")
Back to Journals » Journal of Hepatocellular Carcinoma » Volume 10
Hepatic Arterial Infusion Chemotherapy Plus Lenvatinib and Tislelizumab with or Without Transhepatic Arterial Embolization for Unresectable Hepatocellular Carcinoma with Portal Vein Tumor Thrombus and High Tumor Burden: A Multicenter Retrospective Study
Authors Chen S, Shi F, Wu Z, Wang L, Cai H, Ma P, Zhou Y, Mai Q, Wang F, Tang S, Zhuang W, Lai J, Chen X, Chen H, Guo W
Received 4 May 2023
Accepted for publication 10 July 2023
Published 27 July 2023 Volume 2023:10 Pages 1209—1222
DOI https://doi.org/10.2147/JHC.S417550
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Laura A. Dawson
Song Chen,1 Feng Shi,2 Zhiqiang Wu,3 Liguang Wang,4 Hongjie Cai,3 Ping Ma,5 Yuanmin Zhou,5 Qicong Mai,2 Fan Wang,3 Shuangyan Tang,3 Wenquan Zhuang,3 Jiaming Lai,6 Xiaoming Chen,2 Huanwei Chen,4 Wenbo Guo3
1Department of Minimally Invasive Interventional Therapy, State Key Laboratory of Oncology in South China, Collaborative Innovation Center for Cancer Medicine, Sun Yat-sen University Cancer Center, Guangzhou, People’s Republic of China; 2Department of Interventional Radiology, Guangdong Provincial People’s Hospital, Guangzhou, People’s Republic of China; 3Department of Interventional Radiology, the First Affiliated Hospital of Sun Yat-sen University, Guangzhou, People’s Republic of China; 4Department of Hepatopancreatic Surgery, the First People’s Hospital of Foshan, Foshan, People’s Republic of China; 5Department of Oncology, the Twelfth People’s Hospital of Guangzhou, Guangzhou, People’s Republic of China; 6Center of Hepato-Pancreato-Biliary Surgery, the First Affiliated Hospital of Sun Yat-sen University, Guangzhou, People’s Republic of China
Correspondence: Huanwei Chen, Department of Hepatopancreatic Surgery, the First People’s Hospital of Foshan, Foshan, People’s Republic of China, Email [email protected] Wenbo Guo, Department of Interventional Radiology, the First Affiliated Hospital of Sun Yat-sen University, Guangzhou, Guangdong, People’s Republic of China, Email [email protected]
Purpose: The current therapeutic strategies for high-risk, unresectable hepatocellular carcinoma (HCC) patients demonstrate suboptimal outcomes. This study aimed to assess the clinical efficacy of the combined approach of hepatic arterial infusion chemotherapy (HAIC), lenvatinib, and tislelizumab, either with or without transhepatic arterial embolization (TAE), in managing HCC patients with portal vein tumor thrombus (PVTT) and significant tumor load.
Patients and Methods: In this multicenter retrospective study, we analyzed patients diagnosed with primary, unresectable HCC presenting with PVTT and substantial tumor load who had undergone treatment with HAIC, lenvatinib, and tislelizumab, with or without TAE (referred to as the THLP or HLP group), between January 2019 and February 2022 across four medical centers in China. The outcomes included objective response rate (ORR), disease control rate (DCR), overall survival (OS), and progression-free survival (PFS).
Results: The study cohort comprised 100 patients, 50 each in the THLP and HLP groups. The THLP group demonstrated a significantly superior ORR (72% vs 52%, P=0.039). However, both groups exhibited comparable DCR (88% vs 76%, P=0.118), as assessed by the modified response evaluation criteria in solid tumors. The median OS and PFS for the entire cohort were 12.5 months (95% CI, 10.9– 14.8) and 5.0 months (95% CI, 4.2– 5.4), respectively. The THLP group exhibited a significantly extended OS (median, 14.1 vs 11.3 months, P=0.041) and PFS (median, 5.6 vs 4.4 months, P=0.037) in comparison to the HLP group. The most frequently reported treatment-related adverse events included abdominal pain and nausea, both reported by 59% of patients.
Conclusion: The combination of HAIC, lenvatinib, tislelizumab, and TAE was feasible in HCC patients with PVTT and high tumor burden, with tolerable safety.
Keywords: hepatocellular carcinoma, transhepatic arterial embolization, hepatic arterial infusion chemotherapy, lenvatinib, tislelizumab
Introduction
Hepatocellular carcinoma (HCC) ranks as the sixth most prevalent cancer and the third leading cause of cancer-related mortality globally.1 First-line treatments such as ablation, surgical resection, and liver transplantation are traditionally reserved for early-stage HCC.2 However, in China, an estimated 30%-62% of patients unfortunately present with portal vein tumor thrombus (PVTT), a complication associated with a bleak prognosis, limiting their treatment options.3,4 Furthermore, a high tumor burden typically predicts poor systemic therapy outcomes in HCC patients with PVTT, which results in their exclusion from some prospective clinical trials.5–7
The landscape of systemic treatment for HCC has been dramatically reshaped since the approval of the tyrosine kinase inhibitor (TKI) sorafenib in 2007, heralding a new era of therapeutic prospects.8 This shift was then followed by the approval of further first-line single-agent systemic regimes, such as lenvatinib.9 The exploration of immune checkpoint inhibitors (ICIs), particularly targeting programmed cell death 1 (PD-1), in advanced HCC paralleled this progress. The potential of ICIs to significantly increase the chance of achieving complete response (CR) in patients, as shown in the MOUSEION-03 trial, offers a promising future direction for HCC treatment.10 Phase I/II trials, such as CheckMate 040 and KEYNOTE-224, evaluated nivolumab and pembrolizumab, revealing an objective response rate (ORR) of 14–20% and a safety profile comparable to other solid tumors.11,12 Nevertheless, the efficacy of single-agent ICIs was questioned as the confirmatory Phase III trials failed to demonstrate a statistically significant improvement in overall survival (OS).
As the results of IMbrave150 were reported in 2020, atezolizumab combined with bevacizumab had replaced sorafenib and lenvatinib as the preferred first-line treatment option.13 Other clinical trials, such as ORIENT-3114 and RESCUE,15 which investigated the combination of anti-VEGF antibodies and ICIs (bevacizumab plus sintilimab and apatinib plus camrelizumab, respectively), also yielded promising results, solidifying the role of combined immunotherapies in the evolving narrative of HCC treatment. The efficacy of ICIs in combination with VEGFR antibody for the treatment of HCC has been already confirmed, but subsequent therapy after the onset of primary resistance to ICIs is often poor. Notably, it has been shown that ICIs combined with local therapy such as 90Yttrium transarterial radioembolization (90Y-TARE) may help overcome primary resistances.16 Meanwhile, debate continues around the role and risk of systemic adjuvant treatment in HCC.17 However, identifying predictive biomarkers for patients receiving ICIs remains an unresolved challenge in the field.18 Further challenges and future trends in HCC immunotherapy need to be critically addressed.19
The value of hepatic arterial infusion chemotherapy (HAIC) in the management of HCC, particularly in advanced cases and those with PVTT, is well-documented. Its recommendation as a treatment option by both Japanese and Chinese guidelines underscores its clinical importance.4,20 The FOHAIC-1 trial21 reported better survival outcomes for advanced HCC patients receiving HAIC of oxaliplatin and fluorouracil compared to sorafenib. Further, the combination of sorafenib and HAIC showed promise for HCC patients with major PVTT.22 The use of FOLFOX-HAIC demonstrated significant improvements in OS over transarterial chemoembolization (TACE) in patients with large, unresectable HCC.23 Similarly, a randomized trial24 revealed that sorafenib combined with HAIC of FOLFOX improved OS and had acceptable toxic effects compared to sorafenib alone in HCC patients with PVTT.
Recently, a promising treatment approach combining HAIC with lenvatinib and ICIs has demonstrated improved outcomes.25–28 Our prior study observed that this triple combination therapy for advanced HCC offered extended median OS (17.7 vs 12.6 months) and progression-free survival (PFS, 10.9 vs 6.8 months) compared to lenvatinib and ICIs alone.29 Notwithstanding, over 40% of patients exhibited non-responsiveness to this therapy.29
Transhepatic arterial embolization (TAE), via ischemic damage induced by blood inflow cessation, can facilitate tumor regression in up to 50% of patients.30 Furthermore, the LAUNCH clinical trial indicated superior outcomes with TACE in conjunction with lenvatinib, compared to lenvatinib alone, for advanced HCC patients.31,32 Our prior retrospective study substantiated this, revealing that TACE plus lenvatinib and ICI improved OS for advanced HCC, with acceptable toxicities.33 A recent meta-analysis studying survival outcomes for TACE and TAE found that two out of three trials leaned towards TAE, albeit with borderline significance (P=0.052).34 However, the efficacy and safety of TAE combined with the triple therapy in high-risk HCC patients remain uncharted territory. Consequently, this study aims to assess the clinical outcomes of HAIC plus lenvatinib and tislelizumab, with or without TAE, in HCC patients with PVTT and a high tumor burden.
