")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 15
The Psychosocial Profile of Women Who Defaulted Option B+ HIV Treatment: An Interpretive Phenomenological Analysis Study
Authors Dhlakama PM, Lelaka CM, Mavhandu-Mudzusi AH
Received 20 March 2023
Accepted for publication 13 August 2023
Published 28 September 2023 Volume 2023:15 Pages 583—598
DOI https://doi.org/10.2147/HIV.S401336
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Patricia Mae Dhlakama,1 Constance Matshidiso Lelaka,2 Azwihangwisi Helen Mavhandu-Mudzusi1
1Department of Health Studies, College of Human Sciences: University of South Africa, Pretoria, Gauteng Province, South Africa; 2The Discipline of Social Work, School of Human & Community Development, University of the Witwatersrand, Johannesburg, 2000, South Africa
Correspondence: Constance Matshidiso Lelaka; Patricia Mae Dhlakama, Email [email protected]; [email protected]
Purpose: The study explored the psychosocial profile of women who defaulted Option B+ HIV treatment at Chitungwiza Municipality clinics in Zimbabwe. Option B+ is a strategy to prevent mother-to-child transmission (PMTCT) of HIV to reduce MTCT rate to less than or equal to 5%.
Methods: An interpretive phenomenological analysis (IPA) design was used. Data were collected from 04 September to 12 October 2020 on twelve purposively selected HIV-positive breastfeeding women aged 18 to 40 years, who defaulted Option B+ HIV treatment. Unstructured individual face-to-face interviews were utilised. Data were analysed thematically using the interpretive phenomenological analysis framework for data analysis.
Results: The study findings revealed that participants experienced the following: psychosocial and emotional challenges due to HIV positive results, shown emotional distress and suicidal tendencies which affected their mental health. Their relationship was derailed due to abuse, infidelity, partner’s high-risk behaviour and to lack of support stemming from their partners and family members.
Conclusion: Strengthening adherence support interventions and effective counselling on HIV-positive status disclosure and male partner involvement is important for retaining women in care and for improving their quality of life. Comprehensive, integrated, and tailor-made interventions should be adopted. Couple HIV counselling and testing should be encouraged. Psychosocial and mental health should be encouraged. Furthermore, community sensitization, risk reduction behaviour, education on purpose and side effects of ART as well as the benefits of Option B+ to new enrolments should be intensified and strengthened to minimize defaulting of treatment and LTFUP. Vigorous patient tracing and visit reminders help retain women in care.
Keywords: breastfeeding, HIV, Option B+, PMTCT, pregnant, psychosocial, treatment default, women
Introduction
The Human Immunodeficiency Virus (HIV) and Acquired Immune Deficiency Syndrome (AIDS) remain the major causes of maternal and child morbidity and mortality.1 Early antiretroviral therapy (ART) initiation reduces HIV-related morbidity, improves early linkage to care, and strengthens the immune system.2 The chances of transmitting HIV from mother to child of an HIV-positive pregnant woman who is not on treatment are 15% to 45% globally despite the availability of ART and other interventions can reduce this risk to below 5%.3,4 Zimbabwe recently achieved the 2020 targets of 90% of people with HIV knowing their status, 90% of people diagnosed with HIV infection being on lifelong ART and 90% on ART having viral suppression and is now on track to reach the UNAIDS 2025 targets of 95–95–95% targets for HIV testing, treatment, and viral suppression by 2025, reports.5 Of recent it has been reported that ZIMBABWE has reached the UNAIDS set 95–95–95 HIV targets, securing a place in the list of other Southern African countries such as Botswana that have attained the goal.6
In 2002, the WHO introduced the first guidelines on the use of ART for HIV infection in adults and adolescents. In 2004, the guidelines expanded to cover the use of ART for the prevention of mother–to–child transmission (PMTCT) of HIV.7 It has been difficult to achieve in PMTCT programs in sub- Saharan Africa due to weak health systems and a variety of individual, interpersonal and cultural factors.8
The World Health Organisation7 emphasised the need for antiretroviral therapy to be initiated urgently to all pregnant and breastfeeding women, even if they are identified late in pregnancy or post-partum because the most effective way to prevent MTCT of HIV is to reduce maternal viral load. Hence, it was important to understand the psychosocial impact of HIV positive pregnant or breastfeeding women who defaulted Option B+ HIV treatment in order to find ways to reduce defaulting and enhance adherence to treatment. Option B+ is a strategy to prevent mother-to-child transmission (PMTCT) of HIV to reduce MTCT rate to less than or equal to 5%.9
An interpretive phenomenological study conducted in Malawi to understand the experiences of HIV-infected women in relation to the utilization of Option B+ services revealed that women experienced several challenges. The challenges include sub-optimal counselling in relation to the benefits of ART, side effects of ARV drugs, conflicting religious advice, unsupportive spouses, stigma, and geographical, financial accessibility which led women to default or not to adhere to treatment10 indicated that people from remote areas defaulted treatment because of lack of transport to the healthcare facilities.
A study done to assess early retention among women on Option B+ from antenatal care (ANC) until 6 months post ANC booking and at delivery in rural and urban Zimbabwe reports low retention at 3, 6 months and delivery, an impediment to elimination of mother-to-child transmission of HIV in Zimbabwe. The study findings highlight the need for effective interventions to improve early retention such as post-test counselling, patient tracing and visit reminders.9 A study conducted in Uganda to assess retention-in-care among women on Option B+ in Uganda suggests that retention under Option B+ is suboptimal and is under-estimated at health facility level. Patient unreadiness, inadequate counselling, HIV-related stigma and unsupportive partners and drug side-effects were the issues highlighted mostly by the women that were LTFU. The study recommended on improving tracking of women across facilities, using online electronic medical records system to automatically track self-transfers, and improving counselling and support for disclosure mostly among young women and those of low education status.11
A higher incidence of LTFU among women on option B+ PMTCT program comparative to previous studies in Ethiopia, was indicated in a recent study in northwestern Ethiopia conducted by Geremew et al12 who suggest strengthening adherence support interventions and effective counselling on HIV-positive status disclosure and male partner involvement as important to retain women in care.
Zimbabwe officially launched the Option B+ approach in November 2013 to facilitate the achievement of the elimination of mother-to-child HIV transmission (eMTCT) of HIV goals.13 Despite launching Option B+, in 2017, Zimbabwe had one of the highest HIV prevalences in SSA at 13.3%, with 14,816 pregnant women and 76,650 children (0 to 4 years) living with HIV.14 The 2018 antenatal registers indicated that from 1 January 2018 to 31 December 2018, the four clinics under Chitungwiza Municipality enrolled a total of 300 women in Option B+ HIV treatment. Among those enrolled, about 117 women defaulted.15 This gave a defaulter rate of 39%. Such a high defaulter rate was a cause for concern as it might stall progress towards achieving UNAIDS’s goal of elimination of HIV by the year 2030. This is because women may develop resistance to antiretroviral medicine, which will affect viral suppression. When the women’s viral load is not suppressed, there is a higher chance of transmitting HIV to the child and even the partner.2 Defaulting treatment also increases treatment costs as individuals get managed on the expensive second line or third line ARV medicine.2 Despite this high defaulter rate and the negative impact of defaulting treatment, there is no documented study conducted in Chitungwiza Municipality clinics about the psychosocial experiences of women who defaulted Option B+ HIV treatment that showed what might have contributed towards defaulting in this population group. It is therefore imperative that this population group be provided with comprehensive psychosocial support. According to Lelaka et al16 psychosocial refers to the dynamic relationship between the psychological and social dimension of a person and these two influence each other. These also include individual’s thoughts, emotions, behaviours, and perceptions, whilst the social aspects address interaction and relationships among the individual, peers, and community. In addition, the psychosocial support activities are meant to address the psychological and social stressors associated with living with HIV.17 In the study findings reported by Okonji et al,18 the findings demonstrated that communities are needed because they play an important role in providing emotional and psychosocial support for people living with HIV. Mukumbang et al19 also reported that family centred services were found to enhance and promote love, family cohesion and communication, and such enhances shared responsibility of caring for people living with HIV amongst family members. This study explored the psychosocial experiences of women who defaulted Option B+ HIV treatment in Chitungwiza Municipality clinics.
