Back to Journals » Patient Preference and Adherence » Volume 20
Identifying Core Symptoms in Breast Cancer Patients with Different Chemotherapy Phases Using Network Analysis: A Prospective Multicenter Longitudinal Study
Authors He J, Bai D, Chen H, Chen X, Lu X, Ji W, Xu R, Hou C, Gao J ![]()
Received 29 October 2025
Accepted for publication 28 January 2026
Published 11 February 2026 Volume 2026:20 568080
DOI https://doi.org/10.2147/PPA.S568080
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Jiali He,* Dingxi Bai,* Huan Chen,* Xinyu Chen, Xianying Lu, Wenting Ji, Ran Xu, Chaoming Hou, Jing Gao
School of Nursing, Chengdu University of Traditional Chinese Medicine, Chengdu, Sichuan Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chaoming Hou; Jing Gao, Email [email protected]; [email protected]
Background: Network analysis can identify the core symptoms reported by patients at each time point, providing a basis to develop precise symptom strategies for treatment. However, few studies have established symptom networks for breast cancer patients at various treatment stages.
Objective: The purpose of this study was to identify core symptoms that may be targeted for intervention in different chemotherapy phases for breast cancer patients.
Methods: A multicenter prospective longitudinal survey design was employed in this study. 467 breast cancer patients were recruited in the Breast Surgery Ward from November 2022 and October 2023. The Symptoms Assessment Scale for Breast Cancer Patients Receiving Chemotherapy was used to assess breast cancer patients’ symptoms before chemotherapy (T0), after the first chemotherapy (T1), after three chemotherapy treatments (T2), and after the sixth chemotherapy treatment (T3). Symptom networks and node properties were explored using network analysis.
Results: At T0, difficulty sleeping was a symptom with the highest strength (rs=2.43) and closeness (rc=1.51). Depression was a symptom with the highest betweenness (rb=2.47). At T1, decreased appetite was the symptom with the highest strength centrality (rs=2.22). Pain was the symptom with the highest closeness centrality (rc=1.48). Headache was a symptom with the highest betweenness centrality (rb=1.68). Fatigue was the symptom with the highest strength, closeness, and betweenness at T2 and T3 (T2: rs=1.67; rc=2.11; rb=2.30. T3: rs=1.96; rc=2.68; rb=2.15). Except for betweenness centrality at T1, all other centrality measures showed CS coefficients above 0.25, indicating that the symptom networks were substantially stable.
Conclusion: The core symptoms that need to be targeted for intervention in various chemotherapy stages of breast cancer patients differ. Difficulty sleeping and depression should be addressed at T0; decreased appetite and pain were the core symptoms at T1; and fatigue was the most central symptom at T2 and T3 and should be controlled as a priority.
Plain Language Summary: Breast cancer patients usually have many symptoms at the same time throughout the chemotherapy phase, resulting in a significant symptom burden. To better identify and manage these symptoms, we applied a technique called “network analysis” to construct “symptom networks” for breast cancer patients at different chemotherapy stages. Similar to social networks where influential individuals can affect many others, symptom networks contain core symptoms that influence other connected symptoms. By prioritizing interventions targeting these core symptoms, related symptoms may lose their “anchor points”, thereby alleviating the overall symptom burden. Our study found that the core symptoms in breast cancer patients change as chemotherapy progresses. This means that the focus of symptom management should also shift according to the treatment stage.
Keywords: breast cancer, chemotherapy, symptom network, core symptoms
Introduction
Breast cancer is the most common malignant tumor in women, and the most recent global cancer statistics report released by the International Agency for Research on Cancer (IARC) shows that the incidence of breast cancer in women is the second highest in the world, with approximately 2.3 million new cases worldwide, accounting for 11.6% of all new cancer cases.1 The prevalence of breast cancer is increasing year after year, causing significant alarm among medical professionals. Chemotherapy is one of the most prevalent therapies for breast cancer patients, as it efficiently treats the disease and extends patients’ living times. However, the majority of chemotherapy medications used by breast cancer patients cause adverse effects that have an adverse effect on their health and psychology.2 Patients may experience a variety of symptoms during the chemotherapy period.3–6 These symptoms interact with one another, inflicting a significant burden on patients,7 and in some cases, leading to early cessation of chemotherapy, affecting the course of treatment and seriously endangering patients’ lives.8 As a result, it’s critical to recognize symptoms early on in breast cancer chemotherapy patients’ treatment and to effectively manage them.
Numerous studies have been conducted on the management of symptoms in patients undergoing chemotherapy for breast cancer. These studies primarily used cross-sectional studies to investigate the current state of and factors influencing a single symptom or cluster of symptoms9,10 or longitudinal studies to investigate changes in symptoms or clusters of symptoms over time.11 Patients receiving chemotherapy for breast cancer frequently have multiple symptoms, and assessing a single symptom in isolation fails to explain the patient’s problems in a holistic and comprehensive manner, ignoring the patient’s overall symptom burden. In contrast to single symptoms, investigations of symptom clusters account for the co-occurrence of several symptoms in patients and enable the management of multiple symptoms with the goal of symptom alleviation.12 However, in-depth investigations of symptom management in recent years have revealed that the interrelationships between symptoms are not simple linear interactions, but rather intricate interconnections.13 Traditional techniques for investigating symptom clusters have tended to reduce interrelationships between symptoms by category or dimensionality reduction, ignoring the complexity of inter-symptom interactions.14 And in the previous nursing process for a single symptom or symptom clusters, symptoms were not prioritized, and patients with multiple symptoms needed multiple related interventions, which made symptom management less efficient.15 As a result, based on previous studies focusing on the changes of symptom clusters in patients with breast cancer during different chemotherapy periods, it is of great practical significance to further elaborate the complex relationship between symptoms of patients, identify core symptoms, and change the focus of symptom management from simultaneous intervention of multiple symptoms to management of only core symptoms for optimizing.
Network analysis offers a novel perspective on symptom science research in today’s society. The network structure, nodes, and network metrics connecting several symptoms can all be statistically explained by network analysis.16 The primary symptoms that need to be managed can be found via network analysis. Interventions for symptom management that concentrate on the “core symptom” can deprive other symptoms of their “target point” and spread the intervention effect to the peripheral symptoms of the core symptom, thereby alleviating or eliminating other symptoms.17,18 Currently, network analysis has been widely applied in various cancer populations to help in the identification of core symptoms. For example, Wang et al used a symptom network to pinpoint distress as a core symptom for immediate management in digestive cancers.19 Meanwhile, Zhang et al’s network analysis highlighted that the core symptoms among lung cancer survivors varied significantly before and after radiotherapy.20 These applications in diverse tumor research disciplines thoroughly demonstrate that network analysis can find information beyond incidence and severity, highlighting the core symptoms now experienced by patients. This permits targeted interventions to achieve the best management outcomes. The application of this unique research methodology to the study of symptoms during chemotherapy in breast cancer patients has enormous potential. However, there have been fewer studies applying symptom network analysis specifically to breast cancer patients undergoing chemotherapy. In a study by Cai,21 fatigue was identified as the symptom with the highest centrality of intensity and the best association with other symptoms in the network structure. Liang22 also discovered the importance of fatigue in the symptom network in a survey of 468 individuals undergoing chemotherapy for breast cancer. Although the findings are significant, all studies used cross-sectional designs, which do not reflect the dynamic evolution of symptom networks. Given the cyclical nature of chemotherapy and the time-varying nature of patients’ symptoms, this study proposes the following hypothesis: Breast cancer patients’ symptom networks evolve dynamically throughout chemotherapy, with core symptoms varying depending on treatment phase.
Therefore, this study constructed a symptom network of breast cancer patients in different chemotherapy periods with the aim of identifying the core symptoms that need intervention at different time points and providing a reference basis for clinical healthcare professionals to give patients efficient and precise symptom management.