Materials and Methods
Study Design and Patients
This retrospective cohort study evaluated patients diagnosed with unresectable HCC with PVTT and a high tumor burden. These patients received either a quadruple combination treatment (referred to as the THLP group, inclusive of TAE, HAIC, lenvatinib, and tislelizumab) or a triple combination treatment (dubbed the HLP group, comprising of HAIC, lenvatinib, and tislelizumab) from January 2019 to February 2022. The patient records were drawn from four centers across China: the First Affiliated Hospital of Sun Yat-sen University, Guangdong Provincial People’s Hospital, First People’s Hospital of Foshan, and Guangzhou No. 12 People’s Hospital.
The inclusion criteria were as follows: 1) being aged between 18 and 75 years; 2) radiological or pathological diagnosis of HCC according to the American Association for the Study of Liver Diseases practice guidelines;35 3) presence of PVTT and high tumor burden (defined as a maximum tumor diameter exceeding 10 cm) according to imaging assessments; 4) evaluation of HCC as unresectable by a multi-disciplinary team (MDT); 5) lack of prior treatment for HCC; 6) Child-Pugh classification as A or B, and an Eastern Cooperative Oncology Group Performance Status score (ECOG PS) of 0–1; 7) no presence of other malignancies within the preceding five years; 8) receipt of a minimum of two cycles of either THLP or HLP; and 9) availability of complete medical and follow-up data. Laboratory tests and imaging evaluations, including enhanced computed tomography (CT) and magnetic resonance imaging (MRI), were conducted within a week prior to the initial treatment.
This study was approved by the Ethics Committee of the First Affiliated Hospital of Sun Yat-sen University and conducted in strict accordance with the principles of the Declaration of Helsinki. The requirement for informed consent was waived by the committee because of the retrospective nature of the study. All patient-related data used in this study were de-identified and anonymized to protect privacy.
Treatment Procedures
Each treatment cycle spanned three weeks. In the HLP group, patients received HAIC treatment as previously described.29 Depending on tumor size, location, and arterial supply, the catheter tip was superselectively inserted into the femoral artery branches supplying the tumor. The HAIC regimen included oxaliplatin (130 mg/m2 from hour 0 to 2 on day 1), leucovorin (200 mg/m2 from hour 2 to 4 on day 1), and fluorouracil (400 mg/m2 as a fluorouracil bolus within 15 minutes, followed by a continuous infusion of 2400 mg/m2 of fluorouracil over 46 hours on days 1 and 2). After HAIC administration, the catheter and sheath were removed. Subsequently, all patients were given an intravenous infusion of tislelizumab once every three weeks and daily oral lenvatinib (12 mg for patients over 60 kg and 8 mg for patients under 60 kg). Decisions regarding the need for repeated TAE and/or HAIC procedures were guided by the multi-disciplinary team’s judgment.
For the THLP group, TAE using microspheres and a gelatin sponge was performed following the insertion of the catheter tip into the tumor-feeding branches of the femoral artery. The aim was not complete embolization of the tumors but to reduce the tumor burden prior to HAIC and to prevent excessive liver damage. The typical embolization endpoint was a subjective angiographic chemoembolization endpoint scale (SACE) level II, indicating a reduction in antegrade arterial flow and tumor blush.36 The procedures that followed were identical to those in the HLP group.
Adverse events (AEs) of grade 1 or 2, as defined by the National Cancer Institute Common Terminology Criteria for Adverse Events (NCI CTCAE) 5.0, were managed promptly without modifying treatment regimens. If AEs of grade 3 or higher were encountered, the regimen was adjusted slightly until the AEs resolved or improved. If these AEs persisted, treatment was halted until they resolved. The adjustments were guided by clinical judgment and an evaluation of residual lesions.
Assessment and Outcomes
Contrast-enhanced CT or MRI scans were performed every two cycles and independently reviewed by two experienced radiologists. Any discrepancies in the assessments were resolved through consensus. Treatment response was evaluated through ORR and disease control rates (DCR), as per the modified response evaluation criteria in solid tumors (mRECIST)37 and RECIST version 1.1. The ORR was characterized as the percentage of patients who achieved a CR or a partial response (PR), while DCR encompassed the percentage of patients who achieved CR, PR, or stable disease (SD). OS was the duration from admission to death from any cause, whereas PFS was the interval from admission to either disease progression or death, whichever occurred first. Recurrence-free survival (RFS) was defined as the period from hepatectomy to tumor relapse or death from any cause. AEs during treatment were recorded and classified according to the CTCAE version 5.0. Subgroup analyses of PFS and OS were conducted based on PVTT (I/II and III/IV), presence or absence of extrahepatic metastasis, and alpha-fetoprotein (AFP) levels (≥400 and <400 ng/mL).
Statistical Analysis
The R statistical software (version 4.0.3; R Foundation Inc., Vienna, Austria) and SPSS version 25.0 (SPSS, Chicago, IL, USA) were used for all statistical analyses. Continuous variables were expressed as mean ± standard deviation or median (interquartile range, IQR) and compared using the Student’s t-test or the Mann–Whitney U-test based on their distribution. Categorical variables were presented as counts and percentages, and differences between the two groups were assessed using the chi-square test or Fisher’s exact test. Time-to-event variables were analyzed using the Kaplan-Meier method, and differences were examined using the Log rank test. Univariate and multivariate Cox regression analyses were performed to identify factors associated with survival outcomes. Factors with a P<0.05 in the univariate analysis were included in the multivariate analysis. A two-sided P<0.05 was considered statistically significant.
Results
Patient Characteristics
We assessed the eligibility of 288 patients with unresectable HCC who underwent either THLP or HLP treatment. Out of these, 95 did not present with PVTT and 45 had a lesion diameter less than 10 cm. Additionally, 18 had received previous treatment for HCC and 5 had other types of malignancies. Another 5 patients were classified with Child-Pugh C or an ECOG PS score greater than 1. Twenty patients were lost to follow-up. In the end, our study included 100 patients, with 50 in each treatment group (Figure 1).
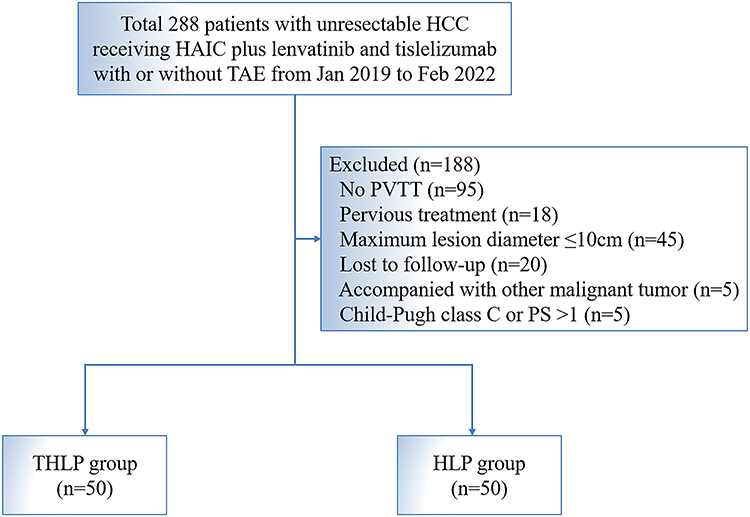 |
Figure 1 Patient flowchart. A patient might meet several exclusion criteria, but they were excluded only once from the uppermost criteria. Abbreviations: HAIC, hepatic arterial infusion chemotherapy; TAE, transhepatic arterial embolization; PVTT, portal vein tumor thrombus; THLP, TAE, HAIC, lenvatinib, and tislelizumab; HLP, HAIC, lenvatinib, and tislelizumab. |
Table 1 provides a summary of the baseline characteristics of the patients. The median age of the patients was 56 years (IQR:38–65), 55 of whom had a PVTT of grades I/II, and 68 had extrahepatic metastases. The baseline characteristics between the two groups were balanced (all P>0.05). The average diameters of tumors were 13.9±5.4 cm and 13.1±4.7 cm in the THLP and HLP groups, respectively (P=0.715). In the HLP group, the median number of HAIC treatments was 5 (range, 2–8), while in the THLP group, the median numbers for TAE and HAIC treatments were 2 (range:1–6) and 4 (range:2–8), respectively.
