Back to Journals » Journal of Hepatocellular Carcinoma » Volume 13
HAIC Combined with Lenvatinib and Pembrolizumab for Unresectable Hepatocellular Carcinoma: A Retrospective Study
Authors Liang J, Yang Z, Yang Z, Li H, Hong J, Pan Y ![]() , Fu Y
, Fu Y ![]() , Wang J, Zhou Z, Zhang Y
, Wang J, Zhou Z, Zhang Y ![]() , Chen M, Chen J
, Chen M, Chen J ![]() , Hu D
, Hu D
Received 1 February 2026
Accepted for publication 20 May 2026
Published 26 May 2026 Volume 2026:13 600557
DOI https://doi.org/10.2147/JHC.S600557
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Jörg Trojan
Jun Liang,1,2,* Zhenyun Yang,1,2,* Zhuolin Yang,1,* Haozhong Li,1,2 Jincheng Hong,1,2 Yangxun Pan,1,2 Yizhen Fu,1,2 Juncheng Wang,1,2 Zhongguo Zhou,1,2 Yaojun Zhang,1,2 Minshan Chen,1,2 Jinbin Chen,1,2 Dandan Hu1,2
1State Key Laboratory of Oncology in South China, Sun Yat-sen University Cancer Center, Guangzhou, 510060, People’s Republic of China; 2Department of Liver Surgery, Sun Yat-sen University Cancer Center, Guangzhou, 510060, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Dandan Hu, Department of Liver Surgery, Sun Yat-sen University Cancer Center, Dongfeng East Road 651, Guangzhou, Guangdong, 510000, People’s Republic of China, Tel +86-20-87343828, Fax +86-20-87343585, Email [email protected] Jinbin Chen, Department of Liver Surgery, Sun Yat-sen University Cancer Center, Dongfeng East Road 651, Guangzhou, Guangdong, 510000, People’s Republic of China, Tel +86-20-87343828, Fax +86-20-87343585, Email [email protected]
Background & Aims: The optimal treatment strategy for unresectable hepatocellular carcinoma (uHCC) remains under active investigation. Hepatic arterial infusion chemotherapy (HAIC) has shown promising outcomes, particularly among patients with high intrahepatic tumor burden. We assessed outcomes and tolerability of HAIC combined with lenvatinib and pembrolizumab (HAIC+L+P) as initial treatment for uHCC.
Methods: We retrospectively identified consecutive, treatment-naïve patients with uHCC (BCLC stage B/C) treated with HAIC+L+P at a single center from January 2019 to January 2024. Tumor responses were evaluated using RECIST 1.1 and mRECIST. Overall survival (OS), progression-free survival (PFS), and treatment-related adverse events (AEs) were analyzed.
Results: Sixty-six patients were analyzed, of whom 81.8% had BCLC stage C disease, 68.2% had vascular invasion, and 45.5% had extrahepatic metastasis. The median PFS was 9.63 months (95% CI, 6.59– 12.68), and the median OS was 27.50 months (95% CI, 18.17– 36.83). The ORR was 47.0% according to RECIST 1.1 and 66.7% according to mRECIST, with a DCR of 90.9% by both criteria. Six patients (9.1%) underwent curative-intent surgical resection during treatment. All AEs were controllable and no treatment-related deaths were recorded.
Conclusion: HAIC combined with lenvatinib and pembrolizumab was associated with encouraging antitumor activity and a manageable safety profile in this real-world cohort. These findings should be considered hypothesis-generating and warrant validation in prospective controlled studies.
Keywords: hepatocellular carcinoma, hepatic arterial infusion chemotherapy, lenvatinib, pembrolizumab
Introduction
In 2022, primary liver cancer ranked as the sixth most frequently diagnosed malignancy and the third leading cause of cancer-related mortality worldwide, with hepatocellular carcinoma (HCC) accounting for approximately 75–85% of cases.1 Owing to the often asymptomatic early course, diagnosis for patients often occurs at intermediate or advanced stages, when curative surgery is usually not feasible.2,3 Consequently, systemic and local therapies have become the backbone of management for many patients.
Combination therapies, integrating both systemic and local approaches, have shown promising results in improving treatment outcomes for HCC. Multiple studies have demonstrated that combining systemic and locoregional treatments can significantly enhance survival.4–7 The LEAP-012 trial provides one example: in patients with unresectable hepatocellular carcinoma (uHCC) without extrahepatic metastasis, adding lenvatinib plus pembrolizumab to transarterial chemoembolization (TACE) resulted in a clear prolongation of PFS versus TACE with placebo, alongside favorable OS signals. In parallel, EMERALD-1 showed that incorporating durvalumab and bevacizumab into a TACE-based strategy substantially extended PFS compared with TACE alone, while no unexpected safety concerns emerged in a clinically diverse uHCC population.8,9
In terms of systemic therapy, targeted therapy and immunotherapy are the most commonly utilized strategies. In the REFLECT study, lenvatinib achieved OS outcomes comparable to sorafenib, meeting the trial’s prespecified non-inferiority criterion in uHCC.10 In addition, the KEYNOTE-394 study reported that pembrolizumab, administered as second-line therapy, significantly prolonged both OS and PFS in previously treated Asian patients with advanced HCC, and produced a higher ORR than placebo.11
Local treatments also play a critical role in HCC management. HAIC is a well-established modality for intermediate and advanced HCC, wherein chemotherapy is delivered via the hepatic artery, ensuring high intrahepatic exposure while minimizing systemic toxicity.12,13 Several studies suggest that HAIC may be more effective than TACE, particularly for large HCCs or those with portal vein thrombosis.14–18 Moreover, a prior report associated the addition of HAIC to lenvatinib plus PD-1 inhibition with longer OS and PFS than systemic therapy alone.19
Despite these advances, the most effective treatment sequence for advanced HCC still remains a subject of ongoing research. Early data indicate that combination of HAIC+L+P may overcome resistance to monotherapy and improve patient outcomes.20 However, evidence specifically evaluating HAIC combined with lenvatinib and pembrolizumab in treatment-naive uHCC remains limited. Therefore, this study aimed to evaluate the efficacy and safety of this combination in a real-world cohort.
