Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Heart Rate Recovery After Cardiopulmonary Exercise Test Predicts Acute Exacerbations in Patients with Moderate Chronic Obstructive Pulmonary Disease
Authors Nie S, Yang A, Yuan W, Jia N, Li Y, Yu Y, Xu B, Xu Q, Wang H ![]() , He X
, He X
Received 16 December 2024
Accepted for publication 29 April 2025
Published 12 May 2025 Volume 2025:20 Pages 1447—1456
DOI https://doi.org/10.2147/COPD.S509504
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Shan Nie,1,* Ailin Yang,1,2,* Wei Yuan,1 Nan Jia,1 Yunxiao Li,1 Yue Yu,1,3 Bo Xu,1 Qiufen Xu,1 Haoyan Wang,1 Xin He1
1Department of Respiratory Medicine, Capital Medical University Affiliated Beijing Friendship Hospital, Beijing, People’s Republic of China; 2Department of Respiratory and Critical Medicine, Sichuan Provincial People’s Hospital, University of Electronic Science and Technology of China, Chengdu, Sichuan, People’s Republic of China; 3Department of Respiratory and Critical Care Medicine, Second Affiliated Hospital of Third Military Medical University (Army Medical University), Chongqing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Haoyan Wang, Email [email protected] Xin He, Email [email protected]
Background: Automatic dysfunction is present in patients with Chronic Obstructive Pulmonary Disease (COPD). Heart rate recovery at 1 min (HRR1) after Cardiopulmonary Exercise Testing (CPET) serves an indicator of automatic function. Despite its potential significance, this primary method is still not well understood or widely utilized in predicting the progression of COPD. This study aimed to determine whether this indicator predicts acute exacerbations of COPD (AECOPD).
Methods: In this prospective cohort study, 62 patients with COPD were recruited from 2013 to 2017. All participants underwent CPET test and followed up for 5 years thereafter. Univariate and multivariate linear regression, as well as Cox regression, were utilized to identify the abnormal HRR1 and the variables influencing AECOPD.
Results: HRR1 after CPET was a significant correlation of COPD progression. According to the Receiver Operating Characteristic curve, 14 beats/min for HRR1 was optimally used to measure the characteristics of COPD patients. HRR1≤ 14 beats/min significantly predicted the time to the first AECOPD (p=0.00032, Log rank test). In the Cox proportional hazard models, HRR1≤ 14 beats/min was also consistently correlated with AECOPD occurrence (Hazards ratio=8.30, p=0.001).
Conclusion: HRR1 after CPET was an independent predictor of AECOPD. Thus, this index can be applied to observe the conditions and treatment results of COPD patients.
Keywords: COPD, exacerbations, heart rate recovery, cardiopulmonary exercise test, autonomic dysfunction
Graphical Abstract:

Introduction
Chronic Obstructive Pulmonary Disease (COPD) is the third leading cause of death worldwide, which is a heterogeneous, multifaceted disease with intrinsic or exogenous disease determinants.1 Currently, no pharmacotherapy has effectively mitigated the rapid decline in forced expiratory volume in 1 second (FEV1). Smoking cessation has only been shown to have the most impactful intervention in changing the natural course of COPD.2 Frequent exacerbations of COPD adversely impact health outcomes, including hospitalizations, readmissions, and disease progression. These exacerbations are the primary drivers of COPD-related morbidity, mortality, and healthcare costs. Consequently, reducing the incidence of acute exacerbations (AE) of COPD (AECOPD) is a crucial aspect of effective disease management.
Autonomic dysfunction is associated with the early stages of COPD.3 Studies in various populations indicate that abnormal heart rate recovery (HRR) following exercise testing is a critical indicator of vagal reactivation.4–6 That is an indicator of determining cardiac autonomic function.5 In respiratory clinical settings, the 6-Minute Walk Test and Cardiopulmonary Exercise Testing are commonly used to assess cardiopulmonary function and exercise capacity. 6WMT is widely used due to its simplicity and well-tolerated ability to provide information on exercise capacity.7 Nevertheless, the 6MWT has limitations as the results can be influenced by the individual’s motivation and subjectivity. Additionally, it provides limited insight for physicians to evaluate the underlying reasons and processes for a patient’s dyspnea or hypoxia. Additionally, 6MWT lacks the capability to capture detailed physiological parameters throughout the exercise interval, such as oxygen uptake (VO2), carbon dioxide production (VCO2), and oxygen pulse. Cardiopulmonary exercise testing (CPET) is a thorough and objective evaluation of an individual’s respiratory, cardiovascular, muscular, and metabolic reactions to physical stress, which adeptly compensates for these limitations. Therefore, we hypothesized that HRR after CPET might predict the prognosis of COPD.
Materials and Method
This is a prospective study that enrolled COPD patients recruited from the outpatient clinic of the Beijing Friendship Hospital between 2013 and 2017. All participants before the training, all participants were provided with written and oral information about this program, and signed an informed consent form. Our study complies with the Declaration of Helsinki. The Ethics Committee of Beijing Friendship Hospital approved the study protocol (No: 2018-P2-048-01, Date: 2018–03-29).
