Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Group B Streptococcus Colonization Among Pregnant Women in Jordan: Prevalence, Outcomes and a Comparison Between Healthcare and Non- Healthcare Providers
Authors Altal O, Hulliel A, Abubaker B, Alshaykh R ![]() , Almasaeid S, Dabash T, Abuzraiq R, Darawsheh B, Al Othman O
, Almasaeid S, Dabash T, Abuzraiq R, Darawsheh B, Al Othman O
Received 10 November 2025
Accepted for publication 30 January 2026
Published 6 February 2026 Volume 2026:19 580372
DOI https://doi.org/10.2147/JMDH.S580372
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Krzysztof Laudanski
Omar Altal,1 Atef Hulliel,2 Basel Abubaker,1 Rawhi Alshaykh,2 Shahed Almasaeid,1 Tala Dabash,3 Reem Abuzraiq,3 Bara’a Darawsheh,1 Omar Al Othman1
1Department of Obstetrics and Gynecology, Faculty of Medicine, Jordan University of Science and Technology, Irbid, Jordan; 2Faculty of Medicine, Jordan University of Science and Technology, Irbid, Jordan; 3Department of Pediatrics, Faculty of Medicine, Al-Balqa Applied University, Salt, Jordan
Correspondence: Omar Altal, Department of Obstetrics and Gynecology, Faculty of Medicine, Jordan University of Science and Technology, Irbid, Jordan, Tel +962797423400, Fax +962 2 7201064, Email [email protected]
Introduction: Group B Streptococcus (GBS) is a leading cause of neonatal sepsis and maternal infections worldwide While general data on GBS prevalence in the Middle East exist, specific studies investigating GBS colonization and its outcomes among healthcare workers remain limited. This study aimed to determine the outcome of rectovaginal GBS colonization among pregnant women in northern Jordan and to compare maternal and neonatal outcomes between medical and non-medical staff.
Methods: A retrospective cohort study was conducted at King Abdullah University Hospital, including 257 GBS-positive pregnant women who delivered during the study period. Participants were categorized as medical staff (n=37) or non-medical staff (n=220). Maternal demographic, obstetric, and neonatal data were collected from hospital records. Statistical analyses were performed using chi-square and t-tests, with multivariable logistic regression adjusting for maternal age, gestational age, parity, and body mass index.
Results: Maternal age was significantly higher among medical staff (p=0.017), while other baseline variables showed no significant differences. There were no significant differences between medical and non-medical groups in maternal morbidity, neonatal intensive care unit (NICU) admission, or neonatal mortality (all p≥ 0.05). Adjusted models confirmed that occupation was not significantly associated with NICU admission (aOR 1.37, 95% CI 0.46– 4.09, p=0.575) or maternal morbidity (aOR 0.83, 95% CI 0.35– 2.00, p=0.685).
Conclusion: Occupational exposure among healthcare workers did not significantly influence GBS-related maternal or neonatal outcomes, and GBS colonization among pregnant women in northern Jordan aligns with global prevalence estimates. Larger, prospective studies are needed to confirm these findings and assess antimicrobial resistance trends in the region.
Keywords: group B streptococcus, pregnant, women, cohort study
Introduction
Group B Streptococcus (Streptococcus agalactiae) is a significant perinatal pathogen associated with severe infections in newborns, including sepsis, meningitis, and pneumonia.1,2 Maternal rectovaginal colonization during childbirth is the primary risk factor for early-onset neonatal infections, which typically manifest within the first seven days of life.3,4 Vertical transmission occurs in up to 50% of infected pregnancies, with invasive illness developing in 1% to 2% of exposed neonates.5 Beyond neonatal complications, GBS colonization has been linked to adverse pregnancy outcomes such as low birth weight, premature labor, and stillbirth.5,6
The global burden of GBS is substantial, with maternal colonization rates ranging from 15% to 25% worldwide, showing considerable regional importance.2,3 While prevalence estimates are somewhat lower in Asia, sub-Saharan Africa and the Americas report higher rates.7,8 Global estimates indicate approximately 400,000 maternal and newborn GBS cases annually, contributing significantly to perinatal morbidity and mortality.9 The emergence of antimicrobial resistance further complicates intrapartum antibiotic prophylaxis (IAP) strategies, as evidenced by studies in various regions.6
Data regarding GBS prevalence in the Middle East remains limited. Previous research in Jordan, reported maternal GBS colonization rates of 18–20%.10 Consistent with findings from Saudi Arabia (24%)11 and other Middle Eastern cohorts. However, northern Jordan, particularly the area served by King Abdullah University Hospital (KAUH), lacks published data on GBS prevalence. Furthermore, the potential impact of occupational exposure on GBS colonization rates, particularly among healthcare professionals, is poorly understood.12,13 This study aimed to determine the outcome of rectovaginal GBS colonization among pregnant women delivering at KAUH and to explore differences in colonization prevalence and associated maternal and neonatal complications between medical and non-medical staff.