Methods
Patient Selection
We retrospectively screened consecutive patients with uHCC treated at Sun Yat-sen University Cancer Center who received HAIC+L+P between January 2019 and January 2024. The Institutional Review Board of Sun Yat-sen University Cancer Center approved the study (Approval number: B2023-673-01). The study adhered to the Declaration of Helsinki, and the requirement for written informed consent was waived due to the retrospective design. Patient confidentiality was strictly maintained, and all data were anonymized.
Eligible patients met all of the following criteria: (a) HCC diagnosis established by imaging and/or pathology according to the American Association for the Study of Liver Diseases (AASLD) guidance; (b) BCLC stage B or C; (c) ECOG performance status 0–1; (d) at least one measurable lesion; (e) receipt of HAIC+L+P as first-line treatment, with at least one cycle completed; (f) complete baseline and follow-up records. Patients were excluded if they had incomplete follow-up information, a history of other malignancies, inability to continue treatment for non-medical reasons, or severe hepatic/renal/cardiopulmonary dysfunction.
Treatment Procedure
HAIC was performed according to institutional standard procedures. Catheter placement was determined based on tumor-feeding arteries and angiographic findings.15,21 After arterial access via the Seldinger technique, angiography was performed to delineate tumor-feeding vessels, and a microcatheter was positioned within the target hepatic arterial branch. To reduce catheter-related thrombosis, heparinized saline was infused after catheter placement. Chemotherapy was then administered through the hepatic artery using a FOLFOX-based regimen: oxaliplatin 85–130 mg/m2 over 2 hours, calcium folinate 400 mg/m2 over 2 hours, and 5-fluorouracil 400 mg/m2 as a 1-hour bolus, followed by continuous 5-fluorouracil 2400 mg/m2 over 23 hours. Treatment cycles were repeated every 3 weeks, accompanied by standard supportive measures (antiemetics, hydration, and hepatoprotective care) during the chemotherapy infusion.22,23
Lenvatinib and pembrolizumab were initiated within 1 week before or after HAIC. Lenvatinib was given orally once daily at 8 mg/day for body weight <60 kg and 12 mg/day for ≥60 kg. Pembrolizumab was given intravenously at 200 mg every 3 weeks.24 Dose modifications of lenvatinib and pembrolizumab were performed based on toxicity, liver function, and clinical judgment according to institutional practice.
The number of HAIC cycles and systemic therapy cycles varied depending on treatment response and tolerance. Subsequent treatments after disease progression were heterogeneous and included systemic therapy, locoregional interventions, or best supportive care.
Efficacy and Safety Evaluation
Patients were followed through 1 October 2025. Clinical assessment was performed at least every 2 months after treatment initiation, together with laboratory tests and contrast-enhanced imaging. Abdominal CT/MRI was routinely obtained, and additional sites (eg, chest, bone, brain) were evaluated when clinically indicated. Up to two target lesions per organ were selected. Lesions were considered measurable when the longest diameter exceeded 1 cm. Tumor response was evaluated using the Response Evaluation Criteria in Solid Tumors version 1.1 (RECIST 1.1) and the modified Response Evaluation Criteria in Solid Tumors (mRECIST) and categorized as complete response (CR), partial response (PR), stable disease (SD), or progressive disease (PD). The objective response rate (ORR) was defined as the proportion of patients achieving CR or PR, and the disease control rate (DCR) as the proportion achieving CR, PR, or SD.
Overall survival (OS) was calculated from treatment start to death from any cause or last follow-up. Progression-free survival (PFS) was calculated from treatment start to radiographic progression or death, whichever occurred first. Treatment-related adverse events(AEs) were recorded and graded according to the Common Terminology Criteria for Adverse Events (CTCAE) version 5.0.
Statistical Analysis
Statistical analyses were performed using SPSS (version 25.0) and R (version 4.4.1). Continuous variables are presented as mean ± standard deviation when approximately normally distributed and as median (IQR) otherwise. Kaplan–Meier curves and waterfall plots were generated in R software. Cox proportional hazards models were used to evaluate associations with OS and PFS; variables with P < 0.05 on univariable testing were entered into multivariable models. All tests were two-sided, with P < 0.05 considered statistically significant. The number of events relative to variables included in multivariable Cox models was considered to minimize overfitting.
Results
Patient Characteristics
Between January 2019 and January 2024, we included 66 treatment-naïve patients with uHCC who received HAIC+L+P. (Figure 1). Baseline characteristics are summarized in Table 1. The cohort had a median age of 57.0 years, and men accounted for 93.9% (62/66). Liver function was generally preserved, with 90.9% classified as Child–Pugh A. Hepatitis B virus infection was prevalent, with 84.8% (56/66) of patients testing positive for hepatitis B surface antigen (HBsAg).