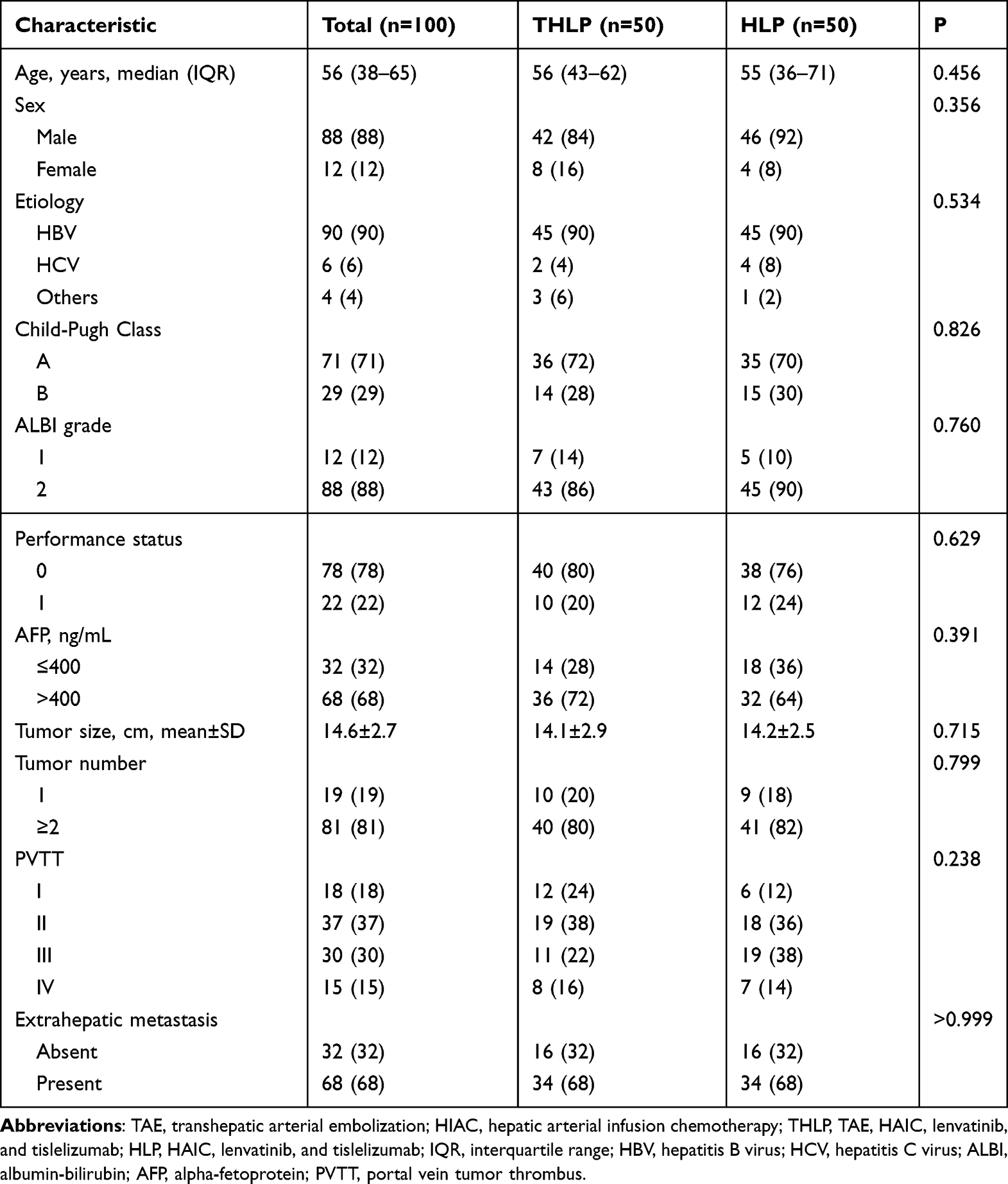 |
Table 1 Baseline Characteristics of Patients in Two Groups |
Effectiveness
The median follow-up periods were 13.8 months (range, 1.5–38.3) in the THLP group and 12.5 months (range, 1.0–21.7) in the HLP group. Based on the mRECIST criteria, the ORR and DCR were 62% and 82%, respectively. For the THLP group, the ORR was 72% per mRECIST and 60% per RECIST version 1.1, with DCR at 88% and 86% respectively. For the HLP group, ORR was 52% per mRECIST and 40% per RECIST version 1.1, with DCR at 76% and 72% respectively (Table 2).
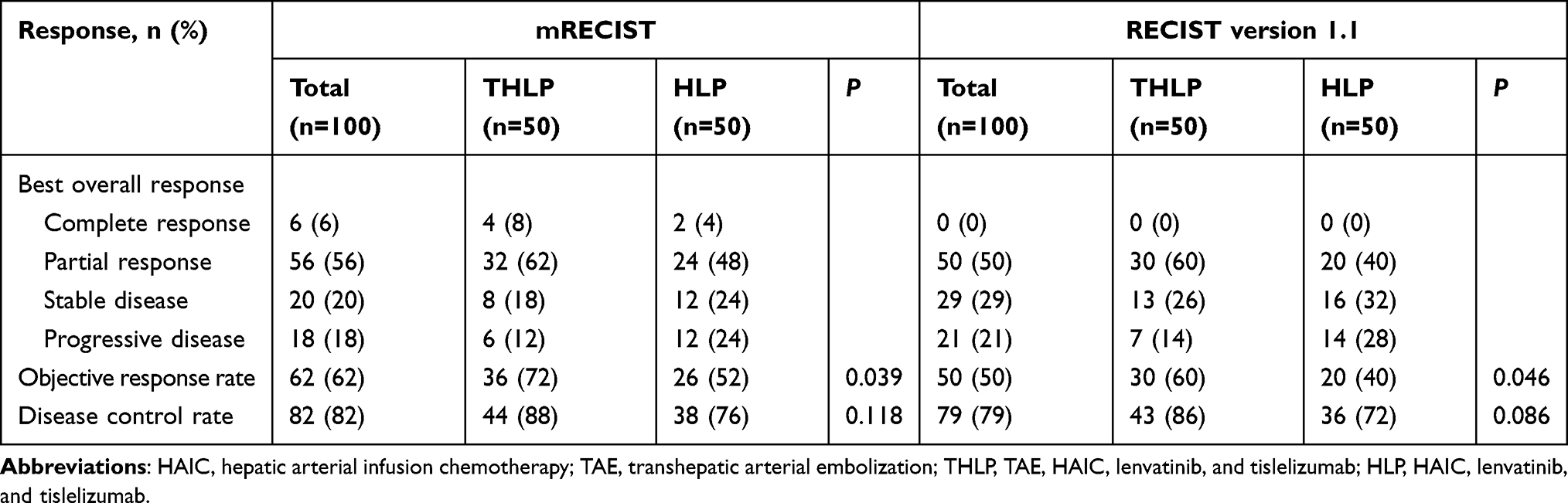 |
Table 2 Tumor Response in Two Groups |
By the end of the follow-up period, a total of 65 patients died, including 30 from the THLP group and 35 from the HLP group. For all patients, the median OS and PFS were 12.5 (95% CI, 10.9–14.8) and 5.0 (95% CI, 4.2–5.4) months respectively (Figure 2A and B). The THLP group exhibited extended OS (median 14.1 [95% CI, 11.9–24.4] vs 11.3 [95% CI, 8.7–13.9] months; hazard ratio [HR]=0.61, 95% CI, 0.38–1.00, P=0.041) and PFS (median 5.6 [95% CI, 4.6–8.3] vs 4.4 [95% CI, 3.9–5.3] months; HR=0.65, 95% CI, 0.42–1.00, P=0.037) (Figure 2C and D).