Methods
Study Design
The study was phenomenological in nature. Qutoshi20 defines phenomenology as a philosophy that provides a theoretical guideline to researchers to understand phenomena at the level of subjective reality with the main purpose of looking very carefully at the phenomena under study to explore the complex world of lived experiences from the point of view of those individuals who live it. However, the researchers used an interpretive phenomenological analysis (IPA) design, which is one type of phenomenology. An interpretive phenomenological analysis design was followed to explore and describe the psychosocial experiences of women who defaulted Option B+ HIV treatment at Chitungwiza municipality clinics and to provide recommendations to strengthen and enhance services for this population group. For the purpose of this study, defaulting is defined as failing to collect treatment for 30 consecutive days or more, as explained to the researcher by the Chief Nursing Officer of Chitungwiza Health Department on 08 July 2019. This design is widely used in social science research as a method to explore and describe the lived experiences of individuals.21 This design was considered the most suitable as it enabled the researchers to engage in dialogue with participants and to gain an interpretation of an experience means from the participant’s point of view.22
Study Setting
The study was conducted at two municipality clinics of Chitungwiza town which is the dormitory town of Harare, the capital city of Zimbabwe. Chitungwiza is the second largest city of Zimbabwe.23 The Chitungwiza Municipality clinics were identified as they had a high defaulter rate of women on Option B+ HIV treatment as seen in patients’ medical records referred to as green books and the Electronic Patient Monitoring System – Zimbabwe.24 Chitungwiza’s urban population was 356, 840 per 2012 population census.25 In Zimbabwe, Option B+ for pregnant and lactating women has two options, namely 1) Preferred Option and 2) Alternative Option. The Preferred Option offers 1st line therapy which includes TDF + 3TC+ EFV600 and 2nd line therapy which includes If TDF was used as first line, use AZT plus 3TC plus ATV/r or LPV/r or If AZT was used as first line, use TDF plus 3TC plus ATV/r or LPV/r. The Alternative Option includes only 1st line which is AZT + 3TC + EFV600 AZT + 3TC + NVP and TDF + 3TC + NVP.
Population and Sampling
The population of the study was HIV-positive pregnant or breastfeeding women who started Option B+ HIV treatment in Chitungwiza Municipality clinics between 1 January to 31 December 2019 and who defaulted treatment. At the time of the interviews, all the pregnant women who had enrolled in Option B+ during their antenatal period from 01 January 2019 to 31 December 2019 had delivered and were all breastfeeding. Asiamah et al26 define the target population as the group of individuals or participants with the specific attributes of interest and relevance. The sample size was determined by data saturation. Data saturation can be reached at the stage where no new data emerge and there is redundancy of data that is already collected.27
Inclusion Criteria
All HIV-positive pregnant or breastfeeding women enrolled in Option B+ from 1 January 2019 to 31 December 2019 who defaulted treatment for 30 consecutive days or more, 18 years and above, diagnosed as HIV-positive at one of the clinics at Chitungwiza Municipality clinics, taken Option B + treatment prior to defaulting for at least a month and still utilising the clinic for antenatal or post-natal care, physically healthy, able to consent and be audio recorded.
Exclusion Criteria
All HIV-positive pregnant or breastfeeding women who were not enrolled in Option B+ from 1 January 2019 to 31 December 2019 who defaulted treatment for 30 consecutive days or more, 18 years and below, diagnosed as HIV-positive at none of the clinics at Chitungwiza Municipality clinics, not taken Option B + treatment prior to defaulting for at least a month, not utilising the clinic for antenatal or post-natal care, women who were physically weak and women who were unable to consent and audio recorded.
Data Collection/Research Instrument
A qualitative interview guide was used as a data collection instrument to get an account of an individual’s experiences, thoughts, and perspectives.28 The interview questions focused on the phenomenon under study. The interview guide was composed of two sections. The first section was for demographic data, while the second section was composed of the grand tour question. Before data collection, the interview guide was piloted on two participants from the study site who met the study’s inclusion criteria to explore the gaps in the tool so that amendments can be made. The data was received from the pilot. The interviews took place in private rooms in the Family Health Services Department of the two municipal clinics and were conducted in Shona, which is the main local language in Chitungwiza. The following grand tour question was asked: “Kindly share with me your experience on Option B+ treatment at Chitungwiza municipality clinics”. To get more detail from participants, the researcher used probes and prompts in addition to having short periods of silence to enable the participant to reflect and talk.29 To ensure confidentiality and privacy and protect their identity pseudonym names were used. All participants consented to the interviews which were audio recorded, lasted between 30 minutes and 45 minutes, were transcribed verbatim and translated from Shona to English within 48 hours.
Ethical Measures
The study complies with the Declaration of Helsinki ethical concerns/considerations because the study involves human participants as part of the study and their data was collected during the interviews. The basic principle of Declaration of Helsinki maintains that participants should be respected all the time both before and after the study, participants need to be informed about the purpose of study so that they can make informed decisions about their choices by means of exercising their rights to self-determination with coercion or interference. For the purpose of this research, the researchers adhered to ethical guidelines which involve protecting human rights, right to freedom from discomfort and harm, confidentiality and anonymity, privacy, and the right to fair treatment30 obtaining informed consent from participants, and protecting institutional rights, which entails submitting a research proposal to institutional review boards.31 Ethical clearance to conduct the study was granted by the Department of Health Studies Research Ethics Committee of the University of South Africa (Ethics clearance number: HSHDC/952/2020). Permission for conducting the study at Seke South and Zengeza clinics in Chitungwiza was obtained from the Chitungwiza Municipality Health Department Ethics Committee and the Director of Health Services. Ethical clearance and approval to carry out the study was also sought from the Medical Research Council of Zimbabwe (MRCZ) and was granted.
Data Analysis
Data analysis was completed following data collection, all the recorded data was transcribed verbatim. Data is divided into demographics as per Table 1 and participants superordinate themes, themes and subthemes as per Table 2. Lewis32 defines data analysis as the preparation, organization, and reduction of the data into themes and the interpretation of the results through a repetitive process that moves in analytic circles rather than a fixed linear approach. Data was analysed manually following the Colaizzi’s (1978) seven steps of phenomenological data analysis described by Praveena and Sasikumar33 as follows: 1) obtaining a general sense of each Transcript and the researcher read transcripts several times while comparing them to the audio recordings and correcting any mistakes; 2) extracting significant statements where the researcher did intensive reading to find and highlight the significant statement regarding participants’ experiences from the transcripts; 3) formulation of meaning where the researcher critically checked the significant statements in order to come up with relevant meaning related to the experiences. This process allowed further immersion in data by the researcher; 4) organization of formulated meanings into clusters of themes and themes and similar meanings were grouped together into clusters of themes. The clusters of themes were further grouped into emergent themes; 5) exhaustively describing the phenomenon where the researcher went through the emergent themes and are analysed again, trying to understand what they are all about. This process led to a description of the exact meaning of the experiences of the participants; 6) describing the fundamental structure of the phenomenon: The description of the phenomenon was rechecked, and repetition identified. Where there was a similar description, the statements were cut off, and the description was then revised to ensure that it was clear and concise in portraying women's experiences; and finally 7) returning to the participants to validate the findings from the study participants: The researcher did member checking to ensure that the emergent themes were not distorting participants' experiences. This process was facilitated by researchers who managed to discuss and compare the list of superordinate theme, themes, and subthemes. The researchers finally had consensus discussion and agreed on the final master table that is supported by quotes from participants' transcripts.