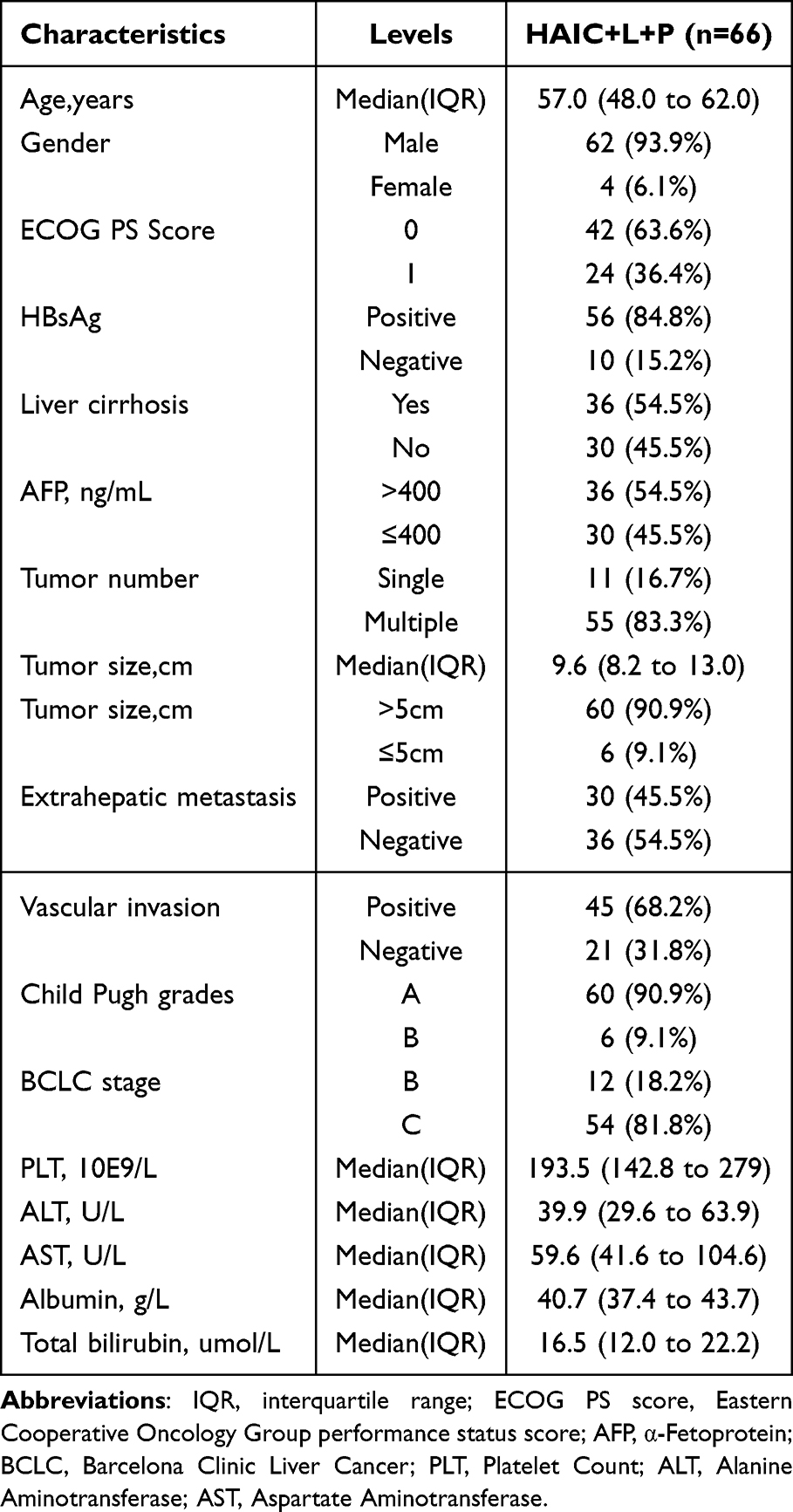 |
Table 1 Baseline Characteristics |
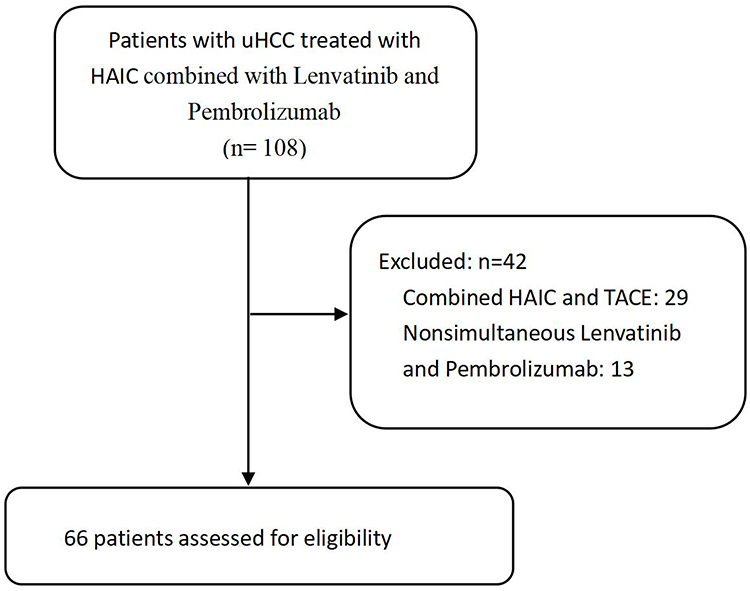 |
Figure 1 The flowchart of the study. |
Regarding tumor burden, most patients presented with advanced disease. A total of 81.8% (54/66) of patients were classified as BCLC stage C, and 83.3% (55/66) had multiple intrahepatic lesions. The median maximum tumor diameter was 9.6 cm (IQR, 8.2–13.0), and tumors larger than 5 cm were observed in 90.9% (60/66) of patients. Vascular invasion was present in 68.2% (45/66) of cases, while extrahepatic metastasis, including lymph node and distant metastases, was observed in 45.5% (30/66) of patients.
Survival Analysis
Patients received a median of 4 HAIC cycles (IQR, 3–5) and a median of 5 pembrolizumab cycles (IQR, 3–9). Following treatment, 6 patients (9.1%) underwent curative-intent surgical resection.
At a median follow-up of 19.9 months (IQR, 11.4–27.5), median PFS was 9.63 months (95% CI, 6.59–12.68), with 3- and 6-month PFS rates of 73.7% and 42.3%, respectively (Figure 2). Median OS was 27.50 months (95% CI, 18.17–36.83) (Figure 3), and OS rates at 6, 12, and 18 months were 93.8%, 79.1%, and 62.2%, respectively (Figure 3).
