Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 19
GLP-1 Receptor Agonists Reduce Aortic Dissection and Hypertensive Crisis in Diabetic Patients with Aortic Aneurysm: A Retrospective Cohort Study
Authors Tsai YF ![]() , Lin HT
, Lin HT ![]() , Liu YF, Chang R, Wu SC
, Liu YF, Chang R, Wu SC ![]()
Received 30 March 2026
Accepted for publication 13 May 2026
Published 23 May 2026 Volume 2026:19 612622
DOI https://doi.org/10.2147/DMSO.S612622
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Donald McClain
Yung-Fong Tsai,1,2 Huan-Tang Lin,1– 3 Yu-Fang Liu,4 Renin Chang,5– 7,* Shao-Chun Wu2,8,*
1Department of Anesthesiology, Chang Gung Memorial Hospital at Linkou, Taoyuan, Taiwan; 2College of Medicine, Chang Gung University, Taoyuan, Taiwan; 3Neuroscience Research Center, Chang Gung Memorial Hospital at Linkou, Taoyuan, Taiwan; 4Department of Anesthesiology, China Medical University Hospital, Taichung, Taiwan; 5Department of Medical Education and Research, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan; 6Center of General Education, Cheng Shiu University, Kaohsiung, Taiwan; 7Center of General Education, Shu-Zen Junior College of Medicine and Management, Kaohsiung, Taiwan; 8Department of Anesthesiology, Kaohsiung Chang Gung Memorial Hospital, Kaohsiung, Taiwan
*These authors contributed equally to this work
Correspondence: Shao-Chun Wu, Department of Anesthesiology, Kaohsiung Chang Gung Memorial Hospital, No. 123, Dapi Road, Niaosong Dist, Kaohsiung, 833, Taiwan, Tel +886-7-7317123 ext. 5041, Email [email protected]; [email protected] Renin Chang, Department of Medical Education and Research, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan, Email [email protected]
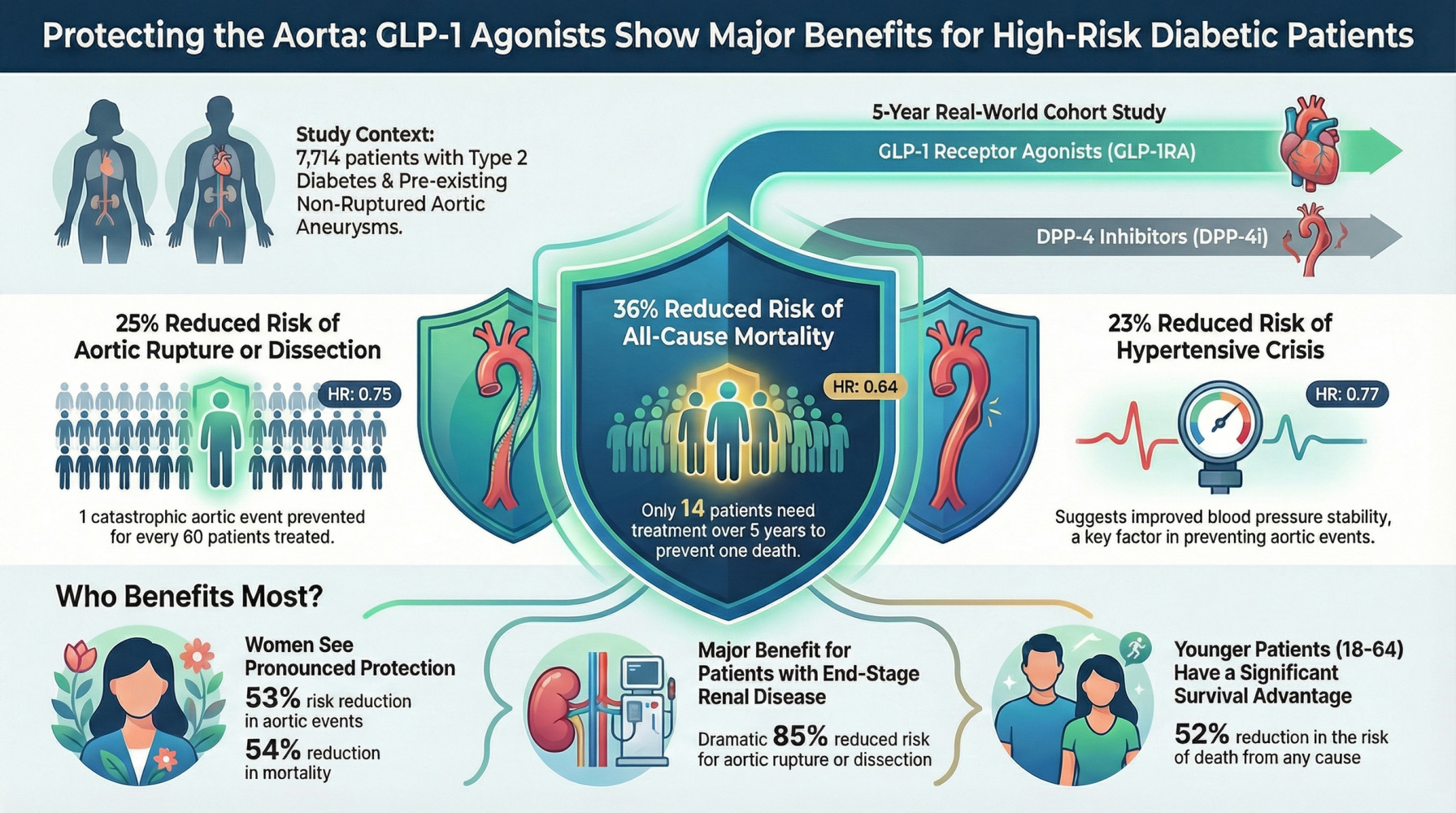
Purpose: Aortic aneurysm rupture and dissection carry mortality exceeding 50%, yet evidence-based medical therapies for this high-risk population remain limited. Despite mechanistic evidence suggesting glucagon-like peptide-1 receptor agonists (GLP-1RAs) stabilize vascular inflammation, no large-scale study has evaluated their impact on acute aortic events in diabetic patients with pre-existing aortic aneurysm.
Methods: This retrospective active-comparator new-user cohort study utilized TriNetX data from 152 US healthcare organizations (2016– 2023). A total of 11,581 adults with type 2 diabetes and documented non-ruptured aortic aneurysm initiating GLP-1RA (n=5676) or dipeptidyl peptidase-4 inhibitors (DPP-4i; n=5905) were identified. DPP-4i was selected as the active comparator given its documented cardiovascular neutrality, whereas sodium-glucose cotransporter-2 inhibitors were not used as a comparator due to their established cardiovascular benefits. After 1:1 propensity-score matching, 3857 patients per group were analyzed using Cox proportional hazards models.
Results: GLP-1RA therapy was associated with lower risks of aortic rupture/dissection requiring surgical repair (hazard ratio [HR] 0.75, 95% CI 0.60– 0.94; P=0.013), hypertensive crisis (HR 0.77, 95% CI 0.61– 0.96; P=0.022), and all-cause mortality (HR 0.64, 95% CI 0.57– 0.72; P< 0.001). Numbers needed to treat were 60, 81, and 14 over 5 years, respectively.
