Back to Journals » International Journal of Women's Health » Volume 18
Perioperative Symptom Trajectories and a Risk Prediction Model for Cervical Cancer: A Prospective Longitudinal Study
Authors Zhang Y, Wu Y, Wang Y, Yang J, Chen L, Xu C
Received 30 March 2026
Accepted for publication 10 June 2026
Published 16 June 2026 Volume 2026:18 613006
DOI https://doi.org/10.2147/IJWH.S613006
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Marta Barba
Yuting Zhang,1 Yaru Wu,1 Yuting Wang,1 Juan Yang,1 Ling Chen,2,3 Chunyan Xu2,3
1School of Nursing, Xinjiang Medical University, Urumqi, Xinjiang, People’s Republic of China; 2Department of Gynecological Surgery, Affiliated Tumor Hospital of Xinjiang Medical University, Urumqi, Xinjiang, People’s Republic of China; 3Health Care Research Center for Xinjiang Regional Population, Urumqi, Xinjiang, People’s Republic of China
Correspondence: Chunyan Xu, Email [email protected] Ling Chen, Email [email protected]
Background: This prospective longitudinal quantitative study aimed to clarify perioperative symptom cluster characteristics in cervical cancer patients, identify influencing factors and hematological indicators, and develop a clinically applicable risk prediction model.
Methods: A prospective longitudinal study was conducted at a tertiary cancer hospital in Northwest China (April 2024–June 2025). Symptoms were assessed using the MDASI-PeriOp-GYN scale at preoperative, postoperative, and pre-discharge time points. Exploratory PCA identified symptom cluster structures. Based on Linear Mixed Model we explore heterogeneous symptom trajectories. Independent predictors were screened using logistic regression and restricted cubic splines. Model performance was evaluated using ROC curves, calibration curves, and decision curve analysis.
Results: Five stable symptom clusters were determined: a general somatic symptom cluster, a psycho-neurological symptom cluster, a gastrointestinal motility and energy cluster, an emotional and eating disorder cluster, and a consciousness and sedation-related cluster; and patients were classified into three trajectories: well-recovered, moderately persistent and severely distressed types. Age, operative duration, fibrinogen, neutrophil-to-lymphocyte ratio and D-dimer were risk factors, while serum albumin and serum potassium were protective factors. The seven-indicator combined model had an AUC of 0.863, with sensitivity 68.4%, specificity 87.8% and accuracy 82.0%, possessing superior predictive effect compared with single indexes.
Conclusion: Patients in the severe distress trajectory showed rapid symptom changes around discharge, representing a high-risk group for perioperative management. The Nomogram prediction model effectively stratifies patients into high- and low-risk groups for severe symptom distress, enabling precise interventions, improving transitional care, and enhancing perioperative symptom management.
Keywords: cervical cancer, perioperative period, symptom clusters, hematological indicators, linear mixed model, longitudinal study, risk prediction model
Introduction
Cervical cancer is the fourth most common malignancy worldwide in terms of diagnosis rate among women, with approximately 660,000 new cases reported in 2022.1,2 Both its incidence and mortality rates remain high. In 2022, China recorded over 150,000 new cases of cervical cancer, ranking first globally.3,4 Although the Chinese government has progressively implemented health programs such as “two cancers” screening5,6 and cervical cancer elimination initiatives,7 the incidence and mortality rates of cervical cancer have continued to rise in recent years, posing a serious threat to women’s health. Surgery remains the primary treatment for early-stage cervical cancer, with postoperative survival rates exceeding 90%.8–10 However, surgery also induces various symptoms during the perioperative period, including fatigue, pain, sleep disturbances, and distress. These symptoms do not exist in isolation but cluster together through synergistic interactions, forming symptom clusters.11 Such symptom clusters can lead to changes in patients’ physical and emotional status, delay postoperative recovery, and present significant challenges to clinical practice.
At present, research on symptom clusters in cervical cancer patients, both domestically and internationally, has primarily focused on the chemoradiotherapy period. Although the composition of symptom clusters during this period varies depending on treatment stage and assessment methods, they generally exhibit relative stability.12,13 Domestic studies have mainly explored the relationship between symptom clusters and quality of life, identifying various types such as psychological and gastrointestinal symptom clusters.14–19, In contrast, systematic investigations of perioperative symptom clusters remain relatively limited, and most existing studies primarily emphasize symptomatic management.
Symptom assessment is a critical indicator for evaluating surgical outcomes and recovery in patients with cervical cancer,20 facilitating timely treatment adjustments and improved prognosis. Laboratory tests and pathological analyses can reflect tumor development and progression; however, pathological examinations are limited in their ability to dynamically monitor postoperative symptoms.21–25 Studies have shown that blood-based inflammatory and coagulation markers (eg, CA, NLR, PLR) can serve as reliable prognostic indicators for tumor patients.26–29 Additionally, clinical data and laboratory parameters have been effectively utilized to predict cancer-related symptoms such as fatigue and pain.30,31 Current research on tumor symptom clusters, both domestically and internationally, largely relies on scale-based assessments and lacks systematic analyses integrating subjective symptoms with objective physiological indicators, making it difficult to accurately identify high-risk patients at an early stage. Hematological markers (eg, NLR, PLR) reflect systemic inflammation, which may drive symptom clustering; therefore, incorporating them could improve prediction accuracy. Unlike previous cross-sectional or cluster-only studies, this study uniquely (1) identifies perioperative symptom trajectories using LMM in cervical cancer; (2) integrates longitudinal symptom data with perioperative hematological markers; and (3) develops a clinically applicable risk prediction model.
Therefore, actively exploring the compositional changes of perioperative symptom clusters and the complex interrelationships among symptoms in cervical cancer patients, identifying relevant hematological indicators and influencing factors, and establishing a scientifically sound and practical risk prediction model hold significant clinical value for early identification of high-risk patients, development of individualized care plans, and alleviation of symptom burden.
Methods
Study Design and Setting
This prospective longitudinal study was conducted at a tertiary grade-A cancer hospital in Northwest China from April 2024 to June 2025, following the TRIPOD reporting guidelines.32
Based on preliminary investigations, the average hospital stay in this Gynecologic Care Center was 11 days, with 75.08% of patients staying≤7 days. Longitudinal assessments were conducted at three time points: T1 (1–2 days preoperatively): Preoperative preparation period, reflecting patients’ initial perceptions and concerns before surgical trauma; T2 (1–3 days postoperatively): Acute recovery period, representing the phase with the highest symptom burden; T3 (before discharge): Critical transition period, marking the shift from acute symptom relief to post-discharge rehabilitation.
Participants
Inclusion criteria were patients diagnosed with cervical cancer scheduled to undergo laparoscopic total hysterectomy with bilateral adnexectomy and/or pelvic lymph node dissection, with preoperative clinical stage T1–T2 and no evidence of lymph node metastasis or distant metastasis;9 aged ≥18 years, without cognitive impairment, and able to communicate effectively with medical staff; patients and their family members not concurrently participating in other similar studies, and are willing to voluntarily participate and provide information for the study.
Exclusion criteria included the presence of other major comorbid diseases; postoperative tumor stage upgrade; occurrence of severe intraoperative or postoperative complications (eg, major hemorrhage) precluding further follow-up; and voluntary withdrawal from the study for personal reasons during the research period.
Study Size
This study aims to develop a risk prediction model for perioperative symptom clusters in cervical cancer patients, representing a multivariable prediction model with a binary outcome. Sample size estimation followed the statistical principles for clinical prediction model development,32 ensuring an events per variable (EPV) ratio of ≥10 to prevent model overfitting and ensure stable estimation of βcoefficients. The total sample size was estimated as 10 to 20 times the number of candidate predictors. An additional 10% to 15% was added to account for potential loss to follow-up and data exclusions.
Based on literature review and clinical availability, 15 candidate predictors were initially included. Using a 15-fold multiplier and considering a 20% attrition rate, the minimum required sample size was 301 cases. A total of 405 questionnaires were distributed at T1. After excluding 12 patients receiving non-surgical treatment, 8 undergoing palliative surgery, 6 with altered surgical procedures and 6 who were discharged after refusing surgery, 373 valid questionnaires were retained. At T2, 6 patients were transferred to the ICU, 5 developed severe complications and 16 voluntarily withdrew from the study, leaving 346 valid questionnaires. At T3, 29 patients were lost to follow-up, and the final number of valid questionnaires was 317.
Instruments
Demographic Characteristics
Demographic characteristics collected included sociodemographic data such as age, education level, and marital status, as well as disease‑related information including body mass index, postoperative tumor stage, and operative duration.
Objective Laboratory Indicators
The indicators included fibrinogen (Fbg), neutrophil-to-lymphocyte ratio (NLR), D-dimer (D-D), albumin (ALB), serum potassium (K), serum sodium (Na), white blood cell count (WBC), hemoglobin (HGB), alanine aminotransferase (ALT), and aspartate aminotransferase (AST), among others.
Chinese Version of the M.D. Anderson Symptom Inventory for Perioperative
Gynecologic Oncology (MDASI-PeriOp-GYN)
This scale was originally developed by the University of Texas MD Anderson Cancer Center in 201833 and subsequently adapted into Chinese by Zheng Yingying et al34 It is applicable to patients with gynecologic malignancies, including cervical, ovarian, and endometrial cancers. The scale consists of 28 items in total, comprising 9 symptom items from the gynecologic oncology-specific module, 13 symptom items from the core cancer-related module, and 6 symptom interference items. Each symptom item is scored from 0 (no symptom) to 10 (worst imaginable severity), with total symptom severity scores ranging from 0 to 220. Higher scores indicate greater perioperative symptom burden.
In this study, 22 symptom items from the gynecologic oncology-specific module and the core cancer-related module were used to assess symptom prevalence and severity. The Chinese version of the scale demonstrated good reliability and validity, with a Cronbach’s α coefficient of 0.798 for the 22 symptom items and content validity indices exceeding 0.71 for each item, supporting its use in clinical research.
Ethical Considerations
This study protocol has been meticulously reviewed and unanimously approved by the Medical Ethics Committee of the Affiliated Cancer Hospital of Xinjiang Medical University (approval number: K-2024218). The review process adhered strictly to the standards set forth in the Helsinki Declaration. Prior to their participation, all study participants provided informed consent.
Statistical Analysis
Step 1: Baseline Data Analysis
Normality test: For continuous variables: present as mean ± standard deviation or median (IQR); between-group comparisons via ANOVA or Kruskal–Wallis H-test; For categorical variables: present as number (percentage); between-group comparisons via Chi-square test or Fisher’s exact test. Descriptive analysis using the tableone package.
Step 2: Symptom Structure Exploration (PCA)
Perform principal component analysis (PCA) solely on baseline symptom items. Apply varimax orthogonal rotation and determine the number of dimensions according to eigenvalues > 1 and scree plot.
Step 3: Symptom Trajectory Clustering (K-Means)
Calculate the average score of items within symptom domains identified by PCA (PCA scores are not used directly); Conduct K-means clustering (class number determined by elbow method and silhouette coefficient based on Euclidean distance). Output trajectory labels.
Step 4: Influencing Factor Analysis (LMM)
Take symptom scores as the dependent variable to establish a linear mixed model (LMM) containing fixed and random effects; Assess differences in symptom change rates among distinct trajectory groups and adjust for confounding factors.