Methods
Design, Setting, and Participants
We conducted a multicenter prospective longitudinal study. Breast cancer patients who met the inclusion and exclusion criteria at four tertiary institutions in Chengdu, Sichuan Province, were chosen using convenience sampling. Participants in this trial were female, aged ≥18, undergoing chemotherapy, expected to finish ≥6 courses, volunteered, and signed an informed consent form. Patients that struggled to communicate were excluded. According to the pairwise Markov random field (PMRF) model, the parameters required for a network include both threshold and pairwise association parameters.23 With 25 symptoms in the current study, this results in 25 threshold parameters and 300 (25×(25–1)/2=300) pairwise association parameters, totaling 325 parameters to be estimated. To reliably estimate this number of parameters, the sample size must exceed this count. Accounting for a 20% loss-to-follow-up rate, this study requires a minimum sample size of 390. The study initially enrolled 512 breast cancer patients. During follow-up, participants were excluded if they discontinued chemotherapy, were lost to follow-up, or voluntarily withdrew. Ultimately, 467 patients completed the entire follow-up period. The final sample size exceeds the minimum requirement of 390, thus providing sufficient statistical power. Furthermore, the multicenter design across four tertiary hospitals improves representativeness. Following similar longitudinal studies that employed network analysis,20,24 this study analyzed data only from patients who completed the full follow-up protocol.
Data Collection
Patients with breast cancer scheduled for chemotherapy between November 2022 and October 2023 were recruited for this study. Specialist nurses conducted the recruitment and assessment at baseline. Before chemotherapy (T0), after the first cycle of chemotherapy (T1), after the third cycle of chemotherapy (T2), and after the sixth cycle of chemotherapy (T3), the subjects were asked to record their symptom experiences. Most study participants were surveyed in-person while they were there, and a small percentage of patients who found it difficult to come back to the hospital to finish the follow-up survey were polled online using a web-based questionnaire. For questionnaires completed on-site, the researchers performed immediate checks and organized the data promptly after collection. To ensure the completeness and validity of the online survey, the following quality control measures were implemented: a unique follow-up link was sent to each patient to prevent duplicate submissions; the platform was configured to require responses to all items in order to eliminate missing data; and timestamp analysis was employed to identify and review responses with anomalously short or long completion times. To guarantee data accuracy, two researchers independently performed double data entry using EpiData software (version 3.1), strictly adhering to a unified protocol.
Measures
Socio-Demographic and Clinical Characteristics
We employed a general information questionnaire to collect socio-demographic and clinical data from patients, including age, ethnicity, place of residence, education, marital status, disease diagnosis, molecular staging of cancer, surgical statuses, chemotherapeutic regimen, and cancer stage.
Symptoms
Breast cancer patients’ symptoms were investigated using the Symptoms Assessment Scale for Breast Cancer Patients Receiving Chemotherapy. Chinese scholar Wen25 developed the scale after reviewing pertinent literature and cancer symptom assessment instruments. The scale contains the following 25 symptom entries: nausea, taste alteration, oral ulceration, skin changes (eg, peeling, allergies, nail discoloration, dryness), vomiting, depression, fatigue, decreased appetite, hair loss, constipation, numbness of fingers/toes, difficulty sleeping, pain, decreased interest in sexuality, cough, dysfunctional menstruation, photophobia of eyes, diarrhea, loss of weight, memory deterioration, lack of concentration, fever, headache, sore throat, bleeding (eg from gums, nose, stool, etc). Each symptom was graded based on its severity, with “none” as 0, “mild” as 1, “moderate” as 2, “severe” as 3, and “very severe” as 4. The Cronbach’s alpha coefficient for this scale was 0.818.
Statistical Analysis
Network analysis was performed using R 4.3.1 software. The graph package was used to construct a symptom network graph based on EBICglasso. Symptoms were the network’s nodes, and the lines connecting them were the network’s edges; the thicker the edges, the stronger the association between the two symptoms. At the same time, three centrality indicators were calculated: strength, closeness, and betweenness. Strength indicates a symptom’s ability to impact other symptoms, whereas closeness centrality indicates a symptom’s central location in the network and betweenness centrality indicates a symptom’s bridging role in the network. A symptom with a high centrality is considered a core symptom in the symptom network. The bootnet package detects the stability in the centrality indicators after reducing the sample size in the network and calculates the Correlation Stability Coefficient (CS Coefficient), which should be at least 0.25 and preferably larger than 0.5.23
Ethical Approval
This study was approved by the Ethics Committee of the Chengdu Jinniu District People’s Hospital (QYYLL-2022-010) and adhered to the principles of the Declaration of Helsinki. All study participants willingly signed informed consent. During the follow-up period, individuals may withdraw at any time without repercussions.
Results
Characteristics of Breast Cancer Patients
The study included 467 female breast cancer patients, with an average age of 49.97±9.41 years. Table 1 shows the baseline characteristics of the patients.
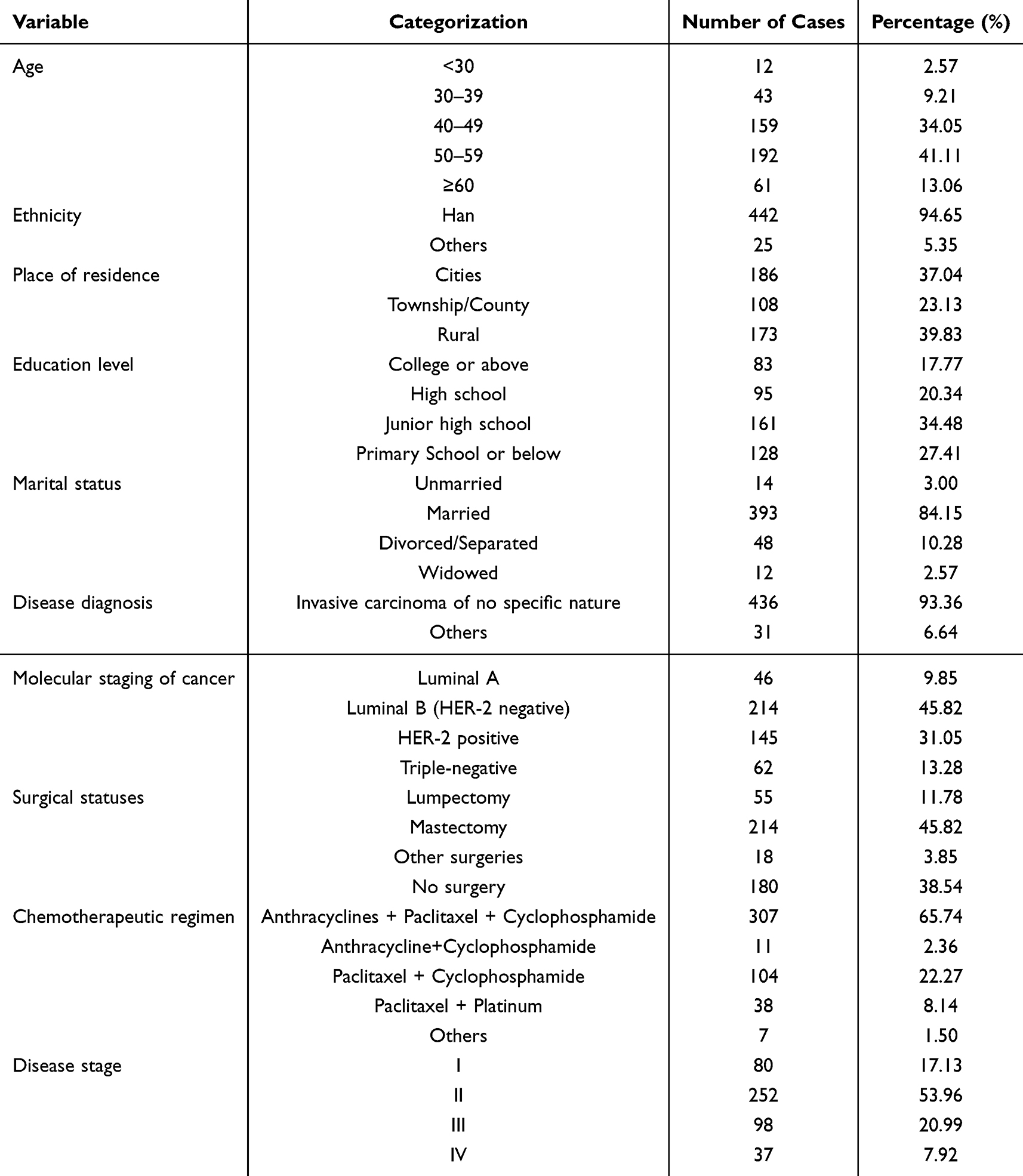 |
Table 1 Patient Characteristics (N= 467) |
Symptom Networks at Different Phases for Breast Cancer Patients
At T0, all symptoms in the network were linked to one another, either directly or indirectly. The symptoms with the highest correlation were depression and difficulty sleeping (r=0.55) and depression and decreased appetite (r=0.50). After the beginning of chemotherapy, nausea and vomiting were the most closely related symptoms (T1: r=0.68; T2: r=0.65; T3: r=0.71). Figure 1 demonstrates the network of symptoms at several time points in breast cancer patients.