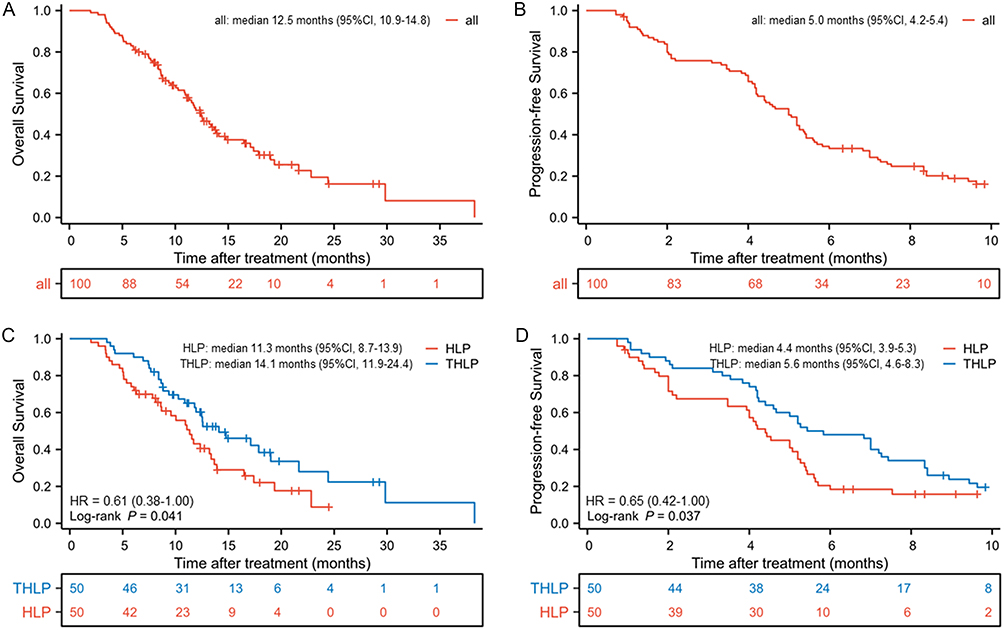 |
Figure 2 Kaplan-Meier curves of (A) overall survival in all patients; (B) progression-free survival in all patients (C) overall survival in two groups; and (D) progression-free survival in two groups. Abbreviations: HR, hazard ratio; CI, confidence interval; HAIC, hepatic arterial infusion chemotherapy; TAE, transhepatic arterial embolization; THLP, TAE, HAIC, lenvatinib, and tislelizumab; HLP, HAIC, lenvatinib, and tislelizumab. |
Eighteen patients met the standard for conversion to resectable HCC, with 11 from the THLP group and 7 from the HLP group (P=0.436). The median interval between initial treatment and surgical resection was 2.5 months (range, 0.7–6.1) for the THLP group and 3.8 months (range, 1.4–7.9) for the HLP group (P=0.029). Post-surgery, all patients continued lenvatinib plus tislelizumab therapy. Following a median post-surgery follow-up period of 9.7 months (range, 3.8–15.9), 10 patients (7 in the THLP group, 3 in the HLP group) had a recurrence, and 6 patients (4 in the THLP group, 2 in the HLP group) died. The median RFS was 9.8 months (95% CI, 4.6–15.3 months), whereas the median OS was not reached (95% CI, 8.4 months-not evaluated).
Subgroup Analysis
The THLP group demonstrated a numerically superior median OS compared to the HLP group across various patient cohorts. These included those with PVTT I/II (19.0 vs 13.9 months), PVTT III/IV (9.4 vs 6.1 months), absence of extrahepatic metastasis (17.1 vs 13.2 months), presence of extrahepatic metastasis (8.6 vs 5.7 months), and AFP levels either ≥400 ng/mL (12.5 vs 10.0 months) or <400 ng/mL (21.7 vs 11.7 months) (Figure 3). Patients in the THLP group who were negative for hepatitis B virus (HBV), had a Child-Pugh score of B, an albumin-bilirubin (ALBI) grade of 1 or 2, an ECOG PS of 0, a maximum tumor diameter of ≤15 cm, more than one tumor, and extrahepatic metastasis also demonstrated superior OS (all P<0.05) (Figure S1). PFS results for these subgroups are illustrated in Figure 4.
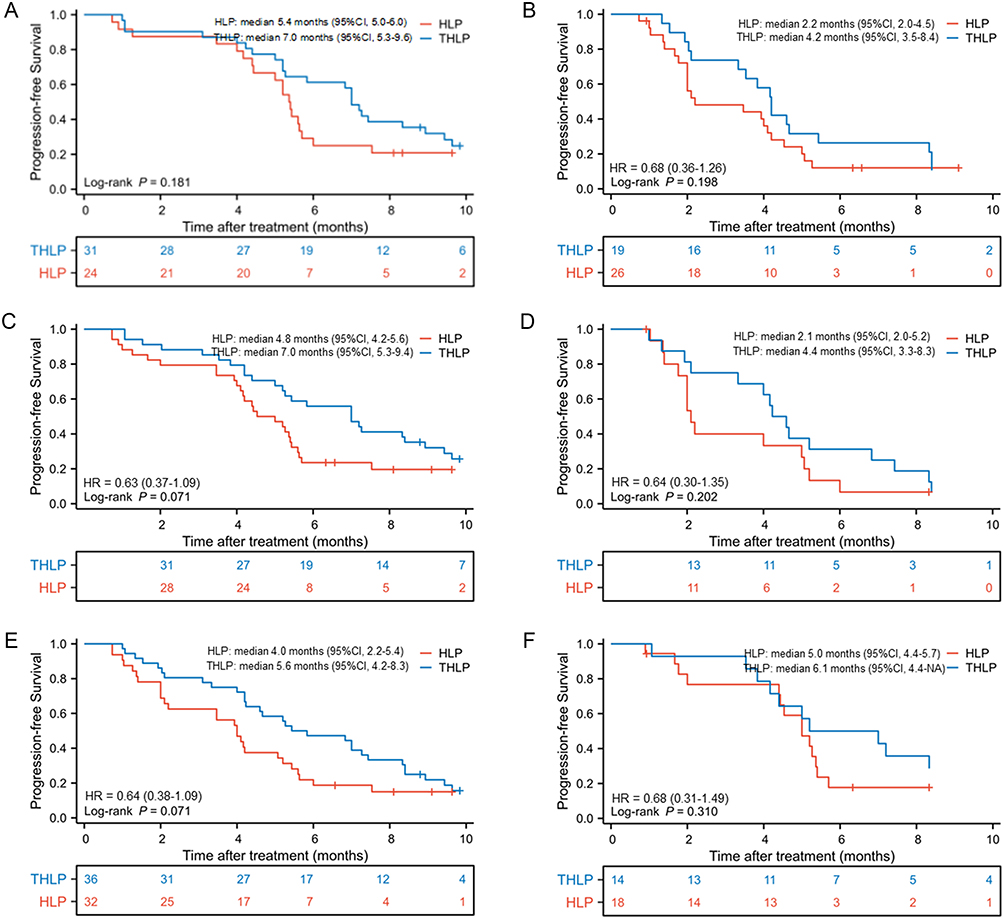 |
