Back to Journals » Advances in Medical Education and Practice » Volume 12
Health Data Management Practice and Associated Factors Among Health Professionals Working at Public Health Facilities in Resource Limited Settings
Authors Ngusie HS ![]() , Shiferaw AM, Bogale AD, Ahmed MH
, Shiferaw AM, Bogale AD, Ahmed MH ![]()
Received 18 May 2021
Accepted for publication 21 July 2021
Published 7 August 2021 Volume 2021:12 Pages 855—862
DOI https://doi.org/10.2147/AMEP.S320769
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Balakrishnan Nair
Habtamu Setegn Ngusie,1 Atsede Mazengia Shiferaw,2 Adina Demissie Bogale,2 Mohammedjud Hassen Ahmed1
1Department of Health Informatics, College of Health Science, Mettu University, Mettu, Ethiopia; 2Department of Health Informatics, Institute of Public Health, College of Medicine and Health Science, University of Gondar, Gondar, Ethiopia
Correspondence: Habtamu Setegn Ngusie Email [email protected]
Background: Despite the vast amount of resources invested in the development of health information systems, health professionals in developing countries are still suffering from lack of adequate skill to perform health data management activities. There is a lack of sound evidence to overcome health data management challenges in this setting. This study aimed to assess health data management practice and its associated factors among health professionals working at public health facilities in North Wollo Zone, Northeast Ethiopia.
Methods: A quantitative cross-sectional study was conducted at public health facilities in North Wollo Zone, Northeast Ethiopia from March 2 to April 15, 2020. A total of 715 health professionalswere selected using a stratified random sampling technique. EpiData version 4.6 and STATA version 15 were used for data entry and analysis, respectively. Descriptive statistics were computed. Multi-variable logistic regression analyses techniques were carried out to show the association between explanatory and outcome variables. Odd ratio at 95% confidence level was used to describe the strength of association.
Results: A total of 643 health professionals participated in this study. The response rate was 90%. Among them, 56.1% (95% CI: 52.3%– 59.9%) demonstrated good data management practice. Working in health center [AOR=1.31 (95% CI: 1.853, 2.003)], having knowledge on data management [AOR=3.74 (95% CI: 2.454, 5.713)], favorable attitude toward data management [AOR=2.64 (95% CI: 1.746, 3.976)], high competency level on data management tasks [AOR=3.12 (95% CI: 1.873, 5.197)], friendliness of data management format [AOR=2.26 (95% CI: 1.478, 3.454)], supervision [AOR=1.78 (95% CI: 1.153, 2.745)] and training [AOR=1.84 (95% CI: 1.115, 3.022)] were significantly associated with good practice of health data management.
Conclusion: Health data management practices of health professionals’ were found to be inadequate. Capacity building to enhance health professionals’ data management knowledge, attitude and their competency level, providing continuous supportive supervision, designing friendly data management format, providing comprehensive data management training are necessary measures to improve data management practice in this study setting.
Keywords: health data management practice, health professionals, Ethiopia
Background
Health Information System (HIS) is a system that integrates data collection, processing, reporting and utilization of the information that are necessary for improving effectiveness and efficiency of healthcare services.1,2 Health Information System is used to design and manage healthcare data in healthcare facilities.3,4 Health data management is one of the six components of HIS that covers all aspect of data collection, storage, quality-assurance, compilation, analysis, display and report.5–7 It is an important alarming area which uses in promoting high standard of patient care and also it is highly significant for the allocation of healthcare budget.8,9 Data management practice is professionals’ routine practice to collect, store, check quality, compilation, analyze, display and report data.5,7 Having a good data management practice is a prerequisite for obtaining quality data for decision-making which enables policymakers, managers, and service providers to make decisions based on evidence.8,10,11
Despite the vast amounts of resources invested in the development of HIS, health providers are still suffering from the lack of adequate skill to perform data management activities.12,13 There are a lot of problems in developing country regarding to HIS implementation.14–21 Evidence showed the presence of poor health data management practice in Africa.22–27 Within the context of Ethiopia; some studies have examined the level of data management practice in the health sectors.10,28 Poor data management knowledge, supervision, feedback, training and resource shortage were the main determining factors associated with health data management practice.29–34
In Ethiopia, different efforts have been made to strengthen routine health information systems (RHIS).35,36 The Federal Ministry Of Health (FMOH) has designed, developed and implemented digital systems for managing health data including, District Health Information System 2 (DHIS2), to manage national reporting system, and electronic Community Health Information System (e-CHIS), to manage community health information system (CHIS).35,37
However, data management is still far behind the expectations and not showing substantial progress.38 The practical challenge in public health facilities is fragmented routine data collection and aggregation process, difficulty in interpreting results and implications of data, and poor informed decision-making practice on the health status of the population.10,39–41 Addressing this problem will have a practical benefit for improving coverage and quality of health services. Accordingly, this study proposes to investigate the practice of health data management and its associated factors among health professionals working at public health facilities in North Wollo Zone, Northeast Ethiopia.
