")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 17
Hand Grip Strength and Likelihood of Moderate-to-Severe Airflow Limitation in the General Population
Authors Kim S , Yoon HK , Rhee CK, Jung HW , Lee H , Jo YS
Received 2 March 2022
Accepted for publication 19 May 2022
Published 25 May 2022 Volume 2022:17 Pages 1237—1245
DOI https://doi.org/10.2147/COPD.S364351
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Russell
Sunyoung Kim,1 Hyoung Kyu Yoon,2 Chin Kook Rhee,3 Hee-Won Jung,4 Hyun Lee,5 Yong Suk Jo3
1Department of Family Medicine, College of Medicine, Kyung Hee University, Seoul, Korea; 2Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Yeouido St Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea; 3Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Seoul St Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea; 4Division of Geriatrics, Department of Internal Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea; 5Division of Pulmonary Medicine and Allergy, Department of Internal Medicine, Hanyang University College of Medicine, Seoul, Korea
Correspondence: Yong Suk Jo, Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Seoul St Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea, Tel +82-2-2258-6067, Fax +82-2-599-3589, Email [email protected]
Background and Objective: Sarcopenia is mainly results from aging; however, it is more prevalent in chronic airway disease such as obstructive pulmonary disease (COPD). Hand grip strength (HGS) can be used as an indicator to evaluate sarcopenia. We aimed to assess the association between HGS and severity of airflow limitation (AFL) in the general population.
Methods: We conducted a cross-sectional study using data from the Korea National Health and Nutrition Examination Survey (KNHANES) from 2014 to 2018. Subjects aged ≥ 40 years who underwent both spirometry and HGS tests were included. AFL was defined by spirometry revealed forced expiratory volume in 1 second (FEV1)/forced vital capacity (FVC) < 0.70). A propensity score-matched comparison was performed, and the risk for moderate-to-very severe AFL was analyzed using logistic regression analysis.
Results: Among 15,950 subjects, 2277 (14.3%) had AFL with mean FEV1 was 77.1% of the predicted value. Male was predominant in both individuals without AFL and with AFL (74.2% vs 73.5%, p = 0.613). The HGS was 32.9 ± 9.5 kg and 33.3 ± 9.5 kg in participants without AFL and with AFL (p = 0.109). However, HGS was significantly decreased as AFL getting more severe: 34.0 ± 9.6 kg in mild, 33.0 ± 9.5 kg in moderate, and 30.8 ± 8.5 kg in severe to very severe AFL group (p< 0.001). As HGS decreased, adjusted odds for moderate-to-very severe AFL increased compared to those with mild AFL (adjusted odds ratio [aOR], 0.97; 95% confidence interval [CI], 0.951– 0.987) and both without AFL and mild AFL group (aOR, 0.98; 95% CI, 0.967– 0.995) in age-, sex-, and body mass index (BMI)-matched comparisons.
Conclusion: Lower HGS is significantly associated with moderate-to-very severe AFL in age-, sex-, and BMI-matched comparisons.
Keywords: hand grip strength, airflow limitation, severity
Introduction
Chronic obstructive pulmonary disease (COPD) is a heterogeneous and complex inflammatory airway disease, characterized by fixed airflow limitation and related chronic respiratory symptoms, such as cough, phlegmon, and progressive dyspnea. COPD is not only a progressive debilitating disease but is also accompanied by multi-morbid conditions, making it difficult to manage and contributing to functional decline and disease progression.1–3 COPD patients suffer from loss of muscle mass, irrespective of measurement method, and muscle weakness and body weight loss are known to be associated with functional impairment.4–7 Moreover, loss of muscle mass and power can be more prominent in patients with moderate-to-severe COPD5 and during acute exacerbation.8
Sarcopenia is the loss of skeletal muscle mass and strength that occurs with aging9. The 2018 European Working Group of Sarcopenia in Older People emphasized the clinical importance of the “secondary sarcopenia” as a result of underlying diseases other than aging, such as COPD.10 Although the precise etiology and mechanism of sarcopenia are not fully understood, potential mechanisms might be linked to multifactorial factors, including aging, inflammation and related cytokines, oxidative stress, physical inactivity and inadequate energy and protein intake.11 Most of these contributing factors are the common features associated with sarcopenia and COPD.2,12 In patients with COPD, sarcopenia is frequently observed with varying prevalence across population settings, and its prevalence is estimated to range from 15% to 55%13 which is much higher than that in the general population. Sarcopenia can also negatively affect the clinical course of COPD patients.5,14,15
Handgrip strength (HGS) has been used as an important index of low muscle strength to diagnose sarcopenia, because low HGS is an indicator of overall muscular strength, nutritional status, muscle mass, and walking performance.16–18 Because of ease of use, HGS is advised for routine use in clinics and community healthcare.10
Prevalence of COPD in Korea reported to ranged from 13.1% to 14.6%; however, only less than 5% of the individuals visited hospitals and treated for COPD.19 The main reasons of low rate of COPD-related hospital visits are considered to be low level of awareness of COPD and low rate of conducting spirometry in those at high risk for COPD. Most of undiagnosed COPD patients might be either a- or mild symptomatic and it is difficult to find those group of individuals before they become over symptomatic COPD. We enable to approach these group of individuals through our nationally representative database. Identifying the association between low HGS and more severe AFL may help guide subjects toward further diagnostic test and treatment for COPD. In this study, we aimed to assess the association between low HGS and severity of AFL in general population.