Figure 3 Kaplan-Meier curves of overall survival between two groups in patients (A) with PVTT I/II; (B) with PVTT III/IV; (C) without extrahepatic metastasis; (D) with extrahepatic metastasis; (E) with AFP ≥400 ng/mL and (F) with AFP <400 ng/mL. Abbreviations: HR, hazard ratio; CI, confidence interval; NA, not available; HAIC, hepatic arterial infusion chemotherapy; TAE, transhepatic arterial embolization; THLP, TAE, HAIC, lenvatinib, and tislelizumab; HLP, HAIC, lenvatinib, and tislelizumab; PVTT, portal vein tumor thrombus; AFP, alpha-fetoprotein. |
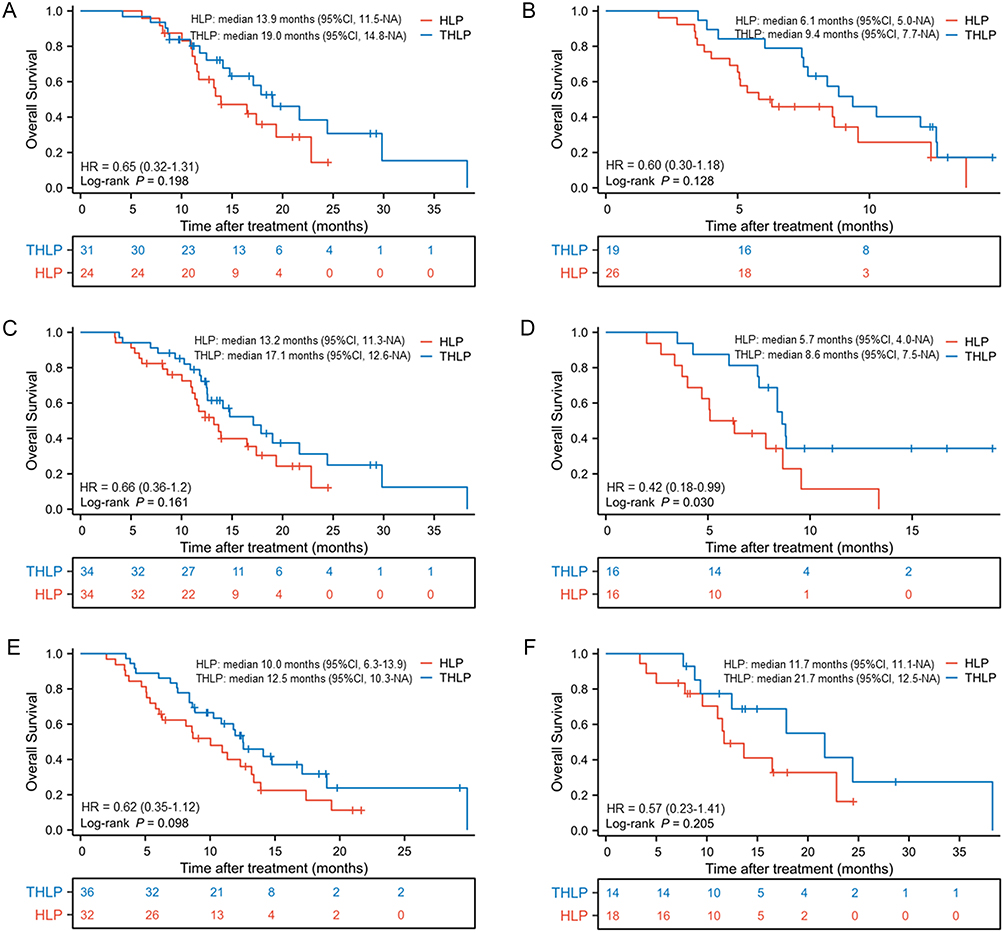 |
Figure 4 Kaplan-Meier curves of progression-free survival between two groups in patients (A) with PVTT I/II; (B) with PVTT III/IV; (C) without extrahepatic metastasis; (D) with extrahepatic metastasis; (E) with AFP >400 ng/mL and (F) with AFP ≤400 ng/mL. Abbreviations: HR, hazard ratio; CI, confidence interval; NA, not available; HAIC, hepatic arterial infusion chemotherapy; TAE, transhepatic arterial embolization; THLP, TAE, HAIC, lenvatinib, and tislelizumab; HLP, HAIC, lenvatinib, and tislelizumab; PVTT, portal vein tumor thrombus; AFP, alpha-fetoprotein. |
Univariate and Multivariate Analysis for Survival
After adjusting for potential confounders, several factors were associated with improved OS, including membership in the THLP group (HR, 0.51; 95% CI, 0.31–0.85, P=0.01), PVTT I/II status (HR, 0.25, 95% CI, 0.13–0.48, P<0.001), and absence of extrahepatic metastasis (HR, 0.34; 95% CI, 0.20–0.69, P=0.002). Similarly, the same factors (THLP group [HR, 0.62, 95% CI, 0.40–0.97, P=0.038], PVTT I/II [HR, 0.51, 95% CI, 0.32–0.81, P=0.004], and no extrahepatic metastasis [HR, 0.57, 95% CI, 0.35–0.92, P=0.021]) served as independent protective factors for PFS (Table 3).
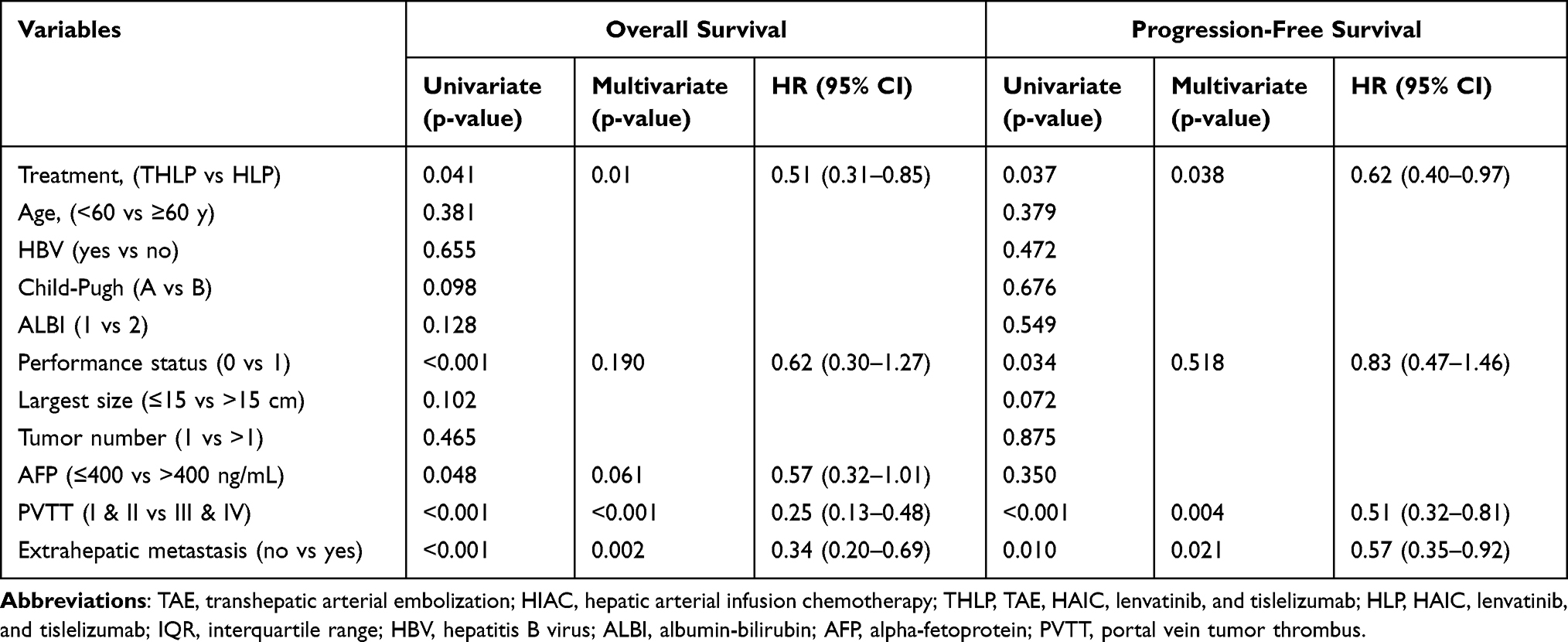 |
Table 3 Univariate and Multivariate Analysis of Risk Factors for Overall Survival and Progression-Free Survival |
Safety
Treatment-related AEs (TRAEs) are detailed in Table 4. The most frequently reported TRAEs included abdominal pain, nausea, and increased aminotransferase levels, with the majority being grade 1 or 2. Grade 3 or 4 TRAEs, such as abdominal pain, nausea, and increased aminotransferase levels, were more prevalent in the THLP group compared to the HLP group (34% vs 18%, 36% vs 22%, and 10% vs 2%, respectively). However, these AEs were manageable and did not lead to any treatment-related deaths. No significant differences were observed between the two groups in terms of albumin, bilirubin, and aminotransferase levels.