The main inclusion criteria of the participants were (1) previous diagnosis of COPD according to the GOLD guidelines (FEV1 to forced vital capacity <0.7 and 30–80% of predicted FEV1 after 400-μg albuterol inhalation) and (2) stable clinical stage (at least 6 weeks without infection or AEs). The exclusion criteria were (1) a previous diagnosis of cardiac disease, such as coronary artery disease, valvular disease, arrhythmia, or heart failure and (2) use of pacemakers, implantable defibrillators, or medications that affect HR (such as beta-blockers and non-dihydropyridine calcium ion-channel blockers) (3) people on supplemental oxygen at rest or during exertion.
The sample size for confidence intervals for a single proportion was calculated using PASS 11.0 (NCSS, Kaysville, UT). Patients were followed up for 5 years after the CPET—all patients were contacted by telephone every 3 months. Investigators recorded the patients’ clinical characteristics and frequency of AECOPD (with or without hospital admission). According to the GOLD guidelines, AECOPD was defined as an acute deterioration of respiratory symptoms that results in additional therapy or leads to a change in medication.2 All CPETs were conducted on a bicycle ergometer with a ramp-protocol cycle test (Via Sprint; CareFusion, Hoechberg, Germany). As described in our previous study8, after a 3-min rest, patients engaged in unloaded pedaling for 3-min intervals with an increasing exercise intensity at a rate of 5–20 W/min (according to the predict peak work). Participants were allowed to set their pedaling pace, provided it remained above 60 rpm. All participants were encouraged to cycle until they reached their maximum physical activity with subjective exhaustion such as leg fatigue, intolerable breathlessness, and myocardial ischemia (usually presenting as chest pain, heart block, loss of balance, dizziness, and even faintness), which prevented further movement. The termination criteria also included the following:9 (1) oxygen saturation via pulse oximetry (SpO2) ≤88%, (2) ventricular tachycardia, (3) ≥2 mm of horizontal or down-sloping ST-segment depression, (4) blood pressure (BP) ≥240/130 mmHg, and (5) a drop in systolic blood pressure ≥20 mmHg from the highest value during exercise. Prior to conducting the CPET, all participants underwent a pulmonary function test using the Master Screen system (Master Screen Body, CareFusion). The test was conducted by a trained exercise technician under physician supervision. Gas exchange and ventilatory response were measured continuously using a breath-by-breath automated computer system. The highest 30-s average value of oxygen uptake (VO2), carbon dioxide production (VCO2), ventilation (VE), and SpO2 were defined as their peak values during the test. HR was measured using an electrocardiogram. BP was measured at two-minute intervals, using a sphygmomanometer. The anaerobic threshold (AT) was determined using the V-slope method. The cardiac function and exercise capability during exercise were estimated by the slopes of HR/VO2, VO2/watts, and VE/VCO2.10 The VE/VCO2 slope (VE plotted versus VCO2 slope) was calculated by linear regression from rest to AT during exercise. HRR1 was calculated as follows:

Avoiding the influence of HRR caused by postural changes,11 the participants remained seated on the cycle for 3 min throughout the recovery phase.
Statistical Analyses
The statistical studies were performed using the R computer language (version 4.2.2). The independent sample t-test and Pearson’s chi-square test were used to analyze the initial characteristics of HRR1 in COPD patients. Mean and standard deviation represent continuous variables, whereas median and interquartile range are used to present categorical data. Univariate and multivariate linear regression models were utilized to identify the abnormal HRR and the variables influencing AECOPD. The receiver operating characteristic (ROC) curve analysis and optimal critical value of HRR1 for AECOPD prediction were performed. Subsequently, examine the relationships between HRR1 and acute exacerbation rate of COPD using a Cox regression model with a stepwise selection from variables. P values in all statistical tests were considered significant at p<0.05.
Results
Two patients were lost during the follow-up period due to lost connection; 60 patients were evaluated in this study, and 21 of them had AECOPD. The demographic and baseline characteristics, pulmonary functions, and CPET characteristics of the patients in COPD with different HRR1 are summarized in Table 1. The characteristics of patients were analyzed by HRR1 stage (HRR1>14 beats/min and HRR1≤14 beats/min). No significant difference was observed between the groups regarding the GOLD stage and Pulmonary Function Test. Otherwise, VO2/HR may potentially influence COPD evaluation in CPET.