Methods and Materials
Patients
This retrospective cohort study included pregnant women who delivered at King Abdullah University Hospital (KAUH) in northern Jordan and were confirmed to have rectovaginal colonization with Group B Streptococcus (GBS). A total of 257 GBS-positive women were identified and included in the final analysis. Participants were categorized into two groups based on occupation: medical staff (n = 37) and non-medical staff (n = 220).
Inclusion criteria encompassed all pregnant women with documented rectovaginal GBS colonization during routine antenatal screening or intrapartum evaluation who subsequently delivered at KAUH within the study period of 2024 (January 1, 2024, to December 31, 2024). Exclusion criteria included incomplete medical records, uncertain GBS culture results, or missing data regarding maternal or neonatal outcomes.
All relevant demographic, obstetric, and neonatal data were obtained from the hospital’s electronic medical records. The study protocol was approved by the Institutional Review Board (IRB) of Jordan University of Science and Technology and King Abdullah University Hospital (IRB Approval No.: Feb2025/179-26).
Data Extraction
Data were extracted retrospectively from the electronic medical records of all GBS-colonized pregnant women and their neonates. Collected variables included baseline maternal characteristics such as age, gestational age at delivery, parity, body mass index (BMI), premature rupture of membranes (PROM), diabetes mellitus (DM), hypothyroidism, chorioamnionitis, and antibiotic administration. Occupational status (medical vs non-medical) was identified from hospital employment records.
Neonatal characteristics included birthweight, NICU admission, duration of NICU stay, respiratory complications, and neonatal death prior to discharge. Maternal morbidity was defined as the presence of any obstetric or infectious complication during the peripartum period, including chorioamnionitis or postpartum infection.
All variables were collected using standardized clinical definitions consistent with institutional protocols at KAUH. Data completeness and accuracy were verified by cross-checking electronic records and delivery logs.
Specimen Collection
In accordance with the recommendations of the Centers for Disease Control and Prevention (CDC)14 and the American College of Obstetricians and Gynecologists, specimens were obtained from the lower third of the vagina and the anorectal area using sterile cotton swabs by the attending midwife. The swabs were promptly delivered to the Microbiology Laboratory at King Abdullah University Hospital. Samples were enriched in broth and incubated at 35–37 °C for 18–24 hours, followed by subculture onto 5% sheep blood agar plates, which were incubated for an additional 18–24 hours in a 5% CO2 environment. Only cultures with confirmed Group B Streptococcus growth were included in the analysis; samples showing mixed or multiple bacterial isolates were excluded.