Conclusion: In diabetic patients with pre-existing aortic aneurysm, GLP-1RA therapy was associated with lower incidence of aortic rupture/dissection, hypertensive crisis, and mortality compared with DPP-4i, supporting preferential consideration of GLP-1RA in this high-risk population.
Keywords: aortic aneurysm, aortic dissection, glucagon-like peptide-1 receptor agonist, diabetes mellitus, cardiovascular outcomes, real-world evidence
Graphical Abstract:
Introduction
Type 2 diabetes mellitus (T2DM) represents a major global health burden, driven predominantly by accelerated macrovascular complications and cardiovascular mortality.1,2 Despite advances in glycemic control, lipid management, and blood pressure optimization, patients with T2DM continue to face substantially elevated cardiovascular risk, underscoring an urgent need for therapeutic strategies that extend beyond traditional metabolic targets.3 Among the most catastrophic vascular complications are aortic aneurysm (AA) and aortic dissection (AD), conditions characterized by progressive degradation of the aortic wall extracellular matrix, culminating in life-threatening rupture or dissection events with substantial mortality.4,5 While T2DM has paradoxically been associated with slower abdominal aortic aneurysm growth in some epidemiological studies,6,7 diabetic patients with established aortic disease nonetheless remain at substantial risk for acute aortic catastrophes, particularly in the setting of suboptimal blood pressure control and systemic inflammation.
In the context of T2DM, aortic aneurysm formation exhibits distinct pathophysiological features compared with non-diabetic populations. Chronic hyperglycaemia leads to accumulation of advanced glycation end-products (AGEs), which induce cross-linking of collagen and elastin within the aortic wall, increasing vascular stiffness, which may contribute to the observed attenuation of aneurysm expansion in epidemiological studies.6,7 However, this apparent protective effect is counterbalanced by enhanced oxidative stress and endothelial dysfunction, which promote medial degeneration and structural fragility.8 In addition, diabetes-related alterations in vascular smooth muscle cell phenotype and impaired extracellular matrix turnover may further compromise aortic wall integrity.9 These mechanisms may explain the paradox whereby diabetes is associated with slower aneurysm growth but does not confer protection against acute aortic complications such as dissection or rupture.
Glucagon-like peptide-1 receptor agonists (GLP-1RAs) have fundamentally transformed T2DM management, with well-established cardiovascular benefits. Given these pathophysiological mechanisms, the pleiotropic cardiovascular protective mechanisms of GLP-1RAs provide compelling biological rationale for potential benefits in aortic disease stabilization.10,11 Beyond glycemic control, these agents exert multifaceted effects including systolic blood pressure reduction of 2–5 mmHg through natriuresis and sympathetic modulation,12–14 anti-inflammatory actions with suppression of C-reactive protein and interleukin-6,15,16 and direct endothelial protection mediated by GLP-1 receptors expressed on vascular endothelium.17,18 Emerging preclinical evidence demonstrates that liraglutide attenuates angiotensin II–induced aortic dissection and aneurysm progression via inhibition of macrophage activation and reduction of matrix metalloproteinase-9 activity in murine models.19 A prospective human study further reported that GLP-1RA therapy slowed ascending aortic dilatation progression over 24 months, accompanied by decreased circulating MMP-9 and increased tissue inhibitor of metalloproteinases-1 (TIMP-1) concentrations.20
Despite emerging mechanistic and translational evidence,19,20 no large-scale clinical study has evaluated whether GLP-1RA therapy can prevent acute aortic events in patients with established non-ruptured aneurysms. A further critical and unexplored dimension is the relationship between GLP-1RA therapy and acute hypertensive crisis. Hypertension is present in approximately 75% of patients with aortic dissection.4,5 Episodic hypertensive crisis, defined by acute blood pressure elevation exceeding 180/120 mmHg with or without end-organ damage, constitutes a direct biomechanical precipitant of aortic rupture and dissection through sudden increases in aortic wall shear stress and intraluminal pressure. Notably, hypertensive crisis has not been evaluated as a predefined endpoint in major GLP-1RA outcome trials, leaving its clinical relevance in patients with aortic aneurysm uncertain. This knowledge gap is of particular importance in patients with pre-existing aortic aneurysm, in whom prevention of episodic hypertensive crisis may represent a discrete and actionable therapeutic target for reducing catastrophic aortic events.
We therefore conducted this large real-world cohort study (n=7714 propensity-matched patients) utilizing DPP-4 inhibitors as an active comparator, a methodologically rigorous choice supported by their cardiovascular neutrality. This design isolates GLP-1RA-specific pleiotropic effects from incretin-related mechanisms. We hypothesized that, in T2DM patients with pre-existing non-ruptured aortic aneurysm, GLP-1RA therapy would be associated with reduced risks of aortic rupture or dissection requiring surgical repair, hypertensive crisis, and all-cause mortality compared with DPP-4 inhibitor therapy, with consistent associations maintained across clinical subgroups.
Materials and Methods
Data Source
This was a retrospective, active-comparator, new-user, propensity score–matched cohort study using de-identified electronic health record data from the TriNetX Global Collaborative Network, a large-scale international health research network aggregating de-identified electronic health records from approximately 275 million patients across 19 countries. For cohort definition and analysis, the study drew on electronic health records from 152 participating US healthcare organizations, providing comprehensive longitudinal data including demographics, diagnostic codes, procedural history, prescription information, laboratory results, and mortality data. For this analysis, only data from participating US healthcare organizations were used. All cohort definitions, exposures, outcomes, and covariates were specified a priori using standardized code lists (ICD-10-CM, CPT/HCPCS, and RxNorm), and no free-text data extraction was performed, thereby minimizing misclassification bias.
Ethics Approval and Informed Consent
This study utilized de-identified data and was determined exempt from institutional review board approval under Kaohsiung Veterans General Hospital (approval number: KSVGH24-CT3-09). Because all data were de-identified and compliant with the Health Insurance Portability and Accountability Act (HIPAA), informed consent was waived. The study was conducted in accordance with the Declaration of Helsinki. All data were de-identified in compliance with HIPAA regulations, consistent with established de-identification standards (45 CFR §164.514(b)(2)), prior to release to investigators.
Study Population
The study population included adults (≥18 years) with documented type 2 diabetes mellitus and non-ruptured aortic aneurysm who received either a GLP-1RA or DPP-4i between January 1, 2016, and December 31, 2023. Patients were excluded if they had a history of ruptured aortic aneurysm or prior aortic repair procedures (Table S1). The flow diagram illustrating patient selection is presented in Figure 1. A total of 11,581 patients were identified (GLP-1RA, n=5676; DPP-4i, n=5905); after 1:1 propensity score matching, 3857 patients remained in each arm (total matched cohort n=7714).