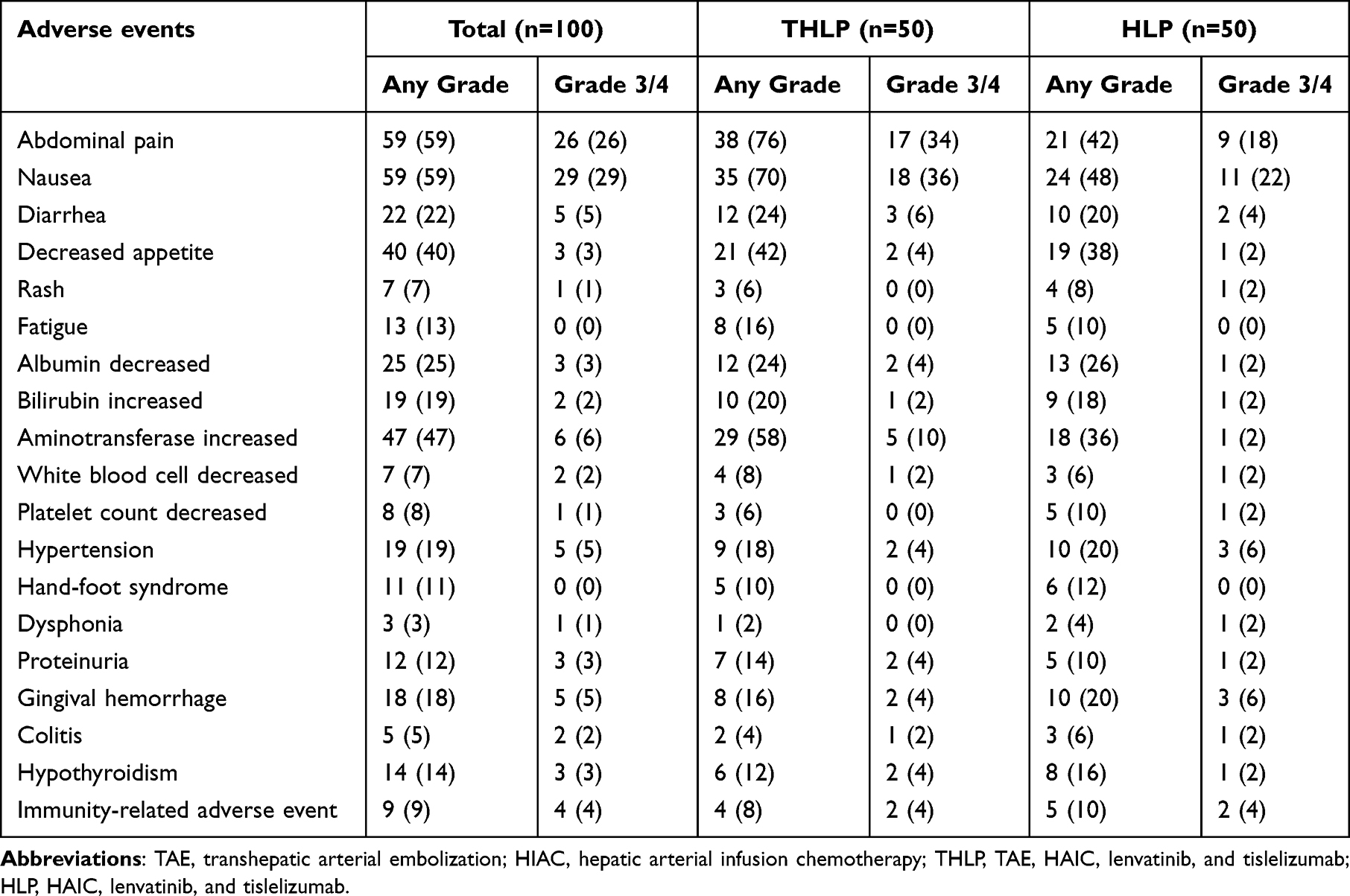 |
Table 4 Treatment-Related Adverse Events |
Discussion
At the inception of this study, lenvatinib combined with ICIs had emerged as a potential systemic therapy for unresectable HCC.38 A fusion of locoregional and systemic therapies is frequently utilized in clinical practice, given their efficacy in tumor control.39 Several retrospective studies have reported prolonged OS and PFS with the combination of HAIC-FOLFOX, lenvatinib, and ICIs, as compared to either lenvatinib plus ICIs or lenvatinib alone.25–27,29 Within the scope of our study, we retrospectively evaluated the clinical outcomes of adding TAE to HAIC, lenvatinib, and tislelizumab in patients with unresectable HCC. The ORRs were 72% and 52% in the THLP and HLP groups, respectively, as per mRECIST. Furthermore, the THLP group demonstrated significantly longer OS and PFS. Quadruple combination therapy (THLP group) was identified as an independent predictor of an improved prognosis. The toxicity of the combination therapy was typically manageable. Collectively, these findings suggest that supplementing TAE to a regimen of HAIC, lenvatinib, and tislelizumab may offer additional clinical benefits to patients with unresectable HCC and PVTT, particularly those with a high tumor burden, while maintaining an acceptable safety profile.
High tumor burden and PVTT are recognized as factors correlating with adverse outcomes in HCC patients.4,5 The post-hoc analysis of the IMbrave 150 study indicated that the median OS was similar between the atezolizumab plus bevacizumab group (7.6 months) and the sorafenib group (5.5 months) among high-risk patients, suggesting that systematic therapy provides limited benefits for high-risk HCC patients.5 In contrast, our study demonstrated a median OS of 12.5 months in all patients, with 14.1 months in the THLP group, and 11.3 months in the HLP group. These figures surpass the median OS in high-risk patients who received either atezolizumab plus bevacizumab or sorafenib. This could potentially be attributed to the synergistic impact of locoregional therapies, such as TACE and HAIC, combined with systemic therapies, like anti-angiogenic agents and ICIs.40–44
In our investigation, quadruple combination therapy comprising of TAE, HAIC, lenvatinib, and tislelizumab demonstrated superior ORR (72% vs 52%), median PFS (5.6 vs 4.4 months), and median OS (14.1 vs 11.3 months) compared to the triple combination therapy of HAIC, lenvatinib, and tislelizumab. Numerous studies underscore the significance of embolization as a foundation and central aspect of combination therapy for high burden tumors.45,46 HAIC, when coupled with chemoembolization, has been found to be more effective than chemoembolization alone in patients with unresectable HCC.45 Additionally, a retrospective study illustrated that combining HAIC with TAE enhanced PFS in patients with unresectable HCC compared to TACE alone, particularly for those at BCLC stage C.46 Considering these findings, merging TAE with HAIC and systemic treatment could yield further benefits than HAIC and systemic treatment alone. Moreover, 18 patients in our study reached the criteria for conversion to resectable HCC post-treatment, hinting that combination therapy may open more avenues for patients to undergo radical treatment.47
In our subgroup analysis of OS, the THLP regimen appeared to benefit most patient cohorts, with the exceptions being those with solitary tumors or a maximum lesion diameter exceeding 15 cm. Previous research suggests that for solitary lesions, HAIC alone might provide sufficient efficacy, rendering the addition of TAE unnecessary.23 For larger tumors, TAE may be unsuitable and lead to over-embolization, escalating liver toxicity and the expression of angiogenic growth factors.48–51 Nevertheless, the absence of a significant difference could be attributed to our limited sample size, necessitating further validation. The multivariate Cox regression analysis identified the treatment group, PVTT grade, and the presence of extrahepatic metastases as independent variables associated with both OS and PFS. As expected, extrahepatic metastases and type III/IV PVTT negatively impacted survival, while THLP emerged as an independent protective factor for both OS and PFS, thereby endorsing the benefits of integrating TAE with HLP.
Our study linked the THLP regimen to a higher incidence of grade ≥3 or total grade AEs compared to the HLP regimen. Post-embolization syndrome and liver damage were commonly observed AEs in the THLP group due to TAE. Consistent with prior studies, abdominal pain, which could be managed with standard therapies, was a frequently reported symptom.52 The primary concern was liver function damage induced by TAE, as previously documented, which could negatively influence patients’ final outcomes.53,54 Consequently, partial rather than complete embolization was performed for TAE in the THLP group. Our study also identified THLP as a factor contributing to more pronounced liver function impairment, particularly in cases of acute liver injury, such as elevated aminotransferase levels. However, these AEs were transient, with aminotransferase levels returning to normal within a relatively short timeframe. This did not impede subsequent treatment nor lead to liver failure. While THLP generally presents a safe treatment option for HCC patients with a high tumor burden, the degree of embolization should be carefully considered.
In the context of our findings, we acknowledge the ongoing exploration in the field of combination treatments for HCC. In particular, a prospective clinical study of lenvatinib combined with a PD-1 inhibitor and HAIC has provided encouraging results.28 Similarly, the CHANCE 001 study demonstrated promising clinical efficacy of TACE combined with TKIs and ICIs in intermediate to advanced HCC.55 However, to our knowledge, no prospective clinical studies have investigated the quadruple combination regimen of TAE with HAIC, TKIs, and PD-1 inhibitors. Our study presents initial retrospective data showing that this approach might improve survival in advanced HCC patients with high tumor burden and PVTT. Looking ahead, we see a compelling opportunity for future clinical trials to validate the clinical efficacy and safety of such quadruple combination regimens. Furthermore, comparative trials against established triple combination therapies could provide additional insights into the optimal combination treatment strategy for this patient population. These efforts will further enhance our understanding of how to leverage multiple therapeutic modalities in the quest for improved patient outcomes in HCC.