Step 5: Risk Prediction Nomogram
Prediction outcome: whether patients fall into the high symptom burden trajectory during follow-up; Screen predictive factors via multivariate logistic regression; Construct a nomogram; Model performance assessment: ROC curve and AUC, calibration curve, decision curve analysis (DCA), and internal validation with Bootstrap resampling (≥1000 iterations).
Two-tailed test. A P value < 0.05 was considered statistically significant. The methodological flowchart is shown in Figure 1.
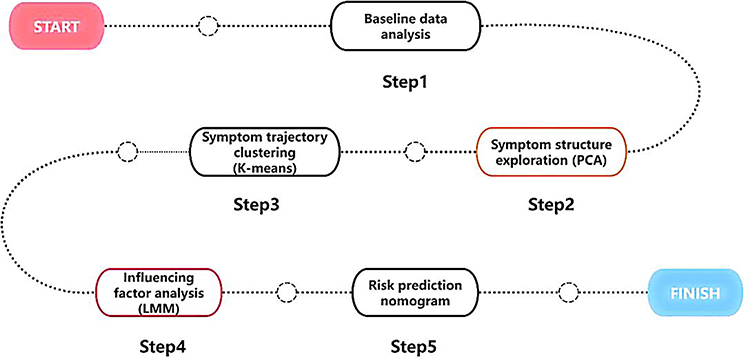 |
Figure 1 Methods flow diagram. |
Results
General Information on the Study Subjects
General Patient Information
A total of 317 patients with cervical cancer were enrolled in this study. Among them, 234 patients (73.82%) were aged >45 years. The majority were married, accounting for 272 cases (85.80%). In terms of educational level, patients with primary school education or below had the highest proportion, with 108 cases (34.07%). Regarding occupation, unemployed/temporary workers constituted the largest group, with 145 cases (45.74%), followed by employees (77 cases, 24.29%) and farmers/herders (45 cases, 14.20%). Regarding tumor differentiation, moderately differentiated tumors accounted for the highest proportion at 44.16%. Additional information is shown in Table 1.
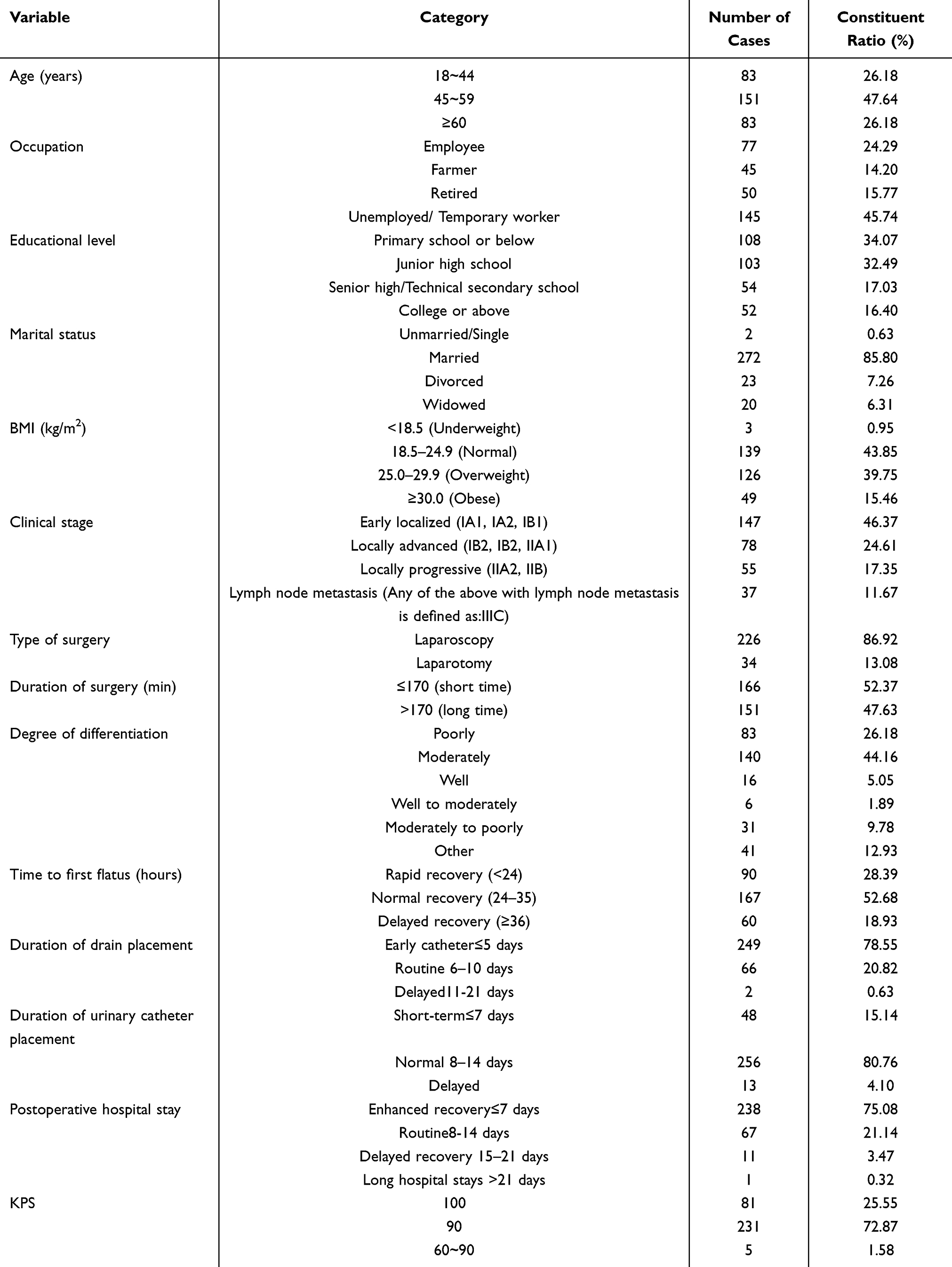 |
Table 1 General Information of the Patients (N=317) |
Laboratory Indicators
The laboratory indicators of 317 cervical cancer patients included in this study are presented for T1, T2, and T3 as follows in Table 2.
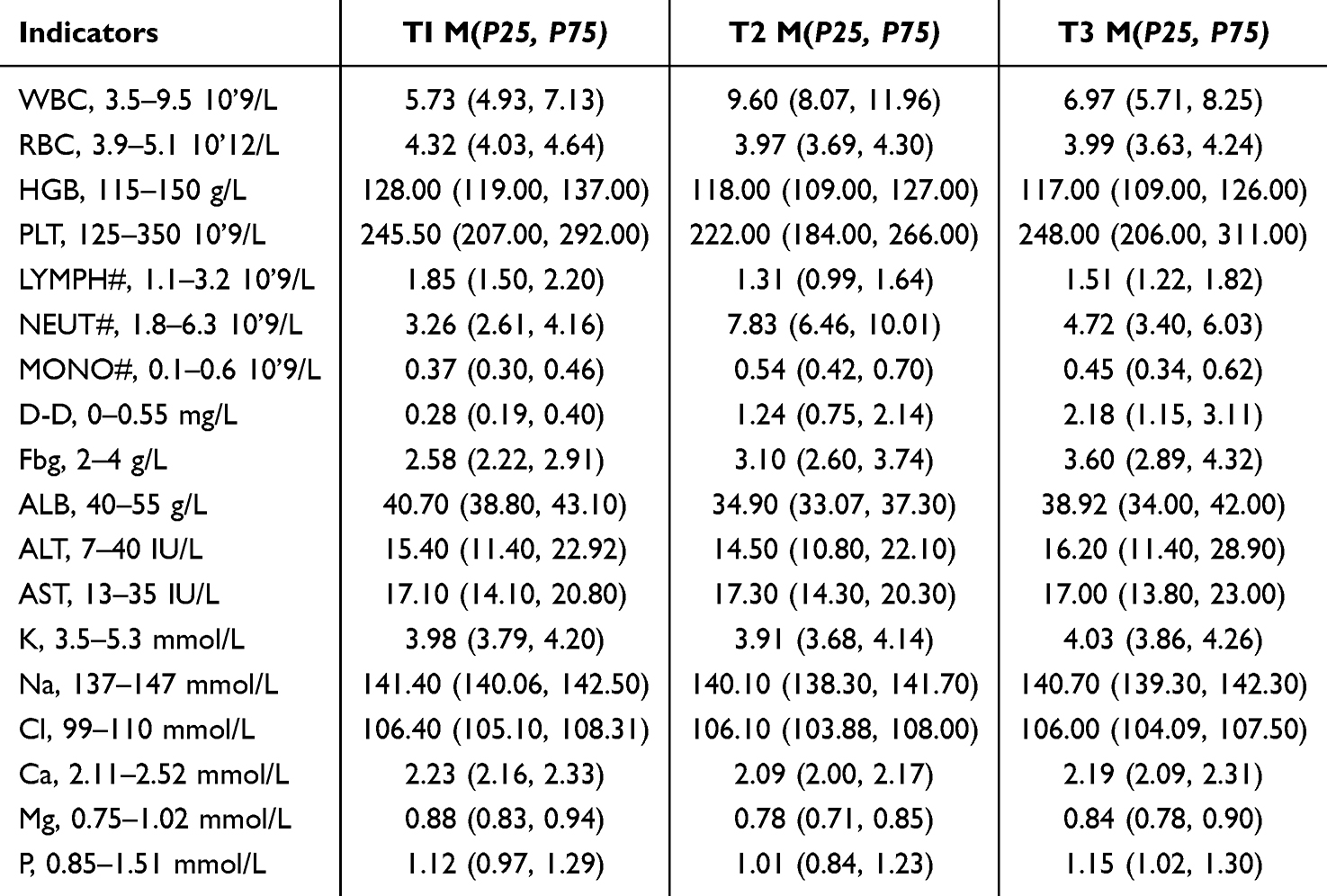 |
Table 2 Perioperative Period Laboratory Parameters of Cervical Cancer Patients |
Symptom Cluster Extraction Outcomes
Incidence and Severity of Symptoms in Cervical Cancer Patients
Incidence and Severity of Symptoms in Cervical Cancer Patients at T1 (Before Surgery)
At T1, 11 symptoms had an incidence rate ≥20%: pain, fatigue, sleep disturbance, distress, forgetfulness, decreased appetite, dry mouth, sadness, limb numbness, abdominal distension, and hot flashes. The three symptoms with the highest incidence rates were sadness (57.7%), distress (49.4%), and forgetfulness (38.2%). Symptom severity was expressed as median [p25, p75]; the symptoms with the highest severity scores were sadness (3 [0, 5]), distress (0 [0, 4]), and sleep disturbance (0 [0, 3]). Among symptoms with an incidence rate <20%, dysuria and urinary urgency were not observed (0%), while the incidence of abdominal colic was only 0.9%. Additional information is shown in Table 3.