Methods
Study Design and Setting
Institutional-based cross-sectional study design was conducted from March 2 to April 15, 2020, at public health facilities in North Wollo Zone. North Wollo is one of the 11 zones of the Amhara Regional state of Northern Ethiopia. The city of North Wollo is Woldia which is located 521 km away from Addis Ababa, the capital city of Ethiopia. It consists of ten rural and four urban districts. District or woreda is the administrative unit next to zone containing a minimum of 100,000 populations.42 There were 2132 health professionals working within six hospitals and 64 health centers.
Study Participants, Sample Size, and Sampling Procedure
The sample size was calculated using a single population proportion formula. It was calculated by considering a 95% level of confidence, a 5% of margin of error, a design effect of 2% and 5% of the non-response rate. There were a total of 2132 health professionals in this study setting. Finally, a total sample size of 715 health professionals was obtained. There are six hospitals and 64 health centers in North Wollo zone. Out of the total public health facilities, 3 hospitals and 29 health centers were selected by stratified random sampling technique. A total sample size of seven hundred fifteen participants proportionally allocated for each selected health center and hospital. Study participants were selected from the selected health centers and hospitals using a simple random sampling technique.
Data Collection Tool and Procedure
Data were collected using a pretested self-administered questionnaire and an observation checklist. The questionnaire was adopted from WHO measure evaluation tools of Health Metrics Network (HMN), Performance of Routine Information Systems Management (PRISM) tools, and related studies.2,7,31,32,36,43 A pretested self-administered questioners were filled by health professionals in order to assess health data management practice, socio-demographic, behavioral, technical, and organizational factors. The questioners consisted of 8 items for socio-demographic and 26 items for behavioral factors. Additionally, 8-item technical factors and 32-item organizational factor questions were used. The health data management practice of the respondents was assessed using 5-point Likert scale questions that ranged from “1 = strongly disagree” to “5 = strongly agree”.
An observational checklist was used to collect data on availability of data management tools, health information resources, guidelines and reporting documents. The content validity of the questioners was checked, and the reliability was calculated using Cronbach alpha (overall Cronbach alpha =0.83). A total of three degree holder health professionals and 9 HIT professionals were participated in data collection process. During the course of data collection, participants were informed about the objective and processes of the study and the confidentiality of the information.
Health professionals who scored greater than & equal to the mean value of Likert scale questions, ranging from “strongly disagree” to “strongly agree”, were labeled as having a good data management practice.31,32 Health professionals who scored less than the mean value were labeled as having poor data management practice. In this study, health professionals were defined as those employees who had at least a diploma certificate in the health profession and directly mange patients’ or clients’ data.
Data Processing and Analysis
After data collection was completed, the result was entered into a computer using EpiData version 4.6 and analysis was done using STATA version 15. Binary logistic regression analysis was conducted to discover the effect of each study variable on the outcome variable. Variables having a P -value <0.2 on the bivariate analysis was entered into a multi-variable logistic regression analysis. The strength of the association was described at 95% CI and P-value less than 0.05 was considered a cutoff point for significance relationship between independent variables and dependent variable. A multi-collinearity test was conducted for the model and none of the variables scored above 10 for the test statistic.
Result
Socio Demographic Characteristics
Out of 715 distributed questionnaires, 643 responses were received with a response rate of 90%. More than half of the respondents 362 (56.3%) were males with the mean age of participants was 34.68 ± 12.6 years. In terms of educational level, this study revealed that 387 (60.2%) of the respondents were degree holders Three hundred sixty-one study participants were rural residents.
Regarding the field of study, 212 (33.0%) respondents were nurses. The study implied that, 247 (38.4%), 162 (25.2%) and 234 (36.4%) respondents had less than 6 years, 6–10 years and above 11 years working experience, respectively. Four hundred ninety-seven of the respondents had above 2800 ETB monthly salaries, as shown in Table 1.