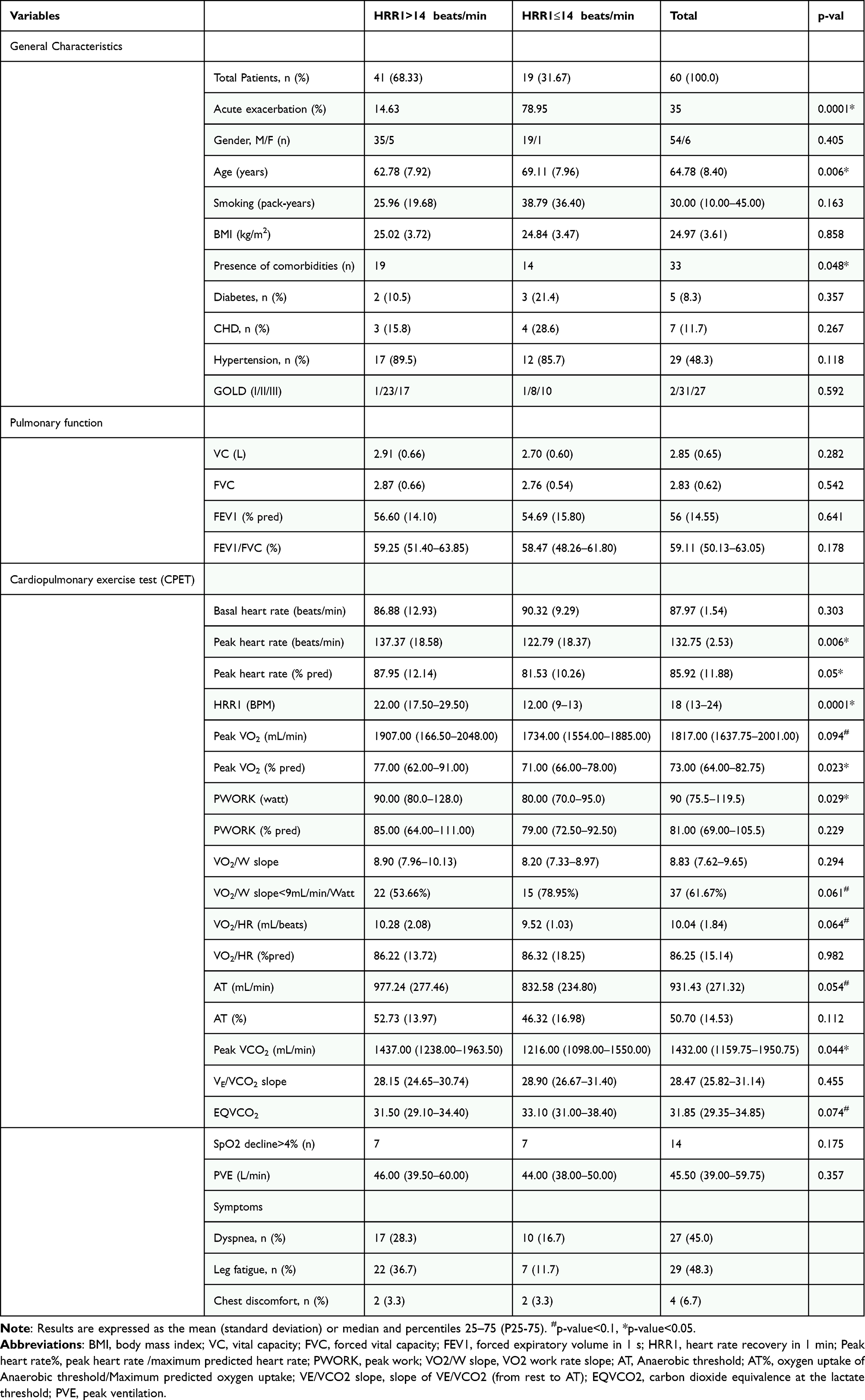 |
Table 1 Demographic and Baseline Characteristics, Pulmonary Functions, and CPET Characteristics of Patients with COPD |
To identify the variables associated with HRR1 after the CPET, univariate and multivariate linear regression were used to analyze in Table 2. HRR1 aft er the CPET test was significantly negatively correlated with AE frequency (p<0.0001), and HRR1 was correlated with FEV1 (p<0.025). In Table 3, both univariate and multivariate regression analyses showed that HRR1 was the only independent predictor of the first exacerbation of COPD at the 5-year follow-up (p<0.0001).
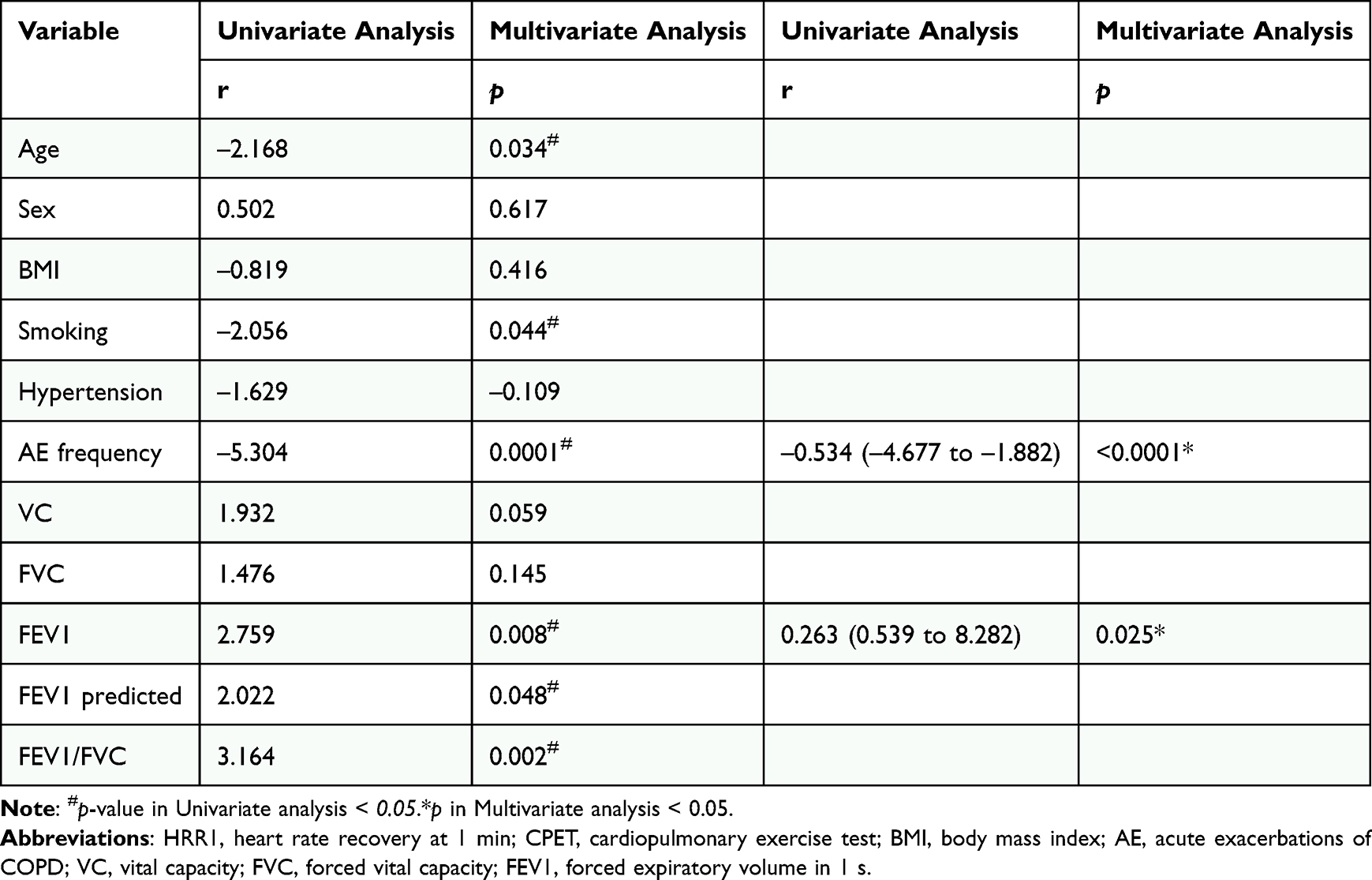 |