Statistical Analysis
Data were entered into a spreadsheet and analyzed using IBM SPSS Statistics for Windows, Version 26.0. Nominal variables were expressed as frequency and percentage, while continuous variables were described using mean (standard deviation) and median (interquartile range). Comparisons between groups were performed using the Chi-square test for categorical variables and the Student’s t-test for continuous variables. A p-value ≤ 0.05 was considered statistically significant.
Sensitivity Analyses
Penalized logistic regression was utilized to assess the stability of estimates, particularly in cases where standard models encountered convergence issues or had small cell counts. These sensitivity analyses produced point estimates that were consistent with those obtained from the main adjusted models, where both were available. It is important to note that penalized fits, in this implementation, do not provide standard errors. Additionally, sensitivity analyses were conducted to account for incomplete antibiotic data by including antibiotic administration (yes/no/missing) as an additional covariate.
Results
Patient Demographics
A total of 257 (23.1%) Group B Streptococcus (GBS) colonized pregnant women (out of 1113 delivery conducted during the study period) were included in this analysis. Of these, 37 (14.4%) were medical staff and 220 (85.6%) were non-medical staff. The baseline characteristics of these two groups are summarized in Table 1.
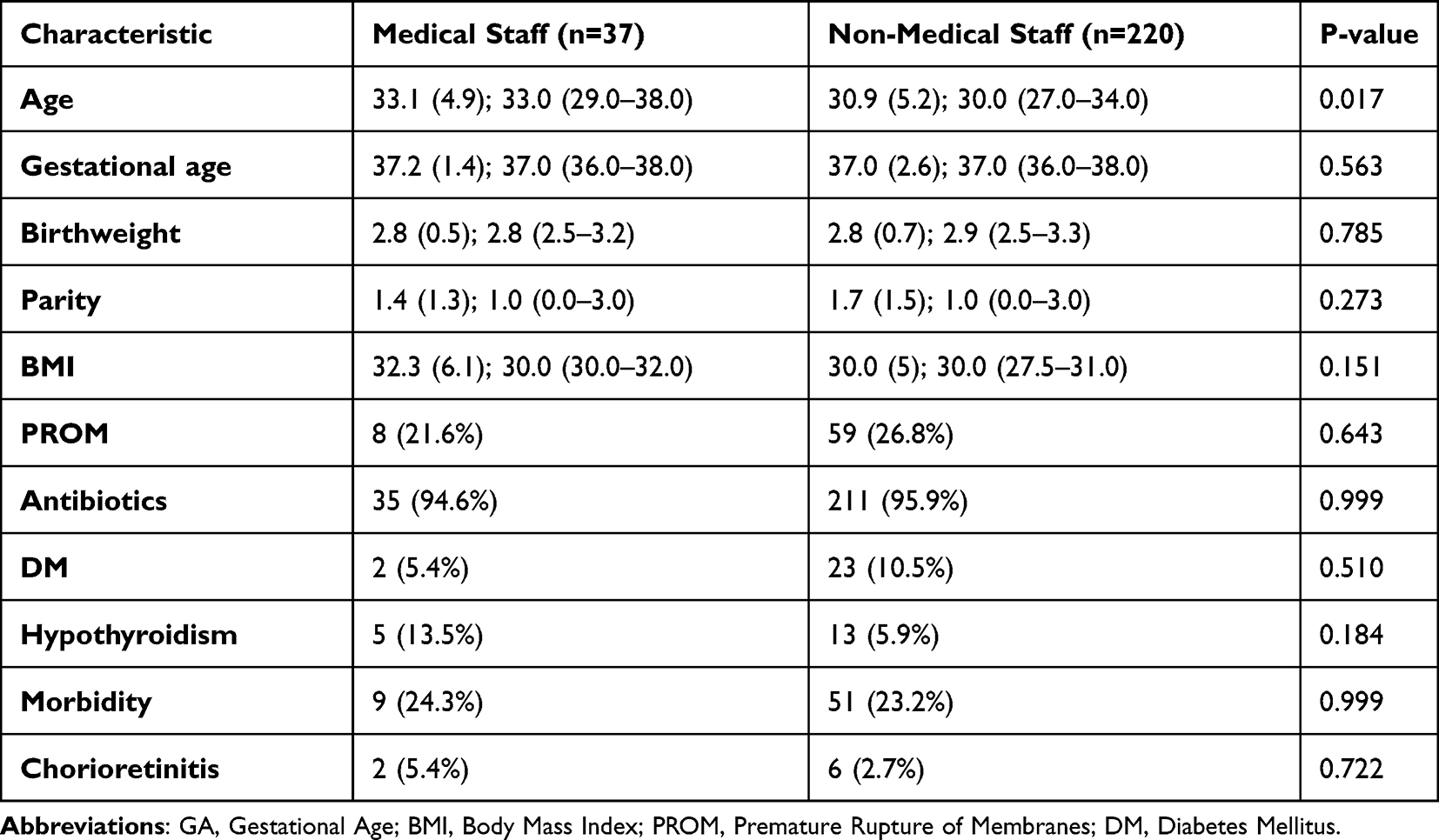 |
Table 1 Baseline Characteristics by Occupation, Reported as Mean (SD); Median (IQR) or n (%) |
Among the baseline characteristics, a statistically significant difference was observed only for maternal age (p=0.017), with medical staff having a slightly higher mean age compared to non-medical staff. All other baseline characteristics, including gestational age (GA), birthweight, parity, BMI, and rates of PROM, antibiotic use, DM, hypothyroidism, treated morbidity, and chorioamnionitis, showed no significant differences between the two occupational groups (all p≥0.05).
The primary analysis focused on comparing key outcomes between medical staff and non-medical staff. Table 2 presents the rates of NICU admission, maternal morbidity, and death for both groups. No statistically significant differences were observed for the primary outcomes (NICU admission, maternal morbidity, and death) between medical staff and non-medical staff (all p≥0.05).
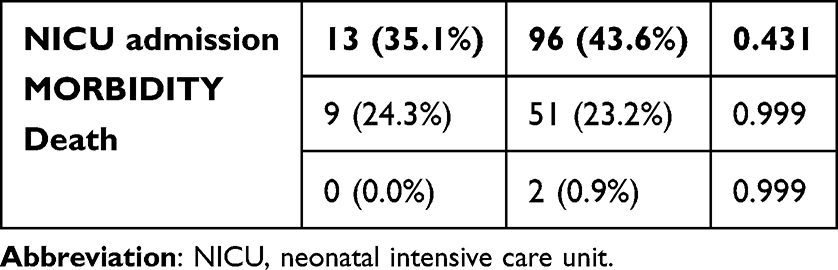 |
Table 2 Primary Outcomes by Occupation |
However, it is important to note that the relatively small sample size of medical staff (n = 37) may have limited the statistical power of the study to detect subtle but potentially clinically meaningful differences in GBS-related outcomes between occupational groups.
Further analysis of specific maternal outcomes also revealed no significant differences between the two occupational groups. Table 3 details the prevalence of various maternal outcomes.