Methods
Study Population
We used cross-sectional data from the Korean National Health and Nutrition Examination Survey (KNHANES), which provides nationwide statistical data on the Korean population’s health and diet annually. The hand grip test has been performed since 2014; thus, we analyzed KNHANES data from 2014 to 2019 and included subjects whose hand grip strength data were available. The KNHANES uses a complex, stratified multistage probability cluster sampling design, and sampling units are households based on geographic region, age, and gender groups. A health-related interview, nutrition survey, and physical examination were performed by trained interviewers for each participant selected throughout Korea. This study used the KNHANES database and was exempted from informed consent by the institutional review board (IRB) of Kyung Hee University Medical Center (IRB No. 2021-12-065).
Definition and Severity of Airflow Limitation
As spirometry was performed only in subjects aged ≥40 years in the KNHANES, we included subjects aged ≥40 years in the analyses. Those who did not perform the spirometry test or who had missing data regarding the hand grip test were excluded. Spirometry was performed by trained technicians in compliance with the standardized manual of the American Thoracic Society/European Respiratory Society (ATS/ERS) Task Force with dry rolling seal spirometers (Model 2130; Sensor Medics, Yorba Linda, CA, USA).20 All equipment are periodically calibrated, and quality control was performed. Normal predicted values for spirometry data were derived from the general population of Korea and all values were pre-bronchodilator results.21
AFL was defined as spirometry revealing forced expiratory volume in 1 second (FEV1)/forced vital capacity (FVC) <0.70). The severity of AFL was classified according to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) stage: stage 1 (mild, FEV1 ≥80% of predicted value), stage 2 (moderate, FEV1 ≥50% and <80% of predicted value), stage 3 (severe, FEV1 ≥30% and <50% of predicted value), and stage 4 (very severe, FEV1 <30% of predicted value).
Measurements of Demographics
KNHANES provides information on various demographic data (ie, age, sex, body mass index (BMI), smoking, economic activity, level of education, income, marital status, living area, and self-perceived income status), nutritional data (ie, calorie and protein intake), and spirometry results. The Korean version of the EuroQol-5 dimensions questionnaire (EQ-5D), a simple health-related quality of life (QoL) instrument consisting of five health dimensions (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression), was used to measure the QoL status.22,23 Dietary intake was estimated using the 24-hour recall method, which was conducted through face-to-face interviews with trained interviewers. Food and nutrient intakes were calculated using the 24-hour dietary recall assessment system of the National Institute of Health, based on the National Rural Living Science Institute database.24
Physical activity was measured using self-report questionnaire responses from the Global Physical Activity Questionnaire (GPAQ). This study divided the types of physical activity into aerobic, walking, and resistance exercises.25
For aerobic exercise, the metabolic equivalent task (MET) was calculated considering exercise intensity using work-related, movement-related, and leisure-related physical activity time (minutes). For work- and leisure-related physical activity, 8 and 4 MET for high-intensity and moderate-intensity physical activity, respectively, were multiplied according to the World Health Organization’s physical activity guidelines to calculate the weekly physical activity metabolic rate (min/week). Movement-related physical activity was multiplied by 4 MET to calculate the metabolic rate of physical activity per week (MET-min/week). For walking exercise, the metabolic rate of physical activity per week (MET-min/week) was calculated by multiplying the physical activity time (min) by 3.3 MET, based on the manipulative definition of low-intensity physical activity.26
Measurement of Hand Grip Strength (HGS)
HGS was measured in kilograms (kg) using a digital grip strength dynamometer (TKK 5401; Takei Scientific Instruments Co., Ltd., Tokyo, Japan). Participants were asked to apply their maximum grip strength in the standing position three times with both the right and left hands, with a resting interval of at least 30 seconds after each measurement. The highest of the six measured values was used.27
In Korea, the mean HGS was 39.5 ± 9.3kg in men and 24.4 ± 5.3 kg in women. The mean HGS was increased from 19 to 39 years, peaked at 35–39 years in both men (46.0 ± 7.2kg) and women (27.2 ± 4.6kg), and aging curve of HGS was steeper in men than in women. It was then decreased after 39 years.28
Comorbidities
Several comorbid conditions, which were identified using each definition, were also included in this study. The presence of hypertension (HTN) was determined by high blood pressure (mean systolic or diastolic blood pressure of ≥140 or ≥90 mmHg, respectively, and/or current intake of antihypertensive medications).29 Diabetes mellitus (DM) was defined as fasting glucose >126 mg/dL, HbA1c >6.5%, or current use of oral hypoglycemic agents or insulin for glycemic control.30 The presence of comorbidities was determined by a positive response to the following two questions: “Have you been diagnosed with the disease by a doctor?” or “Do you take medicine or treatment for the disease?”.