Table 2 Univariate and Multivariate Linear Regression Analyses Used to Identify the Variables Associated with the HRR1 After the CPET |
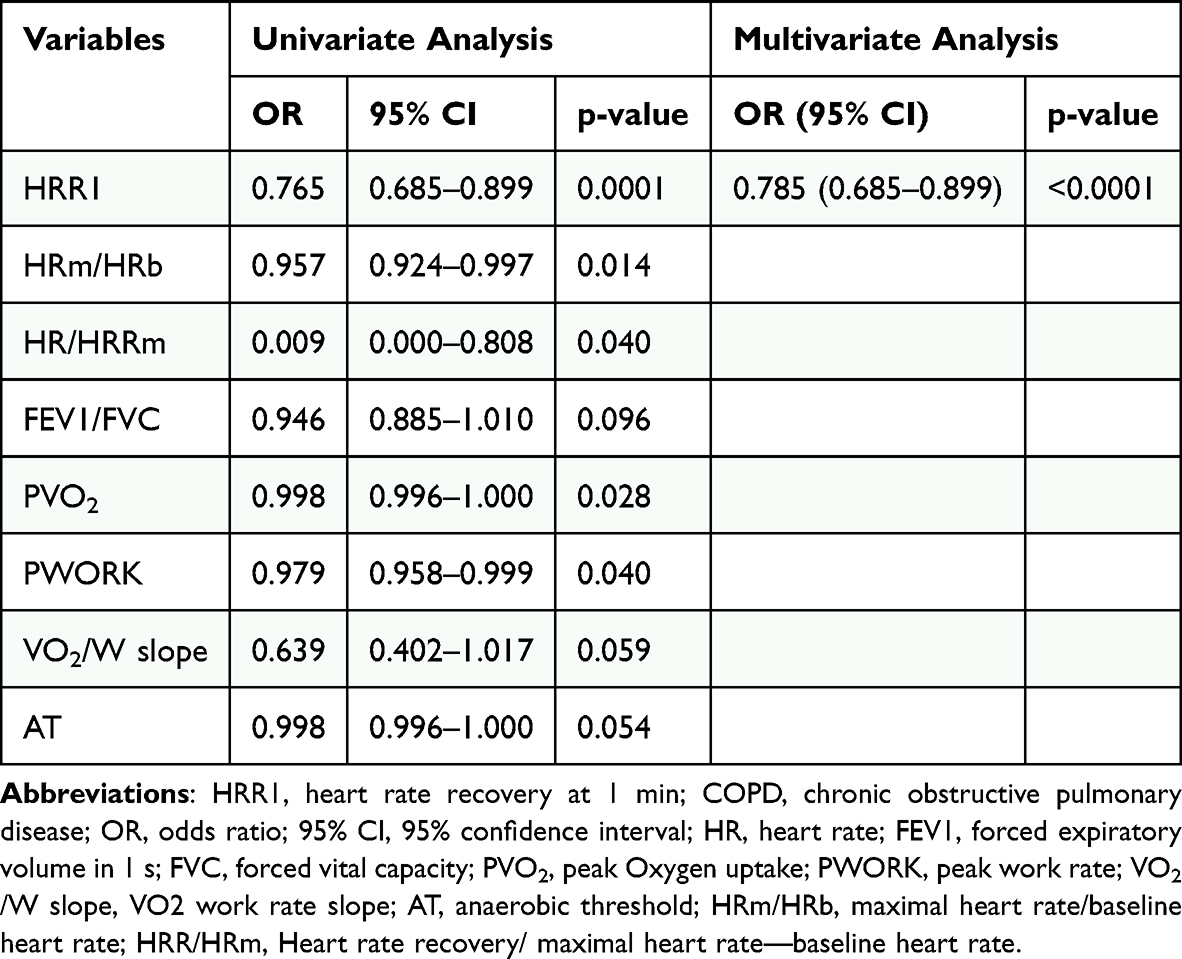 |
Table 3 Univariate and Multivariate Binary Logistic Regression Analyses Evaluating the Effect of HRR1 and Significant Confounders on COPD During 5-year Follow-up |
ROC curves determined that HRR1 was a predictor of AE of COPD (Figure 1), and the cutoff point was 14 beats/min (95% CI, 0.740–0.932). HRR1≤14 beats/min showed a significant possibility of obtaining the first AE time (p=0.00032); the result could be observed significantly in 20 months (Figure 1).