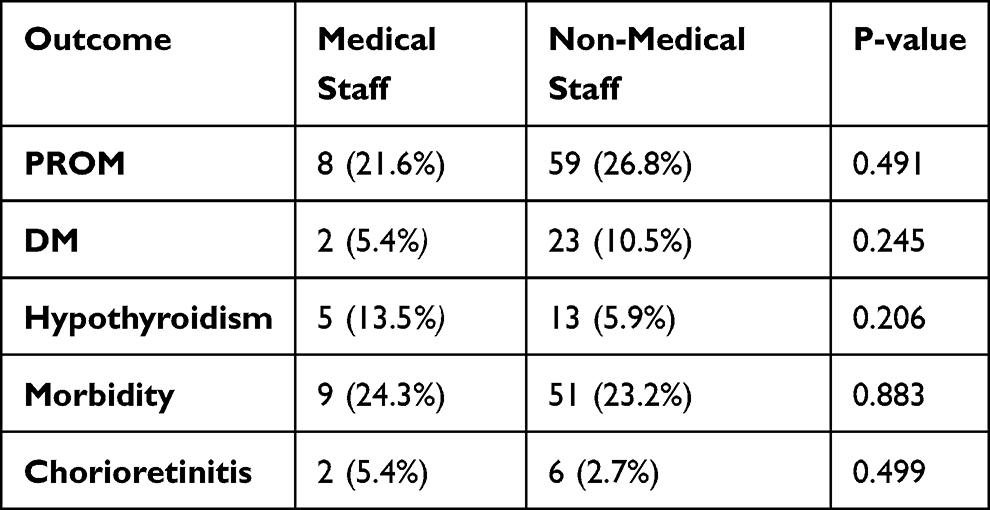 |
Table 3 Maternal Outcomes by Occupation |
No maternal outcome showed a statistically significant difference between occupation groups (all p≥0.05). A forest plot of the adjusted odds ratios for NICU admission and maternal morbidity Figure 1.
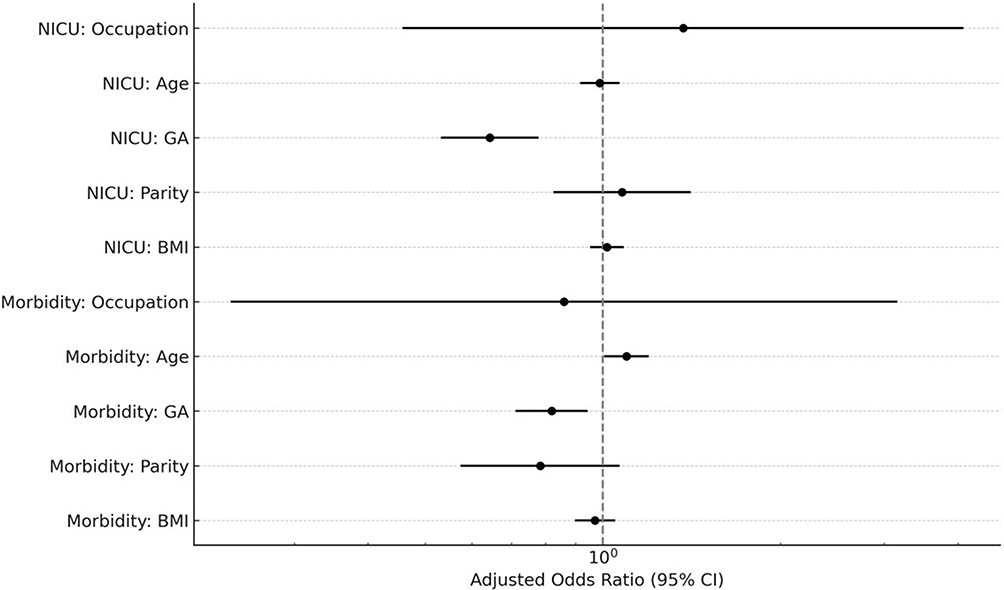 |
Figure 1 A forest plot of the adjusted odds ratios for NICU admission and maternal morbidity. |
Neonatal outcomes were also compared between the medical and non-medical staff groups. The Mann–Whitney U-test was employed for the duration of days spent in the NICU due to a non-normal distribution of this variable. Table 4 presents a summary of the neonatal outcomes.
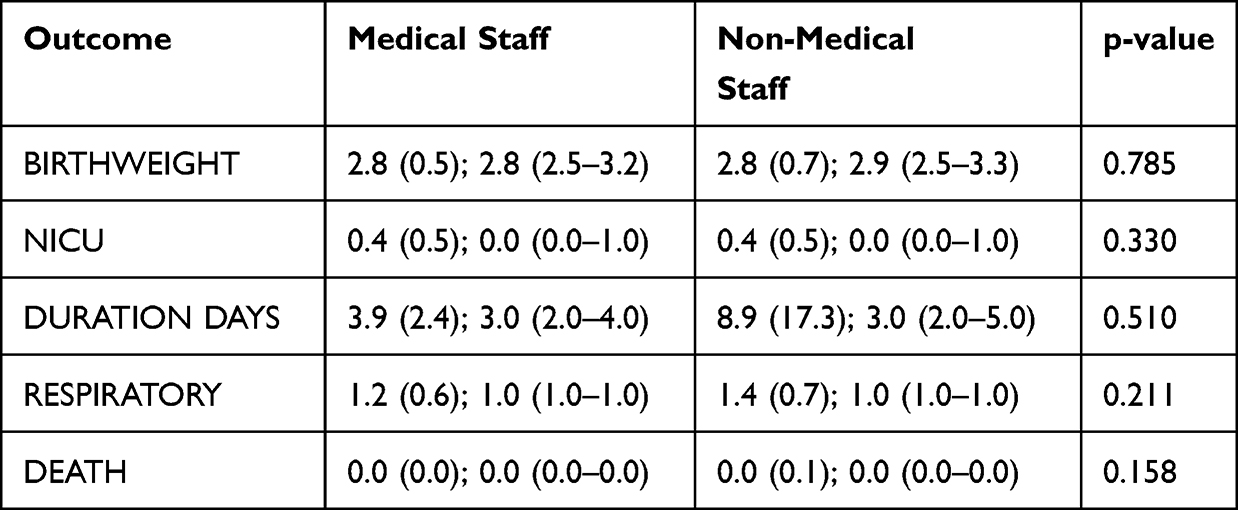 |
Table 4 Neonatal Outcomes by Occupation |
Adjusted logistic regression models were fitted for NICU admission and maternal morbidity, controlling for maternal age (AGE), gestational age (GA), parity (PARITY), and body mass index (BMI). The results, presented as adjusted odds ratios (aOR) with 95% confidence intervals (CI), are shown in Table 5.
