the Ethics Committee of Chaohu Hospital, Anhui Medical University (202009-kyxm-04). This study was conducted in accordance with the declaration of Helsinki. Written informed consent was obtained from all participants.
Acknowledgments
We thank all the participants who volunteered to participate in this study.
Funding
This study was supported by the National Key Clinical Specialty Project Foundation (CN) and the Research Fund Project of Anhui Translational Research Institute (No. 2022zhyx-B01).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Disease G B D, Injury I, Prevalence C. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1789–1858. doi:10.1016/S0140-6736(18)32279-7
2. Ferrari AJ, Somerville AJ, Baxter AJ, et al. Global variation in the prevalence and incidence of major depressive disorder: a systematic review of the epidemiological literature. Psychol Med. 2013;43(3):471–481. doi:10.1017/S0033291712001511
3. Shorey S, Ng ED, Wong CHJ. Global prevalence of depression and elevated depressive symptoms among adolescents: a systematic review and meta-analysis. Br J Clin Psychol. 2022;61(2):287–305. doi:10.1111/bjc.12333
4. Geoffroy PA, Hoertel N, Etain B, et al. Insomnia and hypersomnia in major depressive episode: prevalence, sociodemographic characteristics and psychiatric comorbidity in a population-based study. J Affective Disorders. 2018;226:132–141. doi:10.1016/j.jad.2017.09.032
5. Liu X, Buysse DJ, Gentzler AL, et al. Insomnia and hypersomnia associated with depressive phenomenology and comorbidity in childhood depression. Sleep. 2007;30(1):83–90. doi:10.1093/sleep/30.1.83
6. Alvaro PK, Roberts RM, Harris JK, et al. The direction of the relationship between symptoms of insomnia and psychiatric disorders in adolescents. J Affective Disorders. 2017;207:167–174. doi:10.1016/j.jad.2016.08.032
7. Marino C, Andrade B, Campisi SC, et al. Association between disturbed sleep and depression in children and youths: a systematic review and meta-analysis of cohort studies. JAMA Network Open. 2021;4(3):e212373. doi:10.1001/jamanetworkopen.2021.2373
8. Roberts RE, Duong HT. Depression and insomnia among adolescents: a prospective perspective. J Affective Disorders. 2013;148(1):66–71. doi:10.1016/j.jad.2012.11.049
9. Joshi K, Cambron-Mellott MJ, Costantino H, et al. The clinical, economic, and patient-centric burden of insomnia symptom severity in adults with major depressive disorder in the United States. Brain Behav. 2023;13(8):e3143. doi:10.1002/brb3.3143
10. Alimoradi Z, Majd NR, Broström A, et al. Is alexithymia associated with sleep problems? A systematic review and meta-analysis. Neurosci Biobehav Rev. 2022;133:104513. doi:10.1016/j.neubiorev.2021.12.036