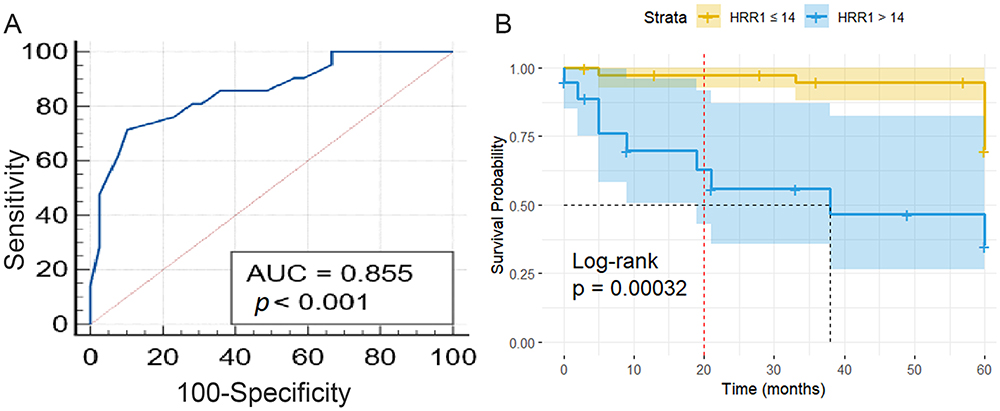 |
Figure 1 HRR1 for AECOPD prediction. (A) ROC curves of HRR1 in predict COPD, with AUC=0.855 (p<0.01). (B) Kaplan–Meier curve of the first AE time according to HRR1 values. Median AE time is 38 month (p=0.00032, Log rank test). Abbreviations: HRR1, heart rate recovery in 1 min; AE, acute exacerbations of COPD. |
In fully adjusted models, the hazard ratio for the occurrence of re-AECOPD in patients with HRR1≤14 beats/min was 8.35 (95% CI, 2.30–30.04, p=0.001); thus, such patients easily experienced AE compared with HRR1 >14beats/min. Age (hazards ratio=0.91; 95% CI, 0.84–1.00, p=0.041) and FEV1/FVC (hazards ratio=0.887; 95% CI, 0.8026–0.9797, p=0.018) also influenced with the occurrence time (Figure 2).
 |
Figure 2 Forest plot of COX regression in AECOPD with HRR1≤14 beats/min. SPO2 decrease level: Based on the baseline, ≤4%=1, >4%=2; HRR1≤14 beats/min (HR=8.3, 95% CI=2.30, 30.04, p=0.001); FEV1/FVC (HR=0.887, 95% CI=0.8026, 0.9797, p=0.018), AGE (HR=0.91, 95% CI=0.84–1.00, p=0.041) (*p<0.05, **p<0.01). Abbreviations: FVC, forced vital capacity; FEV1, forced expiratory volume in 1 s; HRR1, heart rate recovery in 1 min; PVO2, peak oxygen uptake; PWORK, peak work; AT, Anaerobic threshold; VE, ventilation; VCO2, carbon dioxide production; VE/VCO2 slope, slope of VE/VCO2 (from rest to AT). |
Discussion
Our study demonstrated that HRR1≤14 beats/min was significantly associated with the exacerbations in COPD patients who underwent CPET. These strong associations between HRR and prognosis persisted even after controlling for other confounding variables. To the best of our knowledge, this is the first study with a 5-year follow-up observation of HRR following CPET to predict primary outcomes in COPD patients.
In clinical settings, most patients experience breathlessness and AE due to multiple underlying causes. CPET can potentially help detect co-existing diseases in the early stage.9 The dynamic interplay between the sympathetic and parasympathetic regulation controls the HR response. Parasympathetic effects remain active during high-intensity exercise and become particularly pronounced in the initial stages of recovery,12 especially HRR1. This physiological response correlates with plasma norepinephrine concentrations reaching maximal levels approximately 1-minute post-exercise.13
FEV1 is commonly used in pulmonary function testing to evaluate the degree of expiratory flow limitation in COPD patients. Our findings revealed a positive association between FEV1 and HRR1, suggesting that the chronic airflow limitation may contribute to autonomic dysfunction, which is inconsistent with a previous study.14 Hypoxemia and hypercapnia resulting from restricted airflow may induce increased cardiac vagal activity and reduced sympathetic activity in COPD patients.15 Sustained autonomic tension leads to muscle tightness and airway constriction,16 which in turn influence the frequency of AECOPD17,18 and mortality.19,20 As two essential values in the diagnosis and mortality of COPD, AE frequency and FEV1 are independently associated with HRR1 after CPET, suggesting that the value and significance of HRR1 should be considered for COPD diagnosis and prognosis.
