Back to Journals » Advances in Medical Education and Practice » Volume 16
Grade Point Average as a Predictor of Work Performance Among Healthcare Professionals: A Systematic Review
Authors Al-Ziftawi N ![]() , Alhaj Moustafa D, ElKhalifa D, Wazne M, Ibrahim E, Awaisu A
, Alhaj Moustafa D, ElKhalifa D, Wazne M, Ibrahim E, Awaisu A ![]()
Received 26 November 2024
Accepted for publication 12 May 2025
Published 17 October 2025 Volume 2025:16 Pages 1879—1896
DOI https://doi.org/10.2147/AMEP.S508741
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Md Anwarul Azim Majumder
Nour Al-Ziftawi,1 Diala Alhaj Moustafa,1 Dana ElKhalifa,2 Maha Wazne,3 Eman Ibrahim,4 Ahmed Awaisu1
1College of Pharmacy, QU Health, Qatar University, Doha, Qatar; 2Pharmacy Department, Aspetar Hospital, Doha, Qatar; 3Pharmacy Department, Aman Hospital, Doha, Qatar; 4High Institute of Public Health, Alexandria University, Alexandria, Egypt
Correspondence: Ahmed Awaisu, Department of Clinical Pharmacy and Practice, College of Pharmacy, QU-Health, Qatar University, P.O.Box 2713, Doha, Qatar, Tel +974 4403 5596, Email [email protected]
Introduction: Grade point average (GPA) is a widely used measure of academic performance in educational programs. However, its correlation with real-world work performance among healthcare professionals is widely debated.
Objective: To systematically review the literature regarding the relationships between GPA and indicators of job performance and success among healthcare professionals.
Methods: A comprehensive search of the following electronic databases was conducted to retrieve studies published between January 2000 and December 2023: PubMed, EMBASE, CINHAL, and the Cochrane Library. Grey literature was also reviewed for eligibility using ProQuest and Google Scholar. Only original research involving healthcare practitioners after graduation was included in the study. The impact of GPA on relevant work performance indicators was summarized by healthcare professional group. The risk of bias was assessed using the National Institutes of Health (NIH) quality assessment tools.
Results: Fourteen original studies were included in this review. Of these, six studies focused on physicians, six on nurses, and two on pharmacists. Thirteen of the studies were observational cohort studies, whereas one was a case-control study. Four of the studies were rated as “good quality”, five as “fair quality”, and five as “poor quality”. The relationship between GPA and job performance indicators varied across the included studies and healthcare professionals. The findings showed inconsistent correlations: GPA weakly to moderately predicted physicians’ performance, influenced pharmacists’ pursuit of postgraduate training, and had variable effects on nurses’ critical thinking, emotional intelligence, and job turnover.
Conclusion: The link between GPA and work performance differed depending on the healthcare professional group and the specific performance indicator being measured. While GPA may impact certain professional outcomes, its predictive value varies across roles and settings, underscoring the need for further research to clarify its utility as a performance indicator in healthcare.
Keywords: GPA, grade point average, healthcare professionals, physicians, nurses, pharmacists, job performance, work performance indicators, academic achievement
Introduction
In today’s dynamic healthcare landscape, both healthcare systems and practitioners are confronted with escalating demands to meet higher expectations and deliver outstanding healthcare services, while striving to achieve new healthcare goals.1 Consequently, the demand for highly-skilled healthcare professionals has grown significantly, presenting a challenge for healthcare organizations to identify individuals who are both competent and reliable for their teams.1,2 Although various indicators and metrics have been examined to predict work performance in healthcare roles, academic achievement, particularly as reflected by Grade Point Average (GPA) during professional degree programs, has emerged as a potentially significant predictor of effectiveness.3
The study of factors influencing job performance has been a significant area of research in psychology since the early 20th century.4 GPA is widely regarded as a reliable predictor of job performance across different fields due to its accessibility and cost-effectiveness.5,6 In the healthcare sector, academic achievement, often measured by GPA, has been used to evaluate the performance of medical students, with higher GPAs indicating greater academic success.7–9 In the healthcare sector, where the quality of care directly impacts patient outcomes, it is crucial to understand the relationship between academic achievement and job performance.10 However, the degree to which GPA accurately reflects the skills and competencies required for effective performance in healthcare settings remains a topic of debate.11,12 For instance, a 1962 study in medicine found that only GPA from the two clinical years of medical school predicted residents’ performance, while GPA in basic sciences showed a weaker relationship, and pre-medical GPA had no relationship with job performance.13 Moreover, in another study done recently in 2024 that examined the association between medical school GPA and postgraduation success among 552 Kuwait University medical graduates, it was found that a higher GPA was linked to pursuing clinical fellowships, higher monthly income, greater career progress, and increased satisfaction with life and career.14 However, GPA did not predict pursuing postgraduate academic degrees, international practice, or research publications. Gender did not influence fellowship pursuit or international practice, suggesting that while GPA strongly predicts career success and satisfaction, other factors may be more relevant for academic and research achievements.14 On the other hand, GPA has been identified as the most significant predictor for graduate nurses passing the National Council Licensure Examination in the United States of America (USA).15 However, to our knowledge, there has yet to be a comprehensive and up-to-date review of the literature examining the relationship between GPA and work performance, especially among healthcare professionals.
This study aimed to systematically review the existing literature on the relationship between GPA and work performance among healthcare professionals. By exploring the predictive value of GPA for job performance in healthcare settings, this research seeks to offer valuable insights for stakeholders involved in the selection, training, and development of healthcare professionals.
Methodology
Sources and Search Strategy
A comprehensive literature search was conducted across several databases, including PubMed, Embase, CINAHL Ultimate, and the Cochrane Library. To capture grey literature such as abstracts and dissertations not indexed in traditional databases, additional searches were performed using Google Scholar and ProQuest. The search strategy was guided by the PICO (Population, Intervention, Comparison, and Outcome) framework that is described below in Population and Outcomes, with relevant keywords identified for each PICO component. Synonyms, related terms, and alternative spellings were also considered. Boolean operators “AND” and “OR” were used to refine the search by linking primary domains and connecting keywords within the same domain, respectively. Appropriate time filters were used to include studies published between 2000 and 2023. This was done to ensure the inclusion of recent evidence relevant to the evolving healthcare labor market and educational context. Mendeley software was initially used to remove duplicates, followed by Rayyan AI application for further refinement of the duplication removal process. The review protocol was registered on PROSPERO on July 3, 2023 (https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42023438503).
Population and Outcomes
This review included studies involving healthcare professionals who had completed a bachelor’s degree or an equivalent qualification enabling them to practice their respective professions. The following degree types were considered, which represent widely accepted educational standards that grant eligibility for professional practice in healthcare roles.