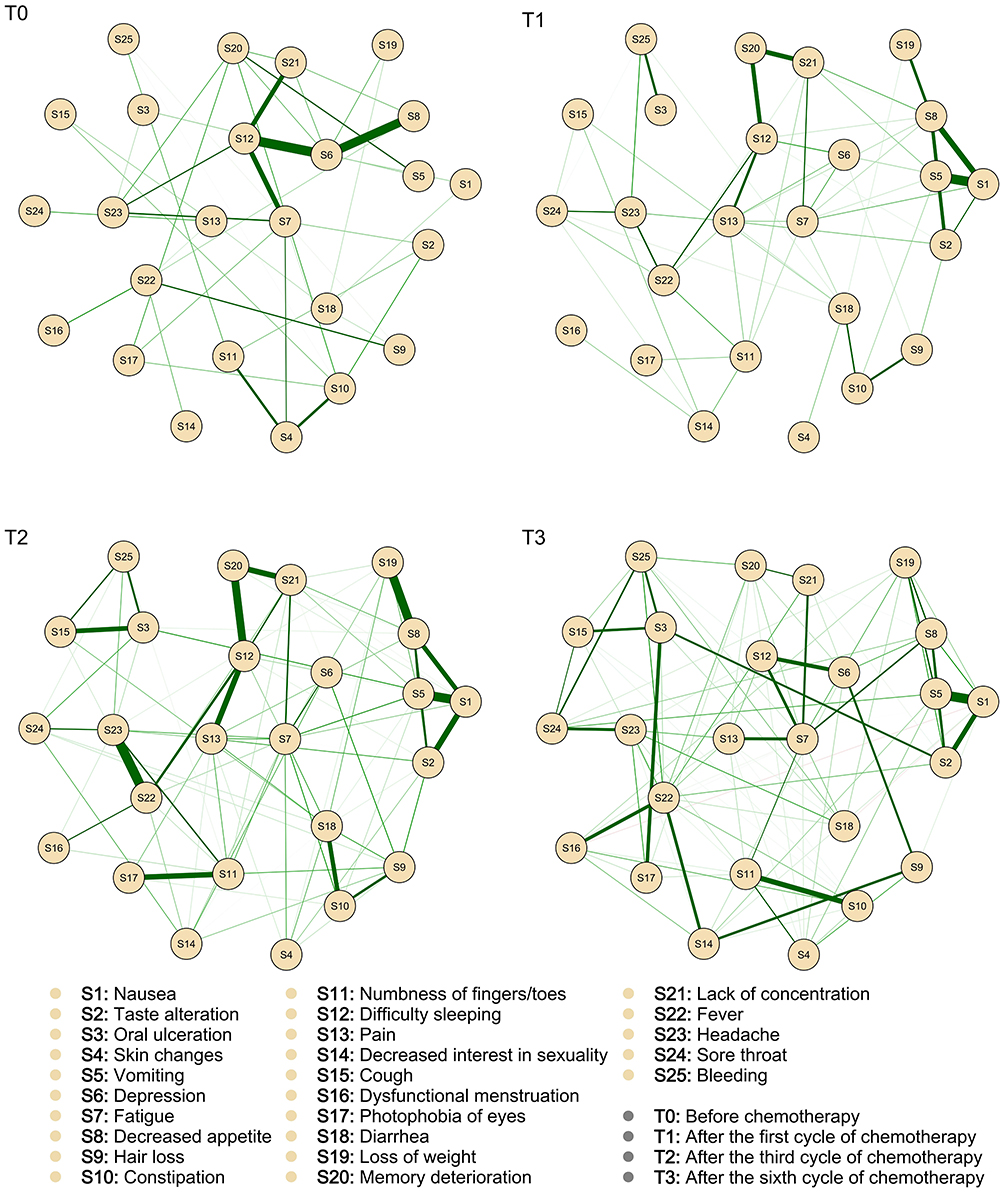 |
Figure 1 Symptom networks at several time points in breast cancer patients. |
Centrality Indices
At T0, difficulty sleeping was the symptom with the highest strength (rs=2.43) and closeness (rc=1.51). Depression was the symptom with the highest betweenness (rb=2.47). At T1, decreased appetite have the highest strength (rs=2.22), pain was the symptom with the highest closeness (rc=1.48), and pain was the symptom with the highest betweenness (rb=1.68). Fatigue have the highest strength, closeness, and betweenness centrality at T2 (rs=1.67; rc=2.11; rb=2.30) and T3 (rs=1.96, rc=2.68, rb=2.15). Figure 2 demonstrates the centrality indices of symptoms at each time point.
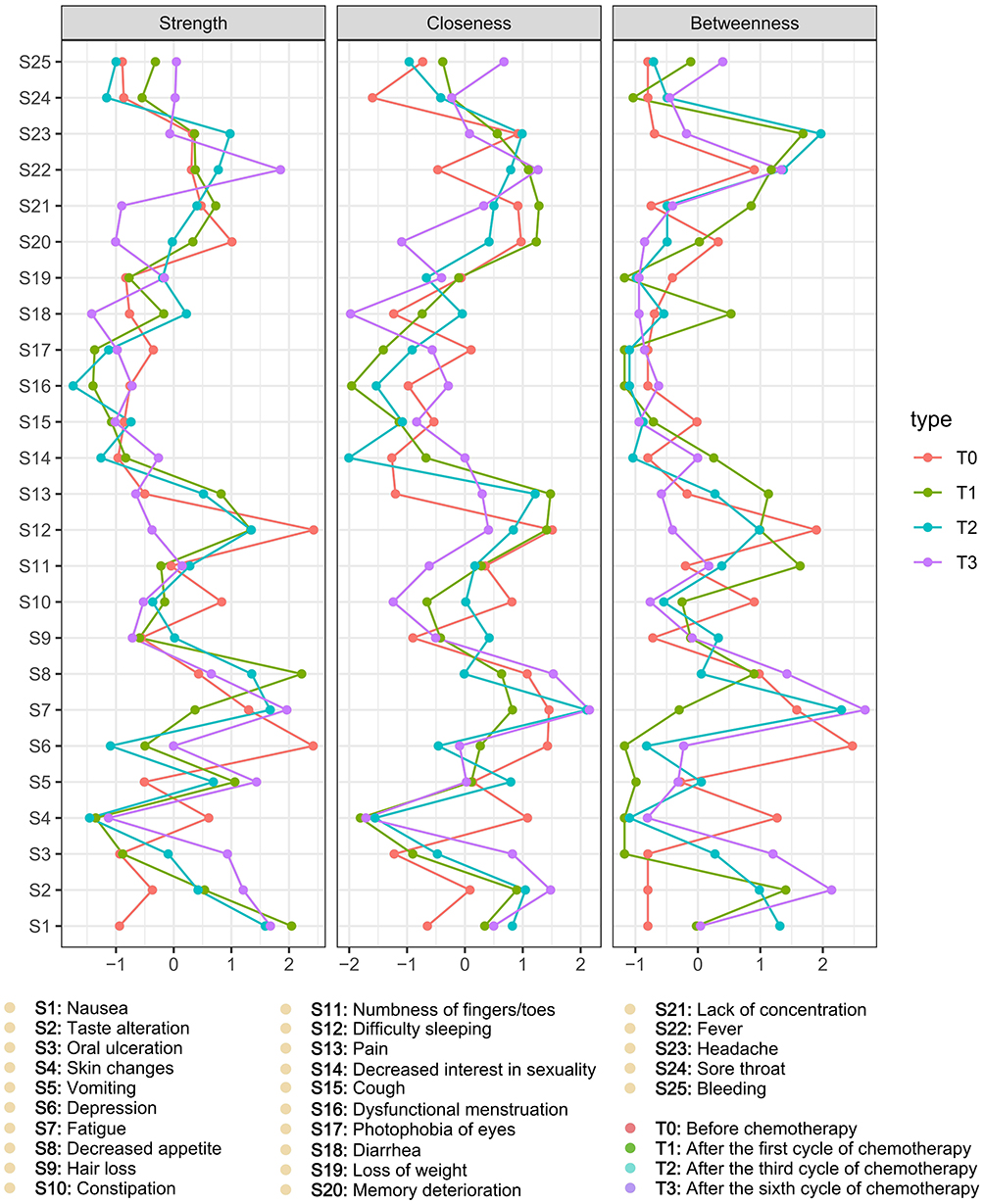 |
Figure 2 The centrality indices of symptoms. |
Stability of Symptom Networks
The stability of the centrality indices was estimated using the subset bootstrap approach, and the results are shown in Figure 3. Meanwhile, we estimated the centrality stability coefficient (CS-coefficient), refer to Table 2. The CS-coefficient for betweenness centrality at T1 was 0.206, suggesting insufficient stability for interpreting its node ranking. This lower stability is methodologically expected because betweenness centrality is a global measure that depends on shortest paths, making it inherently sensitive to structural perturbations. This property results in its lower stability relative to local metrics like strength and closeness.26 When the node ranking stability of a centrality measure is insufficient, its specific order should be interpreted with caution.23 Therefore, our subsequent interpretation of core symptoms at each time point prioritizes findings from indices with robust stability (CS-coefficient > 0.25).