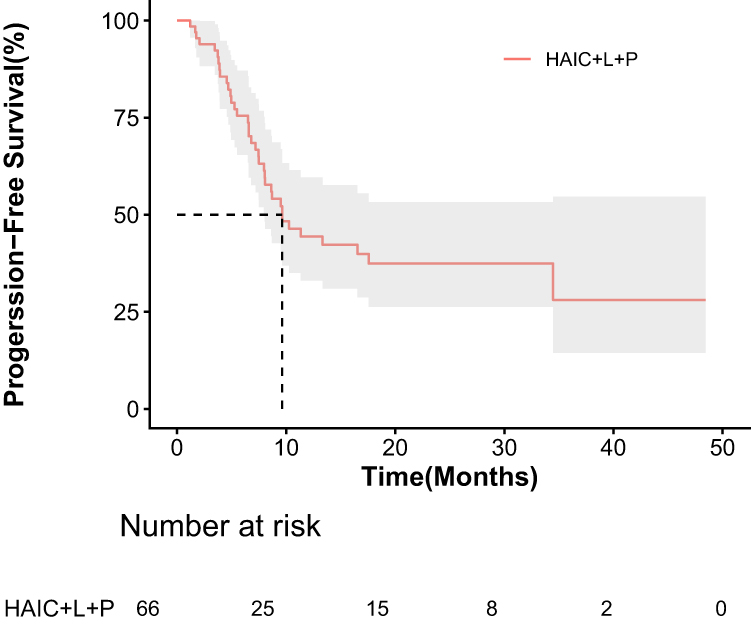 |
Figure 2 Kaplan–Meier curves for progression-free survival. |
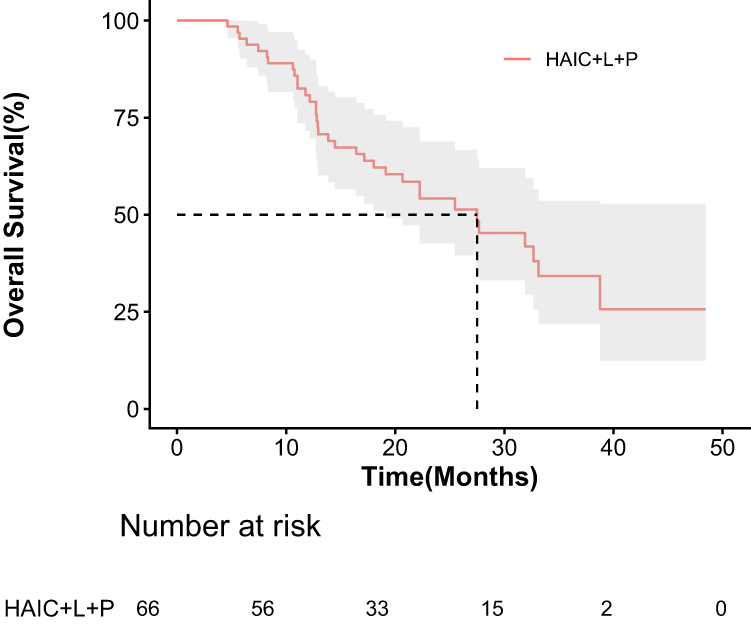 |
Figure 3 Kaplan–Meier curves for overall survival. |
Tumor Response
Most patients experienced a substantial decrease in target-lesion burden relative to baseline (Figure 4). Using RECIST 1.1, the ORR was 47.0% (31/66) and the DCR was 90.9% (60/66). With mRECIST-based evaluation, the ORR rose to 66.7% (44/66), whereas the DCR remained unchanged at 90.9% (60/66).
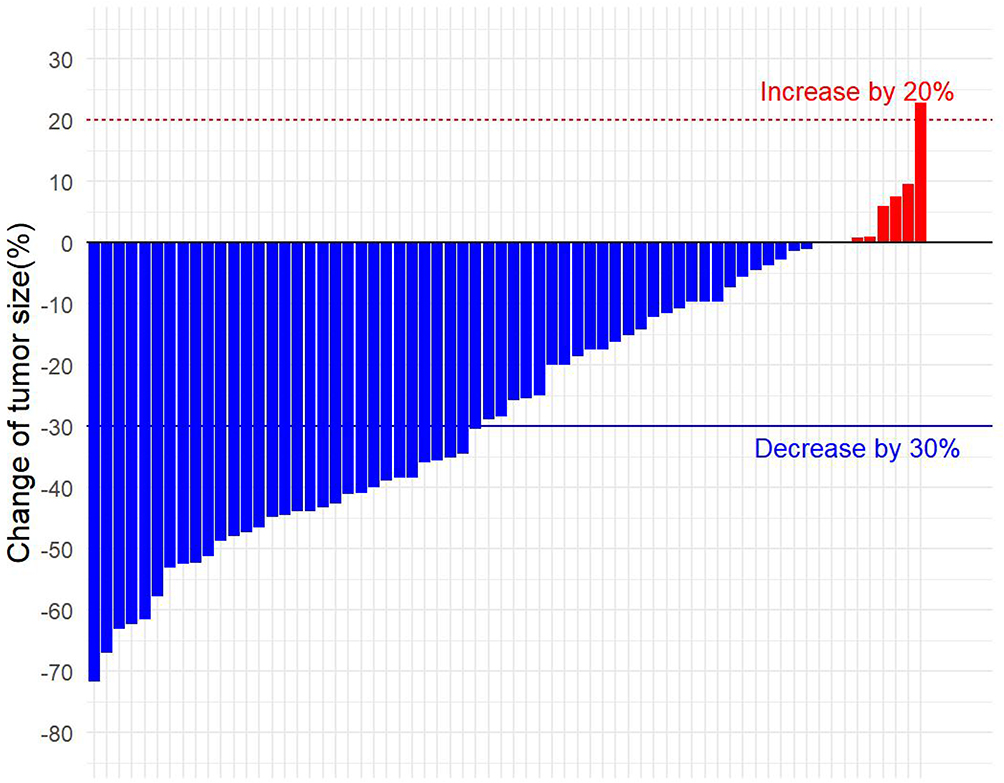 |
Figure 4 Change of tumor size after treatment. |
Under mRECIST criteria, 1 patient (1.5%) achieved CR, whereas no CR were observed according to RECIST 1.1. PR were observed in 31 patients (47.0%) based on RECIST 1.1 and in 43 patients (65.2%) based on mRECIST. SD was observed in 29 patients (43.9%) according to RECIST 1.1 and in 16 patients (24.2%) according to mRECIST. PD occurred in 6 patients (9.1%) under both evaluation criteria, with disease progression primarily driven by the development of distant metastases (5/6) (Table 2).
