Back to Journals » International Journal of General Medicine » Volume 18
Serum Folic Acid Predicted Pre-Operative Aortic Rupture in Symptomatic Aortic Aneurysm Dissection: A Prospective, Single-Center, Observational Study
Authors Song F ![]() , Chen Z, Yang Z, Zou G, Liu B, Li W, Hong Y, Meng J, Zhao G, Bellou A
, Chen Z, Yang Z, Zou G, Liu B, Li W, Hong Y, Meng J, Zhao G, Bellou A ![]() , Li X
, Li X
Received 15 January 2025
Accepted for publication 10 April 2025
Published 5 May 2025 Volume 2025:18 Pages 2417—2427
DOI https://doi.org/10.2147/IJGM.S517646
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Kenneth Adler
Feier Song,1,* Zhengbo Chen,2,* Zhibo Yang,3,* Guoxiang Zou,3 Baojuan Liu,1 Weifeng Li,3 Yimei Hong,1 Jinxiu Meng,4 Gang Zhao,2 Abdelouahab Bellou,5 Xin Li3
1Department of Emergency Medicine and Emergency Intensive Care Unit, Guangdong Provincial People’s Hospital (Guangdong Academy of Medical Sciences), Southern Medical University, Guangzhou, People’s Republic of China; 2Department of Vascular Surgery, Guangdong Provincial People’s Hospital (Guangdong Academy of Medical Sciences), Southern Medical University, Guangzhou, People’s Republic of China; 3Department of Emergency Medicine, Guangdong Provincial People’s Hospital (Guangdong Academy of Medical Sciences), Southern Medical University, Guangzhou, People’s Republic of China; 4Guangdong Provincial Key Laboratory of Coronary Heart Disease Prevention, Guangdong Cardiovascular Institute, Guangdong Provincial People’s Hospital (Guangdong Academy of Medical Sciences), Southern Medical University, Guangzhou, People’s Republic of China; 5Institute of Sciences in Emergency Medicine, Guangdong Provincial People’s Hospital (Guangdong Academy of Medical Sciences), Southern Medical University, Guangzhou, Poeple’s Republic of China
*These authors contributed equally to this work
Correspondence: Gang Zhao, Email [email protected] Xin Li, Email [email protected]
Background and Aims: Folate metabolites have been identified as prognostic markers in cardiovascular, oncologic, and congenital diseases. However, few studies have explored the association between serum folic acid levels and aortic rupture. The aim of this study was to evaluate the predictive value of serum folic acid level for pre-operative adverse events in patients with symptomatic aortic aneurysm/aortic dissection.
Methods and Results: Patients with symptomatic aortic aneurysm/aortic dissection, presenting to the emergency department (ED), were enrolled in the study. Both univariate and multivariate analyses were performed to identify predictors of pre-operative aortic rupture. The optimal cut-off value for folic acid was determined, and a prognostic nomogram was subsequently developed for potential clinical application. Among 639 symptomatic aortic aneurysm/aortic dissection patients, 8.61% experienced rupture prior to surgery/intervention, with a significantly higher incidence observed in patients with higher serum folic acid levels. Multivariate logistic regression analysis revealed that folic acid levels ≥ 9ng/mL were an independent risk factor for pre-operative aortic rupture (OR=2.41). A nomogram was developed based on the combination of Stanford type A aortic dissection, folic acid level, white blood cell count, serum potassium, and random blood glucose, demonstrating excellent discrimination ability with the area under the curve of 0.801.
Conclusion: This large-sample, prospective study suggested that the serum folic acid level was an independent predictor of pre-operative aortic rupture in patients with symptomatic aortic aneurysm/aortic dissection. The developed nomogram highlighted the prognostic value of folic acid and other objective clinical markers, offering a practical tool for early risk stratification, particularly in the ED setting.
Keywords: aortic aneurysm, aortic dissection, folic acid, aortic rupture, predictive model
Introduction
Symptomatic aortic aneurysm/aortic dissection is associated with high mortality due to its pathogenesis, which involves acute alterations to the aortic wall, such as increased wall stress, or hemorrhage within the wall, both of which heighten the risk of aortic rupture.1 In many cases, aneurysms are incidentally detected through medical imaging, often without typical symptoms. When the patients present with pain at the aneurysmal site, differentiating impending rupture from other non-emergent conditions becomes crucial. Rupture at presentation occurred in up to 9.0% of cases of incident aortic syndrome, with a rate of 11.7% in the subgroup of aortic dissection (AD).2 The pre-operative aortic rupture represented a lethal emergency,3 with timely surgical intervention proving to be both effective and safe for most patients. However, in developing countries and regions, some patients may not receive timely or appropriate surgical or interventional treatment. Consequently, identifying high-risk patients with pre-operative aortic rupture is essential for triage and prioritizing treatment.