This study had several limitations. Firstly, our study was retrospective in nature which might introduce inherent bias associated with retrospective analyses. Secondly, the sample size of our study, while multicentric, was relatively small which might limit the power of statistical analyses and the generalizability of our findings. Thirdly, our study population was considerably diverse, including patients with different stages of disease and varying clinical presentations. This heterogeneity could impact the interpretation of our results and their applicability to a more uniform patient population. Lastly, despite efforts to maintain standardization, the application of TAE varied among different centers due to its technical complexity. This variation could potentially influence the outcomes due to different degrees of embolization.
Conclusions
Based on the data from this retrospective study, the combination of HAIC, lenvatinib, tislelizumab, and TAE appears to show promise in improving survival for HCC patients with PVTT and high tumor burden. While these results are encouraging, they should be interpreted with caution given the potential for bias inherent in retrospective studies. Further prospective, randomized controlled trials are needed to validate these findings.
Abbreviations
HCC, hepatocellular carcinoma; PVTT, portal vein tumor thrombus; TKIs, tyrosine kinase inhibitors; ICIs, immune checkpoint inhibitors; HAIC, hepatic arterial infusion chemotherapy; FOLFOX, oxaliplatin, 5-fluorouracil, and leucovorin; OS, overall survival; PFS, progression-free survival; TACE, transhepatic arterial chemoembolization; TAE, transhepatic arterial embolization; THLP, TAE, HAIC, lenvatinib and tislelizumab; HLP, HAIC, lenvatinib and tislelizumab; MDT, multi-disciplinary team; ECOG PS, Eastern Cooperative Oncology Group Performance Status score; CT, computed tomography; MRI, magnetic resonance imaging; SACE, subjective angiographic chemoembolization endpoint scale; AEs, adverse events; NCI CTCAE, National Cancer Institute Common Terminology Criteria for Adverse Events; ORR, overall response rates; DCR, disease control rates; mRECIST, modified response evaluation criteria in solid tumors; CR, complete response; PR, partial response; SD, stable disease; RFS, recurrence-free survival; HR, hazard ratio; AFP, alpha-fetoprotein; HBV, hepatitis B virus; ALBI, albumin-bilirubin; TRAEs, treatment-related AEs.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
This study was approved by the Ethics Committee of the First Affiliated Hospital of Sun Yat-sen University and conducted in strict accordance with the principles of the Declaration of Helsinki. The requirement for informed consent was waived by the committee because of the retrospective nature of the study. All patient-related data used in this study were de-identified and anonymized to protect privacy.
Acknowledgment
The abstract of this paper was presented at the 2022 ESMO Immuno-Oncology Congress as a poster presentation with interim findings. The poster’s abstract was published in “Poster Abstracts” in Annals of Oncology (2022) 16 (suppl_1): 100102-100102 name “88P-Hepatic arterial infusion chemotherapy (HAIC)+lenvatinib (len) and tislelizumab (tis)±transhepatic arterial embolization (TAE) for unresectable hepatocellular carcinoma (uHCC) with portal vein tumor thrombus (PVTT) and high tumor burden: A multicenter retrospective study”. DOI: 10.1016/iotech/iotech 100102.
Funding
This research received no external funding.
Disclosure
All authors have no conflicts of interest to declare.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021;71(3):209–249.
2. Benson AB, D’Angelica MI, Abbott DE, et al. Guidelines Insights: hepatobiliary Cancers, Version 2.2019. J Natl Compr Canc Netw. 2019;17(4):302–310.
3. Yang B, Li CL, Guo WH, et al. Intra-arterial ethanol embolization augments response to TACE for treatment of HCC with portal venous tumor thrombus. BMC Cancer. 2018;18(1):101.
4. Kudo M, Kawamura Y, Hasegawa K, et al. Management of Hepatocellular Carcinoma in Japan: JSH Consensus Statements and Recommendations 2021 Update. Liver Cancer. 2021;10(3):181–223.
5. Breder VV, Vogel A, Merle P, et al. IMbrave150: exploratory efficacy and safety results of hepatocellular carcinoma (HCC) patients (pts) with main trunk and/or contralateral portal vein invasion (Vp4) treated with atezolizumab (atezo) + bevacizumab (bev) versus sorafenib (sor) in a global Ph III study. J Clin Oncol. 2021;39(15_suppl):4073.
6. Tsuchiya K, Kurosaki M, Marusawa H, et al. The efficacy and safety of lenvatinib in patients who did not meet the inclusion criteria of the Phase 3 trial (REFLECT trial) in real-world practice in Japan: a nationwide multicenter study in Japan. J Clin Oncol. 2019;37(15_suppl):e15629–e15629.
7. Cheng AL, Kang YK, Chen Z, et al. Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: a phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2009;10(1):25–34.
8. Llovet JM, Ricci S, Mazzaferro V, et al. Sorafenib in advanced hepatocellular carcinoma. N Engl J Med. 2008;359(4):378–390.
9. Kudo M, Finn RS, Qin S, et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: a randomised phase 3 non-inferiority trial. Lancet. 2018;391(10126):1163–1173.
10. Santoni M, Rizzo A, Kucharz J, et al. Complete remissions following immunotherapy or immuno-oncology combinations in cancer patients: the MOUSEION-03 meta-analysis. Cancer Immunol Immunother. 2023;72(6):1365–1379.
11. El-Khoueiry AB, Sangro B, Yau T, et al. Nivolumab in patients with advanced hepatocellular carcinoma (CheckMate 040): an open-label, non-comparative, Phase 1/2 dose escalation and expansion trial. Lancet. 2017;389(10088):2492–2502.
12. Zhu AX, Finn RS, Edeline J, et al. Pembrolizumab in patients with advanced hepatocellular carcinoma previously treated with sorafenib (KEYNOTE-224): a non-randomised, open-label Phase 2 trial. Lancet Oncol. 2018;19(7):940–952.
13. Finn RS, Qin S, Ikeda M, et al. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N Engl J Med. 2020;382(20):1894–1905.
14. Lu S, Wu L, Jian H, et al. Sintilimab plus bevacizumab biosimilar IBI305 and chemotherapy for patients with EGFR-mutated non-squamous non-small-cell lung cancer who progressed on EGFR tyrosine-kinase inhibitor therapy (ORIENT-31): first interim results from a randomised, double-blind, multicentre, phase 3 trial. Lancet Oncol. 2022;23(9):1167–1179.
15. Xu J, Shen J, Gu S, et al. Camrelizumab in Combination with Apatinib in Patients with Advanced Hepatocellular Carcinoma (RESCUE): a Nonrandomized, Open-label, Phase II Trial. Clin Cancer Res. 2021;27(4):1003–1011.
16. Di Federico A, Rizzo A, Carloni R, et al. Atezolizumab-bevacizumab plus Y-90 TARE for the treatment of hepatocellular carcinoma: preclinical rationale and ongoing clinical trials. Expert Opin Investig Drugs. 2022;31(4):361–369.
17. Rizzo A, Ricci AD, Brandi G. Systemic adjuvant treatment in hepatocellular carcinoma: tempted to do something rather than nothing. Future Oncol. 2020;16(32):2587–2589.
18. Rizzo A, Cusmai A, Gadaleta-Caldarola G, Palmiotti G. Which role for predictors of response to immune checkpoint inhibitors in hepatocellular carcinoma? Expert Rev Gastroenterol Hepatol. 2022;16(4):333–339.
19. Rizzo A, Ricci AD. Challenges and Future Trends of Hepatocellular Carcinoma Immunotherapy. Int J Mol Sci. 2022;23(19):45.
20. Xie DY, Ren ZG, Zhou J, Fan J, Gao Q. 2019 Chinese clinical guidelines for the management of hepatocellular carcinoma: updates and insights. Hepatobiliary Surg Nutr. 2020;9(4):452–463.
21. Lyu N, Wang X, Li JB, et al. Arterial Chemotherapy of Oxaliplatin Plus Fluorouracil Versus Sorafenib in Advanced Hepatocellular Carcinoma: a Biomolecular Exploratory, Randomized, Phase III Trial (FOHAIC-1). J Clin Oncol. 2022;40(5):468–480.