- Physicians: MD or MBBS degrees
- Pharmacists: BSc Pharm or PharmD degrees
- Nurses: Bachelor of Science in Nursing (BSN) or equivalent
- Dentists: Bachelor of Dental Surgery (BDS) or Doctor of Dental Medicine (DMD)
- Allied Health Professionals: Bachelor’s degrees in fields such as physiotherapy, occupational therapy, and clinical laboratory science
- Public Health Practitioners: Bachelor’s degrees in public health or health administration
The primary outcome of this study is postgraduation work performance at all career levels as measured by any appropriate indicator for any aspect of work performance. These indicators included clinical competence, decision-making abilities, and the delivery of high-quality patient care. Professional communication skills, teamwork effectiveness, and emotional intelligence were also considered as essential markers of job performance. Furthermore, leadership capabilities, participation in postgraduate training, and contributions to professional development were evaluated. Additional measures included career advancement, staff retention, and turnover rates, all of which capture the dynamic aspects of healthcare professionals’ performance in real-world practice environments. The following PICO format further illustrate the study outcomes:
- Population (P): Healthcare professionals who have completed a bachelor’s degree or equivalent enabling them to practice in their respective fields (eg, MD/MBBS for physicians, BSc. Pharm/PharmD for pharmacists, BSN for nurses, BDS/DMD for dentists, and equivalent degrees for other healthcare practitioners).
- Intervention (I): Grade Point Average (GPA) as an indicator of academic performance.
- Comparison (C): No specific comparison, but implicit comparisons were made between different levels of GPA and their association with outcomes.
- Outcome (O): Various indicators of work performance, including clinical competence, decision-making, communication skills, teamwork, leadership roles, postgraduate training pursuits, job satisfaction, retention rates, and contributions to professional development.
Eligibility Assessment
Following the literature search, the identified studies were uploaded to the Rayyan AI application and reviewed by two independent reviewers for screening and eligibility assessment. Studies were deemed eligible for inclusion if they were original research investigations published in full-text format, written in the English language, and published between 2000 and 2023. Studies were excluded if they were reviews, personal or expert opinions, conference abstracts only, or did not meet the PICO criteria. The inclusion/exclusion decisions were made using Rayyan by two independent reviewers in a blinded manner. Disagreements between the two reviewers were initially addressed through consensus; if consensus could not be reached, a third reviewer was consulted for an independent assessment. Finally, manual screening of the references from the articles deemed potentially eligible was performed according to the same criteria above.
Quality Assessment
The quality of each article included in the review was independently assessed by two reviewers using the National Institute of Health (NIH) Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies, or the NIH Quality Assessment Tool for Case-Control Studies, as applicable.16 The NIH Tool for Observational Cohort and Cross-Sectional Studies is designed to assess the methodological quality of cohort and cross-sectional studies and consists of 14 questions that address different aspects of study design and conduct. On the other hand, the NIH Tool for Case-Control Studies consists of 12 questions focused on assessing the methodological rigor and robustness of case-control studies. For each tool, the domains were rated as “yes”, “no”, “cannot determine (CD)”, “not applicable (NA)”, or “not reported (NR)”. A score of “yes” indicates that the study meets the criterion for that question, while a score of “no” or “NR” indicates that the study does not meet the criterion. A score of “NA” or “CD” denotes that there was insufficient information to determine whether the study meets the criterion or that the criterion does not apply.
Each question was assigned a numeric score of 1 if the answer was “yes”, and a score of 0 for all other response options. A study was classified as “good quality” if the overall score was at the 75th percentile or more, a “fair quality” if the score was between the 50th and the 75th percentiles and, and of a “poor quality” if the score was below the 50th percentile. For the NIH Tool for Case-Control Studies, a score of 9 or above was considered “good”, a score between 7 and 8 was considered “fair”, and a score of 6 or below was categorized as poor. Any discrepancies in the quality assessment were resolved by consulting a third reviewer.
Results
Search results
The comprehensive literature search yielded a total of 1316 studies: 235 from PubMed, 174 from EMBASE, 498 from CINAHL, and 24 from the Cochrane Library. In addition, 385 articles were identified from grey literature sources through Google Scholar and ProQuest. After removing 222 duplicates, the titles and abstracts of the remaining 1094 articles were screened for eligibility. From this initial screening, 11 studies proceeded to full-text review for eligibility.17–27 All 11 studies were confirmed eligible for inclusion. Further, the references of these 11 articles were manually reviewed, leading to the identification of three additional eligible studies based on full-text screening.28–30 The study inclusion process is outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram (Figure 1).
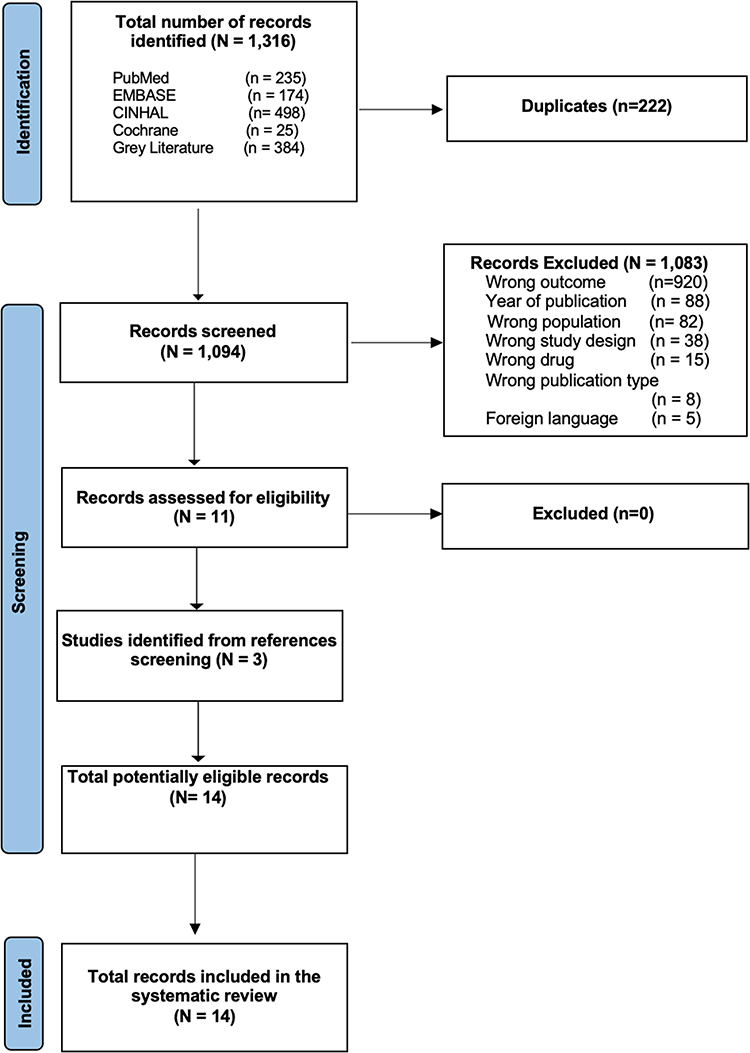 |
Figure 1 PRISMA flow diagram for the systematic review records. |
Characteristics of the Included Studies
Fourteen studies were included in this systematic review.17–30 These studies were published in various journals with varying quality levels, ranging from Q1 to Q3, according to the Scimago Journal Rank metrics. However, two of the studies were theses and dissertations available through ProQuest,24,26 while one study was published in “Dubai Medical Journal”, which is not ranked by Scimago.18 Thirteen of the included studies were cross-sectional,17–26,28–30 and one was a case-control study.27 The geographical distribution of the studies was diverse: nine from the United States of America,21,22,24–26,28–30 two from Australia,19,23 two from South Korea,17,20 and one from the United Arab Emirates (UAE).18 The studies were published between 2001 and 2023 and involved various healthcare professionals: six focused on physicians,18,19,23,27–29 six on nurses,17,20,21,24–26 and two on pharmacists22,30 only. The detailed characteristics of the included studies are summarized in Table 1.