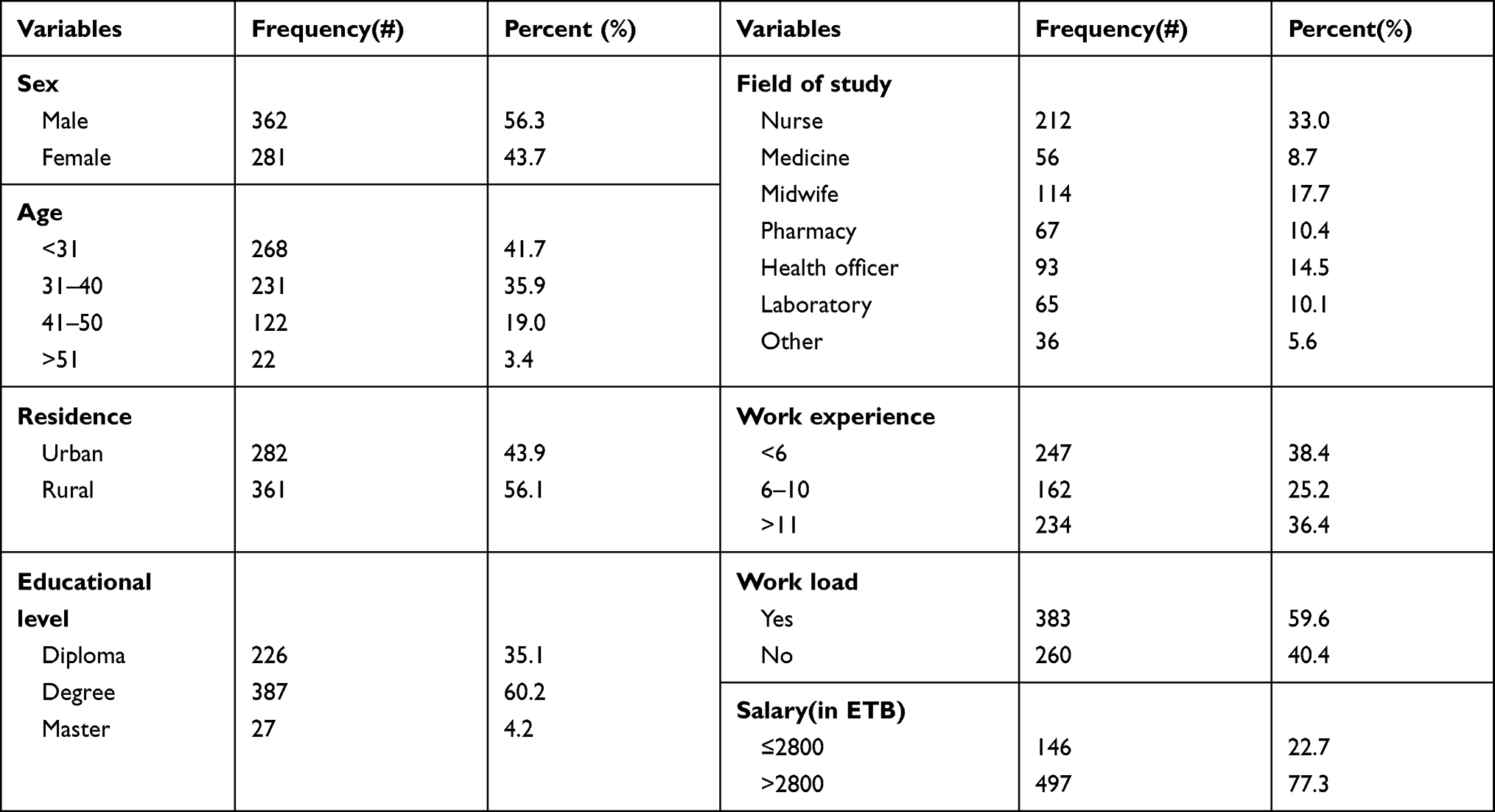 |
Table 1 Socio-Demographic and Economic Characteristics of Health Professionals in North Wollo Zone, Northeast Ethiopia, April, 2020 |
Behavioral Factors
This study implied that health professionals who had good knowledge on data management were found to be 49.6% [95% CI: 45.4, 53.2]. Health professionals who had a favorable attitude on data management were found to be 63.8% [95% CI: 59.2, 68.7]. The overall competence of health professionals for data management tasks was 28.3% [95% CI: 24.9, 31.9].