11. Taylor GJ. Alexithymia: concept, measurement, and implications for treatment. Am j Psychiatry. 1984;141(6):725–732.
12. Habibi Asgarabad M, Salehi Yegaei P, Jafari F, et al. The relationship of alexithymia to pain and other symptoms in fibromyalgia: a systematic review and meta-analysis. Eur J Pain. 2023;27(3):321–337. doi:10.1002/ejp.2064
13. fukunishi I, Kawamura N, Ishikawa T, et al. Sleep characteristics of Japanese working men who score alexithymic on the Toronto Alexithymia Scale. Percept Motor Skills. 1997;84(3 Pt 1):859–865. doi:10.2466/pms.1997.84.3.859
14. Kronholm E, Partonen T, Salminen JK, et al. Alexithymia, depression and sleep disturbance symptoms. Psychother Psychosom. 2008;77(1):63–65. doi:10.1159/000110063
15. Bauermann TM, Parker JDA, Taylor GJ. Sleep problems and sleep hygiene in young adults with alexithymia. Pers Individ Dif. 2008;45(4):318–322. doi:10.1016/j.paid.2008.04.019
16. Ma Q, Zhang X, Zou L. The mediating effect of alexithymia on the relationship between schizotypal traits and sleep problems among college students. Front Psychiatry. 2020;11:153. doi:10.3389/fpsyt.2020.00153
17. Murphy J, Wulff K, Catmur C, et al. Alexithymic traits, independent of depression and anxiety, are associated with reduced sleep quality. Pers Individ Dif. 2018;129:175–178. doi:10.1016/j.paid.2018.03.023
18. Aydın A, Selvi Y, Güzel Ozdemir P. Depresyon Hastalarında Aleksitiminin Bedenselleştirme ve Uyku Kalitesi Üzerine Etkisi. Nöro Psikiyatri Arsivi. 2013;50(1):65–69. doi:10.4274/npa.y6335
19. Bazydlo R, Lumley MA, Roehrs T. Alexithymia and polysomnographic measures of sleep in healthy adults. Psychosomatic Med. 2001;63(1):56–61. doi:10.1097/00006842-200101000-00007
20. Natalucci G, Faedda N, Calderoni D, et al. Headache and alexithymia in children and adolescents: what is the connection? Front Psychol. 2018;9:48. doi:10.3389/fpsyg.2018.00048
21. Son SH, Jo H, Rim HD, et al. A comparative study on alexithymia in depressive, somatoform, anxiety, and psychotic disorders among Koreans. Psychiatry Invest. 2012;9(4):325–331. doi:10.4306/pi.2012.9.4.325
22. Baji I, Lopez-Duran NL, Kovacs M, et al. Age and sex analyses of somatic complaints and symptom presentation of childhood depression in a Hungarian clinical sample. J Clini Psych. 2009;70(10):1467–1472. doi:10.4088/JCP.08m04918
23. Lane RD, Sechrest L, Riedel R. Sociodemographic correlates of alexithymia. Compr Psychiatry. 1998;39(6):377–385. doi:10.1016/S0010-440X(98)90051-7
24. Spitzer C, Brandl S, Rose H-J, et al. Gender-specific association of alexithymia and norepinephrine/cortisol ratios. A preliminary report. J Psychosom Res. 2005;59(2):73–76. doi:10.1016/j.jpsychores.2004.07.006
25. Lumley MA, Sielky K. Alexithymia, gender, and hemispheric functioning. Compr Psychiatry. 2000;41(5):352–359. doi:10.1053/comp.2000.9014
26. Robert JJT, Hoffmann RF, Emslie GJ, et al. Sex and age differences in sleep macroarchitecture in childhood and adolescent depression. Sleep. 2006;29(3):351–358. doi:10.1093/sleep/29.3.351
27. Smith S, Trinder J. Detecting insomnia: comparison of four self-report measures of sleep in a young adult population. J Sleep Res. 2001;10(3):229–235. doi:10.1046/j.1365-2869.2001.00262.x
28. Chung K-F, Kan KK, Yeung W-F. Assessing insomnia in adolescents: comparison of Insomnia Severity Index, Athens Insomnia Scale and Sleep Quality Index. Sleep Med. 2011;12(5):463–470. doi:10.1016/j.sleep.2010.09.019
29. Li E. The Study of validity and Reliability of the Insomnia Severity Index Scale. Southern Medical University; 2018.
30. Bagby RM, Parker JD, Taylor GJ. The twenty-item Toronto Alexithymia Scale—I. Item selection and cross-validation of the factor structure. J Psychosom Res. 1994;38(1):23–32. doi:10.1016/0022-3999(94)90005-1
31. Ling Y, Zeng Y, Yuan H, et al. Cross-cultural validation of the 20-item Toronto Alexithymia Scale in Chinese adolescents. J Psychiatric Ment Health Nurs. 2016;23(3–4):179–187. doi:10.1111/jpm.12298
32. Jinyao Y, Shuqiao Y, Xiongzhao Z. The Chinese version of the Tas-20: reliability and validity. Chin Ment Health J. 2003;17(11):763–767.
