Back to Journals » Risk Management and Healthcare Policy » Volume 15
Comparison of Perceptions About Patient Safety Culture Between Physicians and Nurses in Public Hospitals in Vietnam
Authors Tran TNH, Pham QT ![]() , Tran LH, Vu TA, Nguyen MT, Pham HT, Le TT, Bui TTH
, Tran LH, Vu TA, Nguyen MT, Pham HT, Le TT, Bui TTH ![]()
Received 20 May 2022
Accepted for publication 27 August 2022
Published 6 September 2022 Volume 2022:15 Pages 1695—1704
DOI https://doi.org/10.2147/RMHP.S373249
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mecit Can Emre Simsekler
Thi Nhi Ha Tran,1,* Quoc Thanh Pham,2,* Lien Huong Tran,3 Tuan Anh Vu,4 Minh Tu Nguyen,5 Hung Tien Pham,6 Thanh Tong Le,7 Thi Thu Ha Bui8
1Management Board, Department of Health, Hanoi, Vietnam; 2Center of Digital Health, Hanoi University of Public Health, Hanoi, Vietnam; 3Management Board, Saint Paul Hospital, Hanoi, Vietnam; 4Medicine Department, Agriculture General Hospital, Hanoi, Vietnam; 5Management Board, Phuc Tho hospital, Hanoi, Vietnam; 6Faculty of Clinical Medicine, Hanoi University of Public Health, Hanoi, Vietnam; 7Student, Hanoi University of Public Health, Hanoi, Vietnam; 8Faculty of Social and Behavioral Sciences, Hanoi University of Public Health, Hanoi, Vietnam
*These authors contributed equally to this work
Correspondence: Quoc Thanh Pham, Center of Digital health, Hanoi University of Public Health, Hanoi, 100000, Vietnam, Tel +840 978502383, Fax +84 024 62662385, Email [email protected]
Introduction: Patient safety culture (PSC) is a vital component in ensuring high-quality and safe patient care. Assessment of physicians’ and nurses’ perceptions of existing hospital PSC is the first step to promoting PSC. This paper is aimed to assess physicians’ and nurses’ perceptions of PSC in 5 public general hospitals in Hanoi, Vietnam.
Methods: This cross-sectional study surveyed 410 physicians and 824 nurses utilizing the validated Hospital Survey on Patient Safety Culture in an online format.
Results: The composite positive physician’s perception of PSC varied from 47.8 to 89.6% with the lowest composite score of patient safety for “staffing” (47.8%) and the highest composite score for “teamwork within units” (89.6%). The composite positive responses for perception among nurses varied from 51.3 to 94.2% with the lowest composite score of patient safety for “staffing” (51.3%) and the highest composite score for “teamwork within units” (94.2%).
Conclusion: The mean scores for “supervisor/manager expectations”; “staffing”, “management support for patient safety”, “teamwork across units”, “handoffs and transitions” among nurses were significantly higher than that among physicians (p< 0.05). About two-thirds of physicians and nurses reported no event in the past 12 months (62.8 and 71.7%, respectively). The nurses reported significantly higher patient grades (every good and excellent) than physicians (75% vs 67.1%, p < 0.001). Hospitals could develop and implement intervention programs to improve patient safety, including providing interventions on teamwork and communication, encouraging staff to notify incidents, and avoiding punitive responses.
Keywords: patient safety culture, hospital, physicians, nurses
Introduction
To ensure high quality and safe patient care, it is vital to ensure patient safety culture (PSC).1 It has been reported that unsafe and poor quality care has resulted in about 64% of deaths in low-middle income countries (LMIC) and many of these deaths are preventable.2
Safety culture is regarded as the awareness, values, and perception of safety shared by all members of an organization and directly related to organizational operation.3 The first step that needs to be done to promote PSC in a hospital is to assess the staff’s perception of the hospital’s PSC.4–7 The Hospital Survey on Patient Safety Culture (HSOPSC) was initiated by the Agency for Healthcare Research and Quality and has been applied in various countries.8,9 The HSOPSC measures 12 dimensions at different levels, namely, work area or unit (7 dimensions), hospital (3 dimensions), and outcomes (2 dimensions).9,10 The HSOPSC has been translated, validated11 and used to assess PSC in several hospitals in Vietnam.12–14
Literature has revealed that the most frequent positive safety culture aspects reported in hospitals in different countries including Ethiopia, Saudi Arabia, Switzerland, the US, China, Brazil, Yemen and Vietnam were “organizational learning and continuous improvement”, “teamwork within units”, “feedback and communication about errors”; “communication openness”, while the most frequent negative dimensions were “non-punitive responses to an error”, “staffing”; “handoffs and transitions”; “overall perceptions of safety”, and “frequency of event reporting”.13,15–21 Nonpunitive response to errors often had the lowest scores and teamwork across units often had the highest scores.9,18,21 Other research has also indicated that sharing and trust in safety culture are communicated in a health institution with a positive safety culture assessment, which serves to support work performance.6,22
Physicians and nurses are considered core staff with professional skills, dedicating themselves to health service delivery in hospitals. In general, the physician’s positive response score is higher than nurses on “communication openness and teamwork across unit” in Switzerland;18 Taiwan;23,24 Germany,25 Canada;19 Saudi Arabia;17 China,26 Holland27 and Canada.28 In comparison, nurses have higher positive response scores on “supervisor/managers expectations and actions on improving patient safety” than physicians and lower responses on “staffing” in Saudi Arabia,17,29 China;30 Brazil;20,31 UK;32 and Ethiopia.16 Nurses rate on teamwork within units with lower scores than physicians in Saudi Arabian29 and Taiwan.24
The dimension “overall patient safety grade” was reported quite differently among countries and studies. While physician’s perception was reported higher than nurses in Switzerland (78 vs 60%);18 Taiwan (63.7 vs 52.1%);23 and Germany;25 the opposite results were identified in Saudi Arabia,17,29 China;30 Brazil;20,31 UK;32 and Ethiopia.16 The “feedback and communication about error” was reported higher among physicians in Holland33 while this was lower in USA.19 No differences between physicians and nurses were reported in Palestine.34
Overall there has been a low self-reporting rate with about one-third of health workers reporting at least one error in the last year in countries such as, Saudi Arabia; China; Ethiopia; Brazil; Italia; Palestine and USA.16,29,31,34–37 Blame culture, fear of consequences of reporting, lack of time, missing feedback, work overload, and lack of information resources are common reasons for underreporting6,8,37–39
Vietnam is a low-middle income country located in the Southeast Asian region with a population of around 98 million. The health sector reform was initiated in 1986 under the economic and social reform program named Doi Moi. Under this reform, user fees, health insurance, and hospital autonomization were introduced. The country’s hospital network is organized following the administrative system including 3 levels, namely, district, provincial, and central, and consists of both public and private sectors. Public hospitals share a substantial part in providing health care services.40
Hospitals’ operation is guided by the Ministry of Health’s hospital regulations, in which, main areas including structure, types of activities, and tasks and responsibilities of leaders, managers and staff, hospital management, and technical regulation are stipulated.41 While diagnosis and treatment are the main responsibility of physicians, nurses’ tasks focus on nursing care. These two groups should work as a team to achieve effective and safe patient care.