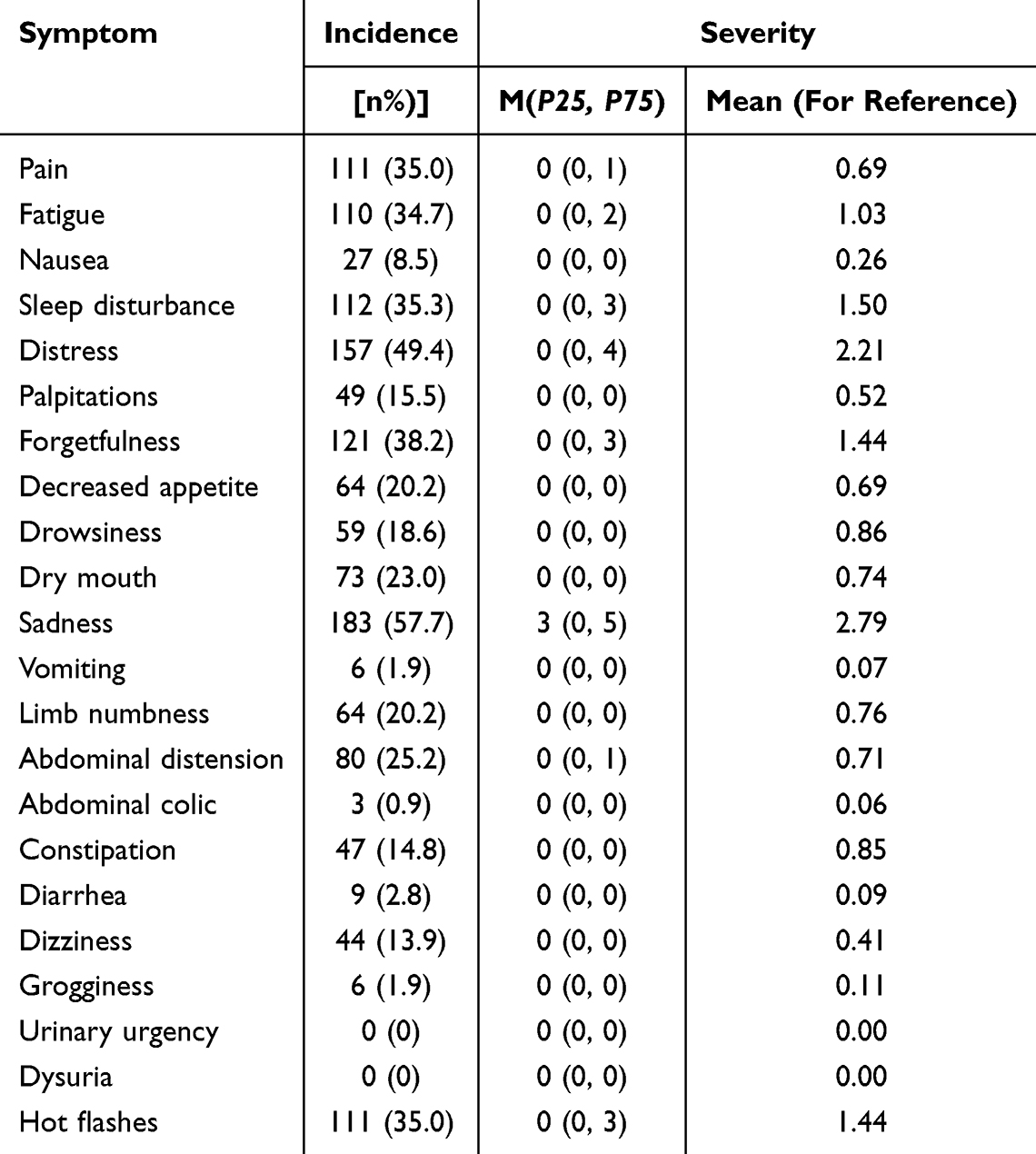 |
Table 3 Incidence and Severity of Symptoms Before Surgery in Cervical Cancer Patients |
Incidence and Severity of Symptoms in Cervical Cancer Patients at T2 (1-2 Days Postoperatively)
At T2, 14 symptoms had an incidence rate ≥20%. The three symptoms with the highest incidence rates were pain (88.0%), fatigue (80.8%), and sleep disturbance (74.8%). The symptoms with the highest severity scores were sleep disturbance (4 [0, 7.5]), pain (3 [2, 5]), and fatigue (3 [2, 4]). Eight symptoms had an incidence rate <20%: palpitations/shortness of breath, forgetfulness, abdominal colic, constipation, diarrhea, grogginess, urinary urgency, and dysuria. Among these, dysuria and urinary urgency were not observed (0%), while diarrhea had the lowest incidence rate (5.0%). Additional information is shown in Table 4.
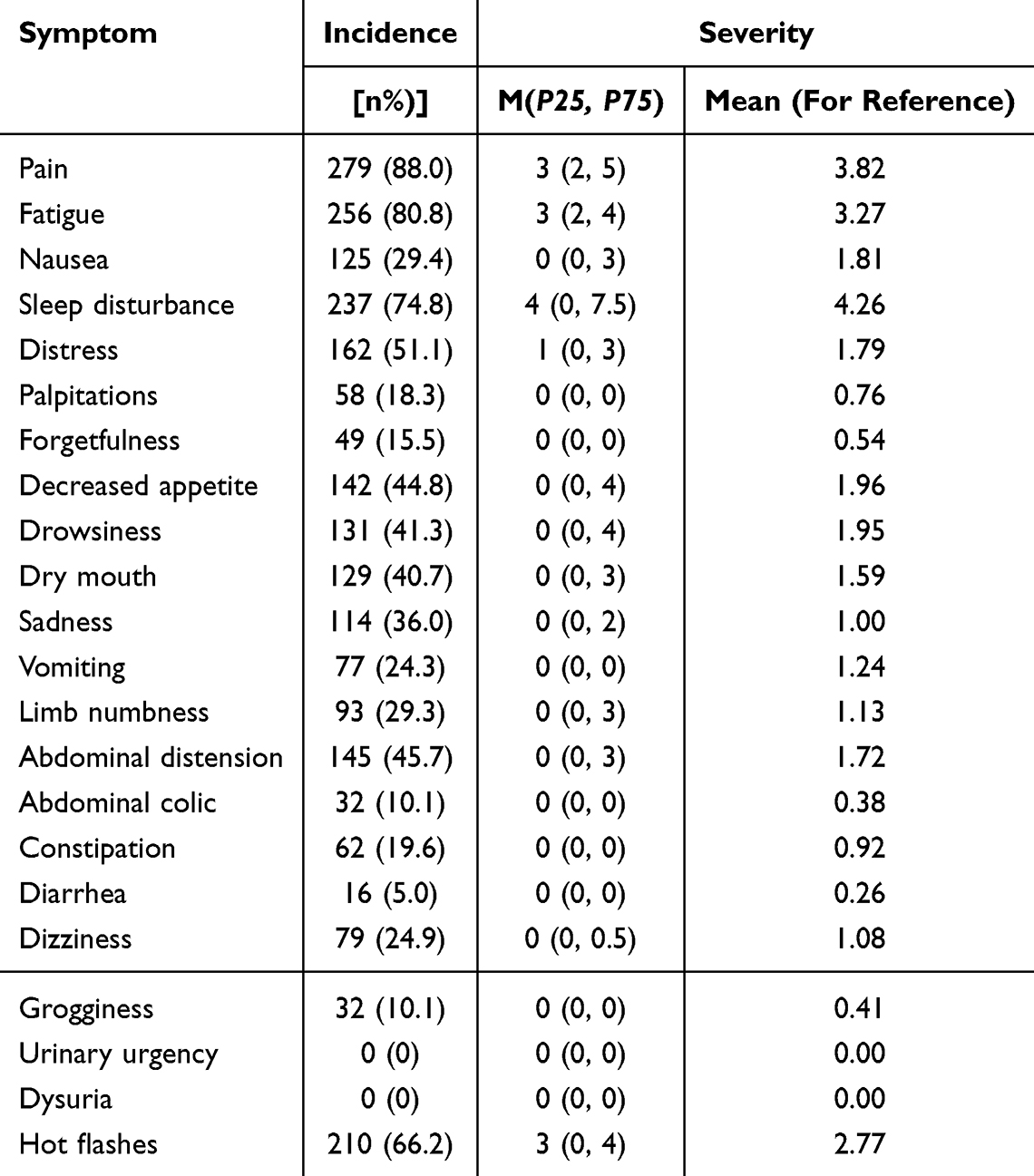 |
Table 4 Incidence and Severity of Symptoms on Postoperative Day 1–2 in Cervical Cancer Patients |
Incidence and Severity of Symptoms in Cervical Cancer Patients at T3 (Before Discharge)
At T3, 10 symptoms had an incidence rate ≥20%: pain, fatigue, sleep disturbance, distress, decreased appetite, sadness, limb numbness, abdominal distension, constipation, and hot flashes. The three symptoms with the highest incidence rates were fatigue (62.5%), hot flashes (56.8%), and sleep disturbance (54.6%). The symptoms with the highest severity scores were fatigue (2 [0, 3]), hot flashes (2 [0, 3.5]), and sleep disturbance (2 [0, 4]). Among symptoms with an incidence rate <20%, grogginess, urinary urgency, and dysuria were not observed (0%). Additional information is shown in Table 5.
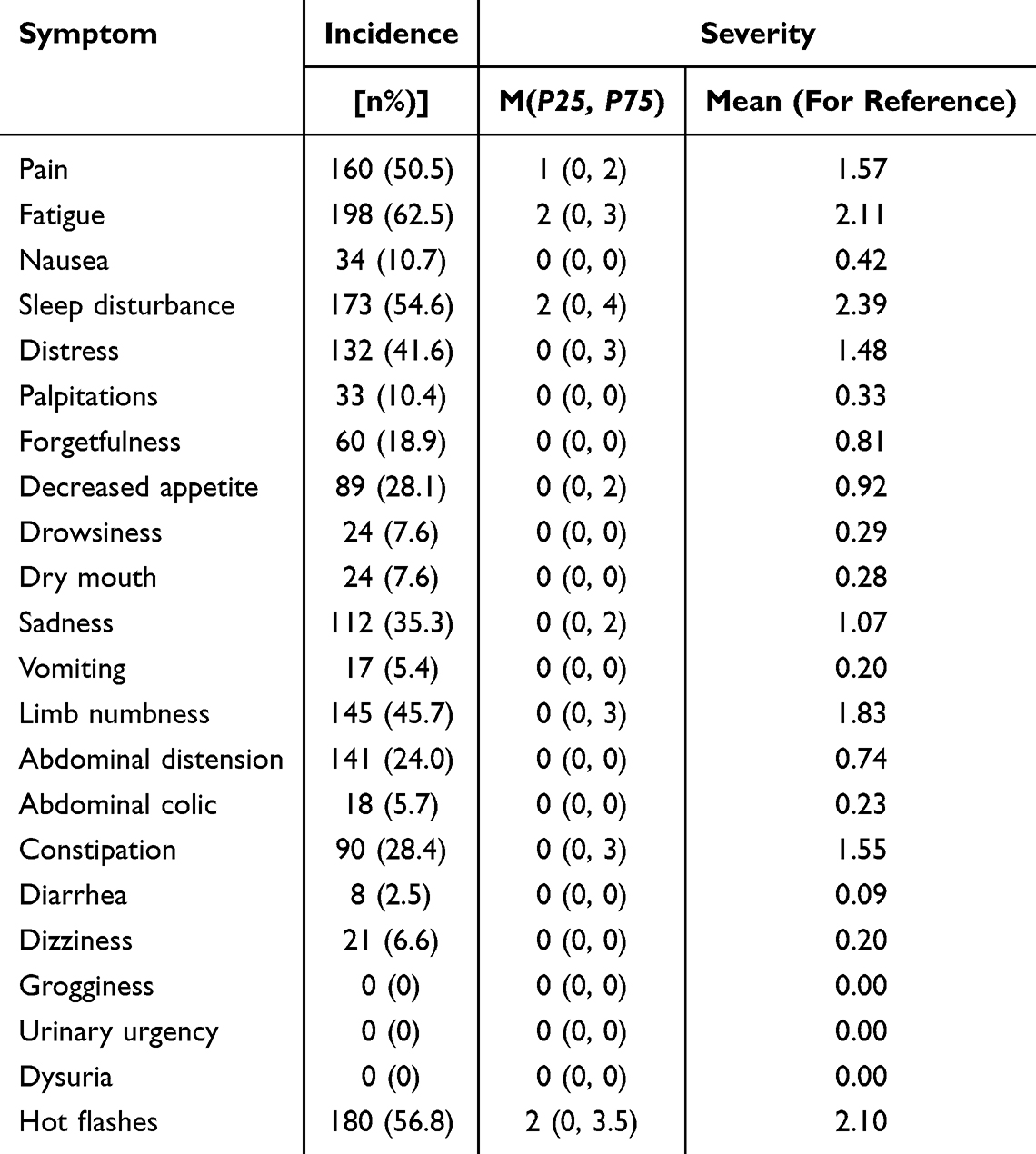 |
Table 5 Incidence and Severity of Symptoms on Before Discharge in Cervical Cancer Patients |
Extraction and Naming of Longitudinal Symptom Clusters in Cervical Cancer Patients During the Perioperative Period
The suitability of the data for analysis was initially examined at each time point. Results showed that the Kaiser–Meyer–Olkin (KMO) values at T1 (0.52) and T3 (0.58) were below the recommended threshold of 0.60, suggesting that separate analyses might yield unstable factor solutions. In contrast, the pooled dataset demonstrated good sampling adequacy (KMO = 0.74; Bartlett’s test of sphericity: χ2= 3701.25, P < 0.001), confirming its appropriateness for factor extraction.