33. Yu L, Jinyao Y, Juan Y. Reliability test of the Chinese version of Tas-20 among 1260 adolescents. Chinese Journal of Clinical Psychology. 2009;17(4). doi:10.16128/j.cnki.1005-3611.2009.04.025
34. Radloff LS. The CES-D scale: a self-report depression scale for research in the general population. Appl Psychol Measure. 1977;1(3):385–401. doi:10.1177/014662167700100306
35. Chen Z-Y, Yang X-D, X-Y L. Psychometric features of CES-D in Chinese adolescents. Chin J Clin Psychol. 2009;17(4):443–445.
36. Juanjuan L, Yanan Z, Liangming H. Study of PHQ-2-C, CES-D and BDI-I-C in the application of screening of adolescents with depressive disorder. J Int Psychiatry. 2017;44(01):23–25+36. doi:10.13479/j.cnki.jip.2017.01.003
37. Yang W, Xiong G, Garrido LE, et al. Factor structure and criterion validity across the full scale and ten short forms of the CES-D among Chinese adolescents. Psychol Assess. 2018;30(9):1186–1198. doi:10.1037/pas0000559
38. Cohen J. Statistical Power Analysis for the Behavioral Sciences. Routledge; 2013.
39. Pei C, Fan C, Luo H, et al. Sleep problems in adolescents with depression: role of childhood trauma, alexithymia, rumination, and self-esteem. J Affective Disorders. 2023;338:83–91. doi:10.1016/j.jad.2023.05.095
40. Ivanenko A, Crabtree VM, Gozal D. Sleep and depression in children and adolescents. Sleep Med Rev. 2005;9(2):115–129. doi:10.1016/j.smrv.2004.09.006
41. Wang S, Zhang Y, Ding W, et al. Psychological distress and sleep problems when people are under interpersonal isolation during an epidemic: a nationwide multicenter cross-sectional study. Eur Psychiatry. 2020;63(1):e77. doi:10.1192/j.eurpsy.2020.78
42. Jahrami HA, Alhaj OA, Humood AM, et al. Sleep disturbances during the COVID-19 pandemic: a systematic review, meta-analysis, and meta-regression. Sleep Med Rev. 2022;62:101591. doi:10.1016/j.smrv.2022.101591
43. Hyyppä MT, Lindholm T, Kronholm E, et al. Functional insomnia in relation to alexithymic features and cortisol hypersecretion in a community sample. Stress Med. 1990;6(4):277–283. doi:10.1002/smi.2460060406
44. Neumann SA, Sollers JJ, Thayer JF, et al. Alexithymia predicts attenuated autonomic reactivity, but prolonged recovery to anger recall in young women. Int J Psychophysiol. 2004;53(3):183–195. doi:10.1016/j.ijpsycho.2004.03.008
45. De Gennaro L, Martina M, Curcio G, et al. The relationship between alexithymia, depression, and sleep complaints. Psychiatry Res. 2004;128(3):253–258. doi:10.1016/j.psychres.2004.05.023
46. Honkalampi K, Saarinen P, Hintikka J, et al. Factors associated with alexithymia in patients suffering from depression. Psychother Psychosom. 1999;68(5):270–275. doi:10.1159/000012343
47. Brewer R, Murphy J, Bird G. Atypical interoception as a common risk factor for psychopathology: a review. Neurosci Biobehav Rev. 2021;130:470–508. doi:10.1016/j.neubiorev.2021.07.036
48. Murphy J, Brewer R, Catmur C, et al. Interoception and psychopathology: a developmental neuroscience perspective. Dev Cognit Neurosci. 2017;23:45–56. doi:10.1016/j.dcn.2016.12.006
49. Huang Y-H, Yang C-M, Huang Y-C, et al. Do alexithymia and negative affect predict poor sleep quality? The moderating role of interoceptive sensibility. PLoS One. 2022;17(10):e0275359. doi:10.1371/journal.pone.0275359