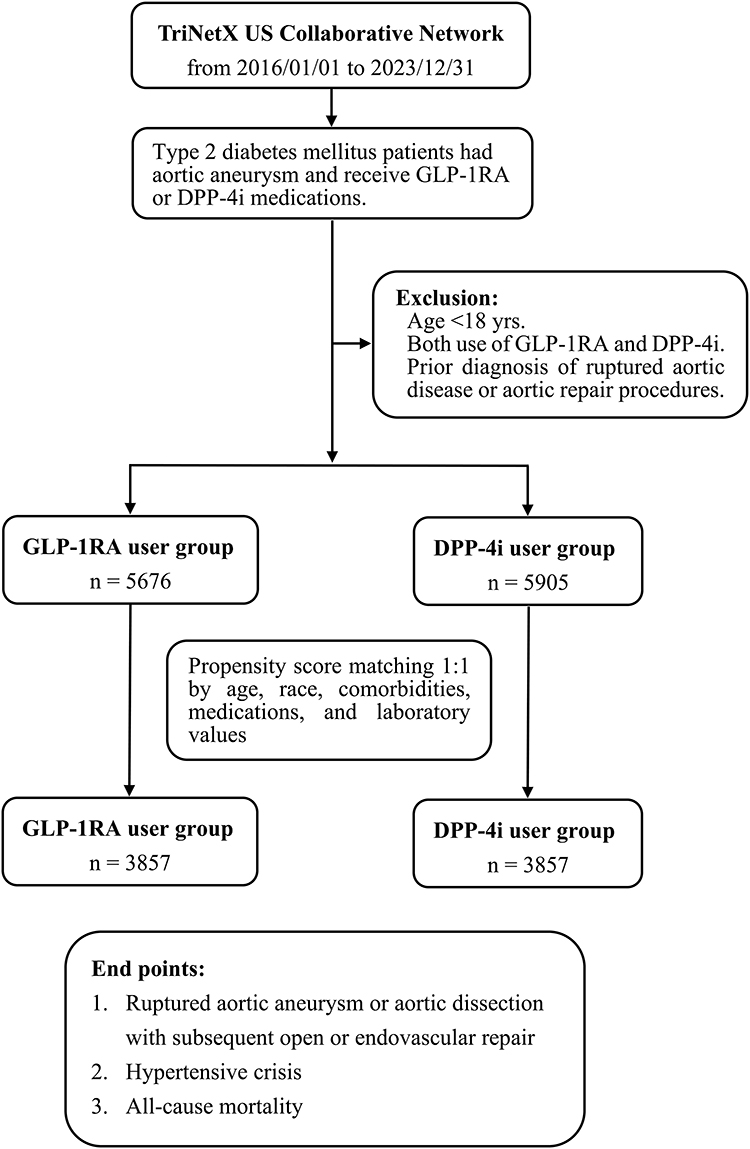 |
Figure 1 Study Flow Diagram and Cohort Selection. Flowchart illustrating patient selection from the TriNetX research network (152 US healthcare organizations, January 1, 2016 to December 31, 2023) and final cohort allocation after 1:1 propensity score matching. Adults with type 2 diabetes and non-ruptured aortic aneurysm initiating either GLP-1RA (n=5676) or DPP-4i (n=5905) were identified, yielding a total cohort of 11,581 patients. Patients were excluded if they were <18 years old or had a history of ruptured aortic aneurysm or prior aortic repair. After matching, 3857 patients per arm were analyzed (total matched cohort n=7714). Abbreviations: GLP-1RA, glucagon-like peptide-1 receptor agonist; DPP-4i, dipeptidyl peptidase-4 inhibitor. |
Exposure Definition and Index Date
For the GLP-1RA cohort, the index date was defined as the date of first GLP-1RA prescription, with no use of DPP-4i during the period prior to index date and for 36 months thereafter. For the DPP-4i cohort, the index date was defined as the date of first DPP-4i prescription, with no use of GLP-1RA during the period prior to index date and for 36 months thereafter.
Comparator Selection and Rationale
DPP-4 inhibitors were selected as the active comparator because they share the incretin pathway with GLP-1 receptor agonists but do not directly activate the GLP-1 receptor. DPP-4i are generally considered cardiovascular neutral based on large randomized cardiovascular outcome trials.21 These agents are prescribed in overlapping patient populations with GLP-1RA, thereby reducing channeling bias.
SGLT2 inhibitors were not selected as the comparator because they confer established cardiovascular and renal benefits, as demonstrated in major outcome trials,22 and are preferentially prescribed to patients with heart failure, chronic kidney disease, and higher baseline cardiovascular risk, resulting in systematic differences in baseline risk profiles and potential channeling bias. In addition, comparison between two active cardioprotective agents may attenuate observable differences and limit interpretability with respect to aortic-specific outcomes.
Propensity-Score Matching
To reduce confounding, propensity scores were estimated using logistic regression models incorporating age, sex, race, documented comorbidities, concomitant medications, and availability of key laboratory values. Patients in the GLP-1RA cohort were matched 1:1 with patients in the DPP-4i cohort using nearest-neighbor matching without replacement, with a caliper width of 0.1 pooled standard deviations of the logit of the propensity score. Availability of laboratory measurements (eg, HbA1c, eGFR, lipid profiles) within 12 months prior to the index date was included as a matching covariate to account for missingness. Cohort queries were independently constructed and executed, with independent verification performed by a separate investigator. Cohort counts were cross-checked, and any discrepancies were resolved through iterative re-evaluation of query definitions until full agreement was achieved.
Outcomes and Follow-Up
Participants were followed from the index date until the earliest occurrence of the outcome of interest, death, loss to follow-up, or administrative censoring (August 2, 2025). For each outcome, follow-up was defined separately. The primary outcome was ruptured aortic aneurysm or aortic dissection requiring open or endovascular repair (Table S1). Secondary outcomes included hypertensive crisis and all-cause mortality.
Statistical Analysis
Baseline characteristics were compared using standardized differences. Cox proportional hazards models, stratified by matched pairs, estimated hazard ratios (HRs) and 95% confidence intervals (CIs) for outcomes. The proportional hazards assumption was assessed using Schoenfeld residuals within the TriNetX platform; however, detailed diagnostic outputs were not retained. Kaplan-Meier methods estimated time-to-event distributions, with between-group differences compared using log-rank tests. All analyses were conducted within the TriNetX Analytics environment. Statistical significance was defined as 2-sided P<0.05. Numbers needed to treat (NNTs) were derived from absolute risk differences at fixed time points (5 years), rather than from hazard ratios. This study is reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines (Table S2). Variables derived from coded data were treated as not recorded when absent and handled according to standard assumptions in real-world EHR-based studies; no imputation was performed.
Results
Study Population and Baseline Characteristics
Between January 1, 2016, and December 31, 2023, we identified 11,581 patients with type 2 diabetes mellitus and documented non-ruptured aortic aneurysm who received either a GLP-1RA (n=5676) or a DPP-4i (n=5905) from the TriNetX Global Collaborative Network. After 1:1 propensity-score matching with a caliper width of 0.1 standard deviations, 3857 patients remained in each treatment cohort (Figure 1). Follow-up extended from the index date to the occurrence of study outcomes, death, loss to follow-up, or administrative censoring. Baseline characteristics were generally well balanced between groups, although a small number of covariates retained residual imbalance (standardized difference >0.10), as shown in Table 1. The mean age was approximately 69 years, about one-quarter were women, and prevalence of major comorbidities was similar across groups.