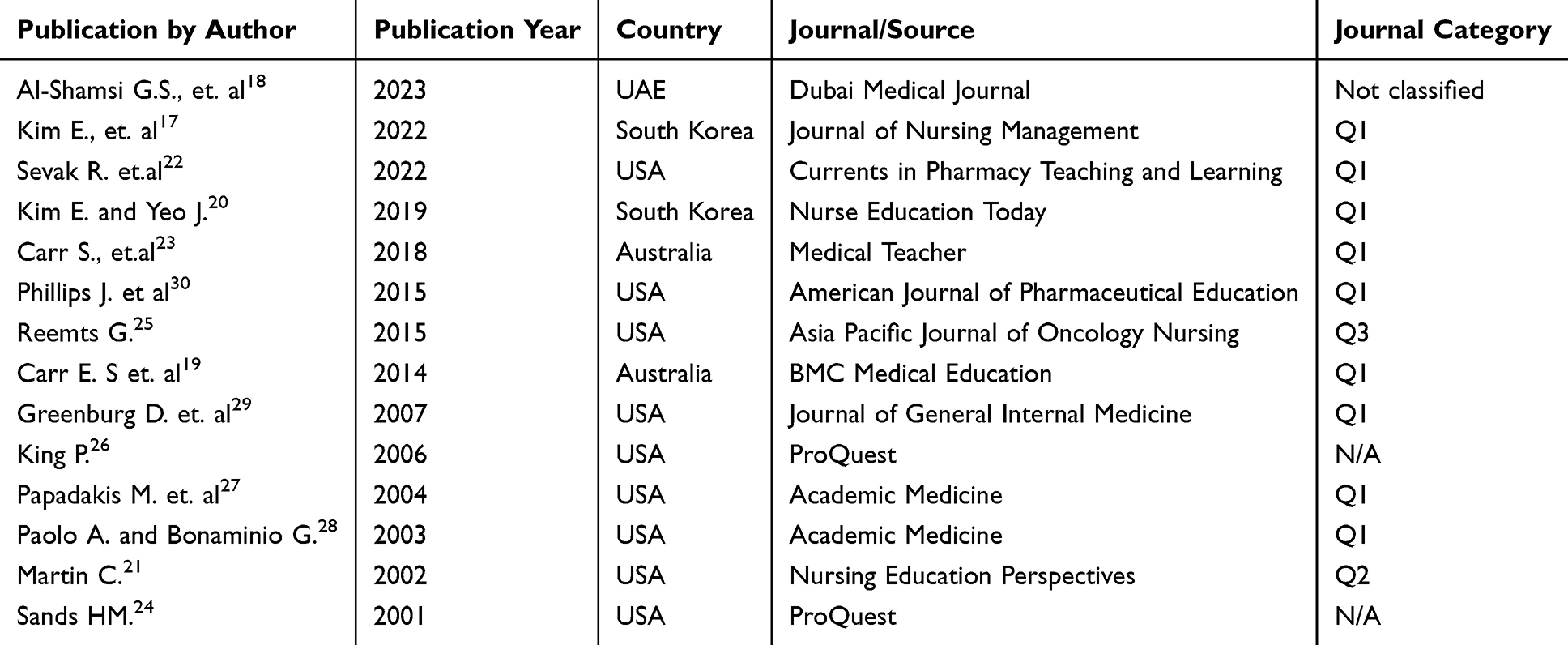 |
Table 1 General Characteristics of the Included Studies |
Quality Assessment of the Studies
Overall, four out of the 14 included studies were rated as “good quality”,17,23,27,29 five were rated as “fair quality”,19,20,24,25,28 and the remaining five were classified as “poor quality”.18,21,22,26,30 Among the 13 cross-sectional studies assessed, none complied with the quality assessment criterion for “outcome assessors’ blindness”, resulting in a 0% compliance rate. The criterion for “measurement of exposure at multiple times” was met by only one study, indicating a compliance rate of 8%. Moreover, “sample size calculations and power justification” criterion was addressed in only three of the 13 cross-sectional studies, reflecting a compliance rate of 23%. On the other hand, there was full compliance in the domains of “clarity of research objective”, “population definition”, and “measurement of exposure before the outcome”. This was followed by 92% compliance with the domain related to “clear definition and reliability of outcome”, with only one study not meeting this criterion. Additionally, the “uniformity of subjects’ recruitment” domain achieved a compliance rate of approximately 77%, with 10 out of 13 studies meeting the standard. The compliance rates for the remaining domains according to the NIH Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies were as shown in Figure 2. In contrast, the included case-control study showed 100% adherence to all the criteria of the NIH Quality Assessment Tool for Case-Control Studies. Figure 3 represents the compliance rates for the case-control study.