Patient safety has recently received attention from the Ministry of Health. In 2013, the issuance of the Circular on quality management provided a foundation for patient safety.42 In 2014, the first training program on patient safety was developed and conducted in different hospitals.43 Research has shown the variation of PSC among hospitals which depends on the hospital autonomous status, level, and bed size.12–14 The strongest areas are often “teamwork within units”, and “organizational learning/continuous improvement”. The poorest areas are typically “staffing”, “non-punitive response to error”, and “handoff and transition”. Different roles in the delivery of health care services could result in physicians having different tasks and challenges even in the same medical environment and, as a result, their perception of PSC may vary. To make effective policies and strategies, it is of great importance for hospital managers to have a good understanding of the hospital’s physicians’ and nurses’ perceptions of PSC. This study aimed to assess and compare the perception of PSC between physicians and nurses in five public general hospitals in Vietnam. The study is expected to identify opportunities for improvement and to inform future interventions on improving PSC for physicians and nurses in hospitals.
Methods
Design
The study employed a cross-sectional descriptive design. The data was obtained using a self-reported online survey.
Setting
The study data was collected from five public general hospitals in Hanoi and Ho Chi Minh City, Vietnam, at the provincial and district level. Table 1 below provides general information about each of the hospitals involved in the study. Three hospitals are autonomous with recurrent expenditure (Hospital A, B and C) and one hospital has an occupancy rate over 100% (Hospital A). Majority of respondents are coming from clinical departments including internal medicine, surgery, obstetric and pediatric (>90%), except hospital E (60.2%).
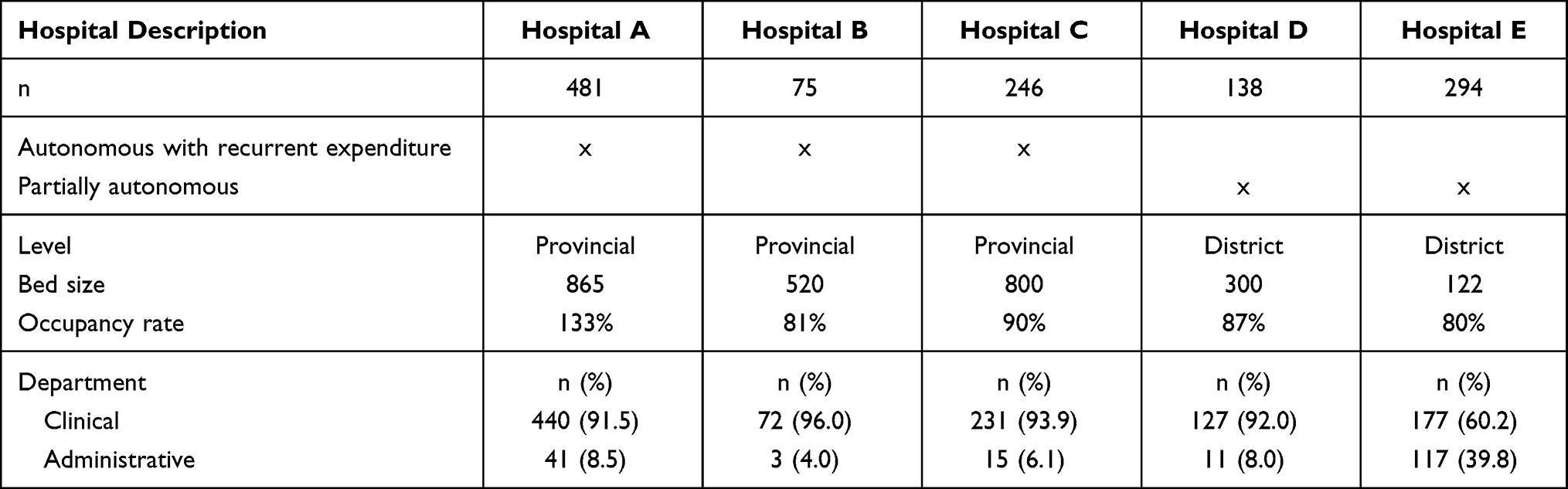 |
Table 1 Description of the hospitals |
Participants
A convenience sampling technique was used and there were 410 physicians and 824 nurses in total having completed the survey, resulting in a response rate of 78.0%. The inclusion criteria included working full-time, having been working in the hospital for at least 6 months, and being willing to participate in the survey. Those potential participants who were on sick leave or on a business trip during the study period were not be involved in the study. Participation in the study was completely voluntary.
Measurements
The study used the Hospital Survey on Patient Safety Culture (HSOPSC) to assess the perception of PSC. This instrument includes 42 questions, measuring 12 dimensions including (1) within-unit teamwork; (2) supervisors’ expectations and actions enhancing patient safety, (3) organizational learning, (4) error feedback and communication, (5) openness in communication, (6) staffing, (7) non-punitive responses to errors, (8) management support for patient safety, (9) across-unit teamwork, (10) handoffs and transitions, (11) overall patient safety perceptions, and (12) frequency of events that are reported.
Each item is a question that is either positively or negatively worded. For each item, the participant is required to respond on a 5-point Likert scale to ascertain agreement (from “strongly disagree” to “strongly agree”) or frequency (from “never” to “always”). In addition, the instrument involves measurement of two outcome variables including the overall patient safety grade and the number of events reported, also using a 5-point liker scale with 1 indicating “failing” and 5 indicating “excellent” for patient safety, and 1 indicating “no event” and 5 indicating “always” for the number of events reported. To get the average scores of each dimension, the items were linearly converted to a scale from 0 to 100 points.21 The average positive response rate refers to the combined percentage of respondents who answered “Strongly agree” or “Agree”, or “Always” or “Most of the time”, which was calculated for every participant based on the HSOPSC instructions.