The folate metabolites have been recognized as important inflammatory prognostic markers in cardiovascular, oncologic, and congenital diseases.4 Elevated plasma total homocysteine levels have been linked to adverse outcomes across a wide range of conditions, including cardiovascular diseases and central nervous system disorders.5 Moreover, serum folic acid levels have been reported to have prognostic value in inflammatory diseases.6 Despite this, folic acid fortification has sparked controversy regarding its effectiveness in preventing major cardiovascular adverse events such as stroke, despite a significant inverse dose–response relationship between the fall in homocysteine after treatment.5
Notwithstanding growing evidence on the use of folic acid and homocysteine as prognostic markers in different cardiovascular diseases, there are no studies assessing their role in patients with aortic aneurysm/aortic dissection. Therefore, the objective of this study was to determine the value of folic acid in predicting preoperative aortic rupture in symptomatic aortic aneurysm/aortic dissection after emergency department (ED) care.
Methods
This observational, prospective cohort study consecutively enrolling patients suspected symptomatic aortic aneurysm or aortic dissection who were admitted to the ED at Guangdong Provincial People’s Hospital in China between June 2020 and October 2022. The hospital served as a referral center for patients with acute cardiovascular emergencies, commonly referred to as a chest pain center. Inclusion criteria were as followed: (1) age ≥18 years; (2) provision of written informed consent; and (3) presentation at the ED with suspected aortic aneurysm or aortic dissection. Exclusion criteria were as followed: (1) missing baseline laboratory data at the ED; (2) non-compliance with the study protocol or medical care; and (3) exclusion of aortic aneurysm or aortic dissection based on enhanced computed tomography (CT) scan.
A series of arterial phase contrast-enhanced images was obtained with thin slice to allow for reconstructions, extending from the thoracic inlet to the level of the femoral arteries, to define the full extent of any dissection or aneurysm.7 The diagnosis of aortic dissection was confirmed by the presence of an intimal flap on an enhanced CT scan,8 using an intravenous iodinated contrast agent. Dissection was classified according to the Stanford classification, with Type A indicating involvement of the ascending aorta and Type B limited to the descending aorta.9 Aortic aneurysm was diagnosed based on the presence of a localized, permanent dilation of the aorta, with the aortic diameter exceeding 1.5 times the normal range value.10 Specifically, an aneurysm was defined when the aortic diameter exceeded 3.0cm in the abdominal aorta and 4.0cm in the ascending aorta or 3.5cm in the descending aorta. Blood samples were collected upon arrival at the ED following standardized procedures. Biomarkers, including serum folic acid and homocysteine, were assayed, along with a complete blood count, serum creatinine, potassium, sodium, calcium concentrations, random blood glucose, and lipid profile. Due to the constraints of the ED setting, detailed assessment of dietary patterns or daily nutritional habits was not feasible. All patients underwent individual management, which included open surgery, endovascular repair, or conservative therapy, as determined by the attending cardiologist or cardiovascular surgeon. The study adhered to the ethical principle outlined in the Declaration of Helsinki and was approved by the institutional ethics committees.
The data collected included clinical information, laboratory tests, imaging findings, and pre-operative outcomes. A venous blood sample was obtained from patients upon admission to the ED. Patients were stratified into quantile groups based on folic acid levels.
All participants were followed up to record pre-operative adverse events. The primary endpoint was the pre-operative aortic rupture. The presence of retroperitoneal and/or intraperitoneal hematoma adjacent to the aneurysm sac on pre-operative CT angiography indicated the rupture of abdominal aorta.11 The rupture thoracic aorta could be either free or contained (including hemothorax, increasing periaortic hematoma, or both, or mediastinal hematoma).7 Secondary endpoints were in-hospital mortality, withdrawal of treatment, and the presence of pre-operative complications (infection, bleeding, renal replacement therapy, liver dysfunction, heart failure, respiratory failure, acute myocardial infarction, heart failure, ischemic stroke, mechanical ventilation, and/or multiple organ dysfunction syndrome). In-hospital mortality was defined as all-cause death during or after the intervention and up to hospital discharge. Acute myocardial infarction was diagnosed according to the fourth universal definition of myocardial infarction.12 Heart failure was characterized by typical symptoms accompanied by signs caused by cardiac abnormality.13 Ischemic stroke was verified via the diagnostic algorithm and testing strategy following the American Heart Association 2021 guidelines.14 Bleeding definitions consisted of both laboratory parameters, such as decreases in hemoglobin and hematocrit scores, and clinical events, including the need for transfusion or surgery, cardiac tamponade, and hematomas. Infection was defined as an illness due to a pathogen or its toxic product, which might induce sepsis. Multiple organ dysfunction syndrome was referred to as the critical illness typified by the dysfunction of two or more organs that occurred simultaneously.15 A renal replacement therapy was employed in place of a patient’s failing or diseased kidney to perform the functions of blood filtration, electrolyte homeostasis, fluid regulation, toxin removal/secretion, and filtrate transport and drainage. Liver dysfunction was defined as hyperbilirubinemia or serum alanine aminotransferase ≥40 U/L.16 Respiratory failure was defined by an arterial oxygen tension (PaO2) of <8.0 kPa (60 mmHg), an arterial carbon dioxide tension (PaCO2) of >6.0 kPa (45 mmHg), or both, or who required mechanical ventilation/noninvasive mechanical ventilation/High Flow nasal Oxygen.17 The data were confirmed via the information available in the electronic medical history.