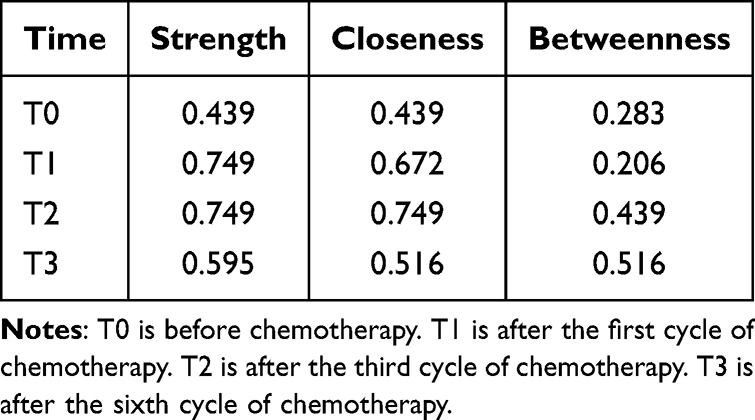 |
Table 2 The Centrality Indices’ CS Coefficient at Various Time Points |
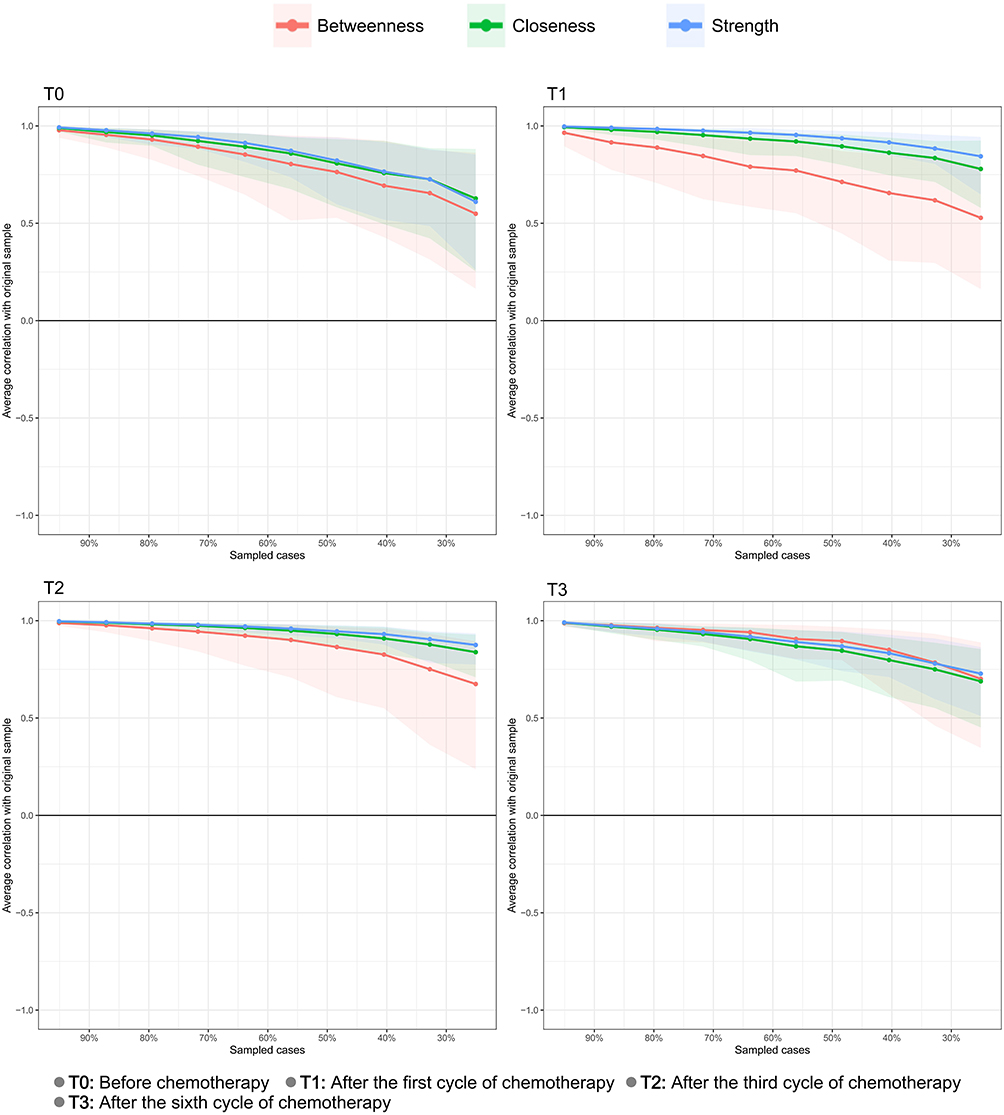 |
Figure 3 Stability of symptom networks. |
Discussion
The present study aimed to construct a symptom network of breast cancer patients undergoing various stages of chemotherapy and to identify the core symptoms that require focus for intervention at various phases. Centrality indicators are quantitative metrics that determine the significance of nodes in a network structure.27 The symptoms with the highest centrality index are core symptoms in the symptom network and serve as significant targets for intervention.28 Our study discovered that the core symptoms of breast cancer patients vary between chemotherapy stages. Difficulty sleeping and depression were the core symptoms at T0, decreased appetite and pain were the core symptoms at T1, and fatigue was the most central symptom at T2 and T3, which should be emphasized for intervention.
Before Chemotherapy (T0), Difficulty Sleeping and Depression Were the Core Symptoms
The results in this study showed that difficulty sleeping in breast cancer chemotherapy patients at T0 was the symptom with the highest both strength centrality and closeness centrality in the symptom network, and the betweenness centrality was also high, with strong correlations with symptoms such as depression, lack of concentration, and fatigue. At this stage, difficulty sleeping may originate from the acute psychogenic stress induced by the cancer diagnosis and impending treatment. Intense fear, uncertainty can trigger disruptions in the sleep-wake circadian rhythm and neuroendocrine alterations, directly compromising sleep homeostasis.29,30 These early physiological changes enable difficulty sleeping to form tight connections with multiple symptoms such as depression and fatigue even before chemotherapy initiation, thereby establishing its central position within the symptom network. Previous research has also shown that poor sleep quality in breast cancer patients receiving chemotherapy is closely correlated with a number of symptoms, including fatigue, sadness, and memory deterioration,31 and improving sleep quality may help relieve other related symptoms.32 Thus, difficulty sleeping is one of the symptoms that should be addressed during the T0 phase, and intervening on it may assist to mitigate the intensity of other symptoms in the network. Difficulty sleeping in patients at this time may be linked to psychological stress connected with cancer diagnosis and therapy,33,34 as well as discomfort associated with the disease and treatment.35 Sleep problems can have substantial consequences for patients’ cognitive function,36 immunological function,37 and quality of life.38 However, most patients believe that all of the side effects of chemotherapy are caused by the medications themselves and neglect sleep issues.39 This suggests that healthcare practitioners ought to remind patients about the hazards of sleep problems and encourage them to actively seek help when they arise. Furthermore, the assessment of sleep quality in breast cancer patients should be strengthened, and individualized and precise intervention programs should be developed to address the degree and causes of difficulty sleeping in order to weaken the impact of it in the symptom network, reduce the severity of the symptom, and improve the precision and efficiency of managing patients’ overall symptom burden.