50. Rezaie L, Fobian AD, Mccall WV, et al. Paradoxical insomnia and subjective-objective sleep discrepancy: a review. Sleep Med Rev. 2018;40:196–202. doi:10.1016/j.smrv.2018.01.002
51. O’callaghan VS, Couvy-Duchesne B, Strike LT, et al. A meta-analysis of the relationship between subjective sleep and depressive symptoms in adolescence. Sleep Med. 2021;79:134–144. doi:10.1016/j.sleep.2021.01.011
52. Drinčić T, Van Dalfsen JH, Kamphuis J, et al. The relationship between insomnia and the pathophysiology of major depressive disorder: an evaluation of a broad selection of serum and urine biomarkers. Int J Mol Sci. 2023;24(9):8437. doi:10.3390/ijms24098437
53. Mason BL, Davidov A, Minhajuddin A, et al. Focusing on insomnia symptoms to better understand depression: a STAR*D report. J Affective Disorders. 2020;260:183–186. doi:10.1016/j.jad.2019.08.094
54. Benca RM, Buysse DJ. Reconsidering insomnia as a disorder rather than just a symptom in psychiatric practice. J Clini Psych. 2018;79(1):49–54. doi:10.4088/JCP.me17008ah1c
55. Buysse DJ. Insomnia. JAMA. 2013;309(7):706–716. doi:10.1001/jama.2013.193
56. De Zambotti M, Goldstone A, Colrain IM, et al. Insomnia disorder in adolescence: diagnosis, impact, and treatment. Sleep Med Rev. 2018;39:12–24. doi:10.1016/j.smrv.2017.06.009
57. Zhou ES, Owens J. Behavioral treatments for pediatric insomnia. Curr Sleep Med Rep. 2016;2(3):127–135. doi:10.1007/s40675-016-0053-0
58. Schønning T, Dahl H-SJ, Hummelen B, et al. Do sleep disturbances improve following psychoanalytic psychotherapy for adolescent depression? Int J Environ Res Public Health. 2022;19(3):1790. doi:10.3390/ijerph19031790
59. Andreeva VA, Torres MJ, Druesne-Pecollo N, et al. Sex-specific associations of different anthropometric indices with acute and chronic insomnia. Eur j Public Health. 2017;27(6):1026–1031. doi:10.1093/eurpub/ckx123
60. Ren R, Zhang Y, Yang L, et al. Insomnia with physiological hyperarousal is associated with lower weight: a novel finding and its clinical implications. Transl Psychiatry. 2021;11(1):604. doi:10.1038/s41398-021-01672-5
61. Grimaldi M, Bacaro V, Natale V, et al. The longitudinal interplay between sleep, anthropometric indices, eating behaviors, and nutritional aspects: a systematic review and meta-analysis. Nutrients. 2023;15(14):3179. doi:10.3390/nu15143179
62. Li S, Zhang B, Guo Y, et al. The association between alexithymia as assessed by the 20-item Toronto Alexithymia Scale and depression: a meta-analysis. Psychiatry Res. 2015;227(1):1–9. doi:10.1016/j.psychres.2015.02.006
63. Müller J, Bühner M, Ellgring H. Is there a reliable factorial structure in the 20-item Toronto Alexithymia Scale? A comparison of factor models in clinical and normal adult samples. J Psychosom Res. 2003;55(6):561–568. doi:10.1016/S0022-3999(03)00033-3
64. Davydov DM. Alexithymia as a health risk and resilience factor. J Psychosom Res. 2017;101:66–67. doi:10.1016/j.jpsychores.2017.08.004
65. Kajanoja J, Scheinin NM, Karukivi M, et al. Alcohol and tobacco use in men: the role of alexithymia and externally oriented thinking style. Am J Drug Alcohol Abuse. 2019;45(2):199–207. doi:10.1080/00952990.2018.1528267
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.