Statistical Analysis
Continuous variables were expressed as mean and standard deviation or median and interquartile range, according to their distribution. Categorical variables were expressed as absolute and relative frequency. Independent t-tests were performed for normally distributed variables or Wilcoxon tests for non-normal distribution. Categorical variables were analyzed by the chi-square test and Fisher’s Exact Test, as appropriate. Pearson’s correlation coefficient was measured to evaluate the relationship between folic acid and homocysteine. To discriminate independent predictors for aortic rupture, a multivariate analysis was performed using a logistic regression for significant variables identified in the univariate analysis. Significant variables determined by multivariate logistic regression analyses were used to construct the nomogram. The non-linear dose–response association between folic acid and pre-operative aortic rupture was examined. In this study, a complete case analysis was employed. R software (version 4.4.0) was used for data analysis. A p-value <0.05 was considered statistically significant.
Results
Characteristics of Patients
A total of 801 patients with suspected aortic aneurysm/aortic dissection were initially included from the ED during the study period. Of these, 24 patients were excluded after clinical confirmation ruled out the diagnosis of aortic aneurysm or aortic dissection. Additionally, 7 patients were excluded due to lack of follow-up outcomes, and 121 patients were excluded due to missing data on serum folic acid levels. Finally, 10 patients were excluded because of missing essential laboratory results. The final analysis thus included 639 patients with symptomatic, non-ruptured aortic aneurysm/aortic dissection (Figure 1). The study population comprised 512 men (80.13%) and 127 women (19.87%). Median age was 57.22 years (interquartile range (IQR) 25–75%: 47.00–67.15). A total of 375 (58.69%) patients were diagnosed with aortic dissection with Stanford type A, while 217 (33.96%) patients were confirmed with Stanford type B. The remaining 47 (7.36%) patients were classified as abdominal aortic aneurysm, thoracic aortic aneurysm, thoracic-abdominal aortic aneurysm, and penetrating atherosclerotic ulcer. The baseline characteristics of ED visits in the total population (N=639) and among the interquartile folic acid were summarized in Table 1. A significant difference was observed in the ratio of male (p<0.0001), level of homocysteine (p<0.0001), absolute white blood cell (WBC) count (p=0.0002), and neutrophil (p=0.0007). However, there were no significant differences in age and other indexes in complete blood count or comprehensive metabolic panel among interquartile folic acid. Median homocysteine was 13.11 (IQR 25–75%: 9.85–18.76). However, there was no significant correlation between the level of homocysteine and the level of folic acid (p=0.9561, Figure S1).
 |
Table 1 Baseline Characteristics Among Quantile of Folic Acid |
 |
Figure 1 Flowchart of the study. |
Pre-Operative Outcomes
In 17.37% of cases, patients (N=111) underwent endovascular repair, while 39.44% of the individuals (N=252) underwent open repair. The decision to define the type of intervention for each patient depended on the treating physicians/surgeons, according to the surgical risk and the anatomical feasibility of endovascular resolution. Of note, aortic aneurysm/aortic dissection was lethal to 8.14% and might approach 24.10% (plus withdrawal of treatment) of patients who visited the ED in the present study. No significant differences were observed concerning mortality or other pre-operative adverse events among groups, except aortic rupture (Table 2). The most frequent pre-operative complication was infection (23.63%). In total, 49.14% of patients underwent at least one of the adverse events before invasive intervention. About 8.61% (N=55) of the aortic aneurysm/aortic dissection patients were ruptured before the open surgery/endovascular aneurysm repair, and the incidence of aortic rupture was significantly different among interquartile folic acid (p=0.0199). With the increasing level of folic acid, the incidence of aortic rupture grew (from 5.30% to 13.66%).