Depression was the most important bridging symptom in the symptom network, with the highest betweenness centrality, high strength centrality, and closeness centrality, as well as strong relationships with symptoms including difficulty sleeping and decreased appetite. The significant degree of negative emotions experienced by breast cancer patients before treatment has been corroborated by previous studies.40 Similar findings were made by researchers Kalantari,41 who confirmed the high strength centrality of depression and anxious feelings in cancer patients prior to chemotherapy as an issue that needed to be assessed and managed. This might be attributed to the fact that, currently, the patients have not commenced chemotherapy and were uncertain about the potential impact of the treatment on their condition. Perhaps they were more concerned with the prognosis of their illness and the side effects of chemotherapy, which showed up as feeling down. Depression is not only directly associated with potential dysregulation of the neuroendocrine axis due to psychological stress but also forms a tight bidirectional vicious cycle with sleep disturbance.42 Furthermore, the neuroinflammatory state potentially induced by the tumor may provide a shared biological basis for depression and multiple other symptoms such as inattention and fatigue, naturally rendering it a core bridging symptom that connects others within the network.43,44 The link between depression and other symptoms has long been recognized. According to Colagiuri’s research, sleep issues may be caused by increasing depression, and difficulty sleeping may also result in increased depression in patients.45 Many studies have also founded that patients’ psychological difficulties are directly tied to their appetite, with negative emotions having a significant impact on patients’ appetite.46,47 Due to the centrality of depression in the symptom network, managing depression symptoms directly in breast cancer chemotherapy patients at T0 may alleviate other related symptoms, lessen or eliminate their propagating influence on the symptom network, and reduce or break off links between other symptoms. Medical personnel should concentrate on the psychological status of breast chemotherapeutic cancer patients at T0, identify the causes of depression, encourage patients to actively seek professional aid, and give tailored psychological care to patients.
After the First Cycle of Chemotherapy (T1), Decreased Appetite and Pain Were the Core Symptoms
The symptom network analysis revealed that decreased appetite have the highest strength centrality at T1 and was closely associated with nausea, taste alteration, and vomiting, making it the most central symptom in the symptom network at this point. This differs slightly from the results of Zhu et al,48 whose network analysis of 1065 patients after initial treatment found that decreased appetite, while high in strength centrality (second to distress and sadness), was not the most central symptom. The reasons for different findings could be attributed to the heterogeneity of the included patients, changes in evaluation time points, and other factors, but there is enough evidence to conclude that decreased appetite is important in the symptom network of cancer patients. Furthermore, nausea and vomiting have high strength in the symptom network. Reduced appetite, along with nausea and vomiting, comprise a cluster of gastrointestinal symptoms that interact with one another.49,50 Symptoms such as nausea, vomiting, and altered taste sense diminish patients’ food intake by altering their appetite, resulting in the development of other symptoms such as weight loss, fatigue, and depression.51,52 In addition to conventional drug prophylaxis, non-pharmacological treatments such as dietary interventions,53 auricular acupuncture interventions,54 and oral cryotherapy55 can be used to control gastrointestinal symptoms, particularly decreased appetite, in patients undergoing chemotherapy for breast cancer, which enabled patients to ensure their basic energy intake in order to better cope with the disease and the treatment’s adverse effects. This may help to decrease the occurrence of additional symptoms.
Pain is a real or potentially unpleasant emotional experience or sensation caused by tissue injury.56 The findings of this study showed that pain has the highest closeness centrality in the symptom network, as well as high strength and betweenness centrality, indicating that it plays a critical role in the symptom network at this stage of the process and that it is a core symptom that should be targeted for intervention. The mechanisms by which pain occurs in individuals undergoing chemotherapy for breast cancer are complex, and their genesis is not entirely understood.57 Post-chemotherapy pain may be associated with paclitaxel-based chemotherapy.58 Paclitaxel-based medication regimens are crucial for improving survival in patients with early-stage invasive breast cancer,59 and the majority of the patients in our study received chemotherapy that contained paclitaxel-based medicines. Pain in breast cancer patients does not occur in isolation but is closely intertwined with multiple distressing symptoms. It can exacerbate fatigue by interfering with sleep.60,61 Furthermore, abnormal inflammatory responses related to cancer and its treatment may promote a bidirectional vicious cycle between pain and symptoms like fatigue and depression through several interrelated pathways.62 These interactions collectively render pain a core symptom connecting physical and psychological symptom domains. As a result, active pain assessment and intervention are critical for reducing total symptom burden and increasing patients’ quality of life. In addition to medication, non-pharmacological therapies such as music therapy,63 relaxation therapy,64 and acupuncture65 can be used to intervene in order to alleviate the patient’s pain symptom while weakening the link between pain and other symptoms in the network, as well as to improve symptom management efficiency.
After the third and sixth cycles of chemotherapy (T2 and T3), fatigue was the most core symptom in breast cancer patients, and should be prioritized for management
Fatigue is a subjective, continuous feeling of exhaustion that does not correspond to the quantity of recent activity done.66 The results of the present study showed that the strength, closeness, and betweenness centrality of fatigue were highest at T2 and T3, indicating the central role of it at these two time points. Berger67 observed 219 individuals receiving chemotherapy for breast cancer and discovered that fatigue was a core symptom in the cluster of treatment-related symptoms following the patient’s last chemotherapy cycle. Cai’s network analysis21 also revealed that fatigue was a core symptom in the community of female breast cancer patients undergoing chemotherapy. Previous research has shown that feeling fatigued can occur at any stage of cancer therapy, with prevalence rates ranging from 43% to 85%,68,69 and that fatigue is more severe in breast cancer patients than in other cancers.70 The important significance of fatigue throughout the T2 and T3 phases of chemotherapy in breast cancer patients may be attributed to the cumulative physiological dysregulation caused by multi-cycle chemotherapeutic drugs, as well as the intricate interplay within the symptoms network. As therapy progresses, the buildup of drug toxicity and side effects might trigger the release of pro-inflammatory cytokines, resulting in dysregulation of central regulatory functions and severe and persistent fatigue.71,72 Concurrently, gastrointestinal issues such as nausea, vomiting, and decreased appetite after chemotherapy may impair caloric intake and exercise tolerance, increasing fatigue.4,73 Moreover, fatigue is often tightly interwoven with other symptoms like sleep disturbance, depression, and pain, creating a mutually reinforcing vicious cycle that is difficult to break.74 Within this intricate symptom network, fatigue appears to serve a dual role: it is both a critical outcome of multiple converging pathophysiological mechanisms and a key driver that exacerbates other symptoms and amplifies the overall symptom burden.
Since fatigue was so central to the symptom network, making it a key focus in the symptom management of breast cancer patients at T2 and T3 may help to reduce its transmissive role in the symptom network, alleviate fatigue while improving other symptoms related to it, and improve symptom management efficiency. As a result, assessing and intervening for this symptom in patients is critical. Healthcare professionals should recognize the critical role of fatigue in the symptom network of breast cancer chemotherapy patients, encourage patients to actively report their symptoms, and educate them to manage fatigue through exercise75,76 and music,77 as well as provide timely feedback on the effectiveness of symptom management. Furthermore, relevant studies should be performed to investigate the major role of fatigue in the symptom experience of breast cancer chemotherapy patients, the mechanisms of fatigue, and possible ways to improve the accuracy and effectiveness of symptom management.
Strengths and Limitations
To the best of our knowledge, this is the first study to apply a network analytic approach to uncover changes in core symptoms in breast cancer patients during chemotherapy sessions. In this study, symptom networks of patients were created at various time points, and the robustness of the symptom networks and centrality indicators were investigated to confirm the findings’ reliability. Although our study has many strengths, there are a few limitations that must be addressed. To begin with, this study only sampled breast cancer patients from four tertiary hospitals in Chengdu City, Sichuan Province, for survey follow-up via convenience sampling, so extrapolating the study findings to breast cancer patients in other regions and hospitals requires further verification. Second, due to human, material, and time restrictions, only three follow-up visits were done in this investigation, potentially missing changes in symptoms at more closely spaced time periods. Third, we excluded individuals with significant comorbidities and cognitive deficiencies who were unable to complete the scale assessment, thus the intensity and centrality of symptoms may have been underestimated. Finally, the findings of this investigation revealed that the CS coefficient of betweenness centrality at T1 was just 0.206, suggesting restricted interpretability.23 As a result, we neglected the symptoms of high betweenness centrality at this stage. Future research could increase the sample size to improve the stability of the symptom network’s betweenness centrality.