The survey also involved questions about the demographic characteristics of the participants, asking about their age, gender, length of time working in the hospital and unit, number of working hours per week, total income, current position, and current direct contact with patients.
Data Collection
Data collection was conducted between September and December 2020, when the COVID-19 pandemic was still at a serious situation in the country. Invitation to participate in the study was sent to the participants with the support of the Administration Department at each hospital. Participants were requested to have a good internet connection to complete an online questionnaire sent via email. This questionnaire was designed using Google form and consisted of three parts: 1) Introduction, 2) Consent form, and 3) The main Questionnaire. The introduction provided information about the study objectives and procedures. The participants were requested to express their consent to participate in the study before completing the questionnaire. The questionnaire was anonymous to ensure confidentiality and privacy. Participation in the study was completely voluntary.
Data Analysis
Descriptive statistics were calculated for the prevalence of demographic characteristics, work-related information of the participants, and the mean (±SD) and the percentage of positive responses for each dimension of the HSOPSC instrument. Negatively worded items were reversely scored so that positive responses would demonstrate higher scores. The percentage of positive responses for each item was calculated following the HSOPSC guideline. The t-test was used to examine differences in the mean of the composite scores. A composite positive response rate equal to 75% or higher was identified as strength, whereas a composite positive response rate equal to 50% and below was regarded as weakness.10 The level of statistical significance was set at less than 0.05. All analyses were undertaken using STATA version 12.0 software.
Ethics Declarations
Ethical approval for the study was obtained from the Institutional Review Board of the Hanoi University of Public Health (approval No. 303/2020/YTCC-HD3). Participation in the study was completely voluntary. The participants could withdraw from the study at any time without bearing any consequences.
Results
A total of 1234 participants participated in the study (Table 2) with a significantly higher mean of ages among physicians than nurses (34.9 vs 33.1; p<0.001). There were significantly more males than females among physicians (53.2%) while most nurses were female (81.1%) (p<0.001). The number of physicians from hospital A was significantly higher than the other hospitals (34.9%) (p<0.001). The physicians who had working experience less than 5 year were significantly higher than the other categories (44,6%, p<0.05). Nurses, who worked more than 11 years working in their current profession were higher than the other categories (44.2%; p<0.001). Two-thirds of physicians and nurses worked more than 40-59 hours per week (66.1 and 68.7%, respectively) and about one-fourth worked more than 60 per week (25.1 and 25.8%, respectively).
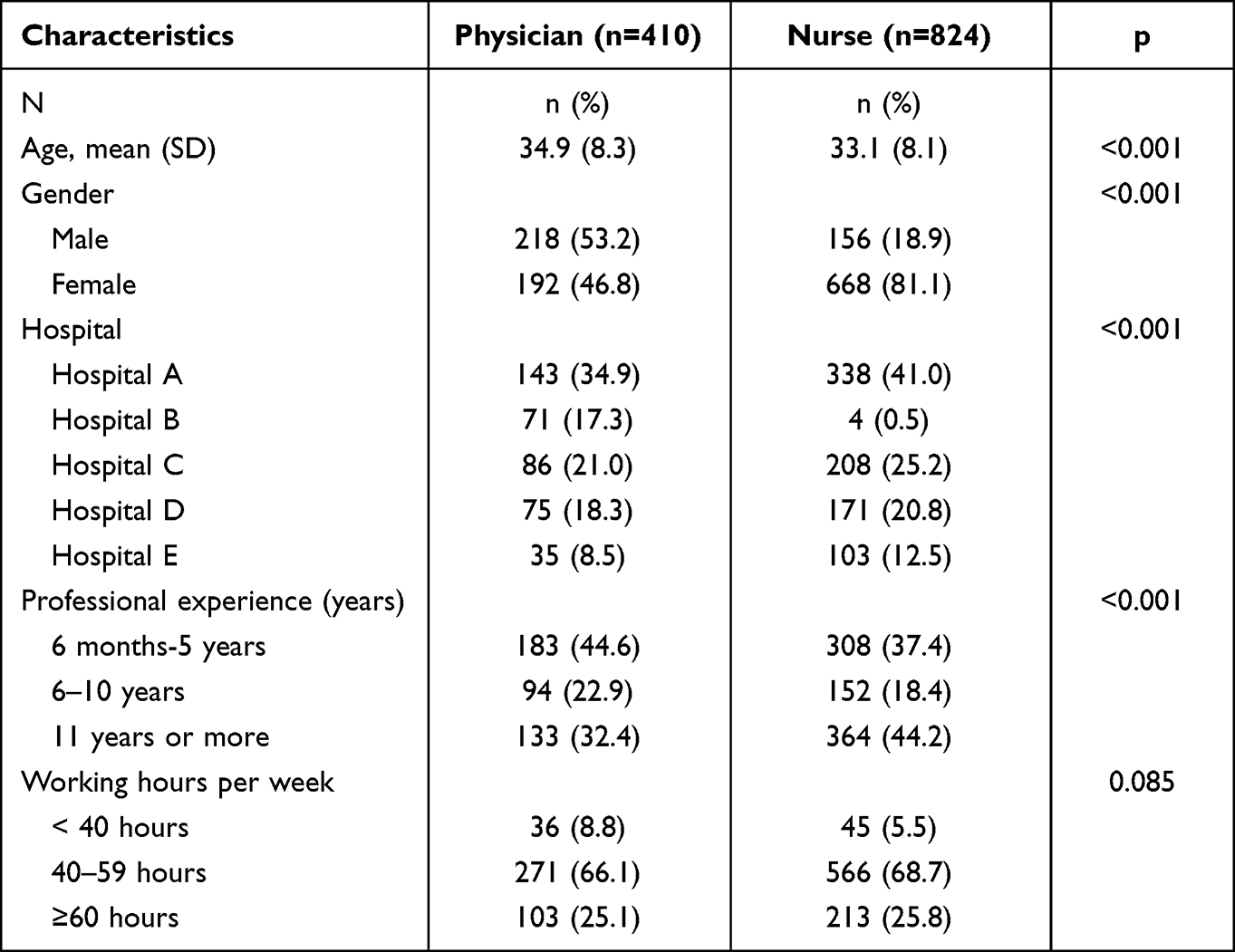 |
Table 2 Characteristics of Participants |
The composite positive physicians’ perception of PSC varied from 47.8 to 89.6% (Table 3). The lowest composite scores for patient safety were “staffing” (47.8%), “nonpunitive response to errors” (48.2%) and the highest composite scores were “teamwork within units” (89.6%) and “feedback and communication about error” (82.8%). Two out of the 12 composites were poor (below 50%); seven were acceptable (between 50% to 75%) and 3 composites were considered as good (over 75%).