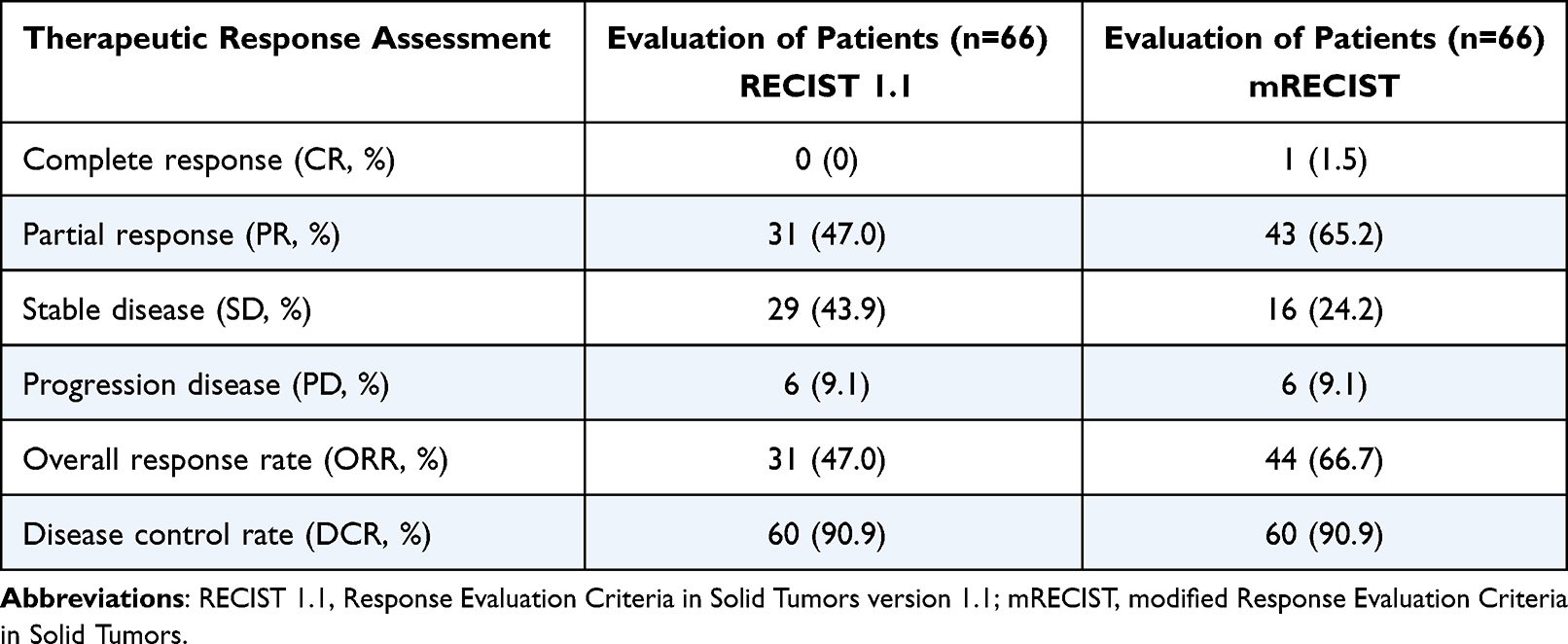 |
Table 2 Tumor Response |
Prognostic Factor Analysis
Cox proportional hazards models were used to explore variables associated with PFS and OS. On univariable analysis, patients with AFP ≤400 ng/mL had better OS, whereas a serum ALB level ≤40 g/L was linked to inferior outcomes for both OS and PFS.
These relationships persisted after multivariable adjustment. AFP ≤400 ng/mL remained an independent favorable factor for OS (hazard ratio [HR], 0.42; 95% CI, 0.21–0.85; P = 0.007). Conversely, ALB ≤40 g/L independently predicted poorer OS (HR, 2.91; 95% CI, 1.44–5.88; P = 0.001) and shorter PFS (HR, 2.15; 95% CI, 1.10–4.21; P = 0.025) (Table 3).
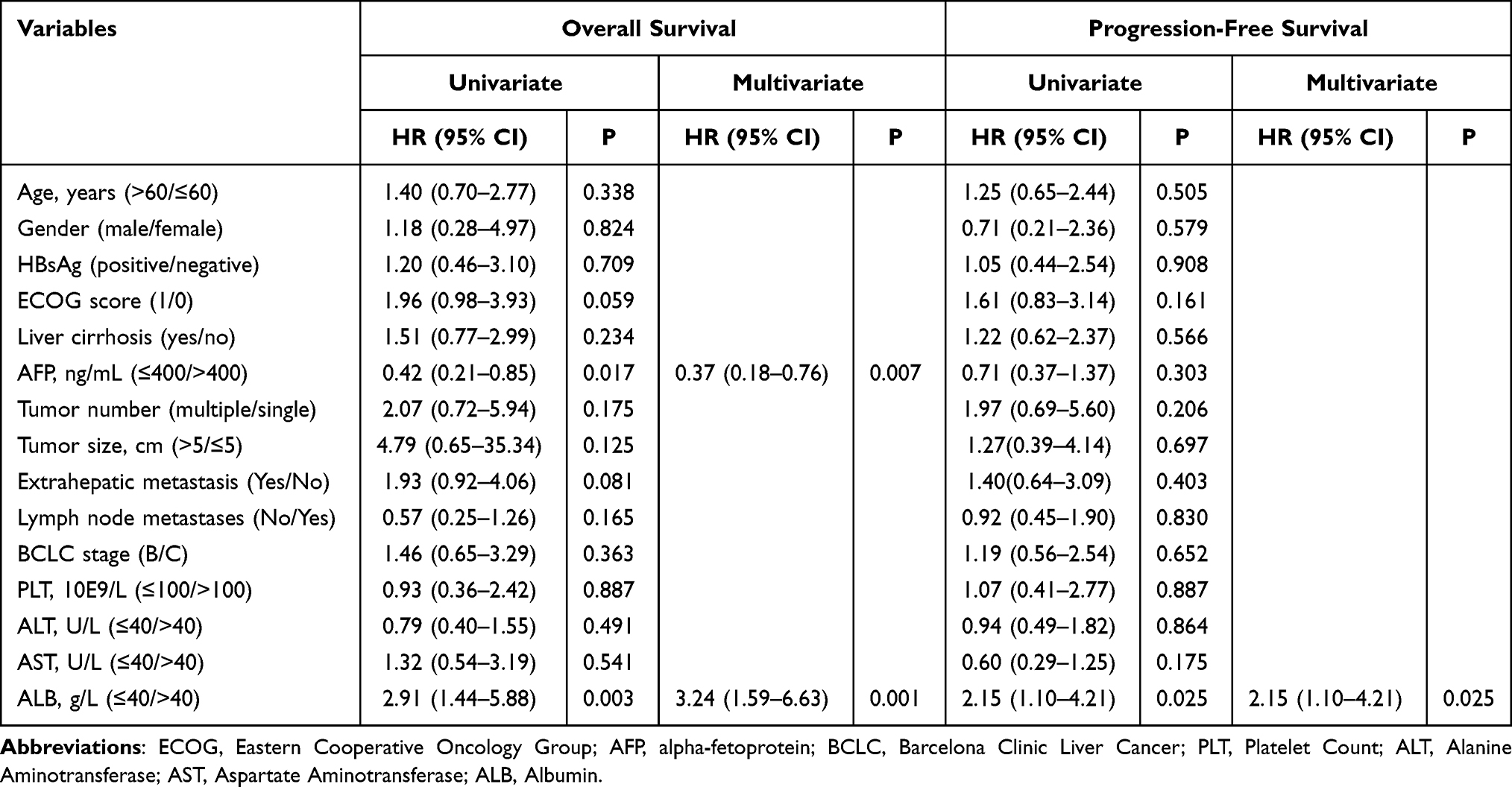 |
Table 3 Univariate and Multivariate Analyses of Prognostic Factors on OS and PFS |
Safety
All adverse events (AEs) were manageable. The most frequent treatment-related AE was abdominal pain, and the most common laboratory abnormality was a decrease in albumin. Grade ≥3 adverse events occurred in 25.8% of patients, with no treatment-related deaths observed (Table 4). The treatment-related adverse events were managed with standard supportive care, dose modification, temporary treatment interruption, or permanent discontinuation when clinically indicated.