HRR1 is a well-established indirect indicator of cardiac autonomic function21 and an essential predictor of overall mortality in some populations.22–24 Several studies have utilized HRR1 to assess heart failure, acute myocardial infarction,25–27 and multiple lung diseases, such as lung cancer survivors;28 COPD29 and Asthma.30,31 The HRR1 can be easily obtained in the recovery periods of CPET. Zhangyi et al32 proposed an HRR1 cutoff value of 19 bpm following CPET as a significant predictor for the prognosis of chronic pulmonary hypertension.32 Prior research has also found a predictive effect of HRR1 on COPD prognosis. For instance, Lacasse et al4 revealed that COPD patients had a lower HRR1 than healthy individuals, and a lower HRR1 (HRR1<14 bpm after CPET) was associated with an increased mortality rate. According to the GOLD2025 guideline, COPD management aims to reduce symptoms, lower exacerbation risk, and improve survival outcomes. Therefore, during the therapy of COPD, for physicians, focus has gradually shifted to the manifestations of disease progression. Our five-year follow-up study corroborates the findings by Diego et al, which identified HRR1 (HRR ≤ 14 bpm) was an independent predictor of AECOPD in 2017.33 Nevertheless, the optimal prognostic threshold for HRR1 varied across studies. Cole et al5 identified that an HRR1≤12bpm following CPET (treadmill protocol) independently predicted all-cause mortality in COPD. Conversely, Minai et al34 identified a lower threshold (HRR1≤10 bpm post-6MWT) that significantly correlated with incident AECOPD. The discrepancies may be attributed to the difference in sample size, exercising testing modalities, baseline of COPD, or study endpoints.
Moreover, our study is based on the heart rate recovery following CPET, which is more applicable in assessing cardiac, pulmonary, and overall motivational functions and perceptions of dyspnea during exercise.9 Therefore, HRR1 after CPET may provide a more comprehensive and objective assessment of the disease.
Additionally, we analyzed the differences in clinical features among patients with different degrees of HRR1. Patients in the reduced HRR1 group exhibited significantly lower Pwork and PVCO2 (p<0.05). Furthermore, the peak HR during CPET and its percentage relative to the predicted maximum HR showed statistically significant differences between two groups (p≤0.05). Considering the clinical work and these effects, we conclude that Peak HR is affected by multiple factors, therefore when a patient cannot reach a level of expected peak value in CPET, the decline in HRR1 might not be representative. But the specific evaluation level remains to be studied. Therefore, we recommend considering the percentage of predicted Peak HR (Peak HR% predicted) before using HRR1 as the predictor of AECOPD. In addition, our study confirmed previous conclusion35 that FEV1/FVC can identify individuals at risk of clinically significant COPD. The rapid reduction in HR after cessation of exercise might be related to enhanced cardiac vagal nerve activation.36 Some experts have observed the effect of Beta-Blockers on the prevention of Acute Exacerbations of COPD.37 However, the relationship between increased vagus nerve activation and risk of chronic obstructive pulmonary disease is still unclear. Further investigation is needed to fully unravel the mechanism behind it. Our study has some limitations. Mainly, only patients with COPD stages II–III were selected, and due to safety concerns, patients with mild and severe COPD were not assessed in follow-up; thus, the sample size in this study was limited, and future studies should investigate this association in a larger cohort of patients.
Conclusions
Our study identifies delayed heart rate recovery at 1-minute post-CPET (HRR1 ≤14 bpm) as an independent predictor of AECOPD (adjusted HR 8.35,95% CI 2.30–30.04, p=0.001). These findings support the integration of HRR1 into existing risk stratification tools to identify high-risk COPD patients warranting intensified monitoring. Furthermore, targeting HRR improvement pulmonary rehabilitation programs or pharmacotherapy may help mitigate exacerbation susceptibility.
Abbreviations
6MWT, 6-min walk test; AE, Acute exacerbation; AECOPD, Acute exacerbations of Chronic Obstructive Pulmonary Disease; AT, Anaerobic threshold; VCO2, Carbon dioxide production; CPET, Cardiopulmonary Exercise Test; COPD, Chronic Obstructive Pulmonary Disease; CI, Confidence interval; FEV1, Forced expiratory volume in 1 s; HR, Heart rate; HRR, Heart rate recovery; SpO2, Oxygen saturation via pulse oximetry; VO2, Oxygen uptake; ROC, Receiver operating characteristic; VE, Ventilation.
Data Sharing Statement
All data generated or analyzed during this study are included in this article. Further enquiries can be directed to the corresponding author – Haoyan Wang.
Ethics Approval and Informed Consent
The Ethics Committee of Beijing Friendship Hospital approved the study protocol (No: 2018-P2-048-01, Date: 2018-03-29).
All participants were provided with written and oral information about this program and signed an informed consent form.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by the National Nature Science Foundation of China (nos. 81870029 and 81700038), Key Clinical Specialty Construction Program of Beijing (2020–2022), Capital’s Funds for Health Improvement and Research (grant no. 2018-2-2-24 and 2024-2-1101).
Disclosure
The authors have no conflicts of interest to declare.