Impact on Practice and Research
The study has significant implications for practice and research. First and foremost, the symptom experience of breast cancer patients will change dynamically with the various cycles of chemotherapy, and dynamic monitoring of patients’ symptoms during the chemotherapy period should be carried out, which can not only monitor the patients’ conditions, but also understand the pattern of change of the patients’ symptoms and manage them with timely and effective interventions, thereby reducing the burden of the patients’ symptoms. Second, this study discovered that the core symptoms of breast cancer patients vary depending on the cycle of chemotherapy they receive. This recommends that medical personnel should have a better grasp of symptom genesis, evolution throughout time, and interaction mechanisms, as well as focus effective care of core symptoms at various time periods to improve patient symptom management efficiency. Furthermore, the concept of symptom networks has promising implications for both study and practice in symptom management science. The symptom network’s main purpose is to determine the network’s core symptoms and explore the mechanism by which various symptoms are associated. By fulfilling these aims, healthcare providers will have a better understanding of how symptoms develop and interact, allowing them to develop more specific and effective interventions. It is important to note that while network analysis can identify core symptoms in patients, the accuracy of its results requires further verification. Currently, some researchers have begun to use symptom networks to explore the influence of biomarkers on symptom development.78,79 A promising direction for future work is to integrate symptoms and biomarkers within a network analytic framework. Such an integrated approach could enable a systematic examination of whether core symptoms are significantly associated with specific biological pathways, providing mechanistic validation for network analysis and possibly revealing potential shared pathobiological mechanisms within complex symptom networks.
Conclusions
We conducted the first dynamic analysis of core symptoms in breast cancer patients across different chemotherapy phases. Our findings revealed that the core symptoms requiring prioritized management differ between chemotherapy cycles. Difficulty sleeping and depression were the core symptoms to manage in the network of pre-chemotherapy symptoms in breast cancer patients; decreased appetite and pain were the core symptoms to focus on after the first chemotherapy treatment; and fatigue is the most central symptom to prioritize for intervention at the T2 and T3 time points. These findings suggest that symptom management for breast cancer patients undergoing chemotherapy should follow a “stage-specific and prioritized” paradigm, with specific interventions targeting the distinct core symptoms at different time periods. Interventions that target these crucial nodes in the symptom network may have a synergistic regulatory effect on other closely related symptoms, thereby facilitating the relief of the entire symptom clusters. The ultimate integrated goals are to reduce patients’ symptom burden and enhance their quality of life. Future research should further validate these conclusions in larger, more diverse patient cohorts and investigate the interplay between core and peripheral symptoms in more detail. Furthermore, the actual effectiveness of intervention strategies targeting core symptoms in improving patients’ overall health outcomes should be scientifically evaluated through relevant research.
Data Sharing Statement
The data that support the findings of this study are available from the two corresponding authors upon reasonable request.
Acknowledgment
The authors would like to thank all the healthcare professionals and breast cancer patients from the four tertiary hospitals. Our sincere appreciation is given to all participating units. Meanwhile, we gratefully acknowledge Dr. Jingting Liao from Chengdu Jinniu District People’s Hospital for securing the ethical approvals critical to this study.
Funding
This work was supported by the Xinglin Scholars Nursery Talent Program of Chengdu University of Traditional Chinese Medicine (Grant No. MPRC2023050).
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;2024:1–15. doi:10.3322/caac.21834
2. Prieto-Callejero B, Rivera F, Fagundo-Rivera J, et al. Relationship between chemotherapy-induced adverse reactions and health-related quality of life in patients with breast cancer. Medicine. 2020;99(33):e21695. doi:10.1097/MD.0000000000021695
3. Rose L, Lustberg M, Ruddy KJ, et al. Hair loss during and after breast cancer therapy. Support Care Cancer. 2023;31(3):186. doi:10.1007/s00520-023-07634-5
4. Naito Y, Kai Y, Ishikawa T, et al. Chemotherapy-induced nausea and vomiting in patients with breast cancer: a prospective cohort study. Breast Cancer. 2020;27(1):122–128. doi:10.1007/s12282-019-01001-1
5. Zhu W, Li W, Gao J, et al. Factors associated with the sleep disturbances of people with breast cancer during chemotherapy in China: a cross-sectional study. Nurs Open. 2023;10(8):5453–5461. doi:10.1002/nop2.1784
6. Guo Y, Ju Q, You M, et al. Depression, anxiety and stress among metastatic breast cancer patients on chemotherapy in China. BMC Nurs. 2023;22(1):33. doi:10.1186/s12912-023-01184-1
7. Wkw S, Law BMH, Ng MSN, et al. Symptom clusters experienced by breast cancer patients at various treatment stages: a systematic review. Cancer Med. 2021;10(8):2531–2565. doi:10.1002/cam4.3794
8. Neugut AI, Hillyer GC, Kushi LH, et al. A prospective cohort study of early discontinuation of adjuvant chemotherapy in women with breast cancer: the breast cancer quality of care study (BQUAL). Breast Cancer Res Treat. 2016;158(1):127–138. doi:10.1007/s10549-016-3855-3
9. Chongkham-ang S, Wonghongkul T, Panuthai S, et al. Symptom experience and symptom clusters of Thai women with breast cancer receiving chemotherapy. Pac Rim Int J Nurs R. 2018;22(1):43–57.
10. Nho J-H, Kim S-R, Park M-H, et al. Symptom clusters and quality of life in breast cancer survivors after cancer treatment in a tertiary hospital in Korea. Eur J Cancer Care. 2018;27(6):e12919. doi:10.1111/ecc.12919
11. Albusoul RM, Berger AM, Gay CL, et al. Symptom clusters change over time in women receiving adjuvant chemotherapy for breast cancer. J Pain Symptom Manage. 2017;53(5):880–886. doi:10.1016/j.jpainsymman.2016.12.332
12. Wong WM, Chan DNS, He X, et al. Effectiveness of Pharmacological and Nonpharmacological Interventions for Managing the Fatigue–Sleep Disturbance–Depression Symptom Cluster in Breast Cancer Patients Undergoing Chemotherapy. Cancer Nurs. 2023;46(2):E70–E80. doi:10.1097/NCC.0000000000001048
13. Papachristou N, Barnaghi P, Cooper B, et al. Network analysis of the multidimensional symptom experience of oncology. Sci Rep. 2019;9(1):2258. doi:10.1038/s41598-018-36973-1
14. Zhu Z, Hu T, Jin Y, et al. Symptom Networks:Basic Concepts and Implementation in Symptom Science. J Nurs Train. 2023;38(24):2214–2218+2224. doi:10.16821/j.cnki.hsjx.2023.24.002
15. Yang Z, Zhu Z, Hu Y, et al. A review of network approach in symptom management. J Nurs Sci. 2022;37(5):91–94. doi:10.3870/j.issn.1001-4152.2022.05.091
16. Fried EI, eBoschloo L, Borkulo C, et al. Commentary: consistent superiority of selective serotonin reuptake inhibitors over placebo in reducing depressed mood in patients with major depression. Front Psychiatry. 2015;6:1–3. doi:10.3389/fpsyt.2015.00117