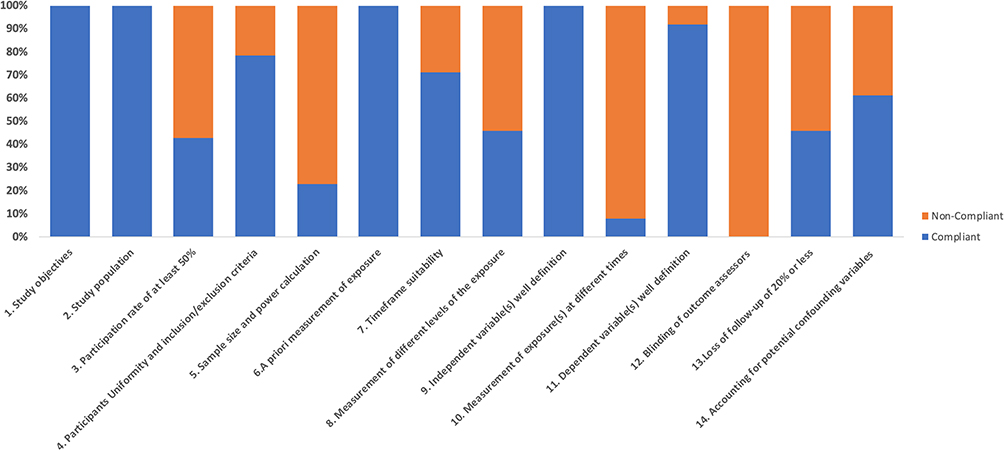 |
Figure 2 Compliance rate to each of the NIH Quality Assessment Tool for Observational and Cohort Studies. The quality of 13 out of the 14 included studies were examined using the NIH Quality Assessment Tool of Observational and Cohort Studies. Blue labeling represents compliance, and Orange represents non-compliance. |
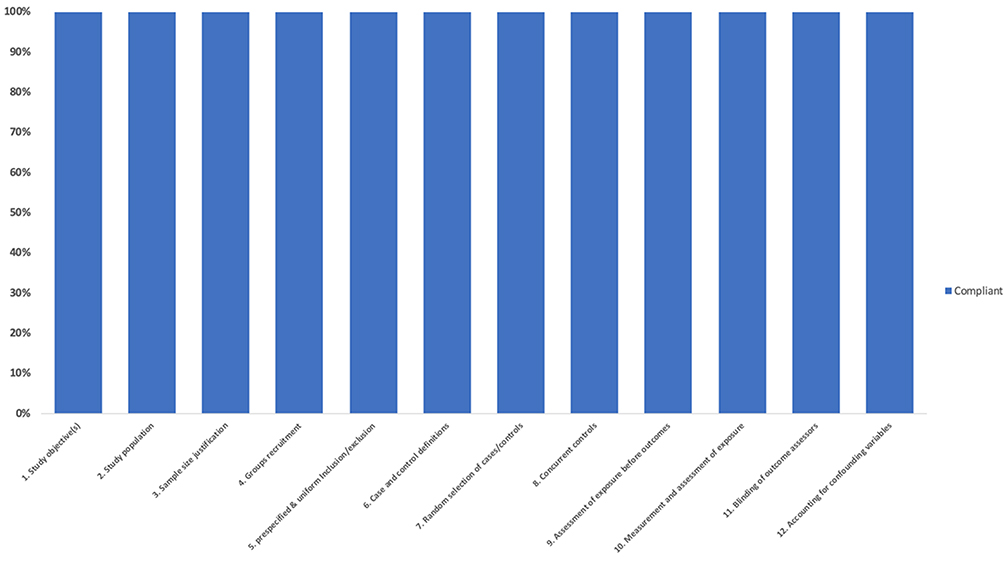 |
Figure 3 Compliance rate to each of the NIH Quality Assessment Tool for Case-Control Studies. The quality of one case-control study was examined and found in complete compliance of all the criteria of the NIH Quality Assessment Tool for Case-Control Studies. The study fully complies with all the criteria of NIH Quality Assessment Tool for Case-Control Studies. |
Study Outcomes
The included studies assessed a range of outcomes related to the relationship between GPA and the work performance of healthcare practitioners. Positive outcomes included performance measured by objective examinations, continuation of higher education, clinical management, communication skills, emotional intelligence, critical thinking, diagnostic reasoning, and professionalism. Negative outcomes reported included job turnover, transition shock, and disciplinary action. Overall, the outcomes were highly heterogenous and the ability of GPA to predict professionalism has shown inconsistent results across different professional groups and settings. A summary of the study outcomes is presented in Table 2. For clarity and comparison, the study outcomes were grouped according to the healthcare professional groups (ie, physicians, pharmacists, and nurses).
 |
Table 2 Results Summarization for the Included Studies with Their Objectives and Job-Performance Indicator as Classified Based on Healthcare Professional Practice |
Relationship Between GPA and Physicians’ Work Performance
GPA was examined as a measure of work performance, knowledge, and professionalism among physicians in six of the included studies.18,19,23,27–29 The Majority of them (n=5) focused on early career-level physicians, particularly those at the residency level.18,19,23,28,29 Only one study investigated the relationship between GPA and professionalism across all career-level physicians.27 Performance markers included objective assessment tools such as the Junior Doctor Assessment Tool (JDAT), which is a validated tool for evaluating clinical management, communication skills, and professional behavior, as well as the number of disciplinary actions taken against physicians.19,23 However, the remaining studies relied on either subjective measure such as program directors’ evaluations of knowledge, performance, and clinical management, or a combination of subjective measures and end-of-the-year exam scores. Overall, the results regarding GPA as a predictor of work performance were inconsistent. For the two studies conducted in Australia using JDAT,19,23 there was a weak correlation between GPA and the JDAT scores (r=0.257; p<0.0001).
The six studies consistently found a relationship between GPA and physicians’ performance, although the strength of this association varied. Al-Shamsia et al found a strong positive correlation (r = 0.665, p < 0.05) between GPA and residents’ self-reported outcomes at the end of the PGY-1 year. Conversely, studies utilizing the JDAT assessment tool reported weak positive correlations (r = 0.229, P = 0.002; and r=0.255, p=0.006, respectively). Another study reported a moderate correlation between basic sciences GPA (r = 0.41) and clinical GPA (r = 0.49) and Residency Directors’ Ratings. Notably, one study revealed that only third-year GPA predicted lower scores for both knowledge (OR = 4.9; 95% CI = 2.7–9.2) and professionalism (OR = 7.3; 95% CI = 4.1–13.0), highlighting the potential importance of performance during a specific timeframe. Finally, a case-control study found a small but statistically significant difference in undergraduate GPA between physicians who received disciplinary actions and those who did not (3.3 vs 3.4, respectively; p=0.04).