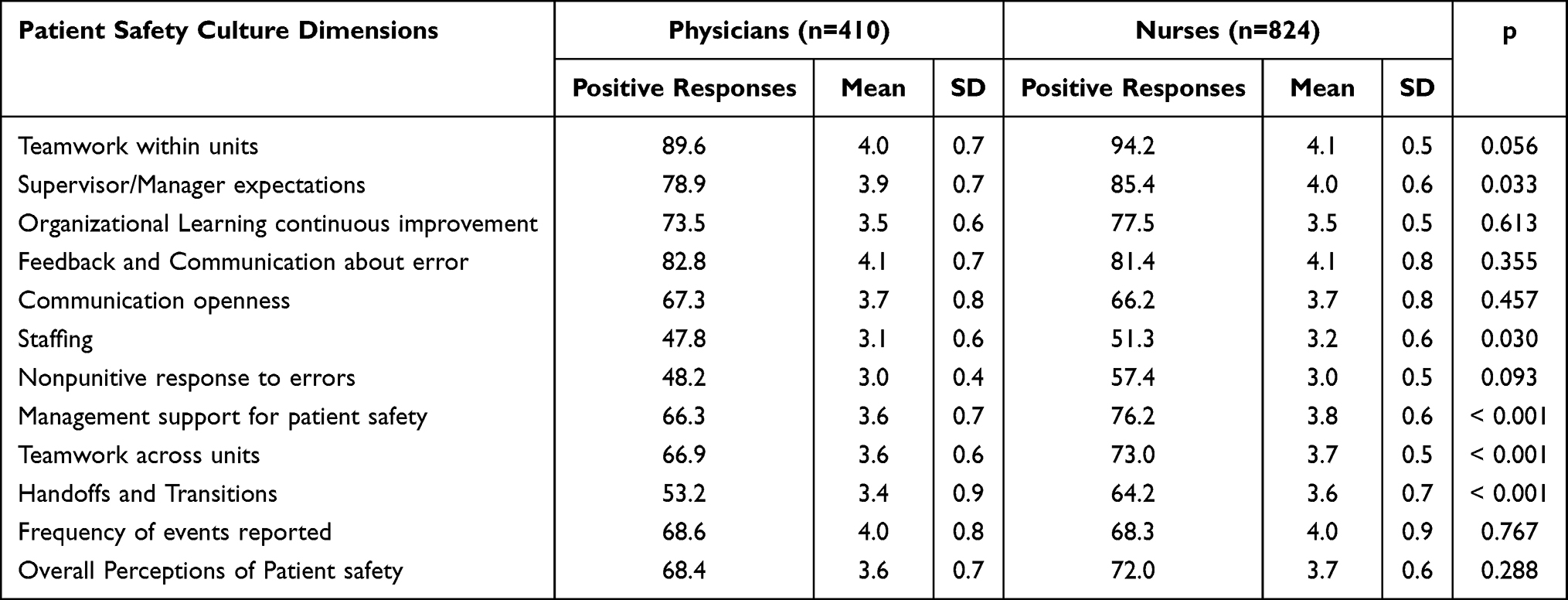 |
Table 3 Scores of PSC Dimensions Among Physicians and Nurses |
The composite positive perception of PSC among nurses varied from 51.3 to 94.2%. The lowest composite scores for patient safety were for “staffing” (51.3%) and “nonpunitive response to errors” (57.4%), and the highest composite scores were for “teamwork within units” (94.2%) and “feedback and communication about error” (85.4%). Seven out of the 12 composites were acceptable (between 50% to 75%) and 5 composites were considered as good (over 75%).
A comparison of the mean score of perceived PSC between physicians and nurses was conducted using the independent t-test. There were significantly higher means of nurses’ perception of PSC than physicians’ for “supervisor/manager expectations”; “staffing”, “management support for patient safety”, “teamwork across units”, and “handoffs and transitions” (p<0.05). The lowest difference was noted for “staffing” and the highest difference was for “handoffs and transitions”. There was no significant difference for the remaining dimensions.
Table 4 presents the comparative analysis on two outcome dimensions: “patient safety grade” and “reported events”. About two-thirds of physicians and nurses did not report any event in the past 12 months (62.8% and 71.7%, respectively). The percentage of physicians working in the clinical department did not report any events in past 12 months was significantly higher than those working in administrative departments (63.3>53.8%; p<0.05). Physicians were more likely to report at least one event than nurses (37.2% > 28.3%, respectively), but the difference was insignificant. Nurses perceived higher patient grades (every good and excellent) than physicians, but the difference was insignificant (75 vs 67.1%, p > 0.05).