References
1. Global strategy for prevention, diagnosis and management of COPD (2025 report). 2025. Available from: https://goldcopd.org/2025-gold-reports/.
2. Alter P, Baker JR, Dauletbaev N, et al. Update in chronic obstructive pulmonary disease 2019. Am J Respir Crit Care Med. 2020;202(3):348–355. doi:10.1164/rccm.202002-0370UP
3. Chhabra SK, De S. Cardiovascular autonomic neuropathy in chronic obstructive pulmonary disease. Respir Med. 2005;99(1):126–133. doi:10.1016/j.rmed.2004.06.003
4. Lacasse M, Maltais F, Poirier P, et al. Post-exercise heart rate recovery and mortality in chronic obstructive pulmonary disease. Respir Med. 2005;99(7):877–886. doi:10.1016/j.rmed.2004.11.012
5. Cole CR, Blackstone EH, Pashkow FJ, Snader CE, Lauer MS. Heart-rate recovery immediately after exercise as a predictor of mortality. N Engl J Med. 1999;341(18):1351–1357. doi:10.1056/NEJM199910283411804
6. Cole CR, Foody JM, Blackstone EH, Lauer MS. Heart rate recovery after submaximal exercise testing as a predictor of mortality in a cardiovascularly healthy cohort. Ann Intern Med. 2000;132(7):552–555. doi:10.7326/0003-4819-132-7-200004040-00007
7. Matos CH, Anjum F. Six-minute walk test. 2024.
8. Yuan W, Nie S, Wang H, Xu Q, Jia N. Anticholinergics aggravate the imbalance of the autonomic nervous system in stable chronic obstructive pulmonary disease. BMC Pulm Med. 2019;19(1):88. doi:10.1186/s12890-019-0848-0
9. ATS/ACCP Statement on cardiopulmonary exercise testing. Vol. 167. 2003:211–277.
10. Zimerman A, Da SA, Borges MS, et al. Functional assessment based on cardiopulmonary exercise testing in mild heart failure: a multicentre study. ESC Heart Fail. 2023;10:1689–1697. doi:10.1002/ehf2.14287
11. Kutac KB, Wagner MC, Davis PR. Variation in cardiopulmonary restoration due to bodily posture post-submaximal exercise in collegiate athletes. J Sport Med Phys Fit. 2023;63:1003–1009.
12. Kannankeril PJ, Le FK, Kadish AH, Goldberger JJ. Parasympathetic effects on heart rate recovery after exercise. J Investig Med. 2004;52(6):394–401. doi:10.1177/108155890405200634
13. Perini R, Orizio C, Comandè A, Castellano M, Beschi M, Veicsteinas A. Plasma norepinephrine and heart rate dynamics during recovery from submaximal exercise in man. Eur J Appl Physiol Occup Physiol. 1989;58(8):879–883. doi:10.1007/BF02332222
14. Chen W, Chen G, Kuo C. Hypoxemia and autonomic nervous dysfunction in patients with chronic obstructive pulmonary disease. Respir Med. 2006;100(9):1547–1553. doi:10.1016/j.rmed.2006.01.006
15. van Gestel AJR, Steier J. Autonomic dysfunction in patients with chronic obstructive pulmonary disease (COPD). J Thorac Dis. 2010;2(4):215–222. doi:10.3978/j.issn.2072-1439.2010.02.04.5
16. Undem BJ, Potenzieri C. Autonomic neural control of intrathoracic airways. Compr Physiol. 2012;2:1241–1267. doi:10.1002/j.2040-4603.2012.tb00428.x
17. Serrão NJ, Porta A, Minatel V, et al. Complexity analysis of heart rate variability in chronic obstructive pulmonary disease: relationship with severity and symptoms. Clin Auton Res. 2020;30:157–164. doi:10.1007/s10286-019-00659-z
18. Alqahtani JS, Aldhahir AM, Alghamdi SM, et al. A systematic review and meta-analysis of heart rate variability in COPD. Front Cardiovasc Med. 2023;10:1070327. doi:10.3389/fcvm.2023.1070327
19. Mohammed J, Meeus M, Derom E, Da SH, Calders P. Evidence for autonomic function and its influencing factors in subjects with COPD: a systematic review. Respir Care. 2015;60(12):1841–1851. doi:10.4187/respcare.04174
20. Wang X, Jiang Z, Chen B, et al. Cardiac autonomic function in patients with acute exacerbation of chronic obstructive pulmonary disease with and without ventricular tachycardia. BMC Pulm Med. 2016;16(1):124. doi:10.1186/s12890-016-0287-0
21. Peçanha T, Bartels R, Brito LC, Paula-Ribeiro M, Oliveira RS, Goldberger JJ. Methods of assessment of the post-exercise cardiac autonomic recovery: a methodological review. Int J Cardiol. 2017;227:795–802. doi:10.1016/j.ijcard.2016.10.057
22. Cheng YJ, Lauer MS, Earnest CP, et al. Heart rate recovery following maximal exercise testing as a predictor of cardiovascular disease and all-cause mortality in men with diabetes. Diabetes Care. 2003;26(7):2052–2057. doi:10.2337/diacare.26.7.2052
23. Yanagisawa S, Miki K, Yasuda N, et al. The prognostic value of treadmill exercise testing in very elderly patients: heart rate recovery as a predictor of mortality in octogenarians. Europace. 2011;13(1):114–120. doi:10.1093/europace/euq422