Organizational and Technical Factors
More than half, 377 (58.6%) of health professionals were supervised at least once within three months. Likewise, only 192 (29.9%) of health professionals had taken training on data management. Additionally, about 313 (48.7%) of the respondents got incentive for managing data. Majority of the respondents responded that reporting format (74.4%), tally sheet (70.8%) and stationery (72.2%) were available. Less than half of health professionals responded that there were available data management guideline (35.5%), graph paper (39.5%) and functional computer (12.6%) as shown in Table 2.
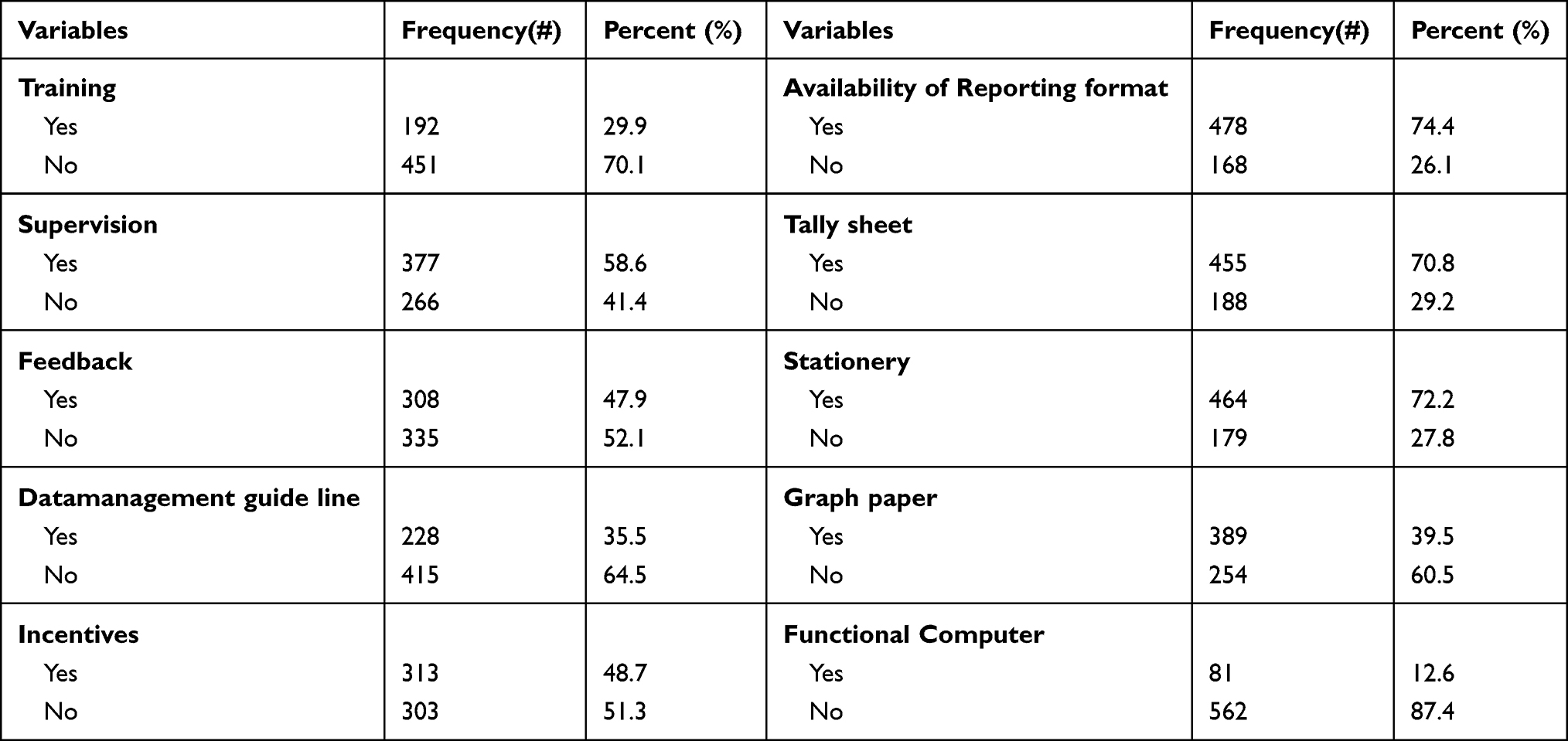 |
Table 2 Organizational and Technical Factors of HP’s in North Wollo Zone Factors Associated with Data Management Practice Northeast Ethiopia, April, 2020 |
In the bi-variable logistic regression analysis, health facility type, patient number per day, knowledge, attitude, competency, and friendliness of data management tools, availability of reference material, reporting format, HIS related training, supervision, feedback and incentive were associated with good routine health information utilization at a p-value of less than 0.2. Consequently, these variables were subjected to the multivariable logistic regression analysis to control potential confounders, and it was noted that, health facility type, knowledge, attitude, competency, friendliness of data management tools, training and supervision were significantly associated with good data management practice at a p-value of 0.05 (See Table 3 for details).