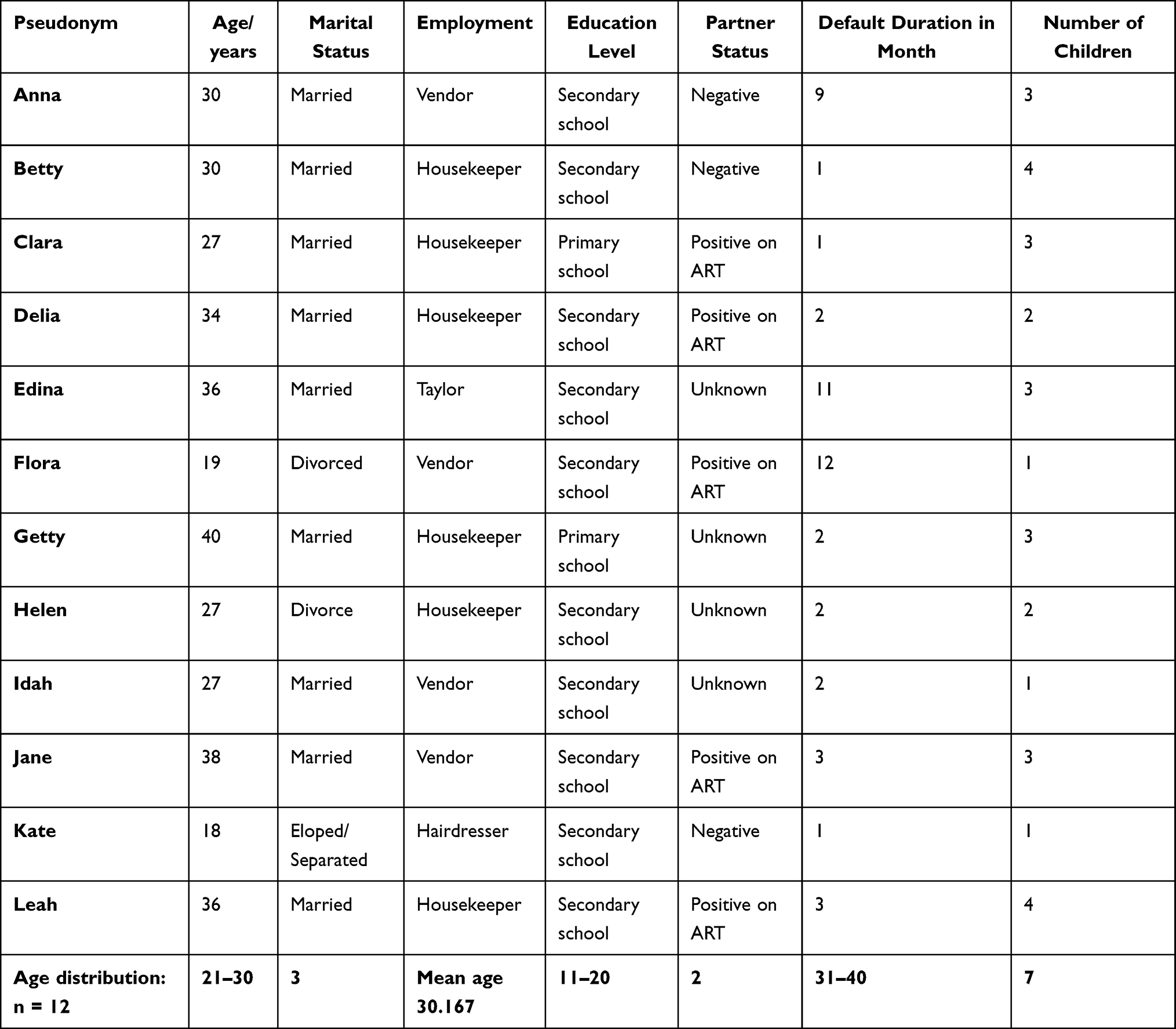 |
Table 1 Demographic Data of the Study Participants |
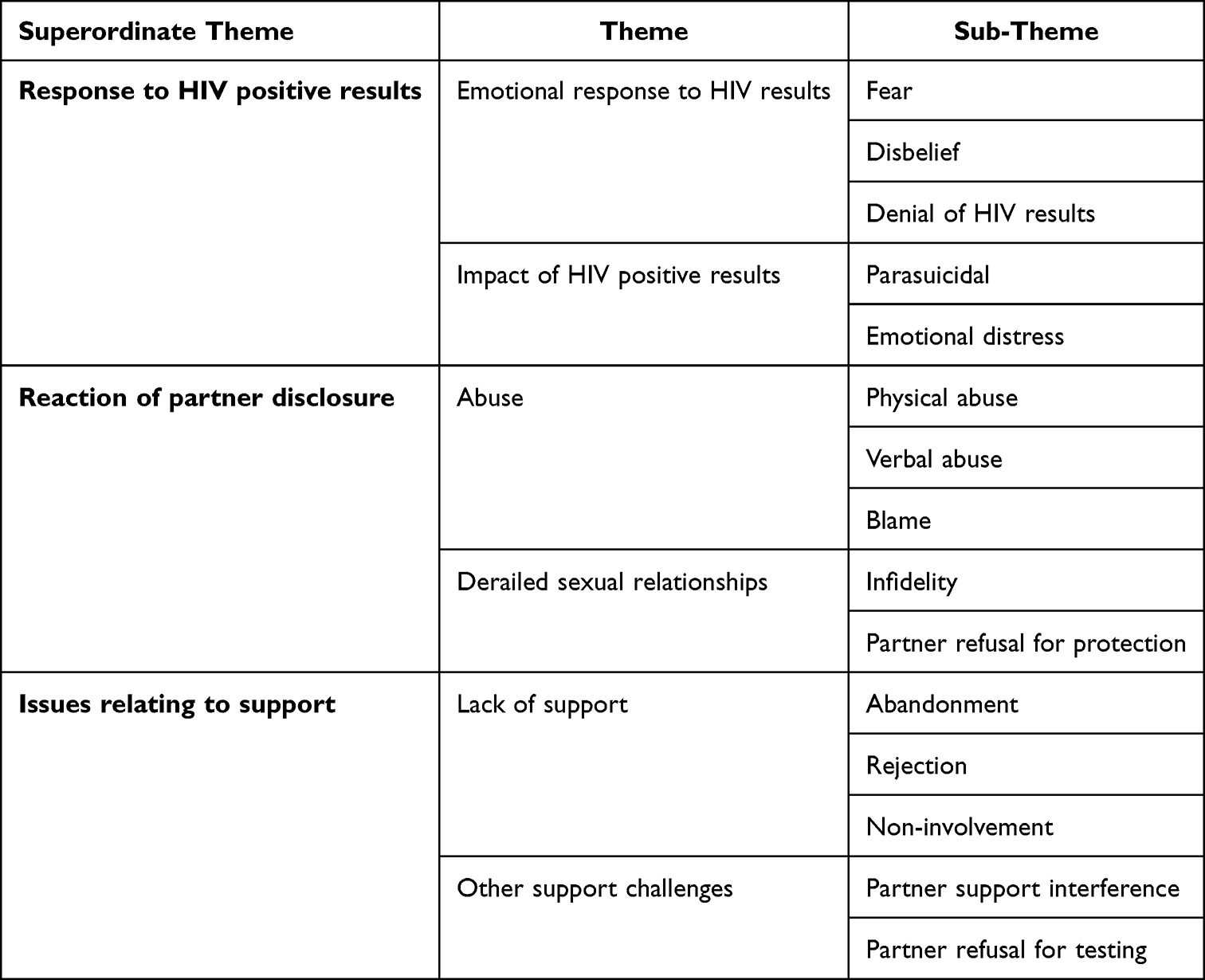 |
Table 2 Summary of Superordinate, Themes, and Sub-Themes |
Trustworthiness
The researcher followed the framework for ensuring trustworthiness explained by Lincoln and Guba.34 The framework includes credibility, dependability, conformability, transferability, and authenticity. Credibility, which is referred to as the truthfulness of data in representing the participant’s accurate view, experience, or belief, giving readers the confidence that the interpretations remain faithful to the insider view35 was maintained by the researcher. In this study, the interviews were conducted with women who defaulted treatment in the Option B+ programme and used Shona language to ensure clarity and understanding. According to Tobin and Begley36 dependability can be demonstrated through an audit trail, where others can examine the inquirer’s documentation of data, methods, decisions, and end product. To ensure dependability for this study, the researcher provided and maintained a detailed description of the research methodology undertaken throughout the study and conducted a pilot study on the interview guide to pick up questions that were misinterpreted or missed out. To ensure confirmability which is concerned with confirming that the researcher’s interpretations and findings are clearly obtained from the data,36 a record of the digitally recorded interview was transcribed verbatim and then coded. Themes were identified by both the researcher and an independent coder separately, compared and agreed on the differences. The direct quotes of the participants were used as verification of the presented themes at the time of presentation of the results. Transferability referred to as the extent to which qualitative findings can be transferred to or applicable in other settings or groups by Polit37 was ensured by the researcher. Authenticity emerges in a report when it conveys the feelings and tone of participants’ lives as they lived.38 To ensure authenticity, all audio recordings were transcribed and translated from Shona to English. To further ensure authenticity, verbatim quotations were presented as they had been recorded during interviews.