24. Kokkinos P, Myers J, Doumas M, et al. Heart rate recovery, exercise capacity, and mortality risk in male veterans. Eur J Prev Cardiol. 2012;19(2):177–184. doi:10.1177/1741826711398432
25. Arena R, Guazzi M, Myers J, Peberdy MA. Prognostic value of heart rate recovery in patients with heart failure. Am Heart J. 2006;151(4):851–857. doi:10.1016/j.ahj.2005.09.012
26. Myers J, Arena R, Dewey F, et al. A cardiopulmonary exercise testing score for predicting outcomes in patients with heart failure. Am Heart J. 2008;156(6):1177–1183. doi:10.1016/j.ahj.2008.07.010
27. Nissinen SI, Mäkikallio TH, Seppänen T, et al. Heart rate recovery after exercise as a predictor of mortality among survivors of acute myocardial infarction. Am J Cardiol. 2003;91:711–714. doi:10.1016/S0002-9149(02)03410-0
28. Ha D, Malhotra A, Ries AL, O’Neal WT, Fuster MM. Heart rate variability and heart rate recovery in lung cancer survivors eligible for long-term cure. Respir Physiol Neurobiol. 2019;269:103264. doi:10.1016/j.resp.2019.103264
29. Jin Q, Li X, Zhang Y, et al. Heart rate recovery at 1 min after exercise is a marker of disease severity and prognosis in chronic thromboembolic pulmonary hypertension. Respiration. 2022;101:455–464. doi:10.1159/000520314
30. Silva ÉP, Soares BA, Reimberg MM, et al. Heart rate recovery in asthmatic children and adolescents after clinical field test. BMC Pulm Med. 2021;21(1):61. doi:10.1186/s12890-020-01355-9
31. Zampogna E, Ambrosino N, Oliva FM, et al. Heart rate recovery in adult individuals with asthma. Monaldi Arch Chest D. 2022;93.
32. Zhang Y, Li X, Luo Q, et al. Heart-rate recovery at 1 min after exercise predicts response to balloon pulmonary angioplasty in patients with inoperable chronic thromboembolic pulmonary hypertension. Front Cardiovasc Med. 2022;9:795420. doi:10.3389/fcvm.2022.795420
33. Rodríguez DA, Kortianou EA, Alison JA, et al. Heart rate recovery after 6-min walking test predicts acute exacerbation in COPD. Lung. 2017;195(4):463–467. doi:10.1007/s00408-017-0027-0
34. Zhao D, Abbasi A, Casaburi R, et al. Identifying a heart rate recovery criterion after a 6-minute walk test in COPD. Int J Chron Obstruct Pulmon Dis. 2021;16:2545–2560. doi:10.2147/COPD.S311572
35. Bhatt SP, Balte PP, Schwartz JE, et al. Discriminative accuracy of FEV1:FVC thresholds for COPD-related hospitalization and mortality. JAMA. 2019;321(24):2438–2447. doi:10.1001/jama.2019.7233
36. Coote JH. Recovery of heart rate following intense dynamic exercise. Exp Physiol. 2010;95(3):431–440. doi:10.1113/expphysiol.2009.047548
37. MacDonald DM, Mkorombindo T, Ling SX, et al. Heart rate variability on 10-second electrocardiogram and risk of acute exacerbation of COPD: a secondary analysis of the BLOCK COPD trial. COPD. 2022;9:226–236. doi:10.15326/jcopdf.2021.0264
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
FIDEPOC: Consensus on Inspiratory Flow and Lung Deposition as Key Decision Factors in COPD Inhaled Therapy
González-Torralba F, Baloira A, Abad A, Fuster A, García-Rivero JL, García-Sidro P, Márquez-Martín E, Palop M, Soler N, Velasco JL
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:1005-1015
Published Date: 4 May 2022
Effect of Recent Exacerbation History on the Efficacy of Once-Daily Single-Inhaler Fluticasone Furoate/Umeclidinium/Vilanterol Triple Therapy in Patients with Chronic Obstructive Pulmonary Disease in the FULFIL Trial
Panettieri Jr RA, Camargo CA Jr, Cheema T, El Bayadi SG, Fiel S, Vila TM, Jain RG, Midwinter D, Thomashow B, Ludwig-Sengpiel A, Lipson DA
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2043-2052
Published Date: 1 September 2022
Plasma Extracellular Vesicle miRNA Profiles Distinguish Chronic Obstructive Pulmonary Disease Exacerbations and Disease Severity
O'Farrell HE, Bowman RV, Fong KM, Yang IA
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2821-2833
Published Date: 4 November 2022
Use of Remote Cardiorespiratory Monitoring is Associated with a Reduction in Hospitalizations for Subjects with COPD
Polsky M, Moraveji N, Hendricks A, Teresi RK, Murray R, Maselli DJ
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:219-229
Published Date: 3 March 2023
Exacerbations and Real-World Outcomes After Single-Inhaler Triple Therapy of Budesonide/Glycopyrrolate/Formoterol Fumarate, Among Patients with COPD: Results from the EROS (US) Study
Strange C, Tkacz J, Schinkel J, Lewing B, Agatep B, Swisher S, Patel S, Edwards D, Touchette DR, Portillo E, Feigler N, Pollack M
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2245-2256
Published Date: 12 October 2023