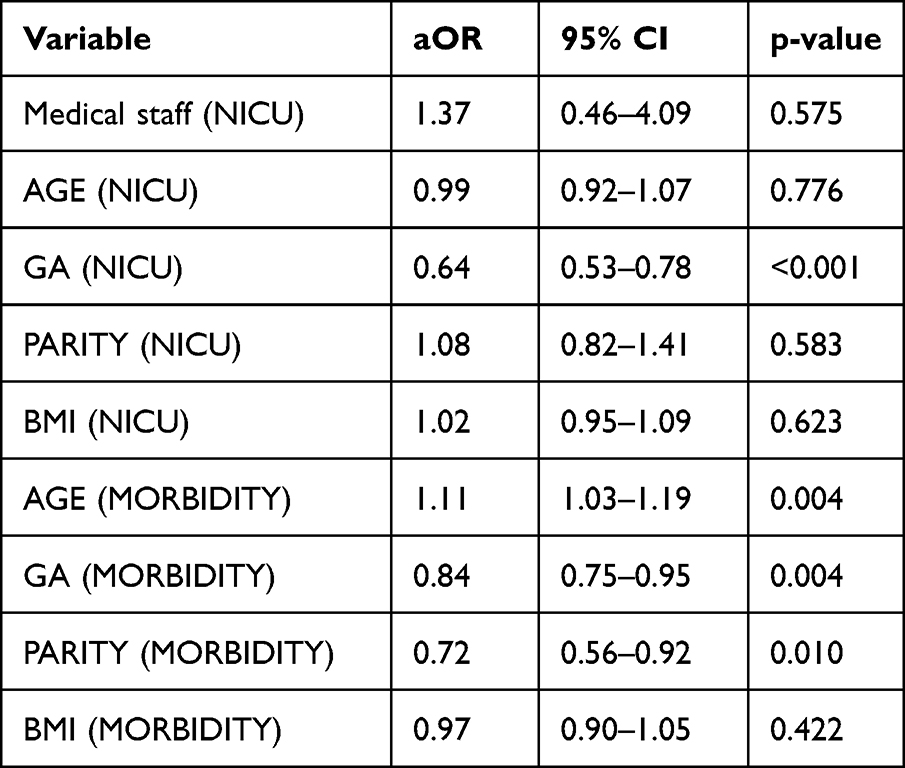 |
Table 5 Multivariable Logistic Regression Results (Adjusted ORs) |
In the multivariable models, occupation (medical staff) was not significantly associated with NICU admission (aOR 1.37, 95% CI 0.46–4.09, p=0.575) or maternal morbidity (aOR 0.83, 95% CI 0.35–2.00, p=0.685). However, gestational age (GA) was a significant predictor for NICU admission (aOR 0.64, 95% CI 0.53–0.78, p<0.001) and maternal morbidity (aOR 0.84, 95% CI 0.75–0.95, p=0.004). Maternal age (aOR 1.11, 95% CI 1.03–1.19, p=0.004) and parity (aOR 0.72, 95% CI 0.56–0.92, p=0.010) were also significant predictors for maternal morbidity.
Discussion
This study investigated the prevalence of rectovaginal Group B Streptococcus (GBS) colonization among pregnant women delivering at King Abdullah University Hospital (KAUH) in northern Jordan, with a particular focus on comparing outcomes between medical and non-medical staff. To the best of our knowledge, this is among the first studies in the Middle East to specifically evaluate GBS outcomes in these occupational groups. Previous research in the Middle East and North Africa (MENA) region has documented the clinical landscape of Group B Streptococcus colonization. Studies from Jordan,10 Saudi Arabia,15 Lebanon,16 and Iran17 have primarily focused on establishing prevalence rates, and identifying general clinical risk factors such as maternal age, parity, and gestational diabetes. Unlike these previous regional studies focusing primarily on general GBS prevalence or specific risk factors in the general population, our work uniquely dissects the impact of distinct occupational roles on GBS outcomes, representing a focused novel contribution to the regional literature. This comparison between healthcare and non-healthcare providers is particularly innovative for the Middle Eastern context, highlighting the novel contribution of our study within the regional context. Among 257 GBS-colonized pregnant women, there were no statistically significant differences in primary outcomes, maternal outcomes, or neonatal outcomes between medical staff (n=37) and non-medical staff (n=220), including NICU admission, maternal morbidity, birthweight, duration of NICU hospitalization, respiratory issues, and neonatal death. Multivariable analyses adjusting for confounders such as body mass index, parity, and gestational age, further supported these observations, demonstrating that occupation was not a significant predictor for NICU admission or maternal morbidity. Sensitivity analyses and subgroup stratifications further supported the lack of significant relationships between occupation and key outcomes, reinforcing the robustness of these findings.