To better identify symptom clusters, exploratory principal component analysis (PCA) with varimax rotation was employed, five common factors with eigenvalues greater than 1 were extracted. Symptoms were grouped according to their factor loadings, typically by assigning items with loadings >0.4 or those with relatively high loadings on the same factor to the same cluster. Given the longitudinal design of this study, pooled PCA was performed by combining data from the three time points (T1, T2, T3). This approach was selected to ensure configural invariance-that is, a consistent factor structure over time-which is a prerequisite for valid longitudinal comparisons of symptom cluster severity. Based on clinical expertise, the five factors were respectively named as: General Somatic Symptoms, Psychological Neurological Symptoms, Gastrointestinal Motility and Energy, Affective-Eating Disturbance, and Consciousness-Sedation Related Symptoms (see Tables 6–8).
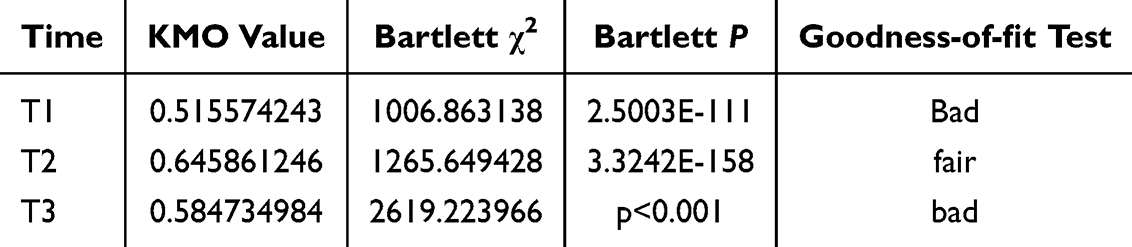 |
Table 6 Goodness-of-Fit Test for Longitudinal Symptom Clusters at Each Time Point in Cervical Cancer Patients During the Perioperative Period |
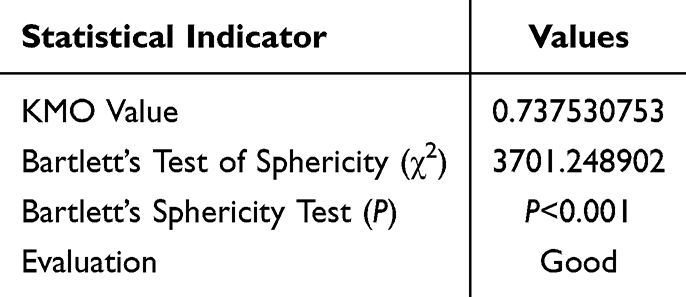 |
Table 7 Goodness-of-Fit Test for Longitudinal Symptom Clusters Dataset in Cervical Cancer Patients During the Perioperative Period |
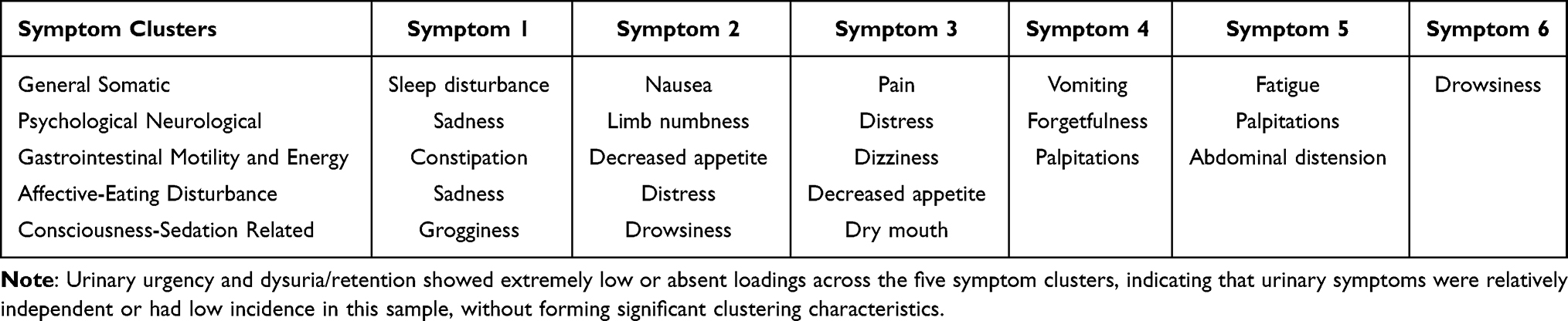 |
Table 8 Composition of Longitudinal Symptom Clusters in Cervical Cancer Patients During the Perioperative Period |
Based on exploratory principal component analysis (PCA), confirmatory factor analysis (CFA) was further performed to verify the stability of the 5-factor symptom cluster structure. The results showed that the 5-factor model fitted the data well, and all goodness-of-fit indices met the recommended statistical criteria. This confirms that the five symptom cluster structures extracted by PCA have favorable construct validity (in Table 9).
 |
Table 9 Confirmatory Factor Analysis of Longitudinal Symptom Clusters During Perioperative Period in Patients with Cervical Cancer |
Identification of Latent Classes for Longitudinal Symptom Cluster Distress Trajectories in Perioperative Cervical Cancer Patients
The elbow method was used to determine the optimal number of clusters. After calculating the within-cluster sum of squares (Inertia) for K=1 to K=9, an obvious inflection point was observed at K=3. Combined with clinical interpretability and previous studies, classifying patients into 3 categories best reflects the distinct evolutionary patterns of symptoms: good recovery, moderate persistence, and severe distress (see Figure 2 and Table 10).
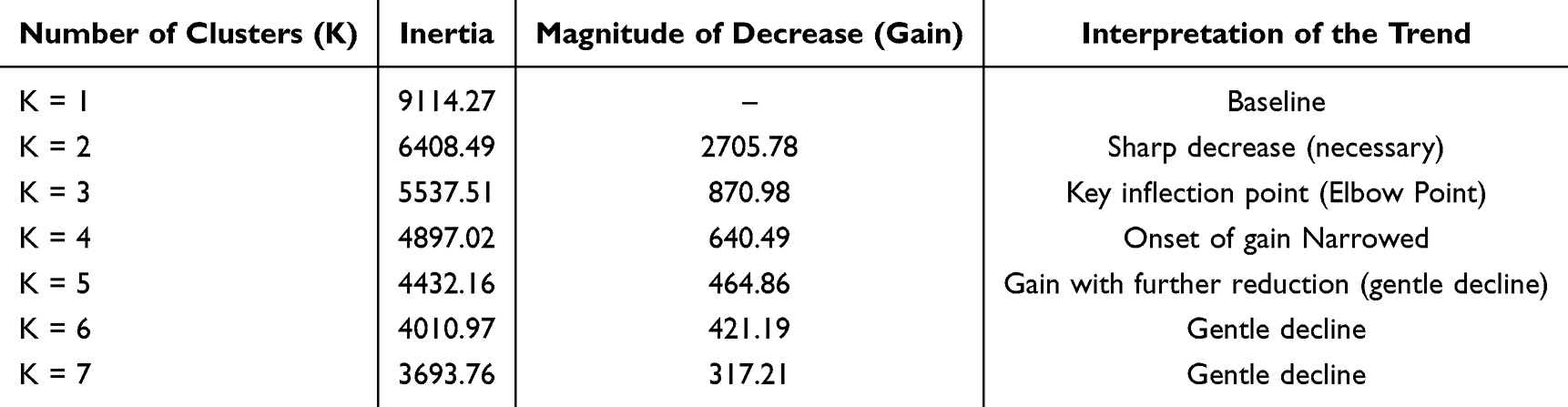 |
Table 10 Symptom Clusters Analysis of Perioperative Symptom Clusters in Cervical Cancer Patients |
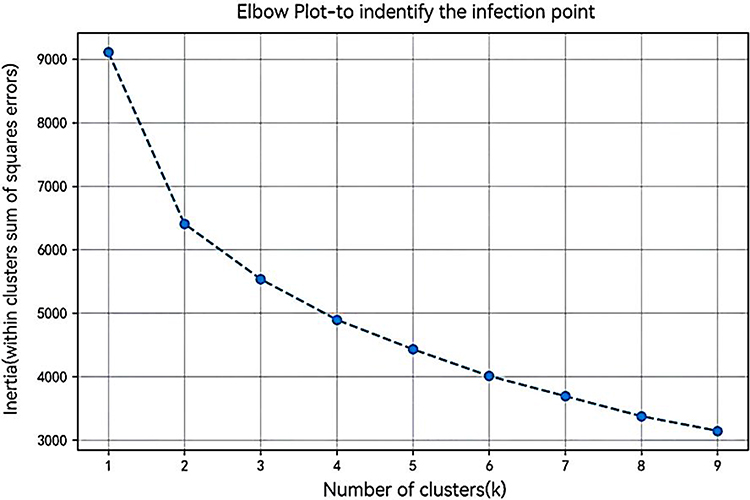 |
Figure 2 Elbow Method Plot. |
Based on longitudinal scores of the five symptom clusters, three distinct trajectories of symptom evolution (Latent Classes) were identified via cluster analysis. According to their temporal dynamic characteristics at T1, T2, and T3, they were respectively labeled as: Class 1 (Good Recovery), Class 2 (Moderate Persistent), and Class 3 (Severe Distress). Symptom Cluster Trajectory Trend in Figure 3.