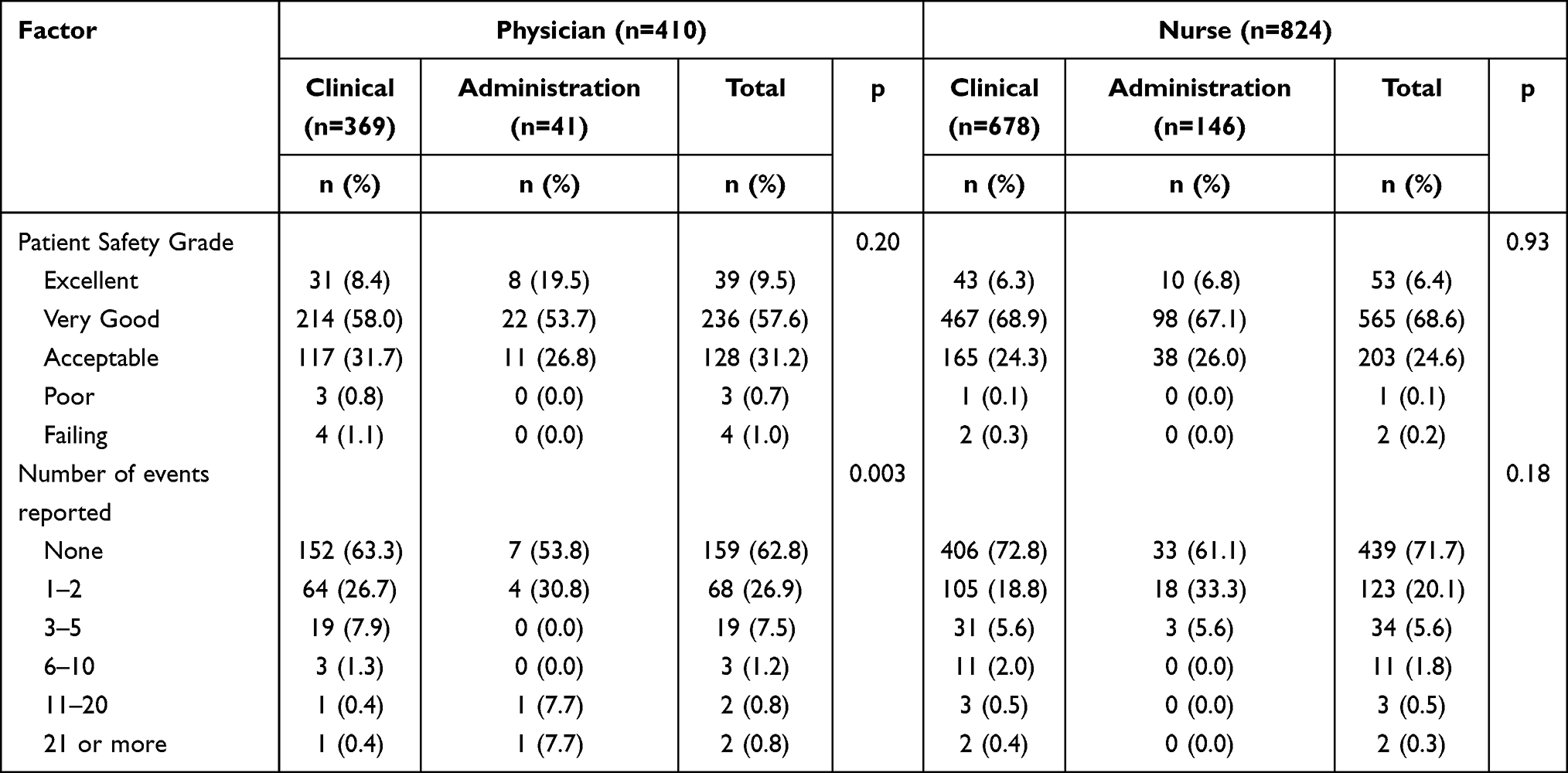 |
Table 4 Patient Safety Grade and Number of Events Reported |
Discussion
In this study, we were able to explore physicians’ and nurses’ perceptions of PSC at 5 public hospitals in Vietnam using the HSOPSC. The dimension “teamwork within units” was identified as the highest positive response item for both physicians and nurses with scores of 89.6% and 94.2%, respectively. The next positive dimension was “feedback and communication about error” for physicians (82.8%) and “supervisor/manager expectations” (85.45) for nurses. The findings are comparable to other studies in various countries like Ethiopia, Saudi Arabia, Switzerland, the US, China, Brazil, and Vietnam.13,15–20
A recent systematic review on patient safety culture revealed that teamwork was one of five factors that significantly impacted patient safety.44 “Teamwork within units” was perceived as a strength in the hospitals by both physicians and nurses in this study. A high score of positive teamwork within units indicates the existence of healthy work relationships and respect among members within a unit.45 Acknowledgement of collaboration and coordination among health workers is important in achieving patient safety.12–14,30,46–48 Strong teamwork, reflected by the agreement on the value on patient safety, will contribute to reducing medical errors and enhancing patient safety. To achieve patient safety, it is essential to improve effective teamwork and well-functioning communication for both physicians and nurses.10
The scores of teamwork across units was < 75% for both physicians and nurses, which indicated the need for improvement. This finding is similar to the current situation, globally.44 Nurses’ average score on “teamwork across units” was significantly higher than that reported by physicians (73.0 > 66.9%; p<0.01). This results is inconsistent with those found in other studies in Switzerland;18 Taiwan;23,24 Germany,25 Canada;19 Saudi Arabia;17 China,26 Holland,27 and Canada.28 Physicians often have barriers in collaborative communication with other professional groups due to their perception of being individually accountable for patient care.38,39,49 Healthcare often relies on interdisciplinary teams of specialists with skill sets needed to perform specialized tasks. Such teams also collaborate to achieve common safety goals. However, in the context of an autonomous hospital, each department is required to have a higher degree of independence in service delivery, and this could result in poorer collaboration across departments in Vietnam.
“Feedback and communication about errors” was a strength in this study for both physicians and nurses (>75%). However, the score was lower for physicians. The understanding of causation and learning from errors is an important approach in continuous quality improvement.34 In addition, the junior staff can learn from more experienced staff as they work together.44 Therefore, individual physicians and teams, as well as managers of hospitals, should take advantage of such opportunities to improve and establish the safety culture.
The “management support for patient safety” was high for nurses (76.2%) but required improvement for physicians (66.3%). This trend is similar to studies in other Southeast Asian countries.15 The difference in scores between physicians and nurses could be related to their working position, as physicians are expected to have a higher level of independence in their job compared to nurses.38,39,49
The responses on “staffing” and “nonpunitive response to errors” were the lowest-rated among both physicians and nurses and need improvement (<75%). These indicated the understaffing and blaming culture in these five hospitals. These findings are consistent with findings in other studies from various countries including, Ethiopia, Saudi Arabia, Switzerland, the US, China, Brazil, and Vietnam.12–20 However, the physicians’ score on staffing was significantly lower than that of nurses’ (48.2 <57.4%; p<0.05). These were different from studies in other countries,16,17,20,29–32 which could be related to the situation of severe shortage of physicians in hospitals in Vietnam, especially those at grassroots levels.50
In 2002, the Vietnam government’s policy on decentralization and autonomation of public hospitals was introduced, aiming to improve the efficiency of service delivery. Partially autonomous public hospitals are not eligible for the government’s subsidy for recurrent expenditure, while fully autonomous hospitals are not eligible for the government’s subsidy for both investment and recurrent expenditure.51 To maintain the operation, hospitals inevitably have to cut down staffing costs and overtime work. Heavy workload, staff shortage, and long working hours are reported as a factor that hindered the PSC.52–54 Improving working conditions and stress management could be a solution for the improvement of PSC in these hospitals.
In this study, the overall frequency of events reported was low for both physicians and nurses. About one-third reported no event for the past 12 months. Physicians working in clinical departments reported lower events compared to those working in administrative departments. This trend is consistent with studies in Saudi Arabia; China; Ethiopia; Brazil; Italia; Palestine and USA.16,29,31,34–37 The low reporting event could be due to blaming culture, fear of the consequences, lack of time, lack of feedback, overload, lack of knowledge on reporting procedures, and skeptical attitudes on adverse events reporting,6,8,31,37–39,49 especially for those working in clinical departments, where they encounter risks of medical incidents daily.