Statistical Analysis
To increase comparability and reliability, 1:1 propensity matching was performed according to age, sex, and BMI. Then, continuous and categorical variables were compared among the three groups by ANOVA and the chi-square test, respectively. To identify the influence of HGS on the severity of airflow limitation, a logistic regression model was used with adjustment for pack-year (PY), CAT score, total physical activity, income status, education level, economic activity, marital status, residential area, and protein intake. We further analyzed this association by applying comorbidities, including HTN, DM, ischemic heart disease (IHD), osteoporosis, depression, chronic kidney disease (CKD), and asthma as covariates.
All tests were two-sided, and a P-value of 0.05 was considered statistically significant. Statistical analysis was performed using STATA (version 16; Stata Corp, College Station, TX, USA).
Results
Prevalence and Severity of Airflow Limitation
Among 15,950 subjects with available spirometry and hand grip strength results, 2277 (14.3%) had AFL (Figure 1). With this, 2277 without AFL and AFL each were enrolled in propensity matching. Among AFL individuals, 45.5% (n = 1036) were mild, 48.7% (n = 1108) were moderate, and 5.8% (n = 133) were severe or very severe. Of the AFL individuals, only 2.6% (n = 60) reported that they had been diagnosed with COPD by a clinician.
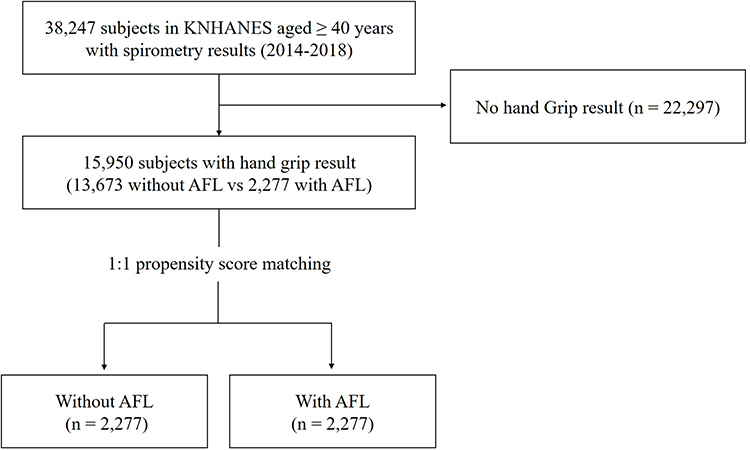 |
Figure 1 Flow of the study. Abbreviations: AFL, airflow limitation; KNHANES, Korean National Health and Nutrition Examination Survey. |
Clinical Manifestation Comparison According to the Severity of Airflow Limitation
A comparison of the clinical features between individuals without AFL and with AFL of mild and moderate-to-very severe AFL is presented in Table 1. Compared with the without AFL group, the proportion of participants who never smoked decreased and that of current smokers increased in the AFL group, especially as AFL became more severe (p<0.001). The mean smoking exposures showed a similar trend (12.01 PY vs 15.48 PY vs 19.29 