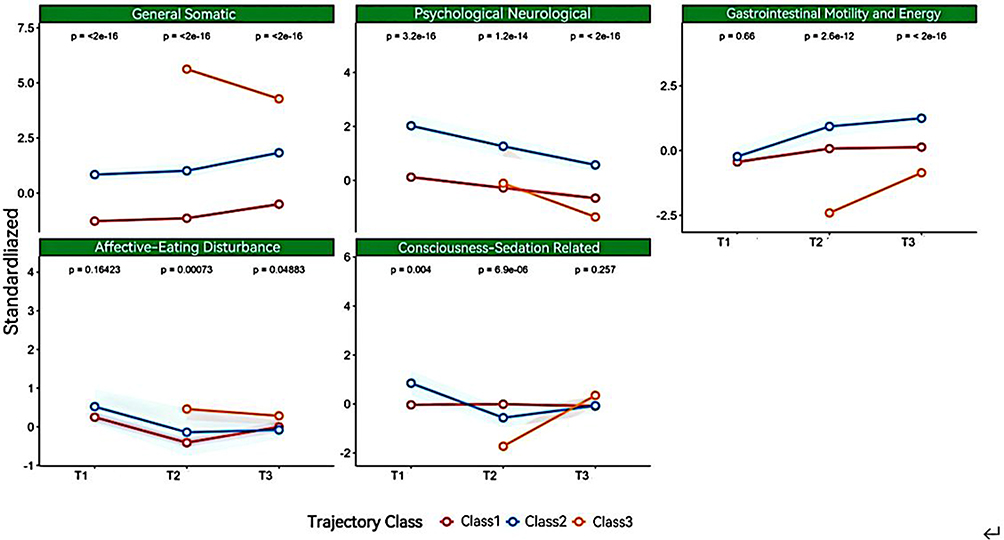 |
Figure 3 Longitudinal Change Trajectories of Perioperative Symptom Clusters in Cervical Cancer Patients. |
Class 1 (Good Recovery): This group accounted for most of the sample (T1: 83.3%, T2: 79.8%, T3: 41.0%). Characterized by low baseline symptom scores at T1 (preoperative), scores for all five symptom clusters remained low or showed a decreasing trend at T2 and T3. Despite undergoing surgical trauma, these patients demonstrated strong physiological and psychological resilience, achieving rapid recovery without significant symptom accumulation.
Class 2 (Moderate Persistent): Patients in this group (T1: 16.7%, T2: 17.7%, T3: 32.8%) exhibited a certain level of symptom burden preoperatively, with particularly higher scores in the Psychological-Neurological Symptoms and General Somatic Symptoms clusters compared to the Good Recovery group. Over time (T2 to T3), their symptom scores fluctuated but remained at a moderate level. This suggests that these patients may have higher sensitivity, leading to persistent postoperative symptoms.
Class 3 (Severe Distress): This group represented the high-risk subgroup identified in this study (T1: 0%, T2: 2.5%, T3: 26.2%). The most notable feature was the absence (or minimal presence) of symptoms at T1, followed by a sharp increase during the early postoperative period at T2, peaking at T3 with scores significantly higher than those of the other two groups. Particularly, the General Somatic Symptoms and Gastrointestinal Motility and Energy clusters showed a markedly increasing trajectory. This indicates that these patients had the poorest tolerance to surgical stress and exhibited significant maladaptation during the recovery phase.
Identification of Latent Classes for Longitudinal Symptom Cluster Distress Trajectories in Perioperative Cervical Cancer Patients
Results of Univariate Predictive Analysis for the Severe Distress Trajectory
To identify early warning indicators for the severe distress class, univariate Logistic regression analysis was performed incorporating patients’ demographic characteristics and clinical laboratory indicators at 1–2 days postoperatively (T2). As a key node in perioperative management linking surgical stress (T1) and discharge outcomes (T3), biological indicators at T2 are valuable for predicting symptom trajectories.
The analysis revealed that among the 15 potential predictors, eight were significantly associated with the occurrence of high symptom burden (P< 0.05). Regarding inflammatory and coagulation parameters, fibrinogen (Fbg) (OR=1.860, 95% CI: 1.171–2.941, P=0.007), neutrophil-to-lymphocyte ratio (NLR) (OR =1.500, P=0.003), and D-dimer (D-D) (OR=1.600, P=0.025) were identified as significant risk factors, indicating that a state of hyperinflammation and hypercoagulability significantly increases the risk of developing an unfavorable symptom trajectory.
Regarding surgical and demographic characteristics, operation duration (OR=1.461, P=0.011) and age (OR=1.053, P=0.009) were statistically significant, suggesting that advanced age and prolonged surgery are risk factors for symptom deterioration. Serum albumin (ALB), serum potassium (K), and serum sodium (Na) exhibited significant protective effects, with serum potassium showing the strongest effect, indicating that maintaining electrolyte homeostasis is crucial for reducing symptom burden. No significant differences were found for BMI, KPS score, postoperative hospital stay, WBC, HGB, and other indicators (P>0.05), as detailed in Table 11.
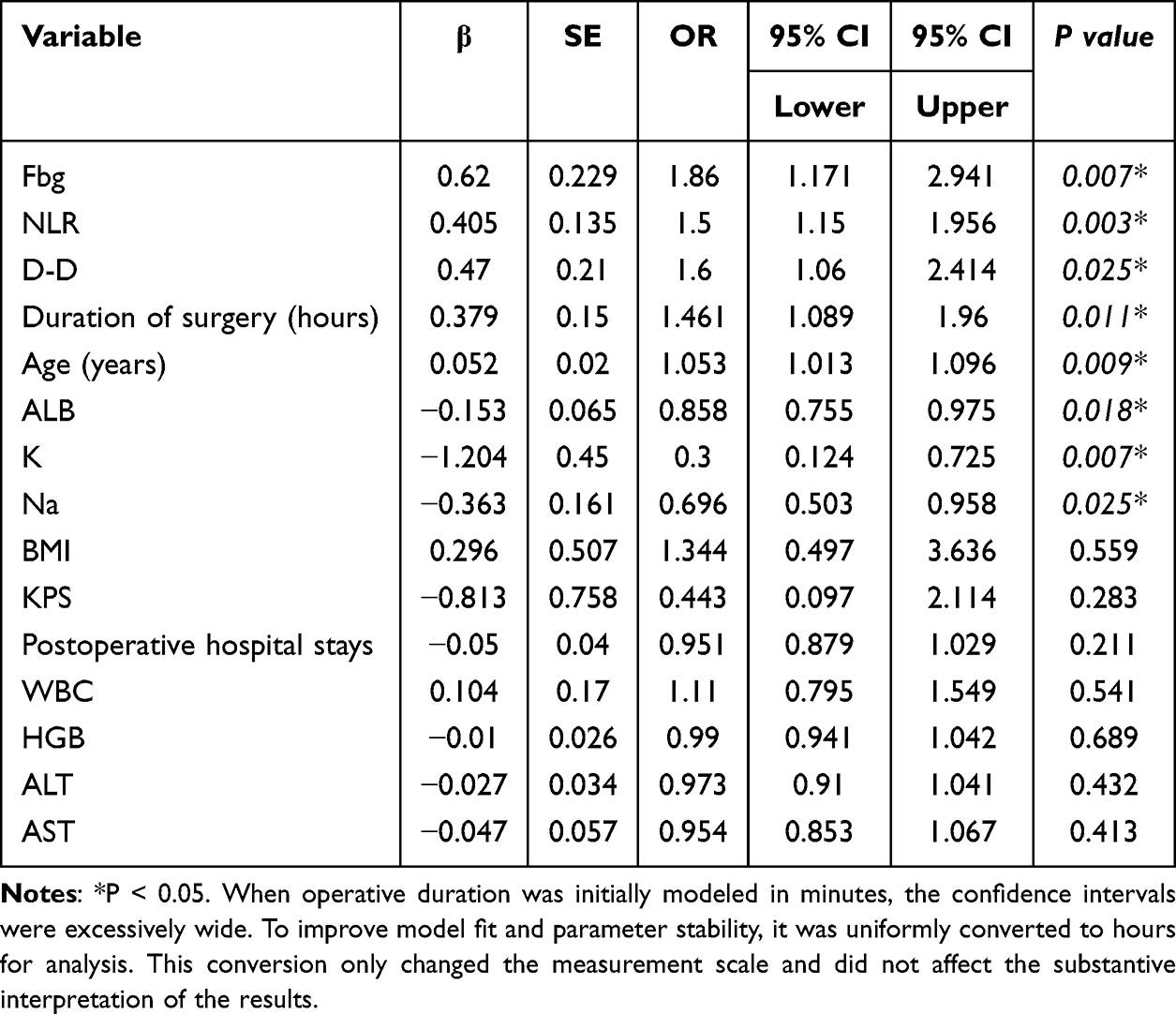 |
Table 11 Results of Univariate Predictive Analysis for the Severe Distress Trajectory |
Results of Multivariate Predictive Analysis for the Severe Distress Trajectory
To further adjust for confounding factors and identify independent predictors for patients being classified into the severe distress group (Class 3), variables with statistical significance in univariate analysis were included in a multivariate Logistic regression model. The model used clinical indicators at T2 as independent variables, and symptom trajectory grouping as the dependent variable (non-severe group=0, severe group=1).
Multivariate analysis results (see Table 12) identified a total of 7 independent predictors. After adjusting for other variables:
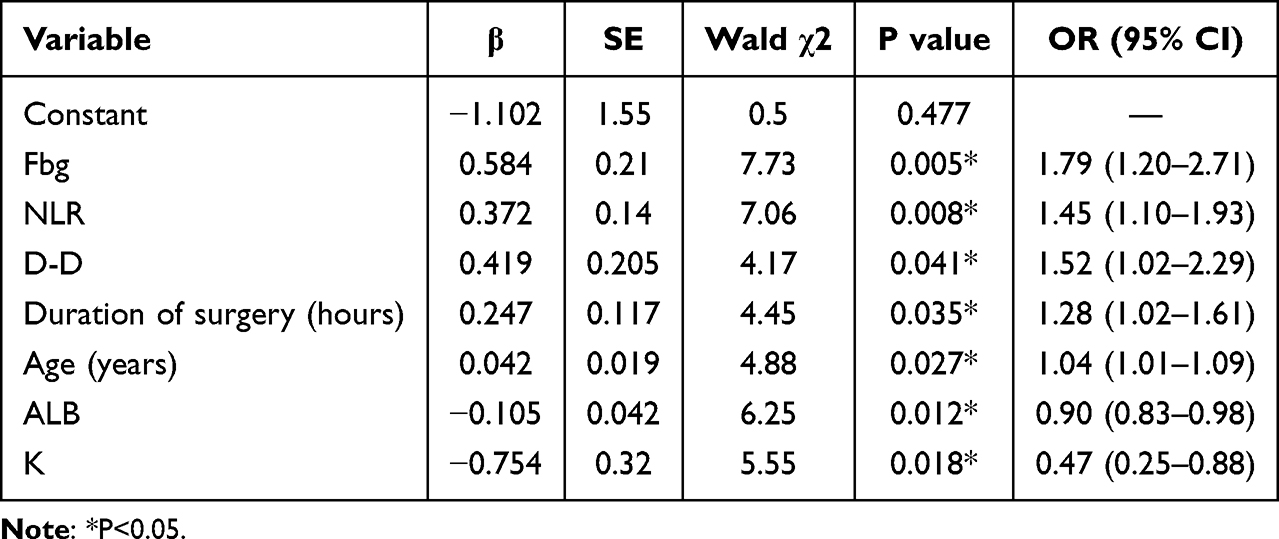 |
Table 12 Results of Multivariate Predictive Analysis for the High Symptom Burden Trajectory |
Inflammatory and Coagulation Indicators
Fibrinogen (Fbg)(OR=1.79, 95% CI: 1.20–2.71, P=0.005), neutrophil-to-lymphocyte ratio (NLR) (OR=1.45, 95% CI: 1.10–1.93, P=0.008), and D-dimer (D-D) (OR=1.52, 95% CI: 1.02−2.29, P=0.041) were independent risk factors for severe symptom distress.