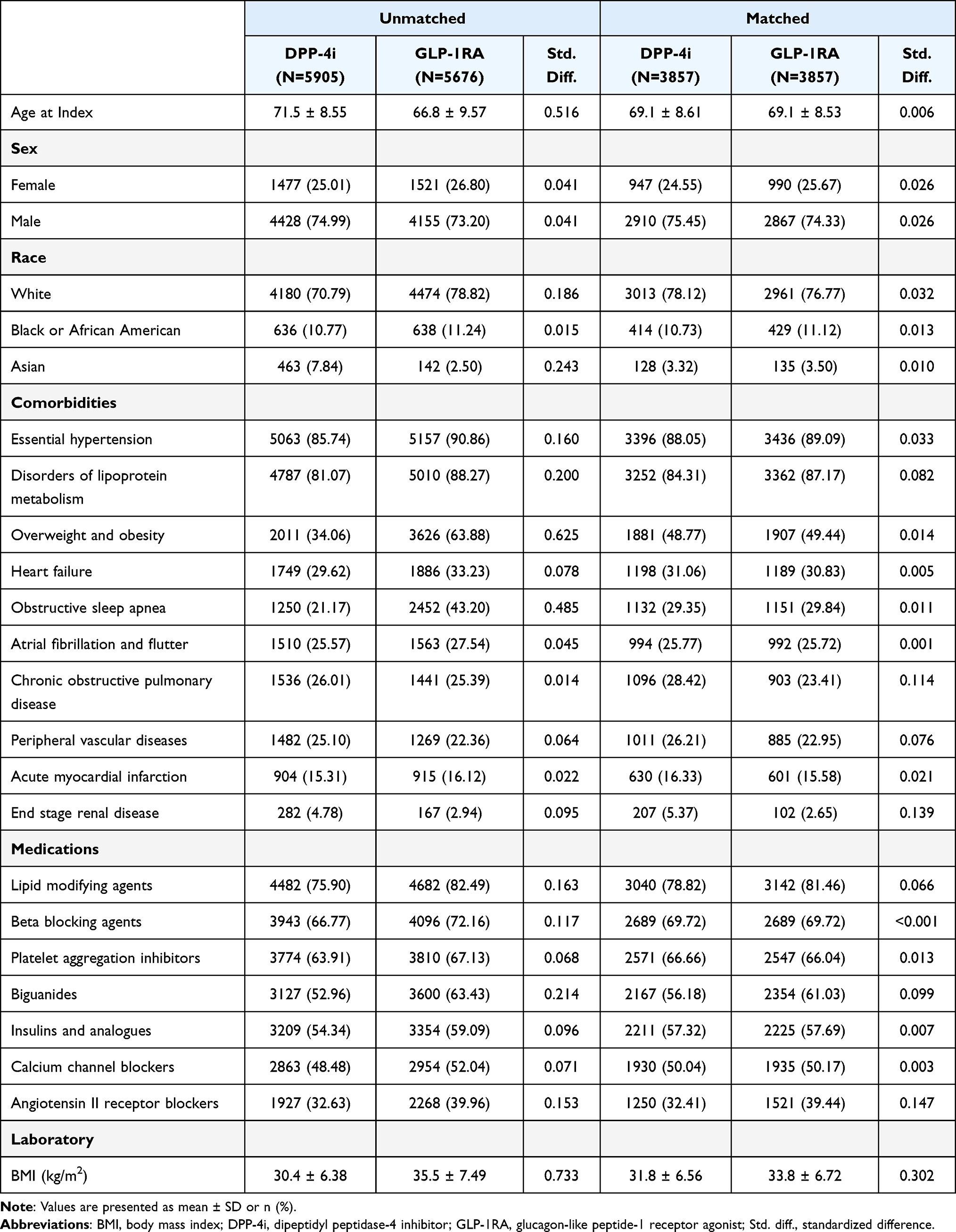 |
Table 1 Baseline Characteristics of the GLP-1RA Cohort and DPP-4i Cohort |
Primary Outcome: Aortic Rupture or Dissection Requiring Intervention
The median follow-up was 31.1 months (interquartile range [IQR]: 17.8–44.4) in the GLP-1RA cohort and 44.0 months (IQR: 18.6–69.4) in the DPP-4i cohort. During follow-up, 169 patients (4.39%) in the GLP-1RA cohort and 234 patients (6.07%) in the DPP-4i cohort experienced the primary composite outcome of ruptured aortic aneurysm or aortic dissection requiring surgical or endovascular repair. The difference in follow-up duration likely reflects temporal differences in drug uptake, with GLP-1RA initiation occurring more frequently in later calendar years, resulting in shorter observable follow-up prior to administrative censoring. Kaplan-Meier analysis (Figure 2) showed early separation of cumulative incidence curves, which progressively widened over time. At 360 days, cumulative incidence was 1.68% (95% CI: 1.31–2.15) in the GLP-1RA group versus 2.18% (95% CI: 1.76–2.72) in the DPP-4i group. By 1800 days, cumulative incidence was 4.39% (95% CI: 3.60–5.36) versus 6.07% (95% CI: 5.19–7.09) (log-rank P=0.013).
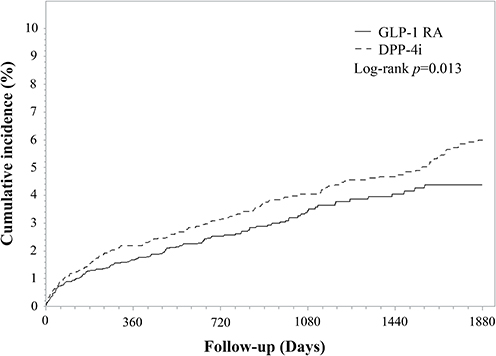 |
Figure 2 Cumulative Incidence of Aortic Rupture or Dissection Requiring Surgical Intervention. Kaplan-Meier curves showing cumulative incidence of aortic rupture or dissection requiring surgical or endovascular repair. The GLP-1RA cohort exhibited lower cumulative incidence throughout follow-up (log-rank P=0.013). Abbreviations: GLP-1RA, glucagon-like peptide-1 receptor agonist; DPP-4i, dipeptidyl peptidase-4 inhibitor. |
In univariable Cox proportional hazards analysis, GLP-1RA use was associated with a lower hazard of the primary outcome compared with DPP-4i therapy (HR 0.75, 95% CI 0.60–0.94; P=0.013). This corresponded to an absolute risk reduction of 1.68 percentage points, yielding an NNT of 60 (95% CI: 35–150) over 5 years. Subgroup analyses (Figure 3) (exploratory and not powered for formal interaction testing) showed generally consistent trends across most categories. Female patients showed a lower hazard estimate (HR 0.47, 95% CI 0.29–0.76; P=0.002), and patients with end-stage renal disease showed a numerically lower hazard estimate (HR 0.15, 95% CI 0.03–0.67; P=0.004).