PY in without AFL vs mild AFL vs moderate-to-very severe AFL; p<0.001). Lower proportion of participants with an education level above high school in the AFL group (p = 0.020). The Medicaid coverage rate was higher in the moderate-to-very severe AFL group (4.0% vs 4.2% vs 6.4% in without AFL vs mild AFL vs moderate-to-severe AFL group; p = 0.004), but there was no difference across the groups in subjective income status and economic activity rates (p = 0.115 and 0.370, respectively). Index of quality of life status was not significantly different across groups (p = 0.090). Medical histories of diabetes and asthma were more commonly accompanied by moderate-to-very severe AFL group as comorbidities (p<0.05 for both groups).
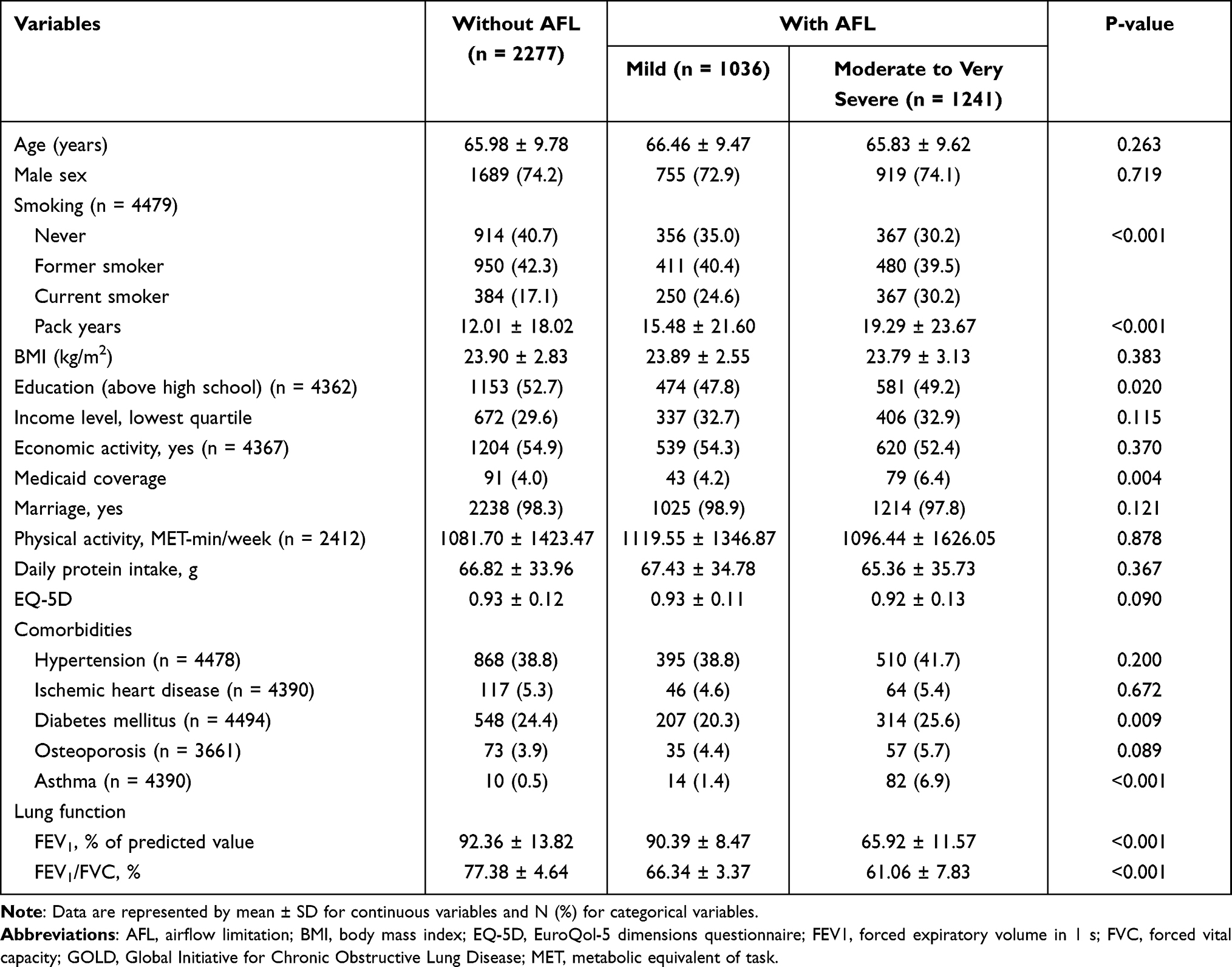 |
Table 1 Baseline Characteristics of Subjects |
HGS Across Groups
The HGS in without AFL and AFL group were 32.9 ± 9.5 kg and 33.3 ± 9.5 kg, respectively, with no significant difference between the two groups. When the HGS was compared by severity of the AFL, HGS of the moderate-to-very severe AFL group was 30.8 ± 8.5 kg, which was significantly lower than that of the without AFL (32.9 ± 9.5 kg) or mild AFL (34.0 ± 9.6 kg) and moderate AFL group (33.0 ± 9.5 kg) (p<0.001) (Figure 2).
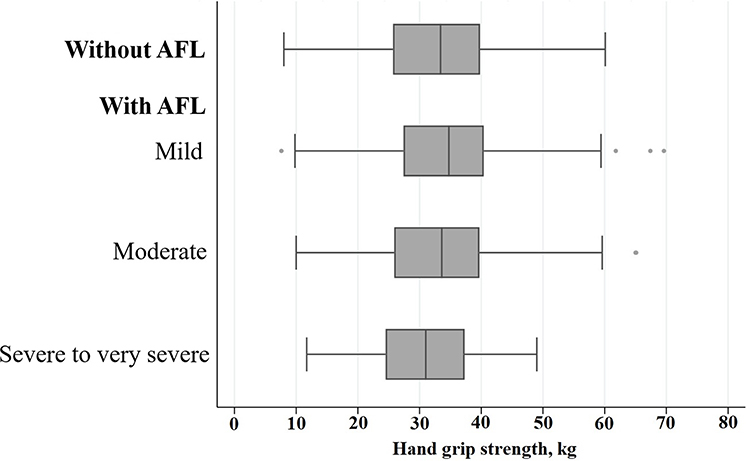 |
Figure 2 Hand grip strength according to the severity of airflow limitation. |
Association Between Severity of AFL and HGS
The association between HGS and the likelihood of moderate-to-very severe AFL was analyzed in two steps (Table 2). First, odds were calculated using mild AFL individuals as a reference, and the 1 kg greater the HGS, the lower the possibility of having moderate-to-very severe AFL (adjusted odds ratio [aOR], 0.97; 95% confidence interval [CI], 0.953–0.989). A similar result was found when chronic comorbid conditions were considered as covariates (aOR, 0.97; 95% CI, 0.954–0.994). Next, the risk was re-analyzed using without AFL and mild AFL together as a reference, and this inverse association between HGS and the likelihood of having moderate-to-very severe AFL persisted.