Surgical and Demographic Characteristics
Each 1-hour increase in operation duration was associated with a 28% higher risk of severe symptom distress (OR=1.28, P=0.035); each 1-year increase in age raised the risk by 4% (OR=1.04, P=0.027).
Protective Factors
Serum albumin (ALB) (OR=0.90, P=0.012) and serum potassium (K) (OR=0.47, P=0.018) were significant independent protective factors. Serum potassium showed the strongest protective effect, and maintaining its level can substantially reduce the risk of adverse symptom trajectories.
Predictors of the Severe Symptom Distress Trajectory and Development of the Nomogram
To evaluate the clinical applicability of the previously developed multivariate risk prediction model, we comprehensively assessed its performance using the receiver operating characteristic (ROC) curve and related diagnostic indices. As shown in Table 13 and Figures 4–6 the combined prediction model, constructed based on seven indicators measured at T2 (Fbg, NLR, D-D, operative duration, age, ALB, and K), demonstrated excellent discrimination, with an area under the curve (AUC) of 0.863 (95% CI: 0.820–0.907). At the optimal cut‑off value determined by the Youden index (0.562), the model achieved a sensitivity of 68.4%, a specificity of 87.8%, and an accuracy of 82.0%. The positive predictive value (PPV) and negative predictive value (NPV) were 70.7% and 86.6%, respectively.
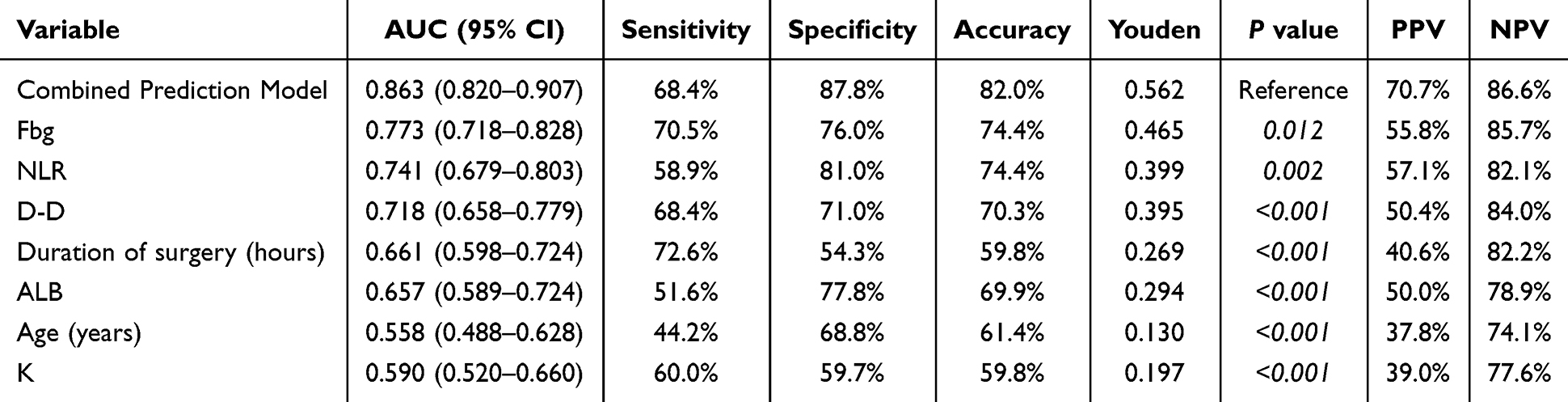 |
Table 13 Predictor Analysis Results |
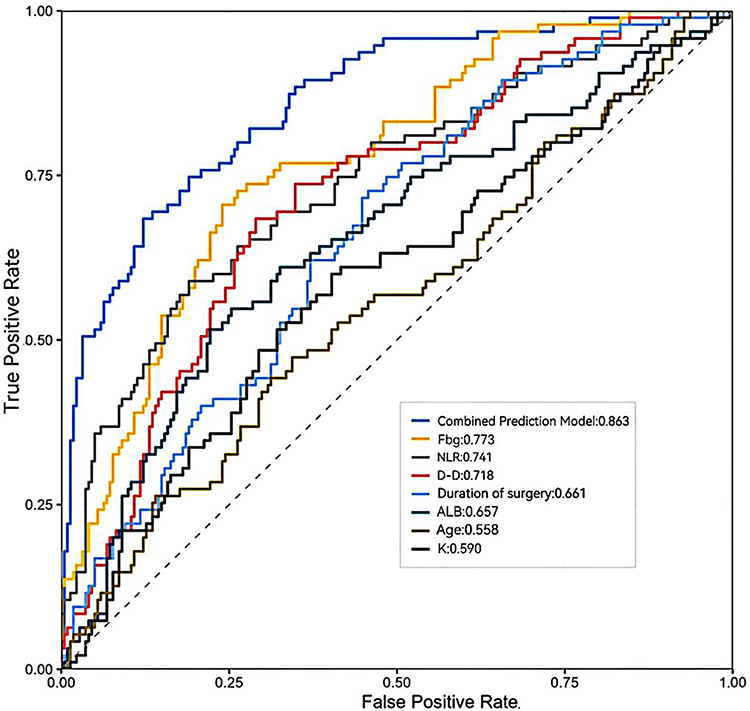 |
Figure 4 Comparison of ROC Curves: The Prediction Model versus Single Indicators. |
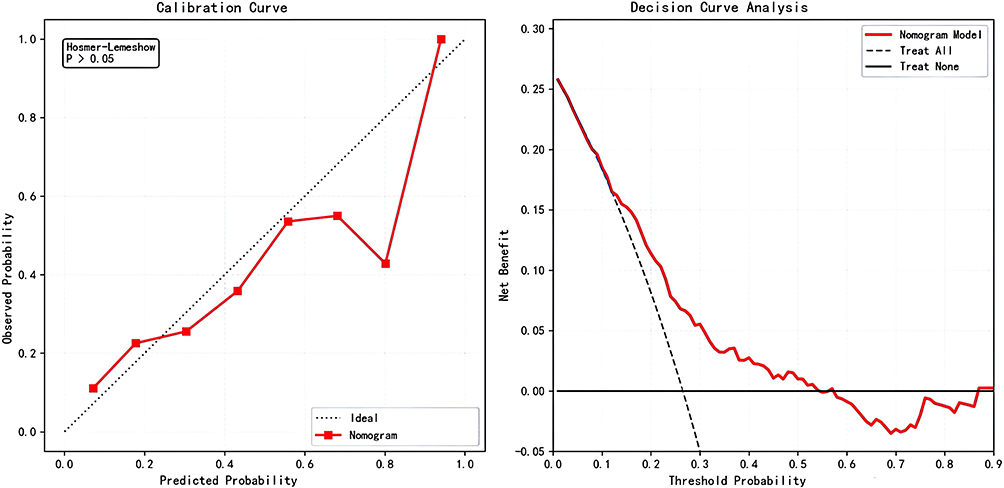 |
Figure 5 Calibration Curve and Decision Curve Analysis (DCA). |
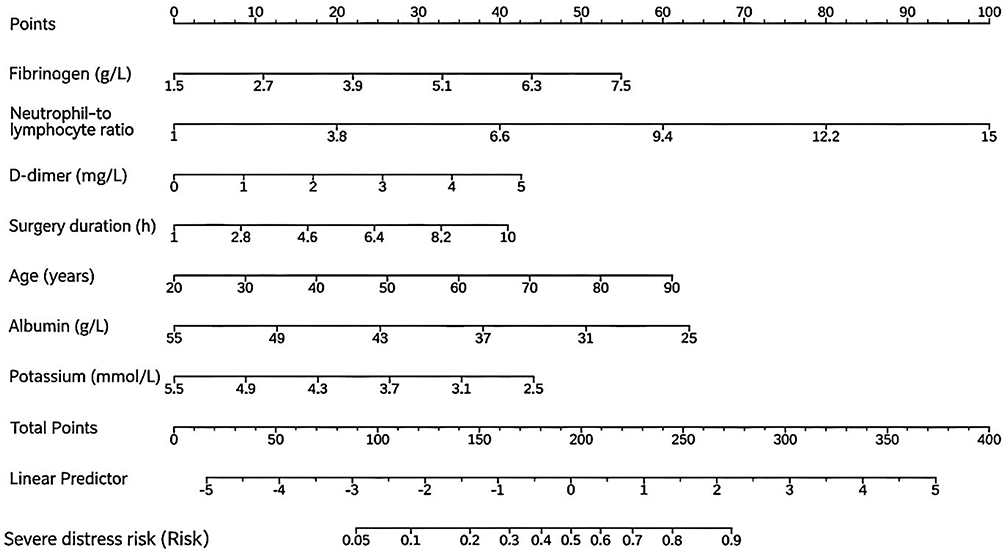 |
Figure 6 Nomogram for Predicting the Risk of Severe Symptom Distress Trajectory. |
Compared with any single predictor, the combined prediction model demonstrated statistically significant superiority (all P<0.05). Among the individual indicators, fibrinogen (Fbg) exhibited the highest predictive performance (AUC=0.773), followed by the neutrophil-to-lymphocyte ratio (NLR) (AUC = 0.741) and D-dimer (D-D) (AUC=0.718), all of which primarily reflect the body’s inflammatory and coagulation status. Notably, although age (AUC=0.558) and serum potassium (K) (AUC=0.590) showed relatively low discriminative ability in univariate analysis, their inclusion as covariates in the multivariate model helped adjust for individual differences in physiological background, thereby enhancing the overall predictive accuracy of the combined model.
Discussion
Composition and Dynamic Trajectories of Symptom Clusters
We identified five symptom clusters using principal component analysis. Sentinel symptoms rarely occur alone but co-exist as clusters. Recognizing these clusters may help reveal shared biological mechanisms and inform future intervention design.
General Somatic Symptoms Cluster
This cluster included pain, fatigue, sleep disturbance, and nausea/vomiting. It aligns with the psycho-neuro-immune symptom cluster described by Dodd et al34 and may relate to inflammatory cytokine release.35 Pain and nausea can disrupt sleep, and sleep loss may lower pain thresholds and worsen fatigue. This cluster is common after gynecologic cancer surgery, and its severity changes over time.36 Combining sleep hygiene with analgesia and antiemetic support could help interrupt this cycle.