The overall prevalence of GBS colonization in our cohort aligns with global estimates, which suggest maternal colonization rates range from 15% to 25%.2,3 A comprehensive meta-analysis reported a global prevalence of maternal GBS colonization at 17.9%.2 Regionally, data from the MENA demonstrate considerable variability, with reported rates ranging from 1.6% to 32%.10 A study conducted in Amman, Jordan, found a prevalence of 19.5% among pregnant women, which is very similar to the prevalence observed in our study.10 This consistency underscores the ongoing burden of GBS in the region and highlights the need for continued surveillance and prevention strategies.
A key aim of our study was to assess whether health professionals differed from non-health staff in terms of GBS colonization and related outcomes. Contrary to the hypothesis that healthcare professionals might have different colonization patterns due to occupational exposure,12,13 our study found no statistically significant differences in GBS-related maternal or neonatal outcomes between these two groups. This finding is noteworthy, as some earlier studies have suggested a potential link between healthcare occupation and increased risk of GBS colonization. For instance, a study by Stapleton et al (2005) identified healthcare occupation as an independent risk factor for GBS colonization (OR 1.22).18 Similarly, Yamamura et al (2005) reported a higher prevalence of GBS colonization among healthcare workers (20%) compared to non-healthcare workers (16.5%), with an odds ratio of 1.28.19
The discrepancy between our findings and some previous literature could be attributed to several factors. Differences in study populations, geographical locations, GBS screening protocols, and infection control practices within healthcare settings may play a role. Differences in GBS screening methods likely contributed to discrepancies with Stapleton et al.18 While that study relied on administrative data and ICD-9 codes to identify GBS, our study used direct microbiological screening of rectovaginal samples per CDC guidelines. This culture-based approach provides more accurate detection at delivery and reducing misclassification. The studies by Stapleton et al and Yamamura et al were conducted in the United States, which may have different occupational exposure risks or GBS epidemiology compared to Jordan. Furthermore, the definition of “healthcare worker” and the specific roles within healthcare can vary, influencing exposure levels. It is also possible that improved infection control measures in healthcare settings over time have mitigated some of these occupational risks.In our cohort, health staff were statistically significantly older than non-health participants (mean 33.1 vs 30.9 years). Although large-scale reviews have not consistently found maternal age to be a significant predictor, it has occasionally been linked to GBS colonization and pregnancy outcomes.2,3 Importantly, in our adjusted models, age emerged as an independent predictor of maternal morbidity, suggesting that physiological and comorbid factors, rather than occupational exposure, may underlie differences in outcomes. Parity also played a role, with higher parity associated with lower morbidity, consistent with population-based studies.3,12 Our study found no significant differences in maternal outcomes such as premature rupture of membranes (PROM), gestational diabetes (DM), hypothyroidism, or chorioamnionitis between medical and non-medical staff. Similarly, neonatal outcomes, including birthweight, NICU admission, duration of NICU stay, respiratory issues, and death, did not differ significantly based on maternal occupation. These results are consistent with the understanding that while GBS colonization is a risk factor for adverse maternal and neonatal outcomes, the direct impact of maternal occupation on these outcomes, independent of GBS status, may be limited.20,21
Previous research has extensively documented the association between maternal GBS colonization and adverse neonatal outcomes. For instance, early-onset GBS disease (EOGBS) is a leading cause of neonatal sepsis and meningitis, with significant morbidity and mortality.22,23 The implementation of intrapartum antibiotic prophylaxis (IAP) has dramatically reduced the incidence of EOGBS in countries where universal screening is routine.14,24 However, the effectiveness of IAP can be challenged by rising antimicrobial resistance, a concern highlighted in various global studies.6,25 Our study did not directly assess the effectiveness of IAP or antimicrobial resistance patterns, but these are crucial considerations for future research in the region.
Regarding maternal complications, GBS has been implicated in chorioamnionitis, postpartum endometritis, and preterm labor.26 While our study observed no significant differences in these outcomes between the occupational groups, the overall rates of some complications, such as PROM, were present in both groups, reflecting the general risks associated with pregnancy and GBS colonization. The lack of significant differences between health and non-health staff suggests that, at least in this cohort, occupational factors did not confer an additional measurable risk for these specific complications.Future research should include larger, prospective studies to confirm these findings and explore additional risk factors for GBS colonization in the Jordanian population. A more detailed assessment of occupational exposure, including specific roles, patient contact hours, and adherence to infection control practices, could provide a nuanced understanding of any subtle occupational risks. Furthermore, investigating the serotype distribution of GBS isolates in northern Jordan, as well as their antimicrobial resistance patterns, is essential for guiding empirical antibiotic choices and informing vaccine development strategies. Finally, studies comparing outcomes between GBS-colonized and non-colonized women in the region would provide a more complete picture of the local burden of GBS disease.