Few reported events in Vietnam can be explained by the perception that reporting on incidents may not lead to improvement.55 This also could be justified for no significant difference in reporting events between physicians and nurses identified in most other studies.16–18,20,23,25,29–31 Furthermore, in Vietnam, error reporting may result in sanctions and is considered a threat to the hospital’s reputation,13 which explains the fact that nonpunitive responses in hospitals are still challenging and need improvement.
Our study found that physicians and nurses had a different perception of PSC, which was initially justified by the different work characteristics, and different basic education and continuing education that was associated with the particularities of each unit and hospital.18,20,27,29,36,56 Interventions for effective interprofessional teamwork and communication has shown to be effective in improving PSC in different countries.25,57 Enhancing communication on patient safety through education, coaching and supervision has been proven effective in another study in Vietnam.13 It is important to understand physicians’ and nurses’ expectations, values, and norms about distinct cultures in health care and engage them in open communication about patient safety. Improved PSC can be obtained by encouraging open communication, creating mutual trust, and establishing a shared perception of how important PSC is and the need to gain confidence in the effectiveness of preventative measures among health professional groups.
Improving PSC requires a long-term plan and assessment of PSC should be taken as the starting point which will, in turn, inform intervention programs that make changes in patient safety,6 especially in the context of hospital autonomization.58 Identifying weaknesses in management practices, deployment of employees, designing work and workspace, and the basic safety culture of healthcare organizations are the first steps in developing interventions for improving patient safety.6
Intervention programs should be well communicated throughout hospitals and made known to all healthcare profession groups, especially hospital managers, physicians, and nurses. Managers should try to enhance safety via a thorough assessment of the safety culture within their hospital and clear guidance for employees under their direct command. The root cause analysis and feedback committee could be a potential intervention for the improvement of hospital PSC.59 Ease in reporting also could provide an opportunity to improve strategy, commitment, and the overall efficacy of PSC in hospitals.44 Blame-free systems, and information sharing and learning from events should become an important part of a desirable working environment.60
The HSOPSC is the most widely used instrument to assess the PSC in hospital settings44 and is validated11 in Vietnam.12–14 Therefore, this should be the first step in developing an intervention program. The difference in job description between physician, nurses, clinical and administrative staff should be taken into account when designing the intervention plan.
Limitations
The study has some limitations that should be taken into consideration when interpreting its results. Firstly, as this study was conducted in Hanoi and Ho Chi Minh city, which may have a different socio-economic context from other parts of the country, the study findings may not be generalized to all hospitals in Vietnam. However, the study contributes to knowledge about perceptions of PSC among health professionals in public hospitals in Vietnam, providing insights into several critical issues of patient safety among physicians and nurses in the country. In this way, the study findings may also be of relevance to other developing countries.
Secondly, due to the cross-sectional nature of the study, the findings only reflected a snapshot of perceptions of PSC at one point in time. It is possible that perceptions of PSC may change over time and there may not be a relationship between perceptions of safety and actual patient safety outcomes.
Thirdly, as the measures in this study relied on self-reports via an online survey, data may have been affected by recall bias, and overestimation or underestimation of the parameters may have occurred. However, as the study was conducted during the COVID-19 pandemic, travel restrictions and other challenges associated with the pandemic made data collection in the field impossible and an online survey was the most feasible option.
Lastly, the main scoring method in this study was based on the calculation of the percentage of positive responses and study did not explore the relationship between PSC dimensions and outcome dimension, such as reported events. Other advanced statistical methods, such as factor analysis and multivariate analysis could yield results on such association. These advanced statistical methods could be employed in the future studies in PSC in Vietnam.
Conclusion
This study provides an insight into how physicians and nurses perceive patient safety in five public hospitals located in Hanoi, Vietnam using HSOPS instrument. The results show that nurses’ perceived scores on PSC were significantly higher than physician on five dimensions: “supervisor/manager expectations”; “staffing”, “management support for patient safety”, “teamwork across units”, and “handoffs and transitions”.
The study findings highlight the need for assessment of PSC using HSOPSC as the first step in designing intervention programs on enhancing patient safety, taking into account the differences in job description of physicians and nurses in hospitals. The intervention should focus on improving teamwork and communication, the encouragement of incident notification, and the minimization of punitive responses.
Acknowledgments
The authors acknowledged the supports of staffs in five hospitals participated in this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Institute of Medicine (IOM). Keeping Patients Safe: Transforming the Work Environment for Nurses. Washington DC: National Academies Press; 2003.
2. Kruk ME, Gage AD, Arsenault C, et al. High-quality health systems in the Sustainable Development Goals era: time for a revolution. Lancet Glob Health. 2018;6(11):e1196–e1252. doi:10.1016/S2214-109X(18)30386-3
3. Advisory Committee on the Safety of Nuclear Installations. Health and Safety Commision. Great Britain. ACSNI. Human Factor Study Group. Third Report. Organising for Safety. Sudbury, England: H.M.S.O; 1993.
4. Hellings J, Schrooten W, Klazinga N, Vleugels A. Challenging patient safety culture: survey results. Int J Health Care Qual Assur. 2007;20(7):620–632. doi:10.1108/09526860710822752
5. World Health Organization. Patient Safety 2020. World Health Organization; 2020:232.
6. Nieva VF, Sorra J. Safety culture assessment: a tool for improving patient safety in healthcare organizations. Qual Saf Health Care. 2003;12 Suppl 2:ii17–23. doi:10.1136/qhc.12.suppl_2.ii17
7. Top M, Tekingündüz S. Patient safety culture in a Turkish Public Hospital: a Study of Nurses’ perceptions about patient safety. Syst Pract Action Res. 2015;28(2):87–110. doi:10.1007/s11213-014-9320-5
8. Lee SE, Scott LD, Dahinten VS, Vincent C, Lopez KD, Park CG. Safety culture, patient safety, and quality of care outcomes: a literature review. West J Nurs Res. 2019;41(2):279–304. doi:10.1177/0193945917747416
9. Julia Hiromi Hori O, Tais Freire G, Marcus Tolentino S. Healthcare professional’s perception of patient safety measured by the hospital survey on patient safety culture: a systematic review and meta-analysis. Sci World J. 2018;2018(11). doi:10.1155/2018/9156301
10. Sorra JS, Nieva VF. Hospital Survey on Patient Safety Culture. Prepared by Westat, Under Contract No. 290-96-0004. AHRQ Publication No. 04-0041. Rockville: Agency for Healthcare Research and Quality; 2004.