Results
Participants’ Demographic Data
A total of twelve participants were enrolled in Option B+ HIV treatment when pregnant from 01 January 2019 to 31 December 2019. The participants’ ages ranged from 18 to 40 years. All the participants were beneficials of Zimbabwe’s recommended ART regimens for pregnant and breast-feeding women as indicated in Table 3. Nine participants were married, and two were divorced, while one had eloped and then separated from the partner. One of the divorced participants re-married. Three participants had two children each, four participants had three children each, two had four children each, and three had one child each. Regarding education, seven participants completed secondary school. Three participants did not complete secondary school, and two participants completed only primary school. Regarding employment, five participants were housewives. Five were vendors, one was a hairdresser who plaited people’s hair, and the last one was a clothes designer and tailor. Table 1 depicts the demographics of the participants.
 |
Table 3 Recommended ART Regimens for Pregnant and Breast-Feeding Women |
The superordinate theme, themes, and sub-themes that emerged from the data analysis of the interview transcripts of the participants are discussed. The emerging theme is discussed under a separate heading. The participants’ views are presented as direct quotations that are indented and italicised to support the identified superordinate theme, themes, and sub-themes.
Response to HIV Results
During pregnancy, antenatal care (ANC) routinely provides an opportunity for women to have HIV counselling and testing and enrolment into Option B+ HIV treatment for the prevention of mother-to-child transmission of HIV. Pregnant women who test negative at the first visit would routinely repeat pregnancy HIV counselling and testing every three months throughout. In this study, all participants tested HIV positive at the first ANC visit except for Betty, who initially tested negative with her partner. After three months, she tested positive, and her partner negative again. This superordinate theme focuses on the emotional response to HIV positive results and the emotional impact of HIV results on participants.
Emotional Response to HIV Positive Results
Emotional reactions experienced by participants to the news of being HIV positive were varied. In describing their feelings after receiving their positive HIV results, words such as hard, difficult, troubling, stressing, disturbed were often present in the participants’ stories. Three sub-themes emerged in exploring the above theme: fear, disbelief, and denial of HIV results.
Fear
In some participants, an HIV-positive result aroused fear during pregnancy as they began to think deeply about the truth of being HIV-positive. Several types of fear became apparent to them. Throughout pregnancy and after delivery, many participants were filled with the fear of dying.
Edina testified about the fear of dying. She explained as follows:
I had some fear that if I die today, what about this baby? At the same time, I am carrying another baby, and I will leave these other children in poverty. (Edina, married, 36 years)
I am mostly afraid of my baby; I fear so much as I want him to remain negative. My baby should not be positive. I pray that God keeps me alive until my baby is grown up. (Delia, married, 34 years)
Disbelief
Some participants experienced the news of being HIV-positive with disbelief. They asked themselves as to where the infection came from looking at how some were living, she was living and how healthy they were, the following experiences illustrate:
It troubled me in my life because I never expected that I am a person who would be told that I am infected with it. What I was, and the way I was living, and how healthy I was, until I planned to have another baby, I did not know that I had this infection. But when I came to know about it when I got pregnant and went to register the pregnancy, it was something that troubled me and could not believe it. (Leah, married, 36 years)
Denial of HIV Status
Denial in the form of non-acceptance was identified in the study. This sub-theme explains what happens soon after the sad news is delivered, and a person is in shock. The person does not believe what has happened and may say: “This can’t be true”. Participants expressed it in words such as “hard to accept”; “difficult to accept”; “troubled”. Some participants were troubled. They found it difficult to accept their HIV-positive status because they had no symptoms and they felt well. This is supported by the following except:
What troubled me was that I was well with no symptoms. I was not sick. Even when I was told that I was HIV positive, it was difficult for me to accept as I was well. I was only treated once for a sexually transmitted disease together with my husband. It was hard to accept my HIV status as I was not sick. Even if you look at me now, do you see me as a sick person? For me to be said I am HIV-positive when my husband is negative and not sick. It is hard for me to understand because he is the only man I had. I do not understand where I got this HIV infection. It troubles me. (Anna, married, 30 years)
Impact of HIV Positive Results
The results of HIV can have a significant impact on individual diagnosed with HIV. This may also disrupt their lives including their mental health. Some participants experienced emotional and mental challenges related experiencing parasuicidal thoughts including emotional distress.
Parasuicidal
Some participants experienced mental health challenges such as suicidal tendencies after being diagnosed as HIV-positive. They were overwhelmed by the desire and feeling to commit suicide due to the depressive event of receiving an HIV-positive result, as testified below:
What I experience is that it troubled me so much to disclose to my husband that at one time I thought of killing myself. I was stressed. When I tested HIV-positive, I failed to understand it properly. So, I said, it is better for me to die because it is also the same with dying. (Flora, divorced, 19 years)
Emotional Distress
Some participants could not adhere to treatment resulting in defaulting because of the continued distress they suffered in their marital relationships.
He never stopped accusing me yet myself. I had never known the door of a beerhall, he found me a virgin after finishing my school, and he disturbed me. The way he scolds me was the reason why I stopped taking my treatment up to now. Moreover, the way he looks after me, he no longer cares for the children and me. (Leah, married, 36 years)
Reaction to Partner Disclosure
Not everyone facing challenges respond with ease in issues relating to HIV and disclosure. Women find themselves as continuously being victims of abuse in different ways in their own homes. This theme describes the reaction of partner to disclosure including the effects this had on their derailed sexual relationships.