This study has several limitations. As a retrospective single-center analysis, findings may not be generalizable to other populations. The small number of medical staff (n=37) may limit statistical power to detect subtle differences. Furthermore, the study was conducted at a single center in northern Jordan, which may limit the generalizability of the findings to other regions or populations. Lastly, detailed information on the specific roles and direct patient contact levels of the medical staff was not available, which could influence the assessment of occupational exposure.
Conclusion
In conclusion, While GBS colonization is a known public health concern, this study found no significant differences in maternal or neonatal outcomes related to GBS colonization between pregnant medical staff and non-medical staff at KAUH in northern Jordan. These findings suggest that occupational exposure as a healthcare worker may not independently increase the risk of adverse GBS-related outcomes in this population. Further prospective studies with larger cohorts and detailed occupational exposure assessments are warranted to confirm these findings and to better understand the epidemiology of GBS in the Middle East, including antimicrobial resistance patterns and the effectiveness of current prevention strategies.
Data Sharing Statement
The datasets used and/or analyzed during the current study are presented in tables and text.
Ethical Approvals
This work was approved by the institutional review board (IRB) committee at Jordan University of Science and Technology and King Abdullah University Hospital. IRB No.: Feb2025/179-26, date: 2/3/2025. The study was conducted in accordance with the Declaration of Helsinki, good clinical practices, and relevant regulatory guidelines. The need for written informed consent was waived due to the retrospective nature of the study. We confirm that the privacy of the participants was saved, and the data was anonymized and maintained with confidentiality.
Funding
This work was funded by a grant from the Deanship of Research, Jordan University of Science and Technology (Grant number: 20250130).
Disclosure
The authors declared no conflicts of interest in this work.
References
1. Wang J, Zhang Y, Lin M, et al. Maternal colonization with group B streptococcus and antibiotic resistance in China: systematic review and meta-analyses. Ann Clin Microbiol Antimicrob. 2023;22(1):5. doi:10.1186/s12941-023-00553-7
2. Russell NJ, Seale AC, O’Driscoll M, et al. Maternal colonization with group B streptococcus and serotype distribution worldwide: systematic review and meta-analyses. Clin Infect Dis. 2017;65(suppl_2):S100–9. doi:10.1093/cid/cix658
3. Kwatra G, Cunnington MC, Merrall E, et al. Prevalence of maternal colonisation with group B streptococcus: a systematic review and meta-analysis. Lancet Infect Dis. 2016;16(9):1076–1084. doi:10.1016/S1473-3099(16)30055-X
4. Madrid L, Seale AC, Kohli-Lynch M, et al. Infant group B streptococcal disease incidence and serotypes worldwide: systematic review and meta-analyses. Clin Infect Dis. 2017;65(suppl_2):S160–s172. doi:10.1093/cid/cix656
5. Bekele H, Debella A, Getachew T, et al. Prevalence of group B streptococcus recto-vaginal colonization, vertical transmission, and antibiotic susceptibility among pregnant women in Ethiopia: a systematic review and meta-analysis. Front Public Health. 2022;10:851434
6. Wang Y, Liu J, Song J, et al. Association between maternal rectovaginal group B streptococcus and the risk of stillbirth: a meta-analysis. PeerJ. 2025;13:e18834. doi:10.7717/peerj.18834
7. Gizachew M, Tiruneh M, Moges F, et al. Streptococcus agalactiae maternal colonization, antibiotic resistance and serotype profiles in Africa: a meta-analysis. Ann Clin Microbiol Antimicrob. 2019;18(1):14. doi:10.1186/s12941-019-0313-1
8. Wadilo F, Hailemeskel E, Kedir K, et al. Prevalence of group B streptococcus maternal colonization, serotype distribution, and antimicrobial resistance in Sub-Saharan Africa: a systematic review and meta-analysis. J Glob Antimicrob Resist. 2023;32:134–144. doi:10.1016/j.jgar.2023.02.004
9. Gonçalves BP, Procter SR, Paul P, et al. Group B streptococcus infection during pregnancy and infancy: estimates of regional and global burden. Lancet Glob Health. 2022;10(6):e807–e819. doi:10.1016/S2214-109X(22)00093-6
10. Clouse K, Shehabi A, Suleimat AM, et al. High prevalence of group B streptococcus colonization among pregnant women in Amman, Jordan. BMC Pregnancy and Childbirth. 2019;19(1):177. doi:10.1186/s12884-019-2317-4
11. Arain FR, Al-Bezrah NA, Al-Aali KY. Prevalence of maternal genital tract colonization by group B streptococcus from Western Province, Taif, Saudi Arabia. 2015.