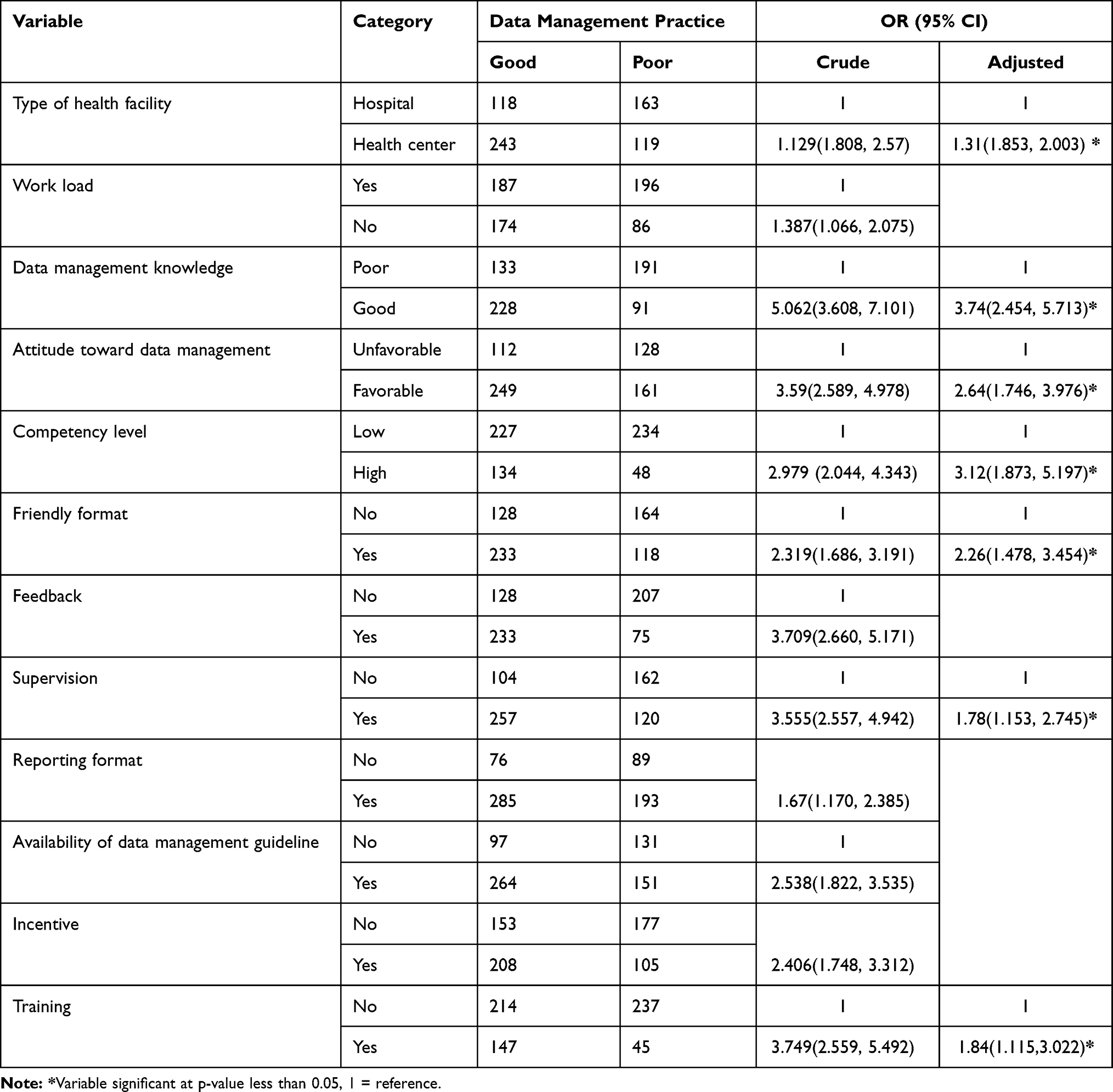 |
Table 3 Bivariate and Multivariable Logistic Regression Factors Associated with Data Management Practice Among HP at Primary Health Facilities in North Wollo Zone, Northeast Ethiopia, 2020 |
Discussion
In this study, based on the operational definition set, the overall data management practice of health professional in the study area was 56.1% (n = 361) [95% CI of 52.3% to 59.9%]. This finding was somewhat comparable to the study in Northwest Ethiopia where 53.3% of health extension workers had good data management practice.31 However, it was considerably higher than the HIS assessment conducted in Zanzibar and Jamaica whereas data management practice were 27%, and 48%, respectively.26,27 This explanation might be due to the difference in the study setting and the variation in health information system structures between Ethiopia and those countries.