11. Tang Chi T. Survey about patient safety culture at Children’s Hospital I in 2012. J Med Ho Chi Minh City. 2012;18(4):8.
12. Huong Tran L, Thanh Pham Q, Nguyen Dinh H, Tran TN, Bui TT. Assessment of Patient Safety Culture in Public General Hospital in Capital City of Vietnam. Health Services Insights; 2021:14.
13. Tran HTN, Pham TQ, Tran HL, Nguyen HD, Nguyen TM, Bui HTT. Patient safety culture in 2 public hospitals in Vietnam: a mixed method study. J Nurs Care Qual. 2021;37:E39–E47. doi:10.1097/NCQ.0000000000000597
14. Luong QD. Assessing the Perceptions of the Health Care Workforce Toward the Patient Safety Culture in Vietnamese Hospitals. Int Surg. 2019;104(11–12):590–607. doi:10.9738/INTSURG-D-15-00308.1
15. Kang S, Ho TTT, Lee NJ. Comparative Studies on Patient Safety Culture to Strengthen Health Systems Among Southeast Asian Countries. Front Public Health. 2020;8:600216. doi:10.3389/fpubh.2020.600216
16. Mekonnen AB, McLachlan AJ, J-aE B, Mekonnen D, Abay Z. Hospital survey on patient safety culture in Ethiopian public hospitals: a cross-sectional study. Saf Health. 2017;3. doi:10.1186/s40886-017-0062-9
17. Saleh Aboufour MA, Subbarayalu AV. Perceptions of patient safety culture among healthcare professionals in Ministry of Health hospitals in Eastern Province of Saudi Arabia. Inform Med Unlocked. 2022;28:100858. doi:10.1016/j.imu.2022.100858
18. Ricklin ME, Hess F, Hautz WE. Patient safety culture in a university hospital emergency department in Switzerland - a survey study. GMS J Med Educ. 2019;36(2). doi:10.3205/zma001222
19. Scherer D, Fitzpatrick JJ. Perceptions of patient safety culture among physicians and RNs in the perioperative area. Aorn j. 2008;87(1):163–175. doi:10.1016/j.aorn.2007.07.003
20. Batista J, EDdA C, Alpendre FT, da Silva DP, Brandâo MB, Gabriel CS. Differences between nursing and medical professionals regarding the surgical patient safety culture. Enfermería Global. 2021;20(3):114–126.
21. Alsabri M, Abdalaziz M, Farouk A, et al. Patient Safety Culture in Emergency Departments of Yemeni Public Hospitals: A Survey Study. Front Emerg Med, Tehran University of Medical Sciences; 2021.
22. World Health Organization. Patient Safety: Making Health Care Safer. Geneva: World Health Organization; 2017.
23. Yu B, Wen CF, Lo HL, Liao HH, Wang PC. Improvements in patient safety culture: a national Taiwanese survey, 2009-16. Int J Qual Health Care. 2020;32(1):A9–a17. doi:10.1093/intqhc/mzz099
24. Huang CH, Wu HH, Lee YC. The perceptions of patient safety culture: a difference between physicians and nurses in Taiwan. Appl Nurs Res. 2018;40:39–44. doi:10.1016/j.apnr.2017.12.010
25. Schmidt J, Gambashidze N, Manser T, et al. Does interprofessional team-training affect nurses’ and physicians’ perceptions of safety culture and communication practices? Results of a pre-post survey study. BMC Health Serv Res. 2021;21(1):341. doi:10.1186/s12913-021-06137-5
26. Zhu J. Measurement equivalence of patient safety climate in Chinese hospitals: can we compare across physicians and nurses? Int J Qual Health Care. 2019;31(6):411–418. doi:10.1093/intqhc/mzy132
27. Listyowardojo TA, Nap RE, Johnson A. Variations in hospital worker perceptions of safety culture. Int J Qual Health Care. 2012;24(1):9–15. doi:10.1093/intqhc/mzr069
28. Dodek PM, Wong H, Jaswal D, et al. Organizational and safety culture in Canadian intensive care units: relationship to size of intensive care unit and physician management model. J Crit Care. 2012;27(1):11–17. doi:10.1016/j.jcrc.2011.07.078
29. Alzahrani N, Jones R, Abdel-Latif ME. Attitudes of doctors and nurses toward patient safety within emergency departments of two Saudi Arabian hospitals. BMC Health Serv Res. 2018;18(1):736. doi:10.1186/s12913-018-3542-7
30. Nie Y, Mao X, Cui H, He S, Li J, Zhang M. Hospital survey on patient safety culture in China. BMC Health Serv Res. 2013;13:228. doi:10.1186/1472-6963-13-228
31. Notaro KA, Corrêa AD, Tomazoni A, Rocha PK, Manzo BF. Safety culture of multidisciplinary teams from neonatal intensive care units of public hospitals. Rev Lat Am Enfermagem. 2019;27:e3167. doi:10.1590/1518-8345.2849.3167
32. Wilson B, Bekker HL, Fylan F. Reporting of clinical adverse events scale: a measure of doctor and nurse attitudes to adverse event reporting. Qual Saf Health Care. 2008;17(5):364. doi:10.1136/qshc.2006.021691
33. Verbeek-Van Noord I, Wagner C, Van Dyck C, Twisk JW, De Bruijne MC. Is culture associated with patient safety in the emergency department? A study of staff perspectives. Int J Qual Health Care. 2014;26(1):64–70. doi:10.1093/intqhc/mzt087
34. Bottcher B, Abu-El-Noor N, Abuowda Y, et al. Attitudes of doctors and nurses to patient safety and errors in medical practice in the Gaza-Strip: a cross-sectional study. BMJ Open. 2019;9:8. doi:10.1136/bmjopen-2018-026788
35. Liu C, Liu W, Wang Y, Zhang Z, Wang P. Patient safety culture in China: a case study in an outpatient setting in Beijing. BMJ Qual Saf. 2014;23(7):556–564. doi:10.1136/bmjqs-2013-002172
36. Tricarico P, Castriotta L, Battistella C, et al. Professional attitudes toward incident reporting: can we measure and compare improvements in patient safety culture? Int J Qual Health Care. 2017;29(2):243–249. doi:10.1093/intqhc/mzx004
37. Taylor JA, Brownstein D, Christakis DA, et al. Use of incident reports by physicians and nurses to document medical errors in pediatric patients. Pediatrics. 2004;114(3):729–735. doi:10.1542/peds.2003-1124-L
38. Rich A, Viney R, Griffin A. Understanding the factors influencing doctors’ intentions to report patient safety concerns: a qualitative study. J R Soc Med. 2019;112(10):428–437. doi:10.1177/0141076819877542
39. McArde D, Burns N, Ireland A. Attitudes and beliefs of doctors towards medication error reporting. Int J Health Care Qual Assur. 2003;16(6/7):326–333. doi:10.1108/09526860310499981
40. Ministry of Health. Joint Annual Health Review. Vietnam’s Health System on the Threshold of the Five-Year Plan 2011–2015. Ministry of Health of Vietnam Hanoi; 2010.