 |
Table 2 Pre-Operative Adverse Events Among Quantile of Folic Acid |
Predictors of Pre-Operative Aortic Rupture
In the univariate analysis, the variables that were significantly associated with the pre-operative aortic rupture were as follows: folic acid (odds ratio (OR)=1.08 for continuous variable; 95% confidence interval (CI) 1.03–1.14, p=0.0013; OR=1.48 for ordinal variable, 95% CI 1.15–1.94, p=0.0032), red cell distribution width – standard deviation (OR=1.08, 95% CI 1.02–1.15, p=0.0101), WBC count (OR=1.16, 95% CI 1.09–1.23, p<0.0001), neutrophil (OR=1.17, 95% CI 1.10–1.25, p<0.0001), serum potassium (OR=3.05, 95% CI 2.01–4.70, p<0.0001), serum calcium (OR=0.07, 95% CI 0.01–0.47, p=0.0059), and random blood glucose (OR=1.13, 95% CI 1.05–1.23, p=0.0027) (Table S1).
For application in clinical practice, categorization of continuous variables was performed when developing multivariate prediction models (Table 3). After adjustment, AD of Stanford type A (OR=4.26, 95% CI 1.85–9.78, p=0.0006), folic acid≥9ng/mL (OR=2.41, 95% CI 1.30–4.47, p=0.0053), and high WBC count (OR=5.96, 95% CI 1.79–19.82, p=0.0036) were independent risk factors of pre-operative aortic rupture. Regarding biochemical indicators, serum potassium ≥4mmol/L (OR=2.88, 95% CI 1.59–5.23, p=0.0005) and random blood glucose ≥8mmol/L (OR=2.12, 95% CI 1.17–3.84, p=0.0132) were associated with pre-operative aortic rupture.
 |
Table 3 Multivariate Logistic Regression for Pre-Operative Aortic Rupture |
Specifically, receiver operator characteristic analysis using the multivariate model demonstrated a good discrimination ability with an area under curve of 0.801 (Figure 2). Furthermore, a nomogram was developed based on the combination of these 5 independent factors to predict pre-operative aortic rupture (Figure 3).
 |
Figure 2 Receiver Operator Characteristics Curve of Pre-Operative Aortic Rupture Prediction (Area under Curve =0.801). |
 |
Figure 3 The Nomogram for Predicting the Risk of Pre-Operative Aortic Rupture. |
Subgroup Analysis for Sex Difference
Despite its higher prevalence among men (80.13% vs 19.87%), women with aortic aneurysm/aortic dissection have a lower incidence of pre-operative respiratory failure (3.15% vs 8.20%, p=0.0486) and composite adverse events (40.16% vs 51.37%, p=0.0237). Among the study population, similar incidences of other pre-operative adverse events were found between different gender groups (Table S2).
Discussion
Symptomatic aortic aneurysm/aortic dissection is one of the most lethal conditions around the world. Early detection of risk factors could effectively reduce the pre-operative adverse events, including aortic rupture. The present study was the first to evaluate the association between serum folic acid at ED admission and pre-operative aortic rupture in a large sample of patients with symptomatic aortic aneurysm/aortic dissection. In the main, serum folic acid was significantly associated with pre-operative aortic rupture in patients with aortic aneurysm/aortic dissection admitted to the ED. The discriminatory performance to predict pre-operative aortic rupture demonstrated a promising and practical utility when combing other common, cost-saving, and objective markers (such as absolute WBC count, serum potassium, and random blood glucose). Therefore, while the level of serum folic acid ≥9ng/mL was proved to be an independent predictor, the odd ratios escalated along with the level increasing and maximized at approximately 15ng/mL. Notably, Sex difference was observed in the prevalence of symptomatic aortic aneurysm/aortic dissection, as well as in the incidence of pre-operative adverse events.
Controversial evidence emerged about folic acid metabolism on cardiovascular disease. A positive correlation between homocysteine and severity of cerebral disease has been reported,18,19 while there were negative studies as well.20 Sbarouni et al found patients with acute AD present with higher homocysteine and lower folate compared to both chronic aneurysms and controls.21 In the present study, the median level of homocysteine was 13.11 (9.85–18.76) μmol/L. Homocysteine level illustrated a decreasing tendency, while the level of folic acid increased (p<0.0001). However, the linear correlation failed between folic acid and homocysteine. In the baseline characteristics, the level of homocysteine was similar between groups of folic acid 9–13ng/mL and ≥13ng/mL. Also, homocysteine was not associated with pre-operative aortic rupture in the present study. On the contrary to previous studies, increasing folic acid level to lower homocysteine did not show a protective factor on pre-operative aortic rupture. Here, the result should be interpreted with caution. The effectiveness of the folic acid supplement or other homocysteine-lowering therapy on the rather chronic course of cardiovascular diseases, such as atherosclerosis and stroke prevention, was still unclear,22 let alone under the background of the acute phase of aortic disease, such as symptomatic aortic aneurysm/aortic dissection.