Abuse
Abuse was reported in various ways and has impacted on participants despite status quo in the relationship. Abuse is regarded as any behaviours that can harm the next person either physically, psychologically, emotionally, sexually or in way that can prove an unacceptable behaviour cruelly. This theme describes the reaction of partner disclosure and its effects on participants’ experiences.
Physical Abuse
On disclosure of results by participants, some partners’ reactions were hostile, violent, and physically abusive to participants, as illustrated by the narratives below:
On disclosing to the husband, violence erupted in the home. My husband slapped me in the face saying, where did you get this from? (Getty married, 40 years).
Verbal Abuse
Some participants experienced verbal abuse because of disclosure of their HIV results, which pained them.
Yes, being scolded, as he goes on to say, I infected you while you were just seated here, what can you do to me, I made you bore children for me, you are here, you will not go anywhere, you wash for me, there is nothing you will do. So, I see as if he takes me as a slave, just being used. (Leah, married, 36 years)
Blame
As a result of participants’ disclosure of their HIV results to partners, some partners blamed the pregnant participants for bringing HIV into the relationship. The blame game did not only occur in discordant couples but also in couples who were both HIV-positive.
What happened is, he is suspecting that I got the infection from somewhere, while he says he, himself, is not infected. But the way I see it, he has not been tested. So, he is harassing me every day because of saying, where did you get the infection from?. (Getty, married, 40 years)
Below, a partner who had not been tested blamed the participant for the HIV infection and threatened her about going to look for another woman who is not infected with HIV. However, later when he was tested, he was found HIV positive. Leah described the experience below:
When I told my husband after registering for the pregnancy of this child I have, for a moment, he remained quiet. So, I was troubled about why he is not answering me. I repeated telling him until he ended up telling me, saying, that is your own problem. I am going to look for another woman who does not have that infection. He never stopped accusing me, yet I have never known the door of a beerhall, he found me a virgin after finishing my school, and he disturbed me. This troubles me. In my mind, I wish if he had left me alone and let me carry on with my life. (Leah, married, 36 years)
Derailed Sexual Relationships
While sexual relationships are meant to be enjoyed by many couples to strengthen their relationships. This is not always for those living and are affected by HIV status of their partners. Derailed sexual relationship among couples was reported to have had a negative impact on participants and impacted on their quality of their lives. This theme will be discussed under the following: infidelity, lack of support, partner interference and partner refusal for testing.
Infidelity
In the study, it was found that being diagnosed with HIV and the disclosure of the HIV status to partners negatively impacted on the marital relationships of the participants. In addition to the previously mentioned physical abuse, abandonment, blame and verbal abuse, other issues that negatively impacted marital relationships due to the disclosure of HIV results include partner’s infidelity. The following are the participants’ narratives of their experiences:
Participant testifies how, after disclosure of status, refusal to use condoms by the partner and his infidelity disrupted their marriage.
I am going to look for another woman who does not have that infection. At times he does not sleep at home for one week, he is not at home, and coming back may be after two months, leaving me all by myself and the children. When he comes, he will lie to me that he had gone there and there, but I now knew that this man, it is his behaviour of infidelity. (Leah, married, 36 years)
Partner Refusal for Protection
It is important to use protection when one partner is infected with HIV. Risk reduction behaviour contributes positively to the reduction of new HIV incident cases. Below participants narrated their experiences on the refusal of partners to use protection in the form of condoms.
When we were tested, were advised to use condoms and me to continue taking my tablets so as not to infect him. During the first days, he agreed to use condoms, but later, he refused and said he could not continue to use condoms. (Anna married, 30 years)
Issues Relating to Support
Many couples in relationships value support for each other since this not only proves care and love for each other but can provide a holistic emotional relief especially during challenging times to reduce stress and improve the quality of life. The issue of lack of support was reported as a concern by participants.
Lack of Support
Issues relating to support were indeed reported to be challenging and contributed negatively to participants’ lives. This theme will be discussed under lack of support and will be supported by the following sub-themes, namely, abandonment, rejection, and non-involvement.
Abandonment
In the study, it was found that some partners threatened the participants with abandonment, while others abandoned them or rejected them when they disclosed their HIV results to them, as illustrated below:
First, I had no one to support me. Then, my husband started rejecting, neglecting, and abandoning me for another woman. From the time I tested positive, he was coming home every day but late. Now he is coming three days a week at midnight or early in the morning. So, I cannot say he is at home. I heard that he has another woman. When I asked him about it, he said, there was no point of living with a person who will infect him with HIV. (Anna, married, 30 years)
The participant below narrates how the owner of the pregnancy abandoned her for good when she went to register the pregnancy which revealed that she was HIV-positive. However, she later married another man who had his own children.
Yes, my partner, the owner of the pregnancy had refused saying, I thought we would end up in only having a good time, now the issue of the baby is your own responsibility. (Edina)
Rejection
This abandonment was not only limited to partners but also some family members also contributed to the negative rejected of participants due to being pregnant. This is supported by the below except:
When I became pregnant, the people who were looking after me, my grandfather and grandmother refused to take me back after I had come back from my husband and his parents’ home where I was staying when I eloped. My grandfather refused to take me back and stay with him as his granddaughter saying he was not able to look after a granddaughter’s child. Maybe considering my HIV status, he thought the baby that was going to be born was also going to be HIV positive such that the burden was going to be heavy for him. (Kate)
Non-Involvement
Some participants shared that they stopped treatment because of a lack of non-involvement support from partners. The support could have been in any form as described by participants in the following narratives:
Support for food in order to take tablets was lacking. I had not enough food to take tablets and to continue with breastfeeding. The tablets made me vomit and weak. With the advice of exclusive breastfeeding, it was hard to get good food. All this made me stop taking my tablets. (Annah, married, 36 years)
Other Support Challenges
Partner Support Interference
The following narratives explain participants’ experiences from Sero-discordant and HIV-positive partners after disclosure of the HIV-positive results:
When I started treatment when I was pregnant, it was a problem for me to take my tablets when he was around. He would become violent, saying, ‘in my house no one takes tablets, if you do that, you will go back to your parents.’ There was a time when I would not take the tablets because he was around. At times I would skip taking the tablets. When he was not there, I would take. (Flora)
Partner Refusal for Testing
About four out of twelve participants complained about their partners’ refusal to be tested for HIV. Idah’s stress due to her HIV-positive status was made was worse by her partner’s refusal to test for HIV.
For the time I have stayed with him, I heard some relatives who were saying, the wife who was here passed on and the way she died we heard that she was taking her pills from next door. I, myself, had disclosed to him not knowing if he is still or was taking pills because if you say, ‘let us go and be tested,’ he refuses. (Edina, married, 36 years)
Discussions
The study found that after testing for HIV participants experienced different emotional responses such as fear, disbelief, and denial of HIV results. The impact of HIV positive results further resulted in participants experiencing parasuicidal and emotional stress on receiving their HIV-positive results when they first registered their pregnancy at the antenatal clinic. This finding is affirmed by Kotzé et al,39 who state that receiving HIV-positive results during pregnancy is a distressing experience for women who are made vulnerable to various emotions as they must deal with pregnancy, fear of transmission of HIV to the baby, disclosure of HIV status, and the decision to start lifelong ART. In relation to fear, participants expressed the fear of infecting the unborn baby with HIV. This is similar to the findings by Tagutanazvo et al,40 where it was shown that women experienced fear of infecting the unborn baby when they become aware of their HIV-positive status. In Malawi, the fear of disclosing an HIV status to avoid potential stigma and discrimination was the main reason for defaulting from ART. In central Thailand, some participants feared disclosing to parents because they feared that parents would not be able to deal with the shocking news, which is similar to the current study’s findings. In receiving their HIV-positive results, participants in this study experienced disbelief as they never expected it.