Relationship Between GPA and Pharmacists’ Work Performance
The direct association between GPA and pharmacists’ work performance has been largely unexplored. However, two studies provide insight into the potential influence of GPA on pharmacists’ career aspirations and personal growth.22,30 Both studies, conducted in the USA, used the pursuit and achievement of postgraduate qualifications, such as residencies or fellowships, as indicators of professional growth. The findings from these studies suggest that GPA may influence professional development among pharmacists. Sevak et al found a significant correlation between GPA and the likelihood of applying for and securing a postgraduate residency or fellowship, among various career stages in pharmacy.22 Every one-point increase in the cumulative GPA, research activity score, and APRS-16 score was associated with increased odds of applying to a residency program by 6.3, 3.3, and 1.07 times, respectively.22 To attain a position, each one-point increase in GPA and self-reported interview performance score was associated with an increase in the odds of matching with a residency position by 9.93 and 5.32 folds, respectively.22 In another study focusing on early career-level pharmacists, a small difference was reported in the median (IQR) pharmacy school GPA between students who applied for residency and those who did not [3.6 vs 3.5, respectively; (p=0.01)].30 In addition, there was a statistically significant difference in the median pharmacy school GPA between students who successfully matched to a residency program and those who did not, with medians of 3.7 and 3.5, respectively (p=0.035).30
Relationship Between GPA and Nurses’ Work Performance
Six studies investigated the effect of GPA on various performance indicators among nurses.17,20,21,24–26 These indicators included early job turnover, transition shock, critical thinking skills, decision-making abilities, and emotional intelligence.17,20,21,24–26 The studies encompassed nurses at different career stages: entry-level (n= 1),24 early career (<5 years) (n= 3),17,20,25 expert level (>5 years of experience) (n= 1),21 or any career level with a mean of 7.3 years of experience (n= 1).26 The impact of GPA on nurse performance was found to be inconsistent across the six studies. Two of the studies explored the relationship between GPA and negative professionalism indicators, specifically, turnover rate and transition shock.17,20 One of these studies revealed a significant association between GPA and job changes and turnover. Nurses with a GPA below 3.5 were about 6 times more likely to change hospitals compared to those with a GPA above 3.5.17 However, regarding transition shock among early career nurses, GPA was not identified as a significant predictor of transition shock.20 On the other hand, other studies examined the relationship between GPA and positive professionalism indicators, including critical thinking, diagnostic reasoning, decision styles, and emotional intelligence. In two of the studies focusing on early career nurses, GPA had a statistically significant influence on diagnostic reasoning score (r = 38, p= 0.001),24 and on one component of emotional intelligence (P<001).26 However, there was no significant relationship between critical thinking dispositions and overall GPA among early career nurses (r = −0.02, p = 0.84).24 Nonetheless, for expert-level nurses, GPA showed a statistically significant correlation with critical thinking and decision-making in one of the studies,21 but no significant relationship with diagnostic skill in another study.26
Discussion
The primary objective of this systematic review was to assess whether GPA is a dependable indicator of work performance success among healthcare professionals. The included studies focused exclusively on physicians, nurses, and pharmacists, excluding other healthcare professions. While the review aimed to assess the relationship between GPA and work performance across various levels of healthcare practitioners, the majority of studies focused on early-career professionals, such as medical residents, pharmacy graduates pursuing postgraduate training, and entry-level employees. Notably, only four of the identified studies addressed practitioners at all career stages, whereas the remaining concentrated on early-career professionals. Our findings from the 14 included studies revealed that the relationship between GPA and work performance varies based on the specific profession, career level, performance indicators/metrics used, and contexts.
Among physicians, GPA was investigated in relation to residency performance, knowledge, and professionalism, particularly for those at the early stages of their careers. Despite the consistent reported positive correlation between GPA and various performance indicators, the strength of this association varied, ranging from weak19,23,27 to moderate,28 and strong correlations.18 For instance, GPA was found to be positively but weakly correlated with disciplinary actions, suggesting that academic achievement may not be a reliable predictor of future professional conduct.27 Remarkably, GPA from particular academic years, such as the third year of medical school, was found to have more predictive potential than cumulative GPA.29 This observation suggests that performance in particular professional years of education might be a better predictor of future work performance. However, the use of various tools in the studies, including both objective and subjective measures, makes it challenging to make a holistic judgment about the reliability of GPA as an indicator of physicians’ work performance. Additionally, a range of competencies, such as communication skills with the multidisciplinary team and patients, ongoing professional development, and board certification scores, also play significant roles in a physician’s overall clinical performance.31–33 In addition, studies have reported that certain factors such as the use of audit and feedback approaches can contribute to improving physicians’ clinical performance.34,35 Therefore, further studies looking at more robust and holistic outcomes should be performed to determine if GPA can be considered a reliable indicator of various aspects of physicians’ performance. While no studies explored the direct association between GPA and pharmacists’ work performance, two publications examined how GPA influences career pursuits and professional development.22,30 This was particularly regarding the pursuit of postgraduate residency or fellowship opportunities.22,30 Both studies implied that a high GPA might increase the likelihood of applying for and securing residency programs opportunities, potentially fostering a commitment to lifelong learning endeavor. Indeed, research has indicated that various factors can contribute to pharmacists’ attainment of higher postgraduate qualifications,36,37 and numerous elements can influence their clinical competence.38–40 For instance, a retrospective study among PharmD students evaluated the predictive value of academic and coursework assessments in identifying factors associated with failure or poor performance in advanced pharmacy practice experiences (APPEs).41 The study found that a professional GPA below 2.7, pharmacotherapy course failure, and professionalism issues during introductory pharmacy practice experiences (IPPEs) were significant predictors of APPE failure.41 Importantly, pursuing higher education alone cannot be considered a definitive indicator of pharmacists’ professional performance. Similar to physicians, the nature of pharmacists’ job is complex, encompassing distinct aspects such as communication skills, clinical reasoning, and the delivery of patient-centered pharmaceutical care.42,43 Pharmacists work in diverse practice settings, including community pharmacies, hospitals, and the pharmaceutical industries.44,45 They can also hold different types of job positions, including operational roles, clinical roles, drug information, quality assurance, and pharmacy informatics.44,45 Hence, future research endeavors should explore the relationship between specific pharmacy job roles and academic GPA. Other assessment methods beyond GPA also merit exploration for their relationship with professional clinical performance. For instance, Heldenbrand et al demonstrated that the multiple mini-interview (MMI) serves as an independent predictor of preceptor-rated performance during the APPE year among PharmD students.46
Studies exploring the predictive value of GPA on nurses’ performance have yielded mixed findings. Although most of the studies reported positive associations,17,21,25 some reported no difference or negative relationships.20,24,47 Similar to the findings for physicians, these results varied depending on the performance indicators and career levels examined. In the two studies that examined GPA in relation to turnover rate and transition shock, GPA was found to be significantly associated with job changes and turnover, especially among entry-level nurses;17 however, it did not affect the transition shock.20 This may be explained by the fact that early career nurses may face challenges in adapting to and understanding their work environment as well as applying their theoretical knowledge into practice. This finding aligns with existing reports indicating that healthcare graduates commonly experience challenges in their early career stages.48–50 Another study targeting the same population of early career nurses, has identified GPA as a significant factor influencing diagnostic reasoning.24 This connection may be attributed to the fact that problem-solving and analytical thinking skills are correlated with higher GPAs.51 However, GPA did not impact critical thinking dispositions, as measured by the CCTDI tool.24 Concerning emotional intelligence, early career nurses’ GPA was found to be a predictor of the “understanding emotions” domain of emotional intelligence, as measured by the MSCEIT tool.25 Nevertheless, it did not influence any of the remaining three emotional intelligence domains of the MSCEIT tool (perceiving emotions, facilitating thoughts, and managing emotions).25 Similarly, a study among first-year nursing students demonstrated a modest but significant correlation between total emotional intelligence and experiential emotional intelligence with GPA.52 However, the study also highlighted lower-than-average scores in several emotional intelligence domains, suggesting that traditional academic metrics, such as GPA, may not fully capture the broader competencies required for postgraduation performance.52 These findings emphasize the need for further research to explore the relationship between traditional and nontraditional measures of success and their correlation with professional performance. In one study focusing on expert-level nurses, GPA was found to have a significant correlation with critical thinking and decision-making skills21 but not with diagnostic abilities.26 This inconsistency could be due to differences in assessment methods, with some studies employing objective standardized tests to evaluate critical thinking, diagnostic reasoning, or decision-making, while others relied on self-reported scales or qualitative approaches. Therefore, there is a need for more rigorous studies to explore the potential relationship between GPA and nurses’ work performance, while taking into consideration the diverse roles within nursing and other clinical performance measures that might affect this relationship.