The mechanisms of aortic aneurysm/aortic dissection formation were complex. The underlying major pathophysiological mechanisms included inflammation, autophagy, necrosis, and apoptosis, further triggering vascular remodeling characterized by matrix degradation and inflammation, leading to the aggravation of aortic injury.23 Notably, oxidative stress has been shown to play a pivotal role in the formation of aortic aneurysm/aortic dissection.24 Folic acid is a structural component of cells and essential for the regulation of homocysteine, DNA and RNA metabolism, and methylation of multiple proteins.25 Folic acid supplementation modulates several disorders, including atherosclerosis, via its antiapoptotic and antioxidative properties.26–28 Reeps et al evaluated the histopathological changes of the AA wall and 18-F fluorodeoxyglucose (FDG) consumption by positron emission tomography and demonstrated that patients with symptomatic AA presented increased FDG metabolism compared with asymptomatic ones, which significantly correlated with elevated densities of inflammatory infiltrates in biopsies, evidencing a central role of aortic wall inflammation in the etiopathogenesis of symptomatic AA.29 To this extent, it might explain the opposite result of the present study, where the elevated folic acid level was associated with poor prognosis such as rupture in the acute phase of aortic lesion, while folic acid prevented adverse cardiovascular events through homocysteine during a chronic course. From a hypothetical perspective, the elevated folic acid levels might represent a compensatory response rather than a direct causative factor, potentially serving as a physiological reaction to the severe accumulation of inflammatory responses and oxidative stress cascades.
Furthermore, the present study exhibited that increased folic acid, WBCs, serum potassium, and random blood glucose were associated with aortic rupture in the pre-operative period. It would be essential to identify patients at risk in the pre-operative evaluation, to take the necessary precautions, and timely surgical/interventional to avoid complications. Chen et al identified potassium levels outside the interval of 3.5 to 4.5 mmol/L to be a risk factor for both in-hospital and long-term death.30 In the present study, nonspecific inflammatory markers, such as WBCs, showed value as predictors. Several studies consistently suggested WBC as a predictive biomarker for in-hospital rupture in thoracic aortic aneurysm/aortic dissection patients, with the cut-off values from 13 to 15×109/L.31,32 The abovementioned indexes were easily obtained, cost-saving, and objective biomarkers in predicting pre-operative aortic rupture in symptomatic aortic aneurysm/aortic dissection. Finally, a nomogram was established to help make a clinical decision and for patient counseling.
Limitations
First, our analysis was conducted at a single tertiary referral center, which limited the external validity and generalizability of the findings to broader populations, including those seen in primary care settings. While this study represented the first large-scale evaluation of the association between serum folic acid levels and pre-operative aortic rupture in patients with symptomatic aortic aneurysm and aortic dissection, future studies should involve multiple centers across diverse settings to better validate our conclusions. Second, the use of on-admission laboratory results, which represented a snapshot of the patient’s physiological state at a single point in time, introduced potential limitations in capturing the dynamic change in folic acid levels. Longitudinal monitoring of folic acid levels over time would provide deeper insights into the underlying mechanisms. Third, our study lacked detailed imaging parameters, such as the lesion diameter and length of the aortic aneurysm and dissections. Incorporating these imaging features in future studies would allow for a more comprehensive analysis regarding the role of serum folic acid in aortic pathology. Fourth, the rationale for the exclusions potentially introduced selection bias; however, these exclusions accounted for only a small proportion of the total sample. Finally, we did not record the time from symptom onset to aortic rupture, which could have refined the predictive model.
Conclusion
Serum folic acid was a widely available, low-cost biomarker that could be easily assessed in all patients consulting at ED. Serum folic acid level≥9ng/mL was identified as an independent predictor of aortic rupture prior to the invasive intervention. Moreover, Stanford type A AD, WBC count, serum potassium level, and random blood glucose were risk factors for pre-operative aortic rupture. These feasible and objective indexes displayed a potential role in prognosticating symptomatic aortic aneurysm/aortic dissection, offering valuable insights for early risk stratification and clinical decision-making.