The findings of this study are also consistent with the findings of Minnaar and Bodkin41 in their study on the mourning process of HIV-positive pregnant women where the women reacted with shock and disbelief when they were informed that they were HIV positive. Masquillier et al42 acknowledges that in their study, PLWHA reacted with disbelief to their HIV-positive test results and some household members reacted in a similar manner when a patient disclosed her status to them. Masquillier et al42 further assert that disbelief driven by lack of knowledge or understanding about the infection and misconceptions about HIV transmission in the family can cause HIV stigma and stop preventive measures such as using protection like condoms. This was also reported in a study conducted by Lelaka et al16 that HIV positive participants and their partners found themselves in disbelief after receiving their results. Some went to the extent of insisting on having retests.
In relation to denial, the sentiments expressed by women in this study are a clear indication of the difficulty they experienced in accepting the HIV-positive diagnosis. They did not expect it because they were asymptomatic, and some had partners who tested negative. It is common to most people diagnosed with HIV to experience different emotional results including shock, denial and disbelief. This is similar to the study conducted16 that some participants reported that their partners reacted with denial to their HIV status results. A study conducted in Cameron further confirmed that the participants defaulted from treatment due to denial of their HIV status.43 This was also supported by Mavhandu-Mudzusi et al44 that though some participants expressed denial, the results brought intense fear and panic which was based on the assumptions that being diagnosed as HIV positive is a one-way ticket to the grave, while other participants verbalised that their fear was related to knowledge of a relative or someone who died of HIV and AIDS-related conditions. In Cape Town, South Africa, women experienced denial on learning their status at antenatal clinics (ANC). These findings are consistent with the findings of this study. In relation mental health as being parasuicidal, women’s experiences of thoughts of wanting to kill themselves and feeling that it was better for them to die as they reflected in a study similar to that found in Connecticut by Simpson and Forsyth.45 The pregnant women in Connecticut experienced suicidal thoughts after receiving an HIV-positive result. Participants in a study conducted by Ahmed et al46 experienced thoughts of dying with loss of hope which hindered them from seeking or continuing with treatment as they held the belief that they will soon die after all. In another study conducted in Ethiopia by Lifson et al,47 most participants believed that HIV diagnosis was a death sentence. Emotional distress, leading to the stopping of treatment, was experienced by participants in this study from continually being blamed for bringing HIV into the family and being scolded and harassed when seen taking medication by partners. In a study conducted by Sariah et al,48 emotional stress, leading to the stopping of treatment, was also experienced by participants, findings which are comparable to the findings of this study.
The findings of this study also suggested that women experienced negative reactions that impacted their sexual relationships on disclosing their HIV-positive results to their partners. The findings also suggested that women felt that being HIV positive strained relationships within their marriages. Women faced a dilemma in disclosing to their partners and feared divorce and violence following disclosure. They experienced physical abuse, abandonment and rejection, blame, verbal abuse, infidelity of partners, lack of partner support, partner interference, partner refusal for testing and partner refusal for protection which disrupted the family in this study. These experiences were reported among pregnant women in other studies. In Uganda, LTFU women described experiencing physical, verbal, and psychological abuse by their husbands or other family members as a result of their disclosure of HIV-positive results and participation in the PMTCT programme and this led to the stopping of treatment.8
Other issues relating to the lack of support included abandonment, rejection and non-involvement of partner were identified in a study conducted by Njunga and Blysta49 in rural Malawi where all of the nine mothers in the in-depth interviews reported that their families were disrupted after they had disclosed their HIV-positive status to their partners. Their partners abandoned them. In another study conducted by Atuyambe et al,50 disclosure led to rejection or outbursts, leading to instances of couples separating beds. In this study, some participants reported that it was difficult to continue taking their treatment due to the non-involvement and they lacked support from their partners after disclosure of their results. Others reported that their partners were no longer providing them with basic needs like food, which enabled them to take their treatment. Consequently, they stopped taking treatment. Similar findings were revealed in a study conducted by Chadambuka et al,13 where non-involvement or poor partner support or lack of it was found as a constraint to ART adherence. In a study conducted by Lelaka et al,16 participants reported the importance of emotional support being a crucial link in the treatment process of an HIV-positive individual as this helps to create peace of mind and a sense of belonging. These findings were also identified in a study conducted in Malawi by Cataldo et al,51 where it was reported that loss to follow-up (LTFU) mothers verbalised treatment defaulting due to lack of male partner support. Infidelity of partners following disclosure of HIV-positive results in this study was observed, this was also reported in a study in Malawi and Uganda where it was shown to be a major barrier to HIV status disclosure and uptake of HIV testing services within couples partly because a positive test result signifies infidelity.52 In a study conducted by Conroy et al,53 the findings revealed that some spouses would prefer not to know their HIV status, or do so secretly, to prevent conflict and possibly loss of benefits of marriage. Further, in other studies, it was observed that disclosure of HIV results caused partner refusal for HIV testing, lack of of partner support, partner interference, partner refusal for HIV testing and partner refusal for protection similar to this study. However, the goal of disclosure of one’s HIV status is to share one’s challenges and get the support that enhances access to care.54
Other support challenges reported included partner interference which hindered women from adhering to treatment. Participants stated that they were forbidden from taking their treatment, and if seen doing so, violence erupted. This was similar to studies conducted on pregnant and breastfeeding women in Option B+ in sub-Saharan Africa by McLean et al,55 where women defaulted treatment due to partners not allowing them to take their medication or to visit the clinic. This agrees with a study that was conducted in Zimbabwe by Scott et al56 in that men stopped their partners from going to the hospital to collect treatment or stole their ARVs for their use secretly or prevented them from attending clinics or support groups. Similar findings were reported in an early study conducted in Zimbabwe by Skovdal et al57 in that it was revealed that men threatened divorce to their partners if they took ARVs. In relation to partner refusal for HIV testing and protection after disclosure of HIV results observed in this study, these findings were also observed in other studies. In Papua, Indonesia, partners refused to go for HIV testing and resorted to violence and prevented women from taking their treatment.58 In an early study conducted in Zimbabwe by Skovdal et al,57 it was identified that men refused to use condoms threatening their partners with the risk of reinfection. These disagreements brought disharmony in the family.
Limitations of the Study
The study was limited to two Chitungwiza Municipality clinics, and the study findings cannot be generalized to other municipal clinics as well as other health facilities in Chitungwiza town. Since all participants had delivered by the time of the interviews and were breastfeeding, interruptions due to babies’ crying occurred, affecting one or two participants’ concentration. The study was conducted in an urban area, and rural women were excluded.
Conclusion and Recommendations
This study’s findings revealed the emotional and psychosocial profile of women who defaulted Option B+ HIV treatment in Chitungwiza municipality clinics. The psychosocial emotional experiences reported included fear, disbelief, denial, emotional stress, and suicidal ideation on receiving HIV-positive results when they were pregnant. On disclosure of results to partners, they further experienced physical abuse, verbal abuse, and shame. Due to disclosure of HIV, they further faced abandonment, rejection, and non-involvement of the partner. Partner interference contributed negatively to participants' quality of life because they were not able to adhere and comply to their HIV treatment. Partner refusal for protection from partners also destabilized marriages and hindered the participants from taking responsibility to adhere to treatment leading them to default from treatment. Interventions to reduce defaulting among women on Option B+ HIV treatment to enhance treatment adherence should focus more on strengthening and promoting comprehensive and integrated couple HIV counselling and testing, enhancing and promoting mental health services, male partner support through community sensitization and involvement of male partners in the PMTCT of HIV programmes to encourage disclosure of HIV results and acceptance and adherence to ART as identified by Chadambuka et al.13 Encouraging and enforcing couple HIV counselling and testing will reduce gender-based violence, encourage acceptance of HIV status and promote risk reduction behaviour which will improve the quality of life of pregnant or breastfeeding mothers as this will reduce the psychological effects resulting from a new unexpected HIV-positive result as shown in a Malawian study conducted by Wesevich et al.59 Addressing stigma and discrimination through community sensitisation and education involving community leaders on the updated information and the benefits of Option B+ HIV treatment.