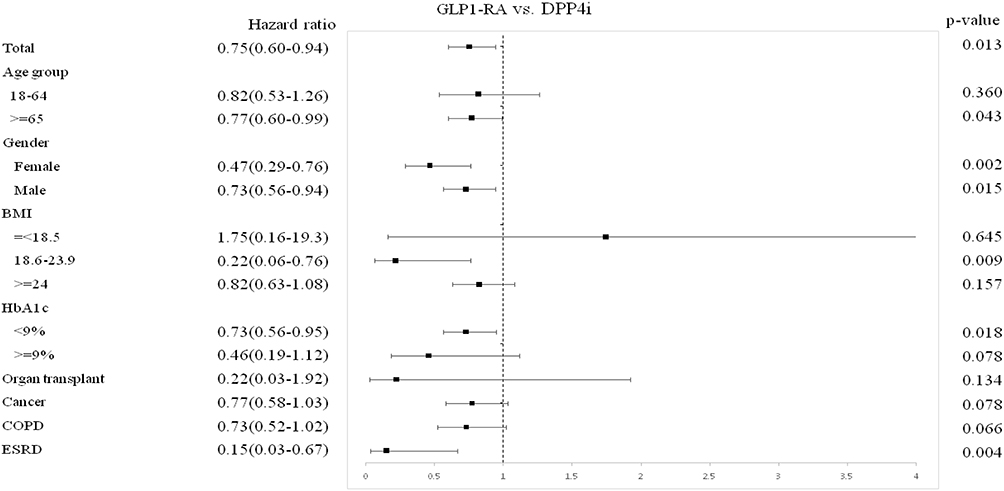 |
Figure 3 Subgroup Analysis for Aortic Rupture/Dissection Outcome. Forest plot displaying hazard ratios and 95% confidence intervals from univariable Cox regression analyses for aortic rupture or dissection requiring repair. Squares represent point estimates; horizontal lines indicate 95% CIs. Abbreviations: CI, confidence interval; HR, hazard ratio. |
Secondary Outcome: Hypertensive Crisis
During follow-up, 192 patients (4.97%) in the GLP-1RA cohort and 239 patients (6.20%) in the DPP-4i cohort experienced hypertensive crisis. The GLP-1RA cohort showed lower cumulative incidence (Figure 4). By 1800 days, cumulative incidence was 4.97% (95% CI: 4.00–6.17) versus 6.20% (95% CI: 5.33–7.22), with an absolute difference of 1.23 percentage points (log-rank P=0.022). In Cox proportional hazards analysis, GLP-1RA treatment was associated with a lower hazard (HR 0.77, 95% CI 0.61–0.96; P=0.022), translating to an NNT of 81 (95% CI: 48–200) over 5 years. Subgroup analyses (Figure 5) (exploratory) revealed similar directional trends across subgroups, including patients with organ transplantation (HR 0.27, 95% CI 0.09–0.82; P=0.013) and malignancy (HR 0.70, 95% CI 0.53–0.94; P=0.015).
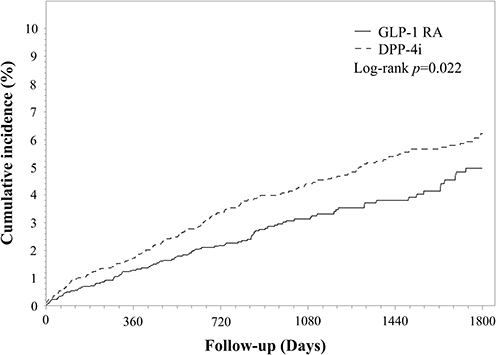 |
Figure 4 Cumulative Incidence of Hypertensive Crisis. Kaplan-Meier curves illustrating cumulative incidence of hypertensive crisis. Patients receiving GLP-1RA exhibited lower risk compared with DPP-4i throughout follow-up (log-rank P=0.022). Abbreviations: GLP-1RA, glucagon-like peptide-1 receptor agonist; DPP-4i, dipeptidyl peptidase-4 inhibitor. |
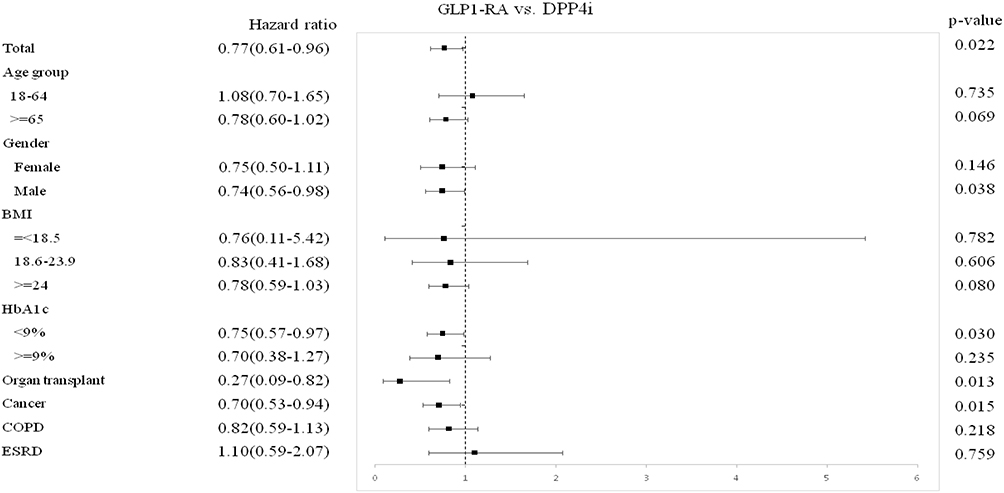 |
Figure 5 Subgroup Analysis for Hypertensive Crisis. Forest plot of univariable Cox regression analyses for hypertensive crisis. Hazard ratios and 95% confidence intervals are presented for GLP-1RA versus DPP-4i across patient subgroups. Abbreviations: CI, confidence interval; HR, hazard ratio. |
Secondary Outcome: All-Cause Mortality
During follow-up, 748 patients (19.39%) in the GLP-1RA cohort and 1026 patients (26.59%) in the DPP-4i cohort died from any cause. Kaplan-Meier survival curves (Figure 6) diverged early and continued to separate throughout follow-up. At 1800 days, survival probability was 80.61% (95% CI: 78.59–82.45) versus 73.41% (95% CI: 71.70–75.04) (log-rank P<0.0001), corresponding to an absolute difference of 7.20 percentage points. In Cox proportional hazards analysis, GLP-1RA treatment was associated with a lower hazard of all-cause mortality (HR 0.64, 95% CI 0.57–0.72; P<0.001), translating to an NNT of 14 (95% CI: 11–18) over 5 years. Consistent directional associations were observed across examined subgroups (Figure 7), with lower hazard estimates in younger patients (age 18–64 years: HR 0.48, 95% CI 0.36–0.64; P<0.001) and women (HR 0.46, 95% CI 0.36–0.58; P<0.001). Mortality patterns were similar across categories of body mass index, glycemic control levels, and major comorbidities. Incidence rates per 1000 person-years were not available from the extracted dataset; cumulative incidence estimates are therefore presented to describe absolute risk.