Apart from GPA, Terry et al conducted a systematic review to evaluate whether coursework summative assessments such as Objective Structured Clinical Examinations (OSCEs) predict the clinical performance of healthcare professionals, including medical doctors and pharmacists.53 Despite evaluating a limited number of studies with heterogeneous outcomes, the review found that OSCEs and written assessments such as multiple-choice, extended matching, and short-answer questions significantly correlate with the clinical performance of healthcare professional students.53 Additionally, Subih et al identified significant predictors of clinical performance among emergency nurses, including secondary traumatic stress, high body mass index, smoking, chronic diseases, and working overtime. The study highlighted a strong negative association between secondary traumatic stress and nursing performance, emphasizing the importance of a holistic approach to predicting clinical performance and implementing interventions to reduce stress levels.54 Similarly, Lee et al found that personal factors, such as self-esteem and work-life balance satisfaction, along with the quality of the clinical learning environment, significantly influenced nursing students’ readiness for practice.55 These findings suggest that other confounding factors should be considered when evaluating GPA as a predictor of work performance among healthcare professionals.
While this systematic review offers a well-structured response to an important and contentious issue, it has some limitations that need to be addressed. First, the methodological heterogeneity in the reported outcomes and study designs did not allow direct comparison or meta-analysis. Second, differences in the assessment tools, work performance metrics, and reported outcomes among the studies introduced additional challenges. Nevertheless, categorizing the studies by healthcare profession facilitated a more organized summary of the findings. Third, only three healthcare professions were identified within the included studies, which limits the ability to generalize the findings to all healthcare professionals.
Conclusion
Overall, this systematic review suggests that GPA may influence certain aspects of work performance in healthcare, but its impact may differ depending on the profession, career stage, and specific context. Therefore, GPA alone should not be used as a primary or definitive indicator of a healthcare professional’s overall work performance. A more accurate evaluation requires a comprehensive assessment that includes clinical competencies, ethical behavior, communication skills, and job-specific responsibilities. For example, healthcare institutions could implement multifactorial hiring frameworks that combine GPA with assessments of clinical skills, professionalism, and communication abilities to better predict job performance.
The findings of this review also underscore that policymakers should avoid over-relying on GPA when hiring healthcare professionals and instead consider a holistic evaluation of candidates. However, the reviewed studies in this review were limited by small sample sizes, heterogeneous methodologies, focus on early career and entry-level professionals, inclusion of limited number of healthcare professions, and a lack of standardized performance metrics, which may affect the generalizability of findings. Future research should employ robust study designs to further explore the relationship between GPA and objective performance metrics, while also considering potential confounding factors, years of experience, and the multifaceted nature of each healthcare profession. This is particularly important as job performance can be affected by a range of factors, including personal beliefs, organizational culture, work environment, and career expectations. Longitudinal studies tracking professionals from their academic years through their careers would be particularly valuable in understanding the long-term relationship between GPA and work performance as well as provide more conclusive evidence.
Finally, the variability in GPA’s impact on work performance across healthcare roles emphasizes the need for tailored approaches. For example, specific competencies like clinical reasoning may be more relevant for physicians, while pharmaceutical centered care and emotional intelligence may be critical for pharmacists and nurses, respectively. Recognizing this diversity is essential for improving workforce evaluation and ensuring high-quality healthcare delivery.
Funding
Qatar University (QU) funded the publication of this article.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kruk ME, Gage AD, Arsenault C, et al. High-quality health systems in the sustainable development goals era: time for a revolution. Lancet Glob Health. 2018;6(11):e1196.
2. Figueroa CA, Harrison R, Chauhan A, Meyer L. Priorities and challenges for health leadership and workforce management globally: a rapid review. BMC Health Serv Res. 2019;19(1):1–11. doi:10.1186/s12913-019-4080-7
3. Chisholm-Burns MA, Berg-Poppe P, Spivey CA, Karges-Brown J, Pithan A. Developing a framework of relationships among noncognitive factors in doctor of pharmacy students’ academic performance. Am J Pharmaceut Educ. 2021;85(10):8608. doi:10.5688/ajpe8608
4. Kanfer R, Wolf MB, Kantrowitz TM, Ackerman PL. Ability and trait complex predictors of academic and job performance: a person–situation approach. Appl Psychol. 2010;59(1):40–69. doi:10.1111/j.1464-0597.2009.00415.x
5. Al-Asmar AA, Oweis Y, Ismail NH, Sabrah AHA, Abd-Raheam IM. The predictive value of high school grade point average to academic achievement and career satisfaction of dental graduates. BMC Oral Health. 2021;21(1):300. doi:10.1186/s12903-021-01662-5
6. Bretz RD. College grade point average as a predictor of adult success: a meta-analytic review and some additional evidence. Public Personnel Manag. 1989;18(1):11–22. doi:10.1177/009102608901800102
7. Muntean LM, Nireștean A, Sima-Comaniciu A, Mărușteri M, Zăgan CA, Lukacs E. The relationship between personality, motivation and academic performance at medical students from Romania. Int J Environ Res Public Health. 2022;19(15):8993. doi:10.3390/ijerph19158993
8. Miller A, Archer J. Impact of workplace based assessment on doctors’ education and performance: a systematic review. BMJ. 2010;341(7775):710. doi:10.1136/bmj.c5064
9. Asghar Hayat A, Salehi A, Koj URIJ, Kojuri J. Medical student’s academic performance: the role of academic emotions and motivation. J Adv Med Educ Prof. 2018;6(4):168.