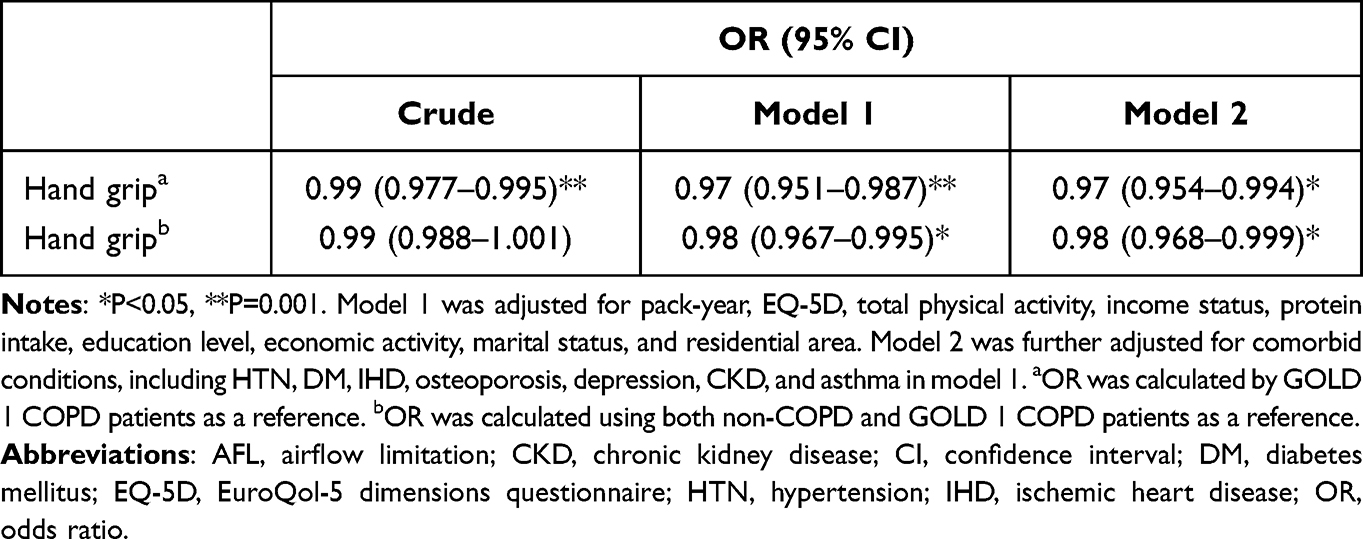 |
Table 2 Impact of Hand Grip Strength on the Risk of Moderate-to-Severe or Very Severe Airflow Limitation |
Discussion
In this population-based cross-sectional study, there was no significant difference in HGS between the subjects with and without AFL. However, we found lower HGS is significantly associated with moderate-to-very severe AFL in age-, sex-, and BMI-matched comparisons. This association between HGS and higher odds for moderate-to-very severe AFL was significant after adjustment for not only pack-years, QoL status, physical activity, income status, protein intake, education level, economic activity, marital status, residential area, but, comorbid conditions, including HTN, DM, and IHD as well compared with those without AFL and/or mild AFL.
Studies have reported contradicting results on the association between HGS and COPD. Some studies showed that severe to very severe AFL was associated with the presence of sarcopenia and lower HGS have an increased likelihood of morbidity and mortality of COPD.31,32 On the contrary, Marino et al reported that peripheral muscle strength as measured by HGS was not associated with the severity indexes for COPD.33 However, HGS measurement using a hand dynamometer is a simple measure to assess muscle strength and widely used. Moreover, it is accepted as useful tool to assess sarcopenia in not only general population but chronic ill patients.10
We defined AFL by spirometry-revealed FEV1/FVC ratio less than 0.7 irrespective of smoking exposure. Individuals with AFL might not representative for COPD and the possibility of overestimation of COPD exists, because there are other chronic respiratory conditions might cause AFL such as bronchiectasis and asthma. Although self-reported asthma history was more prevalent in moderate-to-very severe AFL group, it was only 6.9% (82 out of 1241). Unfortunately, we cannot evaluate bronchiectasis as comorbidity in this study because questionnaire on bronchiectasis was only available in the 2007–2009 in KNAHNES database. Subjects with AFL in this study has mean FEV1 was 77.1% of the predicted value and QoL was almost within normal and only 2.6% reported that they diagnosed as COPD by clinician. This suggestive for these group of individuals might be representative for asymptomatic, mild COPD in general population.
There has been growing attention on early detection and preventive manages on COPD because exacerbations eventually occur in some patients with mild-to-moderate COPD.34 Çolak et al35 reported that 15% of the early COPD patients existed in a population-based cohort when early COPD was defined by FEV1/FVC ratio less than the lower limit of normal in individuals under 50 years of age with 10 pack-years. These subjects had a higher risk for COPD-related hospitalization (hazard ratio [HR], 6.42; 95% confidence interval [CI], 3.39–12.2) and all-cause mortality (HR, 1.79; 95% CI, 1.28–2.52) during the 14.4-year follow-up. Considering the natural course and related socioeconomic burden of COPD, active surveillance for early detection for undiagnosed, mild COPD is required. The results of this study suggest that the hand grip test might be helpful in suspicion of undiagnosed COPD subjects with more than a moderate degree of AFL.