41. Ministry of Health. Hospital Regulation. Hanoi: Medical Publishing House; 1997.
42. Vietnam Medical Services Administration. Circular on Implementation Quality Management of Curative Care in Hospitals. Vietnam Medical Services Administration; 2013.
43. Vietnam Medical Services Administration. Training Program on Patient Safety. Hanoi: Vietnam; 2014.
44. Azyabi A, Karwowski W, Davahli MR. Assessing patient safety culture in hospital settings. Int J Environ Res Public Health. 2021;18:5. doi:10.3390/ijerph18052466
45. Boughaba A, Aberkane S, Fourar Y-O, Djebabra M. Study of safety culture in healthcare institutions: case of an Algerian hospital. Int J Health Care Qual Assur. 2019;32:1081–1097. doi:10.1108/IJHCQA-09-2018-0229
46. Tereanu C, Sampietro G, Sarnataro F, et al. Exploring patient safety culture in preventive medicine settings: an experience from Northern Italy. J Prev Med Hyg. 2017;58(2):E121–e129.
47. Aboul-Fotouh AM, Ismail NA, Ez Elarab HS, Wassif GO. Assessment of patient safety culture among healthcare providers at a teaching hospital in Cairo, Egypt. East Mediterr Health J. 2012;18(4):372–377. doi:10.26719/2012.18.4.372
48. Habibi M, Fesharaki MG, Samadinia H, Mohamadian M, Anvari S. Patient safety culture and factors that impact that culture in Tehran Hospitals in 2013. Iran Red Crescent Med J. 2017;19(1):1–5.
49. Danielsson M, Nilsen P, Rutberg H, Carlfjord S. The professional culture among physicians in Sweden: potential implications for patient safety. BMC Health Serv Res. 2018;18(1):543. doi:10.1186/s12913-018-3328-y
50. Ministry of Health, Health Partnership Group. Joint Annual Health Review 2016. Ministry of Health, Health Partnership Group; 2016.
51. Le G, Thu TB, Mirzoev T, Thanh Nguyen H. Negotiating Compliance: the Case of Autonomous Hospitals in Vietnam. Dev Policy Rev. 2015;33(3):373–390. doi:10.1111/dpr.12112
52. Fujita S, Seto K, Ito S, Wu Y, Huang CC, Hasegawa T. The characteristics of patient safety culture in Japan, Taiwan and the United States. BMC Health Serv Res. 2013;13:20. doi:10.1186/1472-6963-13-20
53. Albalawi A, Kidd L, Cowey E. Factors contributing to the patient safety culture in Saudi Arabia: a systematic review. BMJ Open. 2020;10(10):e037875. doi:10.1136/bmjopen-2020-037875
54. Wu Y, Fujita S, Seto K, et al. The impact of nurse working hours on patient safety culture: a cross-national survey including Japan, the United States and Chinese Taiwan using the Hospital Survey on Patient Safety Culture. BMC Health Serv Res. 2013;13:394. doi:10.1186/1472-6963-13-394
55. Harrison R, Sharma A, Walton M, et al. Responding to adverse patient safety events in Viet Nam. BMC Health Serv Res. 2019;19(1):677. doi:10.1186/s12913-019-4518-y
56. Ng’ang’a N, Byrne MW, Ngo TA. In their own words: the experience of professional nurses in a Northern Vietnamese women’s hospital. Contemp Nurse. 2014;47(1/2):168–179. doi:10.1080/10376178.2014.11081918
57. Lyndon A, Zlatnik MG, Wachter RM. Effective physician-nurse communication: a patient safety essential for labor and delivery. Am J Obstet Gynecol. 2011;205(2):91–96. doi:10.1016/j.ajog.2011.04.021
58. Nguyen Van H, Nguyen ATH, Nguyen TTH, et al. Individual and occupational differences in perceived organisational culture of a central hospital in Vietnam. Biomed Res Int. 2018;2018:3759290. doi:10.1155/2018/3759290
59. Boussat B, Seigneurin A, Giai J, Kamalanavin K, Labarère J, François P. Involvement in root cause analysis and patient safety culture among hospital care providers. J Patient Saf. 2021;17(8):e1194–e1201. doi:10.1097/PTS.0000000000000456
60. National Academies of Sciences E, and Medicine. Crossing the Global Quality Chasm: Improving Health Care Worldwide. Washington, DC: The National Academies Press; 2018.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Level of Patient Safety Culture Awareness Among Healthcare Workers
Albaalharith T, A'aqoulah A
Journal of Multidisciplinary Healthcare 2023, 16:321-332
Published Date: 2 February 2023
Perceived Relationship Between Horizontal Violence and Patient Safety Culture Among Nurses
Jaber HJ, Abu Shosha GM, Al-Kalaldeh MT, Oweidat IA, Al-Mugheed K, Alsenany SA, Farghaly Abdelaliem SM
Risk Management and Healthcare Policy 2023, 16:1545-1553
Published Date: 14 August 2023
Instruments for Measuring Healthcare Professionals’ Medication Safety Competence: A Scoping Review
Stephan C, Kloor D, Wurmbach VS, Mahler C
Journal of Multidisciplinary Healthcare 2025, 18:1745-1758
Published Date: 25 March 2025
Knowledge, Attitude, and Practice of Palliative Care Among Physicians and Nurses in Intensive Care Units in Shanghai, China
He X, Cai H, Zhang J, Chen W, Zhu B
Journal of Multidisciplinary Healthcare 2025, 18:2441-2449
Published Date: 1 May 2025
Factors Associated with Work Life Balance Among Nurses in Hospitals: A Socio-Ecological Scoping Review
Widayana IGAA, Agustina HR, Mediawati AS
Journal of Multidisciplinary Healthcare 2025, 18:4511-4521
Published Date: 31 July 2025