17. Santos HP, Kossakowski JJ, Schwartz TA, et al. Longitudinal network structure of depression symptoms and self-efficacy in low-income mothers. PLoS One. 2018;13(1):e0191675. doi:10.1371/journal.pone.0191675
18. Bekhuis E, Schoevers R, de Boer M, et al. Symptom-specific effects of psychotherapy versus combined therapy in the treatment of mild to moderate depression: a network approach. Psychother Psychosom. 2018;87(2):121–123. doi:10.1159/000486793
19. Wang K, Diao M, Yang Z, et al. Identification of Core Symptom Cluster in Patients With Digestive Cancer: a Network Analysis. Cancer Nurs. 2023;48(1):E55–E63. doi:10.1097/NCC.0000000000001280
20. Zhang J, Zhao X, Zhang G, et al. Network analysis of core symptom changes in lung cancer survivors: a longitudinal study. J Cancer Surviv. 2025. doi:10.1007/s11764-025-01844-y
21. Cai T, Zhou T, Huang Q, et al. Cancer-related symptoms among young and middle-aged women undergoing chemotherapy for breast cancer: application of latent class analysis and network analysis. Eur J Oncol Nurs. 2023;63:102287. doi:10.1016/j.ejon.2023.102287
22. Liang M, Zhong T, Knobf MT, et al. Sentinel and networked symptoms in patients with breast cancer undergoing chemotherapy. Eur J Oncol Nurs. 2024;70:102566. doi:10.1016/j.ejon.2024.102566
23. Epskamp S, Borsboom D, Fried EI. Estimating psychological networks and their accuracy: a tutorial paper. Behav Res Methods. 2018;50(1):195–212. doi:10.3758/s13428-017-0862-1
24. Rha SY, Lee J. Stable symptom clusters and evolving symptom networks in relation to chemotherapy cycles. J Pain Symptom Manage. 2021;61(3):544–554. doi:10.1016/j.jpainsymman.2020.08.008
25. Wen C, Lu Q, Ding Y, et al. Development and psychometric testing of the symptoms assessment inventory for breast cancer patients receiving chemotherapy. Chin J Nurs. 2012;47(5):451–453. doi:10.1002/pon.3907
26. Segarra S, Ribeiro A. Stability and Continuity of Centrality Measures in Weighted Graphs. IEEE Trans Signal Process. 2016;64(3):543–555. doi:10.1109/TSP.2015.2486740
27. Costantini G, Epskamp S, Borsboom D, et al. State of the aRt personality research: a tutorial on network analysis of personality data in R. J Res Pers. 2015;54:13–29. doi:10.1016/j.jrp.2014.07.003
28. Rodebaugh TL, Tonge NA, Piccirillo ML, et al. Does centrality in a cross-sectional network suggest intervention targets for social anxiety disorder? J Consult Clin Psychol. 2018;86(10):831–844. doi:10.1037/ccp0000336
29. Li W, Kwok CC-H, Chan DC-W, et al. Disruption of sleep, sleep-wake activity rhythm, and nocturnal melatonin production in breast cancer patients undergoing adjuvant chemotherapy: prospective cohort study. Sleep Med. 2018;55:14–21. doi:10.1016/j.sleep.2018.11.022
30. Perrier J, Duivon M, Clochon P, et al. Sleep macro- and microstructure in breast cancer survivors. Sci Rep. 2022;12(1):2557. doi:10.1038/s41598-022-06664-z
31. Ratcliff CG, Zepeda SG, Hall MH, et al. Patient characteristics associated with sleep disturbance in breast cancer survivors. Support Care Cancer. 2021;29(5):2601–2611. doi:10.1007/s00520-020-05777-3
32. Dun L, Xian-Yi W, Si-Ting H, et al. Effects of sleep interventions on cancer-related fatigue and quality of life in cancer patients: a systematic review and meta-analysis. Support Care Cancer. 2022;30(4):3043–3055. doi:10.1007/s00520-021-06563-5
33. Shorofi SA, Nozari-Mirarkolaei F, Arbon P, et al. Depression and sleep quality among Iranian women with breast cancer. Asian Pac J Cancer Prev. 2021;22(11):3433–3440. doi:10.31557/APJCP.2021.22.11.3433
34. Aggeli P, Fasoi G, Zartaloudi A, et al. Posttreatment anxiety, depression, sleep disorders, and associated factors in women who survive breast cancer. Asia Pac J Oncol Nurs. 2021;8(2):147–155. doi:10.4103/apjon.apjon_65_20
35. Fakih R, Rahal M, Hilal L, et al. Prevalence and severity of sleep disturbances among patients with early breast cancer. Indian J Palliat Care. 2018;24(1):35–38. doi:10.4103/IJPC.IJPC_137_17
36. Rodriguez N, Fawcett JM, Rash JA, et al. Factors associated with cognitive impairment during the first year of treatment for nonmetastatic breast cancer. Cancer Med. 2021;10(4):1191–1200. doi:10.1002/cam4.3715
37. Ruel S, Ivers H, Savard M-H, et al. Insomnia, immunity, and infections in cancer patients: results from a longitudinal study. Health Psychol. 2020;39(5):358–369. doi:10.1037/hea0000811
38. Mejía-Rojas ME, Contreras-Rengifo A, Hernández-Carrillo M. Quality of life in women treated with chemotherapy for breast cancer in Cali, Colombia. Biomedica. 2020;40(2):349–361. doi:10.7705/biomedica.4971
39. Imanian M, Imanian M, Karimyar M. Sleep Quality and Fatigue among Breast Cancer Patients Undergoing Chemotherapy. Int J Hematol Oncol Stem Cell Res. 2019;13(4):196–200.
40. Luo R, Chen H, Liu Y, et al. Symptom clusters among breast cancer patients in relation to chemotherapy cycles: a longitudinal study. Support Care Cancer. 2023;31(10):573. doi:10.1007/s00520-023-08038-1
41. Kalantari E, Kouchaki S, Miaskowski C, et al. Network analysis to identify symptoms clusters and temporal interconnections in oncology patients. Sci Rep. 2022;12(1):17052. doi:10.1038/s41598-022-21140-4
42. Ahmad MH, Rizvi MA, Fatima M, et al. Pathophysiological implications of neuroinflammation mediated HPA axis dysregulation in the prognosis of cancer and depression. Mol Cell Endocrinol. 2020;520:111093. doi:10.1016/j.mce.2020.111093
43. Al-Bashaireh AM, Khraisat O, Alnazly EK, et al. Inflammatory Markers, Metabolic Profile, and Psychoneurological Symptoms in Women with Breast Cancer: a Literature Review. Cureus. 2021;13(11):e19953. doi:10.7759/cureus.19953
44. Strehle LD, Otto-Dobos LD, Grant CV, et al. Microglia contribute to mammary tumor-induced neuroinflammation in a female mouse model. FASEB J. 2024;38(2):e23419. doi:10.1096/fj.202301580RR
45. Colagiuri B, Christensen S, Jensen AB, et al. Prevalence and predictors of sleep difficulty in a national cohort of women with primary breast cancer three to four months postsurgery. J Pain Symptom Manage. 2011;42(5):710–720. doi:10.1016/j.jpainsymman.2011.02.012
46. Joshy G, Thandrayen J, Koczwara B, et al. Disability, psychological distress and quality of life in relation to cancer diagnosis and cancer type: population-based Australian study of 22,505 cancer survivors and 244,000 people without cancer. BMC Med. 2020;18(1):372. doi:10.1186/s12916-020-01830-4
47. Yoon S-I, Moon H-R, Lee SR, et al. Nutrient Inadequacy in Korean Young Adults with Depression: a Case Control Study. Nutrients. 2023;15(9). doi:10.3390/nu15092195
48. Zheng Z, Yanling S, Yi K, et al. Contemporaneous symptom networks of multidimensional symptom experiences in cancer survivors: a network analysis. Cancer Med. 2022;12(1):663–673. doi:10.1002/cam4.4904
49. Singh K, Kober KM, Paul SM, et al. Gastrointestinal symptoms are associated with trajectories of chemotherapy-induced nausea. Support Care Cancer. 2020;28(5):2205–2215. doi:10.1007/s00520-019-05031-5
50. Singh KP, Kober KM, Ernst B, et al. Multiple Gastrointestinal Symptoms Are Associated With Chemotherapy-Induced Nausea in Patients With Breast Cancer. Cancer Nurs. 2022;45(3):181–189. doi:10.1097/NCC.0000000000000976
51. de Vries YC, van den Berg MMGA, de Vries JHM, et al. Differences in dietary intake during chemotherapy in breast cancer patients compared to women without cancer. Support Care Cancer. 2017;25(8):2581–2591. doi:10.1007/s00520-017-3668-x
52. Kiss N, Symons K, Hewitt J, et al. Taste function in adults undergoing cancer radiotherapy or chemotherapy, and implications for nutrition management: a systematic review. J Acad Nutr Diet. 2021;121(2):278–304. doi:10.1016/j.jand.2020.08.014