The cause of sarcopenia in COPD is a complex interaction of many factors, including poor oxygenation, inflammation triggering muscle proteolysis, oxidative stress, hypercapnia, decreased effect of anabolic hormones such as growth hormone and testosterone, frequent use of corticosteroids, and tobacco smoking.36–38 One longitudinal study of 7 years reported that not only COPD but also smokers not accompanied by COPD had lower muscle mass and strength and accelerated decrease of lean mass and muscle strength compared to former smoking control and never smoking controls.39
Sarcopenia has a multidimensional relationship with clinical features and outcomes in patients with COPD. Reduced muscle strength and impaired physical performance are predictors of poor quality of life and higher mortality in patients with COPD.40 Sarcopenia associated with functional limitation, physical disability, and physical inactivity can cause further deconditioning and deterioration of muscle strength and dyspnea, which are not attributed to COPD itself.41 Whether sarcopenia is a consequence of muscle dysfunction or a leading cause of acute exacerbation of COPD is incompletely understood; the prevalence of sarcopenia is higher in COPD subjects with frequent exacerbation.42 Moreover, the likelihood of readmission within 1 year for acute exacerbation of COPD is associated with low muscle mass at discharge from previous severe exacerbation requiring hospitalizations.43 In patients with COPD, accompanying sarcopenia helps to anticipate the prognosis, such as acute exacerbation, hospitalization, and even mortality; thus, early identification of sarcopenia in COPD might benefit patients centered on clinical decision-making and potentially improve outcomes by providing exercise and rehabilitation programs. Martinez et al31 found pectoralis muscle area and subcutaneous adipose tissue correlated well with HGS, and exacerbation risk (increase of 5% the risk of exacerbation for 1kg decrement in HGS) in COPD cohort. This implies simple measurement of HGS reflects pectoralis muscle and it might be indicative for sarcopenia in COPD.
Although data on muscle mass were not available and thus the approach to sarcopenia in COPD is not sufficient in our study, we considered various clinical and demographic factors related to not only grip strength but also COPD itself, including BMI, nutritional intake, physical activity, and comorbid conditions. The hand grip test is not the gold standard method to assess physical activity and muscle power in COPD patients, but it is a convenient and simple test to screen. Moreover, a decrease in muscle mass, strength, and physical performance is recommended for elderly people aged >65 years.44 We included subjects aged ≥40 years who underwent spirometry in their KNHANES check-up and were more focused on COPD itself rather than aging. KNHANES is not designed to evaluate chronic airway disease, but a nationally representative study designed to assess the health and nutritional status of civilians in Korea. Among 15,950 subjects, 14.3% were identified COPD by spirometry, but almost of them did not get disease-specific medical treatment. However, even these undiagnosed mild COPD patients, exacerbation events happened. A simple measurement of HGS might be helpful in guiding the suspicion of COPD in the general population.
This study had several limitations. First, only pre-bronchodilator spirometry was performed in the KNHANES; thus, fixed airflow limitation was not used to define COPD. However, prebronchodilator and postbronchodilator results were shown to be interchangeable in a large cohort study.6,45 Second, AFL on spirometry alone cannot represent COPD and there is possibility of overestimation. Third, KNHANES was not designed to evaluate sarcopenic status; thus, it does not contain data on muscle mass and power other than HG. Third, the metabolic phenotype of COPD is not restricted to muscle loss and sarcopenia.46 Moreover, more than 80% of AFL individuals have mild-to-moderate severity of AFL, making it difficult to generalize the clinical importance of HGS to COPD.
In conclusion, reduced HGS was more prevalent in moderate-to-very severe AFL individuals in general population, even after adjusting for various factors. A simple hand grip test might help in classifying the severity of AFL and might allow us to consider the need for further evaluation of COPD. Multidimensional studies on early detection and clinical effects in a- or mild symptomatic undiagnosed COPD patients by identifying moderate-to-severe AFL through accompanied sarcopenia are needed.
Institutional Review Board Statement
This study used data from KNHANES, which was approved by the Institutional Review Board of the Korea Centers for Disease Control (IRB No. 1401–047-547), and all participants signed an informed consent form. The present study complied with the Declaration of Helsinki-based ethical principles for medical research involving human subjects. The anonymity of the data is guaranteed, and no individually identifiable information is included.
Data Sharing Statement
The data of KNHANES are publicly available at https://knhanes.kdca.go.kr/knhanes/eng/index.do, accessed on 15 Nov 2021.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests.
References
1. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease; 2021. Available from: http://www.goldcopd.org.
2. Barnes PJ, Celli BR. Systemic manifestations and comorbidities of COPD. Eur Respir J. 2009;33(5):1165–1185. doi:10.1183/09031936.00128008
3. Houben-Wilke S, Augustin IM, Vercoulen JH, et al. COPD stands for complex obstructive pulmonary disease. Eur Respir Rev. 2018;27(148):180027. doi:10.1183/16000617.0027-2018
4. Maltais F, Decramer M, Casaburi R, et al. An official American Thoracic Society/European Respiratory Society statement: update on limb muscle dysfunction in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2014;189(9):e15–62. doi:10.1164/rccm.201402-0373ST
5. Costa TM, Costa FM, Moreira CA, Rabelo LM, Boguszewski CL, Borba VZ. Sarcopenia in COPD: relationship with COPD severity and prognosis. J Bras Pneumol. 2015;41(5):415–421. doi:10.1590/s1806-37132015000000040
6. Vestbo J, Prescott E, Almdal T, et al. Body mass, fat-free body mass, and prognosis in patients with chronic obstructive pulmonary disease from a random population sample: findings from the Copenhagen City Heart Study. Am J Respir Crit Care Med. 2006;173(1):79–83. doi:10.1164/rccm.200506-969OC
7. Pothirat C, Chaiwong W, Phetsuk N, et al. The relationship between body composition and clinical parameters in chronic obstructive pulmonary disease. J Med Assoc Thai. 2016;99(4):386–393.