It is also higher than the HIS assessments done in Ethiopia, whereas data management practice is 13%.28 The increment in the current study might be due to the study period. There is about an 8-year gap between the previous study and the current study; hence, the government concern for data management might be changed within this gap.
On the other hand, this finding was lower compared to the study done in Southern Ethiopia, whereas data management practice was 74.3%.32 This increment might be due to the difference in training, feedback and supervision. The study in southern Ethiopia showed that 93.6% of health extension workers were supervised and 41.6% of the participants got training in data management. On the contrary, only 29.9% of the respondents got training and 58.6% of them were supervised in the current study. The other possible explanation could be the study setting in Southern Ethiopia was health posts, whereas the current study was conducted on health centers and hospitals. Due to this reason, friendliness of data management format might be varying between those health posts and our study setting.
Data management practice is interlinked with socio-demographic, behavioral, and organizational factors. The knowledge of health professionals is highly associated with data management practice. Health professionals who had good knowledge were 3.74 [AOR=3.74 (95% CI: 2.454, 5.713)] times more likely to have good data management practice as compared to those health professionals who had poor knowledge on data management. This is in line with the study conducted before.32 This might be explained as knowing how and what to do is the prerequisite for practicing.
The results in this study indicate that health professionals who had a good attitude were 2.64[AOR=2.64 (95% CI: 1.746, 3.976)] times more likely to had good data management practice than those who had a poor attitude. This is consistent with the finding in previous studies.10,16,19,20,40,41 The explanation for this could be that the attitude of health professionals helps to be committed since they are not consider spent their time when managing routine data. Having a favorable attitude indicates an understanding of the relevance and usage of managing data that could lead to good practice by making health professionals responsible.
Respondents who have a good level of competency are about three [AOR=3.12 (95% CI: 1.873, 5.197)] times more likely to be good data managers. This is supported by the studies in Southern Ethiopia.10,18,40 The possible explanation for this could be low competency shows the skill gap and competency is crucial for performing data management tasks such as data quality checking, calculating percentages, plotting charts, providing a possible explanation of the findings of the data, explain trends with chart, using and interpreting data.
The finding of this study indicates that trained professionals are about 1.84 [AOR=1.84 (95% CI: 1.115, 3.022)] times more likely to be good data manager than who did not get training. This is supported by the previous studies conducted in Ethiopia and Nigeria.32,33 This could be as a result of training can enhance the capacity to carry out data management activities and it might create skilled human resource that are confident and motivated to perform data management tasks.
The odds of data management practice were 1.31 times higher [AOR=1.31 (95% CI: 1.853, 2.003)] among health professionals working at health centers when compared with those at hospitals. This might be due to the great concern for supervising and technical support in health centers. In this regard, this study noted that health professional who had supervision is about 1.78 [AOR=1.78 (95% CI: 1.153, 2.745)] times higher in data management practice than who are not supervised. This observation is supported by studies in different areas of the world.10,17,31 This might be due to supervision initiate health professionals to perform data management activities by providing on-the-job training and technical support.
Furthermore, the odds of data management practice among health professional who had friendly data management format were about 2.26 [AOR=2.26 (95% CI: 1.478, 3.454)] times higher than those who had no such formats. This is consistent with the result of the previous studies in Ethiopia.17,21,40 This might be due to a friendly format which enables health professional to understand easily what and how they do, and also it enables them efficient by saving their time during the overall data management activities. Moreover, having vague/unclear texts and inconsistent data management format might lead to health professionals not to managing health data in a proper way.
Limitation of the Study
All study participants were selected only from public health facilities. So, the major limitation of the study was that it did not include private health facilities. Additionally, the study was not supported by qualitative data.