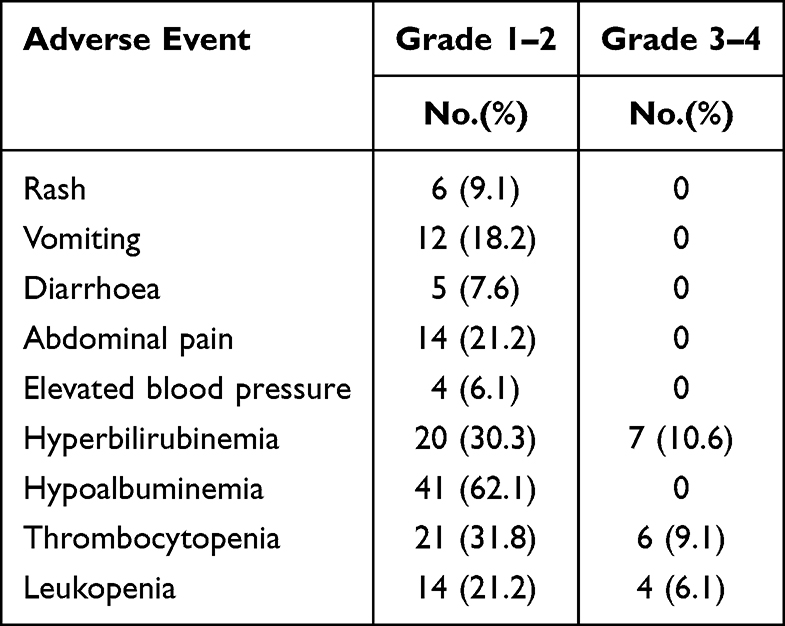 |
Table 4 Treatment-Related Adverse Events |
Discussion
In this single-arm retrospective cohort, we assessed HAIC+L+P as initial therapy for uHCC patients. The combination demonstrated encouraging antitumor activity, with a mPFS of 9.63 months and a mOS of 27.50 months. Given the relatively short median follow-up duration of 19.9 months, overall survival data should be interpreted with caution as they may not yet be fully mature.The ORR ranged from 47.0% by RECIST 1.1 to 66.7% by mRECIST, and the DCR reached 90.9%. Notably, 9.1% of patients underwent surgical resection during treatment, which may reflect the potential for selected patients to achieve sufficient disease control to allow consideration of curative-intent local therapies.
The efficacy of HAIC+L+P is biologically plausible given the complementary mechanisms of its components. HAIC enables high intrahepatic exposure to cytotoxic agents with limited systemic distribution, which may be particularly relevant in patients whose prognosis is driven by uncontrolled intrahepatic disease. Lenvatinib provides antiangiogenic and antiproliferative effects, and PD-1 blockade with pembrolizumab may restore antitumor immunity. The higher ORR assessed by mRECIST than by RECIST 1.1 is consistent with locoregional approaches that induce tumor necrosis without immediate size reduction.25
A clinically informative comparator is LEAP-012, which evaluated TACE plus lenvatinib plus pembrolizumab in unresectable, non-metastatic HCC amenable to embolization. LEAP-012 reported a longer median PFS (14.6 months) than observed in our cohort (9.63 months). LEAP-012 also achieved a higher ORR by mRECIST (71%) than our study (66.7%), while the ORR by RECIST 1.1 was identical (47% in both studies). These differences should be interpreted in light of patient selection: LEAP-012 included only non-metastatic patients and a substantial proportion of BCLC B disease, with tumors <10 cm, whereas our cohort comprised predominantly BCLC C patients (81.8%), with frequent vascular invasion (68.2%) and extrahepatic metastasis (45.5%), and a median tumor size close to 10 cm. Thus, cross-study comparisons are inherently limited, and the numerically lower PFS and mRECIST ORR in our study likely reflect a less favorable baseline profile and broader clinical heterogeneity rather than reduced activity of the systemic backbone. Notably, despite these adverse features, HAIC+L+P maintained high disease control and clinically meaningful responses, suggesting that substituting HAIC for TACE may be a potential feasible strategy for patients beyond the conventional embolization-eligible population. This hypothesis requires confirmation in prospective comparative studies.
Our findings also provide context relative to systemic therapy alone. In LEAP-002, pembrolizumab plus lenvatinib yielded a median OS of 21.2 months and a median PFS of 8.2 months, with 78% of patients classified as BCLC C.24 Although direct comparisons are not appropriate, the survival outcomes observed in our cohort support the hypothesis that adding an intrahepatic intensification component (HAIC) may be clinically relevant in advanced disease with substantial liver tumor burden.