12. van Kassel MN, Janssen SWCM, Kofman S, et al. Prevalence of group B streptococcal colonization in the healthy non-pregnant population: a systematic review and meta-analysis. Clin Microbiol Infect. 2021;27(7):968–980. doi:10.1016/j.cmi.2021.03.024
13. Ngayomela PH, Kiritta R, Remi BA, et al. Streptococcus agalactiae colonization is common among pregnant women with HIV infection and is neither predicted by hospital tier nor trimester in Mwanza, Tanzania. BMC Pregnancy Childbirth. 2025;25(1):478. doi:10.1186/s12884-025-07585-1
14. Verani JR, McGee L, Schrag SJ. Prevention of perinatal group B streptococcal disease--revised guidelines from CDC, 2010. MMWR Recomm Rep. 2010;59(Rr–10):1–36.
15. Alshengeti A. Group B streptococcus among pregnant women and neonates in Saudi Arabia: a systemic review. Pathogens. 2022;11(9):1029. doi:10.3390/pathogens11091029
16. Alfouzan W, Gaddar N, Dhar R, et al. A study of group B streptococcus in pregnant women in Lebanon: prevalence, risk factors, vaginal flora and antimicrobial susceptibility. Infez Med. 2021;29(1):85–93.
17. Darabi R, Tadi S, Mohit M, et al. The prevalence and risk factors of group B streptococcus colonization in Iranian pregnant women. Electron Physician. 2017;9(5):4399–4404. doi:10.19082/4399
18. Stapleton RD, Kahn JM, Evans LE, et al. Risk factors for group B streptococcal genitourinary tract colonization in pregnant women. Obstet Gynecol. 2005;106(6):1246–1252. doi:10.1097/01.AOG.0000187893.52488.4b
19. Yamamura Y, Famuyide A. Prevalence of group B streptococcus among parturients employed in the health care field. Obstetrics Gynecol. 2005;105(4).
20. Chen X, Cao S, Fu X, et al. The risk factors for Group B Streptococcus colonization during pregnancy and influences of intrapartum antibiotic prophylaxis on maternal and neonatal outcomes. BMC Pregnancy Childbirth. 2023;23(1):207. doi:10.1186/s12884-023-05478-9
21. Morgan JA, Zafar N, Cooper DB. Group B streptococcus and pregnancy. In: StatPearls. StatPearls Publishing; 2025. Copyright © 2025, StatPearls Publishing LLC.: Treasure Island (FL) ineligible companies. Disclosure: Nowera Zafar declares no relevant financial relationships with ineligible companies. Disclosure: Danielle Cooper declares no relevant financial relationships with ineligible companies.
22. Berardi A, Rossi C, Lugli L, et al. Group B streptococcus late-onset disease: 2003-2010. Pediatrics. 2013;131(2):e361–8. doi:10.1542/peds.2012-1231
23. Hall J, Adams NH, Bartlett L, et al. Maternal disease with group B streptococcus and serotype distribution worldwide: systematic review and meta-analyses. Clin Infect Dis. 2017;65(suppl_2):S112–s124. doi:10.1093/cid/cix660
24. ACOG Committee. Prevention of group B streptococcal early-onset disease in newborns: ACOG committee opinion, number 797. Obstet Gynecol. 2020;135(2):e51–e72. doi:10.1097/AOG.0000000000003668
25. Wang CH, Kung W-J, Lee C-H, et al. High rates of colonization and antimicrobial resistance of group B streptococcus highlight the need for vaccination even after implementation of guidelines for intrapartum antibiotic prophylaxis. Vaccine. 2022;40(2):282–287. doi:10.1016/j.vaccine.2021.11.069
26. Schuchat A. Epidemiology of group B streptococcal disease in the United States: shifting paradigms. Clin Microbiol Rev. 1998;11(3):497–513. doi:10.1128/CMR.11.3.497
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Psychosocial Profile of Women Who Defaulted Option B+ HIV Treatment: An Interpretive Phenomenological Analysis Study
Dhlakama PM, Lelaka CM, Mavhandu-Mudzusi AH
HIV/AIDS - Research and Palliative Care 2023, 15:583-598
Published Date: 28 September 2023
Association Between Endometriosis and Mental Disorders Including Psychiatric Disorders, Suicide, and All-Cause Mortality -A Nationwide Population-Based Cohort Study in Taiwan
Wang TM, Lee YL, Chung CH, Sun CA, Kang CY, Wu GJ, Chien WC
International Journal of Women's Health 2023, 15:1865-1882
Published Date: 28 November 2023
Associations Between Self-Rated Health and Mortality in the Norwegian Women and Cancer (NOWAC) Study
Killie IL, Braaten T, Lorem GF, Borch KB
Clinical Epidemiology 2024, 16:109-120
Published Date: 20 February 2024
Risk of Depression and Anxiety in Those Who Gave Birth to Children Who Developed Invasive Group B Streptococcal Disease: A Population-Based Cohort Study
Horváth-Puhó E, Chandna J, Paul P, Wilson CA, Sørensen HT, Lawn JE
Clinical Epidemiology 2025, 17:315-325
Published Date: 28 March 2025
Light to Moderate Alcohol Consumption and Cancer Incidence: The Norwegian Women and Health Cohort Study
Llaha F, Licaj I, Sharashova E, Ferrari P, Lukic M, Benjaminsen Borch K
Clinical Epidemiology 2025, 17:807-821
Published Date: 10 October 2025