Abbreviation
AD, aortic dissection; AA, aortic aneurysm; ED, emergency department; CT, computed tomography; IQR, interquartile range; WBC, white blood cell; OR, odds ratio; CI, confidence interval; FDG, fluorodeoxyglucose.
Funding
This study was funded by the National Key Research and Development Program Intergovernmental Key Projects (2023YFE0114300); The Joint Funds of the Natural Science Foundation of China (No. U24A20652); National Science Foundation of China (No. 82272246); Basic and Applied Basic Research Foundation of Guangdong Province (No.2024A1515012697); Science and Technology Program of Guangzhou, China (No. 202206010044); High-level Hospital Construction Project of Guangdong Provincial People’s Hospital (No. DFJHBF202104).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Soto B, Vila L, Dilme JF, Escudero JR, Bellmunt S, Camacho M. Increased peak wall stress, but not maximum diameter, is associated with symptomatic abdominal aortic aneurysm. Eur J Vasc Endovasc Surg. 2017;54(6):706–711. doi:10.1016/j.ejvs.2017.09.010
2. DeMartino RR, Sen I, Huang Y, et al. Population-based assessment of the incidence of aortic dissection, intramural hematoma, and penetrating ulcer, and its associated mortality from 1995 to 2015. Circ Cardiovasc Qual Outcomes. 2018;11(8):e004689. doi:10.1161/CIRCOUTCOMES.118.004689
3. Mussa FF, Horton JD, Moridzadeh R, Nicholson J, Trimarchi S, Eagle KA. Acute aortic dissection and intramural hematoma: a systematic review. JAMA. 2016;316(7):754–763. doi:10.1001/jama.2016.10026
4. Verhaar MC, Stroes E, Rabelink TJ. Folates and cardiovascular disease. Arterioscler Thromb Vasc Biol. 2002;22(1):6–13. doi:10.1161/hq0102.102190
5. Smith AD, Refsum H. Homocysteine - from disease biomarker to disease prevention. J Intern Med. 2021;290(4):826–854. doi:10.1111/joim.13279
6. Jones P, Lucock M, Scarlett CJ, Veysey M, Beckett EL. Folate and inflammation – links between folate and features of inflammatory conditions. Journal of Nutrition & Intermediary Metabolism. 2019;18:100104. doi:10.1016/j.jnim.2019.100104
7. Writing Committee M, Isselbacher EM, Preventza O, et al. 2022 ACC/AHA guideline for the diagnosis and management of aortic disease: a report of the American Heart Association/American College of Cardiology Joint Committee on clinical practice guidelines. J Am Coll Cardiol. 2022;80(24):e223–e393. doi:10.1016/j.jacc.2022.08.004
8. Rakita D, Newatia A, Hines JJ, Siegel DN, Friedman B. Spectrum of CT findings in rupture and impending rupture of abdominal aortic aneurysms. Radiographics. 2007;27(2):497–507. doi:10.1148/rg.272065026
9. Gomes AS, Bettmann MA, Boxt LM, et al. Acute chest pain–suspected aortic dissection. American College of Radiology. ACR Appropriateness Criteria. Radiology. 2000;215(Supp l):1–5.
10. Group JCSJW. Guidelines for diagnosis and treatment of aortic aneurysm and aortic dissection (JCS 2011): digest version. Circ J. 2013;77(3):789–828. doi:10.1253/circj.CJ-66-0057
11. Mellnick VM, Raptis CA, Heiken JP, Bhalla S. The ruptured abdominal aorta: diagnostics. In: Starnes BW, Mehta M, Veith FJ, editors. Ruptured Abdominal Aortic Aneurysm: The Definitive Manual. Cham: Springer International Publishing; 2017:93–100.