Institutional Review Board Statement
Ethical approval was obtained from the University of South Africa, Department of Health’s Ethics Committee HSHDC/952/2020 prior to data collection.
Informed Consent Statement
All participants provided voluntary written informed consent prior to data collection. Confidentiality and anonymity of participants were respected throughout the research process.
Data Sharing Statement
The participants provided consent that their responses provided in this manuscript and Table 1 can be shared and published as anonymous. During the recruitment process, trust and rapport building was built, and the anonymity principle was implemented to protect participants privacy, to observe and uphold research ethical principles. Consent was also provided from participants to publish the related data using pseudonym names. Therefore, the names and quotes used are pseudonyms and do not reflect any of the participants' real names.
Acknowledgment
The authors thank all the support of the following: all women participated in the study and shared their experiences, University of Zimbabwe, the staff at the clinics as well as the Department of Health Services of Chitungwiza Municipality Head Office for proving permission to conduct the study. The author also wishes to thank Dr Constance Matshidiso Lelaka and Prof Azwihangwisi Helen Mavhandu-Mudzusi for their support in putting together the manuscript.
Disclosure
The authors declare that there are no competing interests in this work.
References
1. Onoya D, Sineke T, Brennan AT, Long L, Fox MP. Timing of pregnancy, postpartum risk of virologic failure and loss to follow-up among HIV-positive women. AIDS. 2017;31(11):1593. doi:10.1097/QAD.0000000000001517
2. Antiretroviral TS. Guideline on When to Start Antiretroviral Therapy and on Pre-Exposure Prophylaxis for HIV. World Health Organization; 2015.
3. Avert. At a glance: HIV in Zimbabwe 2021; 2023. Available from: https://www.avert.org/professionals/hiv-around-world/sub-saharan-africa/zimbabwe.
4. Avert. HIV and AIDS in Zimbabwe (Posted on 6 September 2020). UK: Avert; 2019. Available from: https://www.avert.org/professionals/hiv-around-world/sub-saharan-africa/zimbabwe.
5. Herald T. Target to end HIV within reach: VP. Zimbabwe: The Herald; 2021. Available from: https://www.herald.co.zw/zim-achieves-hiv-prevention-target/.
6. Pembere K. MILESTONE: zim attains 95-95-95 HIV targets. Health times; 2022.
7. World Health Organization. Consolidated Guidelines on the Use of Antiretroviral Drugs for Treating and Preventing HIV Infection: Recommendations for a Public Health Approach. World Health Organization; 2016.
8. Flax VL, Yourkavitch J, Okello ES, Kadzandira J, Katahoire AR, Munthali AC. “If my husband leaves me, I will go home and suffer, so better cling to him and hide this thing”: the influence of gender on Option B+ prevention of mother-to-child transmission participation in Malawi and Uganda. PLoS One. 2017;12(6):e0178298. doi:10.1371/journal.pone.0178298
9. Chimwaza AN, Tweya H, Mugurungi O, et al. Early retention among pregnant women on ‘Option B+’in urban and rural Zimbabwe. AIDS Res Ther. 2021;18:1–8. doi:10.1186/s12981-021-00333-3
10. Mulewa P, Satumba E, Mubisi C, Kandiado J, Malenga T, Nyondo-Mipando AL. “I was not told that I still have the virus”: perceptions of utilization of option B+ services at a health center in Malawi. J Int Assoc Provid AIDS Care. 2019;18:2325958219870873. doi:10.1177/2325958219870873
11. Kiwanuka G, Kiwanuka N, Muneza F, et al. Retention of HIV infected pregnant and breastfeeding women on option B+ in Gomba District, Uganda: a retrospective cohort study. BMC Infect Dis. 2018;18:1–11.
12. Geremew H, Wolde A, Kassa GM. Incidence and predictors of loss to follow-up among women on option B+ PMTCT program in northwest Ethiopia. A retrospective follow-up study. PLoS One. 2023;18(1):e0280546. doi:10.1371/journal.pone.0280546
13. Chadambuka A, Katirayi L, Muchedzi A, et al. Acceptability of lifelong treatment among HIV-positive pregnant and breastfeeding women (Option B+) in selected health facilities in Zimbabwe: a qualitative study. BMC Public Health. 2018;18(1):1–8. doi:10.1186/s12889-017-4611-2
14. Care ZMoHC. Ministry of Health and Child Care, Zimbabwe; 2017.
15. Zimbabwe U. Electronic Patient Management System-Epms Zimbabwe. Harare: UNDP Zimbabwe; 2015.
16. Lelaka CM, Moyo I, Tshivhase L, Mavhandu-Mudzusi AH. Psychosocial support for HIV serodiscordant couples. Health Psychol Behav Med. 2022;10(1):537–556. doi:10.1080/21642850.2022.2084098
17. McNatt Z, Boothby NG, Wessells MG, Lo R. Guidance note on psychosocial support: facilitating psychosocial wellbeing and social and emotional learning; 2018.
18. Okonji EF, Mukumbang FC, Orth Z, Vickerman-Delport SA, Van Wyk B. Psychosocial support interventions for improved adherence and retention in ART care for young people living with HIV (10–24 years): a scoping review. BMC Public Health. 2020;20(1):1–11. doi:10.1186/s12889-020-09717-y
19. Mukumbang FC, Knight L, Masquillier C, et al. Household-focused interventions to enhance the treatment and management of HIV in low-and middle-income countries: a scoping review. BMC Public Health. 2019;19(1):1–14. doi:10.1186/s12889-019-8020-6
20. Qutoshi SB. Phenomenology: a philosophy and method of inquiry. Int J Educ Dev. 2018;5(1):215. doi:10.22555/joeed.v5i1.2154
21. Christensen M, Welch A, Barr J. Husserlian descriptive phenomenology: a review of intentionality, reduction and the natural attitude. J Nurs Educ Pract. 2017;7(8):113–118. doi:10.5430/jnep.v7n8p113
22. Magnussen L, Amundson MJ, Smith N. Through the eyes of women: cultural insights into living as a battered woman in Hawaii. Nurs Health Sci. 2008;10(2):125–130. doi:10.1111/j.1442-2018.2008.00383.x
23. World Urban. 2017. Executive summary; 2017. Available from: https://www.metropolis.org/alliances/world-urban-campaign.
24. Apollo T, Takarinda KC, Phillips A, Ndhlovu C, Cowan FM. Provision of HIV viral load testing services in Zimbabwe: secondary data analyses using data from health facilities using the electronic Patient Monitoring System. PLoS One. 2021;16(1):e0245720. doi:10.1371/journal.pone.0245720
25. Agency ZNS. Zimbabwe Population Census, 2012. Zimbabwe National Statistics Agency; 2012.
26. Asiamah N, Mensah H, Oteng-Abayie EF. General, target, and accessible population: demystifying the concepts for effective sampling. Qual Rep. 2017;22(6):1607–1621.