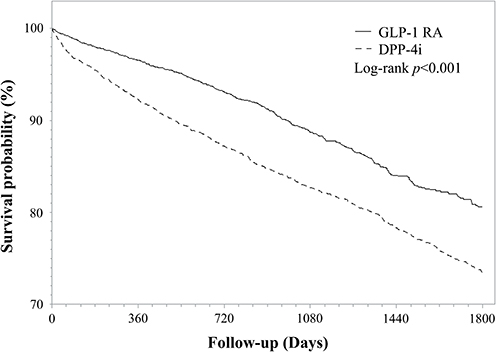 |
Figure 6 All-Cause Mortality During Follow-up. Kaplan-Meier survival curves showing GLP-1RA therapy was associated with significantly improved survival at 1800 days (80.61% vs 73.41%; log-rank P<0.0001), corresponding to an absolute risk reduction of 7.2 percentage points. Numbers at risk are displayed below the x-axis. Abbreviations: GLP-1RA, glucagon-like peptide-1 receptor agonist; DPP-4i, dipeptidyl peptidase-4 inhibitor. |
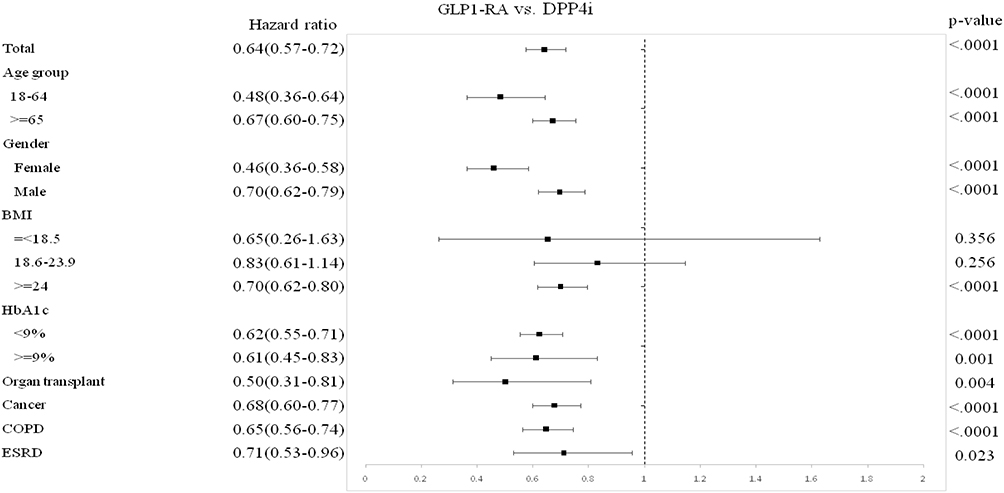 |
Figure 7 Subgroup Analysis for All-Cause Mortality. Forest plot displaying hazard ratios and 95% confidence intervals from univariable Cox regression analyses for all-cause mortality across predefined subgroups. GLP-1RA was associated with a 36% lower hazard of all-cause mortality compared with DPP-4i (HR 0.64, 95% CI 0.57–0.72; P<0.001), with consistent associations across all analyzed subgroups. Vertical dashed line indicates HR=1.0. Abbreviations: CI, confidence interval; HR, hazard ratio. |
Discussion
In this large-scale real-world cohort study of 7714 propensity-matched patients with type 2 diabetes mellitus and pre-existing non-ruptured aortic aneurysm, GLP-1RA therapy, compared with DPP-4i therapy, was associated with lower risks of aortic rupture or dissection requiring surgical intervention, hypertensive crisis, and all-cause mortality. These associations correspond to clinically relevant absolute risk differences over the observed follow-up period. To our knowledge, this is the first large-scale, real-world, active-comparator cohort analysis of GLP-1RA versus DPP-4i specifically in patients with pre-existing aortic aneurysm, addressing an important evidence gap in this high-risk population.
The observed association with lower all-cause mortality (HR 0.64) represents a clinically meaningful difference, with a number needed to treat (NNT; the number of patients who must receive GLP-1RA rather than DPP-4i to prevent one additional event over 5 years) of 14 comparing favorably with other established cardiovascular interventions.3,23 The mortality benefit was consistent across diverse subgroups (Figure 7), with pronounced effects in younger patients (HR 0.48) and women (HR 0.46). Even in high-risk populations with chronic obstructive pulmonary disease (HR 0.65), end-stage renal disease (HR 0.71), and malignancy (HR 0.68), GLP-1RA therapy maintained significant survival advantages. These findings align with evidence from meta-analyses and contemporary randomized trials showing that GLP-1RAs reduce major adverse cardiovascular events across diverse high-risk populations.24–26 Notably, the magnitude of the mortality association observed here is larger than the pooled mortality reduction of approximately 12% (HR ~0.88) reported in the Kristensen et al and Sattar et al meta-analyses of GLP-1RA cardiovascular outcome trials,3,23 likely reflecting the higher baseline mortality of our aortic-aneurysm cohort, the cardiovascular neutrality of the DPP-4i active comparator,21,27 and possibly residual healthy-initiator selection that cannot be fully excluded in pharmacoepidemiological analyses.
The 25% lower risk of aortic rupture or dissection requiring surgical intervention (HR 0.75) is consistent with the recognized cardiovascular benefits of GLP-1RAs in broader populations, and extends these observations into major aortic disease. The cumulative incidence curves diverged early and continued to widen, suggesting rapid and sustained associations with reduced aortic wall instability. While landmark cardiovascular outcome trials demonstrated reductions in MACE,28–30 none specifically examined outcomes in patients with pre-existing aortic aneurysm. Subgroup analyses showed particularly pronounced associations in female patients (HR 0.47) and patients with end-stage renal disease (HR 0.15), supporting preferential consideration of GLP-1RAs for secondary prevention in patients with T2DM and aortic aneurysm. Given the absence of formal interaction testing, these findings should be interpreted with caution.
Several mechanisms may underlie the observed aortic protection. Most notably, the lower incidence of acute hypertensive crisis observed here has not been previously reported in a real-world GLP-1RA cohort of patients with type 2 diabetes and aortic aneurysm, because hypertensive crisis was not included as a pre-specified endpoint in LEADER, SUSTAIN-6, REWIND, or SELECT.26,28–30 The observed lower hazard of hypertensive crisis (HR 0.77) suggests that GLP-1RAs may attenuate episodic hemodynamic surges that impose acute mechanical stress on a compromised aortic wall, a mechanistic pathway that is biologically plausible yet has remained empirically uncharacterized. GLP-1RAs reduce systolic blood pressure by 2–5 mmHg through multiple pathways, including natriuresis, sympathetic nervous system modulation, and atrial natriuretic peptide secretion.12–14 These cumulative antihypertensive mechanisms may be particularly protective against the episodic blood pressure surges that constitute the proximal hemodynamic trigger for aortic rupture and dissection in patients with pre-existing aneurysmal disease. Second, GLP-1RAs possess well-established anti-inflammatory properties, reducing systemic markers such as C-reactive protein and interleukin-6.15,16 Chronic vascular inflammation plays a central role in aortic wall degradation and aneurysm progression.8,9 Recent studies demonstrate that GLP-1RA treatment attenuates vascular inflammation and improves aortic pathology through reductions in matrix metalloproteinase activity, oxidative stress, and inflammatory signaling.19,31,32 Notably, Sardu et al demonstrated that GLP-1RA therapy attenuated ascending aortic dilatation progression over 24 months, accompanied by decreased MMP-9 and increased TIMP-1 concentrations.20 These mechanistic considerations may also help explain the apparent superiority of GLP-1RA over DPP-4i. GLP-1RAs bind and continuously activate vascular endothelial GLP-1 receptors at supraphysiologic concentrations, whereas DPP-4i act indirectly by prolonging the half-life of endogenous incretin hormones, producing only modest and intermittent receptor stimulation that may be insufficient to engage downstream anti-inflammatory and vasoprotective pathways.10,11 GLP-1RAs also yield more consistent suppression of inflammatory biomarkers and vasoprotective signaling than DPP-4i,15,16 providing a coherent biological framework for the differential outcomes observed.