Consistent with prior reports of HAIC-based triple therapy, our outcomes were broadly aligned with published real-world experiences.23,24,26,27 In studies combining HAIC with TKIs and immune checkpoint inhibitors, meaningful response and survival benefits have been reported, including cohorts treated with HAIC plus bevacizumab-based immunotherapy and cohorts treated with HAIC plus lenvatinib and PD-1 inhibitors. In our study, OS and PFS appeared favorable, while ORR and DCR were comparable across studies, supporting the activity of this regimen in uHCC.
The safety profile of HAIC+L+P was manageable. No toxicity-related deaths occurred, and grade ≥3 AEs were observed in 25.8% of patients, consistent with the known toxicity spectra of HAIC, lenvatinib, and PD-1 blockade. Supportive care and standard dose adjustments allowed most patients to continue treatment.
Several limitations should be noted. First, the retrospective, single-center, single-arm design and the absence of a control group limit causal interpretation and may introduce potential selection bias, therefore, the results should be interpreted as hypothesis-generating rather than confirmatory. Second, the cohort size was modest, and subsequent treatments after disease progression were heterogeneous and not standardized, which may have influenced OS. Third, tumor response assessments were performed in routine clinical practice without centralized blinded radiological review. Finally, baseline heterogeneity, including BCLC stage B/C disease, vascular invasion, and extrahepatic metastasis, may affect interpretation. Accordingly, given the retrospective design, small sample size, and heterogeneous patient population, the findings should be interpreted with caution. Further subgroup analyses stratified by disease stage and tumor burden may provide additional insights and should be explored in future studies. What’s more, these results should be confirmed in prospective, multicenter studies incorporating prespecified stratification and standardized post-treatment sequencing.
In summary, HAIC combined with lenvatinib and pembrolizumab was associated with encouraging antitumor activity and a manageable safety profile in this real-world cohort. These findings support further prospective evaluation of this regimen.
Data Sharing Statement
All data that support the findings of this study are provided within the article. Requests for additional information should be addressed to the corresponding author.
Ethics Approval
The study was performed according to the principles of the Declaration of Helsinki and was approved by the Institutional Review Board of Sun Yat-sen University Cancer Center (Approval number: B2023-673-01).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare no conflicts or competing interests related to this study.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–11. doi:10.3322/caac.21834
2. Roayaie S, Jibara G, Tabrizian P, et al. The role of hepatic resection in the treatment of hepatocellular cancer. Hepatology. 2015;62(2):440–451. doi:10.1002/hep.27745
3. Romagnoli R, Mazzaferro V, Bruix J. Surgical resection for hepatocellular carcinoma: moving from what can be done to what is worth doing. Hepatology. 2015;62(2):340–342. doi:10.1002/hep.27831
4. Zhong BY, Fan W, Guan JJ, et al. Combination locoregional and systemic therapies in hepatocellular carcinoma. Lancet Gastroenterol Hepatol. 2025;10(4):369–386. doi:10.1016/S2468-1253(24)00247-4
5. Zhu HD, Li HL, Huang MS, et al. Transarterial chemoembolization with PD-(L)1 inhibitors plus molecular targeted therapies for hepatocellular carcinoma (CHANCE001). Signal Transduct Target Ther. 2023;8(1):58. doi:10.1038/s41392-022-01235-0
6. Kudo M, Ueshima K, Saeki I, et al. A Phase 2, prospective, multicenter, single-arm trial of transarterial chemoembolization therapy in combination strategy with lenvatinib in patients with unresectable intermediate-stage hepatocellular carcinoma: TACTICS-L trial. Liver Cancer. 2024;13(1):99–112. doi:10.1159/000531377
7. Zheng Y, Xiang Y, Shi H, et al. Transarterial chemoembolization combined with atezolizumab plus bevacizumab versus transarterial chemoembolization alone in intermediate-stage hepatocellular carcinoma: a multicenter retrospective study. J Hepatocell Carcinoma. 2024;11:1079–1093. doi:10.2147/JHC.S461630
8. Kudo M, Ren Z, Guo Y, et al. Transarterial chemoembolisation combined with lenvatinib plus pembrolizumab versus dual placebo for unresectable, non-metastatic hepatocellular carcinoma (LEAP-012): a multicentre, randomised, double-blind, Phase 3 study. Lancet. 2025;405(10474):203–215. doi:10.1016/S0140-6736(24)02575-3
9. Sangro B, Kudo M, Erinjeri JP, et al. Durvalumab with or without bevacizumab with transarterial chemoembolisation in hepatocellular carcinoma (EMERALD-1): a multiregional, randomised, double-blind, placebo-controlled, phase 3 study. Lancet. 2025;405(10474):216–232. doi:10.1016/S0140-6736(24)02551-0
10. Kudo M, Finn RS, Qin S, et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: a randomised phase 3 non-inferiority trial. Lancet. 2018;391(10126):1163–1173. doi:10.1016/S0140-6736(18)30207-1
11. Qin S, Chen Z, Fang W, et al. Pembrolizumab versus placebo as second-line therapy in patients from asia with advanced hepatocellular carcinoma: a randomized, double-blind, Phase III trial. J Clin Oncol. 2023;41(7):1434–1443. doi:10.1200/JCO.22.00620
12. Kemeny N, Fata F. Hepatic-arterial chemotherapy. Lancet Oncol. 2001;2(7):418–428. doi:10.1016/S1470-2045(00)00419-8