22. Zheng K, Zhu X, Fu S, et al. Sorafenib Plus Hepatic Arterial Infusion Chemotherapy versus Sorafenib for Hepatocellular Carcinoma with Major Portal Vein Tumor Thrombosis: a Randomized Trial. Radiology. 2022;303(2):455–464.
23. Li QJ, He MK, Chen HW, et al. Hepatic Arterial Infusion of Oxaliplatin, Fluorouracil, and Leucovorin Versus Transarterial Chemoembolization for Large Hepatocellular Carcinoma: a Randomized Phase III Trial. J Clin Oncol. 2022;40(2):150–160.
24. He M, Li Q, Zou R, et al. Sorafenib Plus Hepatic Arterial Infusion of Oxaliplatin, Fluorouracil, and Leucovorin vs Sorafenib Alone for Hepatocellular Carcinoma With Portal Vein Invasion: a Randomized Clinical Trial. JAMA Oncol. 2019;5(7):953–960.
25. He MK, Liang RB, Zhao Y, et al. Lenvatinib, toripalimab, plus hepatic arterial infusion chemotherapy versus lenvatinib alone for advanced hepatocellular carcinoma. Ther Adv Med Oncol. 2021;13:17588359211002720.
26. Mei J, Tang YH, Wei W, et al. Hepatic Arterial Infusion Chemotherapy Combined With PD-1 Inhibitors Plus Lenvatinib Versus PD-1 Inhibitors Plus Lenvatinib for Advanced Hepatocellular Carcinoma. Front Oncol. 2021;11:618206.
27. Liu BJ, Gao S, Zhu X, et al. Real-world study of hepatic artery infusion chemotherapy combined with anti-PD-1 immunotherapy and tyrosine kinase inhibitors for advanced hepatocellular carcinoma. Immunotherapy. 2021;13(17):1395–1405.
28. Lai Z, He M, Bu X, et al. Lenvatinib, toripalimab plus hepatic arterial infusion chemotherapy in patients with high-risk advanced hepatocellular carcinoma: a biomolecular exploratory, phase II trial. Eur J Cancer. 2022;174:68–77.
29. Chen S, Xu B, Wu Z, et al. Pembrolizumab plus lenvatinib with or without hepatic arterial infusion chemotherapy in selected populations of patients with treatment-naive unresectable hepatocellular carcinoma exhibiting PD-L1 staining: a multicenter retrospective study. BMC Cancer. 2021;21(1):1126.
30. Forner A, Gilabert M, Bruix J, Raoul JL. Treatment of intermediate-stage hepatocellular carcinoma. Nat Rev Clin Oncol. 2014;11(9):525–535.
31. Peng Z, Fan W, Zhu B, et al. Lenvatinib Combined With Transarterial Chemoembolization as First-Line Treatment for Advanced Hepatocellular Carcinoma: a Phase III, Randomized Clinical Trial (LAUNCH). J Clin Oncol. 2023;41(1):117–127.
32. Fu Z, Li X, Zhong J, et al. Lenvatinib in combination with transarterial chemoembolization for treatment of unresectable hepatocellular carcinoma (uHCC): a retrospective controlled study. Hepatol Int. 2021;15(3):663–675.
33. Chen S, Wu Z, Shi F, et al. Lenvatinib plus TACE with or without pembrolizumab for the treatment of initially unresectable hepatocellular carcinoma harbouring PD-L1 expression: a retrospective study. J Cancer Res Clin Oncol. 2022;148(8):2115–2125.
34. Marelli L, Stigliano R, Triantos C, et al. Transarterial therapy for hepatocellular carcinoma: which technique is more effective? A systematic review of cohort and randomized studies. Cardiovasc Intervent Radiol. 2007;30(1):6–25.
35. Heimbach JK, Kulik LM, Finn RS, et al. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology. 2018;67(1):358–380.
36. Lewandowski RJ, Wang D, Gehl J, et al. A comparison of chemoembolization endpoints using angiographic versus transcatheter intraarterial perfusion/MR imaging monitoring. J Vasc Interv Radiol. 2007;18(10):1249–1257.
37. Lencioni R, Llovet JM. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin Liver Dis. 2010;30(1):52–60.
38. Finn RS, Ikeda M, Zhu AX, et al. Phase Ib Study of Lenvatinib Plus Pembrolizumab in Patients With Unresectable Hepatocellular Carcinoma. J Clin Oncol. 2020;38(26):2960–2970.
39. Palmer DH, Malagari K, Kulik LM. Role of locoregional therapies in the wake of systemic therapy. J Hepatol. 2020;72(2):277–287.
40. Pinato DJ, Murray SM, Forner A, et al. Trans-arterial chemoembolization as a loco-regional inducer of immunogenic cell death in hepatocellular carcinoma: implications for immunotherapy. J Immunother Cancer. 2021;9(9):76.
41. Zhu H, Shan Y, Ge K, Lu J, Kong W, Jia C. Oxaliplatin induces immunogenic cell death in hepatocellular carcinoma cells and synergizes with immune checkpoint blockade therapy. Cell Oncol. 2020;43(6):1203–1214.
42. Yamamoto Y, Matsui J, Matsushima T, et al. Lenvatinib, an angiogenesis inhibitor targeting VEGFR/FGFR, shows broad antitumor activity in human tumor xenograft models associated with microvessel density and pericyte coverage. Vasc Cell. 2014;6:18.
43. Deng H, Kan A, Lyu N, et al. Dual Vascular Endothelial Growth Factor Receptor and Fibroblast Growth Factor Receptor Inhibition Elicits Antitumor Immunity and Enhances Programmed Cell Death-1 Checkpoint Blockade in Hepatocellular Carcinoma. Liver Cancer. 2020;9(3):338–357.
44. Chung AS, Lee J, Ferrara N. Targeting the tumour vasculature: insights from physiological angiogenesis. Nat Rev Cancer. 2010;10(7):505–514.
45. Gao S, Zhang PJ, Guo JH, et al. Chemoembolization alone vs combined chemoembolization and hepatic arterial infusion chemotherapy in inoperable hepatocellular carcinoma patients. World J Gastroenterol. 2015;21(36):10443–10452.
46. Guo W, Gao J, Zhuang W, Wu Z, Li B, Chen S. Efficacy and safety of hepatic arterial infusion chemotherapy combined with transarterial embolization for unresectable hepatocellular carcinoma: a propensity score-matching cohort study. JGH Open. 2020;4(3):477–483.
47. Song T, Lang M, Ren S, Gan L, Lu W. The past, present and future of conversion therapy for liver cancer. Am J Cancer Res. 2021;11(10):4711–4724.
48. Geschwind JF, Ramsey DE, Cleffken B, et al. Transcatheter arterial chemoembolization of liver tumors: effects of embolization protocol on injectable volume of chemotherapy and subsequent arterial patency. Cardiovasc Intervent Radiol. 2003;26(2):111–117.
49. Kobayashi N, Ishii M, Ueno Y, et al. Co-expression of Bcl-2 protein and vascular endothelial growth factor in hepatocellular carcinomas treated by chemoembolization. Liver. 1999;19(1):25–31.
50. Xiong ZP, Yang SR, Liang ZY, et al. Association between vascular endothelial growth factor and metastasis after transcatheter arterial chemoembolization in patients with hepatocellular carcinoma. Hepatobiliary Pancreat Dis Int. 2004;3(3):386–390.
51. Rhee TK, Young JY, Larson AC, et al. Effect of transcatheter arterial embolization on levels of hypoxia-inducible factor-1alpha in rabbit VX2 liver tumors. J Vasc Interv Radiol. 2007;18(5):639–645.
52. Wu Z, Guo W, Chen S, Zhuang W. Determinants of pain in advanced HCC patients recieving hepatic artery infusion chemotherapy. Invest New Drugs. 2021;39(2):394–399.
53. Kudo M, Han KH, Ye SL, et al. A Changing Paradigm for the Treatment of Intermediate-Stage Hepatocellular Carcinoma: Asia-Pacific Primary Liver Cancer Expert Consensus Statements. Liver Cancer. 2020;9(3):245–260.
54. Galle PR, Tovoli F, Foerster F, Wörns MA, Cucchetti A, Bolondi L. The treatment of intermediate stage tumours beyond TACE: from surgery to systemic therapy. J Hepatol. 2017;67(1):173–183.
55. Zhu HD, Li HL, Huang MS, et al. Transarterial chemoembolization with PD-(L)1 inhibitors plus molecular targeted therapies for hepatocellular carcinoma (CHANCE001). Signal Transduct Target Ther. 2023;8(1):58.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.