10. ALmegewly WH, Rawdhan A, Saleh M, et al. Correlation between emotional intelligence and academic achievement among undergraduate nursing students. Int J Afr Nurs Sci. 2022;17:100491. doi:10.1016/J.IJANS.2022.100491
11. Imose R, Barber LK. Using undergraduate grade point average as a selection tool: a synthesis of the literature. Psychol Manager J. 2015;18(1):1–11. doi:10.1037/MGR0000025
12. Dissen A. A critical issue: assessing the critical thinking skills and dispositions of undergraduate health science students. Discover Edu. 2023;2(1):1–20. doi:10.1007/s44217-023-00044-z
13. Richards JM, Taylor CW, Price PB. The prediction of medical intern performance. J Appl Psychol. 1962;46(2):142–146. doi:10.1037/H0039288
14. ElAbd R, AlShatti R, Sultan S, AlOtaibi N, AlSabah S. Medical School Performance as Measured by GPA: what Can it Predict? 2024. Available from: https://www.researchsquare.com/article/rs-3860391/v1.
15. Romeo EM. The predictive ability of critical thinking, nursing GPA, and SAT scores on first-time NCLEX-RN performance. Nurs Educ Perspect. 2013;34(4):248–253. doi:10.5480/1536-5026-34.4.248
16. Study Quality Assessment Tools | NHLBI, NIH. Available from: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools.
17. Kim EY, Kim SH. Job change among early career nurses and related factors: a postgraduation 4-year follow-up study. J Nurs Manag. 2022;30(7):3083–3092. doi:10.1111/jonm.13713
18. Al-Shamsi GS, Wasfy NF, Eldin MG, Talaat W. Assess the relationship between the emirates medical residency entry examination, grade point average, and multiple mini interview scores and the resident’s end-of-year-one performance in the UAE. Dubai Med J. 2023;6(2):134–143. doi:10.1159/000529840
19. Carr SE, Celenza A, Puddey IB, Lake F. Relationships between academic performance of medical students and their workplace performance as junior doctors. BMC Med Educ. 2014;14(1):1–7. doi:10.1186/1472-6920-14-157
20. Kim EY, Yeo JH. Effects of pre-graduation characteristics and working environments on transition shock of newly graduated nurses: a longitudinal study. Nurse Educ Today. 2019;78:32–36. doi:10.1016/j.nedt.2019.04.002
21. Martin C. The theory of critical thinking of nursing. Nurs Educ Perspect. 2002;23(5):243–247.
22. Sevak RJ, Nguyen AB, Randhawa S, O’Dell KM. Variables affecting pharmacy students’ pursuit and attainment of postgraduate residency and fellowship positions. Curr Pharm Teach Learn. 2022;14(10):1298–1304. doi:10.1016/j.cptl.2022.09.006
23. Carr SE, Celenza A, Mercer AM, Lake F, Puddey IB. Predicting performance of junior doctors: association of workplace based assessment with demographic characteristics, emotional intelligence, selection scores, and undergraduate academic performance. Med Teach. 2018;40(11):1175–1182. doi:10.1080/0142159X.2018.1426840
24. Sands H. Making the diagnosis: factors shaping diagnostic reasoning among entry-level nurse practitioners. Los Angeles: University of California; 2001. Available from: https://search.ebscohost.com/login.aspx?direct=true&db=cul&AN=109876239&site=ehost-live&scope=site&authtype=sso&custid=s3704754.
25. Reemts GS. Emotional intelligence levels in baccalaureate-prepared early career registered nurses. Asia Pac J Oncol Nurs. 2015;2(2):72–81. doi:10.4103/2347-5625.157573
26. King P. A CONSIDERATION OF DIAGNOSTIC REASONING SKILLS IN NURSE PRACTITIONERS-MEASURES AND INFLUENCES. Louisville, Kentucky: University of Louisville; 2006. Available from: https://search.ebscohost.com/login.aspx?direct=true&db=cul&AN=109847516&site=ehost-live&scope=site&authtype=sso&custid=s3704754.
27. Papadakis MA, Hodgson CS, Teherani A, Kohatsu ND. Unprofessional behavior in medical school is associated with subsequent disciplinary action by a state medical board. Acad Med. 2004;79(3):244–249. doi:10.1097/00001888-200403000-00011
28. Paolo AM, Bonaminio GA. Measuring outcomes of undergraduate medical education: residency directors’ ratings of first-year residents. Acad Med. 2003;78(1):90–95. doi:10.1097/00001888-200301000-00017
29. Greenburg DL, Durning SJ, Cohen DL, Cruess D, Jackson JL. Identifying medical students likely to exhibit poor professionalism and knowledge during internship. J Gen Intern Med. 2007;22(12):1711–1717. doi:10.1007/s11606-007-0405-z
30. Phillips JA, McLaughlin MM, Rose C, Gallagher JC, Gettig JP, Rhodes NJ. Student characteristics associated with successful matching to a PGY1 residency program. Am J Pharm Educ. 2016;80(5):84. doi:10.5688/ajpe80584
31. Baker WE. Evaluation of physician competency and clinical performance in emergency medicine. Emerg Med Clin North Am. 2009;27:615–626. doi:10.1016/j.emc.2009.07.010
32. Forster AJ, Turnbull J, Mcguire S, Ho ML, Worthington JR, Ho -michael L. Improving patient safety and physician accountability using the hospital credentialing process. Open Med. 2011;5:e79.