12. Thygesen K, Alpert JS, Jaffe AS, et al. Myocardial TEGobotJESoCACoCAHAWHFTFftUDo: Fourth Universal Definition of Myocardial Infarction (2018). Circulation. 2018;138(20):e618–e651. doi:10.1161/CIR.0000000000000617
13. Ponikowski P, Voors AA, Anker SD, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2016;37(27):2129–2200. doi:10.1093/eurheartj/ehw128
14. Kleindorfer DO, Towfighi A, Chaturvedi S, et al. 2021 guideline for the prevention of stroke in patients with stroke and transient ischemic attack: a guideline from the American Heart Association/American Stroke Association. Stroke. 2021;52(7):e364–e467. doi:10.1161/STR.0000000000000375
15. Chinese Society Of Combining Traditional Chinese and Western Medicine Professional Committee Of Emergency Medicine. [Replacing “Lushan conference in 1995” guideline of the staging diagnosis and severity score standard of multiple organ dysfunction syndrome (2015)]. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2016;28(2):99–101. doi:10.3760/cma.j.issn.2095-4352.2016.02.002
16. Kramer L, Jordan B, Druml W, Bauer P, Metnitz PG. Austrian epidemiologic study on intensive care ASG: incidence and prognosis of early hepatic dysfunction in critically ill patients--a prospective multicenter study. Crit Care Med. 2007;35(4):1099–1104. doi:10.1097/01.CCM.0000259462.97164.A0
17. Roussos C, Koutsoukou A. Respiratory failure. Eur Respir J Suppl. 2003;47:3s–14s. doi:10.1183/09031936.03.00038503
18. Tseng YL, Chang YY, Liu JS, Su CS, Lai SL, Lan MY. Association of plasma homocysteine concentration with cerebral white matter hyperintensity on magnetic resonance images in stroke patients. J Neurol Sci. 2009;284(1–2):36–39. doi:10.1016/j.jns.2009.03.030
19. Rost NS, Rahman R, Sonni S, et al. Determinants of white matter hyperintensity volume in patients with acute ischemic stroke. J Stroke Cerebrovasc Dis. 2010;19(3):230–235. doi:10.1016/j.jstrokecerebrovasdis.2009.05.007
20. Longstreth WT, Katz R, Olson J, et al. Plasma total homocysteine levels and cranial magnetic resonance imaging findings in elderly persons: the Cardiovascular Health Study. Arch Neurol. 2004;61(1):67–72. doi:10.1001/archneur.61.1.67
21. Sbarouni E, Georgiadou P, Analitis A, et al. High homocysteine and low folate concentrations in acute aortic dissection. Int J Cardiol. 2013;168(1):463–466. doi:10.1016/j.ijcard.2012.09.127
22. Yang H-T, Lee M, Hong K-S, Ovbiagele B, Saver JL. Efficacy of folic acid supplementation in cardiovascular disease prevention: an updated meta-analysis of randomized controlled trials. European Journal of Internal Medicine. 2012;23(8):745–754. doi:10.1016/j.ejim.2012.07.004