Our findings have several important clinical implications. First, in patients with type 2 diabetes and pre-existing aortic aneurysm, GLP-1RA therapy warrants preferential consideration as a glucose-lowering agent. Second, benefits extend to high-risk subgroups including females, younger adults, and patients with end-stage renal disease, organ transplantation, or malignancy. Third, the marked reduction in hypertensive crisis underscores the importance of blood pressure management. Fourth, favorable NNTs support cost-effectiveness in this high-risk population. Finally, these findings have potential implications for clinical practice guidelines, providing evidence to support inclusion of aortic aneurysm as a high-risk condition warranting preferential GLP-1RA use.11,33
Strengths and Limitations
Our study has notable strengths, including large sample size (11,581 patients; 7714 matched), rigorous propensity score matching achieving satisfactory overall covariate balance, focus on an understudied high-risk population, examination of multiple clinically important outcomes, and longitudinal follow-up extending to 5 years. However, important limitations warrant consideration. First, the observational design precludes definitive causal inference despite propensity score matching, as residual confounding from unmeasured variables (eg, smoking status, aneurysm diameter and morphology, aneurysm growth rate, healthy-initiator selection) remains possible. Second, reliance on ICD-10-CM and CPT codes for adjudication of aortic events and hypertensive crisis is a recognized limitation of claims-based research; non-differential misclassification would generally bias estimates toward the null, although differential coding intensity between arms cannot be excluded. Medication adherence and agent-specific effects could not be verified. Third, we lack key clinical data including detailed aneurysm characteristics, serial blood pressure measurements, inflammatory biomarkers, and vascular imaging. Fourth, despite overall satisfactory propensity score matching, four covariates retained residual imbalance (standardized difference >0.10): BMI (33.8 versus 31.8 kg/m2; SMD 0.302), ARB use (39.4% versus 32.4%; SMD 0.147), ESRD (2.7% versus 5.4%; SMD 0.139), and COPD (23.41% versus 28.42%; SMD 0.114). Higher baseline BMI in the GLP-1RA cohort would attenuate rather than amplify the observed treatment effect, as greater adiposity confers higher basal cardiovascular risk. Higher ARB use in the GLP-1RA group may contribute modest positive confounding given evidence for ARB-mediated aortic protection. Lower ESRD prevalence in the GLP-1RA arm could similarly contribute modest positive confounding. A multivariable sensitivity Cox model adjusting for these four covariates could not be performed because the original TriNetX dataset is no longer re-accessible. Fifth, generalizability may be limited by the predominantly US-based study population. Sixth, extensive subgroup analyses without formal adjustment for multiple comparisons raise the possibility of type I errors. Finally, competing risks were not formally addressed. The new-user design minimized potential immortal time bias by aligning cohort entry at treatment initiation.
Conclusions
In this large real-world cohort of patients with type 2 diabetes and pre-existing aortic aneurysm, GLP-1RA therapy was associated with significantly lower risks of aortic rupture/dissection, hypertensive crisis, and all-cause mortality compared with DPP-4i therapy. The favorable NNTs, particularly 14 to prevent one death over 5 years, underscore clinical relevance. Our findings provide supportive evidence for preferential consideration of GLP-1RAs over DPP-4i in this high-risk population.
Abbreviations
AA, aortic aneurysm; AD, aortic dissection; CI, confidence interval; CVOT, cardiovascular outcome trial; DPP-4i, dipeptidyl peptidase-4 inhibitor; GLP-1RA, glucagon-like peptide-1 receptor agonist; HR, hazard ratio; IQR, interquartile range; MACE, major adverse cardiovascular events; MMP, matrix metalloproteinase; NNT, number needed to treat; STROBE, Strengthening the Reporting of Observational Studies in Epidemiology; T2DM, type 2 diabetes mellitus; TIMP-1, tissue inhibitor of metalloproteinases-1.
Data Sharing Statement
The datasets analyzed during the current study are available from the TriNetX research network but restrictions apply to the availability of these data. Data may be available from the corresponding authors upon reasonable request and with permission of TriNetX.
Author Contributions
Y.-F.T., H.-T.L., Y.-F.L., R.C., and S.-C.W. contributed to Conceptualization and Methodology. Y.-F.T., H.-T.L., and Y.-F.L. contributed to Data curation, Formal analysis, and Investigation. R.C. and S.-C.W. contributed to Supervision, Project administration, and Resources. Y.-F.T. and S.-C.W. contributed to Writing – original draft. All authors contributed to Validation, Visualization, and Writing – review & editing. All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. Renin Chang & Shao-Chun Wu share senior authorship.