13. Datta J, Narayan RR, Kemeny NE, et al. Role of hepatic artery infusion chemotherapy in treatment of initially unresectable colorectal liver metastases: a review. JAMA Surg. 2019;154(8):768–776. doi:10.1001/jamasurg.2019.1694
14. He MK, Le Y, Li QJ, et al. Hepatic artery infusion chemotherapy using mFOLFOX versus transarterial chemoembolization for massive unresectable hepatocellular carcinoma: a prospective non-randomized study. Chin J Cancer. 2017;36(1):83. doi:10.1186/s40880-017-0251-2
15. Li QJ, He MK, Chen HW, et al. Hepatic arterial infusion of oxaliplatin, fluorouracil, and leucovorin versus transarterial chemoembolization for large hepatocellular carcinoma: a randomized Phase III trial. J Clin Oncol. 2022;40(2):150–160. doi:10.1200/JCO.21.00608
16. He B, Deng M, Li S, et al. Transarterial chemoembolization versus hepatic arterial infusion chemotherapy as first treatment for hepatocellular carcinoma with macrovascular invasion. Int J Med Sci. 2025;22(6):1415–1424. doi:10.7150/ijms.108144
17. Deng M, Cai H, He B, et al. Hepatic arterial infusion chemotherapy versus transarterial chemoembolization, potential conversion therapies for single huge hepatocellular carcinoma: a retrospective comparison study. Int J Surg. 2023;109(11):3303–3311. doi:10.1097/JS9.0000000000000654
18. Li S, Mei J, Wang Q, et al. Transarterial infusion chemotherapy with FOLFOX for advanced hepatocellular carcinoma: a multi-center propensity score matched analysis of real-world practice. Hepatobiliary Surg Nutr. 2021;10(5):631–645. doi:10.21037/hbsn.2020.03.14
19. Guan R, Zhang N, Deng M, et al. Patients with hepatocellular carcinoma extrahepatic metastases can benefit from hepatic arterial infusion chemotherapy combined with lenvatinib plus programmed death-1 inhibitors. Int J Surg. 2024;110(7):4062–4073. doi:10.1097/JS9.0000000000001378
20. Long T, Yang Z, Zeng H, et al. Comparable clinical outcomes between transarterial chemoembolization or hepatic arterial infusion chemotherapy combined with tyrosine kinase inhibitors and PD-1 inhibitors in unresectable hepatocellular carcinoma. J Hepatocell Carcinoma. 2023;10:1849–1859. doi:10.2147/JHC.S436211
21. Ganeshan A, Upponi S, Hon LQ, et al. Hepatic arterial infusion of chemotherapy: the role of diagnostic and interventional radiology. Ann Oncol. 2008;19(5):847–851. doi:10.1093/annonc/mdm528
22. Lyu N, Wang X, Li JB, et al. Arterial chemotherapy of oxaliplatin plus fluorouracil versus sorafenib in advanced hepatocellular carcinoma: a biomolecular exploratory, randomized, Phase III trial (FOHAIC-1). J Clin Oncol. 2022;40(5):468–480. doi:10.1200/JCO.21.01963
23. He M, Xie W, Yuan Z, et al. Comparing PD-L1 and PD-1 inhibitors plus bevacizumab combined with hepatic arterial interventional therapies in unresetable hepatocellular carcinoma: a single-center, real-world study. Int J Cancer. 2025;156(10):1972–1985. doi:10.1002/ijc.35341
24. Llovet JM, Kudo M, Merle P, et al. Lenvatinib plus pembrolizumab versus lenvatinib plus placebo for advanced hepatocellular carcinoma (LEAP-002): a randomised, double-blind, Phase 3 trial. Lancet Oncol. 2023;24(12):1399–1410. doi:10.1016/S1470-2045(23)00469-2
25. Lencioni R, Llovet JM. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin Liver Dis. 2010;30(1):52–60. doi:10.1055/s-0030-1247132
26. Luo L, Xiao Y, Zhu G, et al. Hepatic arterial infusion chemotherapy combined with PD-1 inhibitors and tyrosine kinase inhibitors for unresectable hepatocellular carcinoma: a tertiary medical center experience. Front Oncol. 2022;12:1004652. doi:10.3389/fonc.2022.1004652
27. Mei J, Tang YH, Wei W, et al. Hepatic arterial infusion chemotherapy combined with PD-1 inhibitors plus lenvatinib versus PD-1 inhibitors plus lenvatinib for advanced hepatocellular carcinoma. Front Oncol. 2021;11:618206. doi:10.3389/fonc.2021.618206
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparison of the Efficacy and Safety of Transarterial Chemoembolization with or without Lenvatinib for Unresectable Hepatocellular Carcinoma: A Retrospective Propensity Score–Matched Analysis
Chen YX, Zhang JX, Zhou CG, Liu J, Liu S, Shi HB, Zu QQ
Journal of Hepatocellular Carcinoma 2022, 9:685-694
Published Date: 1 August 2022
Lenvatinib Induces Immunogenic Cell Death and Triggers Toll-Like Receptor-3/4 Ligands in Hepatocellular Carcinoma

Zhou C, Yang ZF, Sun BY, Yi Y, Wang Z, Zhou J, Fan J, Gan W, Ren N, Qiu SJ
Journal of Hepatocellular Carcinoma 2023, 10:697-712
Published Date: 24 April 2023
Application and Resistance Mechanisms of Lenvatinib in Patients with Advanced Hepatocellular Carcinoma
Tao M, Han J, Shi J, Liao H, Wen K, Wang W, Mui S, Li H, Yan Y, Xiao Z
Journal of Hepatocellular Carcinoma 2023, 10:1069-1083
Published Date: 10 July 2023
Hepatic Arterial Infusion Chemotherapy Plus Lenvatinib and Tislelizumab with or Without Transhepatic Arterial Embolization for Unresectable Hepatocellular Carcinoma with Portal Vein Tumor Thrombus and High Tumor Burden: A Multicenter Retrospective Study
Chen S, Shi F, Wu Z, Wang L, Cai H, Ma P, Zhou Y, Mai Q, Wang F, Tang S, Zhuang W, Lai J, Chen X, Chen H, Guo W
Journal of Hepatocellular Carcinoma 2023, 10:1209-1222
Published Date: 27 July 2023
Efficacy and Safety of Transarterial Chemoembolization Combined with Hepatic Arterial Infusion Chemotherapy Plus Lenvatinib for Intermediate-Stage Hepatocellular Carcinoma Beyond Up-To-Seven: A Multicentre, Retrospective Propensity Score Matching Analysis
Zhong S, Zhang F, Zhang H, Hu H, Zeng Q, Li Y, Wei Q
Journal of Hepatocellular Carcinoma 2025, 12:445-458
Published Date: 1 March 2025