Conclusion
Health data management practices of health professionals were found to be inadequate. Capacity building to enhance health professionals’ data management knowledge, attitude, and competency level, providing continuous supportive supervision, designing friendly data management format, and providing comprehensive data management training are necessary measures to scale up data management practice in this setting.
Abbreviations
AOR, Adjusted Odds Ratio; CHIS, Community Health Information System; CI, Confidence Intervals; DHIS2, District Health Information System 2; e-CHIS, electronic community health information system; FMOH, Federal Ministry of Health; HIS, Health Information Systems; HMN, Health Metrics Network; MPH, Master of Public Health; PRISM, Performance of Routine Information Systems Management; RHIS, Routine Health information System; WHO, World Health Organization.
Data Sharing Statement
The datasets generated and/or analyzed during the current study will be available upon request from the corresponding author.
Ethics Approval and Consent to Participate
The study protocol was reviewed and approved by the ethical review board of the University of Gondar and Informed consent was obtained from each study participant. Permission letters also obtained from Each Hospital. Names of participants and other personal identifiers were not included in the data collection tool. The participants’ consent included publications of anonymous responses and this study was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
The authors are indebted to the University of Gondar institute of public health ethical review board for the approval of ethical clearance and the Amhara region institute of public health, North Wollo zone health department, and respective district health offices for giving a supporting letter. The authors would like to extend their heartfelt thanks to facility managers, health professionals, data collectors, and supervisors who participated in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that there are no competing interests in this work.
References
1. Mutale W, Bond V, Mwanamwenge MT, et al. Systems thinking in practice: the current status of the six WHO building blocks for health system strengthening in three BHOMA intervention districts of Zambia: a baseline qualitative study. BMC Health Serv Res. 2013;13(1):291.
2. WHO. Health Information System Assessment Tool 2012. Available from: https://www.who.int/healthinfo/country_monitoring_evaluation/documentation/en/.
3. WHO. Assessing the National Health Information System: An Assessment Tool. World Health Organization; 2008.
4. WHO. Information Support for New Public Health Action at District Level: Report of a WHO Expert Committee [Meeting Held in Geneva from 17 to 22 November 1993]; 1994.
5. WHO. Health Metrics Network. Framework and Standards for Country Health Information Systems. Geneva: WHO; 2008:2010.
6. HRSA. Managing Data for Performance Improvement U S Department of Health and Human Services. USA;2011:3–17
7. Heywood A, Boone D. Guidelines for Data Management Standards in Routine Health Information Systems. Measure Evaluation. Geneva: USAID; 2015:23–54.
8. Kessel KA, Combs SE. Data management, documentation and analysis systems in radiation oncology: a multi-institutional survey. Rad Oncol. 2015;10(1):230.
9. WHO. Assessing health information system. HMIS Strategy and implementation plan for the national health management information system Liberia 2009; 2009. Available from: https://www.measureevaluation.org/countries/liberia/index.html.
10. Negash T. Assessment and Enhancement of HMIS Implementation Strategy in Oromiya Region at Chancho Health Center Addis Ababa. Addis Ababa University; 2015. Available from: http://localhost/xmlui/handle/123456789/14294.
11. Kitanbo M. Assessment of Hmis Design and Implementation in Ethiopia: The Case of Selected Public Health Facilities in Addis Ababa Health Bureau. Addis Ababa University; 2012.
12. Lu Z, Su J. Clinical data management: current status, challenges, and future directions from industry perspectives. Open Access J Clin Trials. 2010;2:93–105.
13. USAIDeM. Strengthening Health Information Systems in Low- and Middle-Income Countries: A Model to Frame What We Know and What We Need to Learn.; 2017.
14. Adamki M, Asamoah D, Riverson K. Assessment of data quality on Expanded Programme on Immunization in Ghana: the case of New Juaben municipality. J Health Med Informat. 2015;6(196):2.
15. FMOH. Health Management Information System Indicator Definition, Ethiopia; 2014.
16. Adane T, Tadesse T, Endazenaw G. Assessment on utilization of health management information system at public health centers Addis Ababa City Administrative, Ethiopia. Internet Things Cloud Comput. 2017;5(1):7–18.
17. Dagnew E, Woreta SA, Shiferaw AM. Routine health information utilization and associated factors among health care professionals working at public health institution in North Gondar, Northwest Ethiopia. BMC Health Serv Res. 2018;18(1):685.
18. Dufera MFN, Box P. Assessment of behavioral and organizational determinants of HMIS performance in Beghi, District West Wollega, Oromia, Ethiopia. Assessment. 2018;46.