Funding
This research was supported by grants from Kaohsiung Veterans General Hospital (KSVGH115-D01-1 and KSVGH115-D02-1), Taiwan.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Action to Control Cardiovascular Risk in Diabetes Study Group, Gerstein HC, Miller ME, et al. Effects of intensive glucose lowering in type 2 diabetes. N Engl J Med. 2008;358(24):2545–13. doi:10.1056/NEJMoa0802743
2. Rawshani A, Rawshani A, Franzen S, et al. Risk factors, mortality, and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med. 2018;379:633–644. doi:10.1056/NEJMoa1800256
3. Sattar N, Lee MMY, Kristensen SL, et al. Cardiovascular, mortality, and kidney outcomes with GLP-1 receptor agonists in patients with type 2 diabetes: a systematic review and meta-analysis of randomised trials. Lancet Diabetes Endocrinol. 2021;9:653–662. doi:10.1016/S2213-8587(21)00203-5
4. Howard DP, Banerjee A, Fairhead JF, et al. Population-based study of incidence and outcome of acute aortic dissection and premorbid risk factor control: 10-year results from the Oxford vascular study. Circulation. 2013;127:2031–2037. doi:10.1161/CIRCULATIONAHA.112.000483
5. Kent KC, Zwolak RM, Egorova NN, et al. Analysis of risk factors for abdominal aortic aneurysm in a cohort of more than 3 million individuals. J Vasc Surg. 2010;52:539–548. doi:10.1016/j.jvs.2010.05.090
6. Shantikumar S, Ajjan R, Porter KE, Scott DJ. Diabetes and the abdominal aortic aneurysm. Eur J Vasc Endovasc Surg. 2010;39:200–207. doi:10.1016/j.ejvs.2009.10.014
7. Takagi H, Umemoto T, Group A. Diabetes and abdominal aortic aneurysm growth. Angiology. 2016;67:513–525. doi:10.1177/0003319715602414
8. Hou N, Zhou H, Li J, Xiong X, Deng H, Xiong S. Macrophage polarization and metabolic reprogramming in abdominal aortic aneurysm. Immun Inflamm Dis. 2024;12:e1268. doi:10.1002/iid3.1268
9. Stepien KL, Bajdak-Rusinek K, Fus-Kujawa A, Kuczmik W, Gawron K. Role of extracellular matrix and inflammation in abdominal aortic aneurysm. Int J Mol Sci. 2022;23(19):11078. doi:10.3390/ijms231911078
10. Drucker DJ. Mechanisms of action and therapeutic application of glucagon-like peptide-1. Cell Metab. 2018;27:740–756. doi:10.1016/j.cmet.2018.03.001
11. Marx N, Husain M, Lehrke M, Verma S, Sattar N. GLP-1 receptor agonists for the reduction of atherosclerotic cardiovascular risk in patients with type 2 diabetes. Circulation. 2022;146:1882–1894. doi:10.1161/CIRCULATIONAHA.122.059595
12. Goud A, Zhong J, Peters M, Brook RD, Rajagopalan S. GLP-1 agonists and blood pressure: a review of the evidence. Curr Hypertens Rep. 2016;18:16. doi:10.1007/s11906-015-0621-6
13. Jarade C, Zolotarova T, Moiz A, Eisenberg MJ. GLP-1-based therapies for the treatment of resistant hypertension in individuals with overweight or obesity: a review. EClinicalMedicine. 2024;75:102789. doi:10.1016/j.eclinm.2024.102789
14. Katsurada K, Nakata M, Saito T, et al. Central glucagon-like peptide-1 receptor signaling via brainstem catecholamine neurons counteracts hypertension in spontaneously hypertensive rats. Sci Rep. 2019;9:12986. doi:10.1038/s41598-019-49364-x
15. Bray JJH, Foster-Davies H, Salem A, et al. Glucagon-like peptide-1 receptor agonists improve biomarkers of inflammation and oxidative stress: a systematic review and meta-analysis of randomised controlled trials. Diabetes Obes Metab. 2021;23:1806–1822. doi:10.1111/dom.14399
16. Ren Y, Chen Y, Zheng W, et al. The effect of GLP-1 receptor agonists on circulating inflammatory markers in type 2 diabetes patients: a systematic review and meta-analysis. Diabetes Obes Metab. 2025;27:3607–3626. doi:10.1111/dom.16366
17. Helmstadter J, Frenis K, Filippou K, et al. Endothelial GLP-1 (Glucagon-Like Peptide-1) receptor mediates cardiovascular protection by liraglutide in mice with experimental arterial hypertension. Arterioscler Thromb Vasc Biol. 2020;40:145–158. doi:10.1161/atv.0000615456.97862.30
18. Ussher JR, Drucker DJ. Glucagon-like peptide 1 receptor agonists: cardiovascular benefits and mechanisms of action. Nat Rev Cardiol. 2023;20:463–474. doi:10.1038/s41569-023-00849-3
19. Zhang K, Li R, Matniyaz Y, et al. Liraglutide attenuates angiotensin II-induced aortic dissection and aortic aneurysm via inhibiting M1 macrophage polarization in APOE (-/-) mice. Biochem Pharmacol. 2024;223:116170. doi:10.1016/j.bcp.2024.116170
20. Sardu C, Marfella LV, Fumagalli C, et al. GLP-1 receptor agonists are associated with reduced ascending aorta dilatation in patients with type 2 diabetes: a prospective study. Int J Mol Sci. 2025;26. doi:10.3390/ijms26209977
21. Scirica BM, Bhatt DL, Braunwald E, et al. Saxagliptin and cardiovascular outcomes in patients with type 2 diabetes mellitus. N Engl J Med. 2013;369:1317–1326. doi:10.1056/NEJMoa1307684
22. Zinman B, Wanner C, Lachin JM, et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med. 2015;373:2117–2128. doi:10.1056/NEJMoa1504720
23. Kristensen SL, Rorth R, Jhund PS, et al. Cardiovascular, mortality, and kidney outcomes with GLP-1 receptor agonists in patients with type 2 diabetes: a systematic review and meta-analysis of cardiovascular outcome trials. Lancet Diabetes Endocrinol. 2019;7:776–785. doi:10.1016/S2213-8587(19)30249-9
24. Ghosh-Swaby OR, Goodman SG, Leiter LA, et al. Glucose-lowering drugs or strategies, atherosclerotic cardiovascular events, and heart failure in people with or at risk of type 2 diabetes: an updated systematic review and meta-analysis of randomised cardiovascular outcome trials. Lancet Diabetes Endocrinol. 2020;8:418–435. doi:10.1016/S2213-8587(20)30038-3
25. Kosiborod MN, Abildstrom SZ, Borlaug BA, et al. Semaglutide in patients with heart failure with preserved ejection fraction and obesity. N Engl J Med. 2023;389:1069–1084. doi:10.1056/NEJMoa2306963
26. Lincoff AM, Brown-Frandsen K, Colhoun HM, et al. Semaglutide and cardiovascular outcomes in obesity without diabetes. N Engl J Med. 2023;389:2221–2232. doi:10.1056/NEJMoa2307563
27. White WB, Cannon CP, Heller SR, et al. Alogliptin after acute coronary syndrome in patients with type 2 diabetes. N Engl J Med. 2013;369:1327–1335. doi:10.1056/NEJMoa1305889
28. Gerstein HC, Colhoun HM, Dagenais GR, et al. Dulaglutide and cardiovascular outcomes in type 2 diabetes (REWIND): a double-blind, randomised placebo-controlled trial. Lancet. 2019;394:121–130. doi:10.1016/S0140-6736(19)31149-3
29. Marso SP, Bain SC, Consoli A, et al. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med. 2016;375:1834–1844. doi:10.1056/NEJMoa1607141
30. Marso SP, Daniels GH, Brown-Frandsen K, et al. Liraglutide and cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2016;375:311–322. doi:10.1056/NEJMoa1603827
31. Vinue A, Navarro J, Herrero-Cervera A, et al. The GLP-1 analogue lixisenatide decreases atherosclerosis in insulin-resistant mice by modulating macrophage phenotype. Diabetologia. 2017;60:1801–1812. doi:10.1007/s00125-017-4330-3
32. Zhao X, Cheng Z, Zhang H, et al. Glucagon-like peptide-1 inhibits the progression of abdominal aortic aneurysm in mice: the earlier, the better. Cardiovasc Drugs Ther. 2024;38:873–884. doi:10.1007/s10557-023-07456-x
33. Giugliano D, Scappaticcio L, Longo M, et al. GLP-1 receptor agonists and cardiorenal outcomes in type 2 diabetes: an updated meta-analysis of eight CVOTs. Cardiovasc Diabetol. 2021;20:189. doi:10.1186/s12933-021-01366-8
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Serum Folic Acid Predicted Pre-Operative Aortic Rupture in Symptomatic Aortic Aneurysm Dissection: A Prospective, Single-Center, Observational Study
Song F, Chen Z, Yang Z, Zou G, Liu B, Li W, Hong Y, Meng J, Zhao G, Bellou A, Li X
International Journal of General Medicine 2025, 18:2417-2427
Published Date: 5 May 2025