53. Abdollahi R, Najafi S, Razmpoosh E, et al. The Effect of Dietary Intervention Along with Nutritional Education on Reducing the Gastrointestinal Side Effects Caused by Chemotherapy Among Women with Breast Cancer. Nutr Cancer. 2019;71(6):922–930. doi:10.1080/01635581.2019.1590608
54. Tan J-Y, Liu J, Suen LKP, et al. Development and validation of an evidence-based auricular acupressure intervention for managing chemotherapy-induced nausea and vomiting in breast cancer patients. Complement Ther Med. 2020;52:102502. doi:10.1016/j.ctim.2020.102502
55. Kurt B, Kapucu S, Çakmak Öksüzoğlu BÖ. Effects of Oral Cryotherapy on Anticipatory, and Acute Nausea and Vomiting in Patients With Breast Cancer Undergoing Adjuvant Chemotherapy: a Randomized Controlled Clinical Trial. Clin Breast Cancer. 2024;24(2):112–121. doi:10.1016/j.clbc.2023.10.012
56. Leysen L, Beckwée D, Nijs J, et al. Risk factors of pain in breast cancer survivors: a systematic review and meta-analysis. Support Care Cancer. 2017;25(12):3607–3643. doi:10.1007/s00520-017-3824-3
57. Langford DJ, Paul SM, Cooper B, et al. Comparison of subgroups of breast cancer patients on pain and co-occurring symptoms following chemotherapy. Support Care Cancer. 2016;24(2):605–614. doi:10.1007/s00520-015-2819-1
58. Saito Y, Takekuma Y, Takeshita T, et al. Dexamethasone dose-dependently prevents taxane-associated acute pain syndrome in breast cancer treatment. Support Care Cancer. 2023;31(6):372. doi:10.1007/s00520-023-07852-x
59. De Iuliis F, Taglieri L, Salerno G, et al. Taxane induced neuropathy in patients affected by breast cancer: literature review. Crit Rev Oncol Hematol. 2015;96(1):34–45. doi:10.1016/j.critrevonc.2015.04.011
60. Peoples AR, Pigeon WR, Li D, et al. Association Between Pretreatment Sleep Disturbance and Radiation Therapy-Induced Pain in 573 Women With Breast Cancer. J Pain Symptom Manage. 2021;61(2):254–261. doi:10.1016/j.jpainsymman.2020.07.041
61. Shabangu N, Thebe T, Casey M, et al. Chronic pain in female breast cancer survivors - prevalence, characteristics and contributing factors: a cross-sectional pilot study. BMC Womens Health. 2023;23(1):613. doi:10.1186/s12905-023-02766-6
62. Lyon DE, Starkweather A, Yao Y, et al. Pilot Study of Metabolomics and Psychoneurological Symptoms in Women With Early Stage Breast Cancer. Biol Res Nurs. 2017;20(2):227–236. doi:10.1177/1099800417747411
63. Li Y, Xing X, Shi X, et al. The effectiveness of music therapy for patients with cancer: a systematic review and meta-analysis. J Adv Nurs. 2020;76(5):1111–1123. doi:10.1111/jan.14313
64. Eaton LH, Hulett JP, Langford DJ, et al. How theory can help facilitate implementing relaxation as a complementary pain management approach. Pain Manag Nurs. 2019;20(3):207–213. doi:10.1016/j.pmn.2018.12.008
65. Jeong YJ, Kwak MA, Seo JC, et al. Acupuncture for the Treatment of Taxane-Induced Peripheral Neuropathy in Breast Cancer Patients: a Pilot Trial. Evid Based Complement Alternat Med. 2018;2018:5367014. doi:10.1155/2018/5367014
66. Fabi A, Bhargava R, Fatigoni S, et al. Cancer-related fatigue: ESMO clinical practice guidelines for diagnosis and treatment. Ann Oncol. 2020;31(6):713–723. doi:10.1016/j.annonc.2020.02.016
67. Berger AM, Kumar G, LeVan TD, et al. Symptom clusters and quality of life over 1 year in breast cancer patients receiving adjuvant chemotherapy. Asia Pac J Oncol Nurs. 2020;7(2):134–140. doi:10.4103/apjon.apjon_57_19
68. Thong MSY, van Noorden CJF, Steindorf K, et al. Cancer-related fatigue: causes and current treatment options. Curr Treat Options Oncol. 2020;21(2):17. doi:10.1007/s11864-020-0707-5
69. Puigpinós-Riera R, Serral G, Sala M, et al. Cancer-related fatigue and its determinants in a cohort of women with breast cancer: the DAMA Cohort. Support Care Cancer. 2020;28(11):5213–5221. doi:10.1007/s00520-020-05337-9
70. Mustian KM, Alfano CM, Heckler C, et al. Comparison of pharmaceutical, psychological, and exercise treatments for cancer-related fatigue: a meta-analysis. JAMA Oncol. 2017;3(7):961–968. doi:10.1001/jamaoncol.2016.6914
71. Bower JE, Ganz PA, Irwin MR, et al. Inflammation and behavioral symptoms after breast cancer treatment: do fatigue, depression, and sleep disturbance share a common underlying mechanism? J Clin Oncol. 2011;29(26):3517–3522. doi:10.1200/JCO.2011.36.1154
72. Hiensch AE, Mijwel S, Bargiela D, et al. Inflammation Mediates Exercise Effects on Fatigue in Patients with Breast Cancer. Med Sci Sports Exerc. 2021;53(3):496–504. doi:10.1249/MSS.0000000000002490
73. Charalambous A, Giannakopoulou M, Bozas E, et al. Parallel and serial mediation analysis between pain, anxiety, depression, fatigue and nausea, vomiting and retching within a randomised controlled trial in patients with breast and prostate cancer. BMJ Open. 2019;9(1):e026809. doi:10.1136/bmjopen-2018-026809
74. Qi Y, Li H, Guo Y, et al. Symptom Clusters in Breast Cancer Patients Receiving Adjuvant Chemotherapy: a Systematic Review. J Clin Nurs. 2024;33(12):4554–4567. doi:10.1111/jocn.17479
75. Bland KA, Kirkham AA, Bovard JM, et al. Effect of Exercise During Versus After Chemotherapy for Breast Cancer on Fatigue and Quality Of Life. Med Sci Sports Exercise. 2019;51(6S):5–6. doi:10.1249/01.mss.0000560503.59726.88
76. O’Neill M, Samaroo D, Lopez C, et al. The Effect of Yoga Interventions on Cancer-Related Fatigue and Quality of Life for Women with Breast Cancer: a Systematic Review and Meta-Analysis of Randomized Controlled Trials. Integr Cancer Ther. 2020;19:1534735420959882. doi:10.1177/1534735420959882
77. Qi Y, Lin L, Dong B, et al. Music interventions can alleviate cancer-related fatigue: a metaanalysis. Support Care Cancer. 2021;29(7):3461–3470. doi:10.1007/s00520-021-05986-4
78. Li H, Tong Y, Li J, et al. Network Analysis of Multidimensional Symptoms and Inflammatory Biomarkers in Chinese Patients with Glioma. J Inflamm Res. 2025;18:7083–7095. doi:10.2147/JIR.S517105
79. Santoso AMM, Jansen F, Peeters CFW, et al. Psychoneurological Symptoms and Biomarkers of Stress and Inflammation in Newly Diagnosed Head and Neck Cancer Patients: a Network Analysis. Curr Oncol. 2022;29(10):7109–7121. doi:10.3390/curroncol29100559
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Cost-Effectiveness Analysis of the Oncotype DX Breast Recurrence Score® Test in Node-Negative Early Breast Cancer
Berdunov V, Millen S, Paramore A, Griffin J, Reynia S, Fryer N, Brown R, Longworth L
ClinicoEconomics and Outcomes Research 2022, 14:619-633
Published Date: 19 September 2022
Advice from One Patient to Another: Qualitative Analysis of Patients’ Perspectives About Chemotherapy Initiation
Malinowski C, Paredes E, Housten AJ, Chavez-MacGregor M
Patient Preference and Adherence 2022, 16:3283-3289
Published Date: 14 December 2022
Dietary Behavior and Its Association with Nutrition Literacy and Dietary Attitude Among Breast Cancer Patients Treated with Chemotherapy: A Multicenter Survey of Hospitals in China
Tang H, Wang R, Yan P, Zhang W, Yang F, Guo S, Li T, Yi L, Bai X, Lin S, Zhang Y, Shang L
Patient Preference and Adherence 2023, 17:1407-1419
Published Date: 9 June 2023
Breast Cancer: An Overview of Current Therapeutic Strategies, Challenge, and Perspectives
Wang J, Wu SG
Breast Cancer: Targets and Therapy 2023, 15:721-730
Published Date: 20 October 2023
Cost-Effectiveness Analysis of the Oncotype DX Breast Recurrence Score® Test from a US Societal Perspective
Berdunov V, Cuyun Carter G, Laws E, Luo R, Russell CA, Campbell S, Abdou Y, Force J
ClinicoEconomics and Outcomes Research 2024, 16:471-482
Published Date: 4 June 2024