33. Whitelock-Wainwright E, Koh JW, Whitelock-Wainwright A, Talic S, Rankin D, Gašević D. An exploration into physician and surgeon data sensemaking: a qualitative systematic review using thematic synthesis. BMC Med Inform Decis Mak. 2022;22(1). doi:10.1186/s12911-022-01997-1
34. Jamtvedt G, Young J, Kristoffersen D, Thomson O’Brien M, Oxman A. Audit and feedback: effects on professional practice and health care outcomes. Cochrane Database Syst Rev. 2003. doi:10.1002/14651858.cd000259
35. Veloski J, Boex JR, Grasberger MJ, Evans A, Wolfson DW. Systematic review of the literature on assessment, feedback and physicians’ clinical performance*: BEME Guide No. 7. Med Teach. 2006;28:117–128. doi:10.1080/01421590600622665
36. Woldekidan NA, Mohammed AS, Belachew EA. Pharmacy students motivation, preparation and factors affecting pursuing postgraduate education in ethiopian university. Adv Med Educ Pract. 2020;11:429–436. doi:10.2147/AMEP.S244326
37. Hammond DA, Oyler DR, Devlin JW, et al. Perceived motivating factors and barriers for the completion of postgraduate training among American pharmacy students prior to beginning advanced pharmacy practice experiences. Am J Pharmaceut Educ. 2017;81(5):90. doi:10.5688/ajpe81590
38. Rushworth GF, Jebara T, Tonna AP, et al. General practice pharmacists’ implementation of advanced clinical assessment skills: a qualitative study of behavioural determinants. Int J Clin Pharm. 2022;44(6):1417–1424. doi:10.1007/s11096-022-01484-7
39. Al-Kubaisi KA, Elnour AA, Sadeq A. Factors influencing pharmacists’ participation in continuing education activities in the United Arab Emirates: insights and implications from a cross-sectional study. J Pharm Policy Pract. 2023;16(1). doi:10.1186/s40545-023-00623-3
40. Makhlouf AM, Mohamed Ibrahim MI, Awaisu A, Vyas SK, Yusuff KB. Determinants of community pharmacists’ information gathering and counseling practices during the management of minor ailments. Saudi Pharm J. 2021;29(9):992–998. doi:10.1016/j.jsps.2021.07.016
41. Call WB, Grice GR, Tellor KB, et al. Predictors of student failure or poor performance on advanced pharmacy practice experiences. Am J Pharmaceut Educ. 2020;84(10):ajpe7890. doi:10.5688/ajpe7890
42. Gyllensten H, Fuller JM, Östbring MJ. Commentary: how person-centred is pharmaceutical care? Int J Clin Pharm. 2022;44:270–275. doi:10.1007/s11096-021-01332-0
43. Rahayu SA, Widianto S, Defi IR, Abdulah R. Role of pharmacists in the interprofessional care team for patients with chronic diseases. J Multidisciplinary Healthcare. 2021;14:1701–1710. doi:10.2147/JMDH.S309938
44. Hatahet T, Al-Obaidi H, Tekko IA, Chen T. Strategic job market-guided development of pharmacy bachelor’s curriculum and its importance in maintaining the profession viability in the Middle Eastern countries: colleges of pharmacy in the UAE as a model. Saudi Pharm J. 2022;30(9):1283–1292. doi:10.1016/j.jsps.2022.06.023
45. Knoer SJ, Eck AR, Lucas AJ. A review of American pharmacy: education, training, technology, and practice. J Pharm Health Care Sci. 2016;2(1). doi:10.1186/s40780-016-0066-3
46. Heldenbrand SD, Dayer LE, Martin BC, et al. APPE evaluations are positively associated with MMI, pre-pharmacy GPA and pharmacy GPA. Am J Pharmaceut Edu. 2018;82(7):6326. doi:10.5688/ajpe6326
47. Labreacht P, Bsn K. A CONSIDERATION OF DIAGNOSTIC REASONING SKILLS IN NURSE PRACTITIONERS-MEASURES AND INFLUENCES.
48. Jager A, Harris M, Terry R. The challenges faced by early career international medical graduates in general practice and opportunities for supporting them: a rapid review. BJGP Open. 2023;7(3):
49. Spence Laschinger HK, Wong C, Read E, et al. Predictors of new graduate nurses’ health over the first 4 years of practice. Nurs Open. 2019;6(2):245–259. doi:10.1002/nop2.231
50. Cuesta-Briand B, Coleman M, Ledingham R, et al. Understanding the factors influencing junior doctors’ career decision-making to address rural workforce issues: testing a conceptual framework. Int J Environ Res Public Health. 2020;17(2). doi:10.3390/ijerph17020537
51. Pepe K. A research ofthe relationship between study skills of students and their GPA. Procedia Soc Behav Sci. 2012;47:1048–1057. doi:10.1016/j.sbspro.2012.06.777
52. Codier E, Odell E. Measured emotional intelligence ability and grade point average in nursing students. Nurse Educ Today. 2014;34(4):608–612. doi:10.1016/j.nedt.2013.06.007
53. Terry R, Hing W, Orr R, Milne N. Do coursework summative assessments predict clinical performance? A systematic review. BMC Med Educ. 2017;17(1). doi:10.1186/s12909-017-0878-3
54. Subih M, Al-Amer R, Bani Saleh EG, Thultheen IN. Predictors of clinical performance among emergency nurses: a cross-sectional study. SAGE Open Nurs. 2024;10. doi:10.1177/23779608241281468.
55. Lee T, Lee SJ, Yoon YS, et al. Personal factors and clinical learning environment as predictors of nursing students’ readiness for practice: a structural equation modeling analysis. Asian Nurs Res. 2023;17(1):44–52. doi:10.1016/j.anr.2023.01.003
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Physicians’ Knowledge and Practices Regarding Asthma: A Cross-Sectional Study in Saudi Arabia
Dairi MS
International Journal of General Medicine 2022, 15:6671-6680
Published Date: 19 August 2022
Comparison of Perceptions About Patient Safety Culture Between Physicians and Nurses in Public Hospitals in Vietnam
Tran TNH, Pham QT, Tran LH, Vu TA, Nguyen MT, Pham HT, Le TT, Bui TTH
Risk Management and Healthcare Policy 2022, 15:1695-1704
Published Date: 6 September 2022
Impact of Educational Intervention on Compliance of Health Care Workers Towards Chemotherapy Handling Guidelines
Alaraidh S, Alnaim LS, Almazrou SH
Journal of Multidisciplinary Healthcare 2023, 16:3035-3042
Published Date: 16 October 2023
Instruments for Measuring Healthcare Professionals’ Medication Safety Competence: A Scoping Review
Stephan C, Kloor D, Wurmbach VS, Mahler C
Journal of Multidisciplinary Healthcare 2025, 18:1745-1758
Published Date: 25 March 2025
Knowledge, Attitude, and Practice of Palliative Care Among Physicians and Nurses in Intensive Care Units in Shanghai, China
He X, Cai H, Zhang J, Chen W, Zhu B
Journal of Multidisciplinary Healthcare 2025, 18:2441-2449
Published Date: 1 May 2025