19. Kebede M, Endris Y, Zegeye DT. Nursing care documentation practice: the unfinished task of nursing care in the University of Gondar Hospital. Inform Health Soc Care. 2017;42(3):290–302.
20. Ojuok T. Determinants of Utilization of Health Related Data for Service Improvement: A Case of Healthcare Facilities in Nyando Sub-County, Kenya [a master thesis work].University of Nairobi; 2015.
21. Teklegiorgis K, Tadesse K, Mirutse G, Terefe W. Factors associated with low level of health information utilization in resources limited setting, eastern Ethiopia. Inf Syst. 2014;3(6):69–75.
22. Olagbuji YW, Adejugbagbe AM. Improving the quality of health management information system: determinants of effective data management among data management officers in a South West State in Nigeria. Arch Current Res Int. 2018;21:1–11.
23. Moh W. Assessment of the health information system in angola measure evaluation. Geospatial Health. 2013;1:3.
24. Africa SS. Assessment of the Health Information System in South Africa Measure Evaluation; 2009.
25. Ekwueme O, Aniebue P, Obionu C, Onwasigwe C. Health data recording, reporting and utilization practices among primary health care workers in Enugu State, South Eastern Nigeria. Int J Med Health Develop. 2008;13(2):85–90.
26. Welfare MoHaS. Comprehensive Assessment of Zanzibar Health Information Systems. 2011:4
27. Willie D. National Health Information System Assessment 2011. Jamaica: WHO&MOH; 2014.
28. FMOH. Assessment of the Ethiopian National Health Information System; 2015.
29. Chidi C. Investigation of Factors Influencing Data Management in District Health Planning Process: A Case Study of Kibaha Town Council. Muhimbili University of Health and Allied Sciences; 2017.
30. Mathewos T Community Health Management Information System Performance and Factors Associated with at Health Post of Gurage zone, SNNPR, Ethiopia [M. Sc. thesis]. University of Gondar and Addis Continental Institute of Public Health; 2015.
31. Yitayew S, Asemahagn MA, Zeleke AA. Primary healthcare data management practice and associated factors: the case of health extension workers in Northwest Ethiopia. Open Med Inform J. 2014;13:1.
32. Shagake S, Mengistu M, Zeleke A. Data management knowledge, practice and associated factors of Ethiopian health extension workers in Gamo Gofa zone, southern Ethiopia: a cross-sectional study. J Health Med Informat. 2014;5(150):2.
33. Nwankwo B, Sambo MN. Can training of health care workers improve data management practice in health management information systems: a case study of primary health care facilities in Kaduna State, Nigeria. Pan Afr Med J. 2018;30:1.
34. Solomon M. Assessment of Quality of Data and Associated Factors in the Health Management Information System Among Health Centers of Hadiya Zone, Southern Ethiopia. Addis Ababa Universty; 2018.
35. Ministry of Health FDRoEMoFaED. National Health Information System Road Map 2012; 2012. Available from: http://repository.iifphc.org/handle/123456789/271.
36. Kebede M. Assessment of the Competence of Health Facilities to Operate in the Current Health Management Information System (HMIS) in Dire Dawa. Addis Ababa University; 2010.
37. FMOH. Annual Health Sector Performance Report. FMOH; 2018. Available from: https://www.moh.gov.et.
38. Directorate PPME. Training Module Information Use Facilitators Manual. FMOH. 3–24. 2018.
39. Health FMo. Health Management Information System (HMIS)/Monitoring and Evaluation (M&E) Strategic Plan for Ethiopian Health Sector. HMIS Reform Team; 2008.
40. Tesfaye Ki. Determinants of Health Management Information Utilization for Decision Making in Health Facilities Improvement Project at Woliso Town Administration Health Office S/W/Shoa Zone of Oromia Region. Addis Ababa University; 2015. Available from http://localhost/xmlui/handle/123456789/14406.
41. Shiferaw AM, Zegeye DT, Assefa S, Yenit MK. Routine health information system utilization and factors associated thereof among health workers at government health institutions in East Gojjam Zone, Northwest Ethiopia. BMC Med Inform Decis Mak. 2017;17(1):116.
42. Health EFMo. Ethiopian Population Based National TB Prevalence Survey Research Protocol, Addis Ababa; 2009.
43. Theo HB. Inventory of PRISM Framework and Tools: Application of PRISM Tools and Interventions for Strengthening Routine Health Information System Performance.U.S. Agency for International Development (USAID). 2013.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.