8. Spruit MA, Gosselink R, Troosters T, et al. Muscle force during an acute exacerbation in hospitalised patients with COPD and its relationship with CXCL8 and IGF-I. Thorax. 2003;58(9):752–756. doi:10.1136/thorax.58.9.752
9. Morley JE, Baumgartner RN, Roubenoff R, Mayer J, Nair KS. Sarcopenia. J Lab Clin Med. 2001;137(4):231–243. doi:10.1067/mlc.2001.113504
10. Cruz-Jentoft AJ, Bahat G, Bauer J, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. 2019;48(1):16–31. doi:10.1093/ageing/afy169
11. Biolo G, Cederholm T, Muscaritoli M. Muscle contractile and metabolic dysfunction is a common feature of sarcopenia of aging and chronic diseases: from sarcopenic obesity to cachexia. Clin Nutr. 2014;33(5):737–748. doi:10.1016/j.clnu.2014.03.007
12. Evans RA, Morgan MD. The systemic nature of chronic lung disease. Clin Chest Med. 2014;35(2):283–293. doi:10.1016/j.ccm.2014.02.009
13. Jones SE, Maddocks M, Kon SS, et al. Sarcopenia in COPD: prevalence, clinical correlates and response to pulmonary rehabilitation. Thorax. 2015;70(3):213–218. doi:10.1136/thoraxjnl-2014-206440
14. Byun MK, Cho EN, Chang J, Ahn CM, Kim HJ. Sarcopenia correlates with systemic inflammation in COPD. Int J Chron Obstruct Pulmon Dis. 2017;12:669–675. doi:10.2147/copd.S130790
15. Hwang JA, Kim YS, Leem AY, et al. Clinical implications of sarcopenia on decreased bone density in men with COPD. Chest. 2017;151(5):1018–1027. doi:10.1016/j.chest.2016.12.006
16. Birman MV, Solomon GS, Vender MI. Functional capacity evaluation in hand surgery. J Hand Surg Am. 2016;41(1):133–134. doi:10.1016/j.jhsa.2015.11.008
17. Granic A, Jagger C, Davies K, et al. Effect of dietary patterns on muscle strength and physical performance in the very old: findings from the Newcastle 85+ study. PLoS One. 2016;11(3):e0149699. doi:10.1371/journal.pone.0149699
18. Springstroh KA, Gal NJ, Ford AL, Whiting SJ, Dahl WJ. Evaluation of handgrip strength and nutritional risk of congregate nutrition program participants in Florida. J Nutr Gerontol Geriatr. 2016;35(3):193–208. doi:10.1080/21551197.2016.1209146
19. Park YB, Yoo KH. The current status of chronic obstructive pulmonary disease awareness, treatments, and plans for improvement in South Korea: a narrative review. J Thorac Dis. 2021;13(6):3898–3906. doi:10.21037/jtd-21-172
20. Miller MR, Hankinson J, Brusasco V, et al. Standardisation of spirometry. Eur Respir J. 2005;26(2):319–338. doi:10.1183/09031936.05.00034805
21. Choi JK, Paek D, Lee JO. Normal predictive values of spirometry in Korean population. TRD. 2005;58(3):230–242. doi:10.4046/trd.2005.58.3.230
22. The EuroQol Group. EuroQol–a new facility for the measurement of health-related quality of life. Health Policy. 1990;16(3):199–208. doi:10.1016/0168-8510(90)90421-9
23. Lee YK, Nam HS, Chuang LH, et al. South Korean time trade-off values for EQ-5D health states: modeling with observed values for 101 health states. Value Health. 2009;12(8):1187–1193. doi:10.1111/j.1524-4733.2009.00579.x
24. Park S, Ham J-O, Lee B-K. Effects of total vitamin A, vitamin C, and fruit intake on risk for metabolic syndrome in Korean women and men. Nutrition. 2015;31(1):111–118. doi:10.1016/j.nut.2014.05.011
25. Armstrong T, Bull F. Development of the world health organization global physical activity questionnaire (GPAQ). J Public Health. 2006;14(2):66–70. doi:10.1007/s10389-006-0024-x
26. An KY. Comparison between walking and moderate-to-vigorous physical activity: associations with metabolic syndrome components in Korean older adults. Epidemiol Health. 2020;42:e2020066. doi:10.4178/epih.e2020066
27. Roberts HC, Denison HJ, Martin HJ, et al. A review of the measurement of grip strength in clinical and epidemiological studies: towards a standardised approach. Age Ageing. 2011;40(4):423–429. doi:10.1093/ageing/afr051
28. Lee YL, Lee BH, Lee SY. Handgrip strength in the Korean population: normative data and cutoff values. Ann Geriatr Med Res. 2019;23(4):183–189. doi:10.4235/agmr.19.0042
29. Mancia G, Fagard R, Narkiewicz K, et al. 2013 ESH/ESC guidelines for the management of arterial hypertension: the Task Force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J Hypertens. 2013;31(7):1281–1357. doi:10.1097/01.hjh.0000431740.32696.cc
30. American Diabetes Association. Standards of medical care in diabetes–2013. Diabetes Care. 2013;36(Suppl1):S11–S66. doi:10.2337/dc13-S011