27. Polit DF, Beck CT. Nursing Research: Generating and Assessing Evidence for Nursing Practice. Wolters Kluwer; 2021.
28. Degeling C, Rock M. Qualitative research for one health: from methodological principles to impactful applications. Front Vet Sci. 2020;7:70. doi:10.3389/fvets.2020.00070
29. Moser A, Korstjens I. Series: practical guidance to qualitative research. Part 3: sampling, data collection and analysis. Eur J Gen Pract. 2018;24(1):9–18. doi:10.1080/13814788.2017.1375091
30. Polit DF. Nursing Research: Generating and Assessing Evidence for Nursing Practice. Philadelphia: Wolters Kluwer Health; 2017.
31. Grove SK, Burns N, Gray J. The Practice of Nursing Research: Appraisal, Synthesis, and Generation of Evidence. Elsevier Health Sciences; 2012.
32. Lewis S. Qualitative inquiry and research design: choosing among five approaches. Health Promot Pract. 2015;16(4):473–475. doi:10.1177/1524839915580941
33. Praveena K, Sasikumar S. Application of colaizzi’s method of data analysis in phenomenological research. Med Leg Updat. 2021;21(2):914–918.
34. Lincoln Y, Guba E. Naturalistic Inquiry London Sage Publications; 1985.
35. Moule P, Aveyard H, Goodman M. Nursing Research: An Introduction. Sage; 2016.
36. Tobin GA, Begley CM. Methodological rigour within a qualitative framework. J Adv Nurs. 2004;48(4):388–396. doi:10.1111/j.1365-2648.2004.03207.x
37. Polit DF. Nursing Research: Generating and Assessing Evidence for Nursing Practice. Philadelphia: Wolters Kluwer; 2021.
38. Polit DF, Beck CT. Nursing Research: Generating and Assessing Evidence for Nursing Practice. Lippincott Williams & Wilkins; 2008.
39. Kotzé M, Visser M, Makin J, Sikkema K, Forsyth B. Psychosocial variables associated with coping of HIV-positive women diagnosed during pregnancy. AIDS Behav. 2013;17:498–507. doi:10.1007/s10461-012-0379-7
40. Tagutanazvo OB, Nolte AG, Temane A. Experiences of women enrolled in a prevention of mother to child transmission of human immunodeficiency virus infection programme in Zimbabwe. Health SA Gesondheid. 2019;24(1):1–7. doi:10.4102/hsag.v24i0.1088
41. Minnaar A, Bodkin C. The mourning process of HIV-positive pregnant women. Afr J Nurs Midwifery. 2009;11(2):3–15.
42. Masquillier C, Wouters E, Mortelmans D, Van Wyk B. On the road to HIV/AIDS competence in the household: building a health-enabling environment for people living with HIV/AIDS. Int J Environ Res Public Health. 2015;12(3):3264–3292. doi:10.3390/ijerph120303264
43. Atanga PN, Ndetan HT, Achidi EA, Meriki HD, Hoelscher M, Kroidl A. Retention in care and reasons for discontinuation of lifelong antiretroviral therapy in a cohort of Cameroonian pregnant and breastfeeding HIV‐positive women initiating ‘Option B+’in the South West Region. Trop Med Int Health. 2017;22(2):161–170. doi:10.1111/tmi.12816
44. Mavhandu-Mudzusi AH, Lelaka MC, Sandy PT. The experiences of HIV-serodiscordant couples at the perinatal HIV research unit in Soweto, South Africa. Stud Ethno-Med. 2014;8(2):119–125. doi:10.1080/09735070.2014.11917626
45. Simpson BJ, Forsyth BW. State-mandated HIV testing in Connecticut: personal perspectives of women found to be infected during pregnancy. J Assoc Nurses AIDS Care. 2007;18(5):34–46. doi:10.1016/j.jana.2007.07.008
46. Ahmed SI, Farooqui M, Syed Sulaiman SA, Hassali MA, Lee CK. Facilitators and barriers affecting adherence among people living with HIV/AIDS: a qualitative perspective. J Patient Exp. 2019;6(1):33–40. doi:10.1177/2374373518770805
47. Lifson AR, Demissie W, Tadesse A, et al. Barriers to retention in care as perceived by persons living with HIV in rural Ethiopia: focus group results and recommended strategies. J Int Assoc Provid AIDS Care. 2013;12(1):32–38. doi:10.1177/1545109712456428
48. Sariah A, Rugemalila J, Protas J, et al. Why did I stop? And why did I restart? Perspectives of women lost to follow-up in option B+ HIV care in Dar es Salaam, Tanzania. BMC Public Health. 2019;19:1–11. doi:10.1186/s12889-019-7518-2
49. Njunga J, Blystad A. ‘The divorce program’: gendered experiences of HIV positive mothers enrolled in PMTCT programs-The case of rural Malawi. Int Breastfeed J. 2010;5(1):1–6. doi:10.1186/1746-4358-5-14
50. Atuyambe LM, Ssegujja E, Ssali S, et al. HIV/AIDS status disclosure increases support, behavioural change and, HIV prevention in the long term: a case for an Urban Clinic, Kampala, Uganda. BMC Health Serv Res. 2014;14(1):1–11. doi:10.1186/1472-6963-14-276
51. Cataldo F, Chiwaula L, Nkhata M, et al. Exploring the experiences of women and health care workers in the context of PMTCT option B plus in Malawi. J Acquir Immune Defic Syndr. 2017;74(5):517. doi:10.1097/QAI.0000000000001273
52. Conroy AA, Wong LH. How reliable are self-reports of HIV status disclosure? Evidence from couples in Malawi. Soc Sci Med. 2015;144:28–37. doi:10.1016/j.socscimed.2015.09.007
53. Conroy AA, McKenna SA, Comfort ML, Darbes LA, Tan JY, Mkandawire J. Marital infidelity, food insecurity, and couple instability: a web of challenges for dyadic coordination around antiretroviral therapy. Soc Sci Med. 2018;214:110–117. doi:10.1016/j.socscimed.2018.08.006
54. Liamputtong P. Women, Motherhood and Living with HIV/AIDS: A Cross-Cultural Perspective. Springer Science & Business Media; 2013.
55. McLean E, Renju J, Wamoyi J, et al. ‘I wanted to safeguard the baby’: a qualitative study to understand the experiences of Option B+ for pregnant women and the potential implications for ‘test-and-treat’in four sub-Saharan African settings. Sex Transm Infect. 2017;93(Suppl 3). doi:10.1136/sextrans-2016-052972
56. Scott K, Campbell C, Madanhire C, Skovdal M, Nyamukapa C, Gregson S. In what ways do communities support optimal antiretroviral treatment in Zimbabwe? Health Promot Int. 2014;29(4):645–654. doi:10.1093/heapro/dat014
57. Skovdal M, Campbell C, Nyamukapa C, Gregson S. When masculinity interferes with women’s treatment of HIV infection: a qualitative study about adherence to antiretroviral therapy in Zimbabwe. J Int AIDS Soc. 2011;14(1):1–7. doi:10.1186/1758-2652-14-29
58. Lumbantoruan C, Kermode M, Giyai A, Ang A, Kelaher M. Understanding women’s uptake and adherence in option B+ for prevention of mother-to-child HIV transmission in Papua, Indonesia: a qualitative study. PLoS One. 2018;13(6):e0198329. doi:10.1371/journal.pone.0198329
59. Wesevich A, Mtande T, Saidi F, et al. Role of male partner involvement in ART retention and adherence in Malawi’s Option B+ program. AIDS Care. 2017;29(11):1417–1425. doi:10.1080/09540121.2017.1308464
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.