Psychological Neurological Symptoms Cluster
This cluster included limb numbness and sadness/forgetfulness. It was more prominent in chemotherapy patients but relatively rare perioperatively, suggesting an interaction between neurosensory and emotional factors. Surgical trauma, anesthesia, and medications may contribute to numbness. These physical symptoms can act as persistent stressors and may trigger sadness or distress.37 When patients report numbness or memory decline, assessing emotional status may be useful, as depression can be overlooked. Psychological symptoms persist throughout the perioperative period and warrant ongoing attention.38
Gastrointestinal Motility and Energy Symptoms Cluster & Affective- Eating Disturbance Symptoms Cluster
Decreased appetite loaded onto two distinct clusters, suggesting two mechanisms of appetite loss. This agrees with Laviano et al39 on multiple mechanisms of cancer-related anorexia. In the gastrointestinal cluster, decreased appetite co-occurred with constipation and dizziness, possibly due to analgesics or reduced motility.40 In the affective-eating cluster, it was linked to sadness and distress, reflecting emotional anorexia.41 For the first, relieving constipation may help; for the second, addressing emotional distress may be more important than nutritional support alone.42
Consciousness-Sedation Related Symptoms Cluster
Grogginess/drowsiness and dry mouth formed a cluster with anticholinergic and sedative effects, largely from opioids, antihistamines, and anxiolytics. This matches prior reports in perioperative oncology.43,44 For patients with high scores on this cluster, reviewing medications and watching for drug accumulation or excessive sedation may help prevent falls.45
Latent Class Analysis of Symptom Cluster Trajectories
Based on longitudinal scores of five symptom clusters, we identified three distinct trajectories: Good Recovery, Moderate Persistent, and Severe Distress. Patients show heterogeneous recovery patterns after cervical cancer surgery,46 challenging the view that postoperative symptoms are resolved naturally over time. The Good Recovery class (largest group) had low or decreasing symptoms after surgery and likely needs only routine care. This profile is similar to the low symptom burden subgroup reported by Jiarui L et al47 The Moderate Persistent class (16.7% at T1, rising to 32.8% at T3) had moderate preoperative burden, especially psycho-neurological symptoms, and no spontaneous relief. Preoperative anxiety or comorbidities may increase symptom sensitivity.48 For these patients, offering psychological support or cognitive behavioral therapy during prehabilitation49,50 might reduce baseline sensitivity, though this requires testing.
The Severe Distress class (0% at T1, 26.2% at T3) is the most clinically relevant. These patients had no preoperative symptoms but peaked at discharge, when coping capacity is low. They tolerate surgical stress poorly and struggle with home recovery.38,51 Because they are easily overlooked before surgery, screening for risk at T2 could help identify them. Routine discharge teaching may not be enough; enhanced remote support during the transition period52 might be considered. Across classes, symptom clusters worsened together, supporting a synergistic effect.34,53 Bundled management strategies—combining analgesia with bowel and nutritional support—could be more effective than single-target approaches,54 though this remains a hypothesis.
Interpretation of Laboratory Markers and the Prediction Model
Biological Rationale for Laboratory Markers
Compared with previous studies that focused primarily on psychosocial factors,55 this study examined the predictive value of laboratory biomarkers. Patients in the Severe Distress subgroup exhibited an inflammatory-nutritional imbalance at discharge, characterized by elevated fibrinogen and low albumin. Elevated fibrinogen indicates high systemic inflammatory stress, while decreased albumin reflects inflammation-related nutritional impairment.56,57 Systemic inflammation is a recognized driver of symptom clusters in cancer patients.58 These associations suggest a biological pathway linking unresolved postoperative inflammation to symptom exacerbation during home rehabilitation.
However, several cautions are warranted. First, these associations do not imply causation; elevated inflammatory markers may be a consequence rather than a driver of symptom distress. Second, the clinical utility of incorporating fibrinogen and albumin into risk stratification59 remains to be prospectively validated.
The Prediction Model: Current Status and Limitations
A nomogram prediction model was developed based on seven pre-discharge predictors (fibrinogen, NLR, D-dimer, operation duration, age, albumin, and serum potassium). The model achieved an internally validated AUC of 0.863, indicating good discriminative ability in this cohort. However, the following limitations must be clearly stated: This model has not undergone external validation, so its predictive performance may be overestimated. Further validation using independent cohorts, ideally from multiple centers, is warranted prior to clinical use. Additionally, its incremental value relative to conventional clinical assessment remains unexamined. Prospective studies are needed to explore whether risk stratification guided by this model can improve patient outcomes.
With these caveats, the model currently serves as a hypothesis-generating tool that may inform the design of future intervention studies. For research purposes, patients with a predicted probability ≥56.2% (optimal cutoff by Youden index) could be considered a high-risk phenotype for targeted enrollment in clinical trials of perioperative symptom management.
Methodological Limitations and Future Directions
Study Design and Sampling
Single-center design: Participants were recruited from a single tertiary cancer hospital using convenience sampling. This limits generalizability to other geographic regions, healthcare systems, and patient populations.
Attrition: The final sample was reduced from 373 to 317. Although baseline characteristics did not differ significantly between completers and dropouts, non-random attrition cannot be fully excluded and may introduce bias.
Analytical Approach
The analytical strategy (PCA followed by cluster analysis) assumes linear trajectory shapes and independent observations. Nonlinear patterns or discontinuous changes may not have been captured.
Future Directions
External validation of the prediction model in multicenter, diverse populations.
Prospective intervention studies testing whether trajectory-based risk stratification or model-guided monitoring improves patient outcomes (eg, symptom burden, quality of life, unplanned readmissions).
Qualitative studies to understand patient and family perspectives on symptom management during the discharge transition period, which could inform the design of acceptable and feasible interventions.
Conclusion
Three distinct symptom distress trajectories—well-recovered, moderately persistent, and severely distressed—were identified in cervical cancer patients during the perioperative period. Subgroups differed in symptom severity and temporal trends. Patients in the severely distressed trajectory showed rapid symptom changes around discharge, suggesting they may be a higher-risk population for symptom management. This trajectory was associated with several indicators related to inflammation, coagulation, nutrition, and surgery. A nomogram prediction model based on seven T3 indicators (Fbg, NLR, D-D, operative duration, age, ALB, and K) showed acceptable predictive performance in this cohort (AUC=0.863), with specificity of 87.8% and accuracy of 82.0% at the optimal cut-off value. These findings suggest the model may help distinguish between high- and low-risk patients, though external validation is needed.
Based on these results, perioperative symptom management could take trajectory heterogeneity into account. Clinicians might use the nomogram as one tool to help stratify patients, and for those identified as higher-risk, considering anti-inflammatory support or nutritional intervention could be explored. Enhanced transitional care around discharge may also be worth considering. For patients in the moderately persistent trajectory, psycho-neurological symptoms may persist and deserve attention. Integrating trajectory patterns with a prediction model could support more stratified management, but whether this approach reduces symptom burden or improves care quality requires prospective testing.
Ethical Approval
This study protocol has been meticulously reviewed and unanimously approved by the Medical Ethics Committee of the Affiliated Cancer Hospital of Xinjiang Medical University (approval number: K-2024218). The review process adhered strictly to the standards set forth in the Helsinki Declaration. Prior to their participation, all study participants provided informed consent.
Disclosure
Yuting Zhang and Chunyan Xu reports Support for the manuscript from Grant No.TSYC202301B161, during the conduct of the study, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. World Health Organization. Cervical cancer. Available from: https://www.who.int/news-room/fact-sheets/detail/cervical-cancer.
2. Siegel RL, Kratzer TB, Giaquinto AN, et al. Cancer statistics, 2025. CA Cancer J Clin. 2025;75(1):10–19. doi:10.3322/caac.21871
3. WHO Guidelines Approved by the Guidelines Review Committee. WHO Guideline for Screening and Treatment of Cervical Precancer Lesions for Cervical Cancer Prevention: Use of Dual-Stain Cytology to Triage Women After a Positive Test for Human Papilloma Virus (HPV).
4. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
5. Zhang M, Zhong Y, Bao H, et al. Breast cancer screening rates among women aged 20 years and above-China, 2015. China CDC Wkly. 2021;3(13):267–273. doi:10.46234/ccdcw2021.078
6. Zhang M, Zhong Y, Zhao Z, et al. Cervical cancer screening rates among Chinese women - China, 2015. China CDC Wkly. 2020;2(26):481–486. doi:10.46234/ccdcw2020.128
7. New government plan to speed up elimination of cervical cancer. Available from: https://english.www.gov.cn/policies/policywatch/202302/08/content_WS63e30acdc6d0a757729e681d.html.
8. Ramirez PT, Robledo KP, Frumovitz M, et al. LACC trial: final analysis on overall survival comparing open versus minimally invasive radical hysterectomy for early-stage cervical cancer. J Clin Oncol. 2024;42(23):2741–2746. doi:10.1200/JCO.23.02335
9. Hui Z, Yunyun L, Xiaoli Y, et al. Interpretation of “2026 NCCN clinical practice guidelines for cervical cancer (1st and 2nd Editions)”. Chin J Pract Gynecol Obstetrics. 2026;42(01):76–82. doi:10.19538/j.fk2026010117
10. Junzhuo C, Wei X, Ruiying W, et al. Medical risk perception and influencing factors of cervical cancer patients. J Nurs. 2023;38(22):24–27.
11. Yingying Z. Study on sinicization and clinical application of perioperative module of anderson symptom scale for gynecological cancer. Chengdu University of Traditional Chinese Medicine; 2020.