23. Wang Y, Gao P, Li F, Du J. Insights on aortic aneurysm and dissection: role of the extracellular environment in vascular homeostasis. J mol Cell Cardiol. 2022;171:90–101. doi:10.1016/j.yjmcc.2022.06.010
24. Davis FM, Rateri DL, Daugherty A. Abdominal aortic aneurysm: novel mechanisms and therapies. Curr Opin Cardiol. 2015;30(6):566–573. doi:10.1097/HCO.0000000000000216
25. Ponziani FR, Cazzato IA, Danese S, et al. Folate in gastrointestinal health and disease. Eur Rev Med Pharmacol Sci. 2012;16(3):376–385.
26. Chen TF, Chiu MJ, Huang CT, et al. Changes in dietary folate intake differentially affect oxidised lipid and mitochondrial DNA damage in various brain regions of rats in the absence/presence of intracerebroventricularly injected amyloid beta-peptide challenge. Br J Nutr. 2011;105(9):1294–1302. doi:10.1017/S0007114510005052
27. Li W, Liu H, Yu M, et al. Folic acid alters methylation profile of JAK-STAT and long-term depression signaling pathways in Alzheimer’s disease models. mol Neurobiol. 2016;53(9):6548–6556. doi:10.1007/s12035-015-9556-9
28. Feng Y, Wang S, Chen R, Tong X, Wu Z, Mo X. Maternal folic acid supplementation and the risk of congenital heart defects in offspring: a meta-analysis of epidemiological observational studies. Sci Rep. 2015;5:8506. doi:10.1038/srep08506
29. Reeps C, Essler M, Pelisek J, Seidl S, Eckstein HH, Krause BJ. Increased 18F-fluorodeoxyglucose uptake in abdominal aortic aneurysms in positron emission/computed tomography is associated with inflammation, aortic wall instability, and acute symptoms. J Vasc Surg. 2008;48(2):417–423;discussion424. doi:10.1016/j.jvs.2008.03.059
30. Chen Z, Huang B, Lu H, et al. The effect of admission serum potassium levels on in-hospital and long-term mortality in type A acute aortic dissection. Clin Biochem. 2017;50(15):843–850. doi:10.1016/j.clinbiochem.2017.05.008
31. Wu J, Qiu J, Xie E, et al. Predicting in-hospital rupture of type A aortic dissection using Random Forest. J Thorac Dis. 2019;11(11):4634–4646. doi:10.21037/jtd.2019.10.82
32. Li M, Xu S, Yan Y, et al. Association of biomarkers related to preoperative inflammatory and coagulation with postoperative in-hospital deaths in patients with type A acute aortic dissection. Sci Rep. 2021;11(1):18775. doi:10.1038/s41598-021-98298-w
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
GLP-1 Receptor Agonists Reduce Aortic Dissection and Hypertensive Crisis in Diabetic Patients with Aortic Aneurysm: A Retrospective Cohort Study
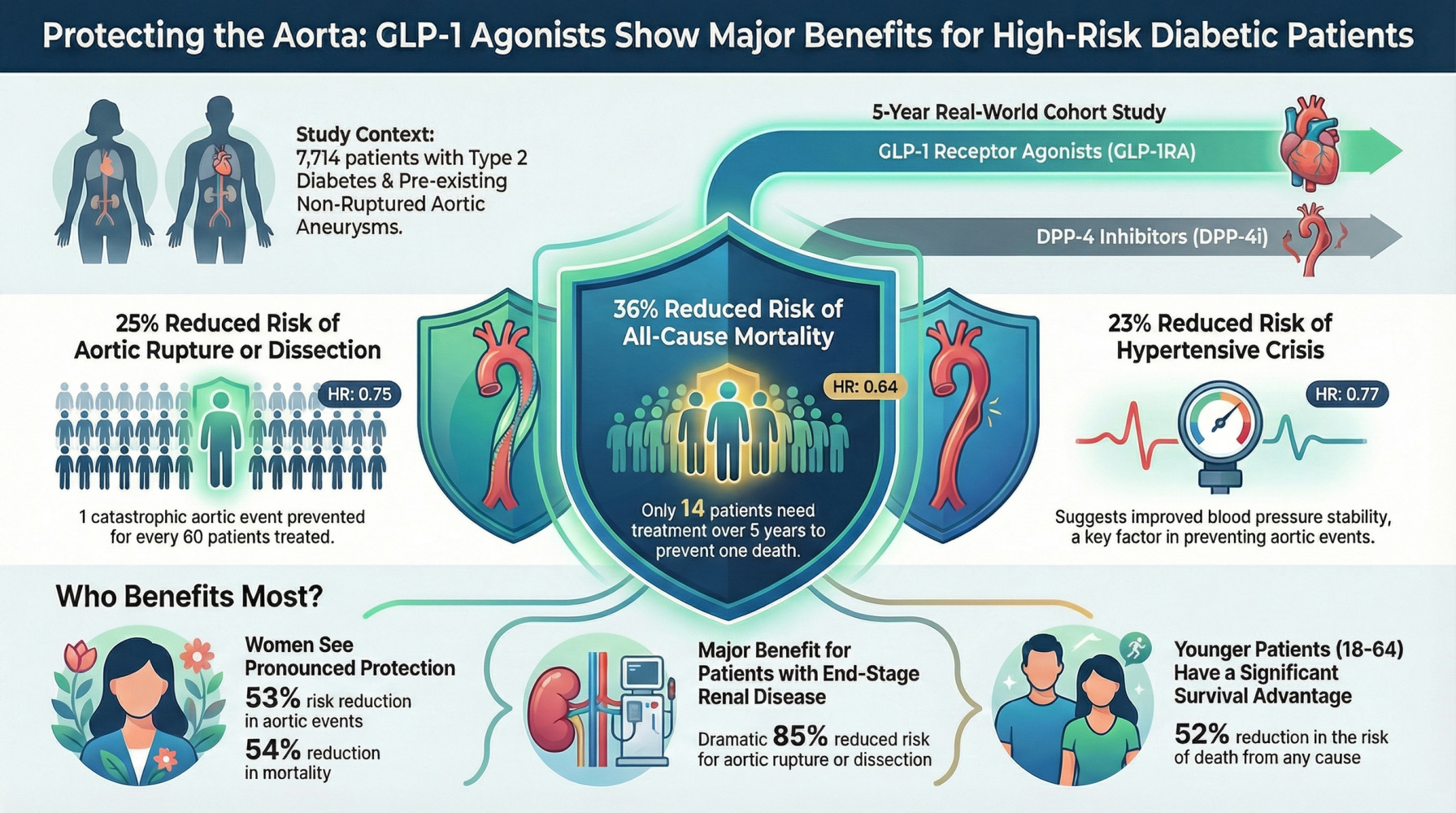
Tsai YF, Lin HT, Liu YF, Chang R, Wu SC
Diabetes, Metabolic Syndrome and Obesity 2026, 19:612622
Published Date: 23 May 2026