31. Martinez CH, Diaz AA, Meldrum CA, et al. Handgrip strength in chronic obstructive pulmonary disease. associations with acute exacerbations and body composition. Ann Am Thorac Soc. 2017;14(11):1638–1645. doi:10.1513/AnnalsATS.201610-821OC
32. Holden M, Fyfe M, Poulin C, et al. Handgrip strength in people with chronic obstructive pulmonary disease: a systematic review and meta-analysis. Phys Ther. 2021;101(6). doi:10.1093/ptj/pzab057
33. Marino DM, Marrara KT, Ike D, De Oliveira AD Jr, Jamami M, Di Lorenzo VA. Study of peripheral muscle strength and severity indexes in individuals with chronic obstructive pulmonary disease. Physiother Res Int. 2010;15(3):135–143. doi:10.1002/pri.454
34. Rhee CK, Kim K, Yoon HK, et al. Natural course of early COPD. Int J Chron Obstruct Pulmon Dis. 2017;12:663–668. doi:10.2147/copd.S122989
35. Çolak Y, Afzal S, Nordestgaard BG, Vestbo J, Prevalence LP. Characteristics, and prognosis of early chronic obstructive pulmonary disease. the Copenhagen general population study. Am J Respir Crit Care Med. 2020;201(6):671–680. doi:10.1164/rccm.201908-1644OC
36. Gea J, Barreiro E, Orozco-Levi M. Free radicals, cytokines, and respiratory muscles in COPD patients. Clin Pulm Med. 2007;14(3):117–126. doi:10.1097/CPM.0b013e3180575dcd
37. Barreiro E, Peinado VI, Galdiz JB, et al. Cigarette smoke-induced oxidative stress: a role in chronic obstructive pulmonary disease skeletal muscle dysfunction. Am J Respir Crit Care Med. 2010;182(4):477–488. doi:10.1164/rccm.200908-1220OC
38. Decramer M, de Bock V, Dom R. Functional and histologic picture of steroid-induced myopathy in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1996;153(6 Pt 1):1958–1964. doi:10.1164/ajrccm.153.6.8665061
39. van den Borst B, Koster A, Yu B, et al. Is age-related decline in lean mass and physical function accelerated by obstructive lung disease or smoking? Thorax. 2011;66(11):961–969. doi:10.1136/thoraxjnl-2011-200010
40. Puhan MA, Siebeling L, Zoller M, Muggensturm P, ter Riet G. Simple functional performance tests and mortality in COPD. Eur Respir J. 2013;42(4):956–963. doi:10.1183/09031936.00131612
41. Rolland Y, Czerwinski S, Abellan Van Kan G, et al. Sarcopenia: its assessment, etiology, pathogenesis, consequences and future perspectives. J Nutr Health Aging. 2008;12(7):433–450. doi:10.1007/bf02982704
42. Perrot L, Greil A, Boirie Y, et al. Prevalence of sarcopenia and malnutrition during acute exacerbation of COPD and after 6 months recovery. Eur J Clin Nutr. 2020;74(11):1556–1564. doi:10.1038/s41430-020-0623-6
43. Greening NJ, Harvey-Dunstan TC, Chaplin EJ, et al. Bedside assessment of quadriceps muscle by ultrasound after admission for acute exacerbations of chronic respiratory disease. Am J Respir Crit Care Med. 2015;192(7):810–816. doi:10.1164/rccm.201503-0535OC
44. Cruz-Jentoft AJ, Baeyens JP, Bauer JM, et al. Sarcopenia: European consensus on definition and diagnosis: report of the European Working Group on sarcopenia in older people. Age Ageing. 2010;39(4):412–423. doi:10.1093/ageing/afq034
45. Ischaki E, Papatheodorou G, Gaki E, Papa I, Koulouris N, Loukides S. Body mass and fat-free mass indices in COPD: relation with variables expressing disease severity. Chest. 2007;132(1):164–169. doi:10.1378/chest.06-2789
46. Schols AM, Ferreira IM, Franssen FM, et al. Nutritional assessment and therapy in COPD: a European Respiratory Society statement. Eur Respir J. 2014;44(6):1504–1520. doi:10.1183/09031936.00070914
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Trajectories of Spirometric Patterns, Obstructive and PRISm, in a Population-Based Cohort in Latin America
Perez-Padilla R, Montes de Oca M, Thirion-Romero I, Wehrmeister FC, Lopez MV, Valdivia G, Jardim JR, Muino A, B Menezes AM
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:1277-1285
Published Date: 21 June 2023
Impaired Skeletal Muscle in Patients with Stable Chronic Obstructive Pulmonary Disease (COPD) Compared with Non-COPD Patients
Wu ZY, Lu XM, Liu R, Han YX, Qian HY, Zhao Q, Niu M
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:1525-1532
Published Date: 19 July 2023
Underdiagnosis of COPD: The Japan COPD Real-World Data Epidemiological (CORE) Study
Koga Y, Deguchi S, Matsuo T, Suzuki A, Terashima G, Tajima T, Shibata Y, Sagara H
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:1011-1019
Published Date: 7 May 2024