12. Pelizzola M, Tanderup K, Chopra S, et al. Co-occurrence of symptoms after radio-chemotherapy in locally advanced cervix cancer patients: a cluster analysis. Acta Oncol. 2023;62(11):1479–1487. doi:10.1080/0284186X.2023.2271252
13. Zhang L, Wang J, Chen T, et al. Symptom clusters and quality of life in cervical cancer patients receiving concurrent chemo-radiotherapy: the mediating role of illness perceptions. Front Psychiatry. 2022;12:807974. doi:10.3389/fpsyt.2021.807974
14. Lin F, Zheng R, Yu C, et al. Predictive role of serum cholesterol and triglycerides in cervical cancer survival. Int J Gynecol Cancer. 2021;31(2):171–176. doi:10.1136/ijgc-2020-001333
15. Ting H, Yuemei C, Qinghua J. Analysis of the mediating effect of illness perception on the relationship between symptom clusters and quality of life in patients with advanced cervical cancer undergoing concurrent chemo-radiotherapy. J Cancer Pharm. 2022;12(04):543–548. doi:10.3969/j.issn.2095-1264.2022.04.19
16. Qinghua J, Yuemei C, Renjing Z. Study on symptom cluster distress and its correlation with quality of life in patients with middle and advanced cervical cancer undergoing concurrent chemo-radiotherapy. Chongqing Med. 2023;52(02):225–229+234. doi:10.3969/j.issn.1671-8348.2023.02.013
17. Hao T, Lirong L, Limei S, et al. Symptom groups and influencing factors of patients with concurrent radiotherapy and chemotherapy for cervical cancer. Chin J Modern Nurs. 2023;29(33):4601–4607. doi:10.3760/cma.j.cn115682-20230329-01227
18. Weishu X, Hongling Z, Yuan Y. Study on correlation between symptoms cluster and quality of life during concurrent radio chemotherapy in patients with cervical cancer. Chongqing Med. 2020;49(03):471–476. doi:10.3969/j.issn.1671-8348.2020.03.029
19. Hongqiu G, Zhirui Z, Zhongheng Z, et al. Clinical prediction models: basic concepts. Application Scenarios, Res Approach.Chin J Evid-Based Cardiovasc. 2018(10):1454–1456+1462. doi:10.3969/j.issn.1674-4055.2018.12.04
20. Ting Z, Zhirong Y, Wang L, et al. Perioperative symptoms of patients with early-stage cervical cancer. General Nurs. 2021;19(01):1–7. doi:10.12104/j.issn.1674-4748.2021.01.001
21. Weiming Z, Yihan X, Jieshou L. Progress in perioperative management——ERAS, perioperative surgical home and perioperative medicine. Chinese J Pract Sur. 2019;39(02):118–121. doi:10.19538/j.cjps.issn1005-2208.2019.02.04
22. Aitijiang G, Rong D. Correlation between serum inflammatory factors and cervical cancer (review). Adv Clin Med. 2023;13(11):18162–18168. doi:10.12677/ACM.2023.13112548
23. Takeda M, Sakuragi N, Okamoto K, et al. Preoperative serum SCC, CA125, and CA19-9 levels and lymph node status in squamous cell carcinoma of the uterine cervix. Acta Obstet Gynecol Scand. 2002;81(5):451–457. doi:10.1034/j.1600-0412.2002.810513.x
24. Onal C, Guler OC, Yildirim BA. Prognostic use of pretreatment hematologic parameters in patients receiving definitive chemoradiotherapy for cervical cancer. Int J Gynecol Cancer. 2016;26(6):1169–1175. doi:10.1097/IGC.0000000000000741
25. Yuan Y, Sun W, Weipeng L. The value of tumor markers in the diagnosis, treatment and prognosis of cervical cancer (Literature Review). J Radioimmunol. 2009;22(3):258–261. doi:10.3969/j.issn.1008-9810.2009.03.041
26. Holdenrieder S, Pagliaro L, Morgenstern D, Dayyani F. Clinically meaningful use of blood tumor markers in oncology. Biomed Res Int. 2016;2016:9795269. doi:10.1155/2016/9795269
27. Sopik V, Narod SA. The relationship between tumour size, nodal status and distant metastases: on the origins of breast cancer. Breast Cancer Res Treat. 2018;170(3):647–656. doi:10.1007/s10549-018-4796-9
28. Jinxin Y, Kai D, Yang Y, et al. Relationship between HPV ctDNA expression level in plasma and tumor tissue and paraaortic lymph node involvement and postoperative recurrence of cervical cancer. J Pract Cancer. 2023;38(12):2046–2050. doi:10.3969/j.issn.1001-5930.2023.12.031
29. Han X, Liu S, Yang G, et al. Prognostic value of systemic hemato-immunological indices in uterine cervical cancer: a systemic review, meta-analysis, and meta-regression of observational studies. Gynecol Oncol. 2021;160(1):351–360. doi:10.1016/j.ygyno.2020.10.011
30. Junfeng C, Xuemin L, Wu X, et al. The value of preoperative plasma fibrinogen combined with neutrophil-to-lymphocyte ratio in evaluating the prognosis of patients with resectable pancreatic cancer. Chinese J General Sur. 2021;36(2):110–113. doi:10.3760/cma.j.cn113855-20200214-00085
31. Zeinali N, Youn N, Albashayreh A, Fan W, Gilbertson White S. Machine learning approaches to predict symptoms in people with cancer: systematic review. JMIR Cancer. 2024;10:e52322. doi:10.2196/52322
32. Collins GS, Reitsma JB, Altman DG, Moons KG. Transparent reporting of a multi-variable prediction model for individual prognosis or diagnosis (TRIPOD): the TRIPOD statement. BMJ. 2015;350(jan07 4):g7594. doi:10.1136/bmj.g7594
33. Wang XS, Shi Q, Williams LA, et al. Validation and application of a module of the MD anderson symptom inventory for measuring perioperative symptom burden in patients with gynecologic cancer (the MDASI-PeriOp-GYN). Gynecol Oncol. 2019;152(3):492–500. doi:10.1016/j.ygyno.2018.11.004
34. Dodd MJ, Miaskowski C, Paul SM. Symptom clusters and their effect on the functional status of patients with cancer. Oncol Nurs Forum. 2001;28(3):465–470. PMID: 11338755.
35. Irwin MR. Inflammation at the intersection of behavior and somatic symptoms. Psychiatr Clin North Am. 2011;34(3):605–620. doi:10.1016/j.psc.2011.05.005
36. Horiba Y, Yoshino T, Yokota M, et al. Climacteric symptoms in postoperative patients among endometrial cancer, cervical cancer, and ovarian cancer: a cross-sectional study. Support Care Cancer. 2022;30(8):6785–6793. doi:10.1007/s00520-022-07117-z
37. Molinares D, Kurtevski S, Zhu Y. Chemotherapy-induced peripheral neuropathy: diagnosis, agents, general clinical presentation, and treatments. Curr Oncol Rep. 2023;25(11):1227–1235. doi:10.1007/s11912-023-01449-7
38. Xiuyun C, Chunyan X, Jing Z, et al. Longitudinal study on the change trajectory of perioperative symptom clusters in middle-aged and elderly patients with gynecological malignancies. Chin J Modern Nurs. 2024;30(17):2323–2329. doi:10.3760/cma.j.cn115682-20231106-01907
39. Laviano A, Meguid MM, Rossi-Fanelli F. Cancer anorexia: clinical implications, pathogenesis, and therapeutic strategies. Lancet Oncol. 2003;4(11):686–694. doi:10.1016/S1470-2045(03)01247-6
40. Cheng Q, Xie J, Duan Y, et al. The psychological distress of gastrointestinal cancer patients and its association with quality of life among different genders. Support Care Cancer. 2024;32(6):329. doi:10.1007/s00520-024-08533-z
41. Xiaohua H, Sanping X, Caili L. Mechanism of reduced food intake in cancer patients. Foreign Med. 2005;25(4):245–247. doi:10.3969/j.issn.1673-534X.2005.04.017
42. Parenteral Nutrition Branch of the Chinese Medical Association. Nutritional support guidelines for cancer patients. Chin J Surg. 2017;55(11):801–829. doi:10.3760/cma.j.issn.0529-5815.2017.11.001
43. Simão D, Barata PC, Alves M, et al. Symptom clusters in patients with advanced cancer: a prospective longitudinal cohort study to examine their stability and prognostic significance. Oncologist. 2024;29(1):e152–e163. doi:10.1093/oncolo/oyad211
44. Guolin W, Jing C, Xiaoming D, et al. Expert consensus on Perioperative Use of non-opioid analgesics in adults [J].Int. J Anesthesiol Resuscitation. 2019;40(1):1–6. doi:10.3760/cma.j.issn.1673-4378.2019.01.001
45. Announcement on the publicity of the Chinese hospital association’s group standards for “hospital quality and safety management” and “specifications for hospital data application and management”. Available from: https://www.cha.org.cn/site/content/245180899596a50aaa81a7f91691fc6a.html.
46. wei J, Yanling J. Wang Ye, et al.Research progress on heterogeneous trajectories of cancer symptom groups. J Nurs Educ. 2025;40(20):2196–2200. doi:10.16821/j.cnki.hsjx.2025.20.011
47. Jiarui L, Xia L, Zhe W, et al. A longitudinal study of early postoperative symptom cluster trajectories in patients with gynecologic malignancies. BMC Womens Health. 2025;26(1):37. doi:10.1186/s12905-025-04221-0
48. Xiaoli L, Pingping W, Tiantian G, et al. Current status of postoperative acute stress disorder in colorectal cancer patients and its correlation with the progression of fear disease and psychological toughness. Health Care Res Pract. 2025;22(10):40–45. doi:10.11986/j.issn.1673-873X.2025.10.07
49. Expert Consensus Preparation Expert Group for Tumor Rehabilitation. Expert consensus on tumor rehabilitation (2025). Chin J Clin. 2025;19(3):165–179. doi:10.3877/cma.j.issn.1674-0785.2025.03.001
50. Fangmei L, Zhang Y. Interpretation of the Chinese expert consensus on integrated rehabilitation of gynecologic malignant tumors. J Oncol. 2025;31(3):181–190. doi:10.11735/j.issn.1671-170X.2025.03
51. Maimaiti M, Juan L, Lei G, et al. Longitudinal study of symptom clusters in perioperative patients with rectal cancer. J Nurs Educ. 2024;39(06):571–576. doi:10.16821/j.cnki.hsjx.2024.06.002
52. Jing Y, Jia Z, Xiuyun C, et al. Current status and influencing factors of discharge preparation of cervical cancer surgery patients. Chin Med Herald. 2024;21(34):88–93. doi:10.20047/j.issn.1673-7210.2024.34.17
53. Jim HS, Jacobsen PB, Phillips KM, et al. Lagged relationships among sleep disturbance, fatigue, and depressed mood during chemotherapy. Health Psychol. 2013;32(7):768–774. doi:10.1037/a0031322
54. Lingling L. Effects of cluster nursing intervention on symptom clusters and negative emotions in lung cancer patients. Int J Nurs. 2020;39(15):2760–2762. doi:10.3760/cma.j.cn221370-20190419-00855
55. Fei Y, Yiqun S, Suhong C. Research progress on symptom cluster management in cancer patients. J Med Philosophy. 2023;44(11):77–80. doi:10.12014/j.issn.1002-0772.2023.11.17
56. Soeters PB, Wolfe RR, Shenkin A. Hypoalbuminemia: pathogenesis and clinical significance. JPEN J Parenter Enteral Nutr. 2019;43(2):181–193. doi:10.1002/jpen.1451
57. Luyendyk JP, Schoenecker JG, Flick MJ. The multifaceted role of fibrinogen in tissue injury and inflammation. Blood. 2019;133(6):511–520. doi:10.1182/blood-2018-07-818211
58. Diakos CI, Charles KA, McMillan DC, Clarke SJ. Cancer-related inflammation and treatment effectiveness. Lancet Oncol. 2014;15(11):e493–503. doi:10.1016/S1470-2045(14)70263-3
59. Lijuan Q, Huile Z, Lece W. Relationship between FAR, AGR, PNI and SII and clinicopathological features of stage I.A~II.A cervical cancer. J Pract Cancer. 2023;38(4):682–685. doi:10.3969/j.issn.1001-5930.2023.04.042
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Identification of Symptom Clusters and Sentinel Symptoms During Radiotherapy in Lung Cancer Patients: A Longitudinal Study
Zhang J, Li S, Wu J, Yang B, Tan X, Zhang G, Zhao X
Cancer Management and Research 2025, 17:2307-2318
Published Date: 7 October 2025
Symptom Clusters and Quality of Life in Cervical Cancer Patients During the Perioperative Period: A Longitudinal Study
Yang J, Zhang Y, Wu Y, Wang Y, Chen L, Xu C
Patient Preference and Adherence 2026, 20:589